
Submitted:
05 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
Background: Laser therapies can cause hyper- and hypopigmentation of the skin. There is little evidence in the literature of effective treatments for these types of problems in Fitzpatrick IV-VI skin phototypes. The main aim of this retrospective study is to evaluate the effects of a new therapy combining the application of electromagnetic fields and vacuum on a subject with Fitzpatrick VI skin phototype, presenting an extensive, laser-induced facial dyschromia. The secondary aim is to test the effectiveness of a free imaging software for assessing skin pigmentation. Methods: The level of improvement after the therapy was evaluated, with a 5-point Likert scale, one month after the end of the treatment by both the subject, and the doctor who performed the treatment, and by two blinded dermatologists. With the free software, a three-dimensional reconstruction of the area treated and the evaluation of colour distribution were performed. Results: Both the subject and the doctors involved in the study positively evaluated the effects of the treatment. The image analysis highlighted the homogenization of the skin colour in the treated area. Conclusions: The combination of electromagnetic fields and vacuum for dyschromia treatments appears promising. The new method of assessing melanin levels resulted particularly efficient.
Keywords:
dyschromia
; dark colour skin
; laser side effects
; electromagnetic field
; vacuum
1. Introduction
Some skin types can develop more side effects than others if subjected to certain cosmetic treatments. Examples of the latter can be laser and non-ablative energy therapies in Fitzpatrick IV-VI skin phototypes [1]. Although in these skins the adverse effects are mainly post-inflammatory hyperpigmentation and erythema [2], irreversible hypopigmentation situations can occur [2,3]. In addition to causing aesthetic damage, all these effects can also lead to psychological damage, and to a deterioration in the quality of life (QoL), as already highlighted for other pigmentary disorders [4,5]. Therefore, it is essential to identify corrective and resolving systems and procedures.
Hypopigmentation is treated, not always with benefit, by means of systems that try to reactivate the melanocytes, or repopulate the affected area, and rebalance the production of melanin [3]. The use of different therapies and techniques for the resolution of the aesthetic damage is documented in the literature. These techniques range from topical therapies, completely non-invasive, to phototherapy with UV rays, laser therapies, combination of more or less invasive therapies, up to the transplantation of melanocytes-keratinocytes [3]. However, the studies performed almost exclusively concern Fitzpatrick I-III skin phototypes, and the results are not always completely satisfactory.
The main aim of this retrospective study is to present the effects of a new aesthetic therapy combining the application of electromagnetic fields and vacuum (V-EMF therapy) on a subject with Fitzpatrick VI skin phototype, presenting an extensive, laser-induced facial dyschromia. The secondary aim is to present a completely free imaging reprocessing model for the assessment of skin pigmentation.
2. Materials and Methods
The present retrospective study was conducted in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. Institutional Review Board approval was not applicable, as the treatment performed was an aesthetic treatment. The subject in this manuscript has given written informed consent to publication of his case details.
2.1. Subject
A 34-year-old man was admitted to the Cardiff Cosmetic Clinic (UK) with a diagnosis of hyperpigmentation associated with diffuse hypopigmentation of the face and neck. He reported that the aesthetic damage had arisen due to an epilation treatment, performed 2 months earlier, with an 808 nm diode laser (unknown model) at another aesthetic clinic.
The subject had a Fitzpatrick VI skin phototype and the macules or patches of both hyper- and hypopigmentation had the clear shape of the laser probe used previously (Figure 1).
Having noted the effects of reactivating melanin function on subjects treated with V-EMF therapy on stretch marks (SMs) and the absence of side effects [6], the aesthetic doctor decided to propose the same treatment to the subject, without guaranteeing any results. This method, in fact, had never been applied to specific problems of dyschromia and dark complexions.
2.2. V-EMF Therapy—Principles
V-EMF therapy is a completely non-invasive aesthetic therapy, that combines the simultaneous application of an electromagnetic field (EMF), with a variable frequency from 0.5 to 2 MHz (average power 4-6 W), with a vacuum of 100-150 millibars.
The principles underlying this therapy have been extensively described in Veronese et al. [7].
Briefly, the EMF is generated by a capacitive type radio frequency, in which the capacitor plates are an electrode, which transmits a high frequency signal, and the tissues to be treated. The insulation that must be present between the two plates is composed by a dielectric material, which covers the electrode, and the epidermis. The current passing from the electrode to the subepidermal tissues generates the EMF.
