
Submitted:
08 January 2024
Posted:
09 January 2024
You are already at the latest version
Abstract
It is unknown whether postprandial plasma glucose measured from blood taken between 4 and 7.9 h (PPG4-7.9h) is associated with mortality from hypertension, diabetes, or cardiovascular disease (CVD). This study aimed to investigate these associations in 4,896 US adults who attended the third National Health and Nutrition Examination Survey. Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of PPG4-7.9h for mortality. This cohort was followed up for 106,300 person-years (mean follow-up, 21.7 years). A 1-natural-log-unit increase in PPG4-7.9h was associated with a higher risk of mortality from hypertension (HR, 3.50; 95% CI, 2.34-5.24), diabetes (HR, 11.7; 95% CI, 6.85-20.0), and CVD (HR, 2.76; 95% CI, 2.08-3.68) after adjustment for all the tested confounders except hemoglobin A1c (HbA1c). After further adjustment for HbA1c, PPG4-7.9h remained positively associated with mortality from hypertension (HR, 2.15; 95% CI, 1.13-4.08) and CVD (HR, 1.62; 95% CI, 1.05-2.51), but was no longer associated with diabetes mortality. Subgroup analyses showed that similar results were obtained in the sub-cohort of participants without a prior diagnosis of myocardial infarction or stroke. In conclusion, PPG4-7.9h predicts mortality from hypertension and CVD independent of HbA1c.
Keywords:
non-fasting
; postprandial
; glucose
; diabetes
; cardiovascular disease
; blood pressure
1. Introduction
Cardiovascular disease (CVD) is the leading cause of death globally, responsible for 17.9 million deaths each year [1]. The global expenditure on CVD ranges between 7.6% and 21.0% of national health expenditures [2]. In the US, CVD costs approximately $320 billion per year [3]. Therefore, there is an urgent medical need to identify new risk factors and effective prevention strategies for CVD mortality.
Diabetes affects 8.5% of adults according to the World Health Organization [4]. It is well known that patients with diabetes have an increased risk of CVD mortality [5,6]. However, the underlying mechanism is not well understood. Postprandial plasma glucose (PPG) is believed to play an important role in diabetes-associated complications [7,8,9]. Therefore, it is of value to investigate the association of PPG with CVD mortality.
To the best of my knowledge, only one study investigated PPG and CVD mortality [10]. That study found that PPG measured from blood taken between 3 and 7.9 h (PPG3-7.9h) was positively associated with CVD mortality [10]. However, the PPG at 3-3.9 h did not return to the baseline level and PPG3-3.9h was higher than PPG4-7.9h [10]. A recent study showed that PPG returned to baseline four hours after a meal regardless of meal type (normal or high carbohydrate) and mealtime (breakfast, lunch and dinner) [11]. Therefore, the use of PPG3-7.9h is inferior to PPG4-7.9h and the association between PPG4-7.9h and CVD mortality needs to be investigated.
In addition, it has been shown that patients with diabetes have an increased risk of hypertension incidence [12]. However, whether PPG4-7.9h is associated with hypertension mortality is unknown, and so is whether PPG4-7.9h is associated with diabetes mortality.
This study aimed to investigate these unaddressed questions, i.e., whether PPG4-7.9h is associated with mortality from hypertension, diabetes, and CVD, using a representative cohort of US adults who attended the third National Health and Nutrition Examination Survey (NHANES III) from 1988 to 1994.
2. Materials and Methods
2.1. Participants
A total of 4,926 adults aged ≥ 20 years who attended the NHANES III had recorded postprandial plasma glucose data measured from blood taken between 4 and 7.9 h. Those who did not have a follow-up time (N=3) or hemoglobin A1c (HbA1c, N=27) were excluded. Therefore, the remaining 4,896 participants were included in this cohort study, including 343 participants with a prior diagnosis of myocardial infarction or stroke (Figure 1).
2.2. Measurement of Plasma Glucose
Plasma glucose was measured using the hexokinase-mediated reaction method as previously described [13].
2.3. Mortality
Data on mortality from CVD (I00-I09, I11, I13, I20-I51, I60-I69), diabetes (E10-E14), and hypertension were directly retrieved from NHANES-linked mortality files [14]. To evaluate mortality status and the cause of death, the National Center for Health Statistics conducted probabilistic matching [15] to link the NHANES data with death certificate records from the National Death Index (NDI) records. The NHANES-linked mortality files used the Underlying Cause of Death 113 (UCOD_113) code to recode all deaths according to the International Classification of Diseases, 9th Revision (ICD-9) or the International Classification of Diseases, 10th Revision (ICD–10) for the underlying cause of death [14]. Follow-up time was the duration from the time when the participant was examined at the Mobile Examination Center until death, or until the end of follow-up (December 31, 2019), whichever occurred first.
2.4. Covariates
Confounding factors included age (continuous), sex, ethnicity, body mass index (continuous), education, poverty-income ratio, survey periods, physical activity, alcohol consumption, smoking status, systolic blood pressure (continuous), total cholesterol (continuous), high-density lipoprotein (HDL) cholesterol (continuous), HbA1c (continuous), family history of diabetes, and fasting time (continuous), as described previously [14,16].
2.5. Statistical Analyses
Data were presented as mean and standard deviation for normally distributed continuous variables, median and interquartile range for not normally distributed continuous variables, or number and percentage for categorical variables to describe the baseline characteristics of the cohort [17]. Differences in continuous variables between two groups were analyzed using Student’s t-test (normally distributed), or Mann Whitney U test (not normally distributed). Differences among categorical variables were analyzed using Pearson's chi-square test [18]. The difference in hourly PPG4-7.9h was analyzed using Kruskal Wallis one-way ANOVA.
Out of 4,896 participants, a total of 115 (2.3%) had missing data including body mass index (N=14), systolic blood pressure (N=11), total cholesterol (N=53), or HDL cholesterol (N=93). The missing data were imputed via multiple imputation by chained equations, with 20 imputed data sets being created [19]. Little’s test showed that the missing data were not missing completely at random (P<0.001). In all the regression analyses, body mass index, systolic blood pressure, total cholesterol, HDL cholesterol, and HbA1c were natural log transformed to improve data distribution.
Cox proportional hazards models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) of PPG4-7.9h for mortality from hypertension, diabetes, and CVD [20]. PPG4-7.9h was treated as a continuous variable (natural log-transformed) or categorical variable. Further analyses were conducted in the sub-cohort of participants without a prior diagnosis of myocardial infarction or stroke.
Sensitivity analyses were conducted when the imputed data were not used, i.e., by excluding those 115 (2.3%) participants with missing data from the analysis, or when those with a follow-up time of <1 year (N=45) or those who were prescribed with insulin or other anti-diabetic medications (N=250) were excluded.
