
Submitted:
03 January 2024
Posted:
05 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Severe acute respiratory syndrome coronavirus 2 infects many people, but many infected individuals do not develop symptoms. COVID-19 is an inflammatory disease that affects a portion of individuals infected with the virus, and it is associated with liver injury and other complications leading to hospitalization, critical illness, and death. Remdesivir is an antiviral agent used for treatment of hospitalized patients with COVID-19 to improve time to recovery, reduce duration of mechanical ventilation, decrease the need for supplemental oxygen, and decrease the risk of mortality. Remdesivir-associated hepatotoxicity has been observed as increased transaminases more than 5 times the upper limit of normal in hospitalized patients with COVID-19 but causality has not been proven. It is generally difficult to distinguish between remdesivir-associated hepatotoxicity and COVID-19-induced hepatotoxicity. The purpose of this review is to evaluate the evidence for remdesivir-associated hepatotoxicity. Current evidence suggests that elevated liver enzymes in hospitalized COVID-19 patients are more likely to be due to the infection than remdesivir and that a 5-day course of remdesivir seems to be safe in regards to hepatotoxicity.
Keywords:
COVID-19
; GS-5734
; hepatotoxicity
; liver
; remdesivir
; SARS-CoV-2
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel betacoronavirus that causes coronavirus disease 2019 (COVID-19), which has rapidly spread worldwide, prompting the World Health Organization (WHO) to declare it a pandemic on March 11, 2020 [1,2]. While 33% to 40% of infected individuals are acutely asymptomatic, symptomatic patients may develop flu-like symptoms and in severe cases develop pneumonia requiring hospitalization and respiratory support [1,3,4,5,6,7,8,9,10,11,12,13,14]. The most common complications of severe illness include acute respiratory distress syndrome (20-67%), arrhythmia (17-18%), acute cardiac injury (7-23%), shock (6-10%), acute kidney injury (3-29%), hepatic dysfunction (1-33%), and disseminated intravascular coagulation (1%) [1,3,4,5,8,9,15,16,17]. About 15% to 65% of patients with severe COVID-19 display signs of hepatobiliary damage [18].
By binding to angiotensin-converting enzyme 2 (ACE2) on the surface of cholangiocytes, SARS-CoV-2 may directly damage the biliary ducts [19]. However, given the low number of ACE2 receptors on hepatocyte surfaces, any injury to the hepatocytes may be indirect, which is supported by the fact that the majority of patients have normal alkaline phosphatase [19,20]. In addition, hepatocyte injury is more common than cholangiocyte injury [20]. Systemic inflammation, cytokine storm, and pneumonia-associated hypoxia might contribute to hepatocyte injury, especially in critically ill patients. Data from retrospective observational studies evaluating hepatic injury in patients with COVID-19 suggest that the pattern of liver injury is predominantly hepatocellular rather than cholestatic [21]. Abnormal liver enzymes are typically only minimally elevated (1-2 times the upper limit of normal) [18,21]. Therefore, it is important to monitor COVID-19 patients’ liver enzymes and manage drug-induced hepatotoxicity to avoid further injury to the liver. The objective of this review article is to evaluate and summarize the evidence for remdesivir-associated hepatotoxicity in patients with COVID-19, using elevated liver enzymes more than 5 times the upper limit of normal as the cut-off to distinguish between liver adaptation and clinically significant liver injury [22].
2. Materials and Methods
We searched PubMed and EMBASE from inception through November 2023 using keyword terms remdesivir, hepatotoxicity, COVID-19, and SARS-CoV-2. References of selected articles were also screened for additional studies. Studies evaluating the efficacy and safety of remdesivir for treatment of COVID-19 published in the English language are evaluated. Hepatotoxicity was defined as elevation of aspartate aminotransferase (AST) or alanine aminotransferase (ALT) more than 5 times the upper limit of normal [23]. Per American College of Gastroenterology guidelines for evaluation of abnormal liver chemistries, a normal ALT level is considered to range from 29 to 33 IU/L for males and 19 to 25 IU/L for females [24]. Levels above these thresholds warrant further evaluation.
3. Results
3.1. Remdesivir’ s role in treatment of COVID-19 in Hospitalized Patients
Initially developed for the treatment of Ebola, remdesivir is a nucleotide analog with a broad-spectrum of viral activity [25,26]. Remdesivir inhibits viral replication of SARS-CoV-2 by incorporating its active metabolite into viral RNA resulting in chain termination [27]. Remdesivir is administered to hospitalized adult patients intravenously over 30 minutes at a typical dose of 200 mg on day 1 followed by 100 mg once daily on days 2 onward for a total of 5 to 10 days [25,27]. Remdesivir is approved by the U.S. Food and Drug Administration for adults and pediatric patients 28 days of age and older and weighing at least 3 kg for the treatment of COVID-19 requiring hospitalization (also approved for non-hospitalized patients who have mild-to-moderate COVID-19 and are at high risk for progression to severe COVID-19, including hospitalization or death). While many randomized clinical trials have failed to show a clear mortality benefit with remdesivir, the primary benefit of treatment with remdesivir seems to be improved time to recovery, reduced duration of mechanical ventilation, decreased need for supplemental oxygen, and increased rate of hospital discharge [28,29,30,31,32,33,34]. Moreover, the final results of ACCT-1 and WHO Solidarity randomized clinical trials suggest that remdesivir offers no substantial benefit to ventilated COVID-19 patients, but aids in reducing death or the need for ventilation in other hospital cases, especially in patients requiring low-flow supplemental oxygen [30,35,36]. Additionally, multiple observational studies, but not all, have shown an association with remdesivir use in hospitalized patients and reduced mortality [33,34,37,38,39,40,41,42,43,44,45]. Finally, a systematic review and individual patient data meta-analysis of eight randomized clinical trials (RCTs) consisting of 10,480 patients hospitalized with COVID-19 found a significant reduction in mortality with remdesivir use compared to non-use (OR 0.88; 95% CI, 0.78 to 1.00; p=0.045) [36]. However, the results were significant only for a subgroup of patients on low-flow oxygen or no oxygen (OR 0.80; 95% CI, 0.70 to 0.93; pinteraction=0.019) but not for those on high-flow oxygen or ventilated (OR 1.10; 95% CI, 0.88 to 1.38).
