Submitted:
04 January 2024
Posted:
05 January 2024
You are already at the latest version
Abstract
Anastomotic Leakage (AL) remains the main cause of post-esophagectomy morbidity and mortality. Early detection can avoid sepsis and reduce morbidity and mortality. This study evaluates the diagnostic accuracy of the NUn-score and its components as early detectors of AL. This single centre observational cohort study included all esophagectomies from 2010-2020. C-reactive Protein (CRP), Albumin (Alb) and White cell count (WCC) were analyzed and Nun-scores calculated. Area under the curves (AUC) were used to assess their predictive accuracy. Seventy-four of the 668 patients (11%) developed an AL. CRP and the NUn-score proved to be good diagnostic accuracy tests on POD2 (CRP AUC:0,859; Nun-score AUC:0,869) and POD4 (CRP AUC:0,924; Nun-score AUC:0,948). A 182mg/L CRP cut-off on POD4 yielded a 87% sensitivity, 88% specificity, a negative predictive value (NPV) of 98% and a positive predictive value (PPV) of 47,7%. A Nun score cut-off>10 resulted in 92% sensitivity, 95% specificity, 99% NPV and 68% PPV. Albumin and WCC have limited value in the detection of post-esophagectomy AL. Elevated CRP and a high NUn score on POD4 provide a high accuracy to predict AL after esophageal cancer surgery. Their high negative predictive value allows to select patients who can safely proceed with enhanced recovery protocols.
Keywords:
NUn score
; esophagectomy
; anastomotic leakage
; risk score
; esophageal cancer
; inflammatory biomarkers
1. Introduction
The incidence of esophageal (EC) is increasing, making it the 6th leading cause of cancer related mortality worldwide (1). The prognosis remains poor with 5 Year overall survival rates varying from 90% for stage 1 cancer to <10% for stage IV cancer patients. For locally advanced cancer, multimodality therapy followed by surgery has convincingly improved both local control and overall survival (2; 3). Surgical resection and lymphadenectomy remain crucial in the treatment of non-metastatic esophageal cancer patients (4; 5). However, the procedure is known for its potentially complicated postoperative course. Large benchmarking series report postoperative complications in more than 50% of cases, even in high volume centers. Pulmonary complications (15-25%), cardiac events (14-15%) and failure of the esophagogastric anastomosis (12-16%) remain the most important sources of both morbidity and mortality after esophagectomy (6; 7; 8). Considerable improvements in surgical technique and perioperative care have resulted in 90-day mortality rates after esophagectomy of less than 5% in experienced centers (6; 7; 8). However, the mortality of AL remains high, ranging from 7 to 17% (9; 10). The severity of AL depends on the location of the anastomosis, the estimated surface and circumference of the defect, the extent of contamination, the degree of sepsis, and the time from occurrence to diagnosis and therapy (11). Early detection and management of an AL can prevent the development of a mediastinitis related sepsis and is critical to improving its outcome (12).
Inflammatory biomarkers have previously been proposed as easy and cheap tests for early diagnosis of postoperative infectious complications after major surgery. C-reactive protein (CRP) is an acute phase protein produced in response to infection, tissue damage and ischemia. A low CRP on postoperative day (POD) 3 and 5 may rule out AL after esophagectomy (12). However, it can be difficult to distinguish the normal systemic inflammatory response to surgical stress from AL associated sepsis. Identifying a clinically relevant, easy to use scoring system may be helpful in the early diagnosis of AL, selecting patients for imaging, and tailoring AL management. Noble and Underwood introduced the NUn score, using acute phase markers white cell count (WCC), CRP and albumin (Alb) as a predictor of AL and major postoperative complications (13). The attempts to validate the score are limited and conflicting (14; 15; 16; 17). We aimed to determine the diagnostic accuracy of these inflammatory response biomarkers and the combined NUn score as early predictors of post-esophagectomy AL.
2. Materials and Methods
The study protocol was approved by the institutional review board of the Ghent University Hospital (reference: B670201111232).
2.1. Surgery and Postoperative care:
Transthoracic (sub)total esophagectomy with 2 or 3-field lymphadenectomy and a right intrathoracic (Ivor Lewis, IL or Transhiatal, THE) or cervical esophagogastric anastomosis (McKeown, McK) was performed in all cases. All procedures were performed by 2 surgeons (PP&EVD). The surgical approach included open as well as hybrid minimally invasive procedures (introduced in 2013). Fully minimal invasive esophagectomy (MIE) was introduced in 2014. All patients received an intrathoracic end-to-side or end-to-end circular esophagogastric anastomosis using a Premium Plus EEA™ (Medtronic) stapler (25 or 28 mm), or a standardized cervical end-to-side hand sewn anastomosis. Patients recovered at the intensive care unit for 12-24h and were then discharged to a dedicated gastrointestinal surgery ward. A nasogastric tube was kept in place during a period of 2-3 days. A water-soluble contrast swallow was obtained on the third postoperative day as a routine screening before initiating oral intake. Patients suspected of AL received an emergency CT scan with oral contrast and/or upper endoscopy. Anastomotic leakage was treated conservatively, endoscopically, or surgically according to clinical presentation. Nutritional support was provided by a feeding jejunostomy. Since 2018 patients were treated according to an Enhanced Recovery After Surgery (ERAS) protocol.
2.2. Patient selection:
This cohort study was based on data gathered from a prospectively kept institutional database supplemented with data from the electronic patient records. Consecutive patients undergoing esophagectomy for cancer and fitting the criteria between January 2010 and December 2020 were included. Patients in whom the esophagus was replaced with the small bowel or the colon, or who underwent concurrent laryngectomy, were excluded.
2.3. Outcomes:
Individual collected data included demographics, American Society of Anesthesiologists (ASA) score, tumor characteristics, type of neoadjuvant therapy, surgical details, pathology reports, laboratory results, and postoperative morbidity and mortality until 90 days postoperatively. Pathological staging was based on the 7th AJCC TNM classification manual. Postoperative morbidity and mortality were classified using the European Complication Consensus Group (ECCG) platform (18) and graded according to the Clavien Dindo classification (19). Anastomotic leakage was defined as a full thickness gastrointestinal defect involving the esophagus, anastomosis, staple line, or conduit irrespective of presentation or method of identification, according to the ECCG classification. Results are reported according to the Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) guidelines (20).
2.4. Inflammatory biomarkers and the NUn score:
Acute phase markers were retrieved from the daily blood samples postoperatively, WCC was measured in cells x 103/µL (reference range 3.6-9.3 103/µL) and converted to 109/L for the NUn score calculation. Serum concentrations of Albumin were expressed in g/L (normal range 35-52 g/L) and CRP in mg/L (normal range < 0.5 mg/L). The NUn score was calculated according the original Noble formula: 11.3894 + (0.005 x CRP in mg/L) + (0.186 x WCC in 109/L) - ( 0.174 x albumin in g/L). Missing data were replaced using the last observation carried forward approach.
