Submitted:
13 January 2024
Posted:
15 January 2024
You are already at the latest version
Abstract
Cadmium (Cd) is an environmental toxicant of worldwide public health significance. Diet is the main non-workplace Cd exposure source other than smoking. The intestinal absorption of Cd involves the transporters for iron, zinc, copper, and calcium. These metal transporters essentially determine the body burden of Cd because only 0.001-0.005% of Cd accumulated in the body can be excreted in urine each day. The International Agency for Research on Cancer listed Cd as a human lung carcinogen. Current evidence, however, suggests that environmental Cd may increase the prevalence of many types of cancer, notably lung, liver, breast, pancreas, and kidney. A two-year bioassay that mimics a lifelong exposure demonstrates Cd caused neoplasms in multiple tissues of mice. Also, several non-tumorigenic human cell lines underwent malignant cell transformation, when they were exposed to a sublethal dose of Cd for a prolonged time. Cd does not directly damage DNA, but it can profoundly affect gene expression through its interactions with various proteins, and Cd can thus be viewed as a transcription modulator. The present review highlights epidemiological studies that connected an enhanced risk of various neoplastic diseases to chronic exposure to environmental Cd. Special emphasis is on the impact of body iron stores on the absorption rate of Cd, and its implications for breast cancer prevention in highly susceptible subpopulation groups of women. Resistance to cell death and other cancer phenotypes acquired during Cd-induced cancer-cell transformation, under in vitro conditions, are briefly discussed. The potential role for ZnT1 efflux transporter in cellular acquisition of tolerance to Cd cytotoxicity are highlighted.
Keywords:
cadmium
; cancer
; cell transformation
; copper
; intestinal absorption
; iron store status
; zinc transporters
1. Introduction
Cadmium (Cd) is a metal with no nutritional or physiological value in humans, but it is found in most people because it is a contaminant in nearly all food types, as such dietary exposure is unavoidable for most people [1,2,3,4,5]. Cigarette smoke is an additional non-workplace Cd exposure source [6]. Airborne Cd is increasingly detectable, especially in urban areas of many countries [7]. Consequently, an inhalation exposure and the existence of a nose-to-brain entry route cause a further concern [8,9].
Cd exists primarily in a divalent state (Cd2+), and as a redox inert metal, it does not undergo valency change [10,11]. However, compared to an essential metal zinc (Zn2+), Cd has a higher binding affinity for sulfur ligands that include the thiol (-SH) functional group of glutathione, zinc-finger transcription factors, and many other proteins [10,11,12,13]. It is well documented that Cd interacts with the cysteine thiols of metallothionine (MT), a group of low molecular-weight protein, capable of sequestering zinc, copper, and Cd [11,12,13]. Also, Cd induces mitochondrial dysfunction, but it does not directly damage DNA [14,15]. Likely, the manifestation of carcinogenic effects of Cd are through its interactions with essential metals, and proteins, i.e., DNA repair enzymes [14,15,16]. Cd is viewed as a modulator of human gene transcription [15]
Chronic exposure to Cd produces a broad range of adverse health effects. This is evident from epidemiological studies that link an incremental risk of infertility, cancer, diabetes, chronic kidney disease, osteoporosis, non-alcoholic fatty liver disease to Cd exposure in the general populations of many countries [1]. The overall health impact of Cd comes from cohort studies which implicate Cd exposure in an increased mortality from all causes [17,18,19,20], heart failure [21,22], and cancer [23,24].
An elevated Cd body burden, smoking, low-level physical activity, and low serum antioxidant nutrient lycopene were found to be associated with an increase in deaths from all causes in the United States [16]. These modifiable mortality risk factors were identified from an analysis of 249 health indicators, included in the U.S. general population studies, known as the National Health and Nutrition Examination Survey (NHANES) [17].
Notably, Cd was found, through mediation analysis, to be responsible for most adverse health effects of active and passive smoking [25]. This result is predictable because of long residence time of Cd in cells in the absence of normal excretory route [1]. Cd concentration in cells increased with age (duration of exposure). The estimated half-life of Cd in the body varied between 7.4 to 30 years; the lower the body burden, the longer the half-life of Cd [26,27,28,29]. In comparison, nicotine, another constituent of cigarette smoke, can be metabolized rapidly, and is eliminated completely through urinary excretion [30,31,32].
The present review was to provide an update of knowledge on metal transporters involved in the assimilation of dietary Cd and key determinants of the intestinal absorption rate, namely body iron store status, iron deficiency, and diet quality. Epidemiological data connecting an enhanced cancer risk of the breast and pancreatic to Cd exposure are provided. Target iron supplement is discussed as a strategy to reduce Cd accumulation and a subsequent reduction in breast cancer risk among highly susceptible group of women. Special emphasis is on Cd-induced malignant cell transformation, and the potential mechanism(s) underlying resistance to apoptosis and other cytotoxicity due to Cd, which are acquired during cell transformation.
2. Dietary Sources and Determinants the Body Burden of Cadmium
2.1. Estimation of Exposure to Cadmium in the Human Diet
Average and high dietary Cd exposure levels of 30 and 93.5 µg/day were estimated from a typical Australian diet, and measured levels of Cd in foods (Table 1).
As data in Table 1 indicate, cereals and vegetables contributed mostly to total dietary Cd exposure. These sources of dieary Cd were also identied when Australian market basket survey data were used [2]. Of total dietary Cd exposure ranging between 9 and 15 µg/day, potatoes, wheat, cocoa, and meat contributed 46, 16, 12 and 7 % of total dietary Cd exposure, respectively, while crustaceans, liver, peanuts and vegetables each contributed 2-3 %, adding a further 11 % to total dietary Cd exposure [33].
2.2. The Intestinal Absorption Rate of Cadmium
Because metals cannot be synthesized nor destroyed by cells, all physiologically required metals must be sourced from an external environment. However, environmental levels of most metals are generally low, termed micronutrients, consequently, highly specific, and efficient uptake mechanisms and transport pathways are necessary to ensure an optimal supply of metals concordance with physiological demand [34,35,36,37,38]. Also, to prevent harmful effects of deficiency or over supply (overload), the body content of metals, especially iron, is tightly regulated. Because no biochemically active mechanism to eliminate metals, the regulation of the entry of metals is a dominant strategy to maintain metal homeostasis.
Likely, the transporters and ion channels involved in the absorption of Cd by enterocytes include those for essential metals; iron, zinc, calcium, manganese, copper, and cobalt (Fe, Zn, Ca, Mn, Cu, and Co) detailed below. Consequently, the intestinal absorption of Cd and its transport follow closely those of essential metals.
Although our knowledge on Cd absorption in humans remains fragmentary, the most likely transporter proteins/carriers involved are depicted in Figure 1.
Studies from Japan suggested that the absorption rate of Cd among women were 24-45% [39,40], but lower Cd absorption rates of 3-7% were assumed in a conventional health risk assessment of Cd [41[. The assumed low intestinal absorption rates resulted in miscalculation and erroneous conclusion concerning health risk posed by dietary Cd exposure. As detailed below, Cd can be taken up by several metal transporters, and in addition, Cd complexed with MT and phytochelatin can be assimilated through transcytosis and receptor-mediated endocytosis [42,43,44].
2.3. Metal Transporters Involved in Cadmium Absorption
Collective human and experimental data suggest that Cd assimilation involves the divalent metal transporter 1 (DMT1), certain calcium channels, and metal transporters of the Zrt-/Irt-like protein (ZIP) family, notably ZIP14 [45,46,47,48,49]. The ZIP14 was found to mediate also iron absorption [48,49] and possibly the exit of Cd from the enterocyte [49]. The zinc-iron interactions have been observed in studies of Bangladeshi women [50,51]. Genome-wide association and genetic linkage studies are consistent with the roles of zinc and iron transporters and proteins of iron homeostasis as determinants of blood and urinary Cd levels [52,53,54]
Expression levels of metal transporters in the intestine are highly variable, depending on age, nutritional status, and physiological requirements for the metals, e.g., in pregnancy or lactation [50,51,55,56].
Normally, the body burden of an individual contaminant is a balance between absorption and elimination rates. Works in 1970s estimated that 0.001-0.005% of total amount of Cd in the body was excreted each day [23,24]. An extremely slow excretion rate of Cd implies that Cd is a cumulative toxicant, in which its level increases with age (duration of exposure) and that the intestinal absorption rate of Cd essentially determines body burden. In the absence of a therapeutically effective chelation for Cd, the most practical and effective preventive measure is to minimize the absorption rate of Cd.
2.3. Determinants of Cadmium Absorption Rate
2.3.1. Body Iron Stores and Iron Deficiency
The absorption rate of iron is increased when the body iron stores are low or depleted, indicated by serum ferritin concentrations less than 20 and 30 µg/L, respectively [56,57,58]. The absorption rate of iron is increased markedly in iron deficient state, indicated by hemoglobin concentrations and body iron indicators, namely serum ferritin, free erythrocyte protoporphyrin, and % transferrin saturation [58].
Universally, an inadequate iron store status, and iron deficiency are more prevalent in females than males, and are more common in children than adults, described below.
The prevalence of iron deficiency amongst Australian women, aged 25-49 years, was 20.3% [59]. The percentages of iron deficiency among Korean adolescents and women aged 19–49 years were 36.5% and 32.7%, respectively [60].
The prevalence of iron deficiency among U.S. children aged 3-19 years enrolled in NHANES 1999–2002 (n = 5224) was 7% [58]. An association between blood Cd and iron status was found to be strongest in females, 16–19 years of age, and high blood Cd levels (≥ 0.5 μg/L) were 1.74 times more prevalent among those with iron deficiency [57]. Lower serum ferritin concentrations were associated with higher blood Cd and manganese among adolescents (12–17 years) in NHANES 2017–2018 [58].
Non-smoking Norwegian women with low body iron stores had higher blood Cd, Mn and Co than similarly aged women whose body iron stores were within a normal range [61]. One in four women with iron deficiency had elevated blood levels of Cd and manganese. In a study of young women, Finley (1999) noted an increased manganese absorption rate in those with low serum ferritin concentrations, which indicate low iron stores [62].
In a study from Thailand, women (mean age 30.5) with low body iron stores were found to excrete Cd at a level 3.4-fold higher than similarly aged women who had adequate iron stores [63]. In a study from Korea, the mean for blood Cd levels in women with iron deficiency was 1.53 µg/L, 48.5% higher than those with normal iron status [60].
2.3.2. Dietary Factors: Diet Quality
The intestinal absorption of Cd has rarely been studied. The findings from limited literature reports are summarized, herein. Cd in a shellfish diet was shown to be bioavailable in the study by Vahter et al. (1996) who found Cd intake to be 11 μg/day for women who consumed mixed-diet and 28 μg/day for those who had high-shellfish diet [64]. No differences in blood or urine Cd levels were observed between the two groups. However, there were 63% and 24% increases in blood and urine Cd among those consuming the high-shellfish diet who had deplete iron stores (plasma ferritin levels < 20 μg/L), compared with those who consumed mixed diets, and had the same low body iron stores. Thus, these studies strongly suggest that Cd in shellfish is bioavailable and that long-term oyster consumption does result in a higher body burden of Cd.
A study from the Torres Strait (Australia) reported a 1.4-fold increment of urinary Cd was associated with consumption of turtle liver and kidney and locally gathered clams, peanuts, and coconuts [65]. The sum of these foods, heavy smoking, age, and waist circumference accounted for 40% of Cd body burden.
A study from British Columbia observed an elevated urinary Cd excretion was associated with a duration of oyster farming of at least 12 years plus an average consumption of 18 oysters/week (87 g/week) [66]. The estimated Cd exposure from consumption of oysters was 174 μg/week (24.8 μg/d), and the mean urinary Cd was 0.76 μg/g creatinine (range: 0.16–4.04 μg/g creatinine). This mean urinary Cd was approximately twofold higher than the mean urinary Cd of 0.35 μg/g creatinine, recorded for non-smokers, aged 20–75 years, in the Canada Health Measure Survey [67].
In experimental studies, levels of calcium, zinc, iron and fibre in the diet can affect absorption and accumulation of Cd [68,69,70]. Levels of Cd accumulation in the liver and kidneys were reduced by 70-80% after 8 weeks of feeding with Cd-tainted food supplemented with calcium, phosphorus iron and zinc [70]. The reduction of Cd accumulation was attributed to the presence of iron (Fe2+). Addition of vitamin C improved iron uptake but did not reduce Cd accumulation. Iron in combination with calcium, phosphorus and zinc produced the most remarkable effect.