Although there were disagreements between various clinical practice guidelines initially regarding the use of remdesivir, the current guidelines are generally in agreement. As of January 2023, the WHO recommends the use of remdesivir in hospitalized patients with severe COVID-19 but recommends against its use in patients with critical COVID-19 [46]. As of February 2022, the Infectious Diseases Society of America (IDSA) guidelines recommend the use of remdesivir in hospitalized patients requiring supplemental oxygen but not on mechanical ventilation or extracorporeal membrane oxygenation (ECMO) [47]. As of October 2023, the National Institute of Health (NIH) guidelines recommend its use in hospitalized patients requiring low-flow supplemental oxygen, high-flow oxygen, or noninvasive ventilation but not in those on mechanical ventilation or ECMO [48]. Additionally, the NIH guidelines recommend remdesivir for hospitalized patients who do not require supplemental oxygen if they are immunocompromised or are at high risk of progressing to severe disease [48]. For patients with liver disease or liver transplant recipients, American Association for the Study of Liver Diseases (AASLD) recommends a 5-day course of remdesivir in hospitalized COVID-19 patients requiring supplemental oxygen [49].
3.2. Remdesivir-Associated Hepatotoxicity
The mechanism of remdesivir-induced hepatotoxicity is not fully understood [50]. As an ester prodrug, remdesivir is hydrolyzed by carboxylesterase-1 to its active metabolite [51]. Additionally, remdesivir is a potent inhibitor of carboxylesterase-2, an enzyme that metabolizes many drugs and toxicans, which may result in toxicity [51,52]. It has been shown on a cellular level that remdesivir can be toxic to human hepatocytes, although the exact mechanism is unknown [53]. In a phase 1 randomized, placebo-controlled clinical trial of healthy volunteers, mild (grade 1) to moderate (grade 2) elevation of ALT was observed in individuals receiving 10 days of remdesivir, which resolved upon discontinuation of remdesivir. As a result, there is a warning listed in remdesivir prescribing information, and both the prescribing information and AASLD recommend considering remdesivir discontinuation if ALT levels increase to greater than 10 times the upper limit of normal and to discontinue remdesivir if ALT elevation is accompanied by signs or symptoms of liver inflammation [49].
The safety profile of remdesivir has been evaluated in multiple studies, including clinical trials, observational studies, and descriptive case reports and case series (Table 1). Prior to COVID-19, a clinical trial investigating remdesivir for treatment of Ebola did not report any severe hepatotoxicity [54]. Since COVID-19 pandemic began, Grein and colleagues reported the first compassionate use of remdesivir in 61 hospitalized patients with severe COVID-19 [55]. Increased hepatic enzymes occurred in 23% of the patients, which were mild to moderate. Antinori and colleagues reported even higher rates of hypertransaminasemia (43%), including in both intensive care unit (ICU) and non-ICU patients [56]. Reports of compassionate remdesivir use by Burwick and colleagues had similar findings [57]. Leegwater and colleagues reported a case of increased liver enzymes 5 days after start of remdesivir, resulting in discontinuation of remdesivir [53]. However, this patient also received amiodarone and chloroquine, both of which are inhibitors of P-glycoprotein with very long half-lives. Since remdesivir is a substrate of P-glycoprotein, inhibitors of P-glycoprotein may reduce efflux rate of remdesivir leading to increased concentrations of remdesivir in the hepatocytes above the toxic threshold [53]. Zampino and colleagues reported a case series of 5 patients in the ICU receiving remdesivir for 10 days demonstrating increases in bilirubin and liver enzymes, suggesting liver injury [58]. However, these patients were also receiving hydroxychloroquine and it is not clear if the liver injury was due to remdesivir, hydroxychloroquine, or the combination.
