Submitted:
17 January 2024
Posted:
18 January 2024
You are already at the latest version
Abstract
Primary bone lymphoma of the scapula is a rare tumor that usually causes local pain. Presented patient suffered for two years from paresthesia, tingling, numbness, and edema of the little and ring finger. The 45-year-old man underwent several radiological and neurological assessments of the palm, elbow and neck prior to radiographs revealing the tumor of the left shoulder. Once diffuse large B cell lymphoma was confirmed, immunochemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and methylprednisolone (R-CHOP) started. The treatment was accompanied by antiviral treatment with lamivudine due to positive hepatitis B virus serology and with bisphosphonate treatment for the prevention of bone resorption. Once immunochemotherapy was finished, the treatment was supplemented by radiotherapy of the shoulder. After more than three years of accomplishing remission, the patient had an ischemic stroke manifesting with right-sided hemiparesis. Following the physical therapy, the patient is currently in the process of evaluation for thrombophilia, as well as further cardiac assessment due to the positive transcranial Doppler bubble test setting high suspicion for the presence of patent foramen ovale.
Keywords:
Primary bone lymphoma
; scapula
; diffuse large B cell lymphoma
; immunochemotherapy
; radiotherapy
1. Introduction
Primary non-Hodgkin lymphoma of the bone is a rare subtype accounting for less than 1% of non-Hodgkin lymphomas (NHL) and approximately 5% of all primary extranodal NHL [1]. We present an uncommon case significant for the localization and clinical presentation of the tumor causing significant delay in diagnosis and treatment, patient’s comorbidities, and specificity of the therapeutic approach.
2. Case Report
A 45-year-old patient reported paresthesia, tingling, numbness, and edema of the little and ring finger of the left hand in mid-2016. Because of inconspicuous clinical presentation, the patient was sent to physical therapy. After it failed, he was referred to a neurologist in August 2016. Neurological examination found a weakened left-hand grip together with weakened small finger abduction and opposition. Also, a positive Tinel sign of the left hand was observed, and the clinical diagnosis of the cubital tunnel syndrome was established. Cervical spine and left elbow X-rays were done, together with electromyoneurography (EMNG) of the arms. As the tests showed normal results, the patient was referred to magnetic resonance imaging (MRI) of the cervical spine and X-ray of the left palm The X-ray findings were normal, while MRI demonstrated subtle signs of C5-C6 level compressive radiculopathy. The patient underwent MRI of the left elbow and left wrist in September 2016. Indirect signs of ulnar nerve neuropathy in the cubital canal were registered – hyperintense nerve signal on T2 and STIR sequences. The instability of the central carpal area was also noted. The EMNG, performed in July 2017, showed no pathology progression in comparison to the earlier one, without clear-cut criteria matched for focal ulnar neuropathy. Finally, as the symptoms did not improve, X-ray images of the patient’s shoulder were obtained at the end of June 2018 (Figure 1). Within the next month, multi-slice computed tomography (MSCT) and MRI of the left shoulder were obtained. MSCT of the left shoulder confirmed the presence of multiple osteolytic lesions with lamellar periosteal reaction and sporadic cortical breaches in the left scapula. MRI of the left shoulder (Figure 2) confirmed the suspicion of a neoplastic process of the left scapula and the need for further orthopedic and diagnostic evaluation. An orthopedic examination revealed a normal range of motion of the left shoulder and positive signs of ulnar nerve compression in the cubital canal of the elbow. Scintigraphy showed an intensified technetium-99 m accumulation in the left scapula. An incisional biopsy of the suspicious lesion was performed at the end of August 2018. Sample morphology demonstrated neoplastic tissue erected from large, atypical, lymphatic cell-type centroblasts. Immunohistochemically, tumor cells were positive for markers such as the cluster of differentiation (CD) CD20, CD10 and B-cell lymphoma 6 (BCL6), C-Myc was positive in around 35% of tumor cells andKi-67 was 80%. Biopsy findings confirmed the clinical diagnosis of non-Hodgkin lymphoma (NHL), Diffuse Large B Cell Lymphoma (DLBCL), germ-cell phenotype (GCB), stage IV. The patient did not have the „B“ symptoms. Treatment with rituximab, cyclophosphamide, doxorubicin, vincristine, and methylprednisolone (R-CHOP) immunochemotherapy started at the end of September 2018. Bisphosphonate zoledronic acid (ZA) for the prevention of bone resorption was given monthly for the next two years. Because of the positive hepatitis B virus (HBV) serology, lamivudine was introduced during R-CHOP treatment to prevent HBV reactivation for one year. Interim Positron Emission Tomography - CT (PET-CT), done in January 2019, showed areas of mixed sclerotic and osteolytic lesions with a slightly higher metabolic activity in the left scapula. No lymphadenopathy was observed. After six cycles of CHOP chemotherapy (final at the end of January 2019) and eight doses of rituximab immunotherapy (final in April 2019), the end of treatment PET-CT was done in May 2019. It has shown no differences compared to the previous PET-CT. Radiotherapy of the left scapula with 30 Gy in 15 fractions was completed in July 2019.