In an experimental study in mice, a diet deficient in iron or calcium led to much greater Cd accumulation in kidneys than a diet deficient in copper, zinc or manganese [71,72]. Renal Cd accumulation levels strongly correlated with intestinal expression of calcium transprrter1 (CaT1) and metallothionein isoform1 (MT1). Younger mice accumulated more Cd in kidneys than older mice, when fed with a calcium-deficient diet. In addition, an iron-deficient diet caused a greater increase in hepatic Cd accumulation than any other diet tested
In experimental animals, a diet high in phytate (fibre) enhanced absorption and renal retention of Cd [69]. Such effects require further study because they could endanger humans with high fiber intake. Supplementation of food commodities with citric acid, which is a common practice, enhances bioavailability of zinc, and may also result in increased Cd absorption [65+4].
Flavonoids and curcumin in the diet may reduce Cd absorption by formation of complexes with Cd [74,75]. A study in mice showed that Cd administration with curcumin resulted in lower Cd levels in blood and organs (liver, kidney) than in mice that received Cd only [74,75]. Regular consumption of curcumin was linked to lowered blood Cd and lowered risk of hypertension in a Korean study [76].
2.3.3. Genetic Factors: The ZIP8, ZIP14, TFR and H63D variants
Argentine Andean women carrying the GT or TT genotype of the rs4872479 ZIP14 variant had 1.25-fold higher blood Cd levels than GG genotype carriers. Also, the Andean women carrying the AG or GG genotype of the rs10014145 ZIP8 variant had 1.18-fold higher blood Cd levels than those carrying the CC genotype [52]. Transferrin receptor variant (TFRC rs3804141) was associated with elevated urinary Cd [53].
In patients with haemochomatosis or iron deficiency, there is an increase in the intestinal expression of the iron transporter DMT1 which creates greater capacity for absorption of iron [34,38]. Because DMT1 has a higher affinity for Cd2+ than Fe2+ [77], an increased expression of the DMT1 in people with haemochromatosis or iron deficiency, in general, would provide them with a greater capacity to absorb iron and possibly Cd.
A longitudinal cohort of the U.S. men, aged 51−97 years, known as the Normative Aging Study, linked high toenail Cd levels to homozygous H63D variant alleles of the hemochromatosis (HFE) gene and to low haemoglobin levels [78].
2.4. Summary: Determinants of Cadmium Absorption Rate
Body iron store status is a major determinant of Cd absorption rate, and thus Cd body burden. Indicators of low body iron stores are associated with elevations of urinary and blood Cd levels in children, adolescent females, and women of reproductive age. Body iron stores in these populations are universally lower than in male counterparts. Habitual consumption of high-Cd-containing foods is an important determinant of the body burden of Cd. A systematic evaluation of the effects on micronutrient status on Cd body burden showed strong evidence for inverse relationships between zinc and iron status and Cd body burden [79].
3. Cadmium as a Multi-Tissue Carcinogen: Epidemiologic Studies
The International Agency for Research on Cancer (IARC) listed Cd as a human lung carcinogen in 1993, based on the incidence of lung cancer in workplace exposure settings [80]. This IARC assertion gained little attention in the evaluation of health risk of dietary Cd exposure because of the perception that cancer risk of Cd was applied only to an inhalational exposure to relatively high doses of volatile metallic and oxide forms of metallic Cd fume and dusts, experienced by workers.
This section summarizes epidemiological data suggesting that Cd may induce the formation of carcinomas in many organs, not limited to lung or exposure routes.
3.1. Cadmium and Human Cancer: Evidence from Meta-Analysis
A summary of carcinogenic risk of Cd evaluated through meta-analysis is in Table 2.
3.1. Impact of Cadmium on Cancer Risk
The carcinogenic risk assessment of Cd provide evidence that lifelong Cd exposure may increase risk of neoplasm in the lung [81,82], kidney [83] and pancreas [84].
Cd exposure was found to be a particularly strong risk factor for breast cancer, only when the urinary excretion of Cd was used as a measure of cumulative long-term exposure (body burden) [85,86]. In contrast, dietary Cd exposure was not associated in breast cancer risk in postmenopausal women [88]. A similar non-association between dietary Cd exposure and breast cancer risk was observed in another two analyses [89,90]. This non-association of dietary Cd exposure and breast cancer risk is not unexpected; as we have elaborated in Section 2, an amount of Cd that reach a target depends largely on absorption rate, not just an amount of Cd in the diet. Thus, the utility of dietary exposure, as an indicator of exposure, in health risk assessment, is questionable.
The central dogma states that for a toxicant to exert its effects, it must first enter the body, and reach its target cells. Accordingly, scalp hair and toenail samples from women with breast cancer contained higher Cd and nickel than non-cancer controls [87]. In addition, Andjelkovic et al. (2012) analyzed levels of Cd in 55 breast tissue samples, obtained during the surgery, where they found almost four times higher Cd quantities in cancer tissues, compared to the surrounding non-cancerous tissues [91].
3.2. Cadmium and Hepatocellular Carcinoma
Carcinogenic potential of Cd accumulation in the liver has attracted little attention although hepatocellular carcinoma (HCC) is the second commonest cause of cancer death worldwide [92,93,94]. The causes of HCC are chronic infection with hepatitis B virus (HBV) or hepatitis C virus (HCV), and dietary exposure to aflatoxin B1 (AFB1), a hepatocarcinogen produced by Aspergillus flavus, grown on peanuts, corns, and soy products [92,93,94]. Mutation in the tumor suppressor protein 53 gene, caused by the G:C-to-T: A transversion, is the molecular signature of HCC in areas with high rates of HBV infection plus AFB1 exposure [95].
Other HCC causative conditions are alcoholic steatohepatitis, iron overload, excessive copper accumulation (Wilson-disease), congenital α1-antitripsin deficiency, autoimmune hepatitis, acquired and congenital glycogen storage disease [96,97,98].
HCC risk factors are male gender, old age and long-term use of oral contraceptives, the immunosuppressant azathioprine [99,100,101]. A genetic defect in the enzyme glucose-6-phosphatase, essential for glucose release from liver glycogen, is another known risk factor in HCC and hepatic adenomas [102].
In 1990, Campbell et al. first observed an association of liver cancer mortality with exposure to Cd in foods of plant origin, but not AFB1 [103]. The reason as to why plant food Cd may have high carcinogenic potential is not known. Probably, it is due to an amount of Cd that form complex with plant phytochelatin, and as discussed earlier that CdPC can be absorbed intact through transcytosis [42] and receptor mediated endocytosis [43,44]. Campbell et al. observed also association of HCC mortality with prevalence of hepatitis B virus surface antigen (HBsAg+) carriers, plasma cholesterol and alcohol consumption.
Recently, a connection between liver cancer and Cd exposure gained some interest, evident from two studies from China [104,105], and a report of a cohort study from Japan [20], which observed increased deaths from carcinoma of the liver and pancreas in men, who showed signs of kidney tubular cell damage and impaired tubular reabsorption function [20]. Previous analysis of data from the same subjects revealed a dose-response relationship between excretion levels of Cd and those signs of nephrotoxicity.
In Australian autopsy studies, increased hepatic sequestration of zinc and copper were found in human liver samples containing Cd ≥ 1 µg/g wet liver weight [106,107,108]. Hepatic levels of copper rose 45-50% in persons with high Cd body burden, compared to similarly aged subjects who had a medium Cd body burden [107]. Excessive liver copper and iron accumulation are known HCC causative factors [92,97].
Evidence for the hepatotoxicity of environmental Cd is summarized in Table 3.
Increased risk of liver inflammation in both U.S. men and women were observed at urinary Cd levels ≥ 0.6 µg/g creatinine as were the risks of non-alcoholic fatty liver (NAFLD) and non-alcoholic steatohepatitis (NASH) in men [109]. Signs of the hepatotoxicity of Cd were noted in U.S. adults [110]. The hepatotoxicity of Cd was more pronounced in boys than girls [111].
3.3. Cadmium and Other Types of Cancer
3.4. Implications for Heath Risk Calculation
Cancer risk evaluation through systematic and meta-analysis, shown in Table 2, have provided evidence that Cd may be involved in the development of carcinoma in many organs. The enhanced cancer risk was observed at a low Cd body burden, indicated by urinary Cd excretion below 1 μg/g creatinine. For example, the risk of breast cancer rises 66% for each 0.5-μg/g creatinine increment of urinary Cd excretion [85].
In a case-control study, a dose response between breast cancer risk and Cd exposure was apparent, when individuals with urinary Cd excretion levels ≤ 0.26 were compared with those with ≥ 0.58 μg/g creatinine, suggesting a 2.29-fold increase in breast cancer risk [125]. In another cohort study of U.S. women, Cd excretion levels ≥ 0.37 μg/g creatinine were associated with a 2.5-fold increase in risk of breast cancer by 2.50-fold [126].
These data cast considerable doubt on current practice of health risk assessment of Cd, which relies solely on kidney tubular dysfunction, defined as urinary excretion of β2-microgloblin (β2M) ≥ 300 μg/g creatinine, as adverse health outcome of concern [41]. Based on this β2M endpoint, upper limits of tolerable intake and acceptable excretion of Cd are 0.83 µg/kg body weight/day and 5.24 µg/g creatinine, respectively. A suggested tolerable intake level is equivalent to 58 µg/day for a 70-kg person. Apparently, these exposure guidelines and nephrotoxicity threshold level of Cd are not sufficiency low to afford health protection. In theory, the toxicity threshold level should be based on the most sensitive endpoint with consideration given to susceptible subpopulations [127].
3.5. Cadmium, Breast Cancer, and Iron Supplement
As an estimate for 2021, there were 281,550 new cases of breast cancer in the US, which formed 30% of all cancer diagnosis in women [128]. Thus, the proportion of breast cancer is approaching epidemic.
Risk factors identified for breast cancer are a female gender, advanced age, positive family history of breast cancer, beginning period at a younger age, no history of pregnancy, and menopause onset at an older age [128]. Obesity, low physical activity, and alcohol abuse were additional risk factors identified, which were modifiable.
It is noteworthy that many cases of female breast cancer do not have any of these identified risk factors. Therefore, there is a need to identify all other factors/conditions that may promote the development of breast carcinoma, from which prevention strategies and a target therapy could be formulated.
An increased risk of breast cancer was noted in individuals who had anemia in a study from South Korea which included 454,304 adults of which 41,947 (9.2 %) had anemia [129]. In another Korean study, female residents of rural areas were found to have a lower risk of breast cancer, compared to women who resided in urban communities [130]. It was suggested urban residents may have had been exposure to higher Cd in dust than rural residents [7].
A causal relationship between pre-existing anemia and living in urban area with consequential breast cancer development is uninvestigated, but it is fundamentally important because almost a quarter of the world’s population has been affected with anemia, whereas women in their reproductive period are broadly anemic. Also, majority of world population live in cities. Evaluation of cancer risk through meta-analyses have identified increased body burden of Cd as a strong risk factor for breast cancer [85,86].
Based on the literature reports of high blood and urinary Cd (body burden) among those with low body iron stores and iron deficiency (Section 2.3), we speculate that environmental exposure to Cd through diet, smoking, and polluted air could contribute to the development or progression of breast cancer, especially in at-risk subpopulations. Arguably, by supplementing iron to women during the reproductive period, particularly those with co-existing anemia, would reduce the body Cd load, and the risk of breast cancer.
3.6. Role of Cadmium in Genesis of Breast Cancer
Understanding precise pathophysiological mechanisms could be useful to predict the risk and formulate rational target therapies. We briefly discuss potential role of Cd in the genesis of breast cancer. Because Cd does not directly damage DNA [14,15], it is suggested that Cd causes breast cancer by several mechanisms, notably dampening DNA repair enzymes [14,15,16], Cd can mimic estrogen activity and is viewed as a xenoestrogen [131]. Siewit et al. have shown that Cd stimulates estrogen receptor ɑ (ERɑ) and promotes glandular cell growth [132].
In the case when, HIF-1 is overexpressed in cancer tissue, cancer is more invasive and patients face poor prognosis [133], also if cancer cells highly express TfR1, patients face unsatisfactory outcome [134,135]. For both cases the mechanisms are the same, namely, TfR1 is HIF- inducible gene and is highly expressed when HIF is generated within the cell. TfR1 mediates absorption of all the metals that were bound to transferrin which can bind both iron and Cd.
Accumulation of Cd in malignant cells may deepen cancer hypoxia, which is linked with worse outcomes and generates additional mutations and promotes metastasis. Cd is procarcinogenic once it reaches breast tissue, and individuals with anemia are heavily loaded with Cd.
Abul-Husn et al found that 1 in 139 individuals have a pathogenic variant of the BRCA1/2 genes. Thus, who there are many individuals have an aberrant form of this gene [136]. Mutations of the BRCA1 and BRCA2genes lead to an increased risk of breast cancer. Individuals who are heterozygote for BRCA1 or BRCA2 are probably born with this mutation, and are more susceptible to developing cancer, but must acquire a second mutation during the lifespan. Other environmental factors may be responsible for the generation of the second mutation, for example, if an individual with one BRCA1 mutation was exposed to radiation, then radiation could generate the second mutation and breast cancer could occur.
