Submitted:
12 July 2025
Posted:
16 July 2025
Read the latest preprint version here
Abstract
The purpose of the study is to analyse and to identify structural characteristics reffering to melanocytic nevi, in youth patients. Using both optical and electronic microscope, could be possible a better describtion related specificity in melanocytic nevi characteristic. Epiderm is composed by specific layers, functions and implications in the life Research studies described possibles malignant status in nevi, in time. Future trends, are important key points in management, including preventive and prophylactic methods.
Keywords:
normal epiderm
; nevi
; young people
; analysis
; diagnostic
Introduction
In order to define a disease, must have in attention a lot of differents factors such as historical points, or social and cultural.. Results of research studies, show us that some connective cells such as fibroblasts, lose their identity, in pathological conditions. [1] Another specific cells, namely melanocytes are known that having a specific structural point that is consider important in structural pathological description. [2] Refering to melanocytic nevi, in medical specific field of study and of research, various pigmented lesions of the epiderm, known as nevi, could be observe in different pars of the body. [3] For a proper diagnostic, an atypical nevus,can be biopsied.[4] In this direction, is important to practice a biopsy beside the extended clinical evaluation in melanocytic nevi A great point in this field of research, could be possible the genetic susceptibility for morphological and functional alterations, in nevi with that surrounding nevi changes. [5] A complete medical examination, play a great point for establishing the medical conduct, for a healthy status improving.[6,7] Structural analysis describe specific cells namely melanocytes as aggregated in ‘nests’, which conduct forming the nevus cells.[8] To the youth patients researchers found specific cells knowing as melanocytes. This specific cells could be found in areas of the epiderm of the parts of the body. [9,10] Theoretical and practical studies, show that melanocytic nevi developing in utero present genetical differences from those that appear later.[11,12] In the present field, we can mention about various informations from scientific literature, referring to specific nevi. [13] Also from literature and from practicum actually are known different scientific informatiuons about extending melanocytic nevi, having specific scientific names.[14] Because are many cases in all of the world, diagnosed as melanocitic nevi, we can mention that currently, the proper treatment of epidermal nevi is challenging. [15,16,17,18]Congenital melanocytic nevi it is known as a subject of research that offer controversy. [19] Clinical monitoring in congenital melanocytic nevi is important for diagnosis and for possible medical treatment strategies applications. [20] A complete examination of the human body, during a medical examination, is important. [21,22] Best to mention that the nowadays higher incidence in melanoma is in acompaniament of the nevi existence of the body and of the increase exposure to the ultraviolet light. [23,24] Practical biopsy is important for diagnosis.[25]One of an important point in the diagnosis of melanocytic nevi is to differentiate melanocitic nevi from a possible melanoma. [26,27] . An earlier diagnosis of the melanoma play a great role in idea that neoplasic lessions could be develop from pre-existing nevi in many cases. [28] Unfortunately, the epidermal melanoma is growing faster., depending of various conditions. [29,30]
Melanocytic Nevi Considerations
From many types of nevi, in the next short written text, we will describe a little bit on Ito’s nevus and Ota’s nevus. This two types of nevi, could be observe in pregnancy, at birdh and also to puberty. Them presence is in concordance with hormonal changes. Research studies described possibles malignant status in Ota’s nevus, rarely in Ito’s nevus. [31,32]This twoo previously mentioned types of nevi, namely Ito and Ota, do not differ from histologically point of view. Ito’s nevus and Ota’s nevus are distinguished by specific location on the body. So, tipically,Ito nevus occurs in the arm region and Ota nevus could be find on the face. [33,34]Ota’s nevus could also found in the supply areas of the first two branches of the trigeminal nerve. [34,35,36,37] Structurally, Ito’s nevus presents as a slate-blue/gray-blue macula in the shoulder/breast and lateral arm region in the supply area of the brachial nerve, in infants or prior puberty.[38] It is know that a specific sign of melanoma within the existing Ito’s nevus as a typical nodule. [39] In rarely malignancy cases in patients diagnosed with Ito’s nevi have been reported in adition, tipical nodules.[40,41]
From birth age, congenital melanocytic nevi (CMN) it is know as one of the frequent skin lesion. [42] From research results and conclusions, could be find rarely medical namely,neuroid differentiation. To a specific analyse, is possible to observe specific areas of cells with myxoid stroma in adition. Possible resemble later than, as neurofibromas.[42]
From a curently research pespective we can mention that in utero, specific stem cells from the neuroectoderm play a signifiant role such as migration to the skin as melanoblasts. Mechanism refers to a differentiate process into melanocytes. In addition, mutations arising in specific cells can occur to well known mosaicisms. Good to know that in the early embryogenesis, multipotent progenitor cells can be affected, leading to the presence of multiple congenital melanocytic nevi and also to extracutaneous alterations..[43,44]
In adition to previously above metioned idea, congenital melanocytic nevi occur as a result of in-utero somatic mutations. In this idea, genes play a great role. So there are know the mitogen-activated protein kinase (MAPK) pathway (mainly NRAS and BRAF). More than,their specific mutations refers to damages in the development of cutaneous and/or extracutaneous previously mentioned mosaicisms.[45] Aditionally to congenital melanocytic nevi, proliferative nodules (PN) constitute nodular lesions. [46] All described epidermal alterations, arel factors incriminate in differentiating proliferative nodule from melanoma.