The patient continued follow-up at the outpatient clinic. Light paresthesia and tingling in feet and hands subsided in the period between the two follow-ups. Control PET-CT was repeated in November 2019. There was no pathological, metabolic activity of the fluorodeoxyglucose. After one and two years, the patient terminated lamivudine and ZA consecutively. The patient had a follow-up by a neurologist in October 2020 due to paresthesia in both forearms and lower legs. The physical exam presented the loss of sensation for the crude touch and temperature in the distal parts of the legs and arms. The sensation of vibration was preserved, and no accompanying motoric weaknesses were present. Clinical diagnosis of polyneuropathy was determined, presumably toxic neuropathy mostly due to vincristine. The patient was ordered for EMNG which showed some signs possible for smaller, myelinated fiber neuropathy. The patient refused therapy for his mild neurologic symptoms. During the regular follow-up in May 2021, the patient reported right axillar lymphadenopathy. He underwent ultrasound-guided fine needle aspiration cytology which showed reactive proliferation. The lymphadenopathy appeared 2 weeks after the coronavirus disease 2019 vaccine, and a few weeks later completely resolved. The patient also had an exam by an orthopedic specialist because of straining and tightening in the left shoulder when he was physically active. Although significantly less pronounced than before hematologic treatment, paresthesia and tingling in the little finger of the left hand were still present. The function of the shoulder was minimally affected as there was only terminal restriction of external rotation and slightly decreased strength of internal and external shoulder rotation. Noteworthy information from the patient’s history is Baker cyst and pigmented villonodular synovitis of the right knee. More than twenty years ago, an open synovectomy of the right knee was done. Despite the remission, during mid-2023 the patient developed right-sided hemiparesis and sensory impairment with the diagnosis of the ischemic stroke. Acetylsalicylic acid and atorvastatin were introduced in therapy. Afterward, the patient successfully passed the rehabilitation period with significant recovery in motor and sensory function. The patient is currently in the process of evaluation for thrombophilia. Also, the patient underwent a transcranial Doppler bubble test which came positive, indicating the existence of a patent foramen ovale. Further cardiac assessment is being planned.
3. Discussion
The unique clinical presentation including paresthesia and edema of the little and ring finger of the left hand caused a delay in diagnosis for more than 2 years. Regardless of atypical primary non-Hodgkin lymphoma of the bone localization - scapula without lymph node involvement, and unusual presentation, appropriate treatment (R-CHOP + radiotherapy) in addition to lamivudine for HBV and bisphosphonates for prevention of bone resorption resulted in complete remission of DLBCL without concomitant complications.