Inhibitors of HIF-1 show positive results in breast cancer treatment [137]. In addition to its potential role as an initiator of cancer cell, Cd may promote the proliferation, migration and invasion of breast cancer cells [138]. Accordingly, we speculate that if individuals with breast cancer were supplemented with iron, then malignant cells will uptake more iron and less circulating Cd, given that both metals are bound to transferrin and are taken up uptake by TfR1. These scenarios will result in a reduced accumulation of Cd in cancer tissue, diminished cancer invasion, and an improved outcome.
By supplementing iron in women during the reproductive period, particularly once with co-existing anemia, we could reduce the body Cd load, reducing the risk of breast cancer. Also, individuals with breast cancer must immediately stop smoking and we recommend that regular breast treatments (e.g.; surgery, HIF-1 inhibitors), should be accompanied by iron supplementation. The beneficial effects of iron should be confirmed in controlled trails.
The mitotic crossover could generate a second mutation as well, as Ivanovski et al discussed, but if the mechanisms of DNA repair function properly then chances for the second mutation are negligible. Cd is an inhibitor of DNA repair and consequently minor errors caused by mitotic crossover or by DNA replication which could affect any part (gene) of the chromosome could lead to the occurrence of second mutation and consequent loss of heterozygosity. Although the DNA replication is a highly accurate process, mistakes may occur leading to known point mutations. If the error affects the opposite BRCA1/2 gene (since mutation number one already exists) both genes will encode non-functional protein. As we already discussed, the final step in this chain of events is lacking in DNA repair, and cadmium can make it function improperly [139,140]. Cd is toxicant, and its impacts are dose-dependent [10], so individuals who are heavily loaded with Cd are at pronounced risk that their DNA repair mechanism will not identify the error caused by DNA replication and a second mutation might be generated.
We hypothesized that accumulation in breast tissue contributes to the occurrence of second mutation in the BRCA1 or BRCA2 as depicted in Figure 2.
4. Cadmium as a Multi-Tissue Carcinogen: Experimental Studies
This section summarizes results from a standard 2-year bioassay, which was designed to evaluate tumorigenesis of a suspected carcinogen over lifespan of rats and mice. It also summarizes the formation of cancer cells after prolonged exposure to Cd in cell culture experiments. In addition, the molecular basis for the tolerance to Cd toxicity and metabolic phenotypes acquired during cancer-cell transformation are provided.
4.1. Cadmium and Tumor Formation in Mice
In a 2-year bioassay that mimics a lifetime exposure scenario of the rodent and murine species, Waalkes and Rehm (1994) found that the tumorigenic actions of Cd depended on genetic background or the strain of animals used [141,142,143,144].
In their landmark experiment {141], Cd was administered to the DBA/2NCr (DBA) and NFS/NCr (NFS) mice at 8 weeks of age (an adult age) by subcutaneous injection, as a single dose of 40 µmol/kg or as weekly dose of 40 µmol/kg for 16 weeks (16 × 40 µmol/kg). Thereafter, mice were observed for two years.
HCC and hepatic adenomas were not found in any of DBA mice, but 1 of 15 control NFS mice, and 9 of 27 NFS mice, treated with weekly repeated Cd administrations. Sarcoma at the injection site occurred in 9 of 35 NFS mice with repeated exposure to Cd. Distinctively, the incidence rates of testicular tumors in the two strains were similar. Intriguingly, lung tumor was found in the NFS mice, treated with a single dose of Cd.
The genetic basis contributing to different sensitivity, or resistance to the tumorigenic effects of Cd among murine strains have not been fully investigated. However, the high testicular toxicity of Cd has been linked to ZIP8, a zinc transporter, responsible for uptake of zinc, manganese, and Cd by cells [46,47,48]. These findings accentuate the influences of metal transporters in determining an intracellular concentration of Cd, and thus its toxicity manifestation.
4.2. The Genesis of Lung and Liver Carcinomas after Cadmium Exposure
A single-dose subcutaneous injection of Cd at 40 µmol/kg was sufficient to cause tumor formation in lungs in the NFS mice, while HCC and hepatic adenomas were formed in the same strain, NFS mice, with weekly repeated Cd administrations [141].
In comparison, induction of lung tumors by benzo(a)pyrene, a ubiquitous environmental carcinogen, present in cigarette smoke, and charred meat products, would require a repeated exposure regime due to the rapid rates of metabolism and elimination [145]. Furthermore benzo(a)pyrene, becomes a potent DNA damaging agent only after conversion to benzo(a)pyrene-7,8-diol-9,10-epoxide (BPDE) by the action of microsomal cytochrome P450 (CYP) enzymes; CYP1A1/1A2, and CYP1B1 [145]. Repeated exposure will result in accumulation of BPDE-DNA adducts to a critical level causing mutations that affect expression of oncogenes and tumor suppressor genes [145].
This is analogous to the G:C-to-T: A transversion mutation caused by AFB1-DNA adducts, leading to inactivation of tumor suppressor protein 53 gene [95]. This mutation represents the molecular signature of HCC in areas with high dietary exposure to AFB1 and a relatively high rate of HBV infection [95].
4.3. Induced Formation of Cancer Cells
There was a long history of an attempt to generate cancer cells in vitro, from immortalized human cell lines that do not form tumors in nude mice, so-called non-tumorigenic or non-neoplastic cells. If successful, this in vitro cell-transformation could be an alternative to a high-cost 2-year bioassay. Such attempt proved to be difficult for the carcinogens like benzo(a)pyrene and AFB1. As discussed above, tumorigenic actions of benzo(a)pyrene and AFB1 depend on a metabolic activation, involving specific CYP enzymes.
Distinctively, the carcinogenic action of Cd does not require any CYP enzymes, and cancer cells have now successfully been produced in vitro. The human and rodent cell lines, Cd concentration and exposure duration used in Cd-induced cell transformation experiments, and histologic phenotypes of cancer cells generated are summarized in Table 4.
The immortalized, non-tumorigenic human cells susceptible to the carcinogenicity of Cd include UROtsa urothelial cells [146,147], MCF-10A breast epithelial cells [148], BEAS-2B bronchial epithelial cells [149], HPL-1D peripheral lung epithelium [150], and HPDE pancreatic ductal epithelial cells [11,151]. The cell line of animal origin, found to be susceptible to Cd carcinogenesis is the rat liver epithelial TRL1215 cell line [152, 153].
The generation of cancer cells simply by exposure of varus cell types to low-level Cd over a long period of time (Table 4) provides further evidence that Cd is a muti-tissue carcinogen as it has been observed in both Cd-exposed humans (Table 2) and Cd-exposed mice (Section 4.2). The Cd-transformed cells (transformants) have been of utility to investigate the molecular fingerprints that can be linked to cellular adaptive responses, enabling transformants to resist cell death and acquired cancer-cell phenotypes such as metabolic reprogramming to glycolysis dominance, known as the Warburg effect [14,15,16,154,155,156]. The notable impact of Cd cellular gene expression profiles has been studied extensively using various types of cancer cells, including MCF-7 breast cancer cells, A549 lung cancer cells and HepG2 hepatocellular carcinoma cells [157,158,159].
4.4. Accquired Resistance to the Cytoxicity of Cadmium: Role of Metal Transporters
Among the susceptible cells, UROtsa urothelial cell line is noteworthy because of limited human cell models of human urinary bladder cancer. The UROtsa cell line is non neoplastic cell line, which shows phenotypic and morphologic characteristics resembling primary transitional epithelial cells [160]. This cell line was derived from the epithelium of the ureter of a 12-year-old female donor, immortalized with SV40 large T-antigen [161]. Chronic exposure to Cd caused the UROtsa cells to undergo neoplastic transformation, expressing the phenotype characteristic of transitional cell carcinoma of the bladder [146]
Resistance to cell death is one of the common cancer-cell phenotypes. In cell transformation experiments (Table 4), the Cd concentrations used range from 1 to 5 µM. In comparison, in the investigation of the effects of Cd on the genes expressed by various cancer cells typically Cd concentrations used were between 10 and 100 µM [157,158,159].
A reduced Cd accumulation has been suggested to be the reason for resistance to cell death. In an experiment using TRL1215 rat liver epithelial cells, pretreatment of cells with cyproterone, a synthetic steroidal antiandrogen with a structure related to progesterone, decreased sensitivity to Cd through a decreased accumulation of Cd [162]. However, the molecular basis for a decrease in Cd accumulation was not investigated. It was shown in another study that silencing the expression of ZnT1 result in an increased Cd accumulation, and thus enhanced Cd toxicity [163]. ZnT1 is an efflux transporter that mediate extrusion of both zinc and Cd, thereby lowering intracellular concentrations of Cd [164].
In a more recent study, the expression of ZnT1 UROtsa cells was increased by 1 µM Cd, the same concentration that used in transformation experiment [146]. Pretreatment of UROtsa cells with an inhibitor of glutathione biosynthesis (buthionine sulfoximine) diminished ZnT1 induction with a resultant increase in sensitivity to the cytotoxicity of Cd [165]. Conversely, pretreatment of UROtsa cells with an inhibitor of DNA methylation, 5-aza-2'-deoxycytidine (aza-dC) did not change the extent of ZnT1 expression level in Cd-treated cells. The induced expression of ZnT1 that remained impervious in cells treated with aza-dC coincided with resistance to Cd cytotoxicity [165].
Expression of ZnT1 in A549 human lung cancer cells rose after exposure to 20 µM Cd [158]. Expression of ZnT1 in Cd-transformed HPL-1D human peripheral lung epithelium also rose together with ZnT5 and ZIP8, leading to a reduced Cd accumulation [150]. Collectively, these experimental data underscore the significance of metal transporter, in particular, ZnT1 efflux transporter in the acquisition of tolerance to Cd by various cancer cells.
5. Conclusions
Carcinogenic risk evaluation of Cd through meta-analysis indicates that chronic exposure to environmental Cd is a risk factor for many types of cancer, which include lung, kidney, pancreas, and breast. There in increasing evidence that Cd may contribute to the genesis or progression of the neoplasms in liver and pancreas.
In a landmark observation made by Waalkes and Rehm in 1994, neoplasms of the lung and liver, lymphoma and sarcoma were found in mice during 2-year observation period after administration of Cd to mice. A single dose subcutaneous injection of Cd at 40 µmol/kg is sufficient to induce lung tumors. This can be attributable to the retention of Cd in cells throughout their lifespan, and thus there is ample of opportunity to exert its tumorigenic actions.
Prolonged exposure to a sublethal concentration of Cd caused non-tumorigenic, immortalized cell lines of human origin to become cancer cells after acquisition tolerance to the toxicity of Cd. The human breast epithelium, MCF-10A cells were transformed to basal-like breast cancer cells after exposure to 2.5 μM Cd2+ for 40 weeks. Other human cells susceptible to carcinogenic action of Cd are UROtsa urothelium, BEAS-2B bronchial epithelium, HPL-1D peripheral lung epithelium and HPDE pancreatic ductal epithelium. The UROtsa urothelial cells transformed to cancer cells after exposure to Cd as low as 1 μM concentration for 8-10 weeks.
Epidemiologic and experimental data provide compelling evidence that Cd is a multi-tissue carcinogen. Avoidance of foods containing high Cd levels is important, but so is a sufficient consumption of dietary essential metals (iron, calcium, and zinc), and maintenance of adequate body iron stores, and optimal body weight. Iron supplement could be a logical intervention to reduce Cd absorption, and its accumulation in breast tissues, especially in highly susceptible subpopulations.
There is no safe level of Cd exposure, and thus public health resources that promote cessation of smoking and educate consumers about foods known to contain high levels of Cd are likely to have significant health benefits.
