
Submitted:
03 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
Obesogens have been identified as a significant factor associated with increasing obesity rates, particularly in developed countries. These substances with obesogenic traits are prevalent in consumer products, including certain pharmaceuticals. Specific classes of pharmaceuticals have been recognized for their ability to induce weight gain, often accompanied by hormonal alterations that can adversely impact male fertility. Indeed, research has supplied evidence underscoring the crucial role of obesogens and therapeutic agents in the normal functioning of the male reproductive system. Notably, sperm count, and various semen parameters have been closely linked to a range of environmental and nutritional factors, including chemicals and pharmacological agents exhibiting obesogenic properties. This review aims to explore studies focused on analyzing male fertility parameters, delving into the intricacies of sperm quality, and elucidating the direct and adverse effects that pharmacological agents may have on these aspects.
Keywords:
Antidiabetics
; Antihypertensives
; Endocrine Disruptors
; Male Fertility
; Obesogens
; Psychotropics
1. Introduction
According to the World Health organization, in 2016, more than 1.9 billion adults aged 18 and over were overweight. Of these, more than 650 million adults were obese. Obesity is considered as a chronic disease, derived from interactions between genetic factors, but also from factors associated with the lifestyle of developed societies (e.g., sedentarism, consumption of high fat diets) and more recently it has been associated with exposure to obesogen compounds [1,2]. These compounds specifically stimulate a rise in adipocyte (fat cell) count and disrupt metabolic and endocrine functions, including the control of appetite and satiety [3,4]. Obesogens emulate the actions of endogenous hormones, resulting in undesirable effects. These compounds attach to receptors situated in cell membranes, cytosol, or even the nucleus, thereby inducing changes in cellular responses and gene expression. Obesogens disrupt adipocytes by altering transcriptional regulators in lipid flow and/or the proliferation/differentiation of these cells, notably through the peroxisome proliferator-activated alpha receptor (PPARα), peroxisome proliferator activated (PPARd), peroxisome proliferator (PPARg) receptor, peroxisome proliferator-activated gamma receptor (PPARg) and steroid receptors [5,6]. The main regulator of adipogenesis is PPARg and its activation provides differentiation of adipocytes and/or induction of lipogenic enzymes [7,8,9,10]. Compounds like organotins, specifically tributyltin (TBT), are regarded as "model obesogens" as they interact with the peroxisome proliferator-activated receptor gamma (PPARγ) [11]. Tributyltin (TBT) functions as an agonist for both peroxisome proliferator-activated receptor gamma (PPARγ) and retinoid X (RXR) receptor. These receptors operate as a heterodimer, robustly encouraging the differentiation and persistence of adipocytes, while also promoting the expression of genes associated with the formation and storage of lipid droplets [11]. In vivo exposure to tributyltin (TBT) during puberty can result in weight gain, insulin resistance, elevated leptin levels, and various other metabolic effects. In adult animals, exposure to TBT leads to an increase in fat mass. However, it remains unclear whether this effect is reversible or permanent [4]. Obesogens are not restricted to organotins and encompass a list of more than 50 compounds. This list includes a diverse array of substances ranging from biocides, plasticizers, industrial chemicals, to pharmaceuticals and personal care products (PPCPs) as well as some natural compounds including certain estrogens [12,13]. Although most studies on obesogens focus on chemicals other than pharmaceuticals, there are substantial evidence that pharmaceuticals may act as obesogens and thus contribute to overweight and obesity [13]. This comes as no surprise if we consider, for example, the well establish association between antidiabetic medications and weight gain. While epidemiological data indicate an association between exposure and effects, it is crucial to consider that most of these studies lack a mechanistic explanation due to inherent limitations. Changes in weight, associated with exposure to obesogen, are a huge public health problem. Exposure to obesogen may also occur in the prenatal period, which may cause complications in the development of the endocrine system of the fetus [4]. Several epidemiological studies have indicated an association between obesogen exposure and elevated body mass index and/or the occurrence of type II diabetes in humans [7,8,14,15]. Additional studies have demonstrated that certain chemicals induce adipogenesis or activate PPARγ. Theoretically, exposure to adipogenic stimuli, such as obesogens, during early age or adolescence, may lead to a permanent increase in the number of adipocytes [16]. In addition to the negative impacts of obesogens on metabolic regulation, exposure to these compounds also influences other mechanisms, including the regulation of male fertility. Typically possessing lipid characteristics, obesogens can easily traverse cell membranes. The male reproductive system is highly susceptible to the detrimental effects of these compounds as they traverse the blood-testicular barrier, leading to damage to reproductive cells. It is important to note that, aside from the impacts of obesogens on male fertility, obesity itself can also adversely affect male reproductive health [17]. Recent reviews already highlighted the impact of obesogens on male reproductive health (e.g. [18,19,20]), however they focused mainly on obesogenic compounds other than pharmaceuticals. This paper aims to provide an updated review, examining the influence of pharmacological agents exhibiting obesogenic characteristics on male reproductive health. The focus is particularly on the regulation of the reproductive axis, potential effects on classical reproductive clinical parameters, and the broader implications for male fertility potential.
2. Pharmacological agents with obesogenic activity
2.1. Corticosteroids
Corticosteroids are despite few studies, weight gain by glucocorticoid (CG) treatment is considered a common long-term side effect. About 70% of all subjects undergoing chronic GC therapy quantified as prednisone equivalent, significantly increase in weight [21]. CG (corticosterone, see Figure 1) stimulate appetite through changes in the activity of protein kinase that is activated by adenosine monophosphate (AMP) in the hypothalamus, consequently influencing the individual's eating habits, increasing their preference for non-dietary foods. Endocannabinoid (eCB) is a potent regulator of food intake, which decreases energy expenditure and leads to fat accumulation in the liver. CG can act through peripheral stimulation of the cannabinoid receptor 1 (CB1R) in the liver, inducing hepatic lipogenesis, steatosis, and dyslipidemia. By increasing the expression of CB1R in adipose tissue, CG induces insulin resistance (IR) and obesity. However, if it is possible to block CB1R, all effects of GC-induced metabolic dysregulation are attenuated. Thus, a potential therapeutic option is the use of selective peripheral CB1R blockers [22].
2.2. Antidiabetics
Antidiabetic drugs are intended to control blood glucose levels and are therefore used in the treatment of diabetes mellitus (DM). Some antidiabetic pharmacological agents cause weight gain, such as the hormone insulin, sulphonylureas (SU) and some thiazolidinediones (TZD). The mechanisms of action of each compound are different and vary depending on certain conditions, such as dose and concentration. Insulin leads to a dose-dependent weight gain by multiple mechanisms [23]. Appetite stimulation, sometimes triggered by hypoglycemia or deep fluctuations in blood glucose, is probably the most important factor in increasing body weight. Thus, the anabolic characteristics of insulin can cause weight gain by inhibiting lipolysis and proteolysis [23,24]. Yet, a study by Mäkimattila and collaborators showed that the addition of metformin can reduce the effect that insulin has on body weight [25]. However, as no known obesogenic effects by metformin are to date, this drug will not be considered in this review. Regarding sulphonylureas (SU) and thiazolidinediones (TZD), weight gain seems to be more pronounced in the first months of therapy. Kahn and collaborators confirmed that the average weight gain of SU is approximately 4 kg during the first year of treatment [26,27]. Additionally, SU causes hyperinsulinemia regardless the glucose levels [28]. Similarly to SU, TZD also generate a weight increase ranging from 1.5 to 4 kg in the first year of treatment [29,30]. The mechanisms by which TZD act causing weight gain include fluid retention, increased storage of lipides, and adipogenesis. However, TZD improves hepatic steatosis, a disease characterized by the accumulation of fat in the liver, usually caused by excessive alcohol consumption and precedents of other pathologies such as obesity and diabetes.
2.3. Antihypertensive
Hypertension is a comorbidity associated with obesity and type 2 diabetes mellitus (T2DM). Antihypertensive therapy should be thoroughly monitored, as drugs that generate weight gain or have other metabolic effects are of concern to hypertensive individuals. β-blockers used as antihypertensives display several effects on weight, they may not lead to any significant change, or they may lead to an increase of 4 kg after 1 year of treatment [31,32]. These effects consist of a decrease in total energy expenditure of 4–9% due to β receptor antagonist therapy [33], since β-blockers reduce the basal metabolic rate by about 12% in obese hypertensive individuals, compared to patients receiving other antihypertensive drugs. Another effect associated with β-blockers is the inhibition of lipolysis in response to adrenergic stimulation, hindering weight loss [34]. Finally, β receptor antagonists have side effects such as fatigue and tiredness, making it difficult for individuals to exercise due to lack of stimulation, thus generating more complications in weight loss. However, some studies concluded that the use of the β-blocker carvedilol did not affect the control of glycemia and even improved some components of the relationship with metoprolol (selective medication of type β-blocker) in individuals with DM and hypertension [32,35,36]. Therefore, selective agents with vasodilators, such as nebivolol and carvedilol, should be a priority when β-blockers are necessary in individuals at high risk of developing secondary metabolic effects [37]. Besides β-blockers, hypertension drugs are related to dosing-associated renal failure and dyslipidemia, which makes them less desirable as priority drugs in the treatment of obese or T2DM patients [37,38].
