
Submitted:
02 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
While typically exhibiting characteristic features, fungal infections can sometimes present in an unusual context, having improbable localization (eyelid, face, joint), mimicking other skin diseases such as eczema, psoriasis, or mycosis fungoides, and appearing with unexpected color, shape, or distribution.
The emergence of such a challenging clinical pictures is attributed to complex interplay of host characteristics (hygiene, aging population), environment (climate change), advances in medical procedures, and agent factors (fungal resistance, species emergence).
We aim to provide a better understanding of unusual epidemiological contexts and atypical manifestations of fungal superficial diseases, knowing that there is no pre-established clinical guide for these conditions.
Keywords:
Atypical mycosis
; tinea incognito
; Tinea corporis
; Onychomycosis
; Dermatophytes
; mycosis fungoides
; Majocchi's disease
1. Introduction
Superficial mycosis is often difficult to identify and have various differential diagnosis especially at an early stage [1]. Misdiagnosis can easily occur when the lesions appear in unexpected appearances, including at unusual ages, previously unaffected geographical areas, atypical body locations, or even unlikely contexts. In addition, uncommon cases are related to unpredictable course (short-term course), local or systemic treatments, and auto-medication [2], leading to dermatitis characterized by high percentage of relapses [3]. Superficial mycosis can adopt atypical presentation [3,4] especially among immunosuppressed individuals [5], and the diagnosis is often delayed because of lack of suspicion [6]. Dermatophytes often go undetected, resulting in continued spread of the fungus within individuals and to other susceptible individuals. [7]. When atypical clinical features are present, tinea incognito is known to mimic several disorders, such as rosacea, cutaneous lupus erythematosus, and granuloma annulare [8]. If a stubborn skin condition doesn't respond to usual treatments, or if its appearance seems unusual, re-evaluating the patient is crucial to rule out a potential fungal pathogen [9]. Atypical presentation is often marked by the virulence of fungal species, extensive forms, unpredictable course, nonspecific histopathological findings, and frequently unsuccessful cultivation [6.2]. Due to the atypical presentations of superficial fungal infections in keratinization disorders, which can closely resemble other skin conditions, achieving a correct diagnosis can be complex and require careful consideration [10]. Despite advances in culture techniques, special strains, and molecular identification of fungi, history and clinical diagnosis remain paramount [1,9]. To the best of our knowledge, no narrative review has been carried out evaluating the spectrum of atypical mycosis.
2. Factors contributing in atypical presentations
The emergence of such a challenging clinical pictures is attributed to complex interplay of host, environment, and agent factors [5,11].
2.1. Atypical epidemiological context
The change in prevalence of fungi causing atypical disease can be linked to the geographic location, to the exposure to an important amount of spores due to warm and humid climate, and hosts characteristics (culture, habits, migration) [12].
- Environmental factors
Fungi are found universally. However, the ecological landscape plays a crucial role in shaping the fungal threat. Their abundance and virulence potential fluctuate across different niches and geographic areas, especially with dermatophytes serving as a prime example, which is more common in tropical regions [13,14].
some fungi are worldwide spread while other rare pathogens are located in specific areas. In Bangladesh and Inda, superficial mycoses are masked by overlapping symptoms from diseases like tuberculosis, chronic inflammation, and malignancies. This underdiagnosis and underreporting paint an incomplete picture of the true fungal burden. Studies in India shed light on how some fungal infections, like "connubial dermatophytosis" in spouses and extensive "tinea corporis" in infants, thrived within the close quarters of families [5,15].
2.1.1. Fungal factors
Superficial mycoses are caused by yeasts, dermatophytes, and less commonly by molds. The number of fungal cases is constantly increasing and many new fungal pathogens are being identified. Fungi can be classified as primary or opportunistic pathogens based on their virulence [12].
Trichophyton rubrum is the fungus most frequently involved in atypical forms [16,17,18], associated with a strong tendency for dissemination and that are usually refractory to topical and systemic therapy [17]. In addition, uncommon cases of Trichophyton tonsurans infection have been previously reported [19], causing atypical tinea corporis in Algeria where this species is not commonly recovered. Furthermore, this dermatophyte can occasionally be responsible of tinea pseudo-imbricata, manifesting as multiple concentric annular erythemas [20,21], especially when long-term topical steroids misuse [5,22,23].
Trichophyton indotineae is another lesser-known species that has recently been reported as a difficult-to-treat dermatophytosis[24].
Interestingly, Nannizzia nana, reported previously as Microsporum nanum has no specific clinical picture [11], and induces onychomycosis of toenails as well as skin lesions. Moreover, improved diagnostic tools have led to an increase in identified Nannizzia nana infections, suggesting that misdiagnosis was previously masking the true prevalence rather than a low infectivity of this agent [2].
Traditionally, diagnoses focused on well-known fungal culprits. But with improved tools (PCR, MALDI-TOF MS), we're now recognizing a wider spectrum of less common fungal species capable of causing superficial mycoses.
Usually, zoophilic species are characterized by more pronounced inflammation than anthropophilic species, with the formation of vesicles [25,26]. Some fungi can act opportunistly causing severe unusual infections [3]. Candida parapsilosis association with environmentally acquired skin ulcers can resemble cutaneous sporotrichosis [27]. While Malassezia species typically reside harmlessly on the skin, they can trigger inflammatory responses leading to symptomatic skin conditions (folliculitis, dandruff, eczema) in both humans and animals [28].
Rare fungi are also responsible of unexpected skin conditions, Prototheca sp are ubiquitous, commonly isolated from grass, soil, and water, this species is responsible of cutaneous infections [29]. Emmonsia crescens formerly known as Chrysosporium parvum var. crescens is a saprophytic soil fungus transmited by inhalation and inducing rare pulmonary disease and exceptional cutaneous localization [29].
Finally, the immune status can specifically play a role in the virulence of some fungal species. Immunosuppression in Blastomycosis has a reduced impact on dissemination of the disease, contrary to histoplasmosis and coccidioidomycosis in which immunosuppression is often necessary and the diagnosis is less ambiguous [30].
2.1.2. Host factors
Numerous host factors are increasing the susceptibility to fungal infection, such as comorbidities (obesity, diabetes mellitus, immunosuppressive disorders, poor circulation) [12], socioeconomic background, lifestyle changing, poor hygiene (sweaty clothing and bedding), poverty, and occupational status [5,11,12,31]. Even diet has been suggested as a factor that contributed to adult kerion associated with onychomycosis in vegetarians individual [32].
The origin of the patients can influence de clinical picture, a surprising highly significant occurrence of tinea capitis due to anthropophilic species was revealed among Spanish school children from African immigrant population [33]. Population migration affects the spread and diversity of fungi [34,35]. Emergent fungi, like Trichophyton tonsurans, are increasing in Europe, particularly due to the growing immigrant population [33,36], and beyond, illustrates how human-animal interactions, including pets, farm, and wild animals can reshape the fungal landscape [11].
Some superficial fungal infections are uncommon in certain age groups. The clinical pictures of superficial fungal infections in children can be diverse, non-distinctive, and somewhat confusing. Tinea capitis is the most frequent dermatomycosis in childhood, however, it is rare in newborns [36,37,38]. There have been unusual cases reported when the newborn had a thick, scaly adherent mass on their scalp without any suppurations or alopecia.
Tinea capitis is unusual in adults, nevertheless, it seems that this mycosis is not so rare, especially in immunocompetent women who spent their childhood in Africa [34]. Similarly, Tinea unguium and tinea pedis have been rarely reported in prepubescent children [39,40,41].
Onychomycosis is more common among adults and elderly with an increasing prevalence with age due to reduced nail growth accompanied by an increase in nail plate thickness. Thumb sucking is a notable behavior in newborns and infants, inducing maceration of the fingers and increasing the risk of oral flora infection to the nail folds and the hyponychium [42].
- Trauma
There are several types of trauma, including accidental trauma, self-induced trauma, non-conventional treatment, modern medical procedures.
Dermatophytosis could be probably initiated by physical trauma, serving as gateway for Trichophyton rubrum [8]. Reportedly, a woman who shaved her legs developed a skin condition that was misdiagnosed as mycosis fungoides, but was in fact a dermatophytosis [1]. Furthermoemre, an adult healthy female presented several axillary and perineal ulcers following incision and drainage of slowly growing nodular lesions over a one-year duration. She admitted to shaving her axillae and pubic region with a safety razor several times. Both culture and histology revealed an important presence of Aspergillus [43].
Traditionally thorn injuries are produced by Sporothrix schenckii, yet Candida parapsilosis has also been implicated following rose thorn injury in an immunocompetent patient, and the wound healed following itraconazole medication [27].
Ear Trauma Some traumas are induced by the patient’s habits; such as ear self-cleaning leading to otomycosis. Moreover, self-inducted injuries are already described in schizophrenia (Figure 1), and Aspergillus flavus otomycosis has been linked to ear self-mutilation [44,45].
Cutaneous Injury, agricultural trauma, traffic injuries, and orthopaedic trauma have all been linked to primary cutaneous aspergillosis [46,47,48]; Usually, the symptoms appear within one month of injury [48]. Moreover, burn wounds can be infected by Aspergillus species [46,49], Panke et al. Described characteristic " Aspergillus fruiting bodies" on the skin of a burned patient [50].
- Underlying diseases
Atypical mycosis is conditioned by the host susceptibility to fungal infection. Associated cutaneous, systemic, or iatrogenic disorders along with immune dysfunction should be taken in account in individuals with recalcitrant dermatophyte infections [15,51,52,53]. Atopic persons and those infected with zoophilic fungi tend to have more inflammation [26]. Atypical morphology of superficial fungal infections is a characteristic feature of keratinization disorders [10].
A delayed keratin scaling in atopic disease may facilitate the persistence of fungal infection [54], mimicking the appearance of eczematous lesions, and potentially leading to misdiagnosis [54,55], moreover, ichthyosis create a favorable environment for fungal growth and proliferation, since abundant keratinized cells provides a rich source of nutrients for dermatophytes [54,56].
Additionally, the more alkaline environment found on the skin of atopic eczema patients enhances the release of allergens from Malassezia sympodialis. Nanovesicles from Malassezia sympodialis and host exosomes induce cytokine responses– novel mechanisms for host-microbe interactions in atopic eczema [57].
When patient originally present with generalized typical skin condition like psoriasis or localized nevus the dermatologist assume that all lesions are the same, while association with fungal is still possible [58], Widespread tinea corporis with psoriasis vulgaris can lead to diagnosis confusion [58].
Reportedly, Rheumatoid arthritis lesions on prednisone led to a leg rash due to Purpureocillium lilacinum [59].
Atypical, invasive, and disseminated clinical presentations are more likely seen in immunocompromised patients [60,61], including those with HIV infection [60,62,63]. A disseminated Fusarium oxysporum infection with skin localization on both calves was diagnosed in a 32-year-old female with relapsing B-acute leukemia during induction chemotherapy [64]. Atypical inflammatory bullous lesions due to Trichophyton mentagrophytes has been described in HIV individuals [65], additionally, dermatophytosis mimicking Kaposi’s sarcoma has been documented in HIV patients [66,67]. Deficiency in caspase recruitment domain containing protein 9 (CARD9) has also been shown to be associated with more severe presentations of tinea infections [68]. Primary and metastatic malignancies may occasionally mimic or coexist with cutaneous fungal infections [69].
Consequently, recognizing uncommon fungal infections as well as fungal cases presenting clinical patterns with other dermatoses is critical for immunocompromised patients to ensure prompt and adequate management [59,60].
- Iatrogenic factors
There are some treatment alternatives that are lengthy, aggressive, or have significant negative effects [1.] It is highly probable that cosmetic products altered the quantity and/or quality of local sebum secretion, creating an environment that promotes infection by Microsporum canis [70].