Author Contributions
Conceptualization, A.C. and S.S.; proposed target iron supplement, drawing figures A.C.; writing—original draft preparation, S.S. and A.C.; writing—review and editing, S.S. and A.C. Both authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This work was supported with resources from the Centre for Kidney Disease Research, Translational Research Institute, and the Department of Kidney and Transplant Services, Princess Alexandra Hospital. It was supported also with resources from the Institute of Anatomy, Faculty of Medicine, University of Belgrade, Serbia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef]
- Callan, A.; Hinwood, A.; Devine, A. (2014) Metals in commonly eaten groceries in Western Australia: a market basket survey and dietary assessment. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk Assess. 2014, 31, 1968–1981. [Google Scholar] [CrossRef]
- Fechner, C.; Hackethal, C.; Höpfner, T.; Dietrich, J.; Bloch, D.; Lindtner, O.; Sarvan, I. Results of the BfR MEAL Study: In Germany, mercury is mostly contained in fish and seafood while cadmium, lead, and nickel are present in a broad spectrum of foods. Food Chem X. 2022, 14, 100326. [Google Scholar] [CrossRef]
- Mhungu, F.; Chen, K.; Wang, Y.; Liu, Y.; Zhang, Y.; Pan, X.; Cheng, Y.; Liu, Y.; Zhang, W. Probabilistic risk assessment of dietary exposure to cadmium in residents of Guangzhou, China-young children potentially at a health risk. Int. J. Environ. Res. Public Health 2022, 19, 9572. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kataoka, Y.; Hayashi, K.; Matsuda, R.; Uneyama, C. Dietary exposure of the Japanese general population to elements: Total diet study 2013-2018. Food Saf. (Tokyo) 2022, 10, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Pappas, R.S.; Fresquez, M.R.; Watson, C.H. Cigarette smoke cadmium breakthrough from traditional filters: Implications for exposure. J. Anal. Toxicol. 2015, 39, 45–51. [Google Scholar] [CrossRef]
- Świetlik, R.; Trojanowska, M. Chemical fractionation in environmental studies of potentially toxic particulate-bound elements in urban air: A critical review. Toxics 2022, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Sunderman, F.W. Jr. (2001) Nasal toxicity, carcinogenicity, and olfactory uptake of metals. Ann. Clin. Lab. Sci. 2001, 31, 3–24. [Google Scholar] [PubMed]
- Cory-Slechta, D.A.; Allen, J.L.; Conrad, K.; Marvin, E.; Sobolewski, M. Developmental exposure to low level ambient ultrafine particle air pollution and cognitive dysfunction. Neurotoxicology 2018, 69, 217–231. [Google Scholar] [CrossRef]
- Valko, M.; Jomova, K.; Rhodes, C.J.; Kuča, K.; Musílek, K. Redox- and non-redox-metal-induced formation of free radicals and their role in human disease. Arch. Toxicol. 2016, 90, 1–37. [Google Scholar] [CrossRef]
- Moulis, J.M.; Bourguinon, J.; Catty, P. Chapter 23 Cadmium. In RSC Metallobiology Series No. 2, Binding, Transport. and Storage of Metal. Ions in Biological Cells; Wolfgang, M., Anthony, W., Eds.; The Royal Society of Chemistry: London, UK, 2014; pp. 695–746. [Google Scholar]
- Petering, D.H. Reactions of the Zn proteome with Cd2+ and other xenobiotics: Trafficking and toxicity. Chem. Res. Toxicol. 2016, 30, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Earley, B.J.; Cubillas, C.; Warnhoff, K.; Ahmad, R.; Alcantar, A.; Lyon, M.D.; Schneider, D.L.; Kornfeld, K. Cadmium hijacks the high zinc response by binding and activating the HIZR-1 nuclear receptor. Proc. Natl. Acad. Sci. USA 2021, 118, e2022649118. [Google Scholar] [CrossRef]
- Cannino, G.; Ferruggia, E.; Luparello, C.; Rinaldi, A.M. Cadmium and mitochondria. Mitochondrion 2009, 9, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Luparello, C.; Sirchia, R.; Longo, A. Cadmium as a transcriptional modulator in human cells. Crit. Rev. Toxicol. 2011, 41, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, A. Metal interaction with redox regulation: an integrating concept in metal carcinogenesis? Free Radic. Biol. Med. 2013, 55, 63–72. [Google Scholar] [CrossRef]
- Patel, C.J.; Rehkopf, D.H.; Leppert, J.T.; Bortz, W.M.; Cullen, M.R.; Chertow, G.M.; Ioannidis, J.P. Systematic evaluation of environmental and behavioural factors associated with all-cause mortality in the United States national health and nutrition examination survey. Int. J. Epidemiol. 2013, 42, 1795–1810. [Google Scholar] [CrossRef]
- Li, Z.; Fan, Y.; Tao, C.; Yan, W.; Huang, Y.; Qian, H.; Xu, Q.; Wan, T.; Chen, Y.; Qin, Y.; Lu, C. Association between exposure to cadmium and risk of all-cause and cause-specific mortality in the general US adults: A prospective cohort study. Chemosphere 2022, 307, 136060. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Lee, J.; Yu, J.M.; Choi, H.; Choi, S.; Park, J.; Choi, K.; Kim, E.; Kim, H.; Kim, M.J.; Park, Y.J. Association between environmental cadmium exposure and increased mortality in the U.S. National Health and Nutrition Examination Survey (1999-2018). J. Expo. Sci. Environ. Epidemiol. 2023, 33, 874–882. [Google Scholar] [CrossRef]
- Nogawa, K.; Watanabe, Y.; Sakuma, S.; Sakurai, M.; Nishijo, M.; Ishizaki, M.; Morikawa, Y.; Kido, T.; Nakagawa, H.; Suwazono, Y. Renal tubular dysfunction and cancer mortality in the Japanese general population living in cadmium-non-contaminated areas. J. Appl. Toxicol. 2022, 42, 1458–1466. [Google Scholar] [CrossRef]
- Xing, X.; Xu, M.; Yang, L.; Shao, C.; Wang, Y.; Qi, M.; Niu, X.; Gao, D. Association of selenium and cadmium with heart failure and mortality based on the National Health and Nutrition Examination Survey. J. Hum. Nutr. Diet 2023, 36, 1496–1506. [Google Scholar] [CrossRef]
- Sears, C.G.; Eliot, M.; Raaschou-Nielsen, O.; Poulsen, A.H.; Harrington, J.M.; Howe, C.J.; James, K.A.; Roswall, N.; Overvad, K.; Tjønneland, A.; et al. Urinary cadmium and incident heart failure: A case-cohort analysis among never-smokers in Denmark. Epidemiology 2022, 33, 185–192. [Google Scholar] [CrossRef]
- Shi, J.-W.; Fan, D.-X.; Li, M.-Q. The Relationship between cadmium exposure and mortality in postmenopausal females: A cohort study of 2001–2018 NHANES. Nutrients 2023, 15, 4604. [Google Scholar] [CrossRef] [PubMed]
- Suwazono, Y.; Nogawa, K.; Morikawa, Y.; Nishijo, M.; Kobayashi, E.; Kido, T.; Nakagawa, H.; Nogawa, K. Renal tubular dysfunction increases mortality in the Japanese general population living in cadmium non-polluted areas. J. Expo. Sci/ Environ. Epidemiol. 2015, 25, 399–404. [Google Scholar] [CrossRef]
- Kim, J.; Song, H.; Lee, J.; Kim, Y.J.; Chung, H.S.; Yu, J.M.; Jang, G.; Park, R.; Chung, W.; Oh, C.M.; Moon, S. Smoking and passive smoking increases mortality through mediation effect of cadmium exposure in the United States. Sci. Rep. 2023, 13, 3878. [Google Scholar] [CrossRef] [PubMed]
- Elinder, C.G.; Lind, B.; Kjellstorm, T.; Linnman, L.; Friberg, L. Cadmium in kidney cortex, liver and pancreas from Swedish autopsies: Estimation of biological half time in kidney cortex, considering calorie intake and smoking habits. Arch. Environ. Health 1976, 31, 292–301. [Google Scholar] [CrossRef]
- Elinder, C.G.; Kjellstöm, T.; Lind, B.; Molander, M.L.; Silander, T. Cadmium concentrations in human liver, blood, and bile: comparison with a metabolic model. Environ Res. 1978, 17, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Suwazono, Y.; Kido, T.; Nakagawa, H.; Nishijo, M.; Honda, R.; Kobayashi, E.; Dochi, M.; Nogawa, K. Biological half-life of cadmium in the urine of inhabitants after cessation of cadmium exposure. Biomarkers 2009, 14, 77–81. [Google Scholar] [CrossRef]
- Ishizaki, M.; Suwazono, Y.; Kido, T.; Nishijo, M.; Honda, R.; Kobayashi, E.; Nogawa, K.; Nakagawa, H. Estimation of biological half-life of urinary cadmium in inhabitants after cessation of environmental cadmium pollution using a mixed linear model. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk Assess. 2015, 32, 1273–1276. [Google Scholar] [CrossRef]
- Satarug, S.; Nishijo, M.; Ujjin, P.; Vanavanitkun, Y.; Baker, J.R.; Moore, M.R. Evidence for concurrent effects of exposure to environmental cadmium and lead on hepatic CYP2A6 phenotype and renal function biomarkers in nonsmokers. Environ Health Perspect. 2004, 112, 1512–1518. [Google Scholar] [CrossRef]
- Satarug, S.; Tassaneeyakul, W.; Na-Bangchang, K.; Cashman, J.R.; Moore, M.R. Genetic and environmental influences on therapeutic and toxicity outcomes: studies with CYP2A6. Curr. Clin. Pharmacol. 2006, 1, 291–309. [Google Scholar] [CrossRef]
- Apinan, R.; Tassaneeyakul, W.; Mahavorasirikul, W.; Satarug, S.; Kajanawart, S.; Vannaprasaht, S.; Ruenweerayut, R.; Na-Bangchang, K. The influence of CYP2A6 polymorphisms and cadmium on nicotine metabolism in Thai population. Environ. Toxicol. Pharmacol. 2009, 28, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Haswell-Elkins, M.R.; Moore, M.R. Safe levels of cadmium intake to prevent renal toxicity in human subjects. Br. J. Nutr. 2000, 84, 791–802. [Google Scholar] [CrossRef]
- Guo, S.; Frazer, D.M.; Anderson, G.J. Iron homeostasis: transport, metabolism, and regulation. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Knez, M.; Graham, R.D.; Welch, R.M.; Stangoulis, J.C. New perspectives on the regulation of iron absorption via cellular zinc concentrations in humans. Crit. Rev. Food Sci. Nutr. 2017, 57, 2128–2143. [Google Scholar] [CrossRef] [PubMed]
- Nishito, Y.; Kambe, T. (2018) Absorption mechanisms of iron, copper, and zinc: An overview. J. Nutr. Sci. Vitaminol. (Tokyo) 2018, 64, 1–7. [Google Scholar] [CrossRef]
- Kondaiah, P.; Yaduvanshi, P.S.; Sharp, P.A.; Pullakhandam, R. Iron and zinc homeostasis and interactions: Does enteric zinc excretion cross-talk with intestinal iron absorption? Nutrients 2019, 11, 1885. [Google Scholar] [CrossRef] [PubMed]
- Charlebois, E.; Pantopoulos, K. Nutritional aspects of iron in health and disease. Nutrients 2023, 15, 2441. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Nomiyama, T.; Kumagai, N.; Dekio, F.; Uemura, T.; Takebayashi, T.; Nishiwaki, Y.; Matsumoto, Y.; Sano, Y.; Hosoda, K.; et al. Uptake of cadmium in meals from the digestive tract of young non-smoking Japanese female volunteers. J. Occup. Health 2003, 45, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Oguma, E.; Sasaki, S.; Miyamoto, K.; Ikeda, Y.; Machida, M.; Kayama, F. Comprehensive study of the effects of age, iron deficiency, diabetes mellitus, and cadmium burden on dietary cadmium absorption in cadmium-exposed female Japanese farmers. Toxicol. Appl. Pharmacol. 2004, 196, 114–123. [Google Scholar] [CrossRef]
- JECFA. JECFA. In Summary and Conclusions. In Proceedings of the Joint FAO/WHO Expert Committee on Food Additives and Contaminants, Seventy-Third Meeting, Geneva, Switzerland, 8–17 June 2010; JECFA/73/SC; Food and Agriculture Organization of the United Nations/World Health Organization: Geneva, Switzerland, In Summary and Conclusions. In Proceedings of the Joint FAO/WHO Expert Committee on Food Additives and Contaminants, Seventy-Third Meeting, Geneva, Switzerland, 8–17 June 2010; JECFA/73/SC; Food and Agriculture Organization of the United Nations/World Health Organization: Geneva, Switzerland, 2011. Available online: https://apps.who.int/iris/handle/10665/44521 (accessed on 3 January 2024).