DLBCL is one of the most common types of NHL, with a crude incidence in Europe of 3.8/100 000/year [1]. A broad spectrum of risk factors for DLBCL development includes genetics, autoimmune pathology, infections, and occupational exposures (mostly agricultural such as fungicide Captafol, herbicide Paraquat and Radon gas) [2,3]. Aside from our patient who had asymptomatic HBV infection, to our knowledge, there were only two other reported cases of DLBCL in the shoulder area with known underlying risk factors [4,5]. The risk factors included human immunodeficiency virus (HIV) infection in the first, and rheumatoid arthritis in the second case.
Most DLBCLs originate in lymph nodes, but ≤ 40% are of extranodal origin [1]. The most common site of extranodal origin is the gastrointestinal tract, but other organs such as testicles, central nervous system and bones can also be affected. The most common osseous localization of extranodal DLBCL are femur, pelvic bones, and spine. To our knowledge, there were only 5 cases of the primary extranodal DLBCL [6,7,8,9,10], without regional lymph node involvement, located in the osseous area of the scapula (Table 1).
It was found that patients treated for DLBCL usually wait for 4 weeks before they seek medical attention and 8 weeks before non-hematology physicians diagnose DLBCL and refer them to a hematologist [11]. Patients with DLBCL localized in the scapula mostly presented with shoulder pain and localized swelling that is consistent with the usual presentation of primary bone lymphoma [12]. Unusual clinical presentation with paresthesia and edema of the little and ring finger on the left hand is unique among patients with osseous DLBCL in the shoulder region. The shortest distance between the DLBCL infiltrate and the distal part of the brachial plexus in our patient was measured to be 33 mm (Figure 2C,D). Due to such a long distance, it is hard to correlate the patient’s neurologic symptoms with the DLBCL infiltration, but the fact that symptoms significantly decreased following hematologic treatment remains.
The delay in diagnosis of DLBCL in our patient was significantly longer (more than 2 years) compared to the average 3 months. As it did not affect the success of treatment in our patient that confirmed the finding that the delay in diagnosis of DLBCL does not impact the outcome [11]. Other than the cell of origin classification, an array of prognostic factors which, if present are associated with poor outcome, include higher age (> 60 years), immunoblastic subtype, presence of pathological fracture and high-grade B-cell lymphomas [13]. Our patient has had a National Comprehensive Cancer Network International Prognostic Index score of 2, which means he belongs to a low-intermediate risk group with an estimated 5-year progression-free survival of 74% and an estimated 5-year overall survival of 82%.
Any bone lesion detected in patients above 40 years old must be ruled out for metastasis and myeloma [14]. Prominent periosteal reaction in our patient was in contrast with earlier findings which associate a higher degree of bone destruction and periosteal reaction with osteosarcoma and Ewing sarcoma [15]. As a result of treatment, persisting bone changes during follow-ups caused difficulty in differentiating between active, malignant disease and bone healing. Signal abnormalities on MRI may persist for up to 2 years, while bone remodeling seen on CT has similarities with Paget’s disease [16]. PET-CT become one of the most reliable sources for treatment response. In case of interim PET-CT positive findings, repeated biopsy of residual masses should be considered [17].
Approximately 20-50% of patients with HBsAg positivity and 3-45% of patients with HbcAb positivity develop HBV reactivation following chemotherapy [18]. The risk for reactivation is twofold higher if patients are managed on rituximab compared to chemotherapy alone [19]. Pre-emptive lamivudine therapy is the main therapy treatment, and it provides much lower HBV reactivation rates compared to starting antiviral treatment after reactivation has already begun [13]. Our patient continued receiving lamivudine for one year, which is longer than the current guidelines recommendation which advises 3-6 months [20]. Two questions concerning such lamivudin application are the risk of HBV-reactivation after the lamivudin withdrawal and HBV DNA mutation induction which can cause the hepatitis flare [21]. Neither one occurred in the patient following cessation of lamivudine treatment.