The EMF has magneto-mechanical transduction (MMT) as its main effect on tissues. This means that the flow of ions present in the treated tissues is activated, in particular sodium Na+, and potassium K+ ions. Both metabolic and catabolic exchanges are promoted, with consequent proliferative and cleareance actions of the tissues and all the cells present in the treated areas [8]. MMT is also strongly related to piezoelectric activation of tissues, particularly connective tissue, present in the extracellular matrix (ECM) [9]. This activation corresponds to the repair of ECM alterations. Finally, the ionic movement, corresponding to the development of kinetic energy, determines a thermal effect, with an increase in intradermal temperature of 1-2°C [10], which further promotes the proliferation and clearance of tissues and cells [11].
2.3. V-EMF Therapy—Treatment
The subject underwent 9 weekly sessions of 15-20 minutes each of V-EMF therapy. The therapy was delivered via the Bi-one® Life Touch Therapy device (Expo Italia Srl, Florence, Italy). This device is capable of delivering EMFs and vacuum, both variable, thanks to an automatic feedback control system, which allows adjustment of the applied frequency based on the thickness of the skin and the heating of the area.
Before each session, the subject’s skin was cleaned with a neutral non-alcoholic cleanser. The treatment was delivered with the subject lying supine on a table. The handpiece of the device was positioned on the skin and slid over the face and neck, to ensure uniformity of action over the entire area.
At the end of each session, no protective, smoothing, or moisturizing products were applied to the skin. The subject was asked not to use topical products during the entire treatment cycle.
2.4. Analysis
One month after V-EMF therapy, the level of satisfaction with the results was tested. Both the subject and the doctor who performed the treatment evaluated the aesthetic results, using a 5-point Likert Scale (I = no improvement, II = slight improvement 1-25%, III = moderate improvement 26-50%, IV = good improvement 51-75%, V = very good improvement 76-100%).
Additionally, anonymized facial images before and after treatment were analyzed by two blinded independent dermatologists. They rated the improvements using the same Likert Scale mentioned above.
2.5. Imaging Analysis
Melanin rebalancing was assessed using a new procedure. Skin coloration analysis was performed indirectly with the free software ImageJ.JS (National Institute of Mental Health, Bethesda, Maryland, USA).
Photographs taken of the subject before and after treatment were converted to grayscale images (transforming them from RGB colour to 8-bit images).
Using the “Surface Plot” function, three-dimensional greyscale reconstructions were performed of both the areas of the face affected by the dyschromia and the adjacent intact areas. This allowed to qualitatively evaluate both the extent of the damage and the improvement after treatment. The more intact the area, the more uniform the three-dimensional representation.
A quasi-quantitative analysis was performed by evaluating the grayscale distribution with the function: “Histogram”. The more intact the area, the narrower the peak in the Gaussian distribution, because there are fewer colour deviations.
3. Results
3.1. Aesthetic Results
One month after V-EMF therapy, the skin colour appeared homogeneous, with the disappearance of both hyperpigmentation macules and hypopigmentation patches (Figure 2). Of note, the post-inflammatory hyperpigmentation had already resolved during the treatment sessions, before the end of the entire cycle. No discomfort or pain on the part of the subject was highlighted during the treatment sessions. No side effects were found after the complete treatment.
As regards the aesthetic effects of the therapy, both the treated subject and the doctor who performed the treatment said they were extremely satisfied, defining the final result as an excellent improvement (level V on the Likert Scale). The two blindly consulted dermatologists also gave the same score to the improvement observed by comparing the photos of the subject before and after the treatment.
3.2. Imaging Evaluations
After converting the pre-treatment photo to grayscale (Figure 3a), selecting 2 areas of the face, one healthy and one damaged, the three-dimensional representation of the 2 areas allowed a qualitative assessment of the levels of melanin present (healthy—Figure 3b; discolored—Figure 3d). The healthy area presented a uniform distribution (Figure 3b), while the damaged area presented a notable inhomogeneity, with the presence of depressions, corresponding to the hypopigmentation patches, and protuberances, corresponding to the hyperpigmentation macules (Figure 3d). Subsequently, the calculation of the distributions of gray values allowed the values of melanin levels to be simulated. Before treatment, the intact area exhibited a narrow-band mono-peak distribution (Figure 3c), confirming the uniformity of the staining. The laser-damaged area had a multi-peak distribution with wide-range values (Figure 3e), confirming the inhomogeneity of the staining.