The self-medication habit of indiscriminately using steroids, antibiotics, and zinc during the COVID-19 pandemic may have contributed to the dysbiosis of the gut microbiota, which in turn caused immune suppression and elevated the risk of mycosis and specifically mucorales [71].
- Misuse of treatment
The majority of misdiagnosed dermatophytosis are mistaken for bacterial infections or infected eczema and are consequently treated with various antibiotics and corticosteroids without effect [72].
Previous treatment with topical corticosteroids might justify some patients being erroneously considered as having LE [73]. A report on patient having pityriasis versicolor with clinical and mycological evidence of palmar lesions and fingernail onychomycosis which was strongly related to mishandling of Malassezia furfur infection [74].
Misuse of treatments can contribute to fungal resistance and potentially mask the true nature of a typical mycosis [1]. Several drugs may be involved, namely:
- Indigenous drugs [5]
- Medical drugs
- Corticosteroids
Typical ringworm aspect is masked by previous topical and/or systemic corticosteroids, alongside concomitant application of emollients [2,75,76]. Unusual manifestations of tinea corporis are known as "Tinea incognito" which is commonly used for steroid-modified cases of dermatophytosis, although later reports also show the use of tacrolimus and pimecrolimus for dermatophytosis [5].
Non-diabetic Covid-19 patients, particularly those who were given high doses of steroids for a long time developped Mucormycosis [71].
- Deferoxamine
Individuals receiving deferoxamine medication are especially vulnerable to developing mucormycosis [71].
- Antithymocyte globulin
Antithymocyte globulin was associated with skin aspergillosis among patient treated for agranulocytosis [77].
- Immunosuppressive drugs
IL17-inhibitor, tocilizumab, pimecrolimus, and tacrolimus have been linked to tinea incognito [5,78,79].
- Chemotherapy
Docetaxel chemotherapy administred to breast cancer patient induced Candida guillermondii onycholyse associated to exudate and oedema [80]. (Figure 2)
- Medical procedures
- Bandage/gauze
cutaneous Aspergillosis are typically found when gauze or bandages come into contact with the skin [81].
- Ventilators
Patients on oxygen/ ventilator support may be incriminated in severe cases of nosocomial mucormycosis [71].
- Catheters
A cutaneous lesion behind a venous catheter's transparent dressing was reported by Smith and Wallace [82].
Skin necrosis around the removed Hickman line site followed by other similar lesions around the arterial and venous cannulation sites [83].
- Injection
Unexpectedly, a 37-year-old woman developed granulomatous lesions on the cheek caused by Trichophyton rubrum after facial injection with hyaluronic acid [84].
- organ transplantation
3. Atypical context of infection
A surprising nosocomial tinea corporis has been described in a HIV patient hospitalized for Cryptococcus meningitis, after an unexpected report of cat transmission [86]. (Figure 3)
Unexpected otomycosis among earmold wearers is possible since the device is offering an occlusive environment facilitating fungi growth. On the other hand, self-mutilation in schizophrenia could lead to surprising filamentous otomycosis [44,87]. (figure)
Tattoos can have several inflammatory complications including allergic contact dermatitis, lichenoid, photo-induced and granulomatous reactions, pseudolymphoma, and skin cancers, or infectious complications such as bacterial infections (Leprosy, syphilis, pyoderma, mycobactriosis, cutaneous tuberculosis), viral infections (molluscum contagiosum, hepatitis B and C, herpes simplex), and fungal infections (dermatophytosis, sporotrichosis) [88]. Injury to the skin caused by tattoo needle, or contaminated ink, or the use of non-sterile instrument, and/or contact with contaminated animal or human source are the principal etiologies of this particular form of the dermatophytosis. Tinea may appear either early during the first two months following tattoos, or later in a healed tattoo [88]. The main dermatophytes isolated from tattoos included Trichophyton rubrum, Microsporum canis, Trichophyton tonsurans, Epidermophyton floccosum, and Microsporum gypseum [89].
Penile shaft dermatophytosis is a rare form described among Indian male’s wearers of ‘lengoty’ the semi-occlusive dress can unexpectedly facilitate the fungal growth [90].
4. Atypical clinical features
Emerging atypical and unusual presentations are widely described in developing countries [5].
Atypical mycosis infections should be treated promptly and properly, otherwise they can become chronic and require oral antifungal medication [91].
In tinea incognito the lesion on the face can be eczema-like, rosacea-like, or discoid lupus, while the trunk and the extremities lesions can be impetigo-like [92,93], examples of atypical dermatophytosis are summarized in Table 1.
Tinea incognito is a rare form of dermatophytosis compared to the more common presentations [1], It often presents with multiple lesions at various sites, exhibiting varying degrees of inflammation [94].
Atypical cases of Microsporum canis were described as nummular eczema, erythema multiforme, granuloma annulare, granuloma faciale, and lymphocytic infiltration of the skin [95], pityriasis rosea, seborrheic dermatitis [95,96,97], lupus erythematosus [98,99] In a multi-center study including 283 tinea incognito patients in Korea, the following diagnoses had been incorrectly applied to tinea incognito patients: nonspecific eczema, atopic dermatitis, contact dermatitis, seborrheic dermatitis, diaper dermatitis, intertrigo, nummular dermatitis, stasis dermatitis, psoriasis, lupus erythematosus, urticaria, and lichen simplex chronicus [100]. Another study presenting 200 cases of tinea incognito revealed that the most common resembling dermatoses were psoriasis, rosacea, impetigo, discoid dermatitis, lupus erythematosus, polymorphic light eruption, seborrheic dermatitis, lichen planus, and erythema migrans [101].
Uncommon retinochoroiditis secondary to fungal infection of the skin caused by Tinea corporis has also been reported [102], the patient had extensive reddish color erythematous plaque-like skin lesions over the abdomen and back.
- -
- Psoriasis-like
Both large plaques with silvery scales and less infiltrated lesions with fewer scales have been seen in cases resembling psoriasis [58,103], the lesions were commonly located on lower extremities, trunk, or palms [103,104,105].
Tinea corporis caused by Trichophyton rubrum was reported to mimic a flare-up of psoriasis under treatment with IL17-inhibitor Ixekizumab [78]. Moreover, pustular psoriasis-like tinea incognito due to Trichophyton rubrum was described [76]. Furthermore, a case of Microsporum canis in elderly woman was initially diagnosed as psoriasis and seborrhoeic dermatitis [106].
- -
- Atopic-like
Trichophyton rubrum has been incriminated as possible trigger in flares of atopic dermatitis [107].
Patient’s atopic dermatitis infection can also be exacerbated by chronic dermatophytosis [108].
- -
- Eczema-like
Eczema and tinea, despite being distinct skin conditions, share the common feature of causing dry, inflamed skin. These presentations are seen in immunosuppressed as well as immunocompetent individuals [94]. In Italy 82% of the tinea incognito observed were eczema-like presentations [79]. Dutta et al. also found that eczema-like lesions were the most common [109].
Atzori et al. observed eczema-like tinea as the most common atypical manifestation of tinea [110].
A case of a fungal skin infection initially mistaken for eczema was later diagnosed as biopsy-confirmed CTCL and successfully treated with antifungal medication [1].
- -
Seborrheic dermatitis-like tinea capitis that was misdiagnosed in an old Chinese man, samples taken from scalp, and nails revealed the presence of Trichophyton rubrum concluding to an association of tinea capitis and tinea unguium [111].
An elderly woman presented seborrhoeic dermatitis which was diagnosed later as a dermotophytosis due to Microsporum canis [106].
- -
- Acne-like
Malassezia fungi can also cause folliculitis, primarily affecting sebum-rich areas like the face, chest, and back. This condition mimics acne but doesn't produce comedones [112].
Although sterile folliculite-like lesions is currently found on torso or back of Behcet’s disease patients, lesions acne-like due to Trichophyton rubrum were described on the back of a patient receiving corticosteroids therapy [113]. (Figure 4)
- -
- Lupus Erythematosus like
The misdiagnosis of tinea mimicking Lupus Erythematous (LE) has been reported in the literature, the great majority of cases are tinea faciale with some exceptions involving the trunk. Some cases coexist with true LE [73]. Tinea is confirmed by the presence of hyphae in systemic LE-like eruptions, the dermatophytes responsible for such infections are varied and include Trichophyton rubrum, Trichophyton mentagrophytes, Trichophyton tonsurans, Trichophyton verrucosum and Microsporum canis [98,99,114,115].
- -
- Sweet’s syndrome-like
A 53-year-old female with a 2-month history of a painful itchy rash on her face, had previously presented with multiple edematous pseudo-vesicular papules that appeared suddenly on the face and shoulders, followed by a febrile upper respiratory tract infection simulating sweet’s syndrome [13].
- -
- Ichtyosis-like
Despite the prevalence of both dermatophytosis and ichthyosis in clinical practice, their concomitant occurrence is seldom documented [54].
- -
- Keloid-like
A 53-year-old man presented with a rapidly growing, plaque on the right forearm. He worked as a seasonal olive harvester and may have unknowingly been scratched by an olive branch. The lesion progressed to keloid-like or brainy form. Mycological study identified Trichophyton rubrum [116].
- -
- Leproy-like
Hypopigmented scaly patches on body, were reported to simulate leprosy [15].
- -
- Rosea-like
Rosacea-like tinea incognito is also a documented atypical form of dermatophytosis [23].
Figure 4.
A) Acne-like lesions on the back of Behcet’s patient B) Trichophyton rubrum culture after skin scraping.
Figure 4.
A) Acne-like lesions on the back of Behcet’s patient B) Trichophyton rubrum culture after skin scraping.
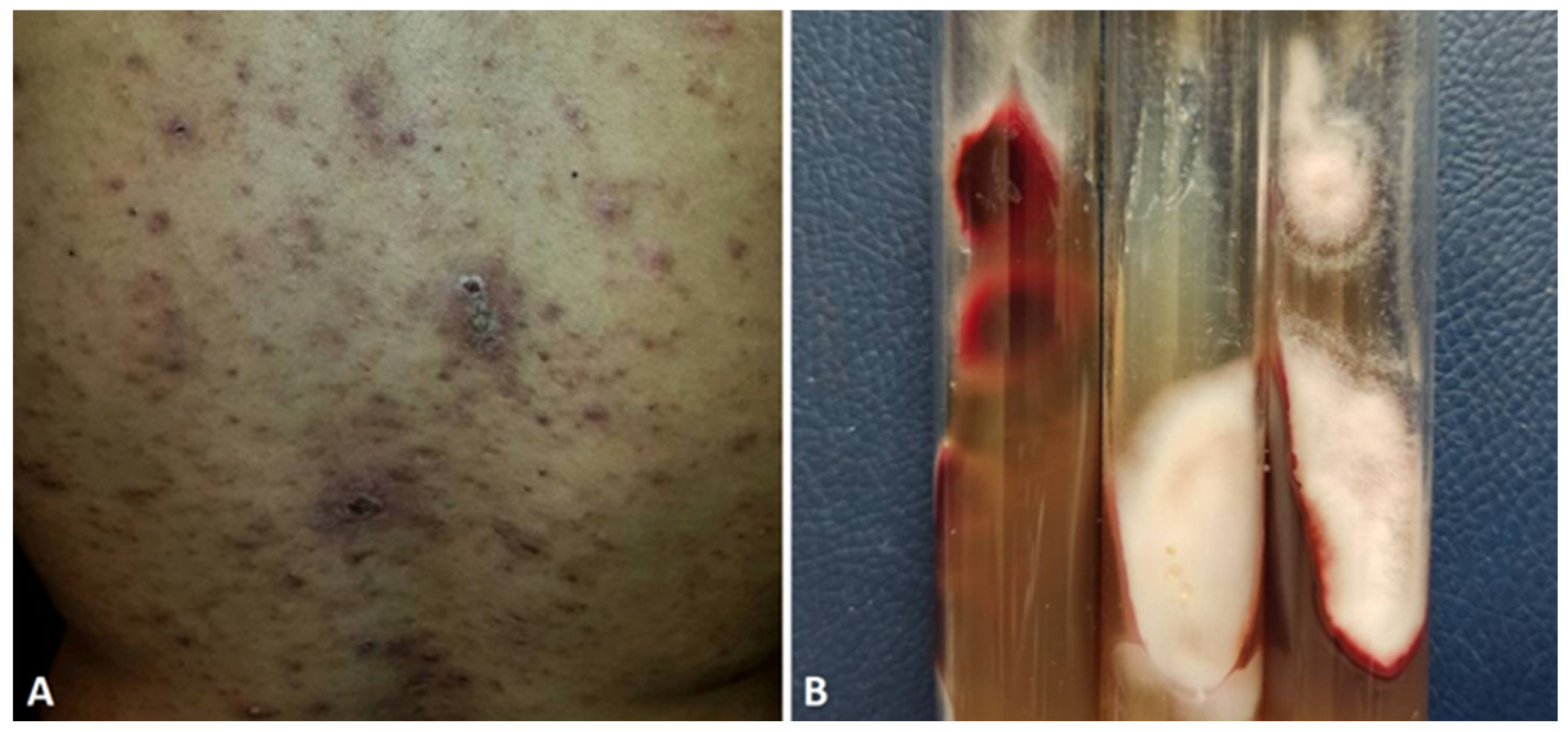

Table 1.