Good to mention that neurocutaneous melanosis is a disease where congenital melanocytic nevi are associated with melanocyte proliferation. Beside, satellite lesions are especially at risk. Clinically are signs and specific symptoms So could be descibe neurological symptoms,with possible intracranial pressure.[47] From literature data there are know a lot of types of melanocytic nevi.[48] Then possible surgical intervention and pathologically diagnosis we can take into consideration. [49] Management directions play also a significant role as future directions.[50] From medical point of view we can mention that in case of an atypical nevus could be practice a proper biopsied. [51] Using this previously mentioned procedure is important to extend tissue excision in the un affected structure.[51] We can mention a lot about possible complications that include in pre-existing immune disorders, new exacerbations.[52]
Histologycally and Pathologycally Key Points of Epiderm
Normal epiderm is composed by specific layers, functions and implications in the human life. There are known a number of layers, namely basale stratum, spinosum stratum, granulosum stratum, lucidum stratum and corneuous stratum. In abnormally conditions, depending on divers factors, epidermal layers could possible to be affected structurally. Morphologically, specific cellularity, cell organelles, jonctions, and not only suffer dameges. Knowing this and reffering to epidermal nevi, previously mentioned possible damages play a role in pathologically status aparence, including nevi in youth patients. From another perspective, in a normal epiderm, there are known four cell populations. Namelly of specific cells are keratinocytes, melanocytes, Langerhans and Merkel cells. Refering to keratinocytes we can mention that comprise the bulk of the epiderm. [53,54] Melanocytes are interesting cells by them function. So this cells synthesize and store pigment namely melanin in specific organelles known as melanosomes. The role of melanocytes is the transfer of melanosomes via dendrites, primarily to keratinocytes.[55] Langerhans cells are antigen-presenting cells found in the epiderm. [56] Merkel cells are neuroendocrine origin. This cells are known by the implication as adapting mechanoreceptors.[57,58 , Figure 1]. [ Figure 2]. Also important to found and to know a little bit about cause of developing the nevi in young peoples. [59] Genetical causes is important in that cases..[60]
Material and Methods
For the purpose of the study we can mention about classic laboratory technique used and about the materials needed. In the specific laboratory, were followed the steps of the classic method, using Hematoxylin Eosin staining. The samples used were from male and female youth patients, before mature age, from urban and rural residence. This are examined using the optical microscope. In adition can be used also specialized microscopes and electron microscopes. The operative pieces are intended to bring in the pathological anatomy service for macroscopic examination for diagnosis.