A pharmacovigilance analysis conducted by Montastruc and colleagues found 387 reports with remdesivir [59]. Hepatic adverse effects were reported in 34% of patients, mostly increased liver enzymes (88%) with a median time to onset of 5.4 days. Compared to other drugs prescribed for COVID-19, remdesivir was associated with increased risk of reporting hepatic disorders (OR 1.94; 95% CI, 1.54 to 2.45). The severity of these hepatic disorders was not reported. Van Laar and colleagues conducted a retrospective single-center observational study evaluating 103 hospitalized patients with COVID-19 who received remdesivir [60]. In patients with normal AST and ALT at baseline, AST and ALT were increased mildly (grade 1) in 39% and 35% of patients, and grade 2 increases were observed in 3% and 6% of patients, respectively. Only one patient had grade 3 increases in AST and ALT (grade 3 is defined as elevation >5 times the upper limit of normal). The investigators found that patients who met the contraindication criteria to remdesivir due to liver impairment were not more likely to develop hepatotoxicity when receiving remdesivir treatment. Garibaldi and colleagues conducted a retrospective multicenter observational study comparing 285 patients who received remdesivir to 285 propensity score-matched control patients, all hospitalized with COVID-19 [34]. The rate of increased ALT or AST was equal between remdesivir (10.2%) and control (10.2%) groups. Increased bilirubin was higher in the control group (6.0%) compared to remdesivir group (3.5%). Only four patients stopped remdesivir early due to increased levels of liver enzyme or bilirubin. It is important to note that none of these studies utilized the full Drug-Induced Liver Injury Network (DILIN) criteria to identify drug-induced liver injury nor the widely used Roussel Uclaf Causality Assessment Method (RUCAM) to assess causality [23,63]. Therefore, these studies could not establish causality of drug-induced liver injury due to remdesivir.
Given the observational nature of these studies, it was difficult to attribute hepatotoxicity to either remdesivir or the COVID-19. Wang and colleagues conducted a randomized, double-blind, placebo-controlled, multicenter trial, enrolling enrolled 236 hospitalized adult patients with severe COVID-19 pneumonia [28]. They excluded patients with cirrhosis, ALT or AST more than 5 times the upper limit of normal. About 66% of patients received corticosteroid therapy concurrently. Increased total bilirubin rate was the same in remdesivir (10%) and placebo (9%) groups with only one grade 3 case in remdesivir group, but the rate of elevated AST was actually lower in remdesivir (5%) group compared to placebo (12%), none of which were grade 3 or higher in severity. Changes in ALT were not reported. Only 2 patients discontinued treatment due to increased liver enzymes, both in the remdesivir group. More patients in the placebo group were receiving invasive mechanical ventilation compared to remdesivir group, which might explain the higher rate of ALT elevation in this group due to higher severity of COVID-19. In the SIMPLE-1 Severe trial, Goldman and colleagues conducted a randomized, open-label, multicenter trial to evaluate 5 days vs 10 days of remdesivir [61]. The study excluded patients with ALT or AST more than 5 times the upper limit of normal. It is not clear what percentage of patients received corticosteroids. The preliminary results including 397 hospitalized patients with severe COVID-19 pneumonia showed similar rates of increased ALT with remdesivir for 5 days (6%) compared to 10 days (8%), although fewer patients in the 5-day group discontinued remdesivir due to increased liver enzymes compared to 10-day group (2.5% vs 3.6%). Again, it was not clear whether increased liver enzymes were due to severity of COVID-19 or duration of remdesivir as more patients in the 10-day group were receiving high-flow oxygen, mechanical ventilation, or ECMO.
In SIMPLE-2 Moderate trial, Spinner and colleagues conducted a randomized, open-label, multicenter trial to 5 days vs 10 days of remdesivir in 584 hospitalized patients with moderate COVID-19, which excluded patients with AST or ALT more than 5 times the upper limit of normal [29]. The study also included a third group that received the standard of care without remdesivir. About 17% of patients received corticosteroids concomitantly. The rate of increased ALT more than 5 times the upper limit of normal was similar between 10-day and 5-day groups, and slightly higher in the standard of care group (3%, 2%, and 8%, respectively). These results suggest that even in moderate COVID-19, patients not receiving remdesivir are likely to have elevated liver enzymes. In ACTT-1 trial, Beigel and colleagues conducted a double-blind, randomized, placebo-controlled trial enrolling 1062 hospitalized patients with moderate (15%) or severe (85%) COVID-19 [30]. Patients with ALT or AST more than 5 times the upper limit of normal at baseline were excluded. About 23% of patients also received corticosteroids. The rate of increased liver enzymes was numerically lower in the remdesivir (6.0%) compared to placebo group (10.7%), including grade 3 or higher nonserious elevations of AST or ALT (4.1% in remdesivir and 5.9% in placebo group).
Moreover, in the ACTT-2 trial, Kalil and colleagues conducted a double-blind, randomized, placebo-controlled trial to evaluate combination of baricitinib and remdesivir vs remdesivir plus placebo [62]. They enrolled 1033 hospitalized adult patients with COVID-19, excluding those with AST or ALT more than 5 times the upper limit of normal. About 12% of patients received concurrent corticosteroids. The rate of increased ALT was similar between the combination of remdesivir plus baricitinib (0.8%) and remdesivir alone (0.6%). Finally, in the DisCoVeRy trial, Ader and colleagues conducted an open-label, multicenter, randomized clinical trial to evaluate 5 to 10 days of remdesivir plus standard of care compared to standard of care alone in 857 hospitalized adult patients with COVID-19 [32]. Patients with elevated liver enzymes at baseline were excluded and about 40% of patients also received concomitant corticosteroid therapy. Transaminases were increased in 3% and 1% of remdesivir and control groups, respectively. AST and ALT increases were not reported separately. Collectively, these clinical trials suggest that remdesivir is unlikely to be the cause of elevated liver enzymes, which is more likely to be due to COVID-19 itself. Moreover, the lower rate of ALT elevation seen in the remdesivir groups compared to control groups in the study by Wang and colleagues, SIMPLE-2, and ACTT-1 (Figure 1), may suggest that the antiviral activity of remdesivir can indirectly reduce COVID-19-associated elevated liver enzymes. Interestingly, some evidence suggests that concomitant administration of systemic corticosteroids, specifically dexamethasone, may alleviate elevation of serum AST and ALT levels compared to remdesivir administration without corticosteroids [64]. Most remdesivir studies were conducted before systemic corticosteroids became the standard of care for hospitalized patients requiring supplemental oxygen [65].