Examples of atypical clinical presentations.
| Description | S/Age | Localization | Fungi | Country | Reference |
| psoriasis-like | - | Body Palms Flexures |
T. rubrum T.mentagrophytes M.gypseum |
India | [105] |
| Trunk, groin, buttocks | T.rubrum | India | [103] | ||
| Lower extremities | T.rubrum | USA | [104] | ||
| M/68 | - | - | Slovenia | [117] | |
| Legs | M. canis | Serbia | [58] | ||
| Body All Nails |
T.rubrum | Switzerland | [78] | ||
| Trunk, lower extremities, toenails | T. rubrum | New Zealand | [118] | ||
| Inverse psoriasis-like | Intertrigous areas | Candida sp | India | [119] | |
| Eczema-like | - |
T.mentagrophytes T.rubrum |
Korea | [79] | |
| Face | T.rubrum | India | [109] | ||
| M/36 | Arms Inguinal region |
Trichophyton eboreum | Switzerland | [120] | |
| F/64 | Hand | Trichosporon asahii | Japan | [101,121] | |
| Seborrheic dermatitis –like | - | Face Scalp |
T. rubrum T.mentagrophytes T.tonsurans M.gypseum |
India | [105] |
| M/77 | Scalp Nails |
T. rubrum | China | [111] | |
| Face Neck |
India | [5] | |||
| Erythema-like | Torso | - | Grenada | [68] | |
| lupus erythematosus-like | - | Face | [73,98,99] | ||
| Furoncle-like | - | Body | T. tonsurans | [105] | |
| Acne-like | M/29 | Back | T.rubrum | Algeria | [113] |
| Prurigo-like | - | T. rubrum | India | [105] | |
| Ichthyosis-like | Body | T.menta | India | [105] | |
| Contact dermatitis-like | M/12 | Right eyebrow | T.menta | Chile | [122] |
| Impetigo-like | M/41 | Right forearm | T. tonsurans | Japan | [123] |
| Allergic-like dermatitis | M/31 | Trunk, upper limbs | T. verrucosum | [124] | |
| Cellulite-like | 4 cases | - | USA | [41] | |
| Pityriasis rubra pilaris | M/54 | Trunk, shoulders, upper arms | Malassezia sp | USA | [125] |
| Myccosis fungoides-like | F/62 | Right chin, Right elbow | - | USA | [1] |
4.1. Atypical localization
Superficial fungal infections of the hair, skin and nails are a major cause of morbidity in the world [126].
Improbable localizations of mycoses can lead to misdiagnosis. Depending on different clinical manifestations, dermatophytosis is classified by the anatomical region where it typically occurs, such as tinea unguium, tinea pedis, tinea cruris, tinea corporis, and tinea capitis [9].
It is important to consider a dermatophyte infection when dealing with dermatosis that may be in an atypical area given the age of the patient, or have an appearance that may be uncommon for a fungal infection [9], examples of atypical localizations of superficial mycosis are depicted in Table 2
When the host is immunocompromised, the infecting organism may be an opportunistic fungal organism or a dermatophyte that would generally not be expected to be recovered from that site [9].
Trichophyton violaceum was responsible of a concomitant tinea of the scalp and eyebrows in 62-year-old diabetic woman [9].
Trichophyton verrucosum often causes inflammatory, deeply infiltrating lesions located on the head, face, hands and forearms, but aphlegmasic superficially spreading lesions affecting other parts of the body have also been reported [127].
Atypical dematophytosis progression without clearing center encourage inflammatory, crusting forms, thickness of corny layer and uncommon anatomical localizations including sebaceous glands, skin folds, and vellus hair follicle [5].
- -
- Facial involvement
Children including infants with facial involvement and adults with tinea capitis have become a frequent clinical presentation in India [5]. In children malassezia-related conditions, atypical facial involvement, particularly on the temples, can be observed, and fine, white, flaky scales may also be present [112].
An erythematous nodule on the lip, due to Trichophyton rubrum was reportedly following a trauma in the same area [128].
Ocular involvement due to dermatophytes can present as eyelid infestation [9].
- -
- Flexual involvement
Infection located at joint can be attributed to psoriasis, there is little documentation regarding the unusual pityriasis versicolor localizations of the body like the scalps, the face, the arms, palms, legs, soles, flexural areas, areolae, penile involvement [129].
The term tinea axillaris has been used only a few times in the literature (Bell), it is considered as a variant of intertriginous tinea, a unique non-occupational Trichophyton verrucosum tinea axillaris has been described [127].
Unusual tinea versicolor of the axilla can appear as well-demarcated erythematous lesion with minimal scale [130].
- -
- Ungueal involvement
Toenails are 25 times more likely to be infected than finger nails as the causative molds are ubiquitous fungi seen in soil, water, and decaying vegetations [131], fingernail localization is more confusing.
- -
- Genital involvement
The base of the penis is most often affected by dermatophytes, followed by the shaft and the prepuce [94].
Atypical pityriasis versicolor forms include penile involvement (Aljabre2) [129], and genitalia [132,133].
Tinea infection has been uncommonly described on the penile shaft [90].
- -
- no evident localization
Allergic dermatophytid is a distant reaction to dermatophytes, it is an allergic rash that will disappear once the original infection has been treated.
Table 2.
Examples of atypical localizations of superficial mycosis.
| Infection location | Presentation/context | Agent | Reference |
| palms and fingernails | Dischromatic lesions | Malassezia sp | [74] |
| Penis | Malassezia sp | [129] | |
| Axilla | Eryth and papular rash | Malassezia sp | [130] |
| Eyebrows | Tinea of the scalps and eyebrows in diabetic elderly | T.violaceum | [134] |
| Right eyebrow | Erythematous lesion | T.mentagrophytes | [122] |
| Scalp and eyebrow | Tinea of the Scalp and Left eyebrow | M.canis | [135] |
| Eyelid and skin | Upper eyelid swelling for 6 months HIV patient with disseminated lesions |
Rhinosporidium sp | [136] |
| Lip | Dermatophyte presenting as a verrucous nodule of the lip | T.rubrum | [128] |
| Penis | infection of the penis/after wearing penile clothe | M.canis | [90] |
4.2. Atypical progression and extension of the lesions
Most of the fungal cutaneous presentations are typically benign and easily treated (Brown) [68].
Dissiminated forms are not linked to age, therefore an extensive form in neonatal patient was attributed to dermatophyte [137].
Reportedly, deep and extensive forms can indicate a more serious underlying immunodeficiency [9,60,68,138], including those with HIV infection [60,62,63]. However, a case of onychomycosis involving all 10 fingers of an immunocompetent male with no co-morbid conditions was caused by the filamentous, Aspergillus niger [131].
The failure of patients and clinicians to recognize a fungal infection early may lead to more extensive, severe, and difficult-to-treat disease [2,139]. Indeed, the delay in diagnosis and application of topical corticosteroids also contributed to the lesion generalization [106].
The clinical description of tinea incognito is highly variable. Compared with the lesions of tinea corporis, the lesions seen in tinea incognito are generally less erythematous and scaly, less well-defined, and generally more extensive [92,93].
It is hypothesized that extensive forms are related to some fungal species. For an instance Microsporum canis transmitted from animals has stronger pathogenicity which make the skin lesion more generalized [106]. Additionally, widespread tinea corporis are resistant to oral antifungals and may not respond well to them, particularly if immunosuppression is present [51].
elderly woman with well-controlled diabetes mellitus presenting with a six-month history of erythema with yellow crusts on her scalp and extensive erythematous patches with scales on the body skin caused by Microsporum canis. The patient’s condition was initially diagnosed as psoriasis and seborrheic dermatitis [106].
fungal rashes are usually harmless and respond well to topical antifungal treatments, more extensive or persistent manifestations could signal an underlying immune deficiency that requires further investigation [68].
Widespread tinea corporis are recalcitrant and could be poorly responsive to oral antifungals, especially if immunosuppression is associated [51], and they present as slightly scaly eruption
Majocchi’s granuloma, also known as nodular granulomatous perifolliculitis, results from fungal penetration throughout the hair follicle to the dermal or subcutaneous tissue, causing a suppurative folliculitis [92].
Tinea incognito refers to cutaneous fungal infections that have lost their typical morphological features due to the use of calcineurin inhibitors or corticosteroids [92,93], the delay in diagnosis and application of topical corticosteroids also contribute to the lesion generalization (Yang) [106]. The clinical presentation of tinea incognito is highly variable. Compared with the lesions of tinea corporis, the lesions seen in tinea corporis are generally less erythematous and scaly, less well-defined, and generally more extensive. The lesion on the face can be eczema-like, rosacea-like, or discoid lupus, while the trunk and the extremities lesions can be impetigo-like [92,93].
The fungal species can also contribute to the spread of the lesions, some extensive forms of pityriasis were attributed to M.globosa whose pathogenicity has been attributed to high lipophilic activity due to the levels of lipases and esterases [101,140]. Moreover, Microsporum canis which is transmitted from animals has stronger pathogenicity which makes the skin lesion more generalized [106], for an instance, a tinea Capitis by Microsporum canis in an elderly diabetic female with gradually extensive infection have been described, dermatophyte Infection included scalp, whole trunk, groin and all extremities with severe pruritus and malaise. The patient’s condition was initially diagnosed as psoriasis and seborrhoeic dermatitis and treated with econazole nitrate and triamcinolone acetonie cream without improvement [106]. Furthermore, a reported extensive tinea corporis du to Trichophyton schoenleinii in an 80-year-old woman on her forearms, thighs, legs, buttocks and trunk, was mimicking parapsoriasis, without scalp involvement [141].
Widespread tinea corporis and unguium affecting also both axillary regions. Trichophyton verrucosum was isolated as the causative agent [127].
Immunocompromised patients (diabetes mellitus, chronic liver and kidney disorders, transplants) are also more likely to develop deep dermatophytosis, a rare disorder characterized by invasion of dermatophytes into the dermis and subcutaneous tissue, rather than just keratinized skin [61].
5. Atypical clinical forms
5.1. Atypical onychomycosis
Reports of onychomycosis in prepubescent children are rare [39,40], this rarity has been attributed to the differences in nail plate structure, less exposure to trauma, and faster linear nail growth. Oral colonization by pathogenic yeasts and finger suckling could be advanced as potential risk factors for the unexpected neonatal onychomycosis. Uncommon cases were attributed to Candida albicans, Candida parapsilosis, Candida tropicalis, Trichophyton rubrum, and Fusarium oxysporum [42,142,143].
