Submitted:
10 January 2024
Posted:
11 January 2024
You are already at the latest version
Abstract
Sodium glucose cotransporter 2 inhibitors (SGLT2i) are currently available for the management of type 2 diabetes mellitus. SGLT2i act by inhibiting renal SGLT2, thereby increasing glucosuria and lowering serum glucose. Recent trials are emerging supporting a role for SGLT2i irrespective of the diabetic status pointing towards that SGLT2i have other mechanisms of actions beyond blood sugar control. In this review, we will shed light on the role of this group of medications that act as SGLT2i in non-diabetics focusing on pre-clinical and clinical data highlighting the mechanism of renoprotection and effects of SGLT2i in the non-diabetic kidneys.
Keywords:
SGLT2i
; CKD
; Blood Pressure
; IGAN
; FSGS
; Proteinuria
; survival
; Non-Diabetics
1. Introduction
Chronic kidney disease (CKD) is defined as persistently reduced estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2, persistently elevated urine albumin excretion or both for more than 3 months. As of 2022, CKD was shown to affect more than 800 million persons worldwide1.
The prevalence of end stage kidney disease (ESKD) as a consequence of progressive CKD and other kidney diseases has more than doubled in the USA from 389, 592 to 807, 920 between the years 2000 to 20202 despite using current management. This continued increase in the prevalence of ESKD poses a huge burden on patients with kidney diseases and the health care system. Trials to add new medications to our armamentarium are much needed to improve outcomes of patients with kidney diseases.
Recent trials evaluating a new group of medications that act on the sodium glucose co-transporters (SGLTs) inhibiting them, have shown promising results for kidney disease patients, especially in patients with diabetes mellitus (DM). Several trials confirmed the benefits of these medications in diabetic patients, yet little is known about their value in non-diabetic patients.
SGLT
SGLTs are transmembrane proteins that function to transport glucose and sodium across cell membranes in several tissues including the proximal renal tubules (PT). While SGLT1 contributes to transport glucose in the PT, it is SGLT2 that carries the burden of reabsorption of about 90% of filtered glucose in the PT. SGLT2 uses the electrochemical gradient of sodium ion to drive the transport of glucose against the concentration gradient3.
In 2008, US food and Drug Administration mandated that SGLT2 inhibitors (SGLT2i) undergo outcome trials. These drugs were later approved to be among the newest classes of medications currently available for the management of type 2 DM4,5. SGLT2i act by inhibiting renal SGLT2, thereby increasing glucosuria and lowering serum glucose6. While their renoprotection in diabetics has been clearly documented7, the potential for SGLT2i use and the mechanisms of nephroprotection8 in non-diabetic chronic kidney disease are still not well defined. Yet, recent trials9,10 weighed heavily in supporting the benefits of using SGLT2i irrespective of the diabetic status pointing towards that SGLT2i have other mechanisms of actions beyond blood sugar control.
In this review we will shed light on the role of these group of medications that act as SGLTi in non-diabetic patients focusing on pre-clinical and clinical data highlighting the mechanism of renoprotection and effects of SGLT2i in the non-diabetic kidneys.
Mechanism of Renoprotection in Non-Diabetic Kidney beyond Glucose Control (Table 1)
The protective effects of SGLT2i can occur independent of blood sugar levels11. In addition to their antihyperglycemic effects, SGLT2i have potential actions on the cardiovascular and renal systems 12. SGLT2i were shown to possess anti-inflammatory and antioxidant actions13, 14. SGLT2i act directly on the endothelial system leading to decrease inflammatory cytokines and reactive oxygen species.
Changes noted in the tubule-glomerular (TG) feedback mechanism on using SGLT2i may contribute to the beneficial effects of these drugs on kidney function. SGLT2i cause natriuresis, promoting TG feedback and decreasing glomerular hyperfiltration15.
Hawley et al.16 showed that while canagliflozin significantly activates adenosine mono-phosphate-activated protein kinase (AMPK), dapagliflozin and empagliflozin effect on AMPK are significantly milder and require higher concentration of these SGLT2i drugs. AMPK when activated, regulates the energy status and energy hemostasis, stimulates autophagy, thus decreasing cellular stress and glomerular and tubular injury17. Furthermore, the increase in adenosine release by SGLT2i may lead to efferent arteriole vasodilatation18. These hemodynamic changes by SGLT2i may mediate an albuminuria-lowering action, further contributing to kidney protection 19. Fioretto et al.20 suggested that improvement of lipid profile and body weight reduction by SGLT2i may also help protect the kidneys.
Other effects of SGLT2i, not related to diabetes control, included the potential modest reduction in both systolic21 and diastolic22 blood pressure, mainly due to natriuresis and decreased circulating volume.
Furthermore, SGLT2i were shown to reduce serum uric acid. Zhao et al.23 reviewed trials examining the effect of SGLT2i on serum uric acid in diabetic patients with at least 4 weeks of follow up (n=62 studies), and showed that SGLT2i significantly decreased serum uric acid compared with control regardless of the SGLT2i drug used.
Yip at al.24 showed similar results on reviewing 43 randomized controlled trials evaluating the effects of SGLT2i on serum uric acid in both patients with- and without diabetes. They showed reduction on serum uric acid by SGLT2i regardless of the diabetes status.
Rassaei et al.25 studied the effect of SGLT2i in non-diabetic patients with CKD stages 3-5 (n=78) and showed a reduction in serum uric acid from 6.4 to 5.6 mg/dl with increase in fractional excretion of urate from 6.76% to 9.22% following the use of dapagliflozin.

Table 1.
Reno-Protective Mechanisms of Actions of SGLT2i.
| -Antihyperglycemic -Anti-inflammatory→ Decreasing inflammatory and reactive oxygen species. -Antioxidant -Promote tubule-glomerular feedback→Decrease glomerular hyperfiltration -Activate adenosine mono-phosphate-activated protein kinase →Decrease glomerular and tubular injury -Hemodynamic changes→Decrease albuminuria -Improve lipid profile -Reduce body weight -Natriuresis→Mild decrease in systolic and diastolic blood pressure -Attenuate renal ischemia-reperfusion injury -Decrease serum uric acid |
2. SGLT2i and Non-Diabetic Kidney Dysfunction-Preclinical Experiments (Table 2)
Dapagliflozin
Dapagliflozin (10 mg/kg/day) for two days attenuated renal ischemia-reperfusion injury, improved renal function, reduced apoptotic cell death and increased renal expression of hypoxia induced factor 1 in C57BL/6 mice. The authors suggested that induction of hypoxia induced factor 1 may play a role in renoprotection in this model26. It was also reported that dapagliflozin (1 and 10 mg/kg/day) for three weeks improved renal function and ameliorated renal fibrosis in a model of adenine (0.2% diet) -induced renal injury in C57BL/6J mice. This was associated with increased mitochondrial metabolism and fatty acid oxidation, reduction of inflammation and oxidative stress. This study suggested that the renoprotective effect of dapagliflozin was related to mitochondrial protection due to inhibition of the transforming growth factor-β1/mitogen activated protein kinase (TGF-β1/MAPK) pathway activation, reduction of inflammation and oxidative stress27. Liu et al. 28 studied the effect of dapagliflozin on renal interstitial fibrosis induced by unilateral ureteral obstruction in C57BL/6J mice. They found that dapagliflozin (10 and 20 mg/kg/day) for two weeks improved renal function and renal fibrosis independent of direct blood glucose control. This was associated with reduced inflammation, apoptosis, oxidative stress and mitochondrial injury in the kidneys. Deger et al.29 showed that in Balb\c albino mice treated with cyclosporine A, dapagliflozin reduced oxidative stress, apoptosis, and histopathological damage in renal tissue caused by cyclosporin A. In C57BL/6N mice with protein-overload proteinuria induced by unilateral nephrectomy and injections of bovine serum albumin, dapagliflozin (1.5 mg/kg/day) treatment for twenty-three days reduced proteinuria and ameliorated podocyte dysfunction and loss and provided renal protection that was similar to lisinopril30.
It was also shown that dapagliflozin has a renoprotective effect in a model of salt-induced hypertension and cardiorenal disease in Dahl salt sensitive rats. In this study, dapagliflozin (0.1 mg/kg/day) for six weeks reduced albuminuria and attenuated renal inflammation and oxidative stress31. Firat et al.6 demonstrated that dapagliflozin (0.1 mg/kg/day) for four weeks preserved the glomerular and mesangial structure and reduced renal oxidative stress in an iron-overload rat model. Chang et al.32 showed that dapagliflozin (10 mg/kg/day) for six weeks attenuated doxorubicin induced glomerular atrophy, renal fibrosis, and dysfunction and suppressed apoptosis and reactive oxygen species production in rats. In spontaneously hypertensive rats, dapagliflozin (10 mg/kg/day) for eight weeks reduced urinary albumin creatinine ratio but had no significant effect on serum creatinine levels or renal histological changes. However, transcriptome analysis showed that dapagliflozin therapy exerted protective effects on the renal tissues that was attributed to alleviation of abnormal metabolism and inflammation33. Xuan et al. 34 showed that dapagliflozin (10 mg/kg/day) treatment for seven days reduced renal fibrosis in a unilateral ureteral obstruction rat model. On the contrary, in 5/6 (subtotally) nephrectomized rats, a model of progressive CKD, dapagliflozin (1 mg/kg/day) for twelve weeks did not attenuate heavy proteinuria, declining glomerular filtration rate, the extent of glomerulosclerosis, tubulointerstitial fibrosis or overexpression of the profibrotic cytokines, transforming growth factor-ß1 mRNA in the kidneys35. In subtotally nephrectomized rats, dapagliflozin (1 mg/kg/day) for eight weeks did not modify renal hemodynamic function nor did it attenuate proteinuria. In addition, dapagliflozin did not affect the increased glomerulosclerosis, increased glomerular collagen IV deposition, loss of glomerular capillaries, and increased infiltration of the tubule-interstitium by macrophages36.