A systematic review and meta-analysis (SR-MA) of four RCTs conducted by Shrestha and colleagues found that compared to placebo, remdesivir recipients had similar rates of overall adverse events (OR 1.10; 95% CI, 0.70 to 1.72; I2 74%) but significantly lower rates of severe adverse effects (OR 0.69; 95% CI, 0.54 to 0.88; I2 0%) [66]. Compared to 5 days of remdesivir treatment, those who received 10 days of remdesivir had significantly higher rates of serious adverse effects (OR 1.77; 95% CI, 1.19 to 2.65; I2 20%), although the rates of overall adverse effects were not significantly different (OR 1.26; 95% CI, 0.93 to 1.69; I2 0%). Similar results were reported in a systematic review and network meta-analyses of five RCTs conducted by Lai and colleagues, a SR-MA of five RCTs by Santenna and colleagues, and a systematic review and individual patient data meta-analysis of eight RCTs [36,67,68]. However, hepatotoxicity specifically was not analyzed in these studies. Nevertheless, another meta-analysis of three RCTs conducted by Chen and colleagues found no statistically significant increase in AST (OR 0.74; 95% CI, 0.46 to 1.18; I2 39%), ALT (OR 0.79; 95% CI, 0.56 to 1.11; I2 0%), or death (OR 0.95; 95% CI, 0.48 to 1.90; I2 0%) in patients receiving remdesivir compared to the control group [69]. Overall, the evidence suggests that a 5-day course of remdesivir seems to be safe in patients with COVID-19 in regards to hepatotoxicity and may even reduce the rate of COVID-19-associated liver enzymes elevation. High vigilance is needed to avoid concomitant use of remdesivir and P-glycoprotein inhibitors (e.g., amiodarone, carvedilol, clarithromycin, propranolol, tacrolimus, etc.) [70]. In the rare event of acute liver failure, the use of acetylcysteine has been reported to be of potential benefit [71].
4. Conclusions
Many individuals infected with SARS-CoV-2 are asymptomatic and the majority do not develop severe disease requiring hospitalization, but some individuals may develop disease that can progress in severity leading to complications, including liver injury, organ failure, and death [13,14]. Remdesivir is an antiviral agent used for treatment of hospitalized patients with COVID-19 to improve time to recovery, reduce duration of mechanical ventilation, decrease the need for supplemental oxygen, and reduce the risk of mortality (remdesivir is also approved for non-hospitalized patients who have mild-to-moderate COVID-19 and are at high risk for progression to severe COVID-19, including hospitalization or death). Remdesivir has been associated with liver injury due to reports of increased transaminases in patients who received this treatment resulting in a warning in the prescribing information and a requirement for monitoring of hepatic function before initiation and during remdesivir therapy. However, causality has not been proven. It is generally difficult to distinguish between remdesivir-associated hepatotoxicity and COVID-19-induced hepatotoxicity. Current evidence suggests that elevated liver enzymes are more likely to be due to COVID-19 and that a 5-day course of remdesivir seems to be safe in regards to hepatotoxicity.
Author Contributions
A.F. and M.M. contributed equally to conceptualization, methodology, investigation, resources, data curation, writing—original draft preparation, and writing—review and editing; supervision, A.F. All authors have read and agreed to the published version of the manuscript.
Funding
There is no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huang, C.; Wang, Y.; Li, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. World Health Organization. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020. Published 2020. Accessed 30 March 2020.