- Fujita, Y.; el Belbasi, H.I.; Min, K.S.; Onosaka, S.; Okada, Y.; Matsumoto, Y.; Mutoh, N.; Tanaka, K. Fate of cadmium bound to phytochelatin in rats. Res. Commun. Chem. Pathol. Pharmacol. 1993, 82, 357–365. [Google Scholar]
- Langelueddecke, C.; Roussa, E.; Fenton, R.A.; Thévenod, F. Expression and function of the lipocalin-2 (24p3/NGAL) receptor in rodent and human intestinal epithelia. PLoS ONE 2013, 8, e71586. [Google Scholar] [CrossRef]
- Langelueddecke, C.; Lee, W.K.; Thévenod, F. Differential transcytosis and toxicity of the hNGAL receptor ligands cadmium-metallothionein and cadmium-phytochelatin in colon-like Caco-2 cells: Implications for in vivo cadmium toxicity. Toxicol. Lett. 2014, 226, 228–235. [Google Scholar] [CrossRef]
- Schneider, S.N.; Liu, Z.; Wang, B.; Miller, M.L.; Afton, S.E.; Soleimani, M.; Nebert, D.W. Oral cadmium in mice carrying 5 versus 2 copies of the Slc39a8 gene: Comparison of uptake, distribution, metal content, and toxicity. Int. J. Toxicol. 2014, 33, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jorge-Nebert, L.F.; Gálvez-Peralta, M.; Landero Figueroa, J.; Somarathna, M.; Hojyo, S.; Fukada, T.; Nebert, D.W. Comparing gene expression during cadmium uptake and distribution: Untreated versus oral Cd-treated wild-type and ZIP14 knockout mice. Toxicol. Sci. 2015, 143, 26–35. [Google Scholar] [CrossRef]
- Fujishiro, H.; Hamao, S.; Tanaka, R.; Kambe, T.; Himeno, S. Concentration-dependent roles of DMT1 and ZIP14 in cadmium absorption in Caco-2 cells. J. Toxicol. Sci. 2017, 42, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, T.B.; Cousins, R.J. The multiple faces of the metal transporter ZIP14 (SLC39A14). J. Nutr. 2018, 148, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, G.J.; Aydemir, T.B.; Troche, C.; Martin, A.B.; Chang, S.M.; Cousins, R.J. Influence of ZIP14 (slc39A14) on intestinal zinc processing and barrier function. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 308, G171–G178. [Google Scholar] [CrossRef]
- Kippler, M.; Goessler, W.; Nermell, B.; Ekström, E.C.; Lönnerdal, B.; El Arifeen, S.; Vahter, M. Factors influencing intestinal cadmium uptake in pregnant Bangladeshi women--a prospective cohort study. Environ. Res. 2009, 109, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Kippler, M.; Ekström, E.C.; Lönnerdal, B.; Goessler, W.; Akesson, A.; El Arifeen, S.; Persson, L.A.; Vahter, M. Influence of iron and zinc status on cadmium accumulation in Bangladeshi women. Toxicol. Appl. Pharmacol. 2007, 222, 221–226. [Google Scholar] [CrossRef]
- Rentschler, G.; Kippler, M.; Axmon, A.; Raqib, R.; Skerfving, S.; Vahter, M.; Broberg, K. Cadmium concentrations in human blood and urine are associated with polymorphisms in zinc transporter genes. Metallomics 2014, 6, 885–891. [Google Scholar] [CrossRef]
- Rentschler, G.; Kippler, M.; Axmon, A.; Raqib, R.; Ekström, E.C.; Skerfving, S.; Vahter, M.; Broberg, K. Polymorphisms in iron homeostasis genes and urinary cadmium concentrations among nonsmoking women in Argentina and Bangladesh. Environ. Health Perspect. 2013, 121, 467–472. [Google Scholar] [CrossRef]
- Ng, E.; Lind, P.M.; Lindgren, C.; Ingelsson, E.; Mahajan, A.; Morris, A.; Lind, L. Genome-wide association study of toxic metals and trace elements reveals novel associations. Hum. Mol. Genet. 2015, 24, 4739–4745. [Google Scholar] [CrossRef]
- Leazer, T.M.; Liu, Y.; Klaassen, C.D. Cadmium absorption and its relationship to divalent metal transporter-1 in the pregnant rat. Toxicol. Appl. Pharmacol. 2002, 185, 18–24. [Google Scholar] [CrossRef]
- Flanagan, P.R.; McLellan, J.S.; Haist, J.; Cherian, M.G.; Chamberlain, M.J.; Valberg, L.S. Increased dietary cadmium absorption in mice and human subjects with iron deficiency. Gastroenterol. 1978, 46, 609–623. [Google Scholar] [CrossRef]
- Silver, M.K.; Lozoff, B.; Meeker, J.D. Blood cadmium is elevated in iron deficient U.S. children: A cross-sectional study. Environ. Health 2013, 12, 117. [Google Scholar] [CrossRef] [PubMed]
- Schildroth, S.; Friedman, A.; Bauer, J.A.; Claus, Henn, B. Associations of a metal mixture with iron status in U.S. adolescents: Evidence from the National Health and Nutrition Examination Survey. New Dir. Child Adolesc. Dev. 2022, 2022, 67–89. [Google Scholar] [CrossRef]
- Ahmed, F.; Coyne, T.; Dobson, A.; McClintock, C. Iron status among Australian adults: Findings of a population- based study in Queensland, Australia. Asia Pac. J. Clin. Nutr. 2008, 17, 40–47. [Google Scholar]
- Suh, Y.J.; Lee, J.E.; Lee, D.H.; Yi, H.G.; Lee, M.H.; Kim, C.S.; Nah, J.W.; Kim, S.K. Prevalence and relationships of iron deficiency anemia with blood cadmium and vitamin D levels in Korean women. J. Korean Med. Sci. 2016, 31, 25–32. [Google Scholar] [CrossRef]
- Meltzer, H.M.; Brantsaeter, A.L.; Borch-Iohnsen, B.; Ellingsen, D.G.; Alexander, J.; Thomassen, Y.; Stigum, H.; Ydersbond, T.A. Low iron stores are related to higher blood concentrations of manganese, cobalt and cadmium in non-smoking, Norwegian women in the HUNT 2 study. Environ. Res. 2010, 110, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Finley, J.W. Manganese absorption and retention by young women is associated with serum ferritin concentration. Am. J. Clin. Nutr. 1999, 70, 37–43. [Google Scholar] [CrossRef]
- Satarug, S.; Ujjin, P.; Vanavanitkun, Y.; Baker, J.R.; Moore, M.R. Influence of body iron store status and cigarette smoking on cadmium body burden of healthy Thai women and men. Toxicol. Lett. 2004, 148, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Vahter, M.; Berglund, M.; Nermell, B.; Akesson, A. Bioavailability of cadmium from shellfish and mixed diet in women. Toxicol. Appl. Pharmacol. 1996, 136, 332–341. [Google Scholar] [CrossRef]
- Haswell-Elkins, M.; Imray, P.; Satarug, S.; Moore, M.R.; O'dea, K. Urinary excretion of cadmium among Torres Strait Islanders (Australia) at risk of elevated dietary exposure through traditional foods. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 372–377. [Google Scholar] [CrossRef]
- Copes, R.; Clark, N.A.; Rideout, K.; Palaty, J.; Teschke, K. Uptake of cadmium from Pacific oysters (Crassostrea gigas) in British Columbia oyster growers. Environ. Res. 2008, 107, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Garner, R.; Levallois, P. Cadmium levels and sources of exposure among Canadian adults. Health Rep. 2016, 27, 10–18. [Google Scholar]
- Rimbach, G.; Pallauf, J. Cadmium accumulation, zinc status, and mineral bioavailability of growing rats fed diets high in zinc with increasing amounts of phytic acid. Biol. Trace Elem. Res. 1997, 57, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Lind, Y.; Engman, J.; Jorhem, L.; Glynm, A.W. Accumulation of cadmium from wheat bran, sugar-beet fibre, carrots and cadmium chloride in the liver and kidneys of mice. Br. J. Nutr. 1998, 80, 205–211. [Google Scholar] [CrossRef]
- Groten, J.P.; Sinkeldam, E.J.; Muys, T.; Luten, J.B.; van Bladeren, P.J. Interaction of dietary Ca, P, Mn, Cu, Fe, Zn and Se with accumulation and oral toxicity of cadmium in rats. Food Chem. Toxicol. 1991, 29, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Min, K.S.; Ueda, H.; Kihara, T.; Tanaka, K. Increased hepatic accumulation of ingested Cd is associated with upregulation of several intestinal transporters in mice fed diets deficient in essential metals. Toxicol Sci. 2008, 106, 284–289. [Google Scholar] [CrossRef]
- Min, K.S.; Sano, E.; Ueda, H.; Sakazaki, F.; Yamada, K.; Takano, M.; Tanaka, K. Dietary deficiency of calcium and/or iron, an age-related risk factor for renal accumulation of cadmium in mice. Biol. Pharm. Bull. 2015, 38, 1557–1563. [Google Scholar] [CrossRef]
- Walter, A.; Rimbach, G.; Most, E.; Pallauf, J. Effect of citric acid supplements to a maize-soya diet on the in vitro availability of minerals, trace elements and heavy metals. J. Vet. Med. 1998, 45, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Kukongviriyapan, U.; Pannangpetch, P.; Kukongviriyapan, V.; Donpunha, W.; Sompamit, K.; Surawattanawan, P. 2014. Curcumin protects against cadmium-induced vascular dysfunction, hypertension and tissue cadmium accumulation in mice. Nutrients 2014, 6, 1194–1208. [Google Scholar] [CrossRef]
- Li, X.; Jiang, X.; Sun, J.; Zhu, C.; Li, X.; Tian, L.; Liu, L.; Bai, W. Cytoprotective effects of dietary flavonoids against cadmium-induced toxicity. Ann. NY Acad. Sci. 2017, 1398, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Oh, C.; Shim, S.Y.; Jeong, S.; Kim, H.S.; Kim, M.S. Reduction in prevalence of hypertension and blood heavy metals among curry-consumed Korean. Tohoku J. Exp. Med. 2018, 244, 219–229. [Google Scholar] [CrossRef]
- Illing, A.C.; Shawki, A.; Cunningham, C.L.; Mackenzie, B. Substrate profile and metal-ion selectivity of human divalent metal-ion transporter-1. J. Biol. Chem. 2012, 287, 30485–30496. [Google Scholar] [CrossRef] [PubMed]
- Ciesielski, T.H.; Schwartz, J.; Bellinger, D.C.; Hauser, R.; Amarasiriwardena, C.; Sparrow, D.; Wright, R.O. Iron-processing genotypes, nutrient intakes, and cadmium levels in the Normative Aging Study: Evidence of sensitive subpopulations in cadmium risk assessment. Environ. Int. 2018, 119, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Li, C.; Zhao, D.; Huang, L. Associations of micronutrients exposure with cadmium body burden among population: A systematic review. Ecotoxicol. Environ. Saf. 2023, 256, 114878. [Google Scholar] [CrossRef]
- IARC (International Agency for Research on Cancer). Cadmium. IARC Monogr. Eval. Carcinog. Risk Hum. 1993, 58, 119–238. [Google Scholar]
- Nawrot, T.S.; Martens, D.S.; Hara, A.; Plusquin, M.; Vangronsveld, J.; Roels, H.A.; Staessen, J.A. Association of total cancer and lung cancer with environmental exposure to cadmium: the meta-analytical evidence. Cancer Causes Control. 2015, 26, 1281–1288. [Google Scholar] [CrossRef]
- Chen, C.; Xun, P.; Nishijo, M.; He, K. Cadmium exposure and risk of lung cancer: a meta-analysis of cohort and case-control studies among general and occupational populations. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 437–444. [Google Scholar] [CrossRef]
- Song, Jk.; Luo, H.; Yin, Xh.; Huang, G.l.; Luo, Sy.; Lin, du R. ; Yuan, D.B.; Zhang, W.; Zhu, Jg. Association between cadmium exposure and renal cancer risk: a meta-analysis of observational studies. Sci. Rep. 2015, 5, 17976. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Xun, P.; Nishijo, M.; Sekikawa, A.; He, K. Cadmium exposure and risk of pancreatic cancer: a meta-analysis of prospective cohort studies and case-control studies among individuals without occupational exposure history. Environ. Sci. Pollut. Res. Int. 2015, 22, 17465–17474. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N.; Wolk, A. Urinary cadmium concentration and risk of breast cancer: A systematic review and dose-response meta-analysis. Am. J. Epidemiol. 2015, 182, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Zhang, F.; Lei, Y. Dietary intake and urinary level of cadmium and breast cancer risk: A meta-analysis. Cancer Epi-demiol. 2016, 42, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Jouybari, L.; Saei Ghare Naz, M.; Sanagoo, A.; Kiani, F.; Sayehmiri, F.; Sayehmiri, K.; Hasanpour Dehkordi, A. Toxic elements as biomarkers for breast cancer: A meta-analysis study. Cancer Manag. Res. 2018, 10, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Van Maele-Fabry, G.; Lombaert, N.; Lison, D. Dietary exposure to cadmium and risk of breast cancer in postmenopausal women: A systematic review and meta-analysis. Environ. Int. 2016, 86, 1–13. [Google Scholar] [CrossRef]
- Florez-Garciam, V.A.; Guevara-Romero, E.C.; Hawkins, M.M.; Bautista, L.E.; Jenson, T.E.; Yu, J.; Kalkbrenner, A.E. Cadmium exposure and risk of breast cancer: A meta-analysis. Environ. Res. 2023, 219, 115109. [Google Scholar] [CrossRef]
- Filippini, T.; Torres, D.; Lopes, C.; Carvalho, C.; Moreira, P.; Naska, A.; Kasdagli, M.I.; Malavolti, M.; Orsini, N.; Vinceti, M. Cadmium exposure and risk of breast cancer: A dose-response meta-analysis of cohort studies. Environ. Int. 2020, 142, 105879. [Google Scholar] [CrossRef]
- Anđelković, M.; Djordjevic, A.B.; Miljaković, E.A.; Javorac, D.; Čolaković, N.; Oprić, S.; Petričević, S.; Granić, M.; Kotur-Stevuljević, J.; Antonijević, B.; et al. Cadmium tissue level in women diagnosed with breast cancer - A case control study. Environ. Res. 2021, 199, 111300. [Google Scholar] [CrossRef]
- Kim, J.U.; Shariff, M.I.; Crossey, M.M.; Gomez-Romero, M.; Holmes, E.; Cox, I.J.; Fye, H.K.; Njie, R.; Taylor-Robinson, S.D. Hepatocellular carcinoma: Review of disease and tumor biomarkers. World J. Hepatol. 2016, 8, 471–484. [Google Scholar] [CrossRef]
- Kew, M.C. Epidemiology of chronic hepatitis B virus infection, hepatocellular carcinoma, and hepatitis B virus-induced hepatocellular carcinoma. Pathologie Biologie 2010, 58, 273–277. [Google Scholar] [CrossRef]
- Bartosch B, Thimme R, Blum HE, Zoulim F. Hepatitis C virus-induced hepatocarcinogenesis. J. Hepatology 2009, 51, 810–820.