In addition to the antiresorptive effect, ZA has a potential antiangiogenic effect by decreasing basal serum vascular endothelial growth factor for the next three weeks and decreasing platelet-derived growth factor for the next two days [22]. Its anti-tumor effect is not so distinctive. ZA was able to induce tumor cell apoptosis in vitro but concentrations needed for that were 10-100x higher than those used in osteoclast apoptosis induction in vitro and in vivo. Another impediment to ZA’s anti-tumor effect in extra-skeletal sites is its pharmacokinetics - rapid elimination from plasma resulting from renal excretion and rapid uptake and accumulation within bone [23]. A relatively recent study performed on patients with DLBCL and bone metastasis exhibited no difference in OS, progression free-survival and complete remission rate in patients treated with ZA compared to the control group [24]. On the other hand, the systematic review and meta-analysis of ZA in patients with metastatic breast cancer concluded that ZA use as adjuvant therapy has a significant impact on the patient’s overall survival and lower fracture rate. The positive outcome was not present after ZA usage for disease-free survival compared to the control group [25]. Currently, the standard interval dosage is 4 weeks. The research conducted a few years ago indicated no difference in pain occurrence or skeletal-related events when patients received bisphosphonate therapy every 12 weeks compared to the standard 4-week interval [26].
Although the patient is currently in the evaluation process regarding thrombophilia, initial laboratory results did not show any signs of hypercoagulability. Despite unremarkable results, according to Iversen et al., patients with NHL suffer from a chronic state of hypercoagulation and have an elevated risk of thromboembolic events [27]. According to Negaard et al. [28], higher coagulation markers were associated with the type of lymphoma and the patient’s remission status.
4. Conclusions
In conclusion, primary neurological symptoms that cannot be explained by neurological and radiological examinations require further investigation of the locomotor system. In the case of underlying lymphoma, a combination of chemoimmunotherapy and radiotherapy is related to high complete remission rates.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vitolo U, Seymour JF, Martelli M, Illerhaus G, Illidge T, Zucca E, et al. Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v91-v102. [CrossRef]
- Ferri GM, Specchia G, Mazza P, Ingravallo G, Intranuovo G, Guastadisegno CM, et al. Risk of lymphoma subtypes by occupational exposure in Southern Italy. J Occup Med Toxicol. doi: 2017;1231. [CrossRef]
- Morton LM, Slager SL, Cerhan JR, Wang SS, Vajdic CM, Skibola CF, et al. Etiologic heterogeneity among non-Hodgkin lymphoma subtypes: the InterLymph Non-Hodgkin Lymphoma Subtypes Project.J Natl Cancer Inst Monogr. 2014;2014(48):130-144. [CrossRef]
- Non-Hodgkin’s lymphoma as an unexpected diagnosis in a shoulder arthroplasty. J Arthroplasty. 1999;14(1):108-111. [CrossRef]
- Chauhan NR, Chick JF, Khurana B. Annihilation of the acromion: a rare case of primary scapular lymphoma. J Emerg Med. 2013;44(6):e389-390. [CrossRef]
- Carroll G, Breidahl W, Robbins P. Musculoskeletal lymphoma: MRI of bone or soft tissue presentations. J Med Imaging Radiat Oncol. 2013;57(6):663–73. [CrossRef]
- Boulytcheva IV, Sciotto C, Soloviev Y., Kushlinskii NE. Diffuse large B-cell lymphoma presented as bone lesions. A study of 21 cases and review of the literature. Кoллектив автoрoв. 2013;44–7.
- Das DK, Pathan SK, Al-Waheeb SKM, Ali AE, Joneja M, Al-Kanderi MG, et al. Chest wall lymphomas: fine needle aspiration cytodiagnosis and review of the literature. Cytopathology. 2017;28(5):364–70. [CrossRef]
- Yousef MHAH, Audat Z, Al-Shorafat DM, Al-Khatib S, Daoud AK. Primary za.