Canagliflozin
Canagliflozin (10 and 25 mg/kg/day) treatment for 5 weeks attenuated adenine-induced chronic kidney disease in rats. This action involved an anti-inflammatory effect as shown by reducing the inflammatory markers, tumor necrosis factor (TNF)-α, interleukin (IL)-6 and IL-1β as well as reduction in oxidative stress14. In Male C57BL/6 mice fed with 0.2% adenine, canagliflozin (10 mg/kg/day) treatment for 2 weeks, started after five weeks of adenine diet, did not ameliorate renal damage, however it reduced the accumulation of uremic toxins including p-cresyl sulfate. The authors suggested that the lack of an effect on renal damage might be due to that the administration period may have been too short37. Moreover, in adenine-induced chronic kidney disease, treatment with canagliflozin (25 mg/kg/day) for four weeks failed to ameliorate the progressive loss of kidney function and there was no decreased interstitial area percentage, nor was there altered expression levels of genes related to fibrosis and inflammation. The authors concluded that canagliflozin dosage was not effective in a therapeutic setting of established nondiabetic CKD since canagliflozin treatment was started after 4 weeks of adenine treatment 38. Canagliflozin (5 mg/kg/day) for one week was also shown to improve kidney function in isoprenaline-treated rats by stimulating antioxidant, anti-inflammatory and anti-apoptotic signaling pathways39. In high-salt (8% sodium chloride) diet-induced Dahl salt-sensitive rats hypertensive renal injury, canagliflozin (30 mg/kg/day) for twelve weeks attenuated the increase in blood pressure and ameliorated the associated hypertensive-induced renal injury. Canagliflozin increased sirtuin 3 expression, decreased epithelial-mesenchymal transition and oxidative stress and inhibited renal fibrosis40. In addition, canagliflozin (10 and 30 mg/kg/day) for ten days reversed the biochemical and histopathological indices of cisplatin-induced nephrotoxicity in mice possibly through its anti-inflammatory and antioxidant effects41. Park et al.42 also showed that in mice, canagliflozin (10 mg/kg/day) treatment for five days protected against cisplatin-induced acute kidney injury by activating adenosine monophosphate-activated protein kinase (AMPK) and autophagy in renal proximal tubular cells. Song et al.43 also showed that in mice, canagliflozin (20 mg/kg/day) for eight days had a nephroprotective effect in cisplatin induce nephrotoxicity. This effect mainly depends on Akt activation as well as reduced uptake of cisplatin in the kidneys. Moreover, canagliflozin (20 mg/kg/day) was effective in providing renal protection in unilateral ureteral occlusion and ischemia-reperfusion renal fibrosis mouse models44. In rats with membranous nephropathy, treatment with canagliflozin (10 mg/kg/day) for eight weeks decreased proteinuria and improved the hyperplasia of glomerular mesangial cells and stroma, the thickening of basement membrane and spiky structure. In addition, canagliflozin reduced renal immune complex deposition and improved podocyte injury. The authors concluded that canagliflozin exerts this renoprotective effect by reversing the imbalance in Helper T 1/Helper T 2 cells and restoring the autophagy of podocytes inhibited by the abnormal immunoglobulin G secretion from B-cells45.
Empagliflozin
In a 5/6 nephrectomy rat model, a model of chronic kidney disease, empagliflozin (15 mg/kg/day) treatment for ninety-five days caused reduced proteinuria, improvement in creatinine clearance and renal interstitial fibrosis and glomerulosclerosis. The authors suggested two mechanisms of renoprotection; tubule-glomerular feedback mediated effects and alterations of gene expression of key components of the complement system8. Lu et al.46 also showed that empagliflozin (15 mg/kg/day) for six weeks had a beneficial effect on kidney function and morphology in the 5/6 nephrectomy rat model. They suggested that this beneficial effect might be due to an inhibition of CD206+CD68+ M2 macrophage polarization by targeting mammalian target of rapamycin (mTOR) and mitophagy pathways and attenuating inflammatory signals from CD8+ effector T cells. Kim et al.47 showed that empagliflozin (20 mg/kg/day) for three weeks, in a rat model salt sensitive hypertension induced by uni-nephrectomy and 8% sodium chloride intake in Sprague Dawley rats, decreased blood pressure and ameliorated renal inflammation. The beneficial renal protective effect of empagliflozin (10 mg/kg/day) for eight weeks was also shown in spontaneously hypertensive rats expressing human C-reactive protein and it was suggested that it was mediated by reduced renal lipid accumulation, inflammation and oxidative stress48. In addition, empagliflozin (10 mg/kg/day) for four weeks reduced blood pressure and had a nephroprotective effect in cyclosporine A induced nephropathy in rats49. In rats with angiotensin II induced hypertension, empagliflozin (10 mg/kg/day) for two weeks prevented the development of renal fibrosis, an effect that was caused by reduction in inflammatory infiltrates50. Reyes-Pardo et al.51 showed also that empagliflozin (10 mg/kg/day) treatment for two weeks attenuated oxidative stress, proteinuria and glomerular filtration rate reduction associated with angiotensin II infusion, thereby reducing kidney damage development in a rat model of angiotensin II dependent kidney damage. In hypertensive and proteinuric renin-transgenic (mRen2)27 rats with additional administration of N(ω)-nitro-L-arginine methyl ester (a nitric oxide synthase inhibitor), treatment with empagliflozin (3 and 10 mg/kg/day) dose dependently reduced proteinuria and induced protection for renal vasculopathy, glomerulopathy, and tubular degeneration52. The combination of the low dose (3 mg/kg/day) of empagliflozin and finerenone, a non-steroidal mineralocorticoid receptor antagonist, resulted in efficacious reduction in proteinuria, plasma creatinine and uric acid and renal lesions52. Empagliflozin (10 mg/kg/day) but not canagliflozin (30 mg/kg/day) for seven days was able to reduce renal tubular dilatation and necrosis in renal ischemia-reperfusion injury model in rats. Empagliflozin did not have a significant effect on serum creatinine and blood urea nitrogen (BUN) levels while canagliflozin increased both parameters than in the placebo-treated group. In addition, the increased renal kidney injury molecule (KIM)-1 expression and decreased urinary microRNA-26a excretion was alleviated by empagliflozin only53. Ala et al.54 also showed that empagliflozin (10 mg/kg/day) for 2 days attenuated renal ischemia-reperfusion injury in rats that was associated with reduced oxidative stress, inflammation and apoptosis. In C57/BL6 mice subjected to renal ischemia-reperfusion injury, empagliflozin (1 mg/kg) given twice protected against renal injury as shown by decreased serum levels of creatinine, attenuated tubular damage, reduced inflammatory markers and inhibited apoptosis55. Ge et al.56 showed that empagliflozin (70 mg/kg/day in the chow) for four weeks reduced podocyte lipotoxicity prevented renal lipid accumulation and improved renal function in a mouse model of Alport syndrome56. In a mouse model with vascular calcification induced by an oral high-phosphorus diet following a 5/6 nephrectomy in Apo E−/− mice, empagliflozin (10 mg/kg/day) treatment for eight weeks improved renal function57. Empagliflozin (10 mg/kg/day) treatment for fourteen days did not affect chronic kidney disease progression in oxalate-related nephrocalcinosis in C57BL/6N mice. This was demonstrated as empagliflozin had no effect on reduced glomerular filtration rate, crystal deposition, tubular injury and markers of interstitial fibrosis58. In three models of chronic kidney disease, fawn-hooded hypertensive rats, uni-nephrectomized salt-loaded rats, and in rats with Goldblatt hypertension (two-kidney, one-clip 2K1C), empagliflozin (10 mg/kg/day) for eight weeks did not provide renoprotection because it did not ameliorate proteinuria, elevated plasma urea and creatinine, oxidative stress or inflammation59.
Ipragliflozin
Ipragliflozin (0.3 and 0.1 mg/kg/day) treatment for four weeks was shown to have a renoprotective effect that was independent from plasma glucose levels and urinary glucose excretion in adenine (0.25% w/w in the diet) induced chronic kidney disease in C57BL/6JJcl mice. The anti-inflammatory and antioxidant effect of ipragliflozin might have contributed to the protective effect 60. In addition, ipragliflozin (1 mg/kg/day) for twelve weeks improved the pathogenesis of chronic kidney disease by reducing ectopic lipid deposition in renal tubules, endoplasmic reticulum stress in a mouse (FLS-ob/ob) model of non-alcoholic steatohepatitis61. Ipragliflozin (0.04%) monotherapy during eight weeks of a high-salt diet did not improve renal glomerulosclerosis or creatinine clearance in Dahl Salt sensitive rats. However, the combination therapy of ipragliflozin and losartan significantly ameliorated glomerulosclerosis compared with ipragliflozin or losartan monotherapy62.