2.5. Statistical analysis:
All analyses were performed using IBM SPSS® version 28 for Windows® and Sigmaplot® version 13 for Windows®. Continuous data are summarized as means with standard deviations (SD), or as medians with interquartile ranges (IQR). Categorical data are reported using frequencies and percentages. Independent samples t test, Pearson chi square, Fisher’s exact and Mann-Witney U tests are used to compare means and proportions. Significance of the different covariates in the prediction of AL were assessed using univariate analysis. Predictive accuracy of the biomarkers and the NUn score was assessed using receiver operating curve (ROC) analyses and the area under (AUC). Sensitivity, specificity, positive and negative predictive value are calculated for the determined cut off values of the biomarkers and the NUn score.
3. Results
3.1. Demographics of the study cohort:
Between January 2010 and December 2020, 668 esophagectomy patients were identified matching the inclusion criteria. Demographic data and their univariable association with AL are detailed in Table 1. Mean age was 64,0 ± 12,2 years (78,9%% male). Overall 74 patients (11,1%) experienced an anastomotic leak. The majority of patients were treated for an adenocarcinoma (67,5%). Univariable analysis could not identify statistically significant differences in demographics, comorbidities, neoadjuvant treatment regimens, histology or clinical staging between the patients with and without leakage, except for a higher percent of ASA 3 patients in the AL group. The surgical procedure, approach and conditions did however significantly influence the AL rate, with a significant higher AL rate in patients with a cervical anastomosis (McK 28% vs IL 10,9% vs THE 5,2%, p=0,010), after total minimally invasive surgery (16,8% vs 8,6% after both open and hybrid procedures, p=0,008) and when an emergency procedure was performed. AL was defined according to the ECCG guidelines, diagnosed on CT-scan and/or upper GI endoscopy and graded according to both the CD (17,6% gr 2; 1,4% gr 3a; 43,2% gr 3b; 27% gr 4a; 8,1% gr 4b and 2,7% gr 5) and ECCG grading system (18,9% type 1; 12,2% type 2 and 68,9% type 3).
3.2. Mean levels of inflammatory biomarkers and severity of the AL:
CRP was available in 642 and 613 patients on POD2 and 4, WCC was measured in 645 and 662 patients on both days and Albumin was available for 596 patients on POD2 and 615 on POD4. Missing data were replaced using the last observation carried forward approach. Nun scores were calculated for all but 5 patients on POD2 and 4 on POD4. Mean CRP, WCC and combined NUN scores were significantly higher in AL patients compared to the non-AL patients, and this significance was confirmed for al ECCG AL types. Mean Alb was significantly lower in the AL group. Mean CRP and WCC levels were higher in patients with a more sever ECCG grade of AL, specifically when type 1 AL were compared to type 2 and 3 AL. The significance was present for the evaluated biomarkers both on POD2 and POD4 (Figure 1). All biomarkers were identified as significant markers for any type of AL at POD2 and POD4 on univariate analysis including the NUn-score proposed by Noble (Table 2).
3.3. Optimal cut-off and predictive accuracy of Albumin:
Mean Albumin levels for patients with and without AL were 25.2 versus 28.0 g/L on POD2 (p<0.001) and 24.3 versus 28.5 g/L on POD4 (p<0,001). Figure 2 shows the ROC curve analyses of albumin, with a fair performance on POD2 (AUC 0.710, 95% CI: 0.646 – 0.774) and POD4 (AUC 0.799, 95% CI: 0.746 – 0.853). A POD4 albumin threshold of 26.5 g/L had the highest but still limited diagnostic accuracy, with a sensitivity of 80%, a specificity of 68%, a negative predictive value of 96% but a positive predictive value of only 24%.
3.4. Optimal cut-off and predictive accuracy of CRP:
The mean CRP levels for patients with and without AL was 218,9 versus 125,9 mg/L respectively on POD2 (p<0,001) and 255,2 mg/L versus 111,1 on POD4 (p<0,001). Figure 2 shows the ROC curve analyses of CRP, with a good performance on POD2 (AUC 0.859, 95% CI: 0.816 – 0.903) and an excellent performance on POD4 (AUC 0.924, 95% CI: 0.896 – 0.953). A POD4 CRP threshold of 181,5 mg/L had the highest diagnostic accuracy compared to all the other individual markers, with a sensitivity of 87%, a specificity of 88%, a negative predictive value of 98% and a positive predictive value of 48%.
3.5. Optimal cut-off and predictive accuracy of WCC:
Mean WCC levels were significantly higher for patients with AL (14.0 and 13.4 x 103/µL on POD 2 and 4) compared to the those from patients without an AL (10.9 and 8.7 x 103/µL on POD2 and 4) (p<0,001). Figure 2 shows the ROC curve analyses of WCC, with a fair performance on POD2 (AUC 0.724 95% CI: 0.662 – 0.786) but a good performance on POD4 (AUC 0.829, 95% CI: 0.777 – 0.880). A POD4 WCC cut-off of 10.9 x 103/µL resulted in a sensitivity of 73%, a specificity of 82%, a negative predictive value of 96% and a positive predictive value of 33%.
3.6. Optimal cut-off and predictive accuracy of the NUn score:
Patients with AL presented a mean NUn score of 10.7 on POD2 and 10.9 on POD2 compared to a 9.2 and 8.6 score on POD 2 and 4 on the non-AL group (p<0,001). The presence of a NUn score>10 on POD4 as presented by Noble and Underwood who designed the score, was identified as a significant risk factor for AL both in univariate and multivariate analysis in this study group. Figure 2 shows the ROC curve analyses of the NUn score, with a good performance on POD2 (AUC 0.869, 95% CI: 0.833 – 0.905) and an excellent performance on POD4 (AUC 0.948, 95% CI: 0.923 – 0.972). This combined score presented an excellent performance on POD4 with an even higher AUC (AUC 0.948) than CRP on POD4 (AUC 0.924). A POD4 NUn score of >10 had the highest diagnostic accuracy compared to all the other individual markers, with a sensitivity of 92%, a specificity of 95%, a negative predictive value of 99% and a positive predictive value of 68% (Table 3).
4. Discussion
Failure of the esophagogastric anastomosis (12-16%) remain the most important source of prolonged hospital stay, increased risk for reoperation and stricture, short term reduced quality of live, increased costs and increased perioperative death (21; 11). The effect of post esophagectomy AL on long term oncological and functional outcome is still under debate (22; 23; 24; 25).
The clinical presentation of AL is diverse and its severity ranges widely, mainly determined by the location and extent of the defect, the extent of the contamination and sepsis, and the time from onset to treatment (11). Early diagnosis and treatment helps to prevent subsequent sepsis and improves AL related outcome. This observational study demonstrates the clinical utility of both CRP and the NUN score in postoperative AL monitoring in esophagectomy patients. The high NPV and the rather low PPV, however suggest that their main value is not the early detection, but rather the early exclusion of an AL.