- of bone: a single-center experience. J Blood Med. 2022;13:143–9. [CrossRef]
- Nikonova A, Guirguis HR, Buckstein R, Cheung MC. Predictors of delay in diagnosis and treatment in diffuse large B-cell lymphoma and impact on survival. Br J Haematol. 2015;168(4):492-500. [CrossRef]
- Messina C, Christie D, Zucca E, Gospodarowicz M, Ferreri AJ. Primary and secondary bone lymphomas. Cancer Treat Rev. 2015;41(3):235-246. [CrossRef]
- Zelenetz AD, Gordon LI, Chang JE, Christian B, Abramson JS, Advani RH, et al. NCCN guidelines(R) insights: B-cell lymphomas, version 5.2021. J Natl Compr Canc Netw. 2021;19(11):1218-1230. [CrossRef]
- Subramanian S, Viswanathan VK. Lytic bone lesions. StatPearls (electronic book section). Treasure Island (FL): StatPearls Publishing; 2022.
- Häussler MD, Fenstermacher MJ, Johnston DA, Harle TS. MRI of primary lymphoma of bone: cortical disorder as a criterion for differential diagnosis. J Magn Reson Imaging. 1999;9(1):93-100. [CrossRef]
- Mengiardi B, Honegger H, Hodler J, Exner UG, Csherhati MD, Brühlmann W. Primary lymphoma of bone: MRI and CT characteristics during and after successful treatment. AJR Am J Roentgenol. 2005;184(1):185-192. [CrossRef]
- Dabaja BS, Vanderplas AM, Crosby-Thompson AL, Abel GA, Czuczman MS, Friedberg JW, et al. Radiation for diffuse large B-cell lymphoma in the rituximab era: analysis of the National Comprehensive Cancer Network lymphoma outcomes project. Cancer. 2015;121(7):1032-1039. [CrossRef]
- Huang H, Li X, Zhu J, Ye S, Zhang H, Wang W, et al. Entecavir vs lamivudine for prevention of hepatitis B virus reactivation among patients with untreated diffuse large B-cell lymphoma receiving R-CHOP chemotherapy: a randomized clinical trial. JAMA. 2014;312(23):2521-2530. [CrossRef]
- Dong HJ, Ni LN, Sheng GF, Song HL, Xu JZ, Ling Y. Risk of hepatitis B virus (HBV) reactivation in non-Hodgkin lymphoma patients receiving rituximab-chemotherapy: a meta-analysis. J Clin Virol. 2013;57(3):209-214. [CrossRef]
- Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50(3):661-662. [CrossRef]
- Gutfreund KS, Williams M, George R, Bain VG, Ma MM, Yoshida EM, et al. Genotypic succession of mutations of the hepatitis B virus polymerase associated with lamivudine resistance. J Hepatol. 2000;33(3):469-475. [CrossRef]
- Santini D, Vincenzi B, Dicuonzo G, Avvisati G, Massacesi C, Battistoni F, et al. Zoledronic acid induces significant and long-lasting modifications of circulating angiogenic factors in cancer patients. Clin Cancer Res. 2003;9(8):2893-2897.
- Winter MC, Holen I, Coleman RE. Exploring the anti-tumour activity of bisphosphonates in early breast cancer. Cancer Treat Rev. 2008;34(5):453-475. [CrossRef]
- Inoue N, Nishimura N, Takahashi A, Kusano Y, Yamauchi H, Ueda K, et al. Negative impact of zoledronic acid in R-CHOP treated DLBCL with bone metastasis. Hematol Oncol. 2017;35(S2):340–1. [CrossRef]
- Valachis A, Polyzos NP, Coleman RE, Gnant M, Eidtmann H, Brufsky AM, et al. Adjuvant therapy with zoledronic acid in patients with breast cancer:asystematic review and meta-analysis.Oncologist.2013;18(4):353-361. [CrossRef]
- Himelstein AL, Foster JC, Khatcheressian JL, Roberts JD, Seisler DK, Novotny PJ, et al. Effect of longer-interval vs standard dosing of zoledronic acid on skeletal events in patients with bone metastases: a randomized clinical trial. JAMA. 2017;317(1):48-58. [CrossRef]
- Iversen PO, Negaard H, Østenstad B, Sandset PM, Kolset SO. Evidence for long-term hypercoagulopathy, but normalization of markers of extracellular matrix turnover, in patients with non-Hodgkin lymphoma. Vol. 56, Leukemia and Lymphoma. 2015. p. 2479–81. [CrossRef]
- Negaard HFS, Iversen PO, Østenstad B, Iversen N, Holme PA, Sandset PM. Hypercoagulability in patients with haematological neoplasia: No apparent initiation by tissue factor. Thromb Haemost. 2008;99(6):1040–8. [CrossRef]
Figure 1.