2.4. Psychotropic
Many classes of psychotropic drugs are associated with significant weight gain and with diseases associated with obesity and its comorbidities such as diabetes, hypertension, and coronary artery disease. Psychiatric patients have a higher tendency to develop obesity when compared to the general population. Multiple factors may be responsible for the association between psychiatric diseases and weight changes, especially the therapy that is applied. Some psychiatric disorders are characterized by chronic stimulation of the hypothalamic-pituitary-adrenal (HPA) axis and increased cortisol, leading to increased abdominal fat, hepatic steatosis and insulin resistance (IR) [39,40]. The bidirectional relationship between obesity and depression is known [41]. Peripheral chronic inflammation induced by visceral fat accumulation and central nervous system inflammation are associated with pathophysiological changes in the brain related to depression [39,41]. Chronic psychosocial stress can cause inflammation and metabolic alterations, which includes weight gain with predominance of visceral fat accumulation and IR [42]. On the other hand, psychotropic drugs also play an important role in the interaction between obesity and psychiatric diseases. There is a positive association between weight gain and time of exposure to psychotropic medication [43]. However, the concrete effect of drugs on weight is often difficult to quantify, since psychiatric disorders can cause changes in mood, appetite, and fitness for physical activity. In order to predict the impact of psychotropic medication on weight gain it is recommended analyzing the amount of weight gain in the first months of therapy [44]. Taking this into account, weight should always be monitored before and after the start of psychotropic medications. An increase of 5% above the baseline after the first month suggests clinicians reconsider new therapeutic options or introduce new strategies to control weight gain [44]. Many drugs of this class (see Figure 2) have the potential to interfere with central appetite-regulating neurotransmitters, altering their effects on dopaminergic, serotonergic, and histaminergic neurotransmission. Thus, through several mechanisms, these affect satiety and metabolic homeostasis [45]. Generally, the differences in the mechanisms that increase weight are partially explained by their differential affinity and effect on the different receptors of neurotransmitters, which may vary from individual to individual [43,46]
2.4.1. Antidepressants
There is a large difference in weight gain during antidepressant therapy as this varies greatly between different classes and their duration. The use of tricyclic antidepressants (TCA) is associated with weight gain both in the acute phase of the disease and in the period of maintenance of therapy [16]. For example, selective serotonin reuptake inhibitors (SSRI's) theoretically have a weight-reducing effect. This is due to its effect on serotonin, which is important in controlling carbohydrate intake. During treatment in the acute phase of the disease, several SSRI's (citalopram, fluoxetine, sertraline, e.g.) and serotonin and norepinephrine reuptake inhibitors (SNRIs), such as venlafaxine and duloxetine, were associated with a slight weight loss. However, the intake of antidepressants such as amitriptyline, nortriptyline and mirtazapine is associated with a considerable weight gain [47].
2.4.2. Lithium
Lithium treatment is associated with side effects associated with metabolic disorders, namely hypothyroidism, hyperparathyroidism, thus generating weight gain. Lithium in turn is responsible for interfering with the production of thyroid hormones by interfering with iodine absorption. Studies showed that 60% of patients who suffer bipolar disorder who undergo lithium therapy have a 5% higher incidence of significant weight gain. A possible mechanism triggered by lithium is direct control over the mechanisms that regulate appetite, from its effects on the hypothalamus, consequently there is an increase in satiety by very caloric foods and beverages [48].
2.4.3. Antipsychotics
Second-generation antipsychotics (SGAP) or atypical antipsychotics are often prescribed for psychotic disorders, such as bipolar disorders. These have a peculiar pharmacological profile because they induce fewer extrapyramidal effects, however, individuals who take SGAP increase their weight by at least 7% [49,50]. The effects of antipsychotics on weight gain are dose and time dependent and as well as psychotropic medication the effects on body weight can be predicted by the progression of how weight may vary in the first weeks of treatment. Clozapine, olanzapine, quetiapine and risperidone are associated with higher weight gain. Aripiprazole, amisulpride and ziprasidone are also associated with weight gain, but less than the former, being classified as neutral weight agents [29,51].
2.4.4. Antiepileptics
The most used antiepileptic drugs are valproate and carbamazepine, which induce weight gain in 43% of patients [52]. Pregabalin and gabapentin may also induce weight gain [53]. It has been demonstrated during valproate therapy weight gain is higher in the first year of treatment and that women appear to be more susceptible than men [54]. The interaction of valproate with leptin and resistin, neuropeptides that regulate appetite in the hypothalamus and with effects on energy expenditure, may be the main responsible for weight gain [16]. One of the side effects of valproate is the induction of hyperglycemia and consequently development of T2DM, since it has a direct effect on IR. It also directly interferes with the release of insulin by an effect mediated by γ-aminobutyric acid (GABA) in β pancreatic cells. Valproate can also cause other problems such as increased cholesterol and triglycerides, or decreased levels of high-density lipoprotein, HDL (dyslipidemia) [55]. On the other hand, the mechanisms in weight gain induced by carbamazepine, pregabalin and gabapentin are not related to increased IR, metabolic syndromes or the risk of hyperglycemia [56]. Topiramate and zonisamide, however, are associated with decreased body weight. Given this, the combination of topiramate with another antiepileptic, antipsychotic or antidepressant or the change in anticonvulsant therapy with topiramate or zonisamide may help prevent obesity [57].
3. Effects of pharmacological agents on male fertility parameters
The regulation of male fertility is a very complex process and can be interrupted by numerous factors such as: life style, drug consumption, exposure to environmental contaminants that present endocrine disrupting and obesogenic properties [58]. In order to understand the impact of such factors, several endpoints need to be evaluated. While all animals are monitored by body weight and fertility indices, there are specifically relevant assessment points that should also be considered, including macroscopic examination and morphology of reproductive organs, observation of development effects and measurement of spermatozoan effects. Weight and histopathological analyses of the testicles, epididymis and accessory sex glands, including the prostate and seminal vesicles, should be conducted because these sex glands are dependent on androgens and these hormones reflect changes in the endocrine state of the animal or testicular function [8,58]. Additionally, as the normal physical development may also be affected by the exposure to obesogens, testicular descent, anogenital distance, and external genitalia structure need to be evaluated. Finally, the evaluations of the number of spermatozoa, morphology and motility is of paramount importance as the number of spermatozoa are derived from spermatid head counts in the testicle and epididymis [59,60,61,62]. Furthermore, the comprehension of the impacts of the exposure to different pharmaceutical agents, is further conditioned by a latency period as the side effects of the drugs may be observed even after the discontinuation of treatment, being necessary 1 to 3 months for the parameters to be restored. Some studies have shown that obesogens can alter endocrine activity in various ways, affecting androgen production. The hypothalamus-pituitary-gonad axis (HPG) is fundamental for male sexual maturity and fertility regulation. The hypothalamus secretes the gonadotrophine-refining hormone (GnRH), which causes an increase in the nocturnal secretion of pulsatile gonadotrophy (luteinizing hormone (LH) and follicle-stimulating hormone (FSH)) by the anterior pituitary [58,63]. In humans, a neonatal testosterone spike during the first 4 months of life leads to testosterone levels that resemble those of a healthy adult man [64]. At 6 months of age, testosterone levels decrease to almost negligible levels and remain low until puberty, at which time sexual characteristics develop. In adult men, pulsatile secretion of gonadotrophin occurs approximately every 90 minutes; the frequency with which this occurs is an important factor in the normal gonadal response [65]. When the pulse frequency of gonadotrophin reaches a critical level, secondary sexual characteristics begin to form; this marks the onset of puberty [63]. While FSH is not used until sperm maturation, LH is released during sleep along with pulsatile GnRH, causing gonadal stimulation and induction of hyperplasia of Leydig cells, responsible for testosterone production [66]. Any therapy that affects testicular endocrine function has as a direct consequence the deregulation of spermatogenesis, compromising the viability of germ cells or even the integrity of Sertoli cells. Sertoli cells play a supporting role in the survival and differentiation of germ cells, as they not only provide physical support, but also ensure the "nutrition" of the germ line [46,67]. Another target of endocrine disruption of the testicles is the production of testosterone by Leydig cells or even the disturbance of the hypothalamus-pituitary axis, which results in deficient testosterone production. Treatments with certain classes of medications (antidiabetic, antihypertensive, antidepressant, antipsychotic and antiepileptic) can cause endocrine disorders, which ends up directly interfering with the male reproductive tract and all molecular mechanisms responsible for the physiological maintenance of male fertility (see Figure 3).