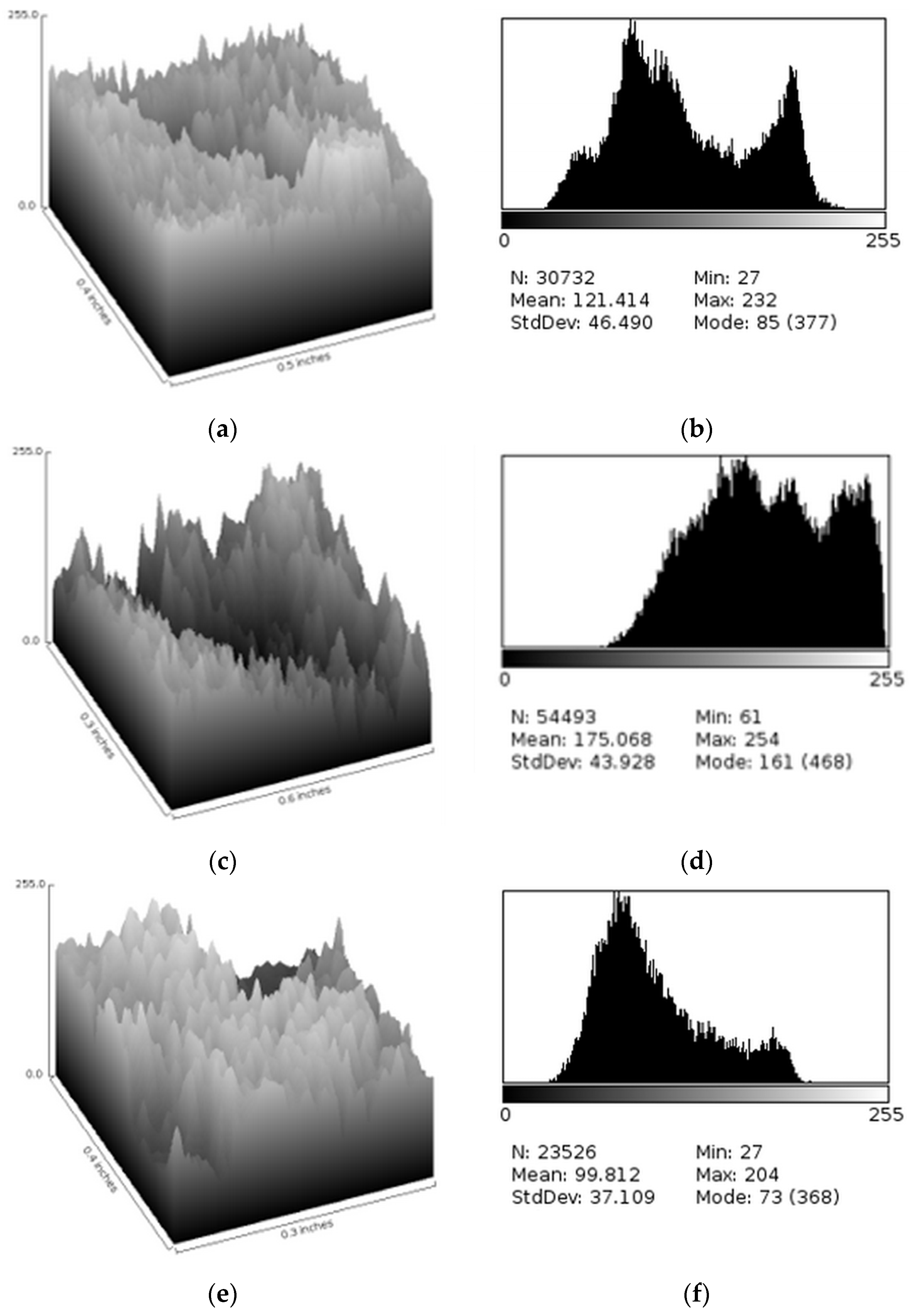
To verify the effectiveness of the method, smaller areas with different types of dyschromia were selected: an area presenting both hyper- and hypopigmentation (Figure 3a—dotted selection), an area with only hypopigmentation (Figure 3a—*), and an area with only hyperpigmentation (Figure 3a—#). Both the three-dimensional reconstruction and the calculation of the distribution of gray levels were performed, confirming the correspondence of depressions for hypopigmentation and bumps for hyperpigmentation.
Figure 4.
Details of skin alterations induced by laser treatment. (a) Three-dimensional representation of an area where the effects of hypo and hyperpigmentation overlap (dotted selection in Figure 3a). Both a depression and a bump are present. (b) Gray level distribution of the same area shown in Figure 4a. A multipeak distribution with a wide range of values is evident, indicating non-uniform staining. (c) Three-dimensional representation of an hypopigmented area (# in Figure 3a). A deep depression is evident. (d) Gray level distribution of the same area shown in Figure 4c. A multipeak distribution with a wide range of values is shown, but this distribution differs from that in Figure 4b because the range of values is shifted towards light colours, indicating low levels of melanin. (e) Three-dimensional representation of an hyperpigmented area (* in Figure 3a). A protuberance shaped like the laser probe is clearly visible. (f) Gray level distribution of the same area shown in Figure 4e. A multipeak distribution with a wide range of values is present, but this distribution differs from that in Figure 4b and in Figure 4d because the range of values is shifted towards dark colours, indicating high levels of melanin.