X-rays, anteroposterior (AP) view of the left shoulder. Multiple areas of decreased bone mineralization and multifocal osteolytic lesions are seen in the left scapula with an area of breached cortical bone in the inferior part of the scapular neck.
Figure 1.
X-rays, anteroposterior (AP) view of the left shoulder. Multiple areas of decreased bone mineralization and multifocal osteolytic lesions are seen in the left scapula with an area of breached cortical bone in the inferior part of the scapular neck.
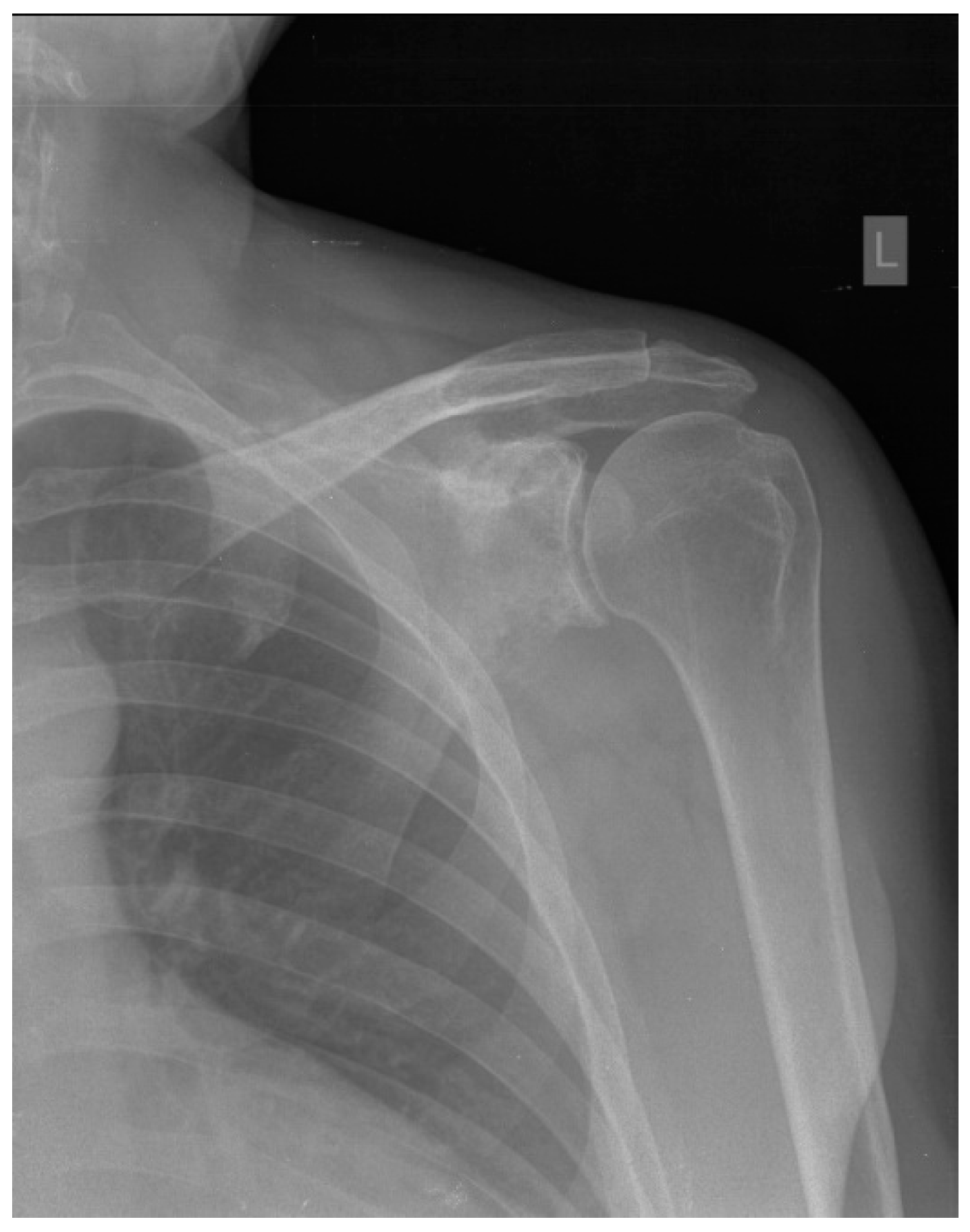
Figure 2.