- Chen, N.; Zhou, M.; Dong, X.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020. [CrossRef] [PubMed]
- Tian, S.; Hu, N.; Lou, J.; et al. Characteristics of COVID-19 infection in Beijing. J Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Ong, S.W.X.; Kalimuddin, S.; et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA. 2020. [CrossRef]
- Lian, J.; Jin, X.; Hao, S.; et al. Analysis of Epidemiological and Clinical features in older patients with Corona Virus Disease 2019 (COVID-19) out of Wuhan. Clin Infect Dis. 2020. [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA internal medicine. 2020. [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; et al. Covid-19 in Critically Ill Patients in the Seattle Region - Case Series. N Engl J Med. 2020. [CrossRef]
- Oran, D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic : A Systematic Review. Ann Intern Med. 2021, 174, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Angulo, F.J.; Finelli, L.; Swerdlow, D.L. Estimation of US SARS-CoV-2 Infections, Symptomatic Infections, Hospitalizations, and Deaths Using Seroprevalence Surveys. JAMA Netw Open. 2021, 4, e2033706. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020. [CrossRef]
- Cao, J.; Hu, X.; Cheng, W.; Yu, L.; Tu, W.J.; Liu, Q. Clinical features and short-term outcomes of 18 patients with corona virus disease 2019 in intensive care unit. Intensive Care Med. 2020. [CrossRef]
- Cao, J.; Tu, W.J.; Cheng, W.; et al. Clinical Features and Short-term Outcomes of 102 Patients with Corona Virus Disease 2019 in Wuhan, China. Clin Infect Dis. 2020. [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt ASt, et al. COVID-19 and liver disease: mechanistic and clinical perspectives. Nat Rev Gastroenterol Hepatol. 2021, 18, 348–364. [CrossRef]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and the liver. J Hepatol. 2020, 73, 1231–1240. [Google Scholar] [CrossRef]
- Praveen, S.; Ashish, K.; Anikhindi, S.A.; et al. Effect of COVID-19 on pre-existing liver disease: What Hepatologist should know? J Clin Exp Hepatol. 2020. [CrossRef]
- Hundt, M.A.; Deng, Y.; Ciarleglio, M.M.; Nathanson, M.H.; Lim, J.K. Abnormal Liver Tests in COVID-19: A Retrospective Observational Cohort Study of 1,827 Patients in a Major U.S. Hospital Network. Hepatology. 2020, 72, 1169–1176. [Google Scholar] [CrossRef]
- Andrade, R.J.; Chalasani, N.; Bjornsson, E.S.; et al. Drug-induced liver injury. Nat Rev Dis Primers. 2019, 5, 58. [Google Scholar] [CrossRef]
- Chalasani, N.; Fontana, R.J.; Bonkovsky, H.L.; et al. Causes, clinical features, and outcomes from a prospective study of drug-induced liver injury in the United States. Gastroenterology. 2008, 135, 1924–1934. [Google Scholar] [CrossRef] [PubMed]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am J Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. Remdesivir: First Approval. Drugs. 2020, 80, 1355–1363. [Google Scholar] [CrossRef]
- Jorgensen, S.C.J.; Kebriaei, R.; Dresser, L.D. Remdesivir: Review of Pharmacology, Pre-clinical Data, and Emerging Clinical Experience for COVID-19. Pharmacotherapy. 2020, 40, 659–671. [Google Scholar] [CrossRef]
- Aleissa, M.M.; Silverman, E.A.; Paredes Acosta, L.M.; Nutt, C.T.; Richterman, A.; Marty, F.M. New Perspectives on Antimicrobial Agents: Remdesivir Treatment for COVID-19. Antimicrob Agents Chemother. 2020, 65. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate COVID-19: A Randomized Clinical Trial. JAMA. 2020, 324, 1048–1057. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Consortium WHOST, Pan, H.; Peto, R.; et al. Repurposed Antiviral Drugs for Covid-19 - Interim WHO Solidarity Trial Results. N Engl J Med. 2021, 384, 497–511. [CrossRef]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): a phase 3, randomised, controlled, open-label trial. Lancet Infect Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Lapadula, G.; Bernasconi, D.P.; Bellani, G.; et al. Remdesivir Use in Patients Requiring Mechanical Ventilation due to COVID-19. Open Forum Infect Dis. 2020, 7, ofaa481. [Google Scholar] [CrossRef] [PubMed]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; et al. Comparison of Time to Clinical Improvement With vs Without Remdesivir Treatment in Hospitalized Patients With COVID-19. JAMA Netw Open. 2021, 4, e213071. [Google Scholar] [CrossRef] [PubMed]
- Consortium WHOST. Remdesivir and three other drugs for hospitalised patients with COVID-19: final results of the WHO Solidarity randomised trial and updated meta-analyses. Lancet. 2022, 399, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, A.; Speich, B.; Mentre, F.; et al. Effects of remdesivir in patients hospitalised with COVID-19: a systematic review and individual patient data meta-analysis of randomised controlled trials. Lancet Respir Med. 2023, 11, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, Z.; Montalti, R.; Temperoni, C.; et al. Effectiveness of remdesivir in patients with COVID-19 under mechanical ventilation in an Italian ICU. J Antimicrob Chemother. 2020, 75, 3359–3365. [Google Scholar] [CrossRef] [PubMed]
- Olender, S.A.; Perez, K.K.; Go, A.S.; et al. Remdesivir for Severe Coronavirus Disease 2019 (COVID-19) Versus a Cohort Receiving Standard of Care. Clin Infect Dis. 2021, 73, e4166–e4174. [Google Scholar] [CrossRef] [PubMed]
- Olender, S.A.; Walunas, T.L.; Martinez, E.; et al. Remdesivir Versus Standard-of-Care for Severe Coronavirus Disease 2019 Infection: An Analysis of 28-Day Mortality. Open Forum Infect Dis. 2021, 8, ofab278. [Google Scholar] [CrossRef] [PubMed]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; et al. Real-World Effectiveness of Remdesivir in Adults Hospitalized With Coronavirus Disease 2019 (COVID-19): A Retrospective, Multicenter Comparative Effectiveness Study. Clin Infect Dis. 2022, 75, e516–e524. [Google Scholar] [CrossRef]
- Benfield, T.; Bodilsen, J.; Brieghel, C.; et al. Improved Survival Among Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) Treated With Remdesivir and Dexamethasone. A Nationwide Population-Based Cohort Study. Clin Infect Dis. 2021, 73, 2031–2036. [Google Scholar] [CrossRef]
- Dunay, M.A.; McClain, S.L.; Holloway, R.L.; et al. Pre-Hospital Administration of Remdesivir During a Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Outbreak in a Skilled Nursing Facility. Clin Infect Dis. 2022, 74, 1476–1479. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Alonso, R.; Camon, A.M.; et al. Impact of remdesivir according to the pre-admission symptom duration in patients with COVID-19. J Antimicrob Chemother. 2021, 76, 3296–3302. [Google Scholar] [CrossRef] [PubMed]
- Metchurtchlishvili, R.; Chkhartishvili, N.; Abutidze, A.; et al. Effect of remdesivir on mortality and the need for mechanical ventilation among hospitalized patients with COVID-19: real-world data from a resource-limited country. Int J Infect Dis. 2023, 129, 63–69. [Google Scholar] [CrossRef]
- Margalit, I.; Tiseo, G.; Ripa, M.; et al. Real-life experience with remdesivir for treatment of COVID-19 among older adults: a multicentre retrospective study. J Antimicrob Chemother. 2023, 78, 1505–1509. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics and COVID-19: living guideline, 13 J anuary 2023. Geneva: World Health Organization; 2023 (WHO/2019-nCoV/therapeutics/2023.1). Lic ence: CC BY-NC-SA 3.0 IGO.