A postoperative drop in albumin (Alb) is thought to be a marker for surgical stress and low concentrations of Alb and prealbumin on POD4-6 are identified as potential risk factors for AL. Five studies evaluated post Alb in relation to AL but only Noble reported a significant association with a POD 5 cut-off <22,5 g/L with fair performance (AUC 0,742) (13; 14; 15; 26; 27; 28; 29). Our analyses identified an equally fair performance for Alb with threshold values of <24,5 on POD2 (AUC 0,710) and <26,5 g/L on POD4 (AUC 0,799). Given the limited AUCs, the authors do not advocate Alb alone as a prediction of AL, however pre albumin, Alb in combined scores (Alb/CRP ratio, CART algorithm) and a perioperative Alb decrease of 11 g/L seem more promising as predictors (29; 27; 30).
Elevated CRP levels are the most common previously identified marker for post esophagectomy complications (13; 14; 15; 17; 27; 28; 29; 30; 31; 32) (33; 34; 35; 36; 37; 38; 39; 40; 41; 42) (43; 44; 45; 46). CRP is an acute phase protein synthesized in the liver in response to endotoxins, and its levels commonly increase within 6h after the onset of the inflammation. It is a marker for acute inflammation with a high sensitivity but often low specificity for its inflammatory origin. CRP values have been studied from POD 1-10 with most studies focusing on POD 3-5. However the earlier the AL is suspected, the earlier adequate diagnosis and treatment can be performed. We therefor focused on POD 2-4, as POD1 CRP showed low diagnostic performance in previous literature. In this study mean CRP levels on POD2-4 were significantly higher in the AL group and proportionally correlated to the ECCG type of the AL. A finding consistent with Hagens’s findings, however due to the small sample size in that cohort, they could not prove statistical significance (46). ROC curves were plotted to identify a CRP cut-off level of 165 mg/L on POD2 with good diagnostic performance (AUC 0.859) and cut-off level of 181 mg/L on POD4 with excellent performance on POD4 (AUC 0.924). Six other studies evaluated POD2 CRP with varying thresholds from 177-300 mg/L (13; 33; 35; 39; 40; 41). All studies identified higher thresholds then ours on POD2, and with lower AUC’s, except Ji who identified a cut-off of 177 mg/L on POD2 with a good performance (AUC 0,994, sens 90%, spec 95%) similar to the one identified in this study. Our POD4 cut-off of 181 mg/L was significantly higher than the cut-off level of 111 mg/L reported by Miki (43) and 106 mg/L by Stuart (44), probably because they only included MIE patients, but in line with the threshold value of 177 mg/L published in a meta-analyses by Aiolfi (12). Based on the high AUC, the relevant sensitivity, specificity, low PPV but high NPV, we could identify POD2-4 CRP levels only to be useful in the exclusion and not in the diagnosis of an AL. Consistent with most other studies who identify CRP as a negative predictor for AL but not as a clinically useful diagnostic test.
Mean WCC levels were significantly different between the AL and the non-AL patients. However our study identified WCC on POD 2 to have only a fair diagnostic accuracy (AUC 0,724) while POD4 had a good diagnostic performance (AUC 0,829) on POD 4. The high NPV and low PPV again suggests clinically use as negative predictor instead of a diagnostic tool. Multiple studies evaluated WCC but only 3 reported cut-off values, however on POD 3 and 5 and with poor diagnostic accuracy, eliminating the possibility for comparison (31; 32; 26; 13; 14; 15; 17; 33; 43; 47).
Noble combined CRP, Alb and white cell count in the NUn score, in an attempt to increase their accuracy as a AL predictor (13). Findlay and Paireder failed to validate the score, potentially because they included all AL, both symptomatic and asymptomatic compared to Noble who included only “leaks sufficient to cause symptoms” (14; 16). Bundred however successfully validated the scores’ cut-off value of 10 on POD4 for AL, however with a fair diagnostic accuracy (AUC 0,77) and again including “any symptomatic leak, confirmed by radiology or endoscopy” consistent to Noble’s definition (15). Liesenfeld identified a sign difference between the mean NUn score of AL negative and positive patients (8.6 vs 9.1, p=0.006) but the optimal cut-off value recommended by Noble could not be confirmed as AL predictor (17). Mean NUn scores on POD2-4 were significantly different between both groups in our cohort. The presence of a NUn score >10 on POD4 was identified as a significant risk factor for AL and the ROC curve analyses showed good performance on POD2 (AUC 0.869) and an excellent performance on POD4 (AUC 0.948), validating the score in this cohort. A POD4 NUn score of >10 had the highest diagnostic accuracy compared to all other markers, with a high sensitivity (92%) and specificity (95%). The NPV of 99% and PPV of 68% again suggest its main value in excluding AL rather than diagnosing them.
This study has multiple pitfalls, it is retrospective in nature but based on prospectively collected data. We included a heterogenic esophagectomy population including different procedures, approaches and types of surgery, all know to have an impact on the AL rate and potentially biasing the results. However we wanted to evaluate cheap and easily available tests and facilitate and standardize their clinical use in postoperative monitoring for all esophagectomy patients. EC cancer is a rare disease resulting in a limited amount of annual esophagectomies, nevertheless we present a large population for a single center observational study. Moreover this is the first study to validate the NUn-score for all ECCG types of AL.
5. Conclusions
CRP and the NUn score both show good diagnostic performance on POD2 and excellent performance on POD4. They are however only valuable for AL exclusion, which can be useful in algorithms for a safe and early discharge. There is no single test that can rule out AL but patients with a CRP <165 mg/L on POD2 are unlikely to develop an AL and can safely continue their ERAS protocol. Patients with a CRP <181 mg/dL and or a NUn score <10 on POD4 can safely be discharged when clinically possible. The value of CRP in the diagnosis of AL however is limited and other diagnostic tools are needed in case of AL suspicion.
Author Contributions
Conceptualization, Elke Van Daele, Hanne Vanommeslaeghe and Piet Pattyn; Data curation, Elke Van Daele, Hanne Vanommeslaeghe, Flo Decoster, Louise Beckers Perletti and Esther Beel; Formal analysis, Elke Van Daele and Wim Ceelen; Investigation, Flo Decoster, Louise Beckers Perletti and Esther Beel; Methodology, Elke Van Daele; Supervision, Yves Van Nieuwenhove, Wim Ceelen and Piet Pattyn; Writing – original draft, Elke Van Daele; Writing – review & editing, Hanne Vanommeslaeghe, Yves Van Nieuwenhove, Wim Ceelen and Piet Pattyn.
Institutional Review Board Statement
Ethical approval for the creation and maintenance of an observational prospective database for patients after esophageal resections was granted by the institutional Ethical committee of the Ghent University Hospital. Belgian registration number: B670201111232. Ethical approval for this retrospective data analysis was granted by the same Ethical committee of the Ghent University Hospital, registration number: BC-07939.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study for the inclusion in the institutional dataset. The authors received a statement from their ethical committee stating that no additional informed consent is required for this retrospective analyses.