In conclusion, preclinical trials showed that dapagliflozin, canagliflozin, empagliflozin or ipragliflozin had renoprotective effects in various animal models of acute kidney injury and chronic kidney diseases.
Table 2.
Effects of SGLT2i on Experimental Animals.
| Drug | Animal | Effects of SGLT2i | Ref. |
|---|---|---|---|
| Dapagliflozin | C57BL/6 mice with renal-reperfusion injury - C57BL/6J mice with adenine (0.2% diet) -induced renal injury -Unilateral ureteral obstruction in C57BL/6J mice -Balb\c albino mice treated with cyclosporine A -C57BL/6N mice with protein-overload proteinuria induced by unilateral nephrectomy and injections of bovine serum albumin - Dahl salt sensitive rats with salt-induced hypertension and cardiorenal disease -Iron-overload rat model -Rats with doxorubicin induced glomerular atrophy -Spontaneously hypertensive rats -Rats with unilateral ureteral obstruction -Rats with 5/6 (subtotally) nephrectomized - Rats with subtotally nephrectomized |
-Attenuated renal ischemia-reperfusion injury, improved renal function, reduced apoptotic cell death and increased renal expression of hypoxia induced factor 1 -Improved renal function and ameliorated renal fibrosis, increased mitochondrial metabolism and fatty acid oxidation, reduction of inflammation and oxidative stress. -Improved renal function and renal fibrosis independent of direct blood glucose control -Reduced oxidative stress, apoptosis, and histopathological damage in renal tissue -Reduced proteinuria and ameliorated podocyte dysfunction and loss and provided renal protection -Reduced albuminuria and attenuated renal inflammation and oxidative stress- Preserved the glomerular and mesangial structure and reduced renal oxidative stress -Attenuated glomerular atrophy, renal fibrosis, and dysfunction -Reduced urinary albumin creatinine ratio but had no significant effect on serum creatinine levels or renal histological changes - Reduced renal fibrosis -Did not attenuate heavy proteinuria, declining glomerular filtration rate, the extent of glomerulosclerosis or tubulointerstitial fibrosis -Did not modify renal hemodynamic function nor attenuated proteinuria |
26 27 28 29 30 31 6 32 33 34 35 36 |
| Canagliflozin | -Rats with adenine-induced chronic kidney disease - Male C57BL/6 mice fed with 0.2% adenine Rats with adenine-induced chronic kidney disease Rats, isoprenaline-treated - Dahl salt-sensitive rats with high-salt diet-inducing hypertensive renal injury. - Mice with cisplatin-induced nephrotoxicity. - Mice with cisplatin-induced nephrotoxicity. -Mice with cisplatin induced nephrotoxicity. -Mice with unilateral ureteral occlusion and ischemia-reperfusion renal fibrosis -Rats with membranous nephropathy |
-Attenuated adenine induced chronic kidney disease, anti-inflammatory effect as well as reduction in oxidative stress -Did not ameliorate renal damage, however it reduced the accumulation of uremic toxins including p-cresyl sulfate -Failed to ameliorate the progressive loss of kidney function and there was no decreased interstitial area percentage, nor was there altered expression levels of genes related to fibrosis and inflammation -Improve kidney function by stimulating antioxidant, anti-inflammatory and anti-apoptotic signaling pathways -Attenuated the increase in blood pressure and ameliorated the associated hypertensive-induced renal injury, decreased epithelial-mesenchymal transition and oxidative stress and inhibited renal fibrosis -Reversed the biochemical and histopathological indices of possibly through its anti-inflammatory and antioxidant effects -Protected against cisplatin-induced acute kidney injury by activating adenosine monophosphate-activated protein kinase and autophagy in renal proximal tubular cells -Nephroprotective effect by Akt activation, reduced uptake of cisplatin in the kidneys. -Renal protection -Decreased proteinuria and improved the hyperplasia of glomerular mesangial cells and stroma, the thickening of basement membrane and spiky structure. |
13 37 38 39 40 41 42 43 44 45 |
| Empagliflozin | - Rats with 5/6 nephrectomy - Rats with 5/6 nephrectomy - Sprague Dawley rats with uni-nephrectomy and salt sensitive hypertension. -Spontaneously hypertensive rats -Rats with cyclosporine A induced nephropathy -Rats with angiotensin II induced hypertension -Rats with angiotensin II dependent kidney damage -Hypertensive and proteinuric renin-transgenic (mRen2)27 rats with additional administration of nitric oxide synthase inhibitor -Rats with renal ischemia-reperfusion injury - Rats with renal ischemia-reperfusion injury - C57/BL6 mice subjected to renal ischemia-reperfusion injury -Mouse model of Alport syndrome - Apo E−/− mice with vascular calcification and 5/6 nephrectomy - C57BL/6N mice with oxalate-related nephrocalcinosis -Fawn-hooded hypertensive rats -Uni-nephrectomized salt-loaded rats -Rats with Goldblatt hypertension |
- Reduced proteinuria, improved in creatinine clearance and renal interstitial fibrosis and glomerulosclerosis. - beneficial effect on kidney function and morphology due to an inhibition of CD206+CD68+ M2 macrophage polarization by targeting mammalian target of rapamycin (mTOR) and mitophagy pathways and attenuating inflammatory signals from CD8+ effector T cells. -Decreased blood pressure and ameliorated renal inflammation. -Beneficial renal protection by reducing renal lipid accumulation, inflammation and oxidative stress -Reduced blood pressure -Prevented the development of renal fibrosis by reducing inflammatory infiltrates -Reduced kidney damage by attenuating oxidative stress, proteinuria and glomerular filtration rate reduction associated with angiotensin II infusion -Reduced proteinuria and induced protection for renal vasculopathy, glomerulopathy, and tubular degeneration -Reduced renal tubular dilatation and necrosis -Attenuated renal injury with reduced oxidative stress, inflammation an apoptosis -Protected against renal injury, attenuated tubular damage, reduced inflammatory markers and inhibited apoptosis -Reduced podocyte lipotoxicity prevented renal lipid accumulation and improved renal function -Improved renal function -Did not affect chronic kidney disease progression in oxalate-related nephrocalcinosis -Did not provide renoprotection because it did not ameliorate proteinuria, elevated plasma urea and creatinine, oxidative stress or inflammation |
8 46 47 48 49 50 51 52 53 54 55 56 57 58 59 |
| Ipragliflozin | - C57BL/6JJcl mice with adenine induced chronic kidney disease -Mouse (FLS-ob/ob) model of non-alcoholic steatohepatitis - Dahl Salt sensitive rats |
- Renoprotective effect that was independent from plasma glucose levels and urinary glucose excretion - Improved the pathogenesis of chronic kidney disease by reducing ectopic lipid deposition in renal tubules, endoplasmic reticulum stress - Did not improve renal glomerulosclerosis or creatinine clearance |
60 61 62 |
3. SGLT2 and Non-Diabetic Kidney Dysfunction-Clinical Trials (Table 3)
3.1. Effects of SGLT2i on CKD
Several original trials and metanalyses studies were done to elicit the effects of SGLT2i on patients with CKD. These studies included both patient with and without DM.
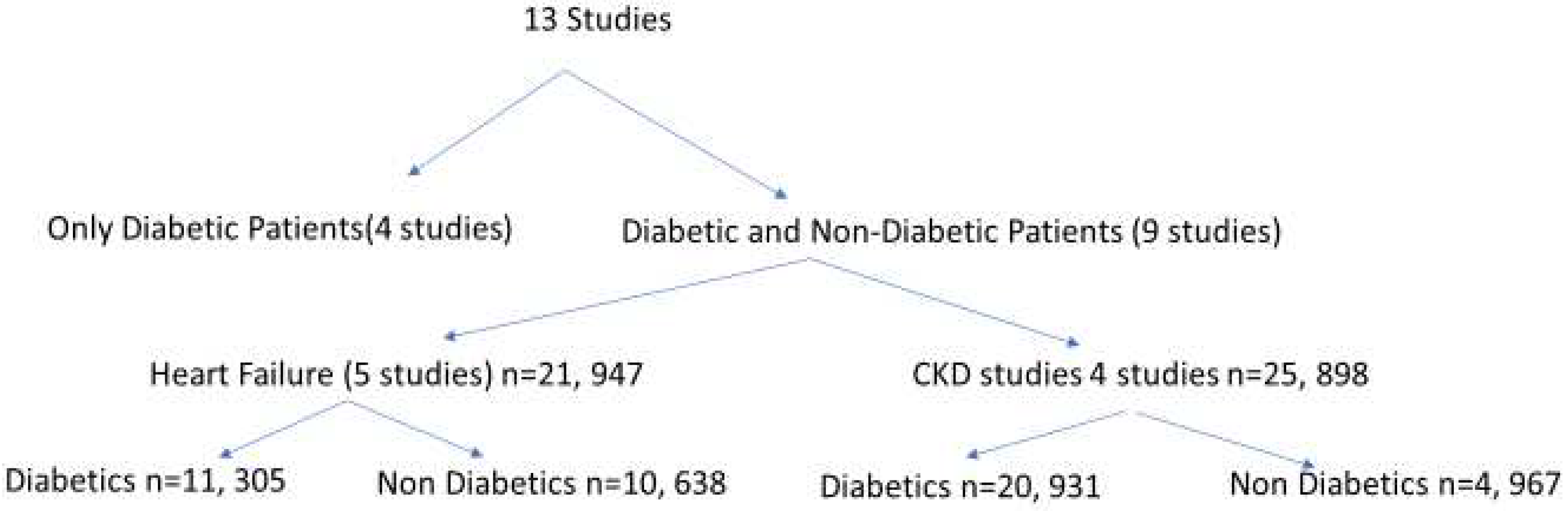
We looked to tease the effect of SGLT2i on non-diabetics in these metanalyses. A recent study63 underwent a systemic review and metanalysis of large placebo-controlled trials using SGLT2i and identified 13 studies with 90, 413 participants (Figure 1). Of those, the number of non-diabetic patients were 15,605/47,845 participant (32.6%).