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin Infect Dis. 2022. [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines.nih.gov/.
- Fix, O.K.; Hameed, B.; Fontana, R.J.; et al. AASLD Expert Panel Consensus Statement: COVID-19 Clinical Best Practice Advice for Hepatology and Liver Transplant Providers. 2022:1-12. https://www.aasld.org/sites/default/files/2022-10/AASLD%20COVID-19%20Guidance%20Document%2010.06.2022F.pdf. Published 2022/10/06.
- Fan, Q.; Zhang, B.; Ma, J.; Zhang, S. Safety profile of the antiviral drug remdesivir: An update. Biomed Pharmacother. 2020, 130, 110532. [Google Scholar] [CrossRef]
- Shen, Y.; Eades, W.; Yan, B. Remdesivir potently inhibits carboxylesterase-2 through covalent modifications: signifying strong drug-drug interactions. Fundam Clin Pharmacol. 2021, 35, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zou, L.; Jin, Q.; Hou, J.; Ge, G.; Yang, L. Human carboxylesterases: a comprehensive review. Acta Pharm Sin B. 2018, 8, 699–712. [Google Scholar] [CrossRef]
- Leegwater, E.; Strik, A.; Wilms, E.B.; et al. Drug-induced Liver Injury in a Patient With Coronavirus Disease 2019: Potential Interaction of Remdesivir With P-Glycoprotein Inhibitors. Clin Infect Dis. 2021, 72, 1256–1258. [Google Scholar] [CrossRef]
- Mulangu, S.; Dodd, L.E.; Davey, R.T., Jr.; et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N Engl J Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N Engl J Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Antinori, S.; Cossu, M.V.; Ridolfo, A.L.; et al. Compassionate remdesivir treatment of severe Covid-19 pneumonia in intensive care unit (ICU) and Non-ICU patients: Clinical outcome and differences in post-treatment hospitalisation status. Pharmacol Res. 1048. [Google Scholar] [CrossRef]
- Burwick, R.M.; Yawetz, S.; Stephenson, K.E.; et al. Compassionate Use of Remdesivir in Pregnant Women with Severe Covid-19. Clin Infect Dis. 2020. [CrossRef]
- Zampino, R.; Mele, F.; Florio, L.L.; et al. Liver injury in remdesivir-treated COVID-19 patients. Hepatol Int. 2020, 14, 881–883. [Google Scholar] [CrossRef] [PubMed]
- Montastruc, F.; Thuriot, S.; Durrieu, G. Hepatic Disorders With the Use of Remdesivir for Coronavirus 2019. Clin Gastroenterol Hepatol. 2020, 18, 2835–2836. [Google Scholar] [CrossRef]
- van Laar, S.A.; de Boer, M.G.J.; Gombert-Handoko, K.B.; Guchelaar, H.J.; Zwaveling, J.; group LU-C-r. Liver and kidney function in patients with Covid-19 treated with remdesivir. Br J Clin Pharmacol. 2021. [CrossRef]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N Engl J Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Danan, G.; Teschke, R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int J Mol Sci. 2015, 17. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Stern, S.; Heil, E.L.; et al. Dexamethasone mitigates remdesivir-induced liver toxicity in human primary hepatocytes and COVID-19 patients. Hepatol Commun. 2023, 7, e0034. [Google Scholar] [CrossRef]
- FakhriRavari, A.; Jin, S.; Kachouei, F.H.; Le, D.; Lopez, M. Systemic corticosteroids for management of COVID-19: Saving lives or causing harm? Int J Immunopathol Pharmacol. 2021, 35, 20587384211063976. [Google Scholar] [CrossRef]
- Shrestha, D.B.; Budhathoki, P.; Syed, N.I.; Rawal, E.; Raut, S.; Khadka, S. Remdesivir: A potential game-changer or just a myth? A systematic review and meta-analysis. Life Sci. 2021, 264, 118663. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Chen, C.H.; Wang, C.Y.; Chen, K.H.; Wang, Y.H.; Hsueh, P.R. Clinical efficacy and safety of remdesivir in patients with COVID-19: a systematic review and network meta-analysis of randomized controlled trials. J Antimicrob Chemother. 2021, 76, 1962–1968. [Google Scholar] [CrossRef] [PubMed]
- Santenna, C.; Vidyasagar, K.; Amarneni, K.C.; et al. The safety, tolerability and mortality reduction efficacy of remdesivir; based on randomized clinical trials, observational and case studies reported safety outcomes: an updated systematic review and meta-analysis. Ther Adv Drug Saf. 2021, 12, 20420986211042517. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.L.; Chao, C.M.; Lai, C.C. The safety of remdesivir for COVID-19 patients. J Med Virol. 2021, 93, 1910–1912. [Google Scholar] [CrossRef] [PubMed]
- Inhibitors and inducers of CYP enzymes and P-glycoprotein. Med Lett Drugs Ther. 2017, 59, e56.