Data Availability Statement
All relevant data are available within the paper. Additional data if needed can be obtained through the corresponding author after approval by the local ethical committee.
Acknowledgments
We thank our study and data nurses for their help in constructing and supporting our esophageal database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, Cuesta MA, Blaisse RJ, Busch OR, ten Kate FJ, Creemers GJ, Punt CJ, Plukker JT, et al CROSS Group. Preoperative chemo radiotherapy for esophageal or junctional cancer. N Engl J Med. 2012 May 31;366(22):2074-84. [CrossRef] [PubMed]
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, Cuesta MA, Blaisse RJB, Busch ORC, Ten Kate FJW, Creemers GM, et al. CROSS study group. Neoadjuvante chemoradiotherapy plus surgery versus surgery alone for esophageal or junctional cancer (CROSS): long term results of a randomized controlled trial. Lancet Oncol. 2015 Sep;16(9):1090-1098. doi: 10.1016/S1470-2045(15)00040-6. Epub 2015 Aug 5. [CrossRef] [PubMed]
- Obermannová R, Alsina M, Cervantes A, Leong T, Lordick F, Nilsson M, van Grieken NCT, Vogel A, Smyth EC and clinicalguidelines@esmo.org., ESMO Guidelines Committee. Electronic address:. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022 Oct;33(10):992-1004. [CrossRef] [PubMed]
- Lordick F, Mariette C, Haustermans K, Obermannová R, Arnold D and Committee., ESMO Guidelines. Oesophageal cancer: ESMO CLinical proactice guidelines for diagnosis, treatment and follow up. Ann Oncol. 2016 Sep;27(suppl 5):v50-v57. [CrossRef] [PubMed]
- Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G, Davies A, D'Journo XB, Gisbertz SS, Griffin SM, Hardwick R, Hoelscher A, Hofstetter W, Jobe B, Kitagawa Y, Law S, Mariette C, Maynard N, Morse CR, Nafteux P, Pera M, Pramesh CS, et al. Benchmarking Complications Associated with Esophagectomy. Ann Surg. 2019 Feb;269(2):291-298. [CrossRef] [PubMed]
- Defining Benchmarks for Transthoracic Esophagectomy: A Multicenter Analysis of Total Minimally Invasive Esophagectomy in Low Risk Patients. Schmidt HM, Gisbertz SS, Moons J, et al. Ann Surg. 2017;266:814–821.
- Collaborative., Oesophago-Gastric Anastomosis Study Group on behalf of the West Midlands Research. Comparison of short-term outcomes from the International Oesophago-Gastric Anastomosis Audit (OGAA), the Esophagectomy Complications Consensus Group (ECCG), and the Dutch Upper Gastrointestinal Cancer Audit (DUCA). BJS Open. 2021 May 7;5(3):zrab010. Erratum in: BJS Open. 2022 Jan 6;6(1):. [CrossRef] [PubMed]
- Turrentine FE, Denlinger CE, Simpson VB, Garwood RA, Guerlain S, Agrawal A, Friel CM, LaPar DJ, Stukenborg GJ, Jones RS. Morbidity, mortality, cost, and survival estimates of gastrointestinal anastomotic leaks. J Am Coll Surg. 2015 Feb;220(2):195-206. Epub 2014 Nov 8. [CrossRef] [PubMed]
- Kassis E, Kosinski A, Ross P Jr, Koppens K, Donahue J, Daniel V. Predictors of anastomotic leak after esophagectomy: an analysis of the society of thoracic surgeons general thoracic database. Ann Thorac Surg. 2013 Dec;96(6):1919-26. Epub 2013 Sep 24. [CrossRef] [PubMed]
- Ubels S, Verstegen M, Klarenbeek B, Bouwense S, van Berge Henegouwen M, Daams F, van Det MJ, Griffiths EA, Haveman JW, Heisterkamp J, Koshy R, Nieuwenhuijzen G, Polat F, Siersema PD, Singh P, Wijnhoven B, Hannink G, et al. TENTACLE—Esophagus Collaborative. Severity of oEsophageal Anastomotic Leak in patients after oesophagectomy: the SEAL score. Br J Surg. 2022 Aug 16;109(9):864-871. [CrossRef] [PubMed]
- Aiolfi A, Asti E, Rausa E, Bonavina G, Bonitta G, Bonavina L. Use of C-reactive protein for the early prediction of anastomotic leak after esophagectomy: Systematic review and Bayesian meta-analysis. PLoS One. 2018 Dec 17;13(12):e0209272. [CrossRef] [PubMed]
- Noble F, Curtis N, Harris S, Kelly JJ, Bailey IS, Byrne JP, Underwood TJ and (SC-OG)., South Coast Cancer Collaboration–Oesophago-Gastric. Risk assessment using a novel score to predict anastomotic leak and major complications after oesophageal resection. J Gastrointest Surg. 2012 Jun;16(6):1083-95. [CrossRef] [PubMed]
- Findlay JM, Tilson RC, Harikrishnan A, Sgromo B, Marshall RE, Maynard ND, Gillies RS, Middleton MR. Attempted validation of the NUn score and inflammatory markers as predictors of esophageal anastomotic leak and major complications. Dis Esophagus. 2015 Oct;28(7):626-33. [CrossRef] [PubMed]
- Bundred J, Hollis AC, Hodson J, Hallissey MT, Whiting JL, Griffiths EA. Validation of the NUn score as a predictor of anastomotic leak and major complications after Esophagectomy. Dis Esophagus. 2020 Jan 16;33(1):doz041. [CrossRef] [PubMed]
- Paireder M, Jomrich G, Asari R, Kristo I, Gleiss A, Preusser M, Schoppmann SF. External validation of the NUn score for predicting anastomotic leakage after oesophageal resection. Sci Rep. 2017 Aug 29;7(1):9725. [CrossRef] [PubMed]
- Liesenfeld LF, Sauer P, Diener MK, Hinz U, Schmidt T, Müller-Stich BP, Hackert T, Büchler MW, Schaible A. Prognostic value of inflammatory markers for detecting anastomotic leakage after esophageal resection. BMC Surg. 2020 Dec 9;20(1):324. [CrossRef] [PubMed]
- Low DE, Alderson D, Cecconello I, Chang AC, Darling GE, DʼJourno XB, Griffin SM, Hölscher AH, Hofstetter WL, Jobe BA, Kitagawa Y, Kucharczuk JC, Law SY, Lerut TE, Maynard N, Pera M, Peters JH, Pramesh CS, Reynolds JV, Smithers BM, van Lanschot JJ. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann Surg. 2015 Aug;262(2):286-94. [CrossRef] [PubMed]
- Dindo D, Demartines N, Clavien P-A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Annals of Surgery 240(2):p 205-213, August 2004. [CrossRef]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP and Initiative., STROBE. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014 Dec;12(12):1495-9. [CrossRef] [PubMed]
- Collaborative., Oesophago-Gastric Anastomosis Study Group on behalf of the West Midlands Research. Rates of Anastomotic Complications and Their Management Following Esophagectomy: Results of the Oesophago-Gastric Anastomosis Audit (OGAA). Ann Surg. 2022 Feb 1;275(2):e382-e39. [CrossRef] [PubMed]
- Aiolfi A, Griffiths EA, Sozzi A, Manara M, Bonitta G, Bonavina L, Bona D. Effect of Anastomotic Leak on Long-Term Survival After Esophagectomy: Multivariate Meta-analysis and Restricted Mean Survival Times Examination. . Ann Surg Oncol. 2023 Sep;30(9):5564-5572. [CrossRef] [PubMed]
- Markar S, Gronnier C, Duhamel A, Mabrut JY, Bail JP, Carrere N, Lefevre JH, Brigand C, Vaillant JC, Adham M, Msika S, Demartines N, Nakadi IE, Meunier B, Collet D, Mariette C, FREGAT Working Group, FRENCH, and AFC. The impact of severe anastomotic leak on long-term survival and cancer recurrence after surgical resection for esophageal malignancy. Ann Surg. 2015;262(6):972–80.