Magnetic resonance imaging (MRI) of the left shoulder. A, B) Coronal short tau inversion recovery sequence images show extensive osteolytic, partly multilocular scapular lesions involving the lateral corpus, coracoid process, acromion, glenoid and spina with periosteal reaction and destruction of cortical bone with extraosseous spread to surrounding soft tissue. No signs of infiltration of the surrounding muscles. C) Axial T1 weighted and D) axial proton density weighted fat saturated images show no signs of infiltration of the brachial plexus. The shortest distance between the distal part of the brachial plexus and the tumor is 33 mm. The rotator cuff tendons and the long head of biceps tendon are unremarkable. No signs of glenohumeral joint effusion or significant labral abnormalities.
Figure 2.
Magnetic resonance imaging (MRI) of the left shoulder. A, B) Coronal short tau inversion recovery sequence images show extensive osteolytic, partly multilocular scapular lesions involving the lateral corpus, coracoid process, acromion, glenoid and spina with periosteal reaction and destruction of cortical bone with extraosseous spread to surrounding soft tissue. No signs of infiltration of the surrounding muscles. C) Axial T1 weighted and D) axial proton density weighted fat saturated images show no signs of infiltration of the brachial plexus. The shortest distance between the distal part of the brachial plexus and the tumor is 33 mm. The rotator cuff tendons and the long head of biceps tendon are unremarkable. No signs of glenohumeral joint effusion or significant labral abnormalities.