3.1. Antidiabetics
Although certain drugs of this class have obesogenic characteristics, such as insulin, SU and some TZDs, pioglitazone and metformin (biguanide) are the most notorious ones. These drugs are used in the treatment of T2DM, being suitable for young people and men of reproductive age. Pioglitazone is a potent synthetic agonist of PPARγ-activated receptors [68]. Activation of these receptors leads to increased transcription of genes related to glucose metabolism. Pioglitazone is available to make combinations with other antidiabetics such as metformin [69]. It differs (heterodimerizes) from retinoid receptor X and binds to responsive nuclear elements, thus modulating transcription of genes that play a role in glucose and lipid metabolism [9]. An adverse effect that this class has is fluid retention, which makes TZD contraindicated in individuals with heart failure, which is one of the leading causes of death in individuals with T2DM [70]. In a recent study it was observed that pioglitazone at the dose of (10 μM) increases lactate production in in vitro cultures of human Sertoli cells without causing morphological changes or considerable metabolic changes. This result is relevant since lactate is a survival factor of some germ cells and thus pioglitazone is a positive factor in testicular metabolic reprogramming [71].
3.2. Antihypertensive drugs
The mechanisms by which these treatments affect sexual function are yet to be properly clarified, with limited studies providing data on the interactions between this class of drugs and sexual dysfunctions. Therefore, it is still difficult to show the impact they may have on the reproductive tract. Some studies suggest that hypertensive erectile dysfunction may be the result of reduced penile pressure, associated with decreased systemic pressure reduced by the antihypertensives themselves [72,73,74]. Other studies have shown that antihypertensives with central action stimulate α2-adrenergic presynapttic receptors, causing a reduction in central sympathetic tone. The increase in sympathetic tone leads to short-blooded tacardia, consequently centrally activated antihypertensives would be a good choice for the treatment of hypertension, however they can generate changes in ejaculatory function, as a sign of hormonal changes [72,75].
Other drugs, including alpha-blockers and calcium channel blockers do not cause erectile dysfunction, but may generate ejaculatory disorders due to spongy bulb muscle contractions [67]. Angiotensin conversion enzyme inhibitors and sartans, on the other hand, do not alter erectile function. In fact, angiotensin II is an important mediator of penile tumescence (erectile dysfunction). The effects of drugs that improve endothelium function in the erection and have been demonstrated that angiotensin II antagonists are very promising [76]. In fact, angiotensin II antagonists are considered a good option for the treatment of hypertension in sexually active individuals, since they improve endothelial function in penile erection [72,77,78,79,80].Some studies, on the implication of antihypertensive drugs in erectile dysfunction, showed that sartans were not associated with the development of sexual dysfunction and that they might be a viable therapeutic treatment option to prevent or correct erectile dysfunctions in patients with hypertension [72,73,77,78,81,82,83]. The administration of drugs with antihypertensive action, such as calcium channel blockers, compromise fertility, particularly by reducing the viability and motility of spermatozoa. The alteration of these clinical parameters prevents the fertilization process because it prevents the sperm and oocyte interaction resulting from the transmembrane movement of the calcium modifier, described in vitro [83,84,85,86]. Although these side effects in hypertensive individuals do not constitute a motive for therapy discontinuation, it is important to consider the beneficial effects that antihypertensives have in relation to cardiovascular problems.
3.3. Psychotropics
3.3.1. Antidepressants
Selective serotonin reuptake inhibitors (SSRI's) are the first-line treatment for depression and tricyclic antidepressants play the role of inhibiting the recapture of catecholamines at the central level. Tricyclic antidepressants and SSRI's are responsible for hyperprolactinemia, which will inhibit the hypothalamus. If hypogonadism is observed, these drugs may cause adverse effects on male fertility as described below [82,83,87,88]. SSRI’s are responsible for the increase in serotonin neurotransmission, thus generated an inhibition in male sexual behavior. Men who are under this type of therapy have loss of libido and anorgasmia during prophylaxis. Delayed ejaculation, or even anejaculation, have also been observed in a few weeks after the start of treatment. Treatment with tricyclic antidepressants is associated with delayed ejaculation/anejaculation [75,78,81,82,83,89,90,91]. At the clinical level, SSRIs alter sperm count and motility. However, there is some controversy in the literature about the adverse effects on reproductive clinical parameters. Antidepressants can also alter sperm quality through a mechanism that affects its transport, since drugs belonging to this class act at the level of the central nervous system and affect the ejaculation process [88,92,93,94]. Monoamine oxidase inhibitors (MAOIs) are also prescribed for the treatment of depression, but with less frequency and priority and rarely generate any erectile disorders, as they are less associated with hyperprolactinemia [87]. Depression is characterized as a chronic condition, and in the event of adverse effects such as changing sexual parameters, in the therapy based and MRI or MAOI discontinuation of treatment is a very viable option. In relation to other antidepressants such as bupropion, mirtazapine and buspirone, it was found that they do not cause considerable changes in male reproductive health [75,81,82,83,89,91,95,96,97].
3.3.2. Antipsychotics
Like tricyclic antidepressants and SSIs’s, "typical" neuroleptics (phenothiazides) are responsible for hyperprolactinemia, the most common abnormality of the hypothalamic-hypothesis axis, caused by exaggerated production and prolactin (PRL) due to central dopamine secretion block. As a result, one of the most relevant adverse effects are changes in spermatogenesis and consequent decrease in sperm quality [83,87,98]. The "typical" neuroleptics can also affect the sexual activity, with e.g., difficulty in reaching orgasm even with sexual stimulation (anorgasmia), decreased libido and disorders of the reaction. On the other hand, "atypical" neuroleptics do not cause an increase in prolactin levels, not causing hyperprolactinemia [81,99]. Dysfunctions that are observed during treatment may also result from an anticholinergic effect induced by antipsychotics of β-adrenergic transmission block [67]. As psychotic conditions are often difficult to interpret, it is difficult to tell whether sexual disorders come from chronic disease or its treatment. If any sexual dysfunction appears during treatment with typical neuroleptics such as haloperidol or amissulpride, it may be possible to switch to a treatment with atypical neuroleptics such as Quetiapine, olanzapine or clozapine, as these have an affinity for 5-HT2 receptors and also for dopamine D2 receptors facilitating sexual behavior by causing fewer side effects [75,81,83,89,99].
3.3.3. Antiepileptics
Sexual dysfunction in individuals with epileptic conditions is due to several causes and may result from the pathophysiology of the disease and/or the treatment with associated anticonvulsants. It is extremely difficult to distinguish the cause of these changes, as epileptic men usually rarely remain without proper treatment, and therefore it makes it difficult to understand that the changes are a result of epilepsy, or the interaction of the drugs used in the treatment. Studies conducted in animal models have shown that valproate administration is responsible for reducing testicular weight in animals [85,100,101]. Valproate does not increase SHGH levels but increases the level of GABA in the central nervous system, thus modifying the production of GnRH. This drug may also be responsible for increased peripheral levels of androgens, and a possible reduction of LH [101,102,103,104,105]. Inducers of liver enzymes such as carbamazepine and phenytoin increase the synthesis of sex hormone binding globulin, the protein involved in testosterone transport, but reduced free levels of androgens [106]. On the clinical level, antiepileptics are believed to have a significant impact on spermatic parameters, and although the underlying molecular pathways are still unclear it is thought that it may be due to the interaction between pharmacological action and the molecular mechanisms underlying pathophysiology. Carbamazepine, valproate and phenytoin reduce sperm motility by interfering with sperm membrane, as valproate reduces the L-carnitine/T-carnitine ratio. Similarly, carbamazepine is believed to be directly related to germ cells, inducing a greater number of necrotic germ cells in the lumen of seminiferous tubules. Thus, it is perceived as valproate is responsible for the reduction of testicular weight in animals, indicating that the drug can be harmful not only in the level of spermatogenesis, but also in the degradation of testicular somatic cells, such as Sertoli cells [85,100,101,107,108].