- Fransen LFC, Berkelmans GHK, Asti E, van Berge Henegouwen MI, Berlth F, Bonavina L, Brown A, Bruns C, van Daele E, Gisbertz SS, Grimminger PP, Gutschow CA, Hannink G, Hölscher AH, Kauppi J, Lagarde SM, Mercer S, Moons J, et al. EsoBenchmark Collaborative. The effect of postoperative complications after minimally invasive esophagectomy on long-term survival: an international multicenter cohort study. Ann Surg. 2021;274(6):e1129-37.
- Kamarajah SK, Navidi M, Wahed S, Immanuel A, Hayes N, Griffin SM, Phillips AW. Anastomotic Leak Does Not Impact on Long-Term Outcomes in Esophageal Cancer Patients. Ann Surg Oncol. 2020 Jul;27(7):2414-2424. [CrossRef] [PubMed]
- Gao C, Xu G, Wang C, Wang D. Evaluation of preoperative risk factors and postoperative indicators for anastomotic leak of minimally invasive McKeown esophagectomy: a single-center retrospective analysis. J Cardiothorac Surg. 2019 Feb 28;14(1):46. [CrossRef] [PubMed]
- Shao CY, Liu KC, Li CL, Cong ZZ, Hu LW, Luo J, Diao YF, Xu Y, Ji SG, Qiang Y, Shen Y. C-reactive protein to albumin ratio is a key indicator in a predictive model for anastomosis leakage after esophagectomy: Application of classification and regression tree analysis. Thorac Cancer. 2019 Apr;10(4):728-737. [CrossRef] [PubMed]
- Lindenmann J, Fink-Neuboeck N, Porubsky C, Fediuk M, Anegg U, Kornprat P, Smolle M, Maier A, Smolle J, Smolle-Juettner FM. A nomogram illustrating the probability of anastomotic leakage following cervical esophagogastrostomy. Surg Endosc. 2021 Nov;35(11):6123-6131. [CrossRef] [PubMed]
- Zhang C, Li XK, Hu LW, Zheng C, Cong ZZ, Xu Y, Luo J, Wang GM, Gu WF, Xie K, Luo C, Shen Y. Predictive value of postoperative C-reactive protein-to-albumin ratio in anastomotic leakage after esophagectomy. J Cardiothorac Surg. 2021 May 17;16(1):133. [CrossRef] [PubMed]
- Labgaa I, Mantziari S, Genety M, Elliott JA, Kamiya S, Kalff MC, Winiker M, Pasquier J, Allemann P, Messier M, van Berge Henegouwen MI, Nilsson M, Reynolds JV, Piessen G, Hübner M, Demartines N, Schäfer M. Early postoperative decrease of albumin is an independent predictor of major complications after oncological esophagectomy: A multicenter study. J Surg Oncol. 2021 Feb;123(2):462-469. [CrossRef] [PubMed]
- Asti E, Bonitta G, Melloni M, Tornese S, Milito P, Sironi A, Costa E, Bonavina L. Utility of C-reactive protein as predictive biomarker of anastomotic leak after minimally invasive esophagectomy. Langenbecks Arch Surg. 2018 Mar;403(2):235-244 . [CrossRef] [PubMed]
- Tsujimoto H, Ono S, Takahata R, Hiraki S, Yaguchi Y, Kumano I, Matsumoto Y, Yoshida K, Aiko S, Ichikura T, Yamamoto J, Hase K. Systemic inflammatory response syndrome as a predictor of anastomotic leakage after esophagectomy. Surg Today. 2012 Jan;42(2):141-6. [CrossRef] [PubMed]
- Hoeboer SH, Groeneveld AB, Engels N, van Genderen M, Wijnhoven BP, van Bommel J. Rising C-reactive protein and procalcitonin levels precede early complications after esophagectomy. J Gastrointest Surg. 2015 Apr;19(4):613-24. [CrossRef] [PubMed]
- Gordon AC, Cross AJ, Foo EW, Roberts RH. C-reactive protein is a useful negative predictor of anastomotic leak in oesophago-gastric resection. ANZ J Surg. 2018 Mar;88(3):223-227. [CrossRef] [PubMed]
- Park JK, Kim JJ, Moon SW. C-reactive protein for the early prediction of anastomotic leak after esophagectomy in both neoadjuvant and non-neoadjuvant therapy case: a propensity score matching analysis. J Thorac Dis. 2017 Oct;9(10):3693-3702. [CrossRef] [PubMed]
- Giulini L, Dubecz A, Solymosi N, Tank J, Renz M, Thumfart L, Stein HJ. Prognostic Value of Chest-Tube Amylase Versus C-Reactive Protein as Screening Tool for Detection of Early Anastomotic Leaks After Ivor Lewis Esophagectomy. J Laparoendosc Adv Surg Tech A. 2019 Feb;29(2):192-197. [CrossRef] [PubMed]