Results
Epiderm protect us during the life, from different factors. For a morphological analyse, structural and ultrastructural characteristics could be describes, using optical and electron microscope. Structural analyse of the epiderm, using colour laboratory techniques, is able to describe the specific layers with their characteristics. More than, using electron microscope, specific compounds as filaggrin which is knowing as an important epidermal protein and/or tight junction located in the granular layer of the epiderm, could be observed. For this purpose, transmission electron microscope examination, is consider one proper method for analyse. Scanning electron microscopy is also a modern method for analyse, which offer results that demonstrate abnormalities in the epiderm ultrastructure. The human body is covers by skin and the epiderm contein differents types of glands, as sebaceous glands and sudoripar glands. In this study direction, it is known a typical physiopathlogic mechanism for the functionality of the body, including epidermal compounds and their body sorroundings. Histopathological analyse describe various modifications to the melanocytic nevi aspect, located on various regions of the body. So we can mention asymmetry, irregular form, cytologic atypia, and mitotic activity. Medical specialists, describe and conclude that to benign melanocytic nevi, could be possible a describtion for atypical pathological characteristics of nevi and more important to mention characteristics when benign nevi are traumatized. Epiderm is a barrier, but is able for conducing to an illness status if include modifications in structural compounds. Histopathological analyse describe the melanocytic nevi located on various regions of the body,with asymmetry, irregular form, cytologic atypia and mitotic activity. More than, medical specialists, describe and conclude related to the structural aspects in benign traumatized melanocytic nevi. In this field, dermoscopy play a role for a proper diagnostic. Dermoscopy play a role for a proper diagnostic important in practice to all ages, including, youth age and children. Immunohistochemistry (IHC) method has limitations from variability in sensitivity and specificity. (Table 1 and Table 2.)
Education Activity Outcomes and Management Strategies
Disease diagnostic and future trends, are important key points in management directions.As future directions good to mention idea including preventive and prophylactic methods. For each patient is important to improve a skin evaluation.In this context a simple clinical skin evaluation could be accompanied by biopsy, excision, surgical practice and other accopaniyng activities. (Table 3)
Discussions
Great interest in knowing epidermal compounds. So, the epiderm, is composed of a number of specific lyers. Specific cells are known. One of the role of the epiderm is implication in differents injuries. Alterations in the compunds of the epiderm layers, contribute to the visual signs of pathologic conditions. One research direction, refer to the role of benign melanocytic lesions with alterations, which conduct to malignant cutanat melanoma. Related to melanocytic nevi, in some circumstances, could be possible that the prognosis be poor having in attention the healthy of the patients having comorbidities. Pathological analyse and diagnosis reffering to melanocytic nevi located on differents regions from the body can find asymmetry, irregularity, cytologic atypia, and mitotic activity. Medical team including dermatologists, pathologists and dermatopathologists play a great role, in idea reffering to differentiate benign melanocytic nevi from malignant melanoma. This is important in order to avoid unnecessary surgical intervention or a treatment. Management and a better clinical evaluation, is a key point for a proper next time abordation in epidermal pathologically compounds as nevi. Structural analyze to the epidermal alterations is important for diagnosis. Next point is dermatological diagnosis. (Table 4)
Conclusions
Techniques for the laboratory diagnosis, as a key point in monitoring pathological status to patients diagnosed with melanocytic nevi, conduct to a proper quality of life. Implication of an interprofessional team is a condition that play a great medical role. Congenital melanocytic nevi are pigmented lesions that are usually present a birth. They are generally benign, but a small percentage (especially the larger ones) can potentially transform into malignant melanoma.Future trends, new laboratory methods and techniques for diagnosis. are in attention, for the next coming period of time.
References
- Salzer M.C., Lafzi A., Berenguer-Llergo A., Youssif C., Castellanos A., Solanas G., Peixoto F.O., Stephan-Otto Attolini C., Prats N., Aguilera M., Martín-Caballero J., Heyn H., Benitah S.A. Identity noise and adipogenic traits characterize dermal fibroblast aging. Cell. 2018;175:1575–1590.e22.
- Palicka GA, Rhodes AR. Acral melanocytic nevi: prevalence and distribution of gross morphologic features in white and black adults. Arch Dermatol. 2010 Oct;146(10):1085-94.
- Wang M, Xu Y, Wang J, Cui L, Wang J, Hu XB, Jiang HQ, Hong ZJ, Yuan SM. Surgical Management of Plantar Melanoma: A Retrospective Study in One Center. J Foot Ankle Surg. 2018 Jul-Aug;57(4):689-693.