The null hypothesis was rejected for two-sided values of P<0.05. All analyses were performed using SPSS version 27.0 (IBM SPSS Statistics for Windows, Armonk, NY, IBM Corporation).
3. Results
3.1. General Characteristics
This cohort included 4,896 adult participants with a mean (standard deviation, SD) age of 49 (19) years. Those who had higher PPG4-7.9h were older and had higher body mass index, systolic blood pressure, and total cholesterol (Table 1). In addition, they were less physically active, had lower HDL cholesterol, and received less education and income (Table 1). Hourly PPG4-7.9h was similar (Figure 2).
3.2. Association of PPG4-7.9h with Mortality
This cohort was followed up for 106,300 person-years with a mean follow-up of 21.7 years. During the follow-up, 337 hypertension deaths, 70 diabetes deaths, and 835 CVD deaths were recorded.
A 1-natural-log-unit increase in PPG4-7.9h was associated with a higher multivariate-adjusted risk of mortality from hypertension (HR, 3.50; 95% CI, 2.34-5.24), diabetes (HR, 11.7; 95% CI, 6.85-20.0), and CVD (HR, 2.76; 95% CI, 2.08-3.68), after adjustment for all the tested confounders except HbA1c (Model 1; Figure 3). After further adjustment for HbA1c (Model 2, Figure 3), PPG4-7.9h remained positively associated with mortality from hypertension (HR, 2.15; 95% CI, 1.13-4.08) and CVD (HR, 1.62; 95% CI, 1.05-2.51). Similar results were obtained when PPG4-7.9h was treated as a dichotomous variable using the top decile as the cutoff (Figure 4). The use of the top decile as the cutoff is based on the estimate from the World Health Organization that 8.5% of adults have diabetes [4]. Subgroup analyses showed that similar results were obtained in those participants without a prior diagnosis of myocardial infarction or stroke (Figure 5).
Sensitivity analyses showed that PPG4-7.9h remained positively associated with mortality from hypertension and CVD when imputed data were not used, i.e., by excluding those 115 participants with missing data (Figure 6), or when those with a follow-up time of <1 year were excluded (Figure 7), or when those who were prescribed with anti-diabetic medications were excluded (Figure 8).
4. Discussion
Using a general cohort of US adults, this study, for the first time, demonstrated that PPG4-7.9h was positively associated with mortality from hypertension and CVD, independent of HbA1c. In addition, these positive associations remained in the sub-cohort of participants who did not have a prior diagnosis of myocardial infarction or stroke.
This study found that PPG4-7.9h was positively associated with hypertension mortality. However, the underlying mechanism is unknown. It is well known that diabetes and hypertension often co-exist in many individuals [21], and these two conditions share some risk factors such as obesity [22,23] and physical inactivity [24,25]. It has been shown that baseline fasting plasma glucose [26], fasting plasma glucose change trajectory [27], and diabetes [12] are positively associated with risks of hypertension incidence [12], suggesting that high blood glucose may disturb blood pressure homeostasis. Consistently, the current study showed that PPG4-7.9h was positively associated with hypertension mortality, independent of well-known confounders including body mass index, physical activity, total cholesterol, and HDL cholesterol, supporting a causal role of high plasma glucose in worsening hypertension outcomes. It has been reported that high plasma glucose may lead to oxidative stress and endothelial dysfunction [28,29]. Whether increased oxidative stress and endothelial dysfunction play a role in mediating the positive association between PPG4-7.9h and hypertension mortality needs to the investigated in the future. So does whether lowering PPG4-7.9h is effective in improving blood pressure control and hypertension mortality.
The association of diabetes with CVD incidence and mortality are well documented. Diabetes is an independent risk factor for CVD [30]. In addition, sodium–glucose cotransporter 2 (SGLT2) inhibitors, a class of anti-diabetic medication, decrease CVD events and mortality [31,32,33]. The mechanism underlying the association of diabetes with CVD events and mortality is not well understood.
A few studies have investigated the association of PPG with cardiovascular events. PPG at 1 or 2 h after breakfast [34,35] or 2 h after lunch [36,37] were reported to be positively associated with CVD events. However, those studies did not investigate CVD mortality. In addition, measuring glucose at 1 or 2 h after a meal may not be ideal, as variation in diet could change PPG by more than 20 mg/dL [11] and variation in blood collection time (± 0.5 h in practice [38]) could introduce bias as PPG is time-sensitive around 1 to 2 h [11].
Only one study investigated PPG and CVD mortality, which found that PPG measured from blood taken between 3 and 7.9 h was positively associated with CVD mortality [10]. However, the use of PPG3-7.9h is inferior to PPG4-7.9h, as PPG at 3-3.9 h did not return to the baseline level and PPG3-3.9h was higher than PPG4-7.9h [10]. In addition, PPG returned to baseline four hours after a meal regardless of meal type and mealtime [11]. Moreover, the current study confirmed that hourly PPG4-7.9h was similar across the duration from 4 to 7.9 h. Therefore, it is necessary to investigate the association between PPG4-7.9h and CVD mortality.
Some studies have investigated the association between fasting plasma glucose and CVD mortality and the results are inconsistent: some show a positive association [39,40] whereas others show no association [41,42]. The reason for this inconsistency is unknown. This may be due to poor reproducibility of fasting plasma glucose [43]. For instance, only 75% of adults were classified into the same diabetes category (normal, prediabetes, or diabetes) based on two consecutive measures of fasting plasma glucose which were conducted 6 weeks apart [43].
The current study showed that PPG4-7.9h was positively and independently associated with CVD mortality, and such a positive association remained in those without a prior diagnosis of myocardial infarction or stroke. Given its stability and reproducibility, PPG4-7.9h may be a better predictor of CVD mortality than fasting plasma glucose and PPG3-7.9h. Whether lowering PPG4-7.9h is a primary prevention strategy to decrease CVD mortality needs to be investigated in the future.
This study found that PPG4-7.9h was positively associated with diabetes mortality and such an association disappeared after future adjustment for HbA1c, suggesting that HbA1c could explain the association between PPG4-7.9h and diabetes mortality.
Some guidelines have started to recommend non-fasting lipids (triglycerides and various forms of cholesterol) as the standard for cardiovascular risk assessment [44,45]. Consistently, the current study suggests that non-fasting plasma glucose (PPG4-7.9h) may be used for cardiovascular risk assessment. The non-fasting plasma glucose test is more convenient than a fasting glucose test. More research is needed to establish whether non-fasting plasma glucose could be eventually used in the clinic for CVD risk assessment. For example, studies replicating the results of the current study using different populations from different countries are needed.