Toenail changes are frequently observed among the subset of patients with vascular disease and Chronic leg ulcer, nail modifications may also be the result of microangiopathy and subsequent chronic ischemia. Onychomycosis can be also confused with dystrophic toe-nails from repeated low-level trauma [144].
Uncommon onychomycosis clinical features such as onycholysis, oedema, and exsudate have been linked to chemotherapy in breast cancers patients [80]. Melanonychia of fungal origin with brown or black pigmentation of the nail unit is a relatively rare clinical sign and can mimic subungual melanoma [145,146,147,148,149]. Exemples of atypical onychomycosis are summarized in Table 3.
Both Aspergillus and other molds are an emerging cause of onychomycosis, mainly affecting the toenails of diabetic individuals [146]. The most common cause of melanonychia are dematiaceous, melanin-producing molds, Scytalidium dimidiatum and Alternaria sp [145,146]. Moreover, subungual onychomycosis due to Aspergillus niger can mimic a glomus tumor [150].
Furthermore, blackening of Nails with pits, could be a result of co-existance of psoriasis and onychomycosis [151].
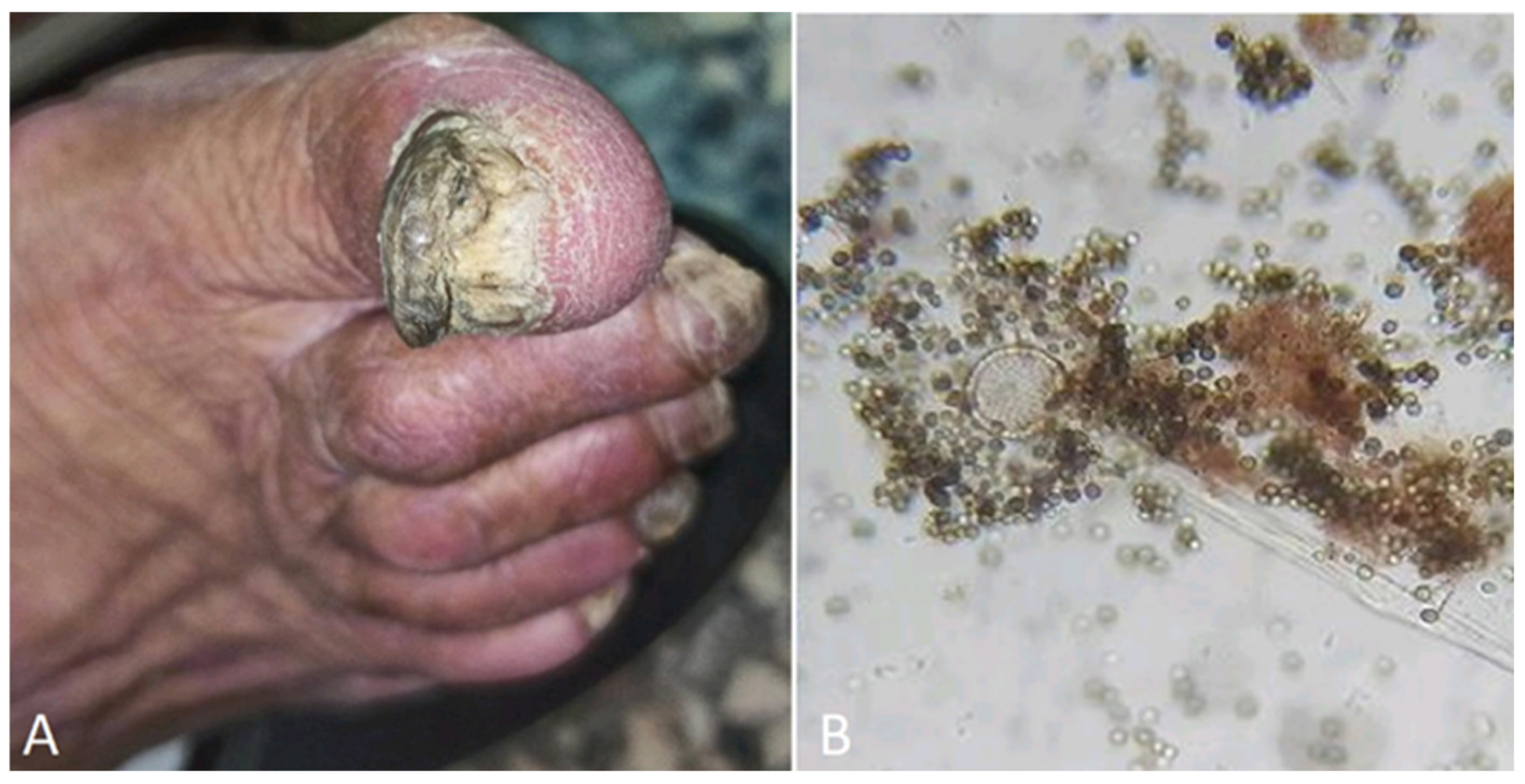
Additional rare clinical deformities include the so-called: “pincer nail deformity,” known as “incurvated nail”, which is a transverse overcurvature of the nail [152]. Although, the underlying pathogenesis is not clearly understood, this condition can hide an onychomycosis [152]. Moreover, onychogryphosis, known as ram’s horn nail, is a rare disorder observed in old people. It is characterized by dark thickening of the nail plate, Aspergillus niger has been implicated as a possible causal agent [149]. (Figure 5)
Even the well-known yeast Candida albicans, rather than any other Candida species, often clinically presents as a misleading paronychia, or onycholysis [142], some of the unusual forms of onychomycosis are depicted in table
Table 3.
Examples of atypical onychomycoses.
| Clinical presentation | Clinical details | Causative agent | Reference |
| Brown pigmentation | Usually diffuse lesions |
Aspergillus niger Alternaria alternata Scytalidium dimidiatum |
[145,149] |
| Longitudinal melanonychia | Distal lesions |
Trichophyton rubrum Candida humicola Candida albicans Candida parapsilosis Scytalidium dimidiatum Alternaris sp Exophiala sp Aspergillus niger |
[89,145,153] |
| Distal and lateral subungual onychomycosis |
Alternaria alternate Scytalidium sp |
[154] | |
| Black pigmentation | Superficial coloration Periungual inflammation Proximal nail |
Aspergillus niger | [146] |
| Onychodystrophy | Nail discoloration | [149] | |
| Onycholysis | greenish-black discolorations | Candida parapsilosis | [155] |
| Subungual onychomycosis | mimicking a glomus tumor |
Aspergillus niger | [150] |
| Onychodystrophy | All fingernails and toenails involved | Cladosporium sp | [7] |
Figure 5.
A) Onychogryphosis in a 75-year-old patient B) Aspergillus niger microscopy after culture.
Figure 5.
A) Onychogryphosis in a 75-year-old patient B) Aspergillus niger microscopy after culture.
5.2. Atypical hair mycosis
Tinea capitis is a common condition among children, nevertheless, it has been unexpectedly described in newborn [36,37,38], and adults [32]. The increasing of adult tinea capitis is probably linked to population aging and immune system modifications induced by diseases such as malignancy, diabetes mellitus, long-term use of glucocorticoids and immunosuppressant [111].
Compared with children adult tinea capitis is more often associated with another superficial mycosis caused by anthropophilic fungi such as Trichophytotn rubrum, Trichophyton violaceum, and Trichophyton tonsurans [111].
Trichophyton rubrum Seborrheic-like lesions of the scalp was described in a 77-year-old Chinese male patient [111], the patient experienced pruritic scaly scalp, with growing hair loss during 6 months. In addition, the patient was suffering from and associated tinea pedis and onychomycosis [111]. Furthermore, tinea capitis can be confused with alopecia areata [144].
- Piedra
These infections are prevalent in tropical regions and appear as soft, attached nodules on scalp hair, but they can also affect the axilla, pubis, and beard areas. These nodules can easily be mistaken for nits, hair casts, or other hair conditions [112,156]. The differential diagnosis of piedra includes chronic intertrigo, hair casts, monilethrix, nits, pediculosis capitis, pediculosis pubis, tinea capitis, trichomycosis axillaris, trichoptilosis, and trichorrhexis nodosa.
5.3. Atypical skin mycosis
5.3.1. Atypical tinea faciei
Tinea faciei is uncommon and often misdiagnosed at first, it is frequently aggravated by sun exposure. It may also present as a kerion (fungal abscess). Therefore, it is a disease nearly exclusively found in adult males. The presence of this kind of lesion on the same areas in women and children are classified as tinea faciei [157].
Tinea barbae is an uncommon superficial dermatophyte infection of the beard and moustache areas, it can mimic many other skin disorders iododerma, contact dermatitis, perioral dermatitis, and actinomycosis [157].
Like tinea capitis, tinea barbae should be treated with oral therapy, systemic anti-fungal medications are able to penetrate the infected hair shaft whereas topical therapies cannot [157].
5.3.2. Atypical breast localization (Tinea mammae)
Tinea mammae (fungal infection of the breast) has been rarely reported [159]. These are unusual locations to find a tinea infection, particularly in someone with a healthy immune system [9].
Similarly, unilateral tinea mammae simulating atopic eczema with gradual increasing size due to Trichophyton rubrum has been described in an elderly man [159]. On the other hand, bilateral and symmetrical dermatophytosis can be found in adults [161], one of the possible explanation of bilateral Tinea mammae might be the use of a contaminated bra [161].
A 28-year-old female presented with a prominent, reddish lesion in her left breast that had grown during the preceding three months and became nodular with yellowish discharge. Surprisingly, the mycological examination was compatible with Trichophyton violaceum [162].
5.3.3. Atypical tinea mannum, and tinea pedis
Tinea pedis and tinea manuum were previously considered uncommon fungal infections in children before puberty [41]. Emerging evidence from dermatological studies indicates that fungal infections of the feet and hands are more prevalent in children than previously thought [39,40]. Moreover, asymptomatic tinea pedis in children has been documented [165].
Some occupations involve handling fruits and vegetable and the contact with these products without wearing gloves could be a predisposing factor for mycosis [131,147]. (Figure 8)
Tinea manuum is less common than tinea pedis [25,26]. Typically, the infection affects one hand and both feet, or both hands and one foot [26].
Both fungal infections and hand eczema can manifest with similar symptoms, including red, itchy rashes. Hand eczema is commonly bilateral and symmetrical, whereas tinea manuum typically affects just one hand. Moreover, tinea manuum can present with nail involvement, while hand eczema nails are not involved. Tinea pedis, also known as athlete's foot, manifests as itchy, red, and inflamed areas on the feet. These lesions can appear on the soles (vesicular type), sides (moccasin type), or between the toes (interdigital type) [166].
Well-circumscribed inflammatory vesicular lesions have been described on the palm of a 2-year-old patient, the child's brother had tinea capitis, with a history of animal contact [167]. This leads us to conside r all clinical findings present in the patient's environment.
5.3.4. Atypical tinea corporis
Tinea corporis is characterized by an annular plaque with advancing, raised erythematous, scaling borders surrounding a clear center [5,68]. Extensive tinea corporis occurs mainly in patients with underlying immune disorders such as HIV infection, or following systematic and topical use of steroids [137,168]. Immunosuppressed patients, including transplant recipients, cancer patients, and those on immunosuppressive therapy, are susceptible to deeper dermatophyte infections beyond the superficial layers [169].
Tinea corporis is a common and often overlooked infection that can also co-occur with other skin conditions [117]. Occasionally, tinea corporis is simulating conditions, including psoriasis, pityriasis rosea, secondary annular syphilis, nummular eczema, lupus erythematosus, granuloma annulare [73,144,170]. The morphology, the facial distribution, and the recurrence of the fungal lesions at regular intervals after sun exposure are misleading signs of cutaneous lupus erythematous [73].