Figure 4.
Details of skin alterations induced by laser treatment. (a) Three-dimensional representation of an area where the effects of hypo and hyperpigmentation overlap (dotted selection in Figure 3a). Both a depression and a bump are present. (b) Gray level distribution of the same area shown in Figure 4a. A multipeak distribution with a wide range of values is evident, indicating non-uniform staining. (c) Three-dimensional representation of an hypopigmented area (# in Figure 3a). A deep depression is evident. (d) Gray level distribution of the same area shown in Figure 4c. A multipeak distribution with a wide range of values is shown, but this distribution differs from that in Figure 4b because the range of values is shifted towards light colours, indicating low levels of melanin. (e) Three-dimensional representation of an hyperpigmented area (* in Figure 3a). A protuberance shaped like the laser probe is clearly visible. (f) Gray level distribution of the same area shown in Figure 4e. A multipeak distribution with a wide range of values is present, but this distribution differs from that in Figure 4b and in Figure 4d because the range of values is shifted towards dark colours, indicating high levels of melanin.
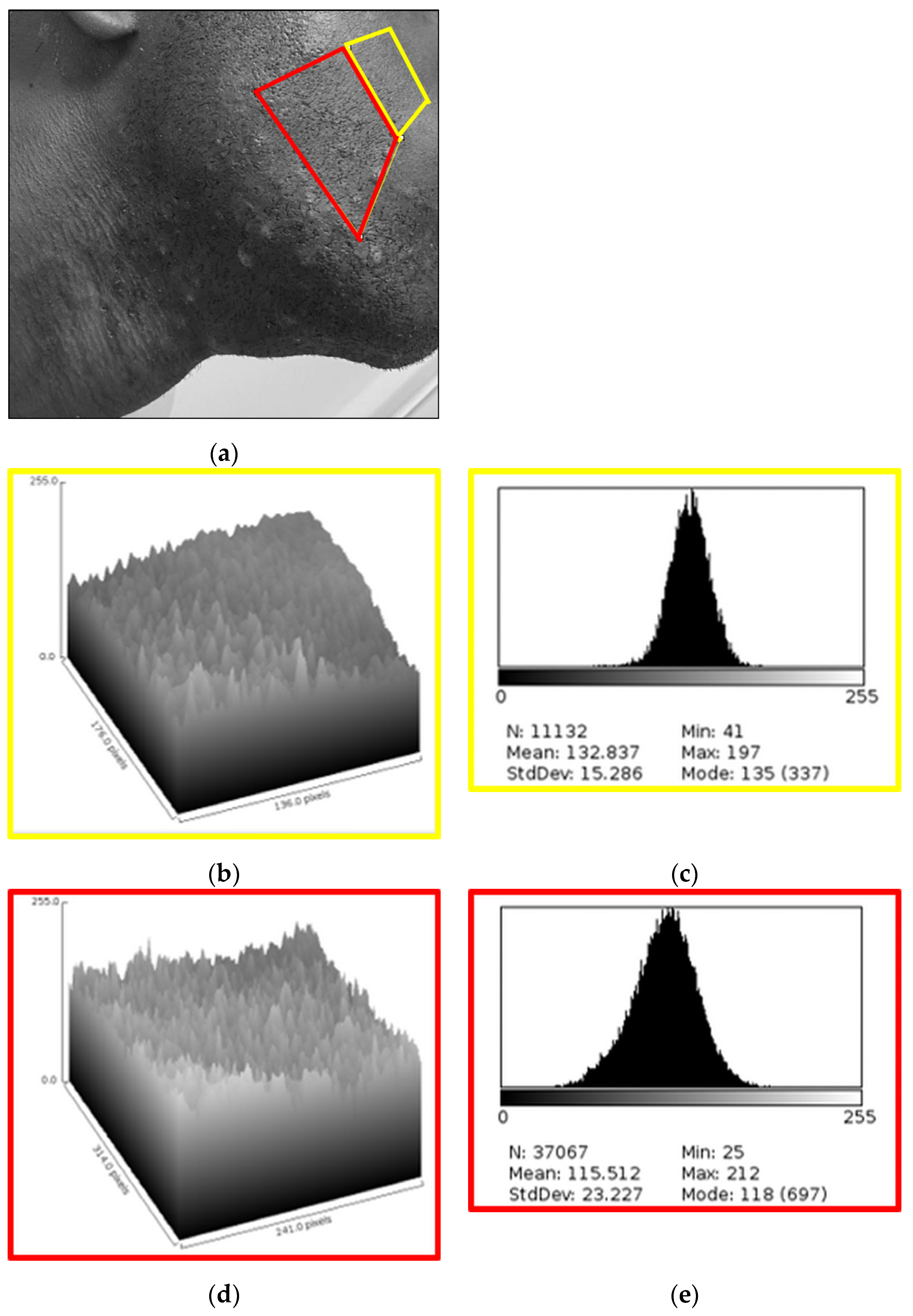
After converting the post-treatment photo to grayscale (Figure 5a), two areas corresponding approximately to those selected in the pre-treatment photo were selected. Three-dimensional representation was performed for both. The healthy area maintained a uniform distribution (Figure 5b), comparable to the pre-treatment reconstruction (Figure 3b). On the contrary, the area damaged by the laser presented a complete modification, with a once again homogeneous three-dimensional reconstruction, free of depressions and protuberances, significant for a normalization of melanin levels (Figure 5d). The grayscale distribution retained its narrow-band mono-peak shape for the healthy area (Figure 5c). A slight difference was noted compared to the pretreatment distribution (Figure 3c). The most represented values were similar (on the scale of 255 gray tones, 196 pre-treatment vs. 197 post-treatment), while the average value was different (on the scale of 255 gray tones, 106,820±15,328 pre-treatment vs. 132,837±15,286 post-treatment). This variation is attributable to the different brightness of the two original photos. The average deviation of the two healthy areas was 10.2%. The grayscale distribution for the damaged area took on a narrow-band mono-peak shape (Figure 5d), thus highlighting the normalization of the structure, i.e., the uniformity of the staining. The difference between the damaged treated area and the adjacent healthy area was attributed to the presence of shaved hair in the treated area.
4. Discussion