Strengths and limitations One strength of this study is its analysis of PPG after meals of free choice in a large representative cohort of US adults. Another strength is its prospective study design with a long follow-up (mean, 21.7 years). A third strength is its adjustment for a large number of confounders. This study also has several limitations. First, mortality outcomes were ascertained by linkage to the National Death Index (NDI) records with a probabilistic match, which could result in misclassification [46]. However, this matching method has been shown to be highly accurate (accuracy, 98.5%) [47]. Second, PG was only measured at one timepoint for each participant, which may lead to bias. Nevertheless, in epidemiological analysis, this bias tends to result in an underestimate rather than an overestimate of risk due to regression dilution [48].
5. Conclusions
This study found that PPG4-7.9h is positively associated with mortality from hypertension and CVD and such positive associations remain in those without a prior diagnosis of myocardial infarction or stroke. Therefore, lowering PPG4-7.9h may be a primary prevention strategy to decrease CVD mortality.
Author Contributions
Y.W. solely contributed to all aspects of this study.
Funding
Y.W. was supported by a grant from the National Health and Medical Research Council of Australia (1062671).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the NHANES Institutional Review Board.
Informed Consent Statement
All participants provided written informed consent. The participants’ records were anonymized before being accessed by the author.
Data Availability Statement
All data in the current analysis are publicly available on the NHANES website (https://www.cdc.gov/nchs/nhanes/index.htm).
Acknowledgments
None.
Conflicts of Interest
The author declares no conflicts of interest.
References
- World Health Organization. Cardiovascular diseases. Available from https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1. Accessed on 4 January 2024 2023.
- Santos, J.V.; Vandenberghe, D.; Lobo, M.; Freitas, A. Cost of cardiovascular disease prevention: Towards economic evaluations in prevention programs. Annals of Translational Medicine 2020, 8, 512. [Google Scholar] [CrossRef]
- Birger, M.; Kaldjian, A.S.; Roth, G.A.; Moran, A.E.; Dieleman, J.L.; Bellows, B.K. Spending on Cardiovascular Disease and Cardiovascular Risk Factors in the United States: 1996 to 2016. Circulation 2021, 144, 271–282. [Google Scholar] [CrossRef]
- World Health Organization. Key facts-Diabetes. Available at https://www.who.int/news-room/fact-sheets/detail/diabetes. Accessed on 18 October 2023.
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J. Diabetes 2015, 6, 1246–1258. [Google Scholar] [CrossRef]
- Wong, N.D.; Sattar, N. Cardiovascular risk in diabetes mellitus: Epidemiology, assessment and prevention. Nature Reviews Cardiology 2023, 20, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Colagiuri, S.; Gerich, J.; Tuomilehto, J. Guideline for management of postmeal glucose. Nutr. Metab. Cardiovasc. Dis. 2008, 18, S17–S33. [Google Scholar] [CrossRef] [PubMed]
- Peter, R.; Okoseime, O.E.; Rees, A.; Owens, D.R. Postprandial glucose - a potential therapeutic target to reduce cardiovascular mortality. Curr. Vasc. Pharmacol. 2009, 7, 68–74. [Google Scholar] [CrossRef]
- American Diabetes Association. Postprandial Blood Glucose. Diabetes Care 2001, 24, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fang, Y. Late non-fasting plasma glucose predicts cardiovascular mortality independent of hemoglobin A1c. Sci. Rep. 2022, 12, 7778. [Google Scholar] [CrossRef]
- Eichenlaub, M.M.; Khovanova, N.A.; Gannon, M.C.; Nuttall, F.Q.; Hattersley, J.G. A Glucose-Only Model to Extract Physiological Information from Postprandial Glucose Profiles in Subjects with Normal Glucose Tolerance. J. Diabetes Sci. Technol. 2022, 16, 1532–1540. [Google Scholar] [CrossRef]
- Tsimihodimos, V.; Gonzalez-Villalpando, C.; Meigs, J.B.; Ferrannini, E. Hypertension and Diabetes Mellitus. Hypertension 2018, 71, 422–428. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y. Postabsorptive homeostasis model assessment for insulin resistance is a reliable biomarker for cardiovascular disease mortality and all-cause mortality. Diabetes Epidemiology and Management 2021, 6, 100045. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y.; Magliano, D.J.; Charchar, F.J.; Sobey, C.G.; Drummond, G.R.; Golledge, J. Fasting triglycerides are positively associated with cardiovascular mortality risk in people with diabetes. Cardiovasc. Res. 2023, 119, 826–834. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y.; Witting, P.K.; Charchar, F.J.; Sobey, C.G.; Drummond, G.R.; Golledge, J. Dietary fatty acids and mortality risk from heart disease in US adults: An analysis based on NHANES. Sci. Rep. 2023, 13, 1614. [Google Scholar] [CrossRef]
- Wang, Y. Definition, prevalence, and risk factors of low sex hormone-binding globulin in US adults. J Clin Endocrinol Metab 2021, 106, e3946–e3956. [Google Scholar] [CrossRef]
- Jungo, K.T.; Meier, R.; Valeri, F.; Schwab, N.; Schneider, C.; Reeve, E.; Spruit, M.; Schwenkglenks, M.; Rodondi, N.; Streit, S. Baseline characteristics and comparability of older multimorbid patients with polypharmacy and general practitioners participating in a randomized controlled primary care trial. BMC Fam. Pract. 2021, 22, 123. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Stage 1 hypertension and risk of cardiovascular disease mortality in United States adults with or without diabetes. J. Hypertens. 2022, 40, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Kubo, Y.; Noguchi, T.; Hayashi, T.; Tomiyama, N.; Ochi, A.; Hayashi, H. Eating alone and weight change in community-dwelling older adults during the coronavirus pandemic: A longitudinal study. Nutrition 2022, 102, 111697. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E. Cox Proportional Hazards Regression Model. In Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis, Harrell, F.E., Ed. Springer New York: New York, NY, 2001; pp. 465-507. [CrossRef]
- Long, A.N.; Dagogo-Jack, S. Comorbidities of diabetes and hypertension: Mechanisms and approach to target organ protection. J. Clin. Hypertens. (Greenwich) 2011, 13, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Shariq, O.A.; McKenzie, T.J. Obesity-related hypertension: A review of pathophysiology, management, and the role of metabolic surgery. Gland Surg 2020, 9, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Gastaldelli, A.; Yki-Järvinen, H.; Scherer, P.E. Why does obesity cause diabetes? Cell Metab. 2022, 34, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Enyew, A.; Nigussie, K.; Mihrete, T.; Jemal, M.; kedir, S.; Alemu, E.; Mohammed, B. Prevalence and associated factors of physical inactivity among adult diabetes mellitus patients in Felege Hiwot Referral Hospital, Bahir Dar, Northwest Ethiopia. Sci. Rep. 2023, 13, 118. [Google Scholar] [CrossRef]