Additionally, tinea corporis is able to Simulate Leukocytoclastic Vasculitis (LCV) [170], which is an inflammatory small vessel diseases provoked by circulating immune complexes, following drug exposure or acute infections. Moreover, the histopathological characteristics of early-onset LCV are also visible in other conditions such as scurvy and tinea corporis [170].
Consequently, an immunosuppression should be investigated and excluded in any patient with an atypical tinea corporis presentation [60].
5.3.5. Tinea recidivans
It represents another uncommon clinical entity, that describes the presence of lesions at the periphery of a healed skin part [94].
6. Atypical type of lesions
6.1. Lesions configuration
6.1.1. Annular lesions
Unusual large annular plaques can be found on scalp, body, and flextures. The responsable species are usualy, Trichophyton rubum, Trichophyton mentagrophytes and Microsporum gypseum [105].
Typically, tinea presents as circular patches. However, in patients with ichthyosis, the lesions often appear less distinct and well-defined [54].
Tinea Imbricata, called "tokelau" and "chimberê" in Brazil is a unique chronic variant of tinea corporis, caused by T. concentricum and characterized by impressive itchy squamous concentric circles, affecting large parts of the body [126]. Unexpectedly, Trichophyton tonsurans infection manifested as multiple concentric annular erythema in a Japanese documented case report [20]. Nonetheless, cases of concentric rings evocative of tinea imbricata in secondary syphilis exist in the literature [171].
6.1.2. Nummular lesions
Atypical cases of Microsporum canis were clinically described as nummular eczema, granuloma annulare, and granuloma faciale [95].
Trichophyton verrucosum has been reported to cause lesions clinically resembling nummular dermatitis in a Korean case report [172].
6.2. Lesions color
6.2.1. Erythematous lesions
Erythematous lesions are non-specific for any particular dermatological condition and frequently accompany atypical superficial mycoses. This lack of specificity can pose diagnostic challenges. For instance, a 64-year-old woman with chronic myelocytic leukemia who developed erythematous hand lesions resembling eczema during chemotherapy for blastic crisis was ultimately diagnosed with Trichosporon asahii infection based on mycological results [121].
Different types of fungal erythemas can occur on various skin locations. Examples include:
- -
- Erythematous skin macules on arms and groin areas: This can be caused by Trichophyton species,
- -
- Erythema annulare on the trunk and upper limbs: This can be caused by Trichophyton verrucosum in adult males [124].
- -
- Multiple erythema annulare with slightly scaly plaques on the torso: This presentation can be associated with HIV infection, as seen in a woman diagnosed with the condition [68].
- -
- Erythema multiforme: This can be attributed to Microsporum canis dermatophytosis, as described by Alteras et al. [95].
6.2.2. Dyschromic lesions
Skin hypochromic lesions can be due to normal aging, environmental factors (cumulative sun exposure and microtrauma), inherited diseases (Ash leaf spots in tuberous sclerosis), nutritional deficiencies such as Kwashiorkor (protein malnutrition condition), iron or vitamin B12 deficiencies.
Inflammatory causes such as vascular diseases, Bier’s spots, Pityriasis alba, post viral exanthema, skin procedures (cryotherapy, dermabrasion), cosmetic inflammation, skin bleaching agents (hydroquinone), and burns.
Possible differential diagnosis of PV will include pigmentary disorders such as vitiligo, idiopathic guttate hypomelanosis and melasma; scaling is usually absent in these disorders. Other diseases to exclude are pityriasis alba, Hansen’s disease, pityriasis rosea, pityriasis rotunda, hypo- or hyperpigmented mycosis fungoides, secondary syphilis, lentigo solaris, piebaldism and post-inflammatory hyperpigmentation [173].
Pityriasis alba often presents with small, hypopigmented patches on the face. The excessive-use of corticosteroid when treating eczema may induce this skin disease. In addition to other factors, sun and wind exposure, nutritional deficiencies (copper, iron), are also frequently incriminated
The presence of greenish-yellow fluorescence under Wood’s light would strongly suggest tinea versicolor, while a negative result, associated to the absence of yeast on tape stripping examination, solidify the diagnosis of pityriasis alba [174,175]. (Figure 9)
Pityriasis rotunda is a rare disorder of keratinization characterized by a persistent, hyperpigmented or hypopigmented, geometrically perfect circular patches of dry ichthyosiform scaling with no inflammatory changes. Pityriasis rotunda lesions may be associated with malignancies and liver diseases and it can be misdiagnosed as PV. In addition, some of the diseases also caused by Malassezia such as seborrheic dermatitis and confluent and reticulated papillomatosis of Gourgerot and Carteaud may co-exist and or resemble PV; thus making diagnosis more difficult [176].
Although less typical, Malassezia can also target the face, scalp, and genital areas. Facial and penile lesions are relatively frequent in infants and immunocompromised individuals [177].
6.2.3. Black lesions
Tinea nigra commonly affects the palms of hands and the soles of feet [112]
Tinea nigra is an infrequent superficial fungal infection caused by a mold that exclusively affects the stratum corneum. It manifests as dark patches on the palms and soles, typically with minimal scaling. [112]. The lesions have a noticeably darker border.
Due to its dark coloration, tinea nigra can sometimes be mistaken for a melanocytic lesion. Dermoscopy can be used to distinguish between these two entities, as tinea nigra exhibits brown strands or "pigmented spicules." [178,179]. This fungal infection is caused by various molds, including Phaeoannellomyces, Hortaea, or Exophiala werneckii [112].
Black superficial lesions are including melanocytic lesions such as melanoma-like lesions, and black eschars caused by Mucorales. Moreover, a documented atypical case report of black dot ringworm lesions was due to Trichophyton tonsurans [123].
6.3. Lesions morphology
6.3.1. Urticaria
A possible coincidental association between urticaria and dermatophytosis was identified by the presence of Epidemophyton floccosum in skin scarping. However, Urticarial lesions of undefined origin should be considered for a clinical picture of Id reaction and patients should be carefully investigated for superficial fungal infections [180].
6.3.2. Purpuric lesions
6.3.3. Papular lesions
Papular presentation is current in dermatophytosis. Due to the atypical presentations of superficial fungal infections in keratinization disorders, which can closely resemble other skin conditions, achieving a correct diagnosis can be complex and require careful consideration [10].
For an exemple, both tinea corporis and congenital ichthyoses are common skin diseases. The association between these two conditions is plausible due to the immune and barrier defects present in ichthyoses [10].
On the other hand, fungal manifestations are defined as atypical when the inflammatory component is more severe, presenting follicular papules and pustules [14,170].
Fulminant papulopustular tinea corporis caused by Trichophyton mentagrophytes was described [75].
Interestingly, Pityriasis rosea is a common viral exanthem, described as a limited papulo-squamous eruption mimicking the common papular tinea corporis [182].
6.3.4. Plaques
An 89-year-old woman presented with plaque-like lesions, accompanied with pustules and desquamation on the back and front of the trunk for approximately one year, until the mycological examination revealed a tinea incognito [183].
6.3.5. Vesicular/Bullous lesions
Fungal infections can manifest as vesicular or even bullous tinea, where erythematous dermatitis presents with annular lesions and raised, blister-like borders [184,185].
Inflammation further promotes fungal colonization and can sometimes lead to vesicle formation at the edges of the affected area [25,26]. Additionally, the intense inflammation caused by the zoophilic fungus Trichophyton mentagrophytes, combined with a significant delayed-type hypersensitivity reaction, are believed to contribute to the development of vesicles or bullae in some cases.
Furthermore, secondary blistering may occur in cases of severe inflammation. The intensity of inflammation is influenced by the type of fungus, the patient's immune system, and the degree of follicular involvement [186].
The atypical clinical cases are generally indicated by the large size of the lesion, and the presence of pustules in the central region [8]. Atypical very inflammatory bullous lesions due to Trichophyton mentagrophytes have been described in HIV individuals [65]. In addition, pustular manifestations are seen at the border of inflammatory erythematous lesions of tinea [94].
A 30-year-old woman with no underlying disease presented with an inflammatory, pustular, and crusted plaque on the pubis and vulva after shaving, which led to a diagnosis of tinea incognito caused by Trichophyton mentagrophytes [187].
Interestingly, the pustular forms of tinea incognito can mimic the appearance of pustular psoriasis especially among immunosuppressed individuals, so it is important to consider it as a possible diagnosis [118].
6.3.6. Abscesses
Reported coexisting diseases that were suspected of inducing an immunosuppression and favoring dermatophytes abscesses are malignancy, renal and liver transplantation, CARD9 deficiency, collagen disease, nephrotic syndrome, bullous pemphigus, and diabetes mellitus. Most reports described unsuspected pre-existing superficial mycosis [188]. Some of the abscessed dermatophytosis are cited in the Table 4.
Multiples abscess of the lower extremities were provoked by Trichophyton rubrum [169].
6.3.7. Nodular
Rare fungal nodular lesions are attributed to Sporothrix sp . Besides, fish tank granuloma is a rare skin infection caused by Mycobacterium marinum. It occurs after exposure of skin abrasions to contaminated water or infected fish. The most common presentation is a solitary nodule, often with sporotrichoid spread [6].
- Majocchi’s granuloma
In rare cases, topical steroid overuse can weaken local immunity, potentially allowing dermatophytes to invade the dermis. This can lead to pruritic papules, pustules, and nodules forming in areas with existing dermatophytic infections [94]. This invasive clinical picture is called "Majocchi granuloma". (Figure 10)
Immunocompromised patients (diabetes mellitus, chronic liver and kidney disorders, transplants) are also more likely to develop deep dermatophytosis, a rare disorder characterized by invasion of dermatophytes into the dermis and subcutaneous tissue, rather than just keratinized skin [61].
Granulomatous lesions due to Trichophyton mentagrophytes, and Trichophyton rubrum [196] have mainly be described.
Moreover, atypical case of Microsporum canis was described as granuloma annulare, and granuloma faciale [95].
Bizarrely, atypical presentation of Majocchi's granuloma with multiple non-tender erythematous folliculo-centric nodules and central pustulation on the lower extremities has been documented. There was no history of trauma or application of topical corticosteroids over the affected area, and the patient denied shaving the affected area [197]. Some of the reported nodular forms of dermatophytosis are depicted in Table 5.
6.3.8. Ulcerative lesions
Cutaneous mucormycosis may be a primary disease following skin barrier break or may occur as a consequence of hematogenous dissemination from other sites, and the outcome of the disease is strictly dependent on the patients’ conditions. Primary cutaneous mucormycosis can involve the subcutaneous tissue as well as the fat, muscle and fascial layers [204].
Patient’s skin necrosis resembling Pyoderma gangrenosum, especially if they are chronically immunocompromised, diabetic, severely malnourished, or treated with broad-spectrum antibiotics, should suggest the possibility of mucormycosis [83].
6.3.9. Tumoral lesions
Fungal infections can coexist with or mimic malignancies, regardless of the site of the lesion, namely, the skin [1], nails, and scalp [25,89,145].
A pediatric patient with Trichophyton verrucosum infection presented with lesions clinically resembling a vascular tumor, likely a consequence of the exceptionally severe and diverse clinical presentations of zoophilic species [205].
There are a few documented cases of dermatophytosis mimicking Kaposi's sarcoma reported in HIV-positive patients [66,67,206]. A study highlighted that one month after stopping HIV medications, erythematous lesions steadily increased and spread to the legs, feet, abdomen, and buttocks of the patient, marking an extensive form of dermatophytosis [67].
Exceptionally, melanized (dematiaceous) fungal infections due to Nigrograna mackinnonia can also simulate skin cancer in organ transplant recipients [207].