- Besaratinia, A.; Kim, S.I.; Hainaut, P.; Pfeifer, G.P. In vitro recapitulating of TP53 mutagenesis in hepatocellular carcinoma associated with dietary aflatoxin B1 exposure. Gastroenterol., 2009, 137, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Millonig, G.; Seitz, H.K. Alcoholic liver disease and hepatitis C: A frequently underestimated combination. World J. Gastroenterol. 2009, 15, 3462–3471. [Google Scholar]
- Savas, N; Canan, O. ; Ozcay, F.; Bilezikci, B.; Karakayali, H.; Yilmaz, U.; Haberal, M. Hepatocellular carcinoma in Wilson's disease: a rare association in childhood. Pediatric Transplantation 2006, 10, 639–643.
- Giannitrapani, L.; Soresi, M.; La Spada, E.; Cervello, M.; D'Alessandro, N.; Montalto, G. Sex hormones and risk of liver tumor. Ann. N.Y. Acad. Sci. 2006, 1089, 228–236. [Google Scholar] [CrossRef]
- Bartley, J.; Loddenkemper, C.; Lange, J.; Mechsner, S.; Radke, C.; Neuhaus, P.; Ebert, A.D. Hepatocellular adenoma and focal nodular hyperplasia after long-term use of danazol for endometriosis: a case report. Arch. Gynecol. Obstet. 2004, 269, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Cattan, S.; Wendum, D.; Chazouilleres, O.; Schmitz, J.; Gendre, J.P. Hepatocellular carcinoma and focal hepatic glycogenosis after prolonged azathioprine therapy. Human Pathol. 2000, 31, 874–876. [Google Scholar] [CrossRef]
- Ishida, M. ; Naka S; Shiomi, H. ; Tsujikawa, T.; Andoh, A.; Nakahara, T.; Saito, Y.; Kurumi, Y.; Takikita-Suzuki, M.; Kojima, F.; Hotta, M.; Tani, T.; Fujiyama, Y.; Okabe, H. Hepatocellular carcinoma occurring in a Crohn's disease patient. World J. Gastroenterol. 2010, 16, 3215–3218. [Google Scholar]
- Bannasch, P. Hepatocellular glycogenosis and hepatic neoplasms. Toxicol. Pathol. 010, 38, 1000-1002.
- Campbell, T.C.; Chen, J.S.; Liu, C.B.; Li, J.Y.; Parpia, B. Non-association of aflatoxin with primary liver cancer in a cross-sectional ecological survey in the People's Republic of China. Cancer Res. 1990, 50, 6882–6893. [Google Scholar]
- Jiang, A.; Gong, L.; Ding, H.; Wang, M. Cancer mortality and long-term environmental exposure of cadmium in contaminated community based on a third retrospective cause of death investigation of residents living in the Guangdong Province from 2004 to 2005. Biol. Trace. Elem. Res. 2021, 199, 4504–4515. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Y.; Li, T.; Zhuo, W.; Zhu, Y. Elevated serum and hair levels of cadmium as a risk factor for liver carcinoma: A meta-analysis. Nutr. Cancer 2023, 75, 1438–1447. [Google Scholar] [CrossRef]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Changes in zinc and copper homeostasis in human livers and kidneys associated with exposure to environmental cadmium. Hum. Exp. Toxicol. 2001, 20, 205–213. [Google Scholar] [CrossRef]
- Satarug, S. Long-term exposure to cadmium in food and cigarette smoke, liver effects and hepatocellular carcinoma. Curr. Drug Metab. 2012, 13, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Hyder, O.; Chung, M.; Cosgrove, D.; Herman, J.M.; Li, Z.; Firoozmand, A.; Gurakar, A.; Koteish, A.; Pawlik, T.M. Cadmium exposure and liver disease among US adults. J. Gastrointest. Surg. 2013, 17, 1265–1273. [Google Scholar] [CrossRef]
- Hong, D.; Min, J.Y.; Min, K.B. Association between cadmium exposure and liver function in adults in the United States: A cross-sectional study. J. Prev. Med. Public Health 2021, 54, 471–480. [Google Scholar] [CrossRef]
- Xu, Z.; Weng, Z.; Liang, J.; Liu, Q.; Zhang, X.; Xu, J.; Xu, C.; Gu, A. Association between urinary cadmium concentrations and liver function in adolescents. Environ. Sci. Pollut. Res. Int. 2022, 29, 39768–39776. [Google Scholar] [CrossRef]
- Kang, M.Y.; Cho, S.H.; Lim, Y.H.; Seo, J.C.; Hong, Y.C. Effects of environmental cadmium exposure on liver function in adults. Occup. Environ. Med. 2013, 70, 268–273. [Google Scholar] [CrossRef]
- Kim, D.W.; Ock, J.; Moon, K.W.; Park, C.H. Association between Pb, Cd, and Hg Exposure and Liver Injury among Korean Adults. Int. J. Environ. Res. Public Health 2021, 18, 6783. [Google Scholar] [CrossRef]
- Park, E.; Kim, J.; Kim, B.; Park, E.Y. Association between environmental exposure to cadmium and risk of suspected non-alcoholic fatty liver disease. Chemosphere 2021, 266, 128947. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Sung, G.H.; Lee, S.; Han, K.J.; Han, H.J. Serum cadmium is associated with hepatic steatosis and fibrosis: Korean national health and nutrition examination survey data IV-VII. Medicine (Baltimore) 2022, 101, e28559. [Google Scholar] [CrossRef]
- Seo, M.N.; Eom, S.Y.; Lim, J.A.; Lee, J.E.; Choi, B.S.; Kwon, H.J.; Hong, Y.S.; Kim, H.; Park, J.D. Effects of environmental cadmium exposure on the liver in Korean adults: Cross-sectional and longitudinal studies. Arch. Environ. Contam. Toxicol. 2023, 84, 237–247. [Google Scholar] [CrossRef] [PubMed]
- McElroy, J.A.; Hunter, M.I. Cadmium: a new risk factor for endometrial cancer? Expert Rev. Anticancer Ther. 2019, 19, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Cirovic, A.; Cirovic, A. Iron deficiency as promoter of heavy metals-induced acute myeloid leukemia. Leuk. Res. 2021, 112, 106755. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. The evolving role for zinc and zinc transporters in cadmium tolerance and urothelial cancer. Stresses 2021, 1, 105–118. [Google Scholar] [CrossRef]
- Satir, S. The relationship between oral cancer and cadmium: a review. Mol. Biol. Rep. 2022, 49, 2413–2419. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli Pirzaman, A.; Mansoori, R.; Hosseini, S.M.; Abolhosseini, A.; Khosravi, S.; Moghadamnia, A.A.; Kazemi, S. Toxic mechanisms of cadmium and exposure as a risk factor for oral and gastrointestinal carcinomas. Hum. Exp. Toxicol. 2024, 43, 9603271231223506. [Google Scholar] [CrossRef]
- Rezapour, M.; Rezapour, H.A.; Chegeni, M.; Khanjani, N. Exposure to cadmium and head and neck cancers: a meta-analysis of observational studies. Rev. Environ. Health 2021, 36, 577–584. [Google Scholar] [CrossRef]
- Chen, C.; Xun, P.; Nishijo, M.; Carter, S.; He, K. Cadmium exposure and risk of prostate cancer: a meta-analysis of cohort and case-control studies among the general and occupational populations. Sci. Rep. 2016, 6, 25814. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, Y.; Hao, R.; Shao, M.; Luo, Y. Cadmium levels in tissue and plasma as a risk factor for prostate carcinoma: A meta-analysis. Biol. Trace Elem. Res. 2016, 172, 86–92. [Google Scholar] [CrossRef]
- McElroy, J.A.; Shafer, M.M.; Trentham-Dietz, A.; Hampton, J.M.; Newcomb, P.A. Cadmium exposure and breast cancer risk. J. Natl. Cancer Inst. 2006, 98, 869–873. [Google Scholar] [CrossRef]
- Gallagher, C.M.; Chen, J.J.; Kovach, J.S. Environmental cadmium and breast cancer risk. Aging (Albany NY) 2010, 2, 804–814. [Google Scholar] [CrossRef]
- Moffett, D.B.; Mumtaz, M.M.; Sullivan, D.W., Jr.; Whittaker, M.H. Chapter 13, General Considerations of Dose-Effect and Dose-Response Relationships. In Handbook on the Toxicology of Metals, 5th ed.; Volume I: General, Considerations, Nordberg, G., Costa, M., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 299–317. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.A. Anemia may increase the overall risk of cancer: Findings from a Cohort Study with a 12-year follow-up period in South Korea. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 1440–1448. [Google Scholar] [CrossRef]
- Lee, P.-J.; Jhuang, J.-R.; Chen, Y.-C.; Su, S.-Y.; Chiang, C.-J.; Yang, Y.-W.; Hsieh, P.-C.; Chen, M.-J.; Lee, W.-C. Urban–rural disparity in birth cohort effects on breast cancer incidence. J. Urban Health 2023, 100, 341–354. [Google Scholar] [CrossRef]
- Ronchetti, S.A.; Miler, E.A.; Duvilanski, B.H.; Cabilla, J.P. Cadmium mimics estrogen-driven cell proliferation and prolactin secretion from anterior pituitary cells. PLoS One 2013, 8, e81101. [Google Scholar] [CrossRef] [PubMed]
- Siewit, C.L.; Gengler, B.; Vegas, E.; Puckett, R.; Louie, M.C. Cadmium promotes breast cancer cell proliferation by potentiating the interaction between ERalpha and c-Jun. Mol Endocrinol. 2010, 24, 981–992. [Google Scholar] [CrossRef]
- Nalwoga, H.; Ahmed, L.; Arnes, J.B.; Wabinga, H.; Akslen, L.A. Strong expression of hypoxia-inducible factor-1α (HIF-1α) is associated with Axl expression and features of aggressive tumors in African breast cancer. PLoS One 2016, 11, e0146823. [Google Scholar] [CrossRef] [PubMed]
- Habashy, H.O.; Powe, D.G.; Staka, C.M.; Rakha, E.A.; Ball, G.; Green, A.R.; Aleskandarany, M.; Paish, E.C.; Douglas Macmillan, R.; Nicholson, R.I.; et al. Transferrin receptor (CD71) is a marker of poor prognosis in breast cancer and can predict response to tamoxifen. Breast Cancer Res. Treat. 2010, 119, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Li, X.; Dong, D.; Zhang, B.; Xue, Y.; Shang, P. Transferrin receptor 1 in cancer: a new sight for cancer therapy. Am. J. Cancer Res. 2018, 8, 916–931. [Google Scholar]