- Gamage, A.U.; Seneviratne, R.A. Physical inactivity, and its association with hypertension among employees in the district of Colombo. BMC Public Health 2021, 21, 2186. [Google Scholar] [CrossRef]
- Luo, B.; Feng, L.; Bi, Q.; Shi, R.; Cao, H.; Zhang, Y. Fasting Plasma Glucose and Glycated Hemoglobin Levels as Risk Factors for the Development of Hypertension: A Retrospective Cohort Study. Diabetes Metab. Syndr. Obes. 2023, 16, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Zhang, Y.; Zhao, P.; Qin, P.; Wang, C.; Ma, J.; Peng, X.; Chen, H.; Zhao, D.; Xu, S.; et al. Association of fasting plasma glucose change trajectory and risk of hypertension: A cohort study in China. Endocr Connect 2022, 11, e210464. [Google Scholar] [CrossRef] [PubMed]
- Škrha, J.; Šoupal, J.; Škrha, J.; Prázný, M. Glucose variability, HbA1c and microvascular complications. Reviews in Endocrine and Metabolic Disorders 2016, 17, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Wright, E., Jr.; Scism-Bacon, J.L.; Glass, L.C. Oxidative stress in type 2 diabetes: The role of fasting and postprandial glycaemia. Int. J. Clin. Pract. 2006, 60, 308–314. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47, S179–s218. [Google Scholar] [CrossRef]
- Arnott, C.; Li, Q.; Kang, A.; Neuen, B.L.; Bompoint, S.; Lam, C.S.P.; Rodgers, A.; Mahaffey, K.W.; Cannon, C.P.; Perkovic, V.; et al. Sodium-Glucose Cotransporter 2 Inhibition for the Prevention of Cardiovascular Events in Patients With Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. J. Am. Heart. Assoc. 2020, 9, e014908. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Fitchett, D.; Butler, J.; van de Borne, P.; Zinman, B.; Lachin, J.M.; Wanner, C.; Woerle, H.J.; Hantel, S.; George, J.T.; Johansen, O.E.; et al. Effects of empagliflozin on risk for cardiovascular death and heart failure hospitalization across the spectrum of heart failure risk in the EMPA-REG OUTCOME® trial. Eur. Heart J. 2018, 39, 363–370. [Google Scholar] [CrossRef]
- Hanefeld, M.; Fischer, S.; Julius, U.; Schulze, J.; Schwanebeck, U.; Schmechel, H.; Ziegelasch, H.J.; Lindner, J. Risk factors for myocardial infarction and death in newly detected NIDDM: The Diabetes Intervention Study, 11-year follow-up. Diabetologia 1996, 39, 1577–1583. [Google Scholar] [CrossRef]
- Takao, T.; Suka, M.; Yanagisawa, H.; Iwamoto, Y. Impact of postprandial hyperglycemia at clinic visits on the incidence of cardiovascular events and all-cause mortality in patients with type 2 diabetes. J Diabetes Investig 2017, 8, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Cavalot, F.; Pagliarino, A.; Valle, M.; Di Martino, L.; Bonomo, K.; Massucco, P.; Anfossi, G.; Trovati, M. Postprandial blood glucose predicts cardiovascular events and all-cause mortality in type 2 diabetes in a 14-year follow-up: Lessons from the San Luigi Gonzaga Diabetes Study. Diabetes Care 2011, 34, 2237–2243. [Google Scholar] [CrossRef]
- Cavalot, F.; Petrelli, A.; Traversa, M.; Bonomo, K.; Fiora, E.; Conti, M.; Anfossi, G.; Costa, G.; Trovati, M. Postprandial blood glucose is a stronger predictor of cardiovascular events than fasting blood glucose in type 2 diabetes mellitus, particularly in women: Lessons from the San Luigi Gonzaga Diabetes Study. J Clin Endocrinol Metab 2006, 91, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Takao, T.; Takahashi, K.; Suka, M.; Suzuki, N.; Yanagisawa, H. Association between postprandial hyperglycemia at clinic visits and all-cause and cancer mortality in patients with type 2 diabetes: A long-term historical cohort study in Japan. Diabetes Res. Clin. Pract. 2019, 148, 152–159. [Google Scholar] [CrossRef]
- Qiao, Q.; Pyörälä, K.; Pyörälä, M.; Nissinen, A.; Lindström, J.; Tilvis, R.; Tuomilehto, J. Two-hour glucose is a better risk predictor for incident coronary heart disease and cardiovascular mortality than fasting glucose. Eur. Heart J. 2002, 23, 1267–1275. [Google Scholar] [CrossRef]
- Barr, E.L.; Zimmet, P.Z.; Welborn, T.A.; Jolley, D.; Magliano, D.J.; Dunstan, D.W.; Cameron, A.J.; Dwyer, T.; Taylor, H.R.; Tonkin, A.M.; et al. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: The Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation 2007, 116, 151–157. [Google Scholar] [CrossRef]
- Cohen, B.E.; Barrett-Connor, E.; Wassel, C.L.; Kanaya, A.M. Association of glucose measures with total and coronary heart disease mortality: Does the effect change with time? The Rancho Bernardo Study. Diabetes Res. Clin. Pract. 2009, 86, 67–73. [Google Scholar] [CrossRef]
- Nielsen, M.L.; Pareek, M.; Leósdóttir, M.; Eriksson, K.F.; Nilsson, P.M.; Olsen, M.H. One-hour glucose value as a long-term predictor of cardiovascular morbidity and mortality: The Malmö Preventive Project. Eur J Endocrinol 2018, 178, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Tjaden, A.H.; Edelstein, S.L.; Arslanian, S.; Barengolts, E.; Caprio, S.; Cree-Green, M.; Lteif, A.; Mather, K.J.; Savoye, M.; Xiang, A.H.; et al. Reproducibility of Glycemic Measures Among Dysglycemic Youth and Adults in the RISE Study. J Clin Endocrinol Metab 2023, 108, e1125–e1133. [Google Scholar] [CrossRef] [PubMed]
- Darras, P.; Mattman, A.; Francis, G.A. Nonfasting lipid testing: The new standard for cardiovascular risk assessment. CMAJ 2018, 190, E1317–E1318. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; Ferranti, S.d.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Higher fasting triglyceride predicts higher risks of diabetes mortality in US adults. Lipids Health Dis. 2021, 20, 181. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Muntner, P.; Batuman, V.; Silbergeld, E.K.; Guallar, E. Blood lead below 0.48 micromol/L (10 microg/dL) and mortality among US adults. Circulation 2006, 114, 1388–1394. [Google Scholar] [CrossRef]
- MacMahon, S.; Peto, R.; Cutler, J.; Collins, R.; Sorlie, P.; Neaton, J.; Abbott, R.; Godwin, J.; Dyer, A.; Stamler, J. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet 1990, 335, 765–774. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of the study participants. HbA1c, hemoglobin A1c; MI, myocardial infarction; NHANES III, the third National Health and Nutrition Examination Survey; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 1.