7. Conclusion
The rise in atypical superficial mycoses is a complex puzzle with multiple contributing factors. To avoid diagnostic pitfalls, it's crucial to re-evaluate patients with chronic inflammatory dermatosis who do not improve with standard treatment or exhibit unusual clinical presentations, such as severe inflammation or extensive lesions.A thorough history and physical examination can help rule out potential fungal infections.
References
- Babakoohi S, McCall CM. Dermatophytosis Incognito Mimicking Cutaneous T-Cell Lymphoma. Cureus. 2022 Jun 10;14(6):e25809. [CrossRef]
- Abraham AG, Kulp-Shorten CL, Callen JP. Remember to consider dermatophyte infection when dealing with recalcitrant dermatoses. South Med J. 1998 Apr;91(4):349-53. [CrossRef]
- Vest BE, Kraulan K. Malassezia furfur. StatPearls, May 22, 2023.
- Narang T, Dogra S, Kaur I. Co-localization of Pityriasis versicolor and BT Hansen's disease. Int J Lepr Other Mycobact Dis. 2005 Sep;73(3):206-7.
- Dogra S, Narang T. Emerging atypical and unusual presentations of dermatophytosis in India. Clin Dermatol Rev 2017;1:S12-8. [CrossRef]
- Trčko K, Plaznik J, Miljković J. Mycobacterium marinum hand infection masquerading as tinea manuum: a case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2021 Jun;30(2):91-93. [CrossRef]
- Nikitha S, Kondraganti N, Kandi V (2022) Total Dystrophic Onychomycosis of All the Nails Caused by Non-dermatophyte Fungal Species: A Case Report. Cureus 14(9): e29765.
- Turra N, Navarrete J, Magliano J, Bazzano C. Follicular tinea faciei incognito: the perfect simulator. An Bras Dermatol. 2019;94(3):372-4. [CrossRef]
- Gupta AK. Uncommon localization or presentation of tinea infection. JEADV (2001) 15, 7–8. [CrossRef]
- Szlávicz E, Németh C, Szepes É, Gyömörei C, Gyulai R, Lengyel Z. Congenital ichthyosis associated with Trichophyton rubrum tinea, imitating drug hypersensitivity reaction. Med Mycol Case Rep. 2020 ;29:15-17. [CrossRef]
- Gnat S, Lagowski D, Nowakiewicz A. Major challenges and perspectives in the diagnostics and treatment of dermatophyte infections. Journal of Applied Microbiology 129. [CrossRef]
- Ahasan HN, Noor N. Fungal infection: a recent concern for physician. BJM Vol. 33 No. [CrossRef]
- Viera MH, Costales SM, Regalado J, Alonso-Llamazares J. Inflammatory Tinea Faciei Mimicking Sweet's Syndrome. Actas Dermosifiliogr. 2013;104(1):75–76. [CrossRef]
- Nicola A, Laura A, Natalia A, Monica P. A 20-year survey of tineafaciei. Mycoses. 2010;53:504-8. [CrossRef]
- Bishnoi A, Vinay K, Dogra S. Emergence of recalcitrant dermatophytosis in India. Lancet Infect Dis 2018; 18: 250. [CrossRef]
- Ramonda S, Salerni G, Macia A et al. Micosis superficiales más frecuentes en pacientes infectados por HIV. Rev Argent Dermatol 1994; 75: 34–35.
- Giudice MC, Szeszs MW, Scarpini RL et al. Clinical and epidemiological study in an AIDS patient with Microsporum gypseum infection. Rev Iberoam Micol 1997; 14: 184–187.
- Tsang P, Hopkins T, Jimenez-Lucho V. Deep dermatophytosis caused by Trichophyton rubrum in a patient with AIDS. J Am Acad Dermatol 1996; 34: 1090–1091. [CrossRef]
- Hryncewicz-Gwóźdź A, Beck-Jendroschek V, Brasch J, Kalinowska K, Jagielski T. Tinea capitis and tinea corporis with a severe inflammatory response due to Trichophyton tonsurans. Acta Dermato-Venereologica, 91 (2011), pp. [CrossRef]
- Ouchi TNagao K, Otuka T, Inazumi T. Trichophyton tonsurans infection manifesting as multiple concentric annular erythema. J Dermatol. 2005 Jul;32(7):565-8. [CrossRef]
- Suzuki T, Sato T, Horikawa H, Kasuya A, Yaguchi T. A Case of Tinea Pseudoimbricata Due to Trichophyton tonsurans Induced by Topical Steroid Application. Med Mycol J. 2021;62(4):67-70. [CrossRef]
- Garrido PM, Ferreira J, Filipe P. Disseminated tinea pseudoimbricata as the early warning sign of adult T-cell leukaemia/lymphoma. Clin Exp Dermatol. 2022 Feb;47(2):410-412. [CrossRef]
- Gorani A, Schiera A, Oriani A. Case report. Rosacea-like tinea incognito. Mycoses 2002;45:135-7.
- Chowdhary A, Singh A, Kaur A, Khurana A (2022) The emergence and worldwide spread of the species Trichophyton indotineae causing difficult-to-treat dermatophytosis: A new challenge in the management of dermatophytosis. PLoS Pathog 18(9): e1010795. [CrossRef]
- Hainer BL. Dermatophytes infections. American Family Physician 2003, 67(1):101-108.
- Noble SL, Forbes RC, Stamm PL. Am Fam Physician. Diagnosis and Management of Common Tinea Infections. 1998;58(1):163-174.
- Turkal N.W., Baumgardner D.J. Candida parapsilosis infection in a rose thorn wound. J Am Board Fam Pract. 1995;8(6):484–485.
- Saunders CW, Scheynius A, Heitman J (2012) Malassezia Fungi Are Specialized to Live on Skin and Associated with Dandruff, Eczema, and Other Skin Diseases. PLOS Pathogens 8(6): e1002701. [CrossRef]
- Pfaller MA, Diekema DJ Unusual Fungal and Pseudofungal Infections of Humans. JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2005, p. 1495–1504. [CrossRef]
- McBride JA, Sterkel AK, Matkovic E, Broman AT, Gibbons-Burgener SN, Gauthier GM. Clinical Manifestations and Outcomes in Immunocompetent and Immunocompromised Patients With Blastomycosis. Clin Infect Dis. 2021 ;72(9):1594-1602. [CrossRef]
- Salci TP, Salci MA, Marcon SS, Salineiro PHB, Svidzinski TIE, 2011. Trichophyton tonsurans in a family microepidemic. An Bras Dermatol 86: 1003–1006. [CrossRef]
- Xiujiao Xia, Huilin Zhi, Zehu Liu, Hong Shen. Adult kerion caused by Trichophyton rubrum in a vegetarian woman with onychomycosis. Clinical Microbiology and Infection, 2022. [CrossRef]
- Cuétara MS, Palacio A, Pereiro M, Noriega AR. Prevalence of undetected tinea capitis in a prospective school survey in Madrid: emergence of new causative fungi. Br J Dermatol 1998; 138: 658–660. [CrossRef]
- Dogra S, Uprety S. The menace of chronic and recurrent dermatophytosis in India: Is the problemdeeper than we perceive? Indian Dermatol Online J 2016;7:73-6. [CrossRef]
- AK, Mahajan R. Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review Indian Dermatol Online J. 2016;7:77–86. [CrossRef]
- Gilaberte Y, Rezusta A, Coscojuela C. Tinea capitis in a newborn infected by Microsporum audouinii in Spain. J Eur Acad Dermatol Venereol. 2003 Mar;17(2):239-40. [CrossRef]
- Offidani A, Simonchini C, Arzeni D et al. Tinea capitis due to Microsporum gypseum in an adult. Mycoses 1998; 41: 239–241. [CrossRef]
- Dell’Antonia M, Mugheddu C, Ala L, Lai D, Pilloni L, Ferreli C, Atzori L. Dermoscopy of tinea incognito. Mycopathologia. 2023 Aug;188(4):417-418. [CrossRef]
- Geary RJ, Lucky AW. Tinea pedis in children presenting as unilateral inflammatory lesions of the sole. Pediatr Dermatol 1999; 16: 255–258. [CrossRef]
- Gupta AK, Sibbald RG, Lynde CW et al. Onychomycosis in children: prevalence and treatment strategies. J Am Acad Dermatol 1997; 36: 395–402. [CrossRef]
- Sweeney SM. Inflammatory tinea pedis/manuum masquerading as bacterial cellulitis. Arch Pediatr Adolesc Med, 156 (2002), pp. 1149-1152. [CrossRef]
- Carvalho VO, Vicente VA, Werner B. Et.al. Onychomycosis by Fusarium oxysporum probably acquired in utero. Med Mycol Case Rep. 2014;6:58–61. [CrossRef]
- Tahir, C.; Garbati, M.; Nggada, H.A.; Terna Yawe, E.H.; Auwal, A.M. Primary Cutaneous Aspergillosis in an Immunocompetent Patient. J. Surg. Tech. Case Rep. 2011, 3. [CrossRef]
- Yassine M, Haiet AH. Self-injury in schizophrenia as predisposing factor for otomycosis. Medl Mycol Case Rep. 2018 May 3;21:52-53. [CrossRef]
- Merad Y, Derrar H, Belmokhtar Z, Belkacemi M. Aspergillus genus and its various human superficial and cutaneous features. Pathogen. 2021 May 23;10(6):643. [CrossRef]
- Anh-Tram, Q. Infection of burn wound by Aspergillus fumigatus with gross appearance of fungal colonies. Med. Mycol. Case Rep. 2019, 24, 30–32. [CrossRef]
- Ozer, B.; Kalaci, A.; Duran, N.; Dogramaci, Y.; Yanat, A.N. Cutaneous infection caused by Aspergillus terreus. J. Med. Microbiol. 2009, 58, 968–970. [CrossRef]
- Vitrat-Hincky, V.; Lebeau, B.; Bozonnet, E.; Falcon, D.; Pradel, P.; Faure, O.; Aubert, A.; Piolat, C.; Grillot, R.; Pelloux, H. Severe filamentous fungal infections after widespread tissue damage due to traumatic injury: Six cases and review of literature. Scand. J. Infect. Dis. 2009, 41, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.D.D.S.B.; Leitão, V.M.S.; Neto, M.A.C.D.S.; Maciel, L.B.; Filho, W.E.M.; Viana, G.M.D.C.; Bezerra, G.F.D.B.; Da Silva, M.A.C.N. Eco-epidemiologic study of emerging fungi related to the work of babacu coconut breakers in the State of Maranhao, Brazil. Rev. Soc. Bras. Med. Trop. 2014, 47, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Panke, T.W.; McManus, A.T.J.; McLeod, C.G.J. “Fruiting bodies” of Aspergillus on thee skin of a burned patient. Am. J. Clin. Pathol. 1978, 69, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Hubert JN, Callen JP. Recalcitrant tinea corporis as the presenting manifestation of patch-stage mycosis fungoides. Cutis. 2003 Jan;71(1):59-61.