- McAnena P, Neary C, Doyle C, Kerin MJ, McAnena OJ, Collins C. Serial CRP levels following oesophagectomy: a marker for anastomotic dehiscence. Ir J Med Sci. 2020 Feb;189(1):277-282. [CrossRef] [PubMed]
- Prochazka V, Marek F, Kunovsky L, Svaton R, Farkasova M, Potrusil M, Moravcik P, Kala Z. C-reactive protein as predictor of anastomotic complications after minimally invasive oesophagectomy. J Minim Access Surg. 2019 Jan-Mar;15(1):46-50. [CrossRef] [PubMed]
- Dutta S, Fullarton GM, Forshaw MJ, Horgan PG, McMillan DC. Persistent elevation of C-reactive protein following esophagogastric cancer resection as a predictor of postoperative surgical site infectious complications. World J Surg. 2011 May;35(5):1017-25. [CrossRef] [PubMed]
- Ji L, Wang T, Tian L, Gao M. The early diagnostic value of C-reactive protein for anastomotic leakage post radical gastrectomy for esophagogastric junction carcinoma: A retrospective study of 97 patients. Int J Surg. 2016 Mar;27:182-186. [CrossRef] [PubMed]
- Babic B, Tagkalos E, Gockel I, Corvinus F, Hadzijusufovic E, Hoppe-Lotichius M, Lang H, van der Sluis PC, Grimminger PP. C-reactive Protein Levels After Esophagectomy Are Associated With Increased Surgical Trauma and Complications. Ann Thorac Surg. 2020 May;109(5):1574-1583. [CrossRef] [PubMed]
- Neary C, McAnena P, McAnena O, Kerin M, Collins C. C-Reactive Protein-Lymphocyte Ratio Identifies Patients at Low Risk for Major Morbidity after Oesophagogastric Resection for Cancer. Dig Surg. 2020;37(6):515-523. [CrossRef] [PubMed]
- Miki Y, Toyokawa T, Kubo N, Tamura T, Sakurai K, Tanaka H, Muguruma K, Yashiro M, Hirakawa K, Ohira M. C-Reactive Protein Indicates Early Stage of Postoperative Infectious Complications in Patients Following Minimally Invasive Esophagectomy. World J Surg. 2017 Mar;41(3):796-803. [CrossRef] [PubMed]
- Stuart SK, Kuypers TJL, Martijnse IS, Heisterkamp J, Matthijsen RA. C-reactive protein and drain amylase: their utility in ruling out anastomotic leakage after minimally invasive Ivor-Lewis esophagectomy. . Scand J Gastroenterol. 2023 May;58(5):448-452. [CrossRef] [PubMed]
- Rat P, Piessen G, Vanderbeken M, Chebaro A, Facy O, Rat P, Boisson C, Ortega-Deballon P. C-reactive protein identifies patients at low risk of anastomotic leak after esophagectomy. Langenbecks Arch Surg. 2022 Dec;407(8):3377-3386. [CrossRef] [PubMed]
- Hagens ERC, Feenstra ML, Lam WC, Eshuis WJ, Lameris W, van Berge Henegouwen MI, Gisbertz SS. C-Reactive Protein as a Negative Predictive Marker for Anastomotic Leakage After Minimally Invasive Esophageal Surgery. World J Surg. 2023 Aug;47(8):1995-2002. [CrossRef] [PubMed]
- Baker EH, Hill JS, Reames MK, Symanowski J, Hurley SC, Salo JC. Drain amylase aids detection of anastomotic leak after esophagectomy. J Gastrointest Oncol. 2016 Apr;7(2):181-8. [CrossRef] [PubMed]
Figure 1.
Mean levels of Albumin, CRP, WCC and Nun score on postoperative day 2 and 4 in patients with and without AL, stratified by ECCG type of AL (data displayed as means with standard deviation). (a) Correlation between mean Alb and type of AL, (b) Correlation between mean CRP and type of AL, (c) Correlation between mean WCC and type of AL, Correlation between mean NUn and type of A.
Figure 1.
Mean levels of Albumin, CRP, WCC and Nun score on postoperative day 2 and 4 in patients with and without AL, stratified by ECCG type of AL (data displayed as means with standard deviation). (a) Correlation between mean Alb and type of AL, (b) Correlation between mean CRP and type of AL, (c) Correlation between mean WCC and type of AL, Correlation between mean NUn and type of A.
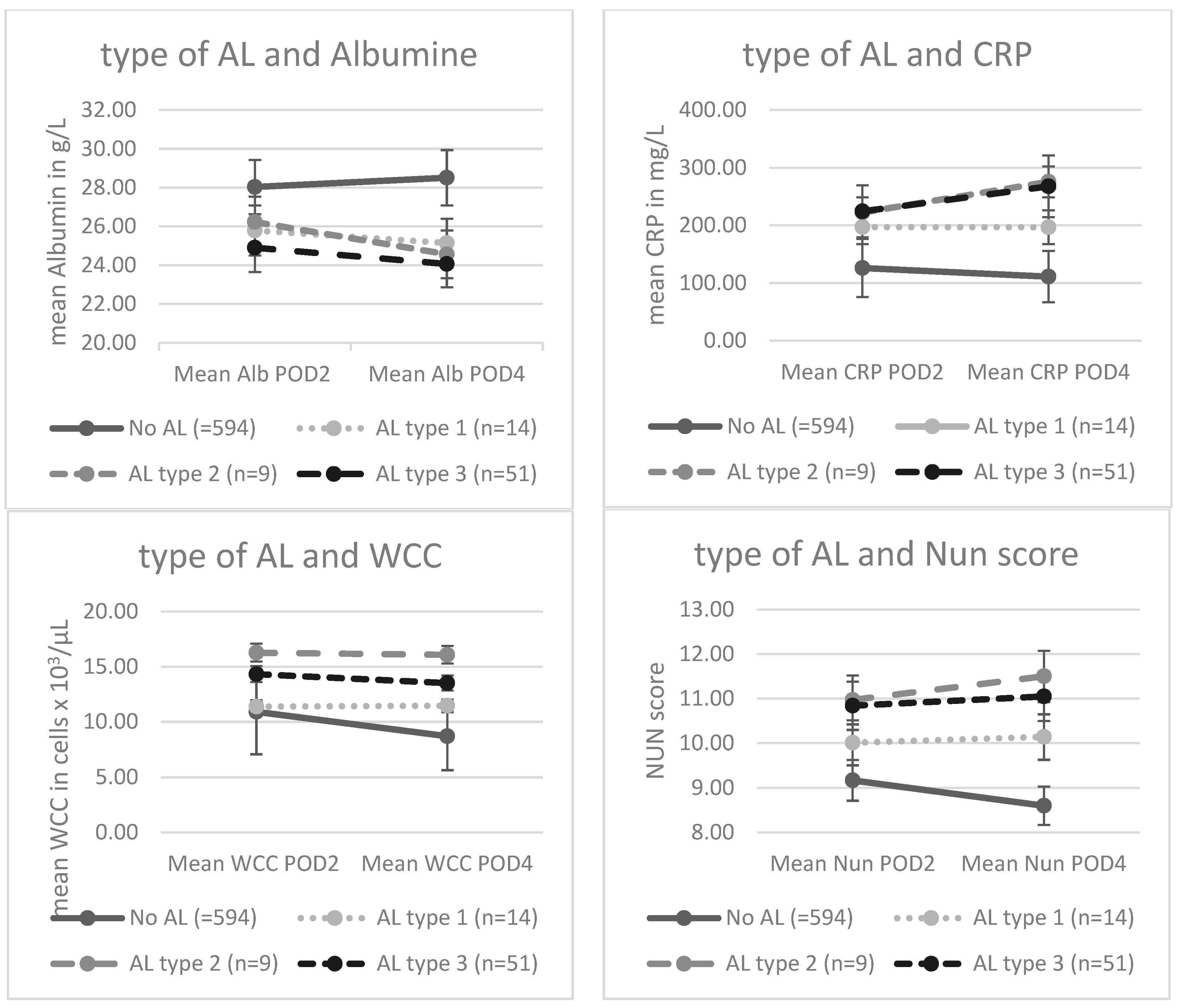
Figure 2.