The treatment of irreversible hypopigmentation in individuals with Fitzpatrick IV-VI skin phototypes remains a challenge in dermatology. A recent work by Rao et al. [3] exhaustively documents the possible causes of skin hypopigmentation and the corrective treatments known so far. Compared to hypopigmentation caused by viruses, bacteria, and fungi, which is mainly treated pharmacologically, iatrogenic hypopigmentation is mainly treated with mechanical devices. The literature documents several cases. However, overall, there are few cases of treatments for Fitzpatrick IV-VI skin phototypes.
Kang et al. [16] highlighted the ineffectiveness of many techniques in the treatment of dyschromia in African Americans and Hispanics. However, they also highlighted that interventions on these people are scarce, mainly for economic reasons. In fact, since these are problems, understood almost exclusively as purely aesthetic, the costs are totally borne by the interested parties. This fact is extremely serious, if we consider that pigmentation disorders often lead to the onset of psychological effects and worsening of QoL [4.5].
The case described in this study can be considered rare, as both hyper- and hypopigmentation were co-present, and dyschromia was widely spread on the face and neck. This made the choice of treatment particularly difficult, having to resolve opposite situations, with the risk of healing one problem and worsening the other. Since hyperpigmentation spots are often post-inflammatory, and tend to resolve or reduce over time, even without specific treatments, the aesthetic doctor focused on depigmentation.
V-EMF therapy had already been used successfully for the treatment of SMs [6] and scars [7,17] with reduction of visual stigmatization, and in a large number of cases as rejuvenation therapy [18]. An effect of increased metabolism and catabolism of the treated areas was observed, with regeneration of the extracellular matrix and rebalancing of the physical characteristics of the skin [6,7,17,18]. In particular, in the treatment of albae SMs, an increase in the number of melanocytes was observed after therapy, and the SMs had regained the ability to tan after exposure to the sun [6]. At the same time, no hyperpigmentation effects in the areas adjacent to the SMs were reported. This means that the treatment favoured the proliferation of melanocytes, and reactivated the function of the few residues present in the depigmented areas, without unbalancing the number and functionality of the melanocytes present in the surrounding undamaged areas. For this reason, the application of this type of treatment to the case described was not considered a gamble, but a possible practice.
The results obtained were excellent, both from an aesthetic point of view, and for the speed with which they were achieved. However, it should be underlined that the treatment was performed in a private aesthetic clinic and the entire cost was borne by the interested subject. That is, the ethical and not irrelevant problem of covering the costs relating to the treatment of dyschromia of dark phototypes remains [16].