4. Conclusions
Within clinical settings where obesity and/or male fertility are considerations, it is imperative to conduct a thorough analysis of individuals' histories. This examination should encompass potential pathologies and drug interactions. In this mini-review, data were gathered specifically on drugs possessing obesogenic properties, with a primary focus on the context of obesity pathology and an extension into the realm of male fertility. The review highlights the principal classes of drugs exhibiting obesogenic actions and their potential to induce hormonal changes that impact male reproductive parameters. Numerous studies have confirmed that the use of certain pharmacological agents leads specifically to weight gain. Concurrently, weight gain itself elicits unfavorable effects on the body. In alignment with existing literature and the focus of this research, it is evident that both weight gain and the pharmacological agents under investigation induce various consequences for the male reproductive system. While all drugs with obesogenic activity generally have adverse effects on male fertility, certain classes stand out due to their more pronounced consequences. Notably, these include antihypertensives (such as alpha-blockers and Ca2+ channel blockers), antidepressants (specifically serotonin reuptake inhibitors or SRIs), antipsychotics (particularly atypical neuroleptics like haloperidol and amisulpride), antiepileptics (valproate), and antidiabetics (including TZD and SU). To advance the current research, it will be crucial in the future to address the existing gaps in information and methodological approaches used to study the impact of these agents on male fertility. Therefore, further investigations will be necessary to comprehensively understand and delineate the molecular actions of drugs on male reproductive physiology.
Author Contributions
Conceptualization, L.R.; methodology, L.R.; validation A.C.A.S. and L.R.; formal analysis, C.M., AC.A.S. and L.R.; investigation, C.M. and L.R.; writing—original draft preparation, C.M.; writing—review and editing, AC.A.S. and L.R.; visualization, A.C.A.S; supervision, L.R. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
Ana C. A. Sousa acknowledges the Comprehensive Health Research Centre (CHRC) funded through the Foundation for Science and Technology, under the project UIDP/04923/2020 and La Mer Project funded by the Japanese Ministry of Education, Culture, Sports, Science, and Technology (MEXT). L. Rato acknowledges the CICS-UBI projects UIDB/00709/2020 and UIDP/00709/2020, financed by national funds through the Portuguese Foundation for Science and Technology/MCTES.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Heindel, J.; Schug, T., The Obesogen Hypothesis: Current Status and Implications for Human Health. Curr Envir Health Rpt 2014, 1, (4), 333-340.
- Lars Lind; P. Monica Lind; Margareta H. Lejonklou; Linda Dunder; Åke Bergman; Carlos Guerrero-Bosagna; Erik Lampa; Hong Kyu Lee; Juliette Legler; Angel Nadal; Youngmi Kim Pak; Richard P. Phipps; Laura N. Vandenberg; Daniel Zalko; Marlene Ågerstrand; Öberg, M.; Bruce Blumberg; Jerrold J. Heindel; Birnbaum, L. S., Uppsala Consensus Statement on Environmental Contaminants and the Global Obesity Epidemic. Envir. Health Perspect. 2016, 124, (5), A81-A83.
- De Coster, S.; Van Larebeke, N., Endocrine-disrupting chemicals: associated disorders and mechanisms of action. Journal of environmental and public health 2012, 2012.
- Janesick, A. S.; Blumberg, B., Obesogens: an emerging threat to public health. American journal of obstetrics and gynecology 2016, 214, (5), 559-565.
- Darbre, P. D., Endocrine disruptors and obesity. Current obesity reports 2017, 6, 18-27.
- Yang, O.; Kim, H. L.; Weon, J.-I.; Seo, Y. R., Endocrine-disrupting chemicals: review of toxicological mechanisms using molecular pathway analysis. Journal of cancer prevention 2015, 20, (1), 12.
- Diamanti-Kandarakis, E.; Bourguignon, J.-P.; Giudice, L. C.; Hauser, R.; Prins, G. S.; Soto, A. M.; Zoeller, R. T.; Gore, A. C., Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocrine reviews 2009, 30, (4), 293-342.
- Gore, A. C.; Chappell, V. A.; Fenton, S. E.; Flaws, J. A.; Nadal, A.; Prins, G. S.; Toppari, J.; Zoeller, R. T., EDC-2: the Endocrine Society's second scientific statement on endocrine-disrupting chemicals. Endocrine reviews 2015, 36, (6), E1-E150.
- Tontonoz, P.; Spiegelman, B. M., Fat and beyond: the diverse biology of PPARγ. Annu. Rev. Biochem. 2008, 77, 289-312.
- Lustig, R. H.; Collier, D.; Kassotis, C.; Roepke, T. A.; Ji Kim, M.; Blanc, E.; Barouki, R.; Bansal, A.; Cave, M. C.; Chatterjee, S.; Choudhury, M.; Gilbertson, M.; Lagadic-Gossmann, D.; Howard, S.; Lind, L.; Tomlinson, C. R.; Vondracek, J.; Heindel, J. J., Obesity I: Overview and molecular and biochemical mechanisms. Biochem. Pharmacol. 2022, 115012.
- Goldberg, E. D., TBT An environmental dilemma. Environment;(United States) 1986, 28, (8).
- Heindel, J. J.; Blumberg, B.; Cave, M.; Machtinger, R.; Mantovani, A.; Mendez, M. A.; Nadal, A.; Palanza, P.; Panzica, G.; Sargis, R., Metabolism disrupting chemicals and metabolic disorders. Reproductive toxicology 2017, 68, 3-33.
- Heindel, J. J.; Howard, S.; Agay-Shay, K.; Arrebola, J. P.; Audouze, K.; Babin, P. J.; Barouki, R.; Bansal, A.; Blanc, E.; Cave, M. C.; Chatterjee, S.; Chevalier, N.; Choudhury, M.; Collier, D.; Connolly, L.; Coumoul, X.; Garruti, G.; Gilbertson, M.; Hoepner, L. A.; Holloway, A. C.; Howell, G.; Kassotis, C.; Kay, M. K.; Ji Kim, M.; Lagadic-Gossmann, D.; Langouet, S.; Legrand, A.; Li, Z.; Le Mentec, H.; Lind, L.; Monica Lind, P.; Lustig, R. H.; Martin-Chouly, C.; Munic Kos, V.; Podechard, N.; Roepke, T. A.; Sargis, R. M.; Starling, A.; Tomlinson, C. R.; Touma, C.; Vondracek, J.; vom Saal, F.; Blumberg, B., Obesity II: Establishing Causal Links Between Chemical Exposures and Obesity. Biochem. Pharmacol. 2022, 115015.
- Casals-Casas, C.; Desvergne, B., Endocrine disruptors: from endocrine to metabolic disruption. Annual review of physiology 2011, 73, 135-162.
- Quagliariello, V.; Rossetti, S.; Cavaliere, C.; Di Palo, R.; Lamantia, E.; Castaldo, L.; Nocerino, F.; Ametrano, G.; Cappuccio, F.; Malzone, G., Metabolic syndrome, endocrine disruptors and prostate cancer associations: biochemical and pathophysiological evidences. Oncotarget 2017, 8, (18), 30606.
- Verhaegen, A. A.; Van Gaal, L. F., Drug-induced obesity and its metabolic consequences: a review with a focus on mechanisms and possible therapeutic options. Journal of endocrinological investigation 2017, 40, 1165-1174.
- Palmer, N. O.; Bakos, H. W.; Fullston, T.; Lane, M., Impact of obesity on male fertility, sperm function and molecular composition. Spermatogenesis 2012, 2, (4), 253-263.
- Mínguez-Alarcón, L.; Gaskins, A. J.; Meeker, J. D.; Braun, J. M.; Chavarro, J. E., Endocrine disrupting chemicals and male reproductive health. Fertil. Steril. 2023.
- Thacharodi, A.; Hassan, S.; Acharya, G.; Vithlani, A.; Hoang Le, Q.; Pugazhendhi, A., Endocrine disrupting chemicals and their effects on the reproductive health in men. Environ. Res. 2023, 236, 116825.
- Sousa, A. C. A.; Alves, M. G.; Oliveira, P. F.; Silva, B. M.; Rato, L., Male Infertility in the XXI Century: Are Obesogens to Blame? International Journal of Molecular Sciences 2022, 23, (6), 3046.
- Curtis, J. R.; Westfall, A. O.; Allison, J.; Bijlsma, J. W.; Freeman, A.; George, V.; Kovac, S. H.; Spettell, C. M.; Saag, K. G., Population-based assessment of adverse events associated with long-term glucocorticoid use. Arthritis Care & Research 2006, 55, (3), 420-426.