- Richtig, E. ASCO Congress 2018: melanoma treatment. Memo. 2018;11(4):261-265.
- Wang B, Qu XL, Chen Y. Identification of the potential prognostic genes of human melanoma. J Cell Physiol. 2019 Jun;234(6):9810-9815.
- Bristow I, Bower C. Melanoma of the Foot. Clin Podiatr Med Surg. 2016 Jul;33(3):409-22.
- Lallas A, Kyrgidis A, Koga H, Moscarella E, Tschandl P, Apalla Z, Di Stefani A, Ioannides D, Kittler H, Kobayashi K, Lazaridou E, Longo C, Phan A, Saida T, Tanaka M, Thomas L, Zalaudek I, Argenziano G. The BRAAFF checklist: a new dermoscopic algorithm for diagnosing acral melanoma. Br J Dermatol. 2015 Oct;173(4):1041-9.
- Tronnier M. Melanotische Flecke und melanozytäre Nävi. In: Plewig G, Ruzicka T, Kaufmann R, Hertl M. Braun-Falcos Dermatol. Venerol. Allergol. Springer Berlin Heidelberg, 7. Auflage, 2016.
- Tolleson WH. Human Melanocyte Biology, Toxicology, and Pathology. J Environ Sci Health Part C 2005; 23: 105–61.
- Thomas AJ, Erickson CA. The making of a melanocyte: the specification of melanoblasts from the neural crest. Pigment Cell Melanoma Res 2008; 21: 598–610.
- Colebatch AJ, Ferguson P, Newell F et al. Molecular genomic profiling of melanocytic nevi. J Invest Dermatol 2019; 139: 1762–8.
- Kinsler VA, Thomas AC, Ishida M et al. Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. J Invest Dermatol 2013; 133: 2229–36.
- Bandyopadhyay D. Halo nevus. Indian Pediatr 2014; 51: 850.
- Fernandez-Flores A. Eponyms, Morphology, and Pathogenesis of some less mentioned types of melanocytic nevi. Am J Dermatopathol 2012; 34: 607–18.
- Kim JJ (Department of Dermatology, Henry Ford Health System, Detroit, MI 48202, USA), Chang MW, Shwayder T. Topical tre-tinoin and 5-fluorouracil in the treatment of linear verrucous epi dermal nevus. J Am Acad Dermatol. 2000 Jul;43(1 Pt 1):129–132.
- Brown HM, Gorlin RJ. Oral mucosal involvement in nevus unius lateris (Icthyosis Hysterix). Arch Dermatol. 1960 Apr;81:509–515.
- Zvulunov A (Soroka Medical Center, Ben-Gurion University, Beer-Sheva Israel), Grunwald MH, Halvy S. Topical calcipotriol for treatment of infammatory linear verrucous epidermal nevus. Arch Dermatol. 1997 May;133(5):567–568.
- Boyce S (Washington Institute of Dermatologic Laser Surgery, Washington, DC 20037, USA), Alster T. CO2 laser treatment of epidermal nevi: Long-term success. Dermatol Surg. 2002 Jul;28(7):611–614.
- Arad Ehud, Zuker M. Ronald, The shifting paradigm in the management of giant congenital melanocytic nevi: review and clinical applications, Plast Reconstr Surg., 2014 Feb;133(2):367-376.
- Mologousis MA, Tsai SY, Tissera KA, Levin YS, Hawryluk EB., Updates in the Management of Congenital Melanocytic Nevi., Children (Basel). 2024 Jan 2;11(1):62.
- Bristow I, Bower C. Melanoma of the Foot. Clin Podiatr Med Surg. 2016 Jul;33(3):409-22.
- Lallas A, Kyrgidis A, Koga H, Moscarella E, Tschandl P, Apalla Z, Di Stefani A, Ioannides D, Kittler H, Kobayashi K, Lazaridou E, Longo C, Phan A, Saida T, Tanaka M, Thomas L, Zalaudek I, Argenziano G. The BRAAFF checklist: a new dermoscopic algorithm for diagnosing acral melanoma. Br J Dermatol. 2015 Oct;173(4):1041-9.