Of the four CKD studies, two studies involved most of the non-diabetic patients. The study by Heerspink et al.64 (DAPA-CKD) included 1398/4304 (32.5%) non diabetics while the EMPA-CKD trial10 had 3569/6609 (54.0%) with no DM. Their mean baseline eGFR ranged from 37-56 ml/min/1.73 m2 with a follow up of 1.3-2.6 years.
The study by Heerspink et al.64 was prematurely stopped as dapagliflozin proved its efficacy versus placebo over a median of 2.4 years. They showed a reduced risk of a composite of a sustained decline in the estimated GFR of at least 50%, ESKD, or death from renal or cardiovascular causes with dapagliflozin than with placebo. Similarly, Empagliflozin showed a similar superiority over placebo in decreasing the composite of progression of kidney disease10. In both studies, the diabetic status, the baseline eGFR and primary cause of CKD had no impact on the renal outcomes.
Four out of the 5 heart failure studies included non-diabetic patients65-68. Their mean eGFR ranged 62 to 68 ml/min/1.73 m2, with a follow up ranging between 0.8- 2.2 years. Analyzing these studies showed that SGLT2i deceased the risk of CKD progression regardless of the presence or absence of DM, baseline eGFR or the primary etiology of CKD.
A year later, Rassaei et al.69 added 5 more studies to the prior metanalysis and studied the impact of SGLT2i on renal parameters focusing on non-diabetic patients. Out of 46 full texts, they reviewed 7 studies in depth9, 36, 64, 70-73. Studies reviewed had a follow up period ranging from 6 weeks-2.4 years, 6 trials used dapagliflozin 9, 36,64, 70-72 while one trial used empagliflozin 73. Their review demonstrated that SGLT2i had a reno-protective effect as demonstrated by delaying reduction of eGFR and decreasing urine albumin: creatinine ratio (UACR). Vart et al.74 further suggested that adding RAAS blockers to SGLT2i in non-diabetic albuminuric patients may increase the kidney failure-free survival. While in one study70, dapagliflozin was shown to cause reversible decrease in eGFR in 6 weeks after washout period following stopping the drug, another study36 failed to show that dapagliflozin benefits patients who had preserved kidney function.
3.2. Effects of SGLT2i on Glomerular Disorders
3.2.1. IgA Nephropathy (IgAN)
Wheeler et al.71 analyzed the DAPA-CKD study based9 on the primary etiology of CKD. The studied outcome was the effects of dapagliflozin on sustained decline in eGFR of 50% or more, ESKD, or death from a kidney disease-related or cardiovascular cause. The study included 270 participants with investigator-reported IgAN (confirmed by renal biopsy in 94% of the participants). Only 14.1% of the cohort had DM. Participants receiving dapagliflozin (n=137) and those receiving placebo (n=133) were followed for a median of 2.1 years (0.025-3.2 years). Mean eGFR and median UACR were 44.3 (12.4) ml/min/1.73 m2 and 889.5 (557.5-1472.0) mg/g and 43.2 (12.0) ml/min/1.73 m2 and 902.5 (500.5-1633.0) mg/g in the dapagliflozin and placebo, respectively. The study showed superiority of dapagliflozin over placebo on primary composite (p=0.005) and secondary kidney-specific outcomes (p= 0.002). There was 76% reduction in ESKD and >50% reduction in eGFR decline and in renal death. These effects did not differ based on eGFR or UACR with annual decline in eGFR less in the dapagliflozin group versus Placebo (-2.2 +/- 0.5 vs -4.6 +/- 0.47 ml/min /1.73 m2).
Similar results were found on analyzing the EMPA-KIDNEY trial10 with 817 patients in the study having IgAN. Empagliflozin reduced the kidney endpoint of IgAN patients (progression of CKD disease) by about 30% versus placebo. Combining results of these 2 studies showed a 51% decrease in CKD progression in patients with IgAN75.
Dong et al.76 followed a cohort of Chinese patients with biopsy-proven IgAN for 3 and 6 months after being treated with SGLT2i. Most of the IgAN cohort were non-diabetic (81.7%). The authors observed a significant reduction in proteinuria in their patient cohort independent of immunosuppressive agents and baseline eGFR and proteinuria levels, again confirming a role of SGLT2i in the management of IgAN.
3.2.2. Focal Segmental Glomerulosclerosis (FSGS)
Rajasekeran et al. studied36 the effect of 8 weeks of dapagliflozin on GFR in humans (n=10) and in experimental FSGS. The secondary end points were related to changes in the renal hemodynamic function, proteinuria, and blood pressure. They noted non statistical difference in PAH-based GFR. When stratified in 2 subgroups based on GFR, the researches noted a significant decrease in GFR in the group of patients with GFR> 90 m/min/1.73 m2. They further showed that dapagliflozin failed to modify kidney hemodynamics or attenuate proteinuria.
Two years after the prior study, Cherney et al.70 performed a short-term crossover, randomized controlled trial (DIAMOND) at six hospitals in three countries. Their goal was to investigate the efficacy of SGLT2i in proteinuric kidney disease without diabetes. Eleven patients with FSGS were randomly assigned (1:1) to receive placebo followed by dapagliflozin 10 mg per day or vice versa. Each treatment period lasted 6 weeks with a 6-week washout period in between. The primary outcome was the effect of dapagliflozin on proteinuria and other hemodynamic parameters. While the researchers demonstrated a nonsignificant reduction in proteinuria compared with placebo, GFR was temporary decreased during the six weeks of dapagliflozin.
A larger study analyzing patients with biopsy-proven FSGS (n= 104) in the DAPA-CKD trial 64 showed reduced rate of eGFR decline versus placebo but failed to show any statistically significant difference between the drug and the placebo group77. It is postulated that this negative result could be attributed to the small number of events (4 primary outcomes in dapagliflozin versus 7 in the placebo group).
Thus, data remains non- conclusive as for the role of SGLT2i in managing patients with FSGS. The lack of long-term data and a larger study population to address the potential efficacy of SGLT2i in FSGS leave a knowledge gap that begs for further studies.
3.3. Effects of SGLT2i on Blood Pressure
Miyata et al.11 reviewed the mechanisms of decreasing blood pressure upon using SGLT2i. They suggested that the decrease in plasma volume as a result of their diuretic and natriuretic effects, weight loss and the anti-inflammatory action of these drugs may contribute to the anti-hypertensive effects. Other mechanisms identified that may contribute to the SGLT2i effects on blood pressure was the noted improvement in arterial stiffness and endothelial function21,78.
While the effect of SGLT2i in lowering blood pressure in diabetics is well established79, studies of the role of SGLT2i in lowering blood pressure in non-diabetics did not show the same effect 36, 70. Cherney et al.70 studied non-diabetic patients (n=53, GFR>25 ml/min, proteinuria 500-3500 mg/g) comparing dapagliflozin effects on blood pressure versus placebo over 6 weeks. Patient who started on dapagliflozin (n= 27) were switched to placebo, and patients on placebo (n=26) were switched to receive dapagliflozin. The researchers showed no change in systolic (SBP) and diastolic (DBP) blood pressure with no hypoglycemic episodes. Decrease in body weight with dapagliflozin was 1.5 kg (p=0.046).
Zanchi et al.80 performed a randomized control study on non-diabetic normotensive patients (n=39) comparing the effect of empagliflozin (n-26) versus placebo (n=13) on blood pressure. Their results were different than the prior studies where empagliflozin was shown to decrease SBP/DBP (-5+ 7 and -2 + 6 respectively) over a one-month study period. Similarly, Bays et al.81 underwent a randomized, double blinded study comparing canagliflozin effect in 3 different dosages on blood pressure in non-diabetics versus placebo (n=376). At the end of the study (12 weeks), the researchers demonstrated a decrease in blood pressure in both canagliflozin and placebo groups. While the reduction in SBP was more in the canagliflozin groups (-2.0 to -3.3 versus -1.4 mmHg), the reduction in DBP was more in the placebo group (-1.8 versus -0.7 to -1.4 mmHg). Diaz-Cruz et al.82 was also able to show a decrease in both SBP and DBP on using dapagliflozin in patients who were pre-diabetics.