- Bowles, N. P.; Karatsoreos, I. N.; Li, X.; Vemuri, V. K.; Wood, J.-A.; Li, Z.; Tamashiro, K. L.; Schwartz, G. J.; Makriyannis, A. M.; Kunos, G., A peripheral endocannabinoid mechanism contributes to glucocorticoid-mediated metabolic syndrome. Proceedings of the National Academy of Sciences 2015, 112, (1), 285-290.
- Russell-Jones, D.; Khan, R., Insulin-associated weight gain in diabetes–causes, effects and coping strategies. Diabetes, Obesity and Metabolism 2007, 9, (6), 799-812.
- Van Gaal, L.; Scheen, A., Weight management in type 2 diabetes: current and emerging approaches to treatment. Diabetes care 2015, 38, (6), 1161-1172.
- Mäkimattila, S.; Nikkilä, K.; Yki-Järvinen, H., Causes of weight gain during insulin therapy with and without metformin in patients with type II diabetes mellitus. Diabetologia 1999, 42, 406-412.
- Kahn, S. E.; Haffner, S. M.; Heise, M. A.; Herman, W. H.; Holman, R. R.; Jones, N. P.; Kravitz, B. G.; Lachin, J. M.; O'Neill, M. C.; Zinman, B., Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. New England Journal of Medicine 2006, 355, (23), 2427-2443.
- Turner, R. C., The UK prospective diabetes study: a review. Diabetes care 1998, 21, (Supplement_3), C35-C38.
- Inzucchi, S. E., Oral antihyperglycemic therapy for type 2 diabetes: scientific review. JAMA 2002, 287, (3), 360-72.
- Domecq, J. P.; Prutsky, G.; Leppin, A.; Sonbol, M. B.; Altayar, O.; Undavalli, C.; Wang, Z.; Elraiyah, T.; Brito, J. P.; Mauck, K. F., Drugs commonly associated with weight change: a systematic review and meta-analysis. The Journal of Clinical Endocrinology & Metabolism 2015, 100, (2), 363-370.
- Medici, V.; McClave, S. A.; Miller, K. R., Common medications which lead to unintended alterations in weight gain or organ lipotoxicity. Current gastroenterology reports 2016, 18, 1-12.
- Messerli, F. H.; Bell, D. S.; Fonseca, V.; Katholi, R. E.; McGill, J. B.; Phillips, R. A.; Raskin, P.; Wright Jr, J. T.; Bangalore, S.; Holdbrook, F. K., Body weight changes with β-blocker use: results from GEMINI. The American journal of medicine 2007, 120, (7), 610-615.
- Sharma, A. M.; Pischon, T.; Hardt, S.; Kunz, I.; Luft, F. C., Hypothesis: β-adrenergic receptor blockers and weight gain: a systematic analysis. Hypertension 2001, 37, (2), 250-254.
- Welle, S.; Schwartz, R. G.; Statt, M., Reduced metabolic rate during β-adrenergic blockade in humans. Metabolism 1991, 40, (6), 619-622.
- Koch, G.; Franz, I.-W.; Lohmann, F., Effects of Short-Term and Long-Term Treatment with Cardio-Selective and non-Selective β-Receptor Blockade on Carbohydrate and Lipid Metabolism and on Plasma Catecholamines at Rest and during Exercise. Clinical Science 1981, 61, (s7), 433s-435s.
- Bakris, G. L.; Fonseca, V.; Katholi, R. E.; McGill, J. B.; Messerli, F. H.; Phillips, R. A.; Raskin, P.; Wright, J. T., Jr.; Oakes, R.; Lukas, M. A.; Anderson, K. M.; Bell, D. S.; Investigators, G., Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 2004, 292, (18), 2227-36.
- Ripley, T. L.; Saseen, J. J., β-blockers: a review of their pharmacological and physiological diversity in hypertension. Annals of Pharmacotherapy 2014, 48, (6), 723-733.
- Landsberg, L.; Aronne, L. J.; Beilin, L. J.; Burke, V.; Igel, L. I.; Lloyd-Jones, D.; Sowers, J., Obesity-related hypertension: Pathogenesis, cardiovascular risk, and treatment—A position paper of the The Obesity Society and the American Society of Hypertension. Obesity 2013, 21, (1), 8-24.
- Elliott, W. J.; Meyer, P. M., Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis. The Lancet 2007, 369, (9557), 201-207.
- Ménard, C.; Pfau, M. L.; Hodes, G. E.; Russo, S. J., Immune and neuroendocrine mechanisms of stress vulnerability and resilience. Neuropsychopharmacology 2017, 42, (1), 62-80.
- Naughton, M.; Dinan, T. G.; Scott, L. V., Corticotropin-releasing hormone and the hypothalamic–pituitary–adrenal axis in psychiatric disease. Handbook of clinical neurology 2014, 124, 69-91.
- Capuron, L.; Lasselin, J.; Castanon, N., Role of adiposity-driven inflammation in depressive morbidity. Neuropsychopharmacology 2017, 42, (1), 115-128.
- Chuang, J.-C.; Krishnan, V.; Hana, G. Y.; Mason, B.; Cui, H.; Wilkinson, M. B.; Zigman, J. M.; Elmquist, J. K.; Nestler, E. J.; Lutter, M., A β3-adrenergic-leptin-melanocortin circuit regulates behavioral and metabolic changes induced by chronic stress. Biological psychiatry 2010, 67, (11), 1075-1082.
- Zimmermann, U.; Kraus, T.; Himmerich, H.; Schuld, A.; Pollmächer, T., Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. Journal of psychiatric research 2003, 37, (3), 193-220.
- Vandenberghe, F.; Gholam-Rezaee, M.; Saigí-Morgui, N.; Delacretaz, A.; Choong, E.; Solida-Tozzi, A.; Kolly, S.; Thonney, J.; Gallo, S. F.; Hedjal, A., Importance of early weight changes to predict long-term weight gain during psychotropic drug treatment. The Journal of clinical psychiatry 2015, 76, (11), 8736.
- Himmerich, H.; Minkwitz, J.; C Kirkby, K., Weight gain and metabolic changes during treatment with antipsychotics and antidepressants. Endocrine, Metabolic & Immune Disorders-Drug Targets (Formerly Current Drug Targets-Immune, Endocrine & Metabolic Disorders) 2015, 15, (4), 252-260.
- Casey, D. E.; Zorn, S. H., The pharmacology of weight gain with antipsychotics. Journal of Clinical Psychiatry 2001, 62, 4-10.
- Serretti, A.; Chiesa, A., A meta-analysis of sexual dysfunction in psychiatric patients taking antipsychotics. International clinical psychopharmacology 2011, 26, (3), 130-140.
- Livingstone, C.; Rampes, H., Lithium: a review of its metabolic adverse effects. Journal of Psychopharmacology 2006, 20, (3), 347-355.
- Spertus, J.; Horvitz-Lennon, M.; Abing, H.; Normand, S. L., Risk of weight gain for specific antipsychotic drugs: a meta-analysis. NPJ Schizophr 2018, 4, (1), 12.
- Allison, D. B.; Mentore, J. L.; Heo, M.; Chandler, L. P.; Cappelleri, J. C.; Infante, M. C.; Weiden, P. J., Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999, 156, (11), 1686-96.
- Balf, G.; Stewart, T. D.; Whitehead, R.; Baker, R. A., Metabolic adverse events in patients with mental illness treated with antipsychotics: a primary care perspective. Primary care companion to the Journal of clinical psychiatry 2008, 10, (1), 15.
- Ben-Menachem, E., Weight issues for people with epilepsy--a review. Epilepsia 2007, 48 Suppl 9, 42-5.
- Agró, L.; Demurtas, R.; Sander, J. W., Anticonvulsant Agents: Gabapentin and Pregabalin. In NeuroPsychopharmacotherapy, Riederer, P.; Laux, G.; Mulsant, B.; Le, W.; Nagatsu, T., Eds. Springer International Publishing: Cham, 2020; pp 1-14.
- Verrotti, A.; D'Egidio, C.; Mohn, A.; Coppola, G.; Chiarelli, F., Weight gain following treatment with valproic acid: pathogenetic mechanisms and clinical implications. Obes Rev 2011, 12, (5), e32-43.
- Belcastro, V.; D’Egidio, C.; Striano, P.; Verrotti, A., Metabolic and endocrine effects of valproic acid chronic treatment. Epilepsy research 2013, 107, (1-2), 1-8.
- Swann, A. C., Major system toxicities and side effects of anticonvulsants. Journal of Clinical Psychiatry 2001, 62, (14), 16-21.