However, the use of completely free treatment effectiveness evaluation systems, such as the one used in this study, could help reduce the cost of the treatments themselves, as it would reduce the economic burden on dermatology clinics. The image analysis system used in the present study made it possible to obtain qualitative and semi-quantitative data from the photos, i.e., indirect measures of the effectiveness of the treatment performed. There are numerous non-free software systems on the market for reprocessing facial images, and numerous devices equipped with probes that measure skin parameters. These parameters detect values of the external surface and allow to obtain, again indirectly, information on the intradermal effects of the treatments. A free system, like the one used in this study, could represent a step forward for systems for evaluating the effects of skin care. Furthermore, by helping to reduce clinical costs, it could help reduce the costs of treatments, making them accessible to a wider population.
V-EFM therapy is a new, non-medical treatment, used mainly in the aesthetic field. In this study it was applied to a very particular case. For this reason, the results obtained can only be defined as promising. The application of this therapy to a greater number of subjects is certainly necessary in order to be able to consider it as a standard therapy in solving the problems of dyschromia in general, and of dyschromia in subjects with dark skin. Even the new method of evaluating melanin levels seems to be particularly efficient, and being totally free, accessible to all people. This methodology also needs to be tested on a larger number of subjects.
5. Conclusions
Given the results of the case described and the previous applications reported in the literature, V-EMF therapy can be considered a promising technique, guaranteeing rapid effects and resulting painless for the treated subjects. The effects on dyschromia make us reflect on its possible extension to problems of vitiligo and forms of scleroderma. The new system for assessing melanin levels also appears to be extremely promising.
Author Contributions
S.V. and A.S. conceive the study; acquisition of data, their analysis and interpretation, and drafting of the manuscript were performed by S.V., R.S., T.G., and A.S.; administrative, technical, or material support were warranted by R.A. and T.G.; A.S. performed critical revision of the manuscript for important intellectual content, and supervision of the entire study.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Institutional Review Board approval was not applicable, as the treatment performed was an aesthetic treatment.
Informed Consent Statement
The subject in this manuscript has given written informed consent to publication of his case details.
Data Availability Statement
All relevant data is included in the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hu, S.; Atmakuri, M.; Rosenberg, J. Adverse Events of Nonablative Lasers and Energy-based Therapies in Subjects with Fitzpatrick Skin Phototypes IV to VI: A Systematic Review and Meta-analysis. Aesthet Surg J. 2022, 42(5), 537-547. [CrossRef]
- Alexis, A.F. Lasers and Light-based Therapies in Ethnic Skin: Treatment Options and Recommendations for Fitzpatrick Skin Types V and VI. Br J Dermatol. 2013, 169 Suppl 3, 91-97. [CrossRef]
- Rao, M.; Young, K.; Jackson-Cowan L.; Kourosh, A.; Theodosakis, N. Post-inflammatory Hypopigmentation: Review of the Etiology, Clinical Manifestations, and Treatment Options. J Clin Med. 2023, 12(3), 1243-1263. [CrossRef]
- Dabas, G.; Vinay, K.; Parsad, D.; Kumar, A.; Kumaran, M.S. Psychological Disturbances in Patients with Pigmentary Disorders: A Cross-sectional Study. J Eur Acad Dermatol Venereol. 2020, 34(2), 392-399. [CrossRef]
- Ajose, F.O.; Parker, R.A.; Merrall, E.L.; Adewuya, A.O.; Zachariah, M.P. Quantification and Comparison of Psychiatric Distress in African Patients with Albinism and Vitiligo: A 5-year Prospective Study. J Eur Acad Dermatol Venereol. 2014, 28(7), 925-932. [CrossRef]
- Scarano, A.; Sbarbati, A.; Amore, R.; Iorio, E.L.; Ferraro, G.; Lorusso, F.; Amuso, D. A New Treatment for Stretch Marks and Skin Ptosis with Electromagnetic Fields and Negative Pressure: A Clinical and Histological Study. J Cutan Aesthet Surg. 2021, 14(2), 222-228. [CrossRef]