3.4. Effects of SGLT2i on Nephrotic Proteinuria
Kalay et al.83 reviewed studies examining the effects of SGLT2i on patients with nephrotic range proteinuria and identified 9 studies. While most patients in these studies were diabetics, two studies included non-diabetic patients with FSGS84, 85.
Boeckhaus et al.84 reported on 2 cases with FSGS where SGLT2i reduced UACR ratio by 84% at 11 months in one patient and by 18% at 3 months in another. Same data was reported in another study85 on a patient with FSGS where UACR was decreased by 61% after one months and by 37% after 9 months of using SGLT2i.
4. Effects of SGLT2i on Survival
Awad et al.86 reviewed randomized clinical trials (12 studies) focusing on the effect of SGLT2i on mortality in both diabetic and non-diabetic patients. While mortality risks were decreased in both groups, it was not statistically significant in the non-diabetic patients (RR=0.93, 95% CI 0.70-1.23).
Heerspink et al.9 showed that dapagliflozin decreased risk of both renal and cardiovascular mortality, and when RAAS blockers were added to dapagliflozin, patients’ survival was further increased. More recently, McEwan et al.87 used a model analysis on DAPA-CKD trial and showed that dapagliflozin may reduce all-cause mortality.
Table 3.
Renal Beneficial Effects of SGLT2i in Non-Diabetic Patients.
|
- Delay progression of CKD - Role in management of IgA Nephropathy - Potential role in the management of Focal segmental Glomerulosclerosis - Decrease Blood Pressure - Decrease Proteinuria - Improve renal-related survival |
5. SGLT2i Side Effects
While using SGLT2i were not associated with hypoglycemia in non-diabetic patients, several significant side effects were noted when using these drugs.
Hypotension secondary to diuresis9, natriuresis and volume depletion has been reported. Furthermore, the excessive diuresis may impact poorly on patients’ quality of life. Urinary tract infection (UTI) mainly secondary to yeast infection has been associated with the use of SGLT2i 88. UTI can range from mild to severe infections. A more severe form of infection, genital mycotic infection, has been described in diabetics, but not in non-diabetics89.
Other side effects were suggested to be associated with SGLT2i as bone fractures, amputations and malignancies, but results are controversial90.
6. Future Directives
Addition of newer agents that showed benefits in managing patients with kidney diseases to SGLT2i may be beneficial. Zhang et al.91 performed a systemic literature search of randomized control trials comparing mineralocorticoid receptor antagonist (finerenone), SGLT-2i and glucagon-like peptide-1 receptor agonists (GLP-1 RA) in diabetics with CKD. They identified 18 studies (n=51,496) that demonstrated that while SGLT2i significantly decreased the risk of renal events compared with finerenone and GLP-1 RA, their cardiac outcome effects were comparable.
Trials comparing additive effects of SGLT2i with GLP-1 RA, mineralocorticoid or endothelin receptor antagonist to SGLT2i alone in both diabetics and non-diabetics may prove to be very helpful in improving renal outcomes.
7. Conclusions
SGLT2i group play a major role in managing non-diabetic patients with kidney diseases. This group of drugs can achieve their role through different mechanisms unrelated to glycemic control. More studies looking at effects of SGLT2i on different renal pathologies causing CKD, examining the effects of SGLT2i alone or in combination of other therapeutic groups, their possible side effects and mechanism of action are very much needed.
References
- Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022 Apr;12(1):7-11. Epub 2022 Mar 18. PMID: 35529086; PMCID: PMC9073222. [CrossRef]
- https://usrds-adr.niddk.nih.gov/2022/end-stage-renal-disease/1-incidence-prevalence-patient-characteristics-and-treatment-modalities.Accessed 12/23/2023.
- Vallon V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu Rev Med. 2015;66:255-70. Epub 2014 Oct 17. PMID: 25341005. [CrossRef]
- Baker WL, Buckley LF, Kelly MS, Bucheit JD, Parod ED, Brown R, Carbone S, Abbate A, Dixon DL. Effects of Sodium-Glucose Cotransporter 2 Inhibitors on 24-Hour Ambulatory Blood Pressure: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2017 May 18;6(5):e005686. PMID: 28522675; PMCID: PMC5524106. [CrossRef]
- Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW; CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019 Jun 13;380(24):2295-2306. Epub 2019 Apr 14. PMID: 30990260. [CrossRef]
- Fırat SN, Kuşkonmaz ŞM, Çaydere M, Şeneş M, Hücümenoğlu S, Çulha C. Renoprotective effects of dapagliflozin in an iron overload non-diabetic rat model. Adv Med Sci. 2022 Sep;67(2):311-315. [CrossRef]
- Xuan MY, Piao SG, Ding J, Nan QY, Piao MH, Jiang YJ, Zheng HL, Jin JZ, Li C. Dapagliflozin alleviates renal fibrosis by inhibiting RIP1-RIP3-MLKL-mediated necroinflammation in unilateral ureteral obstruction. Front Pharmacol. 2022 Jan 7;12:798381. eCollection 2021. [CrossRef]
- Chen X, Delić D, Cao Y, Shen L, Shao Q, Zhang Z, Wu H, Hasan AA, Reichetzeder C, Gaballa MMS, Krämer BK, Klein T, Yin L, He B, Morgera S, Hocher B. Renoprotective effects of empagliflozin are linked to activation of the tubuloglomerular feedback mechanism and blunting of the complement system. Am J Physiol Cell Physiol. 2023 Apr 1;324(4):C951-C962. Epub 2023 Feb 13. [CrossRef]
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, Mann JFE, McMurray JJV, Lindberg M, Rossing P, Sjöström CD, Toto RD, Langkilde AM, Wheeler DC; DAPA-CKD Trial Committees and Investigators. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020 Oct 8;383(15):1436-1446. Epub 2020 Sep 24. PMID: 32970396. [CrossRef]
- The EMPA-KIDNEY Collaborative Group; Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR, Preiss D, Judge P, Mayne KJ, Ng SYA, Sammons E, Zhu D, Hill M, Stevens W, Wallendszus K, Brenner S, Cheung AK, Liu ZH, Li J, Hooi LS, Liu W, Kadowaki T, Nangaku M, Levin A, Cherney D, Maggioni AP, Pontremoli R, Deo R, Goto S, Rossello X, Tuttle KR, Steubl D, Petrini M, Massey D, Eilbracht J, Brueckmann M, Landray MJ, Baigent C, Haynes R. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023 Jan 12;388(2):117-127. Epub 2022 Nov 4. PMID: 36331190; PMCID: PMC7614055. [CrossRef]
- Miyata KN, Zhang SL, Chan JSD. The Rationale and Evidence for SGLT2 Inhibitors as a Treatment for Nondiabetic Glomerular Disease. Glomerular Dis. 2021 Mar 19;1(1):21-33. PMID: 36751486; PMCID: PMC9677741. [CrossRef]
- Lovshin JA, Gilbert RE (2015) Are SGLT2 inhibitors reasonable antihypertensive drugs and renoprotective. Curr Hypertens Rep 17(6):551. [CrossRef]
- Tang L, Wu Y, Tian M, Sjöström CD, Johansson U, Peng XR, Smith DM, Huang Y (2017) Dapagliflozin slows the progression of the renal and liver fibrosis associated with type 2 diabetes. Am J Physiol Endocrinol Metab 313:E563-E576.