- Hay RJ, Baran R, Moore MK, et al. Candida onychomycosis--an evaluation of the role of Candida species in nail disease. Br J Dermatol. 1988;118(1):47–58. [CrossRef]
- Jones HE, Reinhardt JH, Rinaldi MG. Acquired immunity to dermatophytes. Arch Dermatol 1974;109:840-8. [CrossRef]
- Freitas CF, Mulinari-Brenner F, Fontana HR, Gentili AC, Hammerschmidt M. Ichthyosis associated with widespread tinea corporis: report of three cases. An Bras Dermatol. 2013 Jul-Aug;88(4):627-30. [CrossRef]
- Thammahong A, Kiatsurayanon C, Edwards SW, Rerknimitr P, Chiewchengchol D. The clinical significance of fungi in atopic dermatitis. Int J Dermatol. 2020 Aug;59(8):926-935. [CrossRef]
- Ludwig RJ, Woodfolk JA, Grundmann-Kollmann M, Enzensberger R, Runne U, Platts-Mills TA, et al. Chronic dermatophytosis in lamellar ichthyosis: relevance of a T-helper 2-type immune response to Trichophyton rubrum. Br J Dermatol. 2001;145:518-21. [CrossRef]
- Gehrmann U, Rqazi KR, Johansson C, Hultenby K, Karlsson M, et al. (2011) Nanovesicles from Malassezia sympodialis and host exosomes induce cytokine responses– novel mechanisms for host-microbe interactions in atopic eczema. PLoS ONE 6: e21480. [CrossRef]
- Jankovic A, Binic I, Glgorijevic J, Jankovic D, Ljubenovic M, Jancic S. Mimicking each other psoriasis wit tinea incognito. Dermatol Sin. 2011;29(4):149-150. [CrossRef]
- Adel FWM, Bellamkonda V. Atypical Fungal Rash. Clin Pract Cases Emerg Med. 2019;3(2):166-167.
- Ziemer M, Seyfarth F, Elsner P, Hipler UC. Atypical manifestations of tinea corporis. Mycoses. 2007;50 Suppl 2:31-5. [CrossRef]
- Lanternier F, Cypowyj S, Picard C, et al.: Primary immunodeficiencies underlying fungal infections. Curr Opin Pediatr. 2013, 25:736-747. [CrossRef]
- Lowinger-Seoane M, Torres-Rodriguez JM, MadrenysBrunet N, Aregall-Fuste S, Saballs P. Extensive dermatophytoses caused by Trichophyton mentagrophytes and Microsporum canis in a patient with AIDS. Mycopathologia 1992; 120: 143–6. [CrossRef]
- Munoz-Perez MA, Rodriguez-Pichardo A, Camacho F, Rios JJ. Extensive and deep dermatophytosis caused by Trichophyton mentagrophytes var. interdigitalis in an HIV-1 positive patient. J Eur Acad Dermatol Venereol 2000; 14: 61–63. [CrossRef]
- Durand-Joly I, Alfandari S, Benchikh Z, Rodrigue M, Espinel-Ingroff A, Catteau B, Cordevant C, Camus D, Dei-Cas E, Bauters F, Delhaes L, De Botton S. Successful outcome of disseminated Fusarium infection with skin localization treated with voriconazole and amphotericin B-lipid complex in a patient with acute leukemia. J Clin Microbiol. 2003 Oct;41(10):4898-900. [CrossRef]
- Aly, R. & Berger, T. Common superficial fungal infections in patients with AIDS. Clin Infect Dis. 1996;22:S128–S132. [CrossRef]
- Crosby DL, Berger TG, Woosley JT, Resnick SD: Dermatophytosis mimicking Kaposi’s sarcoma in human immunodeficiency virus disease, Dermatologica, 182: 135–137, 1991. [CrossRef]
- Kwon KS, Jang HS, Son HS, Oh CK, Kwon YW, Kim KH, Suh SB. Widespread and invasive Trichophyton rubrum infection mimicking Kaposi's sarcoma in a patient with AIDS. J Dermatol. 2004 Oct;31(10):839-43. [CrossRef]
- Brown J, Carvey M, Beiu C, Hage R. Atypical Tinea Corporis Revealing a Human Immunodeficiency Virus Infection. Cureus. 2020 Jan 3;12(1):e6551. [CrossRef]
- Sun, J., Zhu, YZ., Shao, PP. et al. Malignant melanoma mimic fungal infection a case report. Diagn Pathol 17, 33 (2022). [CrossRef]
- Vozza A, Fiorentini E, Cutr FT, Di Girolamo F, Satriano RA. Tinea capitis in two young women: possible favouring role of hair styling products. JEADV (2001) 15, 357–377. [CrossRef]
- Kumar M, Sarma DK, Shubham S, Kumawat M, Verma V, Singh B, Nagpal R, Tiwari RR. Mucormycosis in COVID-19 pandemic: Risk factors and linkages, Current Research in Microbial Sciences, Volume 2,2021,100057. [CrossRef]
- Young M, Keane C, English L. Misdiagnosed dermatophytosis. J Infect. 1982 Mar;4(2):127-9. [CrossRef]
- Daude E, Bartolome B, Pascual M, Fraga J, Garcia-Diez A. Auto involutive Photoexacerbated Tinea Corporis Mimicking a Subacute Cutaneous Lupus Erythematosus.
- Zawar V, Chuh A (2009). Case report on Malassezia infection of palms and fingernails – speculations on cause for therapeutic failure in pityriasis versicolor., 23(2), 171–172. [CrossRef]
- Bornkessel A, Ziemer M, Yu S, Hipler C, Elsner P. Fulminant papulopustular tinea corporis caused by Trichophyton mentagrophytes. Acta Derm Venereol 2005;85:92. [CrossRef]
- Serarslan G. Pustular psoriasis-like tinea incognito due to Trichophyton rubrum. Mycoses 2007;50:523-4. [CrossRef]
- Van Burik, J.-A.; Colven, R.; Spach, D.H. Cutaneous Aspergillosis. J. Clin. Microbiol. 1998, 36, 3115–3121. [Google Scholar] [CrossRef] [PubMed]
- Emilianov V, Feldmeyer L, Yawalkar N, Heidemeyer K. Tinea corporis with Trichophyton rubrum mimicking a flare-up of psoriasis under treatment with IL17-inhibitor Ixekizumab. Case Rep Dermatol. 2021 Jul 9;13(2):347-351. [CrossRef]
- Kim W-J, Kim T-W, Mun J-H et al. Tinea incognito in Korea and it risk factors: nine-year multicenter survey. J Korean Med Sci 2013;28(1):145-151. [CrossRef]
- Merad Y, Derrar H, Tabouri S, Berexi-Reguig F. Candida guilliermondii Onychomycosis Involving Fingernails in a Breast Cancer Patient under Docetaxel Chemotherapy. Case Reports in Oncology 14 (3), 1530-1535, 2022. [CrossRef]
- Torrelo, A.; Hernández-Martín, A.; Scaglione, C.; Madero, L.; Colmenero, I.; Zambrano, A. Primary Cutaneous Aspergillosis in a Leukemic Child. Actas Dermosifilogr. 2007, 98, 276–278. [Google Scholar] [CrossRef]
- Smith, W.F.; Wallace, M.R. Cutaneous aspergillosis. Cutis 1997, 59, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Kerr OA, Bong C, Wallis C, Tidman MJ. Primary cutaneous mucormycosis masquerading as pyoderma gangrenosum. Br J Dermatol. 2004 Jun;150(6):1212-3. [CrossRef]
- Liu J, Xin WQ, Liu LT, Chen CF, Wu L, Hu XP. Majocchi's granuloma caused by Trichophyton rubrum after facial injection with hyaluronic acid: A case report. World J Clin Cases 2020; 8(17): 3853-3858. [CrossRef]
- Langlois, R.P.; Flegel, K.M.; Meakins, J.L.; Morehouse, D.D.; Robson, H.G.; Guttmann, R.D. Cutaneous aspergillosis with fatal dissemination in a renal transplant recipient. Can. Med. Assoc. J. 1980, 122, 673–676. [Google Scholar] [PubMed]
- Merad Y, Adjmi-Hamoudi H, Tabet-Derraz N. Tinea corporis caused by Microsporum canis in HIV patient treated for neuromeningeal cryptococcis: report of a nosocomial outbreak. Journal of Current Medical Research and Opinion, 1(04),16, 2018. [CrossRef]
- Merad Y, Adjmi-Hamoudi H, Lahmer K, Saadaoui E, Cassaing S, Berry A. Les otomycoses chez les porteurs d’aides auditives : Etude retrospective de 2010 a 2015. Journal deMycologie Medicale, 26(1) :71. [CrossRef]
- Oanţă A, Irimie M. Tinea on a Tattoo. Acta Dermatovenerol Croat. 2016 Aug;24(3):223-4.
- Cohen RR, Shurman J. Fungal melanochya as a solitary black linea vertical nail plate treak: case report and literature review of Candida-associated longitudinal melanonychia Striata. Cureus. 2021 Apr 1;13(4):e14248.
- Bardazzi F, Neri I, Marzaduri S et al. Microsporum canis infection of the penis. Genitourin Med 1997; 73: 579–581. [CrossRef]
- Torres CS, Granoble KG, Pazmiño JEU, Parra Vera HJ. Presentación clínica inusual de tiña corporis en un adolescente causada por Trichophyton mentagrophytes. Centro Dermatológico Dr. Úraga, Vol 4, Nº 2 2022.
- Leung AK, Lam JM, Leong KF, Hon KL. Tinea corporis: an updated review. Drugs Context. 2020 Jul 20;9:2020-5-6. [CrossRef]
- del Boz J, Crespo V, Rivas-Ruiz F, de Troya M. Tinea incognito in children: 54 cases. Mycoses. 2011;54(3):254–258. [CrossRef]
- Verma SB, Panda S, Nenoff P, Singal A, Rudramurthy SM, Uhrlass S, et al. The unprecedented epidemic-like scenario of dermatophytosis in India: I. Epidemiology, risk factors and clinical features. Indian J Dermatol Venereol Leprol 2021;87:154-75. [CrossRef]
- Alteras I, Feuerman EJ, David M, Segal R. The increasing role of Microsporum canis in the variety of dermatophytic manifestations reported from Israel. Mycopathologia 1986; 95: 105–7. [CrossRef]
- Virgili A, Corazza M, Zampino MR. Atypical features of tinea in newborns. Pediatr Dermatol 1993; 10: 92. [CrossRef]
- Alteras 2 I, Feuerman EJ. Atypical cases of Microsporum canis infection in the adult. Mycopathologia 1981; 74: 181–5.
- Singh R, Bharu K, Ghazali W, Nor M, Kerian K. Tinea faciei mimicking lupus erythematosus. Cutis 1994; 53: 297–8.
- Dauden E, Bartolome B, Pascual M, Fraga J, Garcia-Diez A. Autoinvolutive photoexacerbated tinea corporis mimicking a subacute cutaneous lupus erythematosus. Acta Derm Venereol 2001; 81: 141–2.
- Won-Jeong K, Tae-Wook K, Je-Ho M, et al: Tinea incognito in Korea and its risk factors: nine-year multicenter survey. J Korean Med Sci. 2013;28:145-51.
- Romano C, Mariatiti E, Gianni C. Tinea incognito in Italy: A 15-year survey. Mycoses 2006;49(5):383-387. [CrossRef]
- Agarwal, M., Gupta, C., Gujral, G.S. et al. Tinea corporis infection manifestating as retinochoroiditis—an unusual presentation. J Ophthal Inflamm Infect 9, 8 (2019). [CrossRef]
- Zawar V, Kumavat S, Rathi S. Dermatophytosis mimicking psoriasis: A classic presentation of steroid treated tinea. Images In Dermatlogy 113(6):622-623. [CrossRef]
- Dyrholm M, Rubenstain E. Tinea incognito: Majocchi granuloma masquerading as psoriasis. Consultant360, 2017, 57(4).
- Salecha AJ, Sridevi K, Senthil KAL, Sravani G, Rama Murthy DVSB. The menace of tinea incognito: clinic-epidemiological study with microbiological correlation from south India. JPAD Vol. 33, No.4 (2023.
- Yang, Z., Chen, W., Wan, Z. et al. Tinea Capitis by Microsporum canis in an Elderly Female with Extensive Dermatophyte Infection. Mycopathologia 186, 299–305 (2021). [CrossRef]
- Klein PA, Clark RA, Nicol NH. Acute infection with Trichophyton rubrum associated with flares of atopic dermatitis. Cutis. 1999 Mar;63(3):171-2.