- Veronese, S.; Brunetti, B.; Minichino, A.M.; Sbarbati, A. Vacuum and Electromagnetic Fields Treatment to Regenerate a Diffuse Mature Facial Scar Caused by Sulfuric Acid Assault. Bioengineering (Basel). 2022, 9(12), 799-808. [CrossRef]
- Maurer, M.; Lammerding J. The Driving Force: Nuclear Mechanotransduction in Cellular Function, Fate, and Disease. Annu Rev Biomed Eng. 2019, 21, 443-468. [CrossRef]
- Fukada, E.; Yasuda, I. Piezoelectric Effects in Collagen. Jpn. J. Appl. Phys. 1964, 3, 117-121. [CrossRef]
- Gracies, J.M. Physical Modalities Other than Stretch in Spastic Hypertonia. Phys Med Rehabil Clin N Am. 2001, 12(4), 769-792. [CrossRef]
- Cole, A.J.; Eagleston, R.A.; Herring, S.A. The Benefits of Deep Heat. Phys Sportsmed. 1994, 22(2), 76-88. [CrossRef]
- Martino, F.; Perestrelo, A.R.; Vinarský, V.; Pagliari, S.; Forte, G. Cellular Mechanotransduction: From Tension to Function. Front Physiol. 2018, 9, 824-844. [CrossRef]
- Moortgat, P.; Anthonissen, M.; Meirte, J.; Van Daele, U.; Maertens, K. The Physical and Physiological Effects of Vacuum Massage on the Different Skin Layers: A Current Status of the Literature. Burns Trauma. 2016, 4, 34-45. [CrossRef]
- Charras, G.; Yap, A.S. Tensile Forces and Mechanotransduction at Cell-Cell Junctions. Curr Biol. 2018, 28(8), R445-R457. [CrossRef]
- Pinheiro, D.; Bellaïche, Y. Mechanical Force-Driven Adherens Junction Remodeling and Epithelial Dynamics. Dev Cell. 2018, 47(1), 3-19. Erratum in: Dev Cell. 2018, 47(3), 391. [CrossRef]
- Kang, S.J.; Davis, S.A.; Feldman, S.R.; McMichael, A.J. Dyschromia in Skin of Color. J Drugs Dermatol. 2014, 13(4), 401-406.
- Veronese, S.; Beatini, A.; Urbani, C.; Lanza, E.; Paz, O.M.; Saussaye, Y.; Lomuto, M.; Sbarbati, A. V-EMF treatment of Facial Scar: First Results. J Tissue Viability. 2022, 31(4), 614-618. [CrossRef]
- Laura, S.; Veronese, S.; Alberti, G.; Bacci, P.A.; Beatini, A.; Fulgione, E.; Urbani, C.; Sbarbati, A. Vacuum and Electromagnetic Field in Synergy for Skin Rejuvenation: A Retrospective Study on 217 Patients. J Cosmet Dermatol. 2023, 22(11), 2989-2995. [CrossRef]
Figure 1.
Before treatment, the skin showed both macules of post-inflammatory hyperpigmentation and patches of hypopigmentation throughout the beard area.
Figure 1.
Before treatment, the skin showed both macules of post-inflammatory hyperpigmentation and patches of hypopigmentation throughout the beard area.

Figure 2.
After the treatment, the excellent resolution of the dyschromia was noted. Melanocytic reactivation was evident.
Figure 2.
After the treatment, the excellent resolution of the dyschromia was noted. Melanocytic reactivation was evident.

Figure 3.
Assessment of pre-treatment melanin levels. (a) Conversion of the subject photo to a grayscale image (range 255 pixels). Clearly defined areas of hypo- (#), and hyperpigmentation (*), and areas where the two effects overlap (dotted selection) are evident. (b) Three-dimensional representation of the healthy area, which has a uniform texture (yellow selection in Figure 3a). (c) Gray level distribution of the healthy area, levels directly related to melanin levels. Intact, untreated skin shows a single-peak distribution with a narrow range of values, indicating uniform staining. (d) Three -dimensional representation of the area treated with the 808 Nm diode laser for epilation (red selection in Figure 3a). The skin texture appears uneven with depressions and bumps. (e) Gray level distribution of the treated area. The multi-peak profile indicates uneven skin pigmentation.
Figure 3.
Assessment of pre-treatment melanin levels. (a) Conversion of the subject photo to a grayscale image (range 255 pixels). Clearly defined areas of hypo- (#), and hyperpigmentation (*), and areas where the two effects overlap (dotted selection) are evident. (b) Three-dimensional representation of the healthy area, which has a uniform texture (yellow selection in Figure 3a). (c) Gray level distribution of the healthy area, levels directly related to melanin levels. Intact, untreated skin shows a single-peak distribution with a narrow range of values, indicating uniform staining. (d) Three -dimensional representation of the area treated with the 808 Nm diode laser for epilation (red selection in Figure 3a). The skin texture appears uneven with depressions and bumps. (e) Gray level distribution of the treated area. The multi-peak profile indicates uneven skin pigmentation.