- Ali BH, Al Salam S, Al Suleimani Y, Al Za'abi M, Abdelrahman AM, Ashique M, Manoj P, Adham SA, Hartmann C, Schupp N, Nemmar A. Effects of the SGLT-2 inhibitor canagliflozin on adenine-induced chronic kidney disease in rats. Cell Physiol Biochem. 2019;52(1):27-39. Epub 2019 Feb 18. [CrossRef]
- Rajasekeran, Harindraa,b; Cherney, David Z.a,b,*; Lovshin, Julie A.c,*. Do effects of sodium–glucose cotransporter-2 inhibitors in patients with diabetes give insight into potential use in non-diabetic kidney disease?. Current Opinion in Nephrology and Hypertension 26(5):p 358-367, September 2017. [CrossRef]
- Hawley SA, Ford RJ, Smith BK, Gowans GJ, Mancini SJ, Pitt RD, Day EA, Salt IP, Steinberg GR, Hardie DG. The Na+/Glucose Cotransporter Inhibitor Canagliflozin Activates AMPK by Inhibiting Mitochondrial Function and Increasing Cellular AMP Levels. Diabetes. 2016 Sep;65(9):2784-94. Epub 2016 Jul 5. PMID: 27381369; PMCID: PMC5689380. [CrossRef]
- Packer M. Interplay of adenosine monophosphate-activated protein kinase/sirtuin-1 activation and sodium influx inhibition mediates the renal benefits of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes: A novel conceptual framework. Diabetes Obes Metab. 2020 May;22(5):734-742. Epub 2020 Feb 20. PMID: 31916329. [CrossRef]
- van Bommel EJM, Muskiet MHA, van Baar MJB, Tonneijck L, Smits MM, Emanuel AL, Bozovic A, Danser AHJ, Geurts F, Hoorn EJ, Touw DJ, Larsen EL, Poulsen HE, Kramer MHH, Nieuwdorp M, Joles JA, van Raalte DH. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than pre-glomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 2020 Jan;97(1):202-212. Epub 2019 Oct 10. Erratum in: Kidney Int. 2020 May;97(5):1061. PMID: 31791665. [CrossRef]
- Jongs N, Greene T, Chertow GM, McMurray JJV, Langkilde AM, Correa-Rotter R, Rossing P, Sjöström CD, Stefansson BV, Toto RD, Wheeler DC, Heerspink HJL; DAPA-CKD Trial Committees and Investigators. Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021 Nov;9(11):755-766. Epub 2021 Oct 4. PMID: 34619106. [CrossRef]
- Fioretto P, Zambon A, Rossato M, Busetto L, Vettor R. SGLT2 Inhibitors and the Diabetic Kidney. Diabetes Care. 2016 Aug;39 Suppl 2:S165-71. PMID: 27440829. [CrossRef]
- Lambers Heerspink HJ, de Zeeuw D, Wie L, Leslie B, List J. Dapagliflozin a glucose-regulating drug with diuretic properties in subjects with type 2 diabetes. Diabetes Obes Metab. 2013 Sep;15(9):853-62. Epub 2013 Jun 5. PMID: 23668478; PMCID: PMC3906841. [CrossRef]
- Storgaard H, Gluud LL, Bennett C, Grøndahl MF, Christensen MB, Knop FK, Vilsbøll T. Benefits and Harms of Sodium-Glucose Co-Transporter 2 Inhibitors in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. PLoS One. 2016 Nov 11;11(11):e0166125. PMID: 27835680; PMCID: PMC5106000. [CrossRef]
- Zhao Y, Xu L, Tian D, Xia P, Zheng H, Wang L, Chen L. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2018 Feb;20(2):458-462. Epub 2017 Sep 27. PMID: 28846182. [CrossRef]
- Yip ASY, Leong S, Teo YH, Teo YN, Syn NLX, See RM, Wee CF, Chong EY, Lee CH, Chan MY, Yeo TC, Wong RCC, Chai P, Sia CH. Effect of sodium-glucose cotransporter-2 (SGLT2) inhibitors on serum urate levels in patients with and without diabetes: a systematic review and meta-regression of 43 randomized controlled trials. Ther Adv Chronic Dis. 2022 Mar 23;13:20406223221083509 PMID: 35342538; PMCID: PMC8949773. [CrossRef]
- Rasaei N, Malekmakan L, Gholamabbas G, Mashayekh M, Hadianfard F, Torabi M. Sodium-Glucose Cotransporter-2 Inhibitors in Patients with Non-diabetic Chronic Kidney Disease: A Systematic Review. Iran J Kidney Dis. 2023 Jul;17(4):175-183. PMID: 37634243.
- Chang WT, Chang YK, Choi H, Jeong JY, Na KR, Lee KW, Lim BJ, Choi DE. Dapagliflozin, SGLT2 inhibitor, attenuates renal ischemia-reperfusion injury. PLoS One. 2016 Jul 8;11(7):e0158810. Erratum in: PLoS One. 2016;11(7):e0160478. PMID: 27391020; PMCID:PMC4938401. [CrossRef]
- Zeng J, Huang H, Zhang Y, Lv X, Cheng J, Zou SJ, Han Y, Wang S, Gong L, Peng Z. Dapagliflozin alleviates renal fibrosis in a mouse model of adenine-induced renal injury by inhibiting TGF-β1/MAPK mediated mitochondrial damage. Front Pharmacol. 2023 Mar 7;14:1095487. eCollection 2023. [CrossRef]
- Liu Y, Wang Y, Chen S, Bai L, Xie X, Zhang L, Wang X. Investigation into the effect and mechanism of dapagliflozin against renal interstitial fibrosis based on transcriptome and network pharmacology. Int Immunopharmacol. 2022 Nov;112:109195. Epub 2022 Sep 5. [CrossRef]
- Deger M, Kaya B, Akdogan N, Kaplan HM, Bagir E, Izol V, Aridogan IA. Protective effect of dapagliflozin against cyclosporine A-induced nephrotoxicity. Drug Chem Toxicol. 2022 Nov;45(6):2637-2643. Epub 2021 Sep 27. [CrossRef]
- Cassis P, Locatelli M, Cerullo D, Corna D, Buelli S, Zanchi C, Villa S, Morigi M, Remuzzi G, Benigni A, Zoja C. SGLT2 inhibitor dapagliflozin limits podocyte damage in proteinuric nondiabetic nephropathy. JCI Insight. 2018 Aug 9;3(15):e98720. eCollection 2018 Aug 9. [CrossRef]
- Urbanek K, Cappetta D, Bellocchio G, Coppola MA, Imbrici P, Telesca M, Donniacuo M, Riemma MA, Mele E, Cianflone E, Naviglio S, Conte E, Camerino GM, Mele M, Bucci M, Castaldo G, De Luca A, Rossi F, Berrino L, Liantonio A, De Angelis A. Dapagliflozin protects the kidney in a non-diabetic model of cardiorenal syndrome. harmacol Res. 2023 Feb;188:106659. Epub 2023 Jan 14. [CrossRef]
- Chang WT, Wu CC, Liao IC, Lin YW, Chen YC, Ho CH, Lee WC, Lin YC, Chen ZC, Shih JY, Wu NC, Kan WC. Dapagliflozin protects against doxorubicin-induced nephrotoxicity associated with nitric oxide pathway-A translational study. Free Radic Biol Med. 2023 Aug 5;208:103-111. [CrossRef]
- Wei J, Tan F, Long X, Fang Q, Wang Y, Wang J, He J, Yuan X, Du J. RNA-Seq transcriptome analysis of renal tissue from spontaneously hypertensive rats revealed renal protective effects of dapagliflozin, an inhibitor of sodium-glucose cotransporter 2. Eur J Pharm Sci. 2023 Oct 1;189:106531. Epub 2023 Jul 20. [CrossRef]
- Xuan MY, Piao SG, Ding J, Nan QY, Piao MH, Jiang YJ, Zheng HL, Jin JZ, Li C. Dapagliflozin alleviates renal fibrosis by inhibiting RIP1-RIP3-MLKL-mediated necroinflammation in unilateral ureteral obstruction. Front Pharmacol. 2022 Jan 7;12:798381. eCollection 2021. [CrossRef]
- Zhang Y, Thai K, Kepecs DM, Gilbert RE (2016) Sodium-glucose linked cotransporter-2 inhibition does not attenuate disease progression in the rat remnant kidney model of chronic kidney disease. PLoS ONE 11(1): e0144640. [CrossRef]
- Rajasekeran, H.; Reich, H.N.; Hladunewich, M.A.; Cattran, D.; Lovshin, J.A.; Lytvyn, Y.; Bjornstad, P.; Lai,V.; Tse, J.; Cham, L.; et al. Dapagliflozin in focal segmental glomerulosclerosis: A combined human-rodent pilot study. Am. J. Physiol. Renal Physiol. 2018, 314, F412–F422.