Flow diagram of the study participants. HbA1c, hemoglobin A1c; MI, myocardial infarction; NHANES III, the third National Health and Nutrition Examination Survey; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
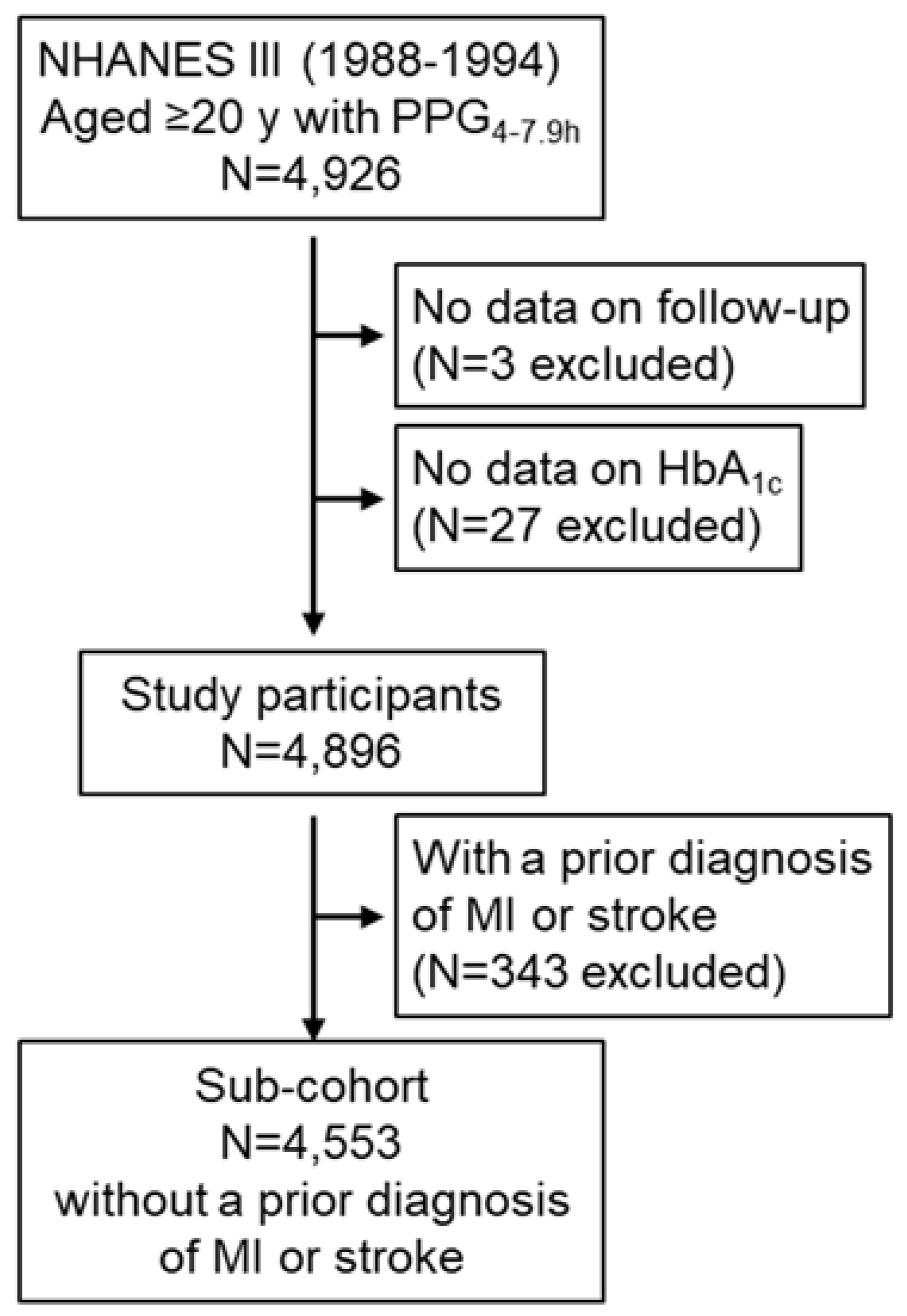
Figure 2.
Hourly PPG4-7.9h. PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 2.
Hourly PPG4-7.9h. PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
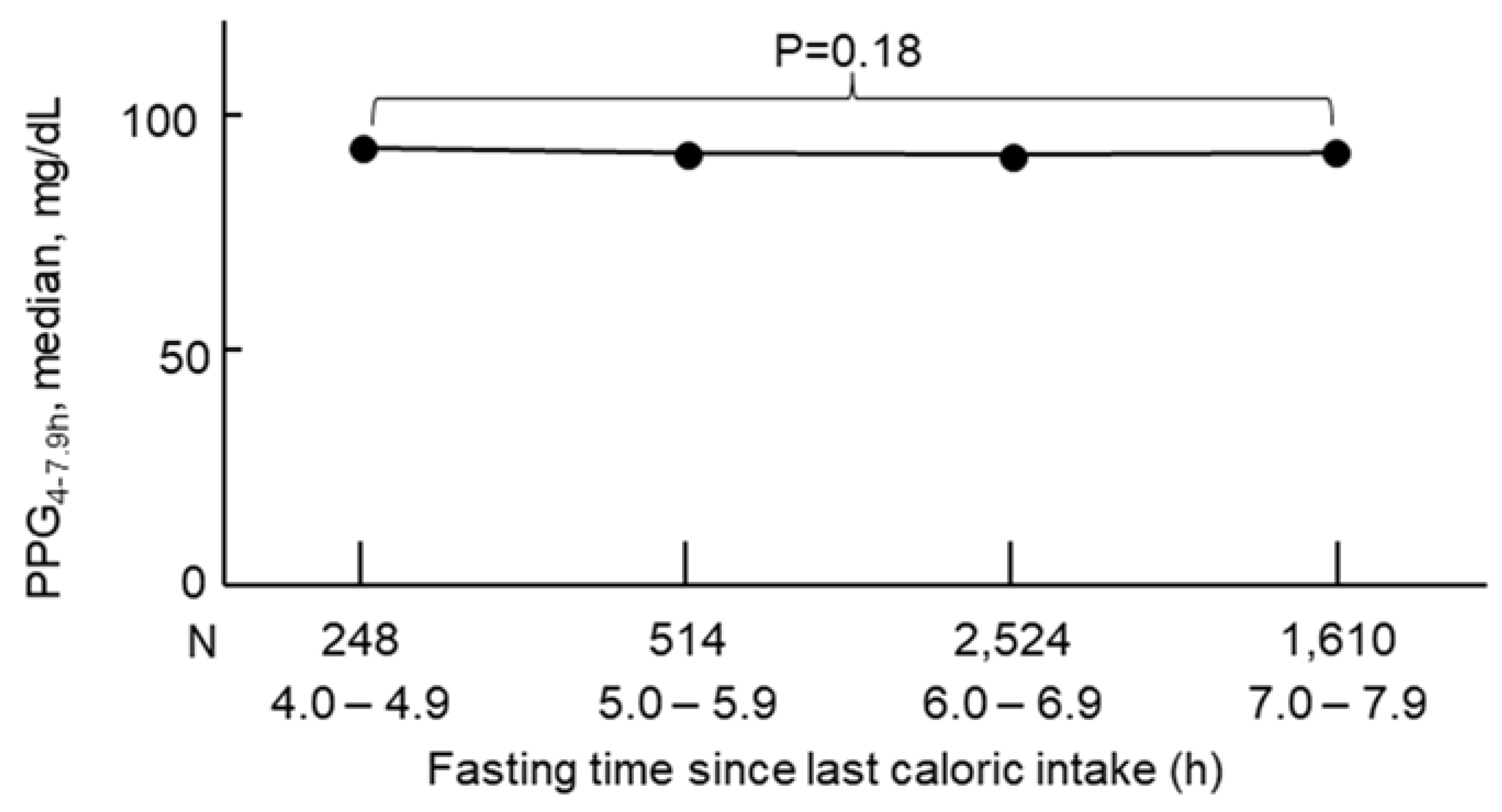
Figure 3.
Mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,896 participants. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 3.
Mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,896 participants. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
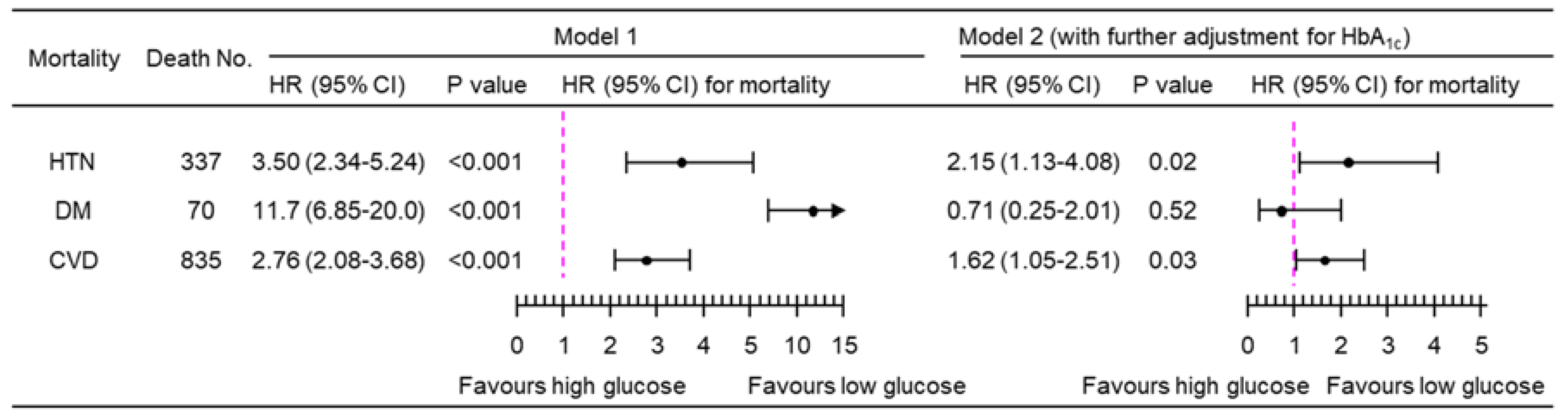
Figure 4.
Mortality risk associated with categorical PPG4-7.9h (top decile versus bottom nine deciles) in 4,896 participants. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 4.
Mortality risk associated with categorical PPG4-7.9h (top decile versus bottom nine deciles) in 4,896 participants. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
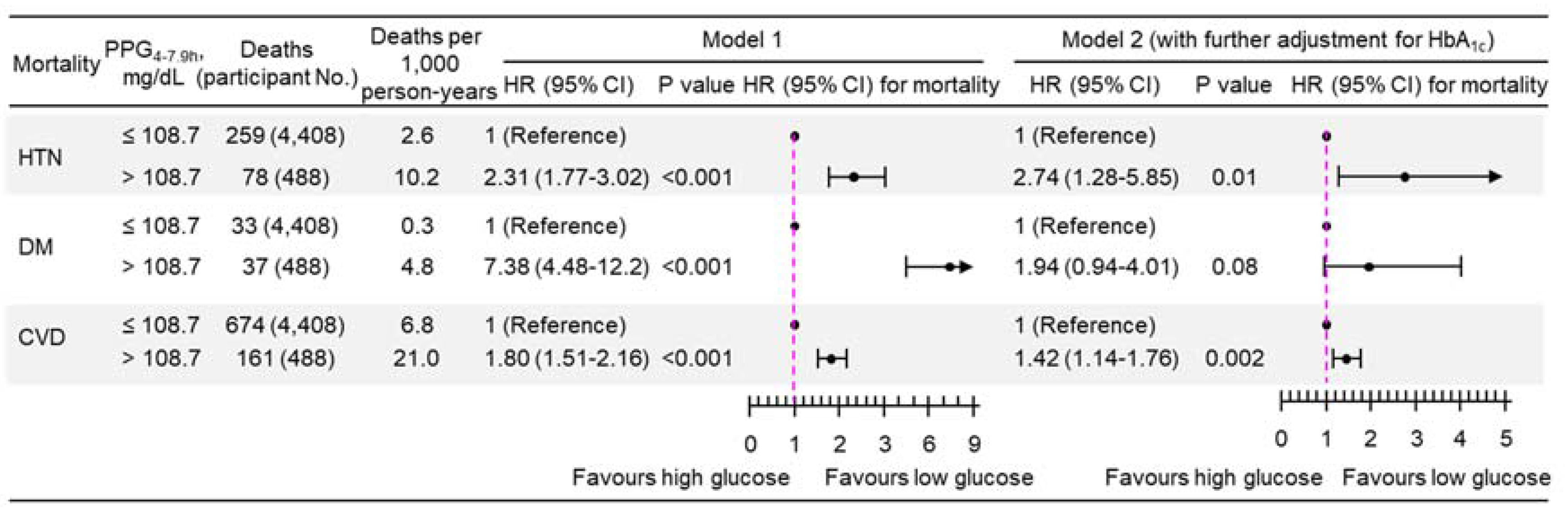
Figure 5.
Mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in the sub-cohort of 4,553 participants without a prior diagnosis of myocardial infarction or stroke. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 5.
Mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in the sub-cohort of 4,553 participants without a prior diagnosis of myocardial infarction or stroke. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
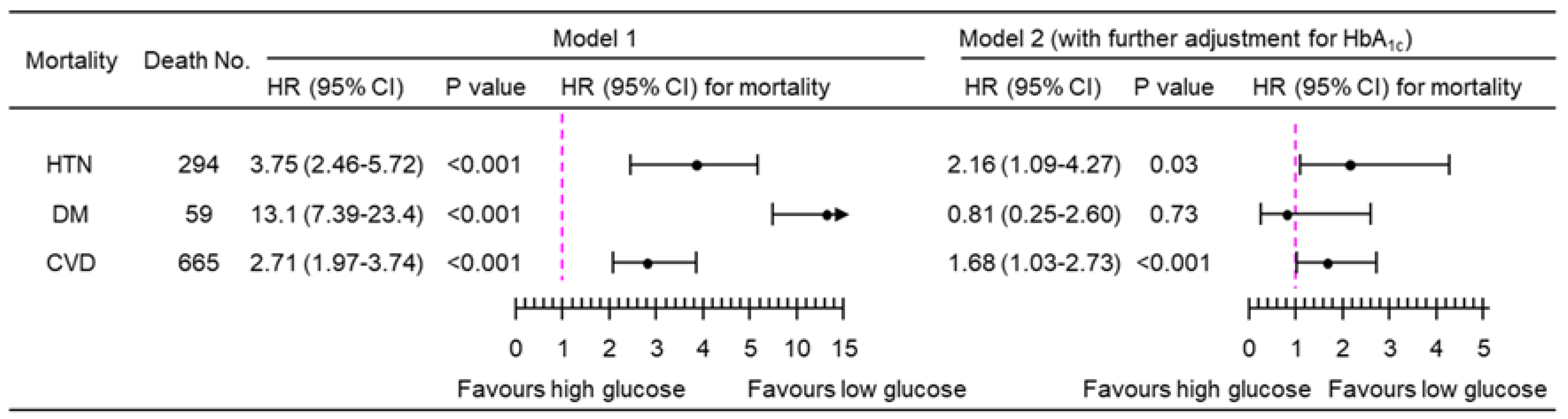
Figure 6.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,781 participants when the imputed data were not used. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 6.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,781 participants when the imputed data were not used. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
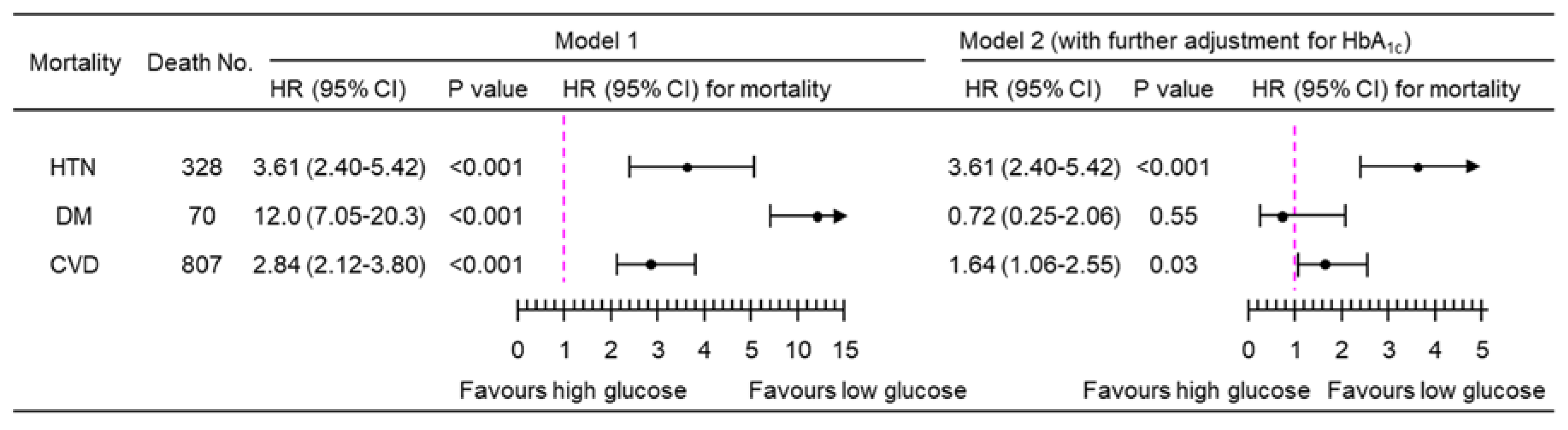
Figure 7.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,851 participants when those with a follow-up time of <1 year were excluded. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 7.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,851 participants when those with a follow-up time of <1 year were excluded. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
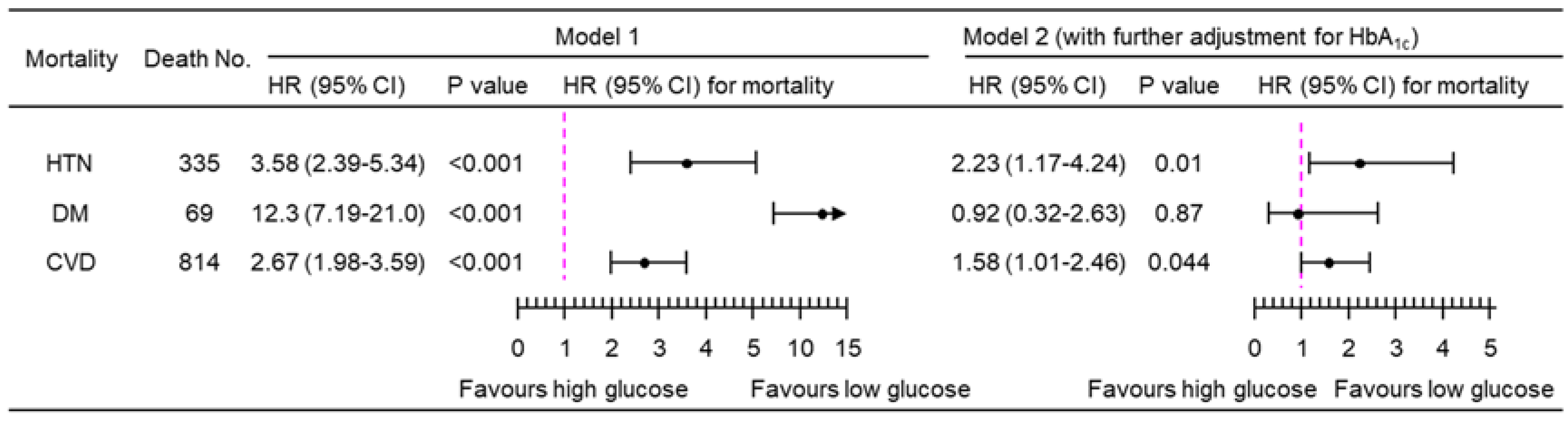
Figure 8.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,646 participants when those who were prescribed with anti-diabetic medications (N=250) were excluded. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
Figure 8.