Receiver operating curve (ROC) for Albumin, C-reactive protein, White cell count and the Nun score on POD2 (light gray) and POD4 (dark grey) and their diagnostic accuracy in detecting AL. (a) ROC curve for Alb, (b) ROC curve for WCC, (c) ROC curve for CRP, (a) ROC curve for the Nun score.
Figure 2.
Receiver operating curve (ROC) for Albumin, C-reactive protein, White cell count and the Nun score on POD2 (light gray) and POD4 (dark grey) and their diagnostic accuracy in detecting AL. (a) ROC curve for Alb, (b) ROC curve for WCC, (c) ROC curve for CRP, (a) ROC curve for the Nun score.
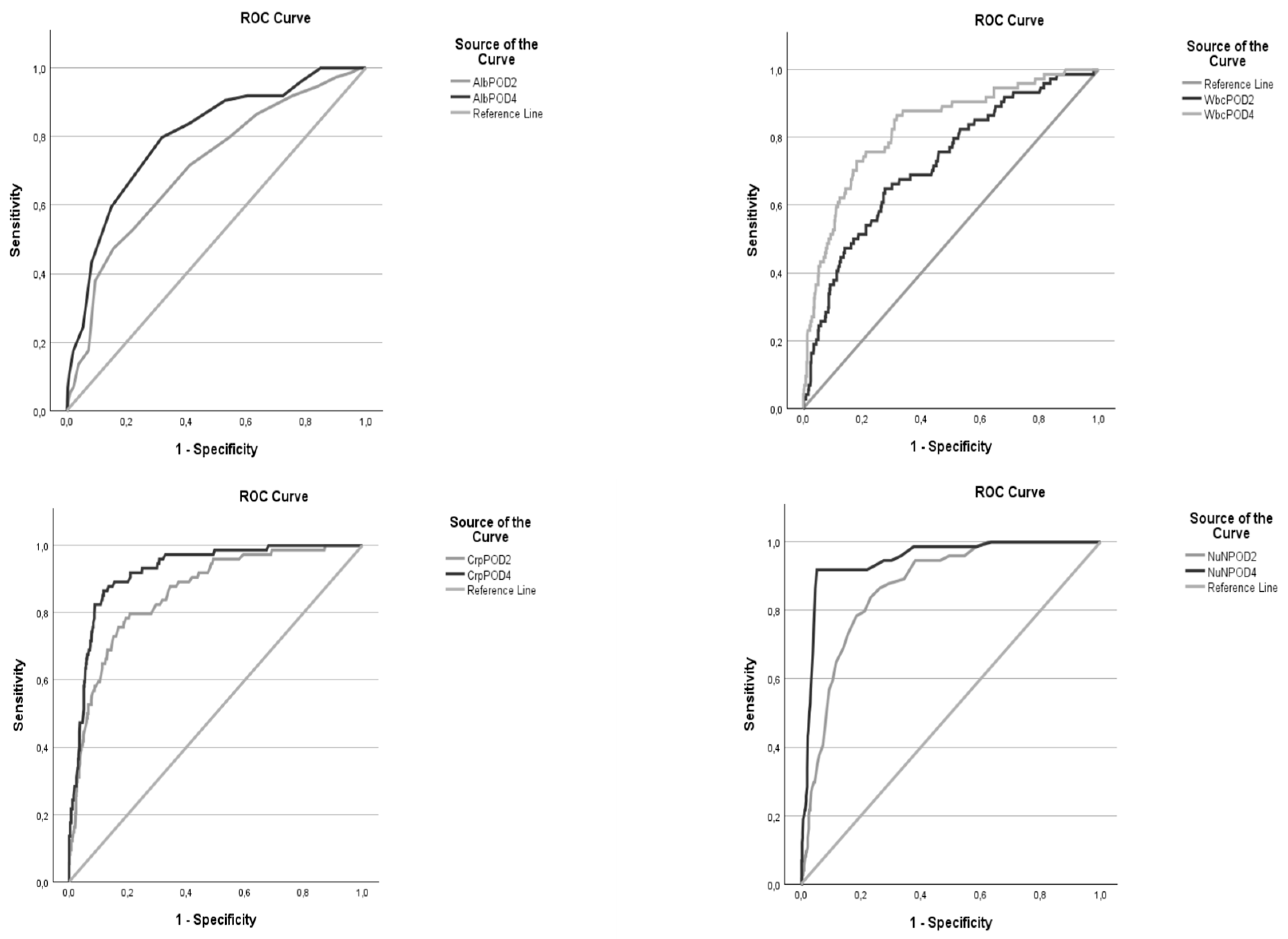

Table 1.
Baseline characteristics.
|
All patients (n= 668) |
no AL (n= 594) |
AL (n= 74) |
P value | ||
|---|---|---|---|---|---|
| Age, (y) | Mean ± SD | 64,0 ± 12,2 | 64,8 ± 10,2 | 65,6 ± 8,9 | 0,508 |
| BMI (kg/m2) | Mean ± SD | 25,3 ± 4,6 | 25,2 ± 4,5 | 25,9 ± 4,9 | 0,252 |
| ASA score, n (%) | 1 | 27 (4,0%) | 24 (4,1%) | 3 (4,1%) | 0,036 |
| 2 | 286 (42,8%) | 261 (43,9%) | 25 (33,7%) | ||
| 3 | 335 (50,1%) | 292 (49,2%) | 43 (58,1%) | ||
| 4 | 4 (0,6%) | 2 (0,3%) | 2 (2,7%) | ||
| Gender, n (%) | Male | 527 (78,9%) | 468 (78,8%) | 59 (79,7%) | 0,851 |
| Female | 141 (21,1%) | 126 (21,2%) | 15 (20,3%) | ||
| Comorbidities, n (%) | Kidney disease | 21 (3,1%) | 19 (3,2%) | 2 (2,7%) | 0,818 |
| Cardiovascular disease | 257 (38,5%) | 226 (38,0%) | 31 (41,9%) | 0,522 | |
| Pulmonary disease | 161 (24,1%) | 140 (23,6%) | 21 (28,4%) | 0,362 | |
| Diabetes | 88 (13,2%) | 75 (12,6%) | 13 (17,6%) | 0,236 | |
| Smoking | 230 (34,4%) | 200 (33,7%) | 30 (40,5%) | 0,241 | |
| Corticosteroids | 20 (3,0%) | 16 (2,7%) | 4 (5,4%) | 0,197 | |
| Tumor Location, n (%) | proximal | 17 (2,5%) | 12 (2,0%) | 5 (6,8%) | 0,094 |
| mid | 121 (18,1%) | 110 (18,5%) | 11 (14,9%) | ||
| distal | 402 (60,2%) | 357 (60,1%) | 45 (60,8%) | ||
| GEJ | 128 (19,2%) | 115 (19,4%) | 13 (17,6%) | ||
| Neoadjuvant therapy, n (%) | none | 179 (26,8%) | 158 (26,6%) | 21 (28,4%) | 0,932 |
| Chemotherapy | 97 (14,5%) | 87 (14,6%) | 10 (13,5%) | ||
| Radiochemotherapy | 392 (58,7%) | 349 (58,8%) | 43 (58,1%) | ||
| Histology, n (%) | Adeno Ca | 451 (67,5%) | 402 (67,7%) | 49 (66,2%) | 0,719 |
| Squamous cell Ca | 200 (29,9%) | 176 (29,6%) | 24 (32,4%) | ||
| Other | 17 (2,5%) | 16 (2,7%) | 1 (1,4%) | ||
| cT-stage, n (%)* | Tx | 8 (1,2%) | 7 (1,2%) | 1 (1,4%) | 0,641 |
| T1 | 56 (8,4%) | 49 (8,2%) | 7 (9,5%) | ||
| T2 | 136 (20,4%) | 118 (19,9%) | 18 (24,3%) | ||
| T3 | 455 (68,1%) | 407 (68,5%) | 48 (64,9%) | ||
| T4 | 13 (1,9%) | 13 (2,2%) | 0 (0,0%) | ||
| cN-stage, n (%)* | N0 | 227 (34,0%) | 203 (34,2%) | 24 (32,4%) | 0,898 |
| N1 | 308 (46,1%) | 276 (46,5%) | 32 (43,2%) | ||
| N2 | 112 (16,8%) | 97 (16,3%) | 15 (20,3%) | ||
| N3 | 13 (1,9%) | 11 (1,9%) | 2 (2,7%) | ||
| cM-stage, n (%)* | M0 | 625 (93,6%) | 556 (93,6%) | 69 (93,2%) | 0,989 |
| M1 | 35 (5,2%) | 31 (5,2%) | 4 (5,4%) | ||
| Procedure, n (%) | IL | 586 (87,7%) | 522 (87,9%) | 64 (86,5%) | 0,010 |
| McK | 25 (3,7%) | 18 (3,0%) | 7 (9,5%) | ||
| THE | 57 (8,5%) | 54 (9,1%) | 3 (4,1%) | ||