- Mishima E, Fukuda S, Kanemitsu Y, Saigusa D, Mukawa C, Asaji K, Matsumoto Y, Tsukamoto H, Tachikawa T, Tsukimi T, Fukuda NN, Ho HJ, Kikuchi K, Suzuki C, Nanto F, Suzuki T, Ito S, Soga T, Tomioka Y, Abe T. Canagliflozin reduces plasma uremic toxins and alters the intestinal microbiota composition in a chronic kidney disease mouse model. Am J Physiol Renal Physiol. 2018 Oct 1;315(4):F824-F833. Epub 2017 Nov 22. [CrossRef]
- Corremans R, Neven E, Maudsley S, Leysen H, De Broe ME, D'Haese PC, Vervaet BA, Verhulst A. Progression of established non-diabetic chronic kidney disease is halted by metformin treatment in rats. Kidney Int. 2022 May;101(5):929-944. Epub 2022 Mar 7. [CrossRef]
- Hasan R, Lasker S, Hasan A, Zerin F, Zamila M, Parvez F, Rahman MM, Khan F, Subhan N, Alam MA. Canagliflozin ameliorates renal oxidative stress and inflammation by stimulating AMPK-Akt-eNOS pathway in the isoprenaline-induced oxidative stress model. Sci Rep. 2020 Sep 4;10(1):14659. [CrossRef]
- Wang Z, Zhai J, Zhang T, He L, Ma S, Zuo Q, Zhang G, Wang Y, Guo Y. Canagliflozin ameliorates epithelial-mesenchymal transition in high-salt diet-induced hypertensive renal injury through restoration of sirtuin 3 expression and the reduction of oxidative stress. Biochem Biophys Res Commun. 2023 Apr 23;653:53-61. Epub 2023 Feb. [CrossRef]
- Abdelrahman AM, Al Suleimani Y, Shalaby A, Ashique M, Manoj P, Nemmar A, Ali BH. Effect of canagliflozin, a sodium glucose co-transporter 2 inhibitor, on cisplatin-induced nephrotoxicity in mice. Naunyn Schmiedebergs Arch Pharmacol. 2019 Jan;392(1):45-53. Epub 2018 Sep 11. [CrossRef]
- Park CH, Lee B, Han M, Rhee WJ, Kwak MS, Yoo TH, Shin JS. Canagliflozin protects against cisplatin-induced acute kidney injury by AMPK-mediated autophagy in renal proximal tubular cells. Cell Death Discov. 2022 Jan 10;8(1):12. [CrossRef]
- Song Z, Zhu J, Wei Q, Dong G, Dong Z. Canagliflozin reduces cisplatin uptake and activates Akt to protect against cisplatin-induced nephrotoxicity. Am J Physiol Renal Physiol. 2020 Apr 1;318(4):F1041-F1052. Epub 2020 Mar 9. [CrossRef]
- Yang Y, Li Q, Ling Y, Leng L, Ma Y, Xue L, Lu G, Ding Y, Li J, Tao S. m6A eraser FTO modulates autophagy by targeting SQSTM1/P62 in the prevention of canagliflozin against renal fibrosis. Front Immunol. 2023 Jan 4;13:1094556. eCollection 2022. [CrossRef]
- Lv X, Wang J, Zhang L, Shao X, Lin Y, Liu H, Ma G, Li J, Zhou S, Yu P. Canagliflozin reverses Th1/Th2 imbalance and promotes podocyte autophagy in rats with membranous nephropathy. Front Immunol. 2022 Dec 1;13:993869. eCollection 2022. [CrossRef]
- Lu YP, Wu HW, Zhu T, Li XT, Zuo J, Hasan AA, Reichetzeder C, Delic D, Yard B, Klein T, Krämer BK, Zhang ZY, Wang XH, Yin LH, Dai Y, Zheng ZH, Hocher B. Empagliflozin reduces kidney fibrosis and improves kidney function by alternative macrophage activation in rats with 5/6-nephrectomy. Biomed Pharmacother. 2022 Dec;156:113947. Epub 2022 Oct 31. [CrossRef]
- Kim S, Jo CH, Kim GH. Effects of empagliflozin on nondiabetic salt-sensitive hypertension in uninephrectomized rats. Hypertens Res. 2019 Dec;42(12):1905-1915. Epub 2019 Sep 19. [CrossRef]
- Malínská H, Hüttl M, Marková I, Miklánková D, Hojná S, Papoušek F, Šilhavý J, Mlejnek P, Zicha J, Hrdlička J, Pravenec M, Vaněčková I. Beneficial effects of empagliflozin are mediated by reduced renal inflammation and oxidative stress in spontaneously hypertensive rats expressing human C-reactive protein. Biomedicines. 2022 Aug 24;10(9):2066. [CrossRef]
- Castoldi G, Carletti R, Ippolito S, Colzani M, Barzaghi F, Stella A, Zerbini G, Perseghin G, Zatti G, di Gioia CRT. Sodium-glucose cotransporter 2 inhibition prevents renal fibrosis in cyclosporine nephropathy. Acta Diabetol. 2021 Aug;58(8):1059-1070. Epub 2021 Mar 24. [CrossRef]
- Castoldi G, Carletti R, Ippolito S, Colzani M, Barzaghi F, Stella A, Zerbini G, Perseghin G, di Gioia CRT. Renal anti-fibrotic effect of sodium glucose cotransporter 2 inhibition in angiotensin II-dependent hypertension. Am J Nephrol. 2020;51(2):119-129. Epub 2020 Jan 7. [CrossRef]
- Reyes-Pardo H, Bautista R, Vargas-Robles H, Rios A, Sánchez D, Escalante B. Role of sodium/glucose cotransporter inhibition on a rat model of angiotensin II-dependent kidney damage. BMC Nephrol. 2019 Aug 2;20(1):292. [CrossRef]
- Kolkhof P, Hartmann E, Freyberger A, Pavkovic M, Mathar I, Sandner P, Droebner K, Joseph A, Hüser J, Eitner F. Effects of finerenone combined with empagliflozin in a model of hypertension-induced end-organ damage. Am J Nephrol. 2021;52(8):642-652. Epub 2021 Jun 10. [CrossRef]
- Chu C, Delić D, Alber J, Feger M, Xiong Y, Luo T, Hasan AA, Zeng S, Gaballa MMS, Chen X, Yin L, Klein T, Elitok S, Krämer BK, Föller M, Hocher B. Head-to-head comparison of two SGLT-2 inhibitors on AKI outcomes in a rat ischemia-reperfusion model. Biomed Pharmacother. 2022 Sep;153:113357. Epub 2022 Jul 2. [CrossRef]
- Ala M, Khoshdel MRF, Dehpour AR. Empagliflozin enhances autophagy, mitochondrial biogenesis, and antioxidant defense and ameliorates renal ischemia/ reperfusion in nondiabetic rats. Oxid Med Cell Longev. 2022 Jan 28;2022:1197061. eCollection 2022. [CrossRef]
- Wang Q, Ju F, Li J, Liu T, Zuo Y, Abbott GW, Hu Z. Empagliflozin protects against renal ischemia/reperfusion injury in mice. Sci Rep. 2022 Nov 11;12(1):19323. [CrossRef]
- Ge M, Molina J, Kim JJ, Mallela SK, Ahmad A, Varona Santos J, Al-Ali H, Mitrofanova A, Sharma K, Fontanesi F, Merscher S, Fornoni A. Empagliflozin reduces podocyte lipotoxicity in experimental Alport syndrome. Elife. 2023 May 2;12:e83353. [CrossRef]
- Lu CW, Lee CJ, Hsieh YJ, Hsu BG. Empagliflozin attenuates vascular calcification in mice with chronic kidney disease by regulating the NFR2/HO-1 anti-inflammatory pathway through AMPK activation. Int J Mol Sci. 2023 Jun 12;24(12):10016. [CrossRef]
- Ma Q, Steiger S, Anders H-J (2017) Sodium glucose transporter-2 inhibition has norenoprotective effects on non-diabetic chronic kidney disease. Physiol Rep 5 (7), 2017, e13228. [CrossRef]
- Hojná S, Kotsaridou Z, Vaňourková Z, Rauchová H, Behuliak M, Kujal P, Kadlecová M, Zicha J, Vaněčková I. Empagliflozin Is Not Renoprotective in Non-Diabetic Rat Models of Chronic Kidney Disease. Biomedicines. 2022 Oct 7;10(10):2509. [CrossRef]
- Yamato M, Kato N, Kakino A, Yamada KI, Inoguchi T. Low dose of sodium-glucose transporter 2 inhibitor ipragliflozin attenuated renal dysfunction and interstitial fibrosis in adenine-induced chronic kidney disease in mice without diabetes. Metabol Open. 2020 Aug 8;7:100049. eCollection 2020 Sep. [CrossRef]
- Hosokawa K, Takata T, Sugihara T, Matono T, Koda M, Kanda T, Taniguchi S, Ida A, Mae Y, Yamamoto M, Iyama T, Fukuda S, Isomoto H. Ipragliflozin ameliorates endoplasmic reticulum stress and apoptosis through preventing ectopic lipid deposition in renal tubules. Int J Mol Sci. 2019 Dec 26;21(1):190. [CrossRef]
- Ito H, Okamoto R, Ali Y, Zhe Y, Katayama K, Ito M, Dohi K. Cardiorenal protective effects of sodium-glucose cotransporter 2 inhibition in combination with angiotensin II type 1 receptor blockade in salt-sensitive Dahl rats. J Hypertens. 2022 May 1;40(5):956-968 Epub 2022 Mar 11. [CrossRef]
- Nuffield Department of Population Health Renal Studies Group; SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet. 2022 Nov 19;400(10365):1788-1801. Epub 2022 Nov 6. PMID: 36351458; PMCID: PMC7613836. [CrossRef]
- Heerspink HJL, Cherney D, Postmus D, Stefánsson BV, Chertow GM, Dwyer JP, Greene T, Kosiborod M, Langkilde AM, McMurray JJV, Correa-Rotter R, Rossing P, Sjöström CD, Toto RD, Wheeler DC; DAPA-CKD Trial Committees and Investigators. A pre-specified analysis of the Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) randomized controlled trial on the incidence of abrupt declines in kidney function. Kidney Int. 2022 Jan;101(1):174-184. Epub 2021 Sep 22. PMID: 34560136. [CrossRef]
- Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett J, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O'Meara E, Vinh PN, Schou M, Tereshchenko S, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Johanson P, Greasley PJ, Boulton D, Bengtsson O, Jhund PS, McMurray JJV. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA. 2020 Apr 14;323(14):1353-1368. Erratum in: JAMA. 2021 Apr 6;325(13):1335. PMID: 32219386; PMCID: PMC7157181. [CrossRef]
- Anker SD, Butler J, Filippatos G, Khan MS, Marx N, Lam CSP, Schnaidt S, Ofstad AP, Brueckmann M, Jamal W, Bocchi EA, Ponikowski P, Perrone SV, Januzzi JL, Verma S, Böhm M, Ferreira JP, Pocock SJ, Zannad F, Packer M. Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients With Heart Failure by Baseline Diabetes Status: Results From the EMPEROR-Reduced Trial. Circulation. 2021 Jan 26;143(4):337-349. Epub 2020 Nov 11. PMID: 33175585; PMCID: PMC7834911. [CrossRef]
- Packer M, Zannad F, Butler J, Filippatos G, Ferreira JP, Pocock SJ, Brueckmann M, Zeller C, Hauske S, Anker 69-SD; EMPEROR-Preserved Trial Study Group. Influence of endpoint definitions on the effect of empagliflozin on major renal outcomes in the EMPEROR-Preserved trial. Eur J Heart Fail. 2021 Oct;23(10):1798-1799. Epub 2021 Aug 30. PMID: 34459076; PMCID: PMC9291539. [CrossRef]
- Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, Shah SJ, Desai AS, Jhund PS, Belohlavek J, Chiang CE, Borleffs CJW, Comin-Colet J, Dobreanu D, Drozdz J, Fang JC, Alcocer-Gamba MA, Al Habeeb W, Han Y, Cabrera Honorio JW, Janssens SP, Katova T, Kitakaze M, Merkely B, O'Meara E, Saraiva JFK, Tereshchenko SN, Thierer J, Vaduganathan M, Vardeny O, Verma S, Pham VN, Wilderäng U, Zaozerska N, Bachus E, Lindholm D, Petersson M, Langkilde AM; DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022 Sep 22;387(12):1089-1098. Epub 2022 Aug 27. PMID: 36027570. [CrossRef]
- Rasaei N, Malekmakan L, Gholamabbas G, Mashayekh M, Hadianfard F, Torabi M. Sodium-Glucose Cotransporter-2 Inhibitors in Patients with Non-diabetic Chronic Kidney Disease: A Systematic Review. Iran J Kidney Dis. 2023 Jul;17(4):175-183. PMID: 37634243.