- Abul-Husn, N.S.; Soper, E.R.; Odgis, J.A.; Cullina, S.; Bobo, D.; Moscati, A.; Rodriguez, J.E.; CBIPM Genomics Team; Regeneron Genetics Center; et al. Exome sequencing reveals a high prevalence of BRCA1 and BRCA2 founder variants in a diverse population-based biobank. Genome Med. 2019, 31, 12. [Google Scholar] [CrossRef] [PubMed]
- Kachamakova-Trojanowska, N.; Podkalicka, P.; Bogacz, T.; Barwacz, S.; Józkowicz, A.; Dulak, J.; Łoboda, A. HIF-1 stabilization exerts anticancer effects in breast cancer cells in vitro and in vivo. Biochem. Pharmacol. 2020, 175, 113922. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Pi, H.; Liao, L.; Tan, M.; Deng, P.; Yue, Y.; Xi, Y.; Tian, L.; Xie, J.; Chen, M.; et al. Cadmium promotes breast cancer cell proliferation, migration and invasion by inhibiting ACSS2/ATG5-mediated autophagy. Environ. Pollut. 2021, 273, 116504. [Google Scholar] [CrossRef]
- Joseph, P. Mechanisms of cadmium carcinogenesis. Toxicol. Appl. Pharmacol. 2009, 238, 272–279. [Google Scholar] [CrossRef]
- Candéias, S.; Pons, B.; Viau, M.; Caillat, S.; Sauvaigo, S. Direct inhibition of excision/synthesis DNA repair activities by cadmium: analysis on dedicated biochips. Mutat. Res. 2010, 694, 53–59. [Google Scholar] [CrossRef]
- Waalkes, M.P.; Rehm, S. Chronic toxic and carcinogenic effects of cadmium chloride in male DBA/2NCr and NFS/NCr mice: strain-dependent association with tumors of the hematopoietic system, injection site, liver, and lung. Fundam. Appl. Toxicol. 1994, 23, 21–31. [Google Scholar] [CrossRef]
- Huff, J.; Lunn, R.M.; Waalkes, M.P.; Tomatis, L.; Infante, P.F. Cadmium-induced cancers in animals and in humans. Int. J. Occup. Environ. Health 2007, 13, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Tokar, E.J.; Benbrahim-Tallaa, L.; Waalkes, M.P. Metal ions in human cancer development. Met. Ions Life Sci. 2011, 8, 375–401. [Google Scholar]
- Zhu, Y.; Costa, M. Metals and molecular carcinogenesis. Carcinogenesis 2020, 41, 1161–1172. [Google Scholar] [CrossRef]
- Alexandrov, K.; Rojas, M.; Satarug, S. The critical DNA damage by benzo(a)pyrene in lung tissues of smokers and approaches to preventing its formation. Toxicol. Lett. 2010, 198, 63–68. [Google Scholar] [CrossRef]
- Sens, D.A.; Park, S.; Gurel, V.; Sens, M.A.; Garrett, S.H.; Somji, S. Inorganic cadmium- and arsenite-induced malignant transformation of human bladder urothelial cells. Toxicol. Sci. 2004, 79, 56–63. [Google Scholar] [CrossRef]
- Hoggarth, Z.E.; Osowski, D.B.; Freeberg, B.A.; Garrett, S.H.; Sens, D.A.; Sens, M.A.; Zhou, X.D.; Zhang, K.K.; Somji, S. The urothelial cell line UROtsa transformed by arsenite and cadmium display basal characteristics associated with muscle invasive urothelial cancers. PLoS ONE 2018, 13, e0207877. [Google Scholar] [CrossRef] [PubMed]
- Benbrahim-Tallaa, L.; Tokar, E.J.; Diwan, B.A.; Dill, A.L.; Coppin, J.-F.; Waalkes, M.P. Cadmium malignantly transforms normal human breast epithelial cells into a basal-like phenotype. Environ. Health Perspect. 2009, 117, 1847–1852. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Liu, L.Z.; Jiang, Y.; Zhu, Y.; Guo, N.L.; Barnett, J.; Rojanasakul, Y.; Agani, F.; Jiang, B.H. Cadmium increases HIF-1 and VEGF expression through ROS, ERK, and AKT signaling pathways and induces malignant transformation of human bronchial epithelial cells. Toxicol. Sci. 2012, 125, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Person, R.J.; Tokar, E.J.; Xu, Y.; Orihuela, R.; Ngalame, N.N.; Waalkes, M.P. Chronic cadmium exposure in vitro induces cancer cell characteristics in human lung cells. Toxicol. Appl. Pharmacol. 2013, 273, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Qu, W.; Tokar, E.J.; Kim, A.J.; Bell, M.W.; Waalkes, M.P. Chronic cadmium exposure in vitro causes acquisition of multiple tumor cell characteristics in human pancreatic epithelial cells. Environ. Health Perspect. 2012, 120, 1265–1271. [Google Scholar] [CrossRef]
- Qu, W.; Diwan, B.A.; Reece, J.M.; Bortner, C.D.; Pi, J.; Liu, J.; Waalkes, M.P. Cadmium-induced malignant transformation in rat liver cells: Role of aberrant oncogene expression and minimal role of oxidative stress. Int. J. Cancer 2005, 114, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Takiguchi, M.; Achanzar, W.E.; Qu, W.; Li, G.; Waalkes, M.P. Effects of cadmium on DNA-(Cytosine-5) methyltransferase activity and DNA methylation status during cadmium-induced cellular transformation. Exp. Cell Res. 2003, 286, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, P.; Schidberger, H.; Mayer, A. The Warburg effect: essential part of metabolic reprogramming and central contributor to cancer progression. Int. J. Radiat. Biol. 2019, 95, 912–919. [Google Scholar] [CrossRef]
- Vaupel, P.; Multhoff, G. Revisiting the Warburg effect: historical dogma versus current understanding. J. Physiol. 2021, 599, 1745–1757. [Google Scholar] [CrossRef] [PubMed]
- Drochioiu, G. Multifactorial distress, the Warburg effect, and respiratory and pH imbalance in cancer development. Stresses 2023, 3, 500–528. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, Y.; Zhu, Y.; Yu, Z.; Shao, M.; Luo, Y. Identification and characterization of cadmium-related genes in liver carcinoma. Biol. Trace Elem. Res. 2018, 182, 238–247. [Google Scholar] [CrossRef]
- Forcella, M.; Lau, P.; Fabbri, M.; Fusi, P.; Oldani, M.; Melchioretto, P.; Gribaldo, L.; Urani, C. Is cadmium toxicity tissue-specific? Toxicogenomics studies reveal common and specific pathways in pulmonary, hepatic, and neuronal cell models. Int. J. Mol. Sci. 2022, 23, 1768. [Google Scholar] [CrossRef]
- Luparello, C. Cadmium-associated molecular signatures in cancer cell models. Cancers (Basel) 2021, 13, 2823. [Google Scholar] [CrossRef]
- Rossi, M.R.; Masters, J.R.W.; Park, S.; Todd, J.H.; Garrett, S.H.; Sens, M.A.; Somji, S.; Nath, J.; Sens, D.A. The immortalized UROtsa cell line as a potential cell culture model of human urothelium. Environ. Health Perspect. 2001, 109, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Petzoldt, L.; Leigh, I.M.; Duffy, P.G.; Sexton, C.; Masters, R.W. Immortalisation of human urothelial cells. Urol. Res. 1995, 23, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Takiguchi, M.; Cherrington, N.J.; Hartley, D.P.; Klaassen, C.D.; Waalkes, M.P. Cyproterone acetate induces a cellular tolerance to cadmium in rat liver epithelial cells involving reduced cadmium accumulation. Toxicology 2001, 165, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Ohana, E.; Sekler, I.; Kaisman, T.; Kahn, N.; Cove, J.; Silverman, W.F.; Amsterdam, A.; Hershfinkel, M. Silencing of ZnT-1 expression enhances heavy metal influx and toxicity. J. Mol. Med. 2006, 84, 753–763. [Google Scholar] [CrossRef]
- Nishito, Y.; Kambe, T. Zinc transporter 1 (ZNT1) expression on the cell surface is elaborately controlled by cellular zinc levels. J. Biol. Chem. 2019, 294, 15686–15697. [Google Scholar] [CrossRef]
- Satarug, S.; Garrett, S.H.; Somji, S.; Sens, M.A.; Sens, D.A. Zinc, zinc transporters, and cadmium cytotoxicity in a cell culture model of human urothelium. Toxics 2021, 9, 94. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The intestinal absorption of cadmium. Cd in the diet is absorbed into the portal blood circulation, delivered to liver first, and then to cells throughout the body [1]. The most likely metal carriers involved in Cd absorption are those for iron, zinc, copper, and calcium (Fe, Zn, Cu and Ca) [42,43,44,45,46]. Abbreviations: DMT1, divalent metal transporter1; ZIP14, Zrt- and Irt-related protein 10; ATP7A, ATPases (Cu-ATPases) ATP7A; TRPV6, Transient receptor potential vanilloid6TRPV6.
Figure 1.
The intestinal absorption of cadmium. Cd in the diet is absorbed into the portal blood circulation, delivered to liver first, and then to cells throughout the body [1]. The most likely metal carriers involved in Cd absorption are those for iron, zinc, copper, and calcium (Fe, Zn, Cu and Ca) [42,43,44,45,46]. Abbreviations: DMT1, divalent metal transporter1; ZIP14, Zrt- and Irt-related protein 10; ATP7A, ATPases (Cu-ATPases) ATP7A; TRPV6, Transient receptor potential vanilloid6TRPV6.
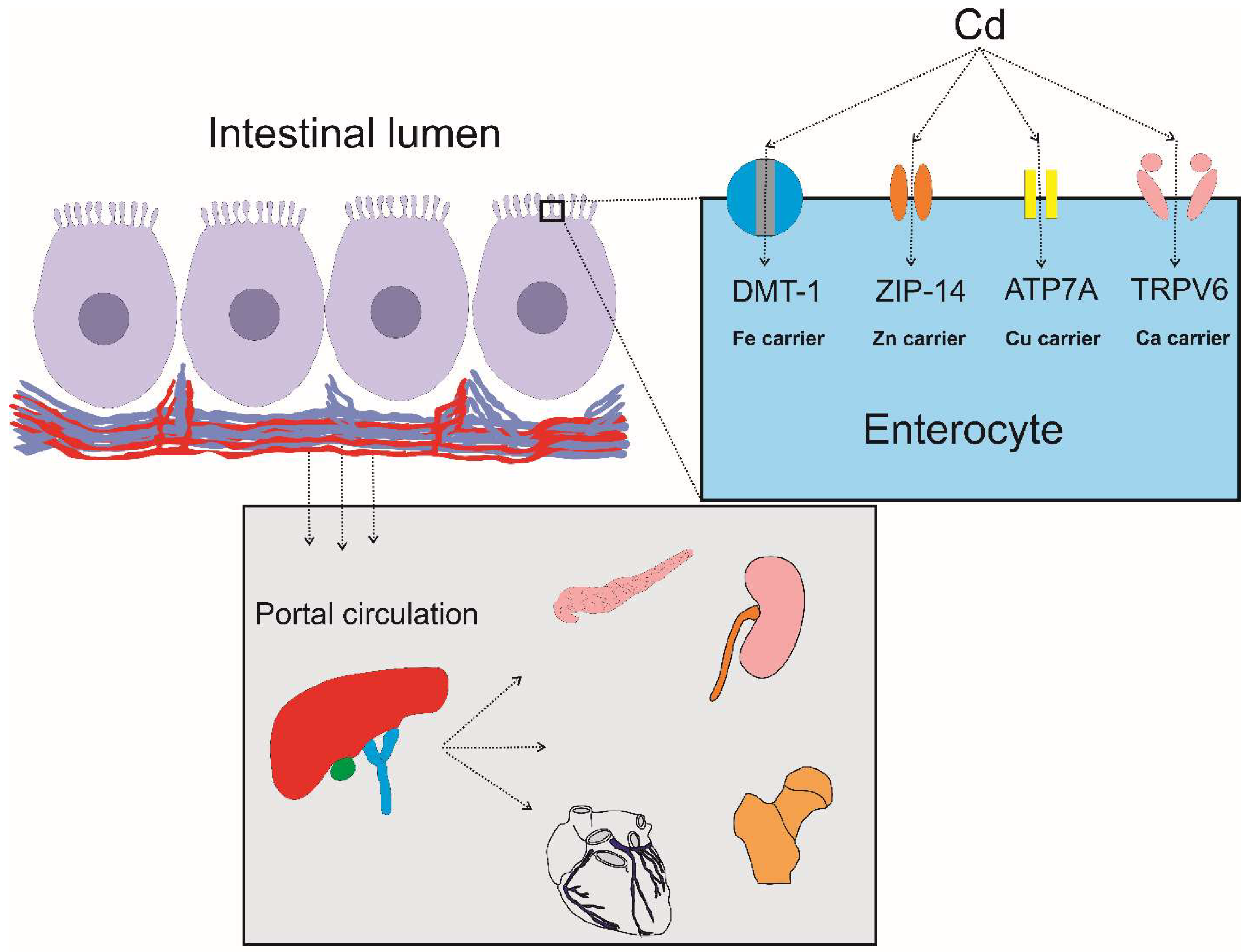
Figure 2.
Hypothetical factors involved in the appearance of second mutation. Cd accumulation in breast tissue may contribute to the occurrence of second mutation of the BRCA1 or BRCA2 gene with resultant loss of heterozygosity Other environmental factors such as radiation may also be contributing factor.
Figure 2.
Hypothetical factors involved in the appearance of second mutation. Cd accumulation in breast tissue may contribute to the occurrence of second mutation of the BRCA1 or BRCA2 gene with resultant loss of heterozygosity Other environmental factors such as radiation may also be contributing factor.