- Carothers, C.; Birrer, K.; Vo, M. Acetylcysteine for the Treatment of Suspected Remdesivir-Associated Acute Liver Failure in COVID-19: A Case Series. Pharmacotherapy. 2020, 40, 1166–1171. [Google Scholar] [CrossRef]
Figure 1.
Rates of Increased AST and ALT in Randomized Clinical Trials. * Intervention group received 10 days of remdesivir, and control group received 5 days of remdesivir. ** Intervention group received remdesivir plus baricitinib and control group received remdesivir plus placebo.
Figure 1.
Rates of Increased AST and ALT in Randomized Clinical Trials. * Intervention group received 10 days of remdesivir, and control group received 5 days of remdesivir. ** Intervention group received remdesivir plus baricitinib and control group received remdesivir plus placebo.
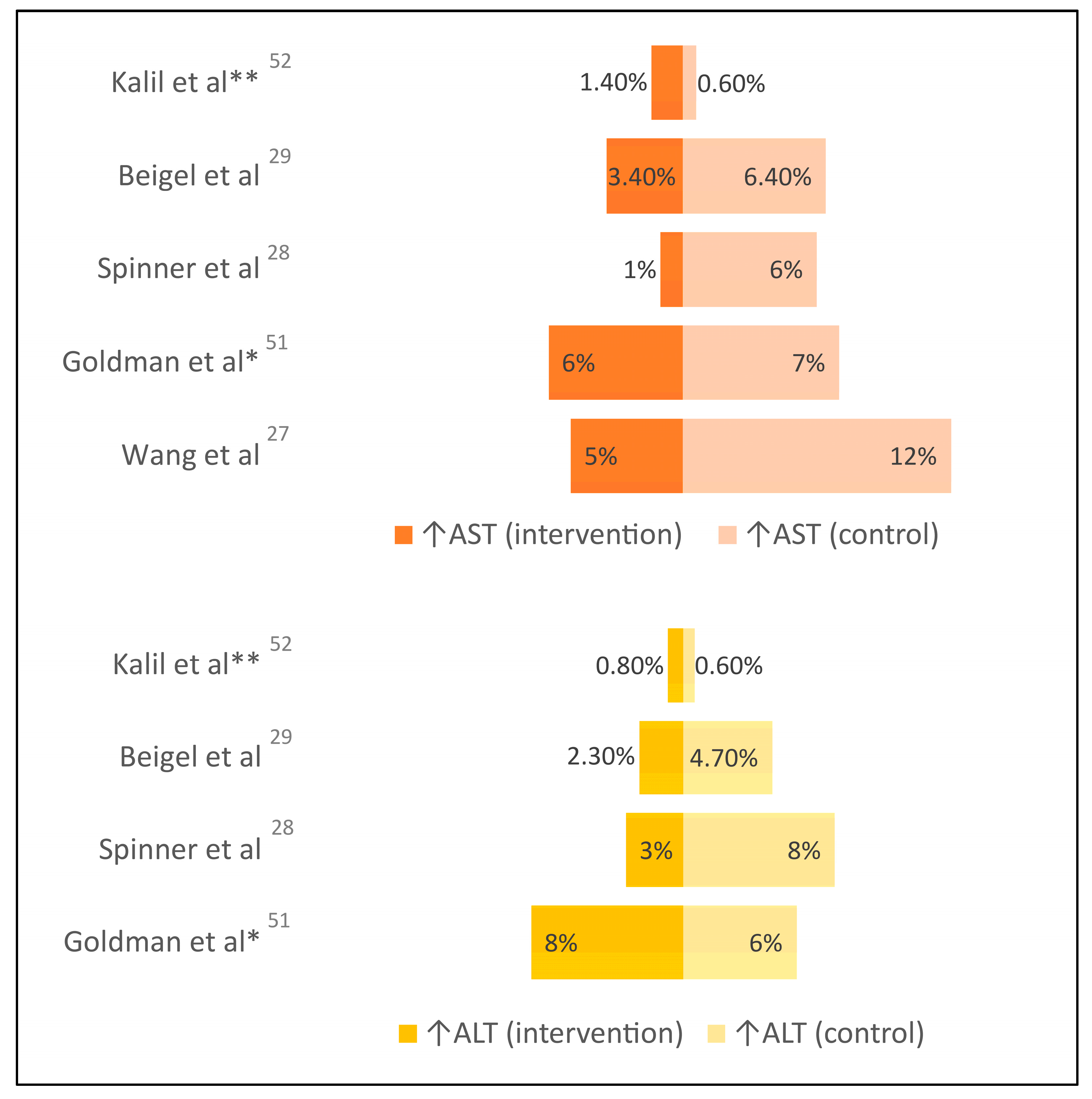

Table 1.