- Antel, J.; Hebebrand, J., Weight-reducing side effects of the antiepileptic agents topiramate and zonisamide. Handb Exp Pharmacol 2012, (209), 433-66.
- Campion, S.; Catlin, N.; Heger, N.; McDonnell, E. V.; Pacheco, S. E.; Saffarini, C.; Sandrof, M. A.; Boekelheide, K., Male reprotoxicity and endocrine disruption. Molecular, Clinical and Environmental Toxicology: Volume 3: Environmental Toxicology 2012, 315-360.
- Creasy, D. M., Evaluation of testicular toxicity in safety evaluation studies: the appropriate use of spermatogenic staging. Toxicologic pathology 1997, 25, (2), 119-131.
- Cardoso, A. M.; Alves, M. G.; Mathur, P. P.; Oliveira, P. F.; Cavaco, J. E.; Rato, L., Obesogens and male fertility. Obes Rev 2017, 18, (1), 109-125.
- Rato, L.; Sousa, A. C. A., The Impact of Endocrine-Disrupting Chemicals in Male Fertility: Focus on the Action of Obesogens. J Xenobiot 2021, 11, (4), 163-196.
- Sousa, A. C. A.; Alves, M. G.; Oliveira, P. F.; Silva, B. M.; Rato, L., Male Infertility in the XXI Century: Are Obesogens to Blame? Int J Mol Sci 2022, 23, (6).
- Traggiai, C.; Stanhope, R., Disorders of pubertal development. Best practice & research Clinical obstetrics & gynaecology 2003, 17, (1), 41-56.
- Wilson, C.; Davies, D., The control of sexual differentiation of the reproductive system and brain. Reproduction 2007, 133, (2), 331-359.
- Rinaldi, S.; Moret, C.; Kaaks, R.; Biessy, C.; Kurzer, M.; Dechaud, H.; Peeters, P.; Van Noord, P., Reproducibility over time of measurements of androgens, estrogens and hydroxy estrogens in urine samples from post-menopausal women. European journal of epidemiology 2003, 18, 417-424.
- Viswanathan, V.; Eugster, E. A., Etiology and treatment of hypogonadism in adolescents. Pediatric Clinics 2011, 58, (5), 1181-1200.
- Semet, M.; Paci, M.; Saïas-Magnan, J.; Metzler-Guillemain, C.; Boissier, R.; Lejeune, H.; Perrin, J., The impact of drugs on male fertility: a review. Andrology 2017, 5, (4), 640-663.
- Kung, J.; Henry, R. R., Thiazolidinedione safety. Expert opinion on drug safety 2012, 11, (4), 565-579.
- Alves, M. G.; Martins, A. D.; Vaz, C. V.; Correia, S.; Moreira, P. I.; Oliveira, P. F.; Socorro, S., Metformin and male reproduction: effects on Sertoli cell metabolism. Br J Pharmacol 2014, 171, (4), 1033-42.
- Krentz, A. J.; Bailey, C. J., Oral antidiabetic agents: current role in type 2 diabetes mellitus. Drugs 2005, 65, 385-411.
- Meneses, M. J.; Bernardino, R. L.; Sa, R.; Silva, J.; Barros, A.; Sousa, M.; Silva, B. M.; Oliveira, P. F.; Alves, M. G., Pioglitazone increases the glycolytic efficiency of human Sertoli cells with possible implications for spermatogenesis. Int J Biochem Cell Biol 2016, 79, 52-60.
- Ferrario, C. M.; Levy, P., Sexual dysfunction in patients with hypertension: implications for therapy. The journal of clinical hypertension 2002, 4, (6), 424-432.
- Grimm Jr, R. H.; Grandits, G. A.; Prineas, R. J.; McDonald, R. H.; Lewis, C. E.; Flack, J. M.; Yunis, C.; Svendsen, K.; Liebson, P. R.; Elmer, P. J., Long-term effects on sexual function of five antihypertensive drugs and nutritional hygienic treatment in hypertensive men and women: Treatment of Mild Hypertension Study (TOMHS). Hypertension 1997, 29, (1), 8-14.
- Manolis, A.; Doumas, M., Antihypertensive treatment and sexual dysfunction. Current hypertension reports 2012, 14, 285-292.
- Jones, D.; Norman, A.; Horwich, A.; Hendry, W., Ejaculatory dysfunction after retroperitoneal lymphadenectomy. European urology 1993, 23, (1), 169-171.
- Shindel, A.; Kishore, S.; Lue, T., Drugs designed to improve endothelial function: effects on erectile dysfunction. Current pharmaceutical design 2008, 14, (35), 3758-3767.
- Becker, A. J.; Ückert, S.; Stief, C. G.; Scheller, F.; Knapp, W. H.; Hartmann, U.; Jonas, U., Plasma levels of angiotensin II during different penile conditions in the cavernous and systemic blood of healthy men and patients with erectile dysfunction. Urology 2001, 58, (5), 805-810.
- Droupy, S. In Epidemiology and physiopathology of erectile dysfunction, Annales D'urologie, 2005; 2005; pp 71-84.
- Karavitakis, M.; Komninos, C.; Theodorakis, P. N.; Politis, V.; Lefakis, G.; Mitsios, K.; Koritsiadis, S.; Doumanis, G., Evaluation of sexual function in hypertensive men receiving treatment: a review of current guidelines recommendation. The Journal of Sexual Medicine 2011, 8, (9), 2405-2414.
- Shindel, A. W.; Althof, S. E.; Carrier, S.; Chou, R.; McMahon, C. G.; Mulhall, J. P.; Paduch, D. A.; Pastuszak, A. W.; Rowland, D.; Tapscott, A. H., Disorders of ejaculation: an AUA/SMSNA guideline. Journal of Urology 2022, 207, (3), 504-512.
- Gratzke, C.; Angulo, J.; Chitaley, K.; Dai, Y.-t.; Kim, N. N.; Paick, J.-S.; Simonsen, U.; Ückert, S.; Wespes, E.; Andersson, K. E., Anatomy, physiology, and pathophysiology of erectile dysfunction. The journal of sexual medicine 2010, 7, (1_Part_2), 445-475.
- Nudell, D. M.; Monoski, M. M.; Lipshultz, L. I., Common medications and drugs: how they affect male fertility. Urologic Clinics 2002, 29, (4), 965-973.
- Schlosser, J.; Nakib, I.; Carré-Pigeon, F.; Staerman, F. In Infertilité masculine: définition et physiopathologie, Annales d'urologie, 2007; Elsevier: 2007; pp 127-133.
- Benoff, S.; Cooper, G. W.; Hurley, I.; Mandel, F. S.; Rosenfeld, D. L.; Scholl, G. M.; Gilbert, B. R.; Hershlag, A., The effect of calcium ion channel blockers on sperm fertilization potential. Fertility and sterility 1994, 62, (3), 606-617.
- Brezina, P. R.; Yunus, F. N.; Zhao, Y., Effects of pharmaceutical medications on male fertility. Journal of reproduction & infertility 2012, 13, (1), 3.
- Kanwar, U.; Anand, R.; Sanyal, S., The effect of nifedipine, a calcium channel blocker, on human spermatozoal functions. Contraception 1993, 48, (5), 453-470.
- De Rosa, M.; Zarrilli, S.; Di Sarno, A.; Milano, N.; Gaccione, M.; Boggia, B.; Lombardi, G.; Colao, A., Hyperprolactinemia in men: clinical and biochemical features and response to treatment. Endocrine 2003, 20, 75-82.
- Tanrikut, C.; Schlegel, P. N., Antidepressant-associated changes in semen parameters. Urology 2007, 69, (1), 185. e5-185. e7.
- Baldwin, D.; Mayers, A., Sexual side-effects of antidepressant and antipsychotic drugs. Advances in Psychiatric Treatment 2003, 9, (3), 202-210.
- Dording, C. M.; Fisher, L.; Papakostas, G.; Farabaugh, A.; Sonawalla, S.; Fava, M.; Mischoulon, D., A double-blind, randomized, pilot dose-finding study of maca root (L. meyenii) for the management of SSRI-induced sexual dysfunction. CNS neuroscience & therapeutics 2008, 14, (3), 182-191.
- Montejo, A. L.; Llorca, G.; Izquierdo, J. A.; Rico-Villademoros, F., Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients. Journal of Clinical Psychiatry 2001, 62, 10-21.