| Approach, n (%) | Open | 327 (49,0%) | 299 (50,3%) | 28 (37,8%) | 0,008 |
| Hybride | 139 (20,8%) | 127 (21,4%) | 12 (16,2%) | ||
| MIE | 202 (30,2%) | 168 (28,3%) | 34 (45,9%) | ||
| type of surgery, n (%) | Elective | 608 (91,0%) | 545 (91,8%) | 63 (85,1%) | <0,001 |
| Emergency | 5 (0,7%) | 1 (0,2%) | 4 (5,4%) | ||
| Salvage | 55 (8,2%) | 48 (8,1%) | 7 (9,5%) |
SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiologists; GEJ, gastro esophageal junction; IL, Ivor-Lewis; McK, McKeown; THE, transhiatal esophagectomy; * cTNM staging according to the AJCC 8th edition; Bold values state statistical significance.
Table 2.
univariate analysis of the mean biomarkers and Nun score on POD2 and 4 according to the ECCG type of AL.
Table 2.
univariate analysis of the mean biomarkers and Nun score on POD2 and 4 according to the ECCG type of AL.
| No AL (=594) | AL type 1 (n=14) | AL type 2 (n=9) | AL type 3 (n=51) | p value | |
|---|---|---|---|---|---|
| Alb POD2 (mean ± SD) | 28,0 (± 3,7) | 25,8 (± 2,6) | 26,2 (± 4,4) | 24,9 (± 4,1) | <,001 |
| Alb POD4 (mean ± SD) | 28,5 (± 3,9) | 25,1 (± 3,4) | 24,6 (± 4,0) | 24,1 (± 3,2) | <,001 |
| CRP POD2 (mean ± SD) | 125,9 (± 55,4) | 197,0 (± 89,8) | 222,3 (± 73,2) | 224,4 (± 67,9) | <,001 |
| CRP POD4 (mean ± SD) | 111,1 (± 62,8) | 196,8 (± 84,9) | 275,4 (± 86,4) | 267,6 (± 74,0) | <,001 |
| WCC POD2 (mean ± SD) | 10,9 (± 5,2) | 11,4 (± 3,6) | 16,3 (± 6,5) | 14,3 (± 4,2) | <,001 |
| WCC POD4 (mean ± SD) | 8,7 (± 2,9) | 11,46 (± 3,7) | 16,1 (± 5,7) | 13,5 (± 4,5) | <,001 |
| Nun POD2 (mean ± SD) | 9,2 (± 1,2) | 10,0 (± 0,8) | 10,9 (± 1,4) | 10,8 (± 1,0) | <,001 |
| Nun POD4 (mean ± SD) | 8,6 (± 1,0) | 10,1 (± 1,2) | 11,5 (± 0,8) | 11,1 (± 0,9) | <,001 |
Table 3.
Threshold values for Alb, CRP, WCC and the Nun score and their diagnostic accuracy for AL .
Table 3.
Threshold values for Alb, CRP, WCC and the Nun score and their diagnostic accuracy for AL .
| variable | AUC | 95% CI | p value | Cut-off | sens | spec | PPV | NPV | PLR | NLR |
|---|---|---|---|---|---|---|---|---|---|---|
| Alb POD2 | 0,710 | 0,646 - 0,774 | < 0,001 | 24,5 | 47,30% | 84,40% | 27,42% | 92,78% | 3,032 | 0,624 |
| POD4 | 0,799 | 0,746 - 0,853 | < 0,001 | 26,5 | 79,70% | 68,20% | 23,79% | 96,42% | 2,506 | 0,298 |
| CRP POD2 | 0,859 | 0,816 - 0,903 | < 0,001 | 165,5 | 79,70% | 79,30% | 32,42% | 96,90% | 3,850 | 0,256 |
| POD4 | 0,924 | 0,896 - 0,953 | < 0,001 | 181,5 | 86,50% | 88,20% | 47,73% | 98,13% | 7,330 | 0,153 |
| WCC POD2 | 0,724 | 0,662 - 0,786 | < 0,001 | 12,255 | 64,90% | 72,30% | 22,59% | 94,30% | 2,343 | 0,486 |
| POD4 | 0,829 | 0,777 - 0,880 | < 0,001 | 10,885 | 73,00% | 82,00% | 33,57% | 96,06% | 4,056 | 0,329 |
| Nun POD2 | 0,869 | 0,833 - 0,905 | < 0,001 | 9,75 | 83,80% | 76,80% | 31,03% | 97,44% | 3,612 | 0,211 |
| POD4 | 0,948 | 0,923 - 0,972 | < 0,001 | 10,05 | 91,90% | 94,70% | 68,36% | 98,95% | 17,340 | 0,086 |
AUC, area under the curve; SE, standard error; CI, confidence interval; Sen, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value; PLR, positive likelihood ratio; NLR, negative likelihood ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