- Bartoš V, Kullová M. Malignant Melanomas of the Skin Arising on the Feet. Klin Onkol. 2018 Summer;31(4):289-292.
- Palicka GA, Rhodes AR. Acral melanocytic nevi: prevalence and distribution of gross morphologic features in white and black adults. Arch Dermatol. 2010 Oct;146(10):1085-94.
- Bristow IR, de Berker DA, Acland KM, Turner RJ, Bowling J. Clinical guidelines for the recognition of melanoma of the foot and nail unit. J Foot Ankle Res. 2010 Nov 01;3:25.
- Gershenwald JE, Ross MI. Sentinel-lymph-node biopsy for cutaneous melanoma. N Engl J Med. (2011) 364:1738–45. 10.1056/NEJMct1002967.
- Eggermont AM, Spatz A, Robert C. Cutaneous melanoma. Lancet. (2014) 383:816–27.
- Elder DE. Precursors to melanoma and their mimics: nevi of special sites. Mod Pathol. (2006) 19(Suppl. 2):S4–20.
- Gershenwald JE, Ross MI. Sentinel-lymph-node biopsy for cutaneous melanoma. N Engl J Med. (2011) 364:1738–45.
- Eggermont AM, Spatz A, Robert C. Cutaneous melanoma. Lancet. (2014) 383:816–27.
- van Krieken JH, Boom BW, Scheffer E. Malignant transformation in a naevus of Ito. A case report. Histopathology 1988; 12: 100–2.
- Wise SR, Capra G, Martin P et al. Malignant melanoma transformation within a nevus of Ito. J Am Acad Dermatol 2010; 62: 869–74.
- Pérez ME, Bley C, Cárdenas C. Nevus of Ota, a classic presentation. Med Clin (Barc) 2019; 153: 92.
- Agarwal P, Patel BC. Nevus of Ota and Ito. StatPearls 2020.
- Kang HY, Kang WH. Bilateral type of nevus of Ota presenting as agminated lentigines. Eur J Dermatol EJD 2003; 13: 205–6.
- Turnbull JR, Assaf C, Zouboulis C, Tebbe B. Bilateral naevus of Ota: a rare manifestation in a Caucasian. J Eur Acad Dermatol Venereol JEADV 2004; 18: 353–5.
- Hori Y, Kawashima M, Oohara K, Kukita A. Acquired, bilateral nevus of Ota-like macules. J Am Acad Dermatol 1984; 10: 961–4.
- Que SKT, Weston G, Suchecki J, Ricketts J. Pigmentary disorders of the eyes and skin. Clin Dermatol 2015; 33: 147–58.
- Martínez-Peñuela A, Iglesias ME, Mercado MR et al. Malignant transformation of a nevus of Ito: description of a rare case. Actas Dermosifiliogr 2011; 102: 817–2.
- Wise SR, Capra G, Martin P et al. Malignant melanoma transformation within a nevus of Ito. J Am Acad Dermatol 2010; 62: 869–74.
- Martínez-Peñuela A, Iglesias ME, Mercado MR et al. Malignant transformation of a nevus of Ito: description of a rare case. Actas Dermosifiliogr 2011; 102: 817–20.
- Zayour M, Lazova R. Congenital melanocytic nevi. Clin Lab Med. 2011 Jun;31(2):267-80.
- Schaffer, JV. Update on melanocytic nevi in children. Clin Dermatol. 2015 May-Jun;33(3):368-86.
- Kinsler VA, O'Hare P, Bulstrode N, Calonje JE, Chong WK, Hargrave D, Jacques T, Lomas D, Sebire NJ, Slater O. Melanoma in congenital melanocytic naevi. Br J Dermatol. 2017 May;176(5):1131-1143.
- Price, HN. Congenital melanocytic nevi: update in genetics and management. Curr Opin Pediatr. 2016 Aug;28(4):476-82.
- Vergier B, Laharanne E, Prochazkova-Carlotti M, de la Fouchardière A, Merlio JP, Kadlub N, Avril MF, Bodemer C, Lacoste C, Boralevi F, Taieb A, Ezzedine K, Fraitag S. Proliferative Nodules vs Melanoma Arising in Giant Congenital Melanocytic Nevi During Childhood. JAMA Dermatol. 2016 Oct 01;152(10):1147-1151.