- Erdemir, F.; Atilgan, D.; Firat, F.; Markoc, F.; Parlaktas, B. S.; Sogut, E., The effect of sertraline, paroxetine, fluoxetine and escitalopram on testicular tissue and oxidative stress parameters in rats. International braz j urol 2014, 40, 100-108.
- Montejo, A. L.; Montejo, L.; Navarro-Cremades, F., Sexual side-effects of antidepressant and antipsychotic drugs. Current opinion in psychiatry 2015, 28, (6), 418-423.
- Safarinejad, M. R., Sperm DNA damage and semen quality impairment after treatment with selective serotonin reuptake inhibitors detected using semen analysis and sperm chromatin structure assay. The Journal of urology 2008, 180, (5), 2124-2128.
- Althof, S. E.; McMahon, C. G.; Waldinger, M. D.; Serefoglu, E. C.; Shindel, A. W.; Adaikan, P. G.; Becher, E.; Dean, J.; Giuliano, F.; Hellstrom, W. J.; Giraldi, A.; Glina, S.; Incrocci, L.; Jannini, E.; McCabe, M.; Parish, S.; Rowland, D.; Segraves, R. T.; Sharlip, I.; Torres, L. O., An Update of the International Society of Sexual Medicine's Guidelines for the Diagnosis and Treatment of Premature Ejaculation (PE). Sex Med 2014, 2, (2), 60-90.
- Taylor, M. J.; Rudkin, L.; Bullemor-Day, P.; Lubin, J.; Chukwujekwu, C.; Hawton, K., Strategies for managing sexual dysfunction induced by antidepressant medication. Cochrane Database of Systematic Reviews 2013, (5).
- Rosen, R. C.; Marin, H., Prevalence of antidepressant-associated erectile dysfunction. Journal of Clinical Psychiatry 2003, 64, 5-10.
- Panidis, D.; Rousso, D.; Skiadopoulos, S.; Panidou, E.; Mamopoulos, M., Evaluation of semen parameters in man with hyperprolactinemia induced by metoclopramide. Archives of andrology 1997, 39, (3), 237-242.
- Howes, O. D.; Wheeler, M. J.; Pilowsky, L. S.; Landau, S.; Murray, R. M.; Smith, S., Sexual function and gonadal hormones in patients taking antipsychotic treatment for schizophrenia or schizoaffective disorder. Journal of Clinical Psychiatry 2007, 68, (3), 361-367.
- Chen, S. S.; Shen, M. R.; Chen, T. J.; Lai, S. L., Effects of antiepileptic drugs on sperm motility of normal controls and epileptic patients with long-term therapy. Epilepsia 1992, 33, (1), 149-153.
- Isojärvi, J.; Löfgren, E.; Juntunen, K.; Pakarinen, A.; Päivänsalo, M.; Rautakorpi, I.; Tuomivaara, L., Effect of epilepsy and antiepileptic drugs on male reproductive health. Neurology 2004, 62, (2), 247-253.
- Herzog, A. G., Disorders of reproduction in patients with epilepsy: primary neurological mechanisms. Seizure 2008, 17, (2), 101-110.
- Lossius, M. I.; Taubøll, E.; Mowinckel, P.; Mørkrid, L.; Gjerstad, L., Reversible Effects of Antiepileptic Drugs on Reproductive Endocrine Function in Men and Women with Epilepsy—A Prospective Randomized Double-Blind Withdrawal Study. Epilepsia 2007, 48, (10), 1875-1882.
- Rättyä, J.; Turkka, J.; Pakarinen, A. J.; Knip, M.; Kotila, M.; Lukkarinen, O.; Myllylä, V.; Isojärvi, J., Reproductive effects of valproate, carbamazepine, and oxcarbazepine in men with epilepsy. Neurology 2001, 56, (1), 31-36.
- Webber, M. P.; Hauser, W. A.; Ottman, R.; Annegesr, J. F., Fertility in persons with epilepsy: 1935–1974. Epilepsia 1986, 27, (6), 746-752.
- Ocek, L.; Tarhan, H.; Uludag, F. I.; Sariteke, A.; Kose, C.; Colak, A.; Zorlu, F.; Zorlu, Y., Evaluation of sex hormones and sperm parameters in male epileptic patients. Acta Neurol Scand 2018, 137, (4), 409-416.
- Isojärvi, J. I.; Taubøll, E.; Herzog, A. G., Effect of antiepileptic drugs on reproductive endocrine function in individuals with epilepsy. CNS drugs 2005, 19, 207-223.
- Oliva, S. U.; Scarano, W. R.; Okada, F. K.; Miraglia, S. M., Harmful effects of carbamazepine on the postnatal development of the rat ventral prostate. Reproductive Biology and Endocrinology 2012, 10, 1-15.
Figure 1.
Illustration of different pharmacological agents with obesogenic activity discussed in this review classified according to the ATC/DD Index (https://www.whocc.no/atc_ddd_index/). Molecular structures retrieved from ChemSpider and PubChem.
Figure 1.
Illustration of different pharmacological agents with obesogenic activity discussed in this review classified according to the ATC/DD Index (https://www.whocc.no/atc_ddd_index/). Molecular structures retrieved from ChemSpider and PubChem.
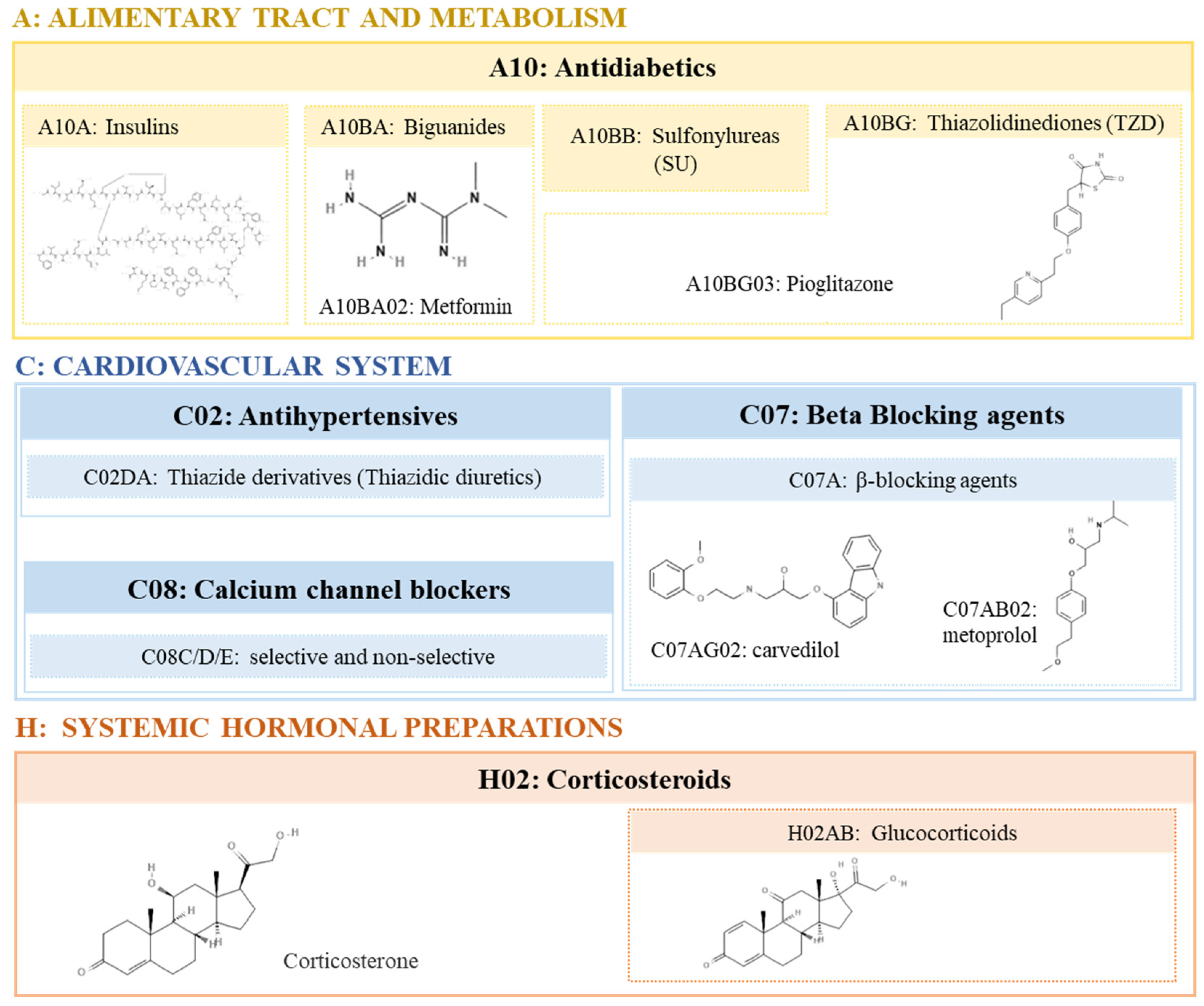
Figure 2.