Studies Evaluating Remdesivir Use in Patients with COVID-19.
| Study | Design (size) | Patients | Intervention | Control | Hepatotoxicity |
|---|---|---|---|---|---|
| Leegwater et al. [53] | Retrospective (N=1) | Hospitalized with severe COVID-19, critically ill | Remdesivir for 5 days plus chloroquine for 5 days | None | ↑liver enzymes (severe) |
| Zampino et al. [58] | Retrospective (N=5) | Hospitalized with severe COVID-19, critically ill | Remdesivir for up to 10 days; 4 patients received hydroxychloroquine | None | ↑liver enzymes in all 4 patients who also received hydroxychloroquine (moderate-severe) |
| Montastruc et al. [59] | Retrospective (N=387) | WHO’s VigiBase database of safety reports | Remdesivir up to 10 days | None | 30% ↑liver enzymes (severity not specified) |
| Van Laar et al. [60] | Retrospective (N=103) | Hospitalized with severe COVID-19, non-critically ill | Remdesivir for 5 days | None | 42% ↑liver enzymes (mild-moderate, except for 1 patient with severe) |
| Garibaldi et al. [34] | Retrospective (N=2,299; 570 propensity matched) | Hospitalized with severe COVID-19 | Remdesivir for 5 to 10 days | Standard of care | 10% ↑liver enzymes (severity not specified) |
| Grein et al. [55] | Prospective, descriptive (N=61) | Hospitalized with severe COVID-19, including critically ill | Remdesivir for 10 days | None | 23% ↑liver enzymes (mild-moderate) |
| Antinori et al. [56] | Prospective, descriptive (N=35) | Hospitalized with severe COVID-19, including critically ill | Remdesivir up to 10 days | None | 43% ↑liver enzymes (severity not specified) |
| Burwick et al. [57] | Prospective, descriptive (N=86) | Pregnant or postpartum women | Remdesivir up to 10 days | None | 9% ↑ALT (grade 3), 5% ↑AST (grade 3) |
| Wang et al. [28] | RCT, double-blind (N=236) | Hospitalized with severe COVID-19; excluded cirrhosis or baseline grade 3 ↑liver enzymes | Remdesivir up to 10 days | Placebo | 10% vs 9% ↑liver enzymes (grade 3 or higher), 5% vs 12% ↑AST (grade 3 or higher) |
| Goldman et al. [61] (SIMPLE-1 Severe) | RCT, open-label (N=397) | Hospitalized with severe COVID-19, non-critically ill; excluded baseline grade 3 ↑liver enzymes | Remdesivir up to 10 days | Remdesivir up to 5 days | 8% vs 6% ↑ALT (grade 3 or higher), 6% vs 7% ↑AST (grade 3 or higher) |
| Spinner et al. [29] (SIMPLE-2 Moderate) | RCT, open-label (N=584) | Hospitalized with moderate COVID-19; excluded baseline grade 3 ↑liver enzymes | Remdesivir up to 10 days | Standard of care | 3% vs 8% ↑ALT (grade 3 or higher), 1% vs 6% ↑AST (grade 3 or higher) |
| Beigel et al. [30] (ACTT-1) | RCT, double-blind (N=1,062) | Hospitalized patients with mild, moderate, or severe COVID-19; excluded baseline grade 3 ↑liver enzymes | Remdesivir up to 10 days | Placebo | 2.3% vs 4.7% ↑ALT (grade 3 or higher), 3.4% vs 6.4% ↑AST (grade 3 or higher) |
| Kalil et al. [62] (ACTT-2) |
RCT, double-blind (N=1,033) | Hospitalized patients with mild, moderate, or severe COVID-19; excluded baseline grade 3 ↑liver enzymes | Remdesivir up to 10 days plus baricitinib up to 14 days | Remdesivir up to 10 days plus placebo | 0.8% vs 0.6% ↑ALT (grade 3 or higher), 1.4% vs 0.6% ↑AST (grade 3 or higher) |
| WHO Solidarity Interim Results [31] | RCT, open-label (N=5,475) | Hospitalized with mild, moderate, or severe COVID-19, including critically ill | Remdesivir up to 10 days | Standard of care | Safety data not reported |
| Ader et al. [32] (DisCoVeRy) | RCT, open-label (N=857) | Hospitalized with moderate or severe COVID-19, including critically ill | Remdesivir up to 10 days plus standard of care | Standard of care alone | 3% vs 1% ↑transaminases |
| WHO Solidarity Final Results [35] | RCT, open-label (N=8,275) | Hospitalized with mild, moderate, or severe COVID-19, including critically ill | Remdesivir up to 10 days | Standard of care | Safety data not reported |
* Tables may have a footer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