- Flores-Sarnat, L. Neurocutaneous melanocytosis. Handb Clin Neurol. 2013;111:369-88.
- Bandyopadhyay D. Halo nevus. Indian Pediatr 2014; 51: 850.
- Bristow IR, de Berker DA, Acland KM, Turner RJ, Bowling J. Clinical guidelines for the recognition of melanoma of the foot and nail unit. J Foot Ankle Res. 2010 Nov 01;3:25.
- Richtig, E. ASCO Congress 2018: melanoma treatment. Memo. 2018;11(4):261-265.
- Crompton JG, Gilbert E, Brady MS. Clinical implications of the eighth edition of the American Joint Committee on Cancer melanoma staging. J Surg Oncol. 2019 Jan;119(2):168-174.
- Richtig, E. ASCO Congress 2018: melanoma treatment. Memo. 2018;11(4):261-265.
- Bergstresser PR, Taylor JR. Epidermal 'turnover time'--a new examination. Br J Dermatol. 1977 May;96(5):503-9.
- Hoath SB, Leahy DG. The organization of human epidermis: functional epidermal units and phi proportionality. J Invest Dermatol. 2003 Dec;121(6):1440-6.
- Delevoye, C. Melanin transfer: the keratinocytes are more than gluttons. J Invest Dermatol. 2014 Apr;134(4):877-879.
- Pasparakis M, Haase I, Nestle FO. Mechanisms regulating skin immunity and inflammation. Nat Rev Immunol. 2014 May;14(5):289-301.
- Van Keymeulen A, Mascre G, Youseff KK, Harel I, Michaux C, De Geest N, Szpalski C, Achouri Y, Bloch W, Hassan BA, Blanpain C. Epidermal progenitors give rise to Merkel cells during embryonic development and adult homeostasis. J Cell Biol. 2009 Oct 05;187(1):91-100.