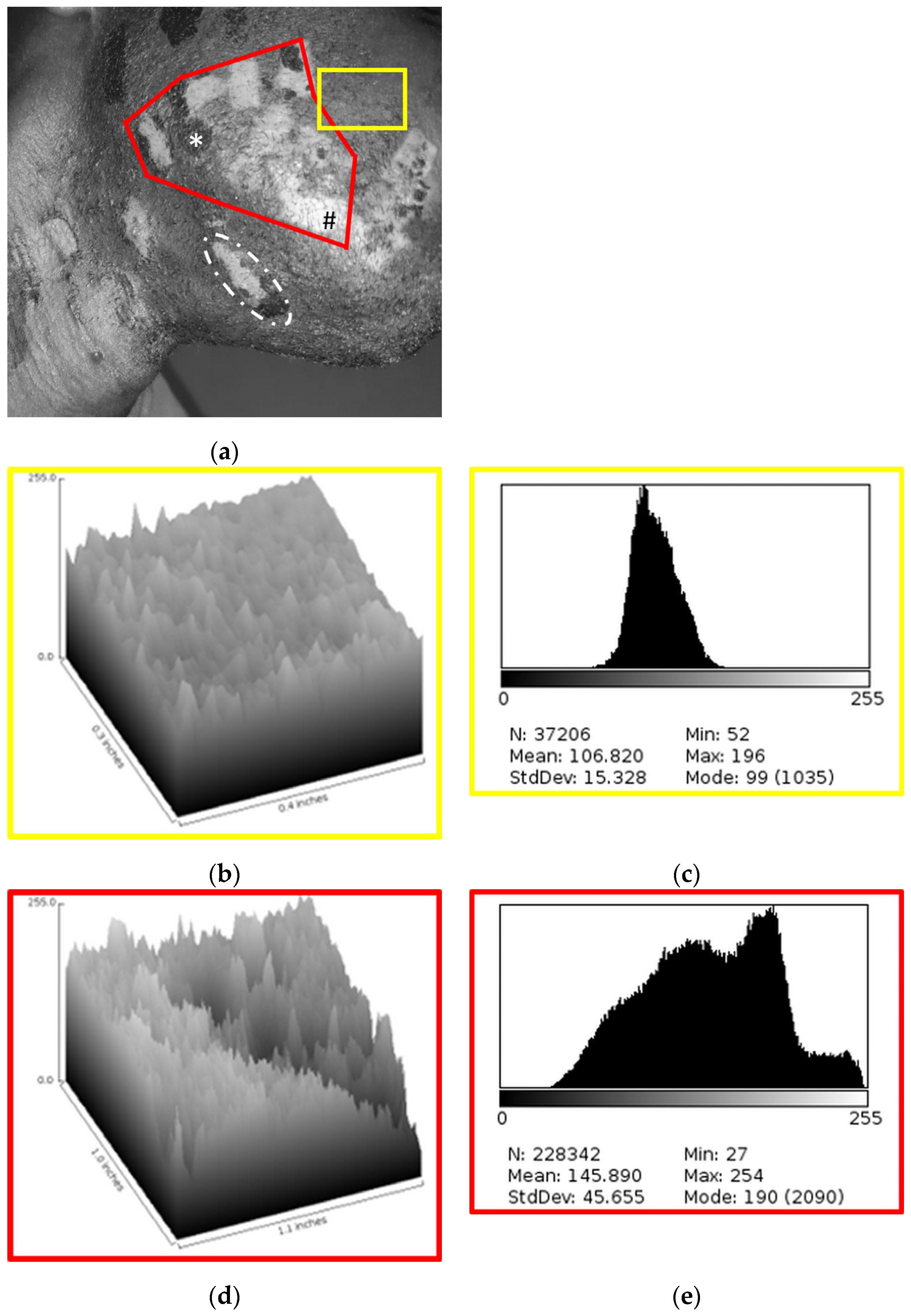
Figure 5.
Assessment of post-treatment melanin levels. (a) Conversion of the subject photo to a grayscale image with 2 selections, yellow for untreated intact skin and red for treated skin. (b) Three-dimensional representation of the healthy area (yellow selection in Figure 5a). (c) Gray level distribution of the healthy area. (d) Three-dimensional representation of the treated area, where the skin assumes the same profile as the intact skin, both with respect to Figure 5b, and with respect to Figure 3b. (e) Gray level distribution of the treated area, which appears mono-peak, signifying the effectiveness of the treatment performed.
Figure 5.
Assessment of post-treatment melanin levels. (a) Conversion of the subject photo to a grayscale image with 2 selections, yellow for untreated intact skin and red for treated skin. (b) Three-dimensional representation of the healthy area (yellow selection in Figure 5a). (c) Gray level distribution of the healthy area. (d) Three-dimensional representation of the treated area, where the skin assumes the same profile as the intact skin, both with respect to Figure 5b, and with respect to Figure 3b. (e) Gray level distribution of the treated area, which appears mono-peak, signifying the effectiveness of the treatment performed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