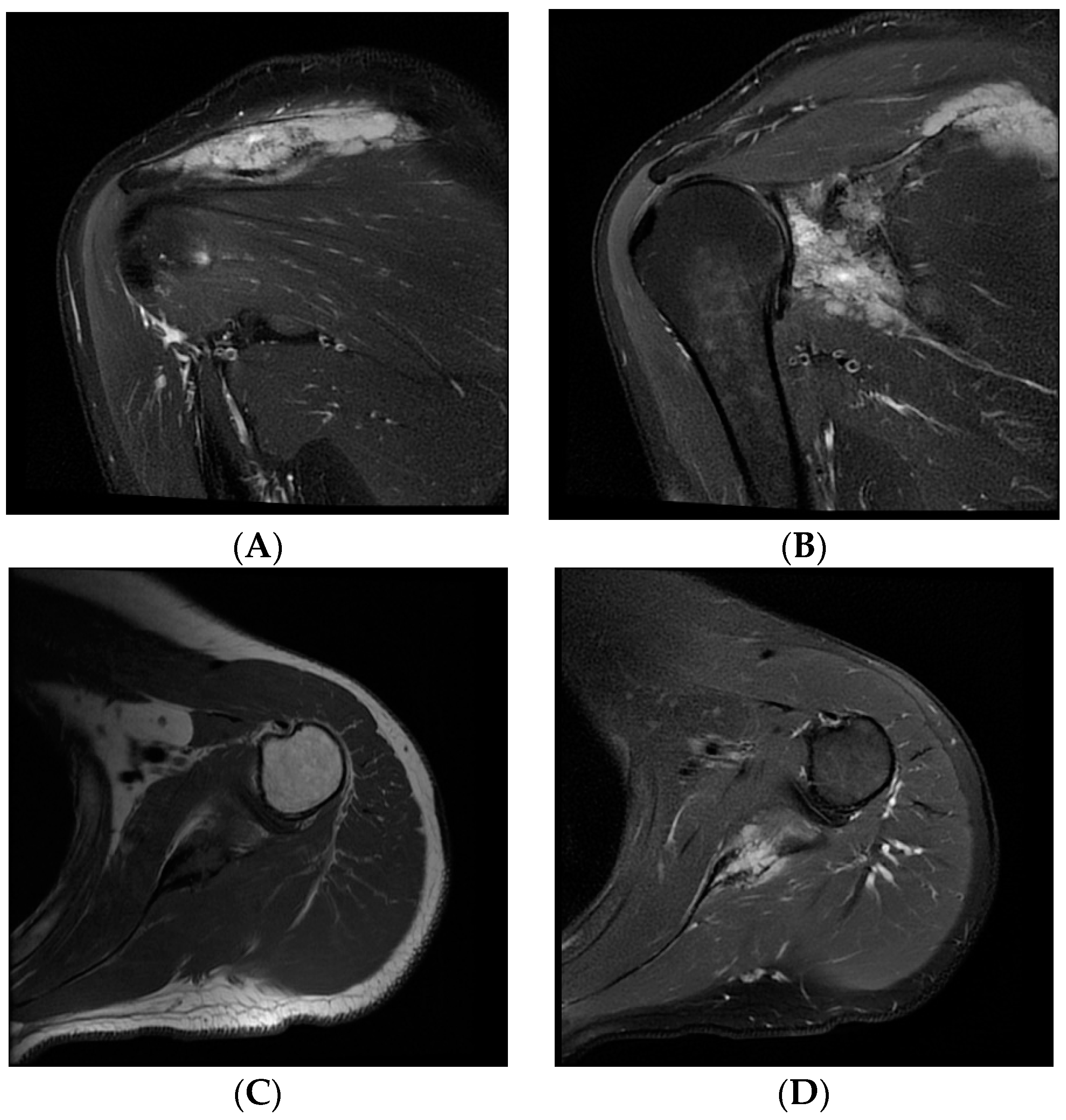

Table 1.
Patients with extranodal Diffuse Large B Cell Lymphoma (DLBCL) localized only in scapula listed by the year of publication.
Table 1.
Patients with extranodal Diffuse Large B Cell Lymphoma (DLBCL) localized only in scapula listed by the year of publication.
| 1st author and year of publication | Sex/age | Presentation | Time between symptoms onset and diagnosis / Time between first hospital visit and diagnosis | Involvement of other sites | Treatment | Outcome |
| Chauhan [6], 2013 | F/84y | Pain | Two months/ days-weeks |
Surrounding soft tissue | R-CHOP chemotherapy | Remission |
| Carroll [7], 2013 |
M/29y | Lump | Nd/Nd | Nd | Nd | Nd |
| Boulytcheva [8], 2013 | F/73y | Nd | Nd | Nd | Radiotherapy | Death |
| Das [9], 2017 | M/73y | Nd | Nd | Nd | Nd | Nd |
| Ayesh Haj Yousef [10], 2022 | F/46y | Mass | Two months/ Nd | Nd | R-CHOP chemotherapy + radiotherapy |
Remission |
| Our patient | M/45y | Paresthesia, tingling, numbness and edema of the little and ring finger | Two years/ two years |
Surrounding soft tissue | R-CHOP chemotherapy + radiotherapy | Remission |
Note: F - female; M - male; Nd - not disclosed; y – years; R-CHOP - rituximab, cyclophosphamide, doxorubicin, vincristine, and methylprednisolone.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