- Patel P, Hussain K. Merkel cell carcinoma. Clin Exp Dermatol. 2021 Jul;46(5):814-819.
- Colebatch AJ, Ferguson P, Newell F et al. Molecular genomic profiling of melanocytic nevi. J Invest Dermatol 2019; 139: 1762–8.
- Kinsler VA, Thomas AC, Ishida M et al. Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. J Invest Dermatol 2013; 133: 2229–36.
Figure 1.
Layers of the normal epiderm. https://en.wikipedia.org/wiki/Epidermis#/media/File:Normal_Epidermis_and_Dermis_with_Intradermal_Nevus_10x.JPG.
Figure 1.
Layers of the normal epiderm. https://en.wikipedia.org/wiki/Epidermis#/media/File:Normal_Epidermis_and_Dermis_with_Intradermal_Nevus_10x.JPG.
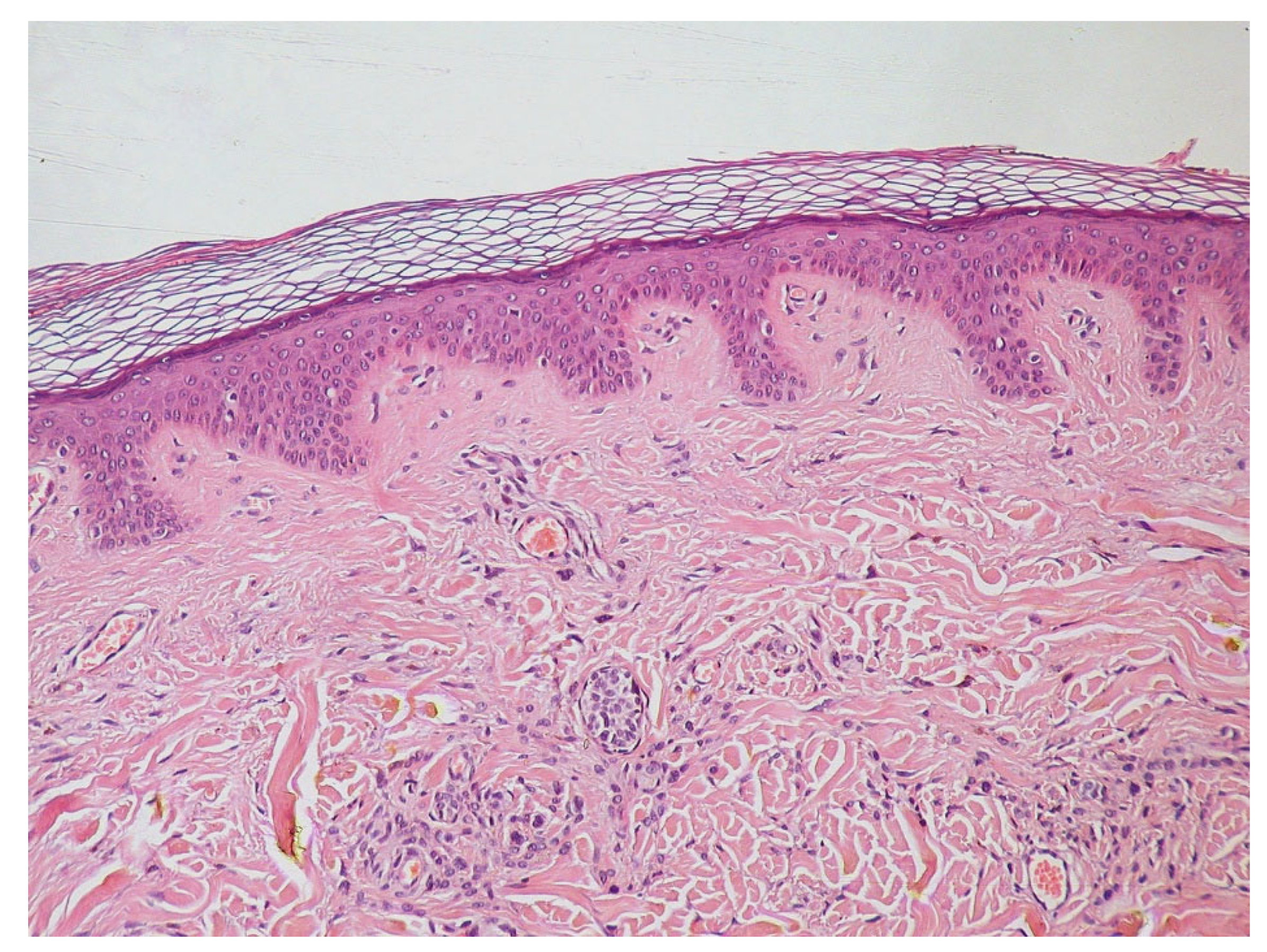
Figure 2.
Lentiginous melanocytic naevus. https://en.wikipedia.org/wiki/Melanocytic_nevus.
Figure 2.
Lentiginous melanocytic naevus. https://en.wikipedia.org/wiki/Melanocytic_nevus.
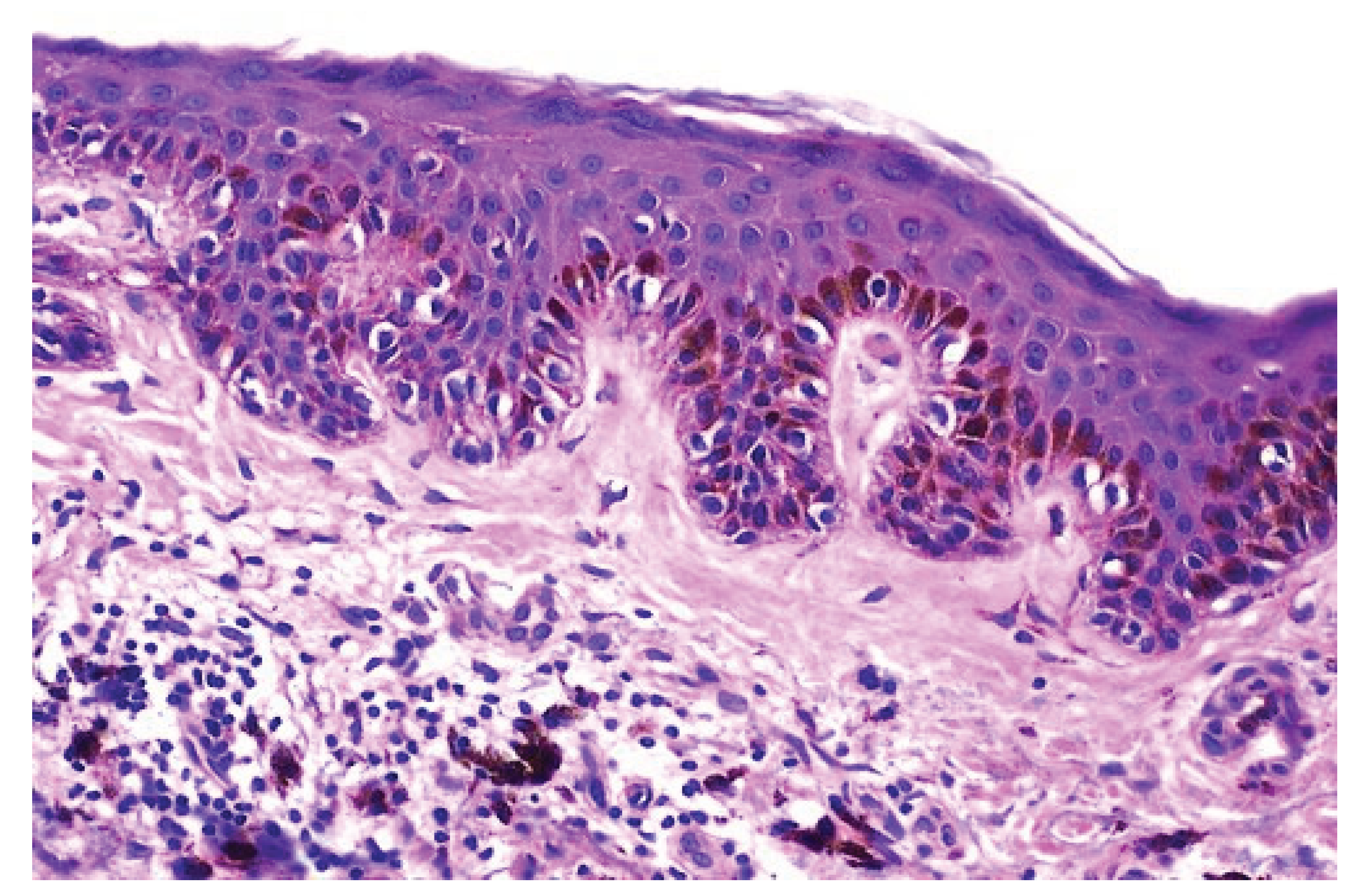

Table 1.
IHC method in diagnostic.
| Immunohistochemistry (IHC) | a process that involves using of selective antibodies to target and stain antigens |
|---|---|
| Immunohistochemistry (IHC) | known to be specific to a particular condition. |
| Immunohistochemistry (IHC) | a process that creates a color signal that can be visualized on light microscopy. |
Table 2.
Light microscopy implications in epidermal nevi.
| Light microscopy | The 100x magnification usually requires a medium between the lens and the slide, such as oil immersion |
| Light microscopy | Most microscopes used in dermatopathology are compound microscopes. |
| Light microscopy | Is the primary means for the magnified examination of tissue blocks. |
| Light microscopy | Generally shows cells as colorless, necessitating the need for various stains. Most tissue is initially stained with hematoxylin and eosin (H&E). |
Table 3.
Nevi characteristics for management directions.
| Review the management options available for melanocytic nevi. | Describe the presentation of a patient with melanocytic nevi. |
| Identify the risk factors for melanocytic nevi. | Outline interprofessional team strategies for improving care coordination and communication to advance the management of melanocytic nevi and improve outcomes. |
Table 4.
Nevi characteristics for differential diagnostic.
| Atypical mole | Basal cell carcinoma | Café au lait spots |
|---|---|---|
| Cutaneous melanoma |
Nevi of Ota and Ito | Nevus spilus |
| Cockade nevus | Nodular lesions | Pyogenic granuloma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