Illustration of the different psychotropic pharmacological agents with obesogenic activity discussed in this review classified according to the ATC/DD Index (https://www.whocc.no/atc_ddd_index/). Molecular structures retrieved from ChemSpider and PubChem.
Figure 2.
Illustration of the different psychotropic pharmacological agents with obesogenic activity discussed in this review classified according to the ATC/DD Index (https://www.whocc.no/atc_ddd_index/). Molecular structures retrieved from ChemSpider and PubChem.
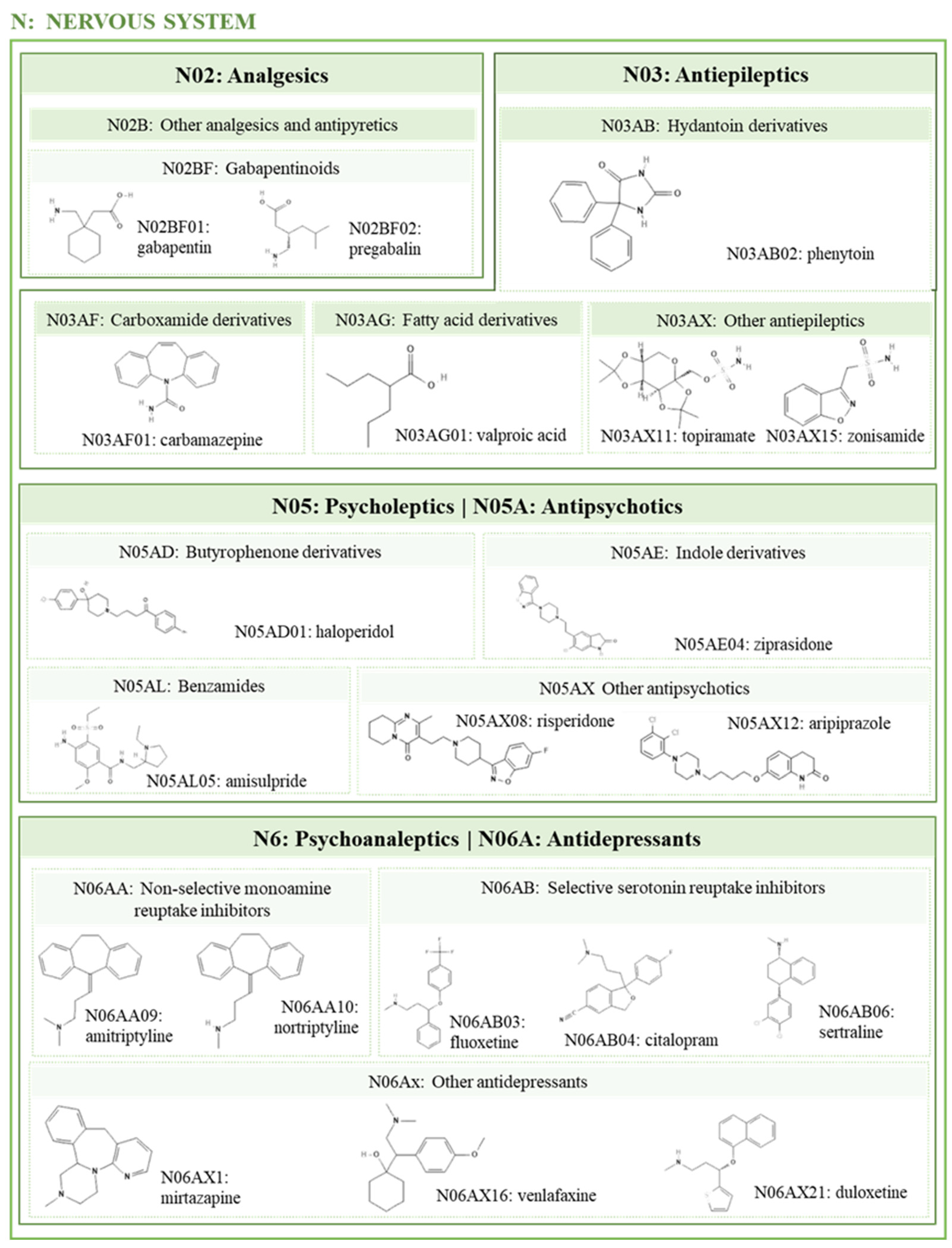
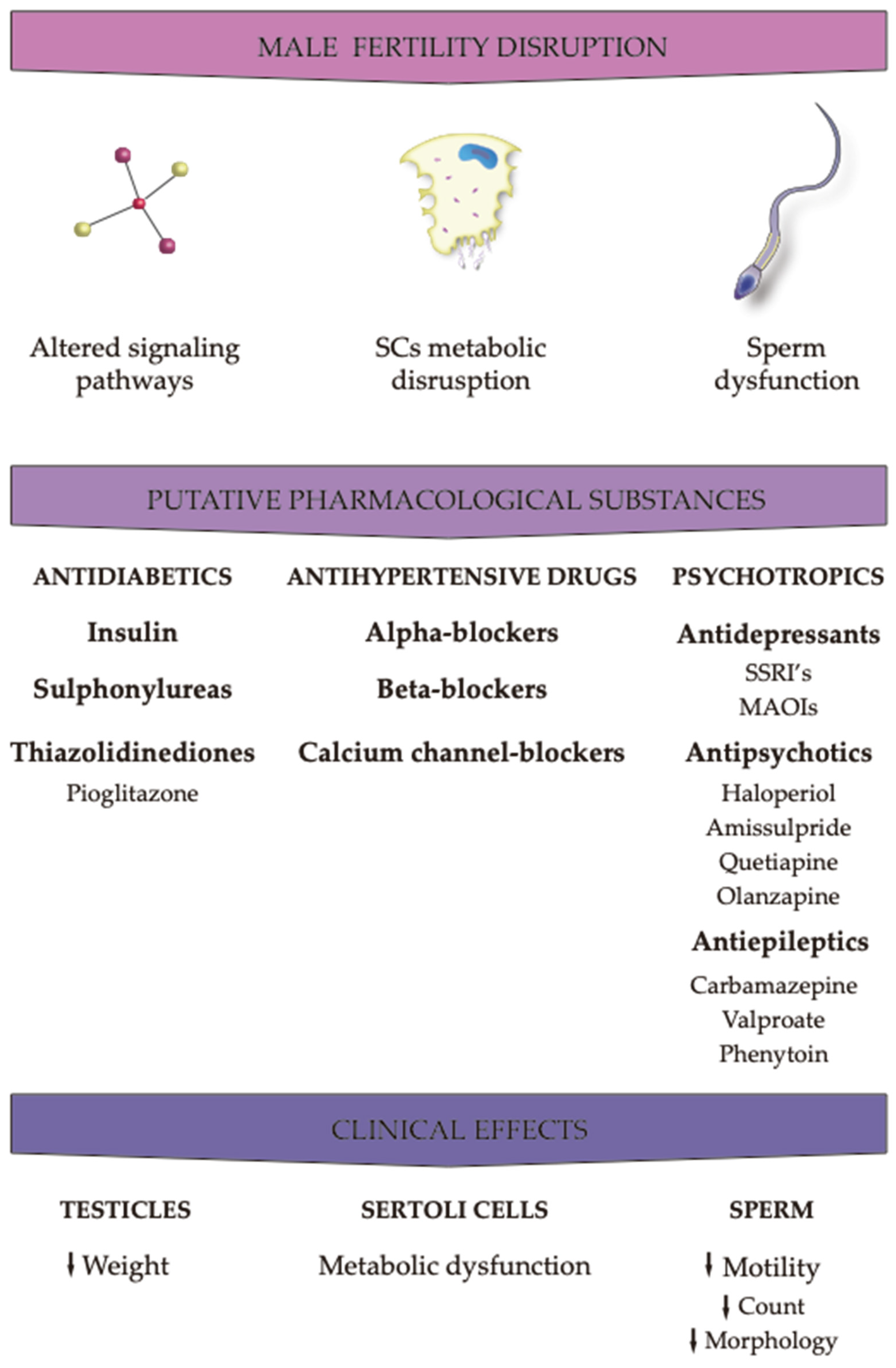
Figure 3.
Effects of the different pharmacological agents on male fertility parameters.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