- Cherney DZI, Dekkers CCJ, Barbour SJ, Cattran D, Abdul Gafor AH, Greasley PJ, et al. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomised, double-blind, cross-over trial. The lancet Diabetes & endocrinology. 2020;8(7):582-93.
- Wheeler DC, Toto RD, Stefánsson BV, Jongs N, Chertow GM, Greene T, et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021;100(1):215-24.
- van der van der Beek AB, Koomen JV, Dekkers CCJ, Barbour SJ, Boulton DW, Gansevoort RT, et al. Evaluation of the Pharmacokinetics and Exposure-Response Relationship of Dapagliflozin in Patients without Diabetes and with Chronic Kidney Disease. Clin Pharmacokinet. 202.
- Zannad F, Ferreira JP, Pocock SJ, Zeller C, Anker SD, Butler J, et al. Cardiac and Kidney Benefits of Empagliflozin in Heart Failure Across the Spectrum of Kidney Function Insights From EMPEROR-Reduced. Circulation. 2021;143(4):310-21.
- Vart P, Vaduganathan M, Jongs N, Remuzzi G, Wheeler DC, Hou FF, McCausland F, Chertow GM, Heerspink HJL. Estimated Lifetime Benefit of Combined RAAS and SGLT2 Inhibitor Therapy in Patients with Albuminuric CKD without Diabetes. Clin J Am Soc Nephrol. 2022 Dec;17(12):1754-1762. Epub 2022 Nov 22. PMID: 36414316; PMCID: PMC9718016. [CrossRef]
- Podestà MA, Sabiu G, Galassi A, Ciceri P, Cozzolino M. SGLT2 Inhibitors in Diabetic and Non-Diabetic Chronic Kidney Disease. Biomedicines. 2023 Jan 19;11(2):279. PMID: 36830815; PMCID: PMC9953060. [CrossRef]
- Dong Y, Shi S, Liu L, Zhou X, Lv J, Zhang H. Effect of SGLT2 inhibitors on the proteinuria reduction in patients with IgA nephropathy. Front Med (Lausanne). 2023 Sep 6;10:1242241. PMID: 37736600; PMCID: PMC10509766. [CrossRef]
- Wheeler DC, Jongs N, Stefansson BV, Chertow GM, Greene T, Hou FF, Langkilde AM, McMurray JJV, Rossing P, Nowicki M, Wittmann I, Correa-Rotter R, Sjöström CD, Toto RD, Heerspink HJL; DAPA-CKD Trial Committees and Investigators. Safety and efficacy of dapagliflozin in patients with focal segmental glomerulosclerosis: a prespecified analysis of the dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial. Nephrol Dial Transplant. 2022 Aug 22;37(9):1647-1656. PMID: 34850160; PMCID: PMC9395378. [CrossRef]
- Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus: Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications. Circulation. 2016 Sep 6;134(10):752-72. Epub 2016 Jul 28. PMID: 27470878. [CrossRef]
- Mazidi M, Rezaie P, Gao HK, Kengne AP. Effect of sodium-glucose cotransport-2 inhibitors on blood pressure in people with type 2 diabetes mellitus: a systematic review and meta-analysis of 43 randomized control trials with 22,528 patients. J Am Heart Assoc. 2017; 6(6):e004007.
- Zanchi A, Pruijm M, Muller ME, Ghajarzadeh-Wurzner A, Maillard M, Dufour N, Bonny O, Wuerzner G, Burnier M. Twenty-Four Hour Blood Pressure Response to Empagliflozin and Its Determinants in Normotensive Non-diabetic Subjects. Front Cardiovasc Med. 2022 Mar 22;9:854230. PMID: 35391843; PMCID: PMC8981729. [CrossRef]
- Bays HE, Weinstein R, Law G, Canovatchel W. Canagliflozin: effects in overweight and obese subjects without diabetes mellitus. Obesity (Silver Spring). 2014 Apr;22(4):1042-9. Epub 2013 Dec 9. PMID: 24227660; PMCID: PMC4285787. [CrossRef]
- Díaz-Cruz C, González-Ortiz M, Rosales-Rivera LY, Patiño-Laguna AJ, Ramírez-Rodríguez ZG, Díaz-Cruz K, Martínez-Abundis E. Effects of dapagliflozin on blood pressure variability in patients with prediabetes and prehypertension without pharmacological treatment: a randomized trial. Blood Press Monit. 2020 Dec;25(6):346-350. PMID: 32815921. [CrossRef]
- Kalay Z, Sahin OE, Copur S, Danacı S, Ortiz A, Yau K, Cherney DZI, Kanbay M. SGLT-2 inhibitors in nephrotic-range proteinuria: emerging clinical evidence. Clin Kidney J. 2022 Aug 24;16(1):52-60. PMID: 36726436; PMCID: PMC9871839. [CrossRef]
- Boeckhaus J, Gross O. Sodium-Glucose Cotransporter-2 Inhibitors in Patients with Hereditary Podocytopathies, Alport Syndrome, and FSGS: A Case Series to Better Plan a Large-Scale Study. Cells. 2021 Jul 18;10(7):1815. PMID: 34359984; PMCID: PMC8303219. [CrossRef]
- Sjuls S, Jensen U, Littmann K, Bruchfeld A, Brinck J. Effective cholesterol lowering after myocardial infarction in patients with nephrotic syndrome may require a multi-pharmacological approach: a case report. Eur Heart J Case Rep. 2021 May 13;5(5):ytab151. PMID: 34124564; PMCID: PMC8189300. [CrossRef]
- A K Awad, M Tarek Hasan, M Shih, A N Attia, H Aboeldahab, M Bendary, A Bendary, Safety and efficacy of SGLT2 inhibitors in diabetic and non-diabetic heart failure patients, a meta-analysis of randomized controlled trials, European Heart Journal, Volume 43, Issue Supplement_2, October 2022, ehac544.941. [CrossRef]
- McEwan P, Boyce R, Sanchez JJG, Sjöström CD, Stefansson B, Nolan S, Correa-Rotter R, Rossing P, Chertow GM, McMurray JJV, Wheeler DC, Heerspink HJL. Extrapolated longer-term effects of the DAPA-CKD trial: a modelling analysis. Nephrol Dial Transplant. 2023 May 4;38(5):1260-1270. PMID: 36301617; PMCID: PMC10157747. [CrossRef]
- Halimi S, Verges B.: Adverse effects and safety of SGLT-2 inhibitors. Diabetes Metab 2014; 40: pp. S28-S34.
- Lega IC, Bronskill SE, Campitelli MA, Guan J, Stall NM, Lam K, McCarthy LM, Gruneir A, Rochon PA. Sodium glucose cotransporter 2 inhibitors and risk of genital mycotic and urinary tract infection: A population-based study of older women and men with diabetes. Diabetes Obes Metab. 2019 Nov;21(11):2394-2404. Epub 2019 Jul 21. PMID: 31264755. [CrossRef]
- Gupta R, Maitz T, Egeler D, Mehta A, Nyaeme M, Hajra A, Goel A, Sreenivasan J, Patel N, Aronow WS. SGLT2 inhibitors in hypertension: Role beyond diabetes and heart failure. Trends Cardiovasc Med. 2023 Nov;33(8):479-486. Epub 2022 May 18. PMID: 35597430. [CrossRef]
- Zhang Y, Jiang L, Wang J, Wang T, Chien C, Huang W, Fu X, Xiao Y, Fu Q, Wang S, Zhao J. Network meta-analysis on the effects of finerenone versus SGLT2 inhibitors and GLP-1 receptor agonists on cardiovascular and renal outcomes in patients with type 2 diabetes mellitus and chronic kidney disease. Cardiovasc Diabetol. 2022 Nov 5;21(1):232. PMID: 36335326; PMCID: PMC9637313. [CrossRef]
Figure 1.
Diabetics versus non-diabetics in metanalysis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