Sensitivity analysis of mortality risk associated with a 1-natural-log-unit increase in PPG4-7.9h in 4,646 participants when those who were prescribed with anti-diabetic medications (N=250) were excluded. Model 1: adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, family history of diabetes, and fasting time. Model 2: adjusted for all the factors in Model 1 plus HbA1c. CI, confidence interval; CVD, cardiovascular disease; DM, diabetes; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR, hazard ratio; HTN, hypertension; No., number; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h.
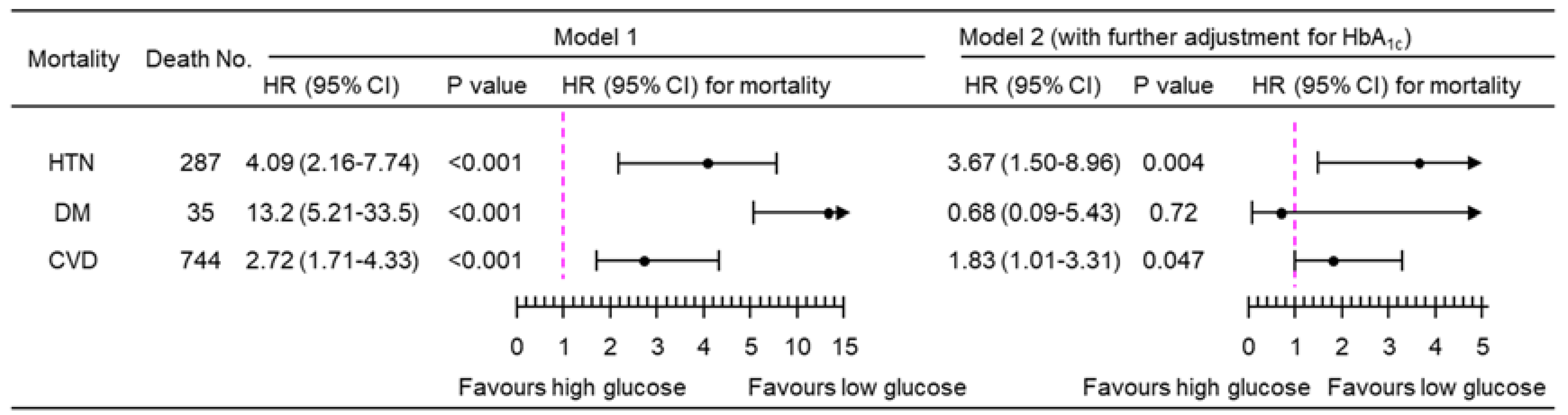

Table 1.
Baseline characteristics of the participants.
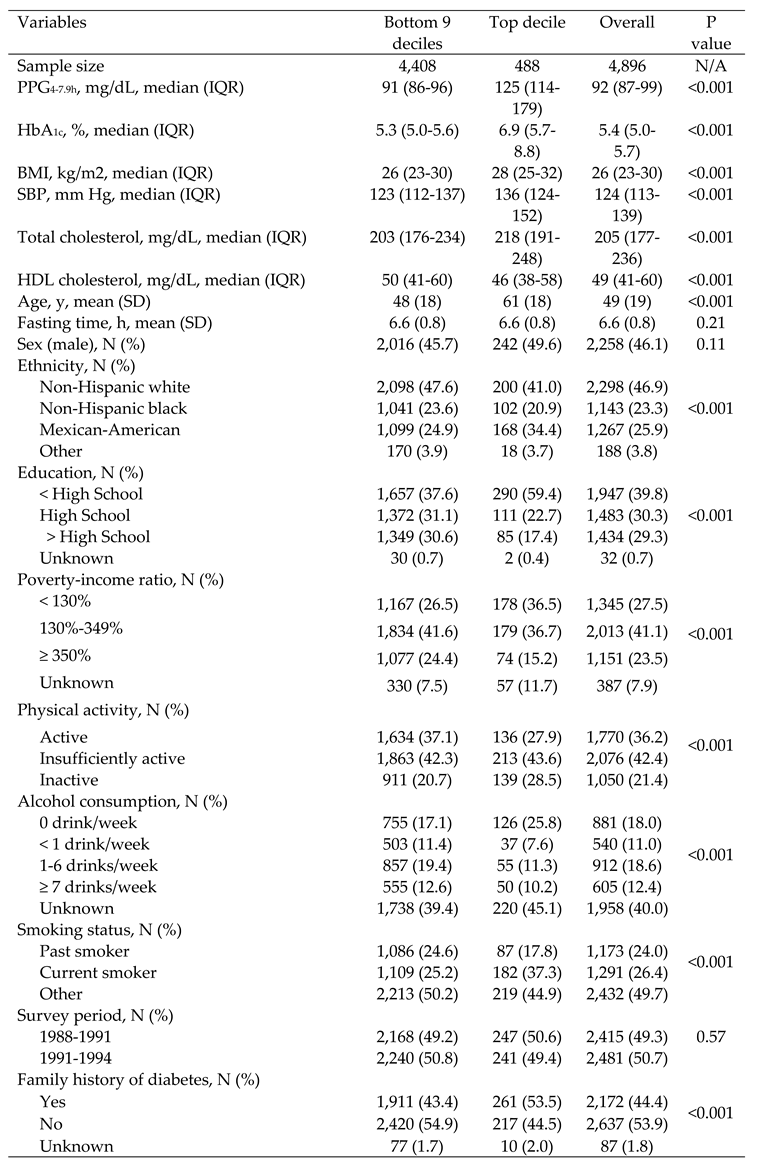 |
Abbreviations: BMI, body mass index; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; IQR, interquartile range; N, number; NA, not applicable; PPG4-7.9h, postprandial plasma glucose measured from blood taken between 4 and 7.9 h; SBP, systolic blood pressure; SD, standard deviation; y, year.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