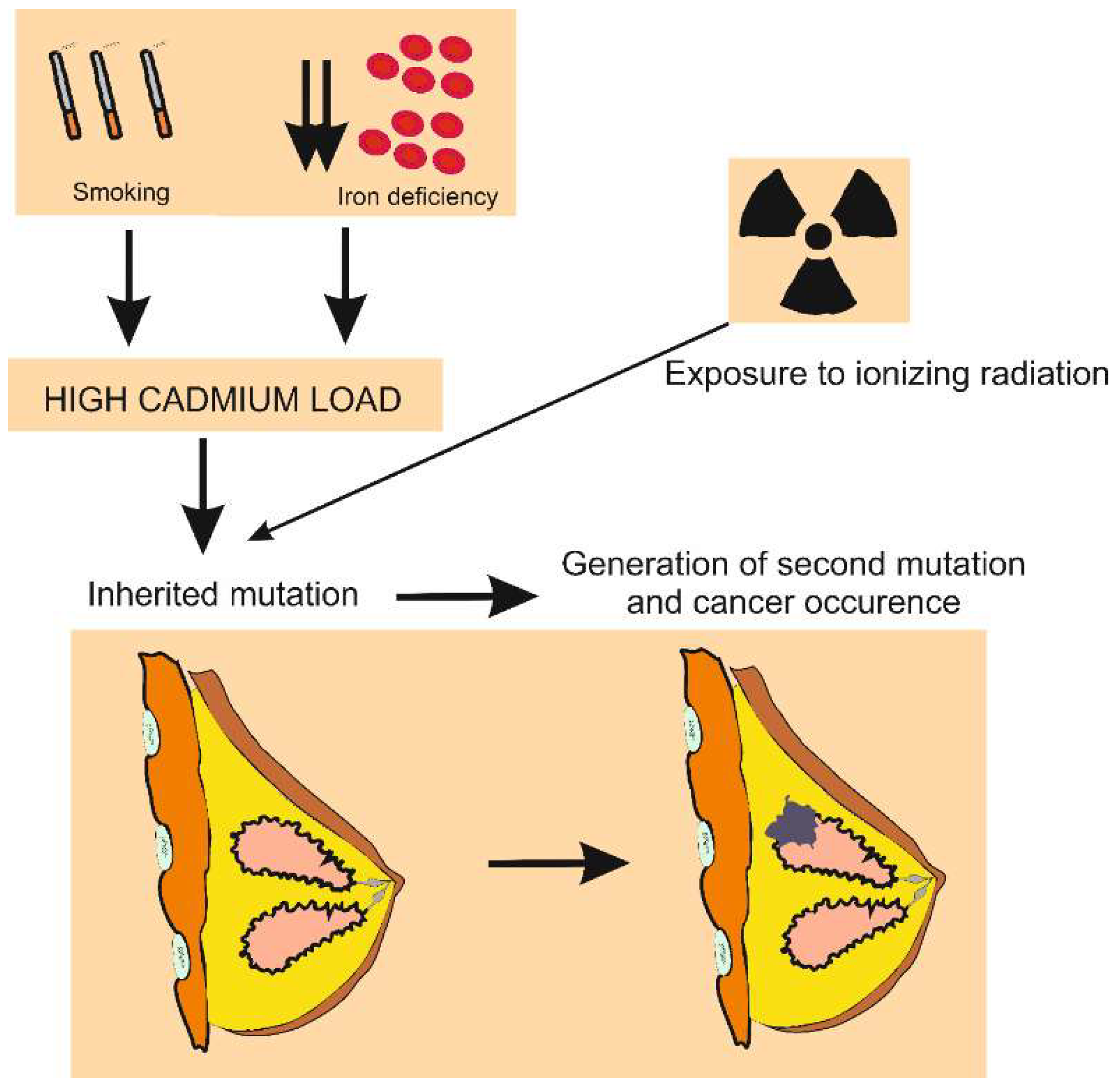

Table 1.
Dietary cadmium exposure estimates from food cadmium concentrations.
| Foods | Cd, mg/kg | Intake rate, g/day | Exposure, µg/day | ||
|---|---|---|---|---|---|
| Maximum | Typical | High | Average | ||
| Vegetables; potatoes, included | 0.1 | 0.05 | 250 | 25 | 12.5 |
| Cereals, pulses, legume; rice, wheat grain included | 0.2 | 0.05 | 200 | 40 | 10 |
| Fruit | 0.05 | 0.01 | 150 | 7.5 | 1.5 |
| Oilseeds and cocoa beans | 1.0 | 0.5 | 1 | 1 | 0.5 |
| Meat; cattle, poultry, pig, sheep | 0.1 | 0.02 | 150 | 15 | 3.0 |
| Liver; cattle, poultry, pig, sheep | 0.5 | 0.1 | 5 | 2.5 | 0.5 |
| Kidney; cattle, poultry, pig, sheep | 2.0 | 0.5 | 1 | 2 | 0.5 |
| Fish | 0.05 | 0.02 | 30 | 1.5 | 0.6 |
| Crustaceans, mollusks | 2 | 0.25 | 3 | 6 | 0.75 |
| TOTAL | − | − | − | 93.5 | 30 |
Food types and intake rates were based on a typical Australian diet [33].
Table 2.
Environmental cadmium exposure and an increased cancer risk .
| Cancer | Exposure and Risk Estimates | References |
|---|---|---|
| Lung | Comparing the highest vs. lowest category of urinary Cd, respective OR (95% CI) values for lung cancer risk and cancer mortality were 1.68 (1.47–1.92) and 1.22 (1.13–1.31). The average urinary Cd excretions across three cohorts ranged from 0.25 to 0.93 µg/g creatinine. |
Nawrot et al. 2015 [81] |
| Lung | Comparing the highest vs. lowest Cd dose category, respective OR (95% CI) values for lung cancer were 1.42 (0.91 − 2.23), 0.68 (0.33 − 1.41) and 1.61 (0.94 − 2.75) in the general population, occupationally-exposed population, and case–control studies, respectively. | Chen et al. 2016 [82] |
| Kidney | Comparing the highest vs. lowest category of Cd dose metrics, OR (95% CI) values for renal cancer risk was 1.47 (1.27−1.71) | Song et al. 2015 [83] |
| Pancreas | Comparing the highest vs. lowest category of Cd dose metrics, respective RR (95% CI) values for pancreatic cancer risk in all subjects, men and women were 2.05 (1.58−2.66), 1.78 (1.04–3.05) and 1.02, (0.63–1.65). | Chen et al. 2015 [84] |
| Breast | Comparing the highest vs. lowest category of urinary Cd, OR value (95% CI) for breast cancer risk was 2.24 (1.50–3.34). For each 0.5-µg/g creatinine increase of urinary Cd, the OR for breast cancer was increased 1.66-fold (95% CI: 1.23–2.25) |
Larsson et al. 2015 [85] |
| Breast | Comparing the highest vs. lowest quartile of urinary Cd, OR value (95% CI) for breast cancer was 2.24 (1.49–3.35) Dietary Cd exposure level was not associated with breast cancer risk (RR 1.01, 95% CI: 0.89–1.15). |
Lin et al. 2016 [86] |
| Breast | Respective mean (95% CI) values for Cd and Ni in scalp hair and toenail samples from women with breast cancer were 2.65 (1.57–3.73) and 2.06 (1.20–3.32), higher than controls. | Jouybari et al. 2018 [87] |
| Breast | Among postmenopausal women, dietary Cd exposure level was not associated with breast cancer risk (RR, 1.03, 95% CI: 0.89–1.19) |
Van Maele-Fabry et al. 2016 [88] |
OR, odds ratio; CI, confidence interval; RR, relative risk; Ni = nickel.
Table 3.
Levels of environmental cadmium exposure and effects on liver.
| Study Population | Exposure Levels and Effects Observed | Reference |
|---|---|---|
| United States NHANES 1988 − 1994 n 12,732, ≥ 20 years |
Urinary Cd levels ≥ 0.83 μg/g creatinine were associated with 1.26-fold increase in risk of liver inflammation in women. Urinary Cd ≥ 0.65 μg/g creatinine were associated with liver inflammation (OR 2.21), NAFLD (OR 1.30), and NASH (OR 1.95) in men |
Hyder et al. 2013 [109] |
| United States NHANES 1999 − 2015 n 11, 838, ≥ 20 years |
A tenfold increment of urinary Cd was associated with elevated plasma levels of ALT (OR 1.36), and AST (OR 1.31) | Hong et al. 2021 [110] |
| United States NHANES 1999 − 2016 n 4411 adolescents |
Urinary Cd quartile 4 was associated with elevated plasma ALT (OR 1.40) and AST (OR 1.64). Liver effect of Cd was larger in boys than girls |
Xu et al. 2022 [111] |
| South Korea, n 3914, ≥ 19 years |
Blood Cd levels ≥ 1.98 μg/L were associated with elevated plamsa levels of AST (OR 3.61) and ALT (OR 2.40) | Kang et al. 2013 [112] |
| Korean National Environmental Health Survey ((2015-2017) n 2953, ≥ 19 year |
Geometric mean urinary Cd was 0.42 µg/L. Top urinary Cd quartile (> 0.88 μg/L) was associated with higher plasma AST and GGT, compared with quartile 1. Urinary Cd quartiles 4, 3, and 2 were associated with higher plasma ALT, compared with bottom. quartile |
Kim et al. 2021 [113] |
| South Korea, n 12,099, ≥ 19 years |
Blood Cd levels higher than 0.96 and 1.41 μg/L were associated with NAFLD (OR 1.91) and NASH (OR 1.41) | Park et al. 2021 [114] |
| Korean NHANES 2008–2017 n 15,783, ≥ 20 years, mean age 46 |
Serum Cd levels >1.41 µg/dL were respectively associated with 1.90, 1.26-, 1.73- and 2.53-fold increases in risk of ALT elevation, hepatic steatosis, fibrosis, and AST elevation, compared to serum Cd levels < 0.651 µg/dL | Han et al. 2022 [115] |
| South Korea Baseline (2011), n 2,086 adults Follow-up (2015), n 503 adult |
The geometric mean blood Cd was higher in females than males (1.16 vs. 0.96 μg/L). No change in blood Cd levels both genders over 5-year duration. ALT and GGT rose only in females. |
Seo et al. 2023 [116] |
NHANES, National Health and Nutrition Examination Survey; n, sample size; OR, odds ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, γ-glutamyl transferase; NAFLD, non-alcoholic fatty liver disease; NASH non-alcoholic steatohepatitis NASH.
Table 4.
The genesis of cancer cells after prolonged exposure to cadmium.
| Immortal Cell Line, Reference |
[Cd], Exposure Duration | Transformant and Tumor Characteristics |
|---|---|---|
| Human urothelium, UROtsa [146,147] | 1 μM Cd2+ 8-10 weeks. |
Soft agar colony formation. Tumorigenic in nude mice with the transitional cell carcinoma phenotypes; gene expression profiles like the basal subtype of muscle invasive bladder carcinomas. Acquired Cd tolerance as an adaptive survival mechanism. |
| Human breast epithelium, MCF-10A [148] |
2.5 μM Cd2+ 40 weeks. |
Basal-like breast cancer cells; ER-α negative, HER2 negative, diminished BRCA1 expression, persistent cell proliferation, elevated expression of cytokeratin 5 and p63, overexpressed c-myc and Kras, and displayed a global DNA hypomethylation state. Tumors were ER-α negative. |
| Human bronchial epithelium, BEAS-2B [149] |
1 µM Cd2+ 6 months. Passage-matched cells as controls. |
Activated ERK and AKT signaling, elevated HIF-1 and VEGF expression. Inhibition of the ROS generation attenuated the activation of ERK, AKT, p70S6K1 and expression of HIF-1α. Tumorigenic in nude mice. Formation of tubes in an in vitro test for angiogenesis. |
| Human peripheral lung epithelium, HPL-1D [150] |
5 μM Cd2+ 20 weeks. |
Soft agar colony formation. Decreased expression of the tumor suppressor genes p16 and SLC38A3, increased expression of the oncoproteins KRAS and NRAS and vimentin, the epithelial-to-mesenchymal transition marker, overexpressed MT-1A, MT-2A, HO-1, HIF-1A, ZnT1, ZnT5 and ZIP8. Acquired Cd tolerance as an adaptive survival mechanism. |
| Human pancreatic ductal epithelium, HPDE [151] |
1 μM Cd2+ 29 weeks. |
Increased secretion of matrix metalloproteinase-9 (MMP-9) and over-expressed the pancreatic cancer marker S100P. Formation of poorly differentiated glandular-like structures on soft agar. |
| Rat liver epithelium, TRL1215 [152,153]. |
2.5 μM Cd2+ for 10 weeks 1 μM Cd2+ for 28 weeks |
Hyperproliferation, increased invasiveness, and reduced dependency on serum, increased DNA methylation, enhanced DNA methyltransferase activity. Over expression of c-myc and c-jun oncogenes. |
[Cd], cadmium concentration; ER-α, Estrogen receptor-alpha; HER2, Human epidermal growth factor receptor 2; BRCA1, breast cancer susceptibility gene1; BERK, extracellular signal-regulated kinases; HIF-1, hypoxia-inducible factor-1; MMP-9, matrix metalloproteinase-9; MT, metallothionein; HO-1, heme oxygenase-1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