- Wilso BB, Deuell B, Mills TA. Atopic dermatitis associated with dermatophyte infection and Trichophyton hypersensitivity. Cutis. 1993 Mar;51(3):191-2.
- Dutta B, Rasul ES, Boro B. Clinico-epidemiological study of tinea incognito with microbiological correlation. India J Dematol Venerol Leprol 2017;83:326-31. [CrossRef]
- Atzori L, Pau M, Aste N, Aste N. Dermatophyte infections mimicking other skin diseases: A 154-person case survey of tinea atypica in the district of Cagliari (Italy). Int J Dermatol 2012;51:410-5. [CrossRef]
- Xie W, Chen Y, Liu W, Li X, Liang G. Seborrheic dermatitis-like adult tinea capitis due to Trichophyton rubrum in an elderly man. Medical Mycology Case Reports, 41, 2023, 16-19. [CrossRef]
- Greywal T, Friedlander SF. Dermatophytes and Other Superficial Fungi. Principles and Practices of Pediatric Infectious Diseases (Fifth Edition), 2018, pages 1282-1287.
- Merad Y, Belkacemi M, Derrar H, Belkessem N, Djaroud S. Trichophyton rubrum skin folliculitis in Behcet’s disease. Cureus 13(120,2021. [CrossRef]
- Weksberg F, Fisher BK. Unusual tinea corporis caused by Trichophyton verrucosum. Int J Dermatol 1986; 25: 653–655. [CrossRef]
- Almeida L, Grossman M. Wide spread dermatophyte infections that mimic collagen vascular disease. J Am Acad Dermatol 1990; 23: 855–857.
- Molina-Leyva A, Perez-Parra S, Garcia-Garcia F. Nodular plaque on the forearm. An Bras Dermatol. 2014;89(5):839-40.
- Dordevic Betetto L, Zgavec B, Bergant Suhodolcan A. Psoriasis-like tinea incognita: a case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2020 Mar;29(1):43-45.
- Eichhoff G. Tinea incognito Mimicking pustular psoriasis in a patient with psoriasis and cushing syndrome. Cutis. 2021 April;107(04):E30-E32. [CrossRef]
- Surya SP, Dewi KP, Regina R. Cutaneous candidiasis mimicking inverse psoriasis lesion in a type 2diabtes mellitus patient. Dermatol Venereol Indones, Vol.5, Issue 1 (2020).
- Keller MC, French LE, Hofbauer GFL, Bosshard PP. Erythematous skin macules with isolation of Trichophyton eboreum – infection or colonisation?. Mycoses, 2012;56(3):373-375. [CrossRef]
- Nakagawa T, Nakashima K, Takaiwa T, Negayama K. Trichosporon cutaneum (Trichosporon asahii ) infection mimicking hand eczema in a patient with leukemia, Journal of the American Academy of Dermatology, 2000, 42(5), 929-931. [CrossRef]
- Quinones C, Hasbun P, Gubelin W. Tinea incognito due to Trichophyton mentagrophytes: case report. Medwave 2016 Oct;16(10):e6598. [CrossRef]
- Shimoyama H, Nakashima C, Hase M, Sei Y. A case of tinea corporis due to Trichophyton tonsurans that manifested as impetigo. Med Mycol J, 57E, 2016. [CrossRef]
- Liu X, Li R, Song Y, Wang A. Generalized tinea corporis caused by Trichophyton verrucosum misdiagnosed as allergic dermatitis and erythema annulare in an adult. Medical Imagery, 2021, 113, 339-340. [CrossRef]
- Darling MJ, Lambiase MC, Young RJ. Tinea versicolor mimicking pityriasis rubra pilaris. Cutis 2005;75:265-7. [CrossRef]
- Dias MF, Quaresma-Santos MV, Bernardes-Filho F, Amorim AG, Schechtman RC, Azulay DR. Update on therapy for superficial mycoses: review article part I. An Bras Dermatol. 2013;88(5):764-774. [CrossRef]
- Bell SA, Röcken M, Korting HC. Tinea axillaris, a variant of intertriginous tinea, due to non-occupational infection with Trichophyton verrucosum. Mycoses. 1996 Nov-Dec;39(11-12):471-4. [CrossRef]
- Swali R, Ramos-Rojas E, Tyring S. Majocchi granuloma presenting as a verrucous nodule of the lip. Proc (Bayl Univ Med Cent). 2018 Jan 10;31(1):115-116. [CrossRef]
- Aljabre SH, Sheikh YH. Penile involvement in pityriasis versicolor. Trop Geogr Med. 1994;46(3):184-5.
- Ferry M, Shedlofsky L, Newman A, et al. (January 17, 2020) Tinea InVersicolor: A Rare Distribution of a Common Eruption. Cureus 12(1): e6689. [CrossRef]
- Banu A, Anand M, Eswari L. A rare case of onychomycosis in all 10 fingers of an immunocompetent patient. Indian Dermatol Online J. 2013;4(4):302-304. [CrossRef]
- Varada S, Dabade T, Loo DS. Uncommon presentations of tinea versicolor. Dermatol Pract Concept. 2014 Jul 31;4(3):93-6. [CrossRef]
- Aljabre SH. Intertriginous lesions in pityriasis versicolor. J Eur Acad Dermatol Venereol. 2003 Nov;17(6):659-62. [CrossRef]
- Noyan A et al. Tinea of the scalp and eyebrows caused by Trichophyton violaceum in a 62-year-old diabetic woman. JEADV 2001; 15: 88.
- Zeng, J., Shan, B., Guo, L. et al. Tinea of the Scalp and Left Eyebrow Due to Microsporum canis. Mycopathologia (2022). [CrossRef]
- John D, Selvin SST, Irodi A. Disseminated Rhinosporidiosis with comjunctival involvement in an immunocompromissed patient. Middle East Afr J Ophtalmol 2017;24:51-53.
- Metkar A, Joshi A, Vishalakshi V, Miskeen AK, Torsekar RG. Extensive neonatal dermatophytoses. Pediatr Dermatol. 2010;27(2):189–91. [CrossRef]
- King D, Cheever W, Hood A et al. Primary invasive cutaneous Microsporum canis infections in immunocompromised patients. J Clin Microbiol 1996; 34: 460–462. [CrossRef]
- Godse KV, Zawarb V. Chronic urticaria associated with tinea infection and success with antifungal therapy—a report of four cases. International Journal of Infectious Diseases 14S (2010) e364–e365.
- Aspiroz C, Ara M, Varea M, Rezusta A, Rubio C. Isolation of Malassezia globosa and M. sympodialis from patients with pityriasis versicolor in Spain. Mycopathologia. 2002;154:111–7. [CrossRef]
- Mansouri P, Farshi S, Khosravi AR, Naraghi ZS, Chalangari R. Trichophyton Schoenleinii-induced widespread tinea corporis mimicking parapsoriasis. J Mycol Med. 2012 Jun;22(2):201-5. [CrossRef]
- Subramanya SH, Subedi S, Metok Y. et al. Distal and lateral subungual onychomycosis of the finger nail in a neonate: a rare case. BMC Pediatr 19, 168 (2019). [CrossRef]
- Koklu E, Gunes T, Kurtoglu S, et al. Onychomycosis in a premature infant caused by Candida parapsilosis. Pediatr Dermatol. 2007;24(2):155–6. [CrossRef]
- Ely JW, Rosenfeld S, Seabury Stone M. Diagnosis and management of tinea infections. Am Fam Physician. 2014 Nov 15;90(10):702-10.
- Finch J, Arena R, Baran R. Fungal melanonychia. J Acad Dermatol. 2012;66:830-41.
- Álvarez-Salafranca M, HernándezOstiz S, Salvo Gonzalo S, Ara Martín M. Onicomicosis subungueal proximal por Aspergillus niger: un simulador de melanoma maligno subungueal. Actas Dermosifiliogr. 2017;108:481---484.
- Y Merad, AA Moulay, H Derrar, M Belkacemi, ad al. Aspergillus flavus onychomycosis in the right fourth fingernail related to phalynx fracture and traumatic inoculation of plants: A vegetable vendor case report. Am. Res. J. Dermatol 2, 1-4, 2020.
- Merad Y, Thorayya L, Belkacemi M, Benlazar F. Tinea unguium, tinea cruris and tinea corporis caused by Trichophyton rubrum in HIV patient: a case report. J Clin Cases Rep 4(4),89-92, 2021.
- Merad Y, Belkacemi, Bassaid A, Derouicha M, Merad Z et al. Onychogryphosis due to Aspergillus niger in a poorly controlled type 2 diabetes mellitus. CMRO 05(09), 1380-1385 (2022).
- Matsuyama Y, Nakamura T, Hagi T, Asanuma K and Sudo A: Subungual onychomycosis due to Aspergillus niger mimicking a glomus tumor: A case report. Biomed Rep 7: 532-534, 2017. [CrossRef]
- Abhinay KPA, Rao SK. Blackening of Nails with Pits – A Combination of Nail Psoriasis and Onychomycosis. Indian J Pediatr 88, 933–934 (2021).
- Noriegaa LF, Di Chiacchioa NG, Figueira de Melloc CDB, Suareza MV, Bet DL, Di Chiacchio N. Prevalence of Onychomycosis among Patients with Transverse Overcurvature of the Nail: Results of a Cross-Sectional Study. Skin Appendage Disord 2020;6:351–354. [CrossRef]
- Singal A, Bisherwal K. Melanonychia: Etiology, diagnosis, and treatment. Indian Dermatol Online J. 2020 Jan 13;11(1):1-11. [CrossRef]
- Martinez-Herrera EO, Arroyo-Camarena S, Porras-Lopez CF, Arenas R. Onychomycosis due to opportunistic molds. An Bras Dermatol. 2015 May-Jun;90(3):334-7. [CrossRef]
- Ge G, Yang Z, Li D, G. de Hoog S, Shi D. Onychomycosis with greenish-black discolorations and recurrent onycholysis caused by Candida parapsilosis. MedicalMycology Case Reports 24 (2019) 48–50. [CrossRef]
- Bonifaz A, Gomez-Daza F, Paredes V, et al. Tinea versicolor, tinea nigra, white piedra, and black piedra. Clin Dermatol 2010;28:140–145. 79. [CrossRef]
- Xavier MHSB, Torturella DM, et al. Sycosiform tinea barbae caused by Trichophyton rubrum. Dermatology Online Journal 2008, 14 (11): 10.
- Yassine Merad, Hichem Derrar, Mohamed Hadj Habib, Malika Belkacemi, Kheira Talha, Mounia Sekouhi, Zoubir Belmokhtar, Haiet Adjmi-Hamoudi.Trichophyton mentagrophytes tinea faciei in acromegaly patient: Case report. Journal of Clinical and Translational Endocrinology: Case Reports, Volume 19,2021, 100079. [CrossRef]
- Bohmer U, Gottlober P, Korting HC. Tinea mammae mimicking atopic eczema. Mycoses 1998; 41: 345–7. [CrossRef]
- Merad Y, Derrar H, Belkacemi M, Drici A, Belmokhtar Z, Drici AEM. Candida albicans mastitis in breastfeeding woman: an under recognized diagnosis. Cureus 12 (12), 2020. [CrossRef]
- Yilmaz M, Kavak A, Yamaner NJ. Bilateral and symmetrical tinea mammae. Dermatol Online J. 2013 Sep 14;19(9):19625. [CrossRef]
- Khanna U, Dhali TK, D'Souza P, Chowdhry S. Majocchi Granuloma of the Breast: A Rare Clinical Entity. CASE AND RESEARCH LETTER, Vol. 107, Issue 7, p 610-612 (September 2016).
- Smith BL, Koestenblatt EK, Weinberg JM. Areolar and periareolar pityriasis versicolor. J Eur Acad Dermatol Venereol. 2004 Nov;18(6):740-1. [CrossRef]
- Sardy M, Korting HC, Ruzicka T, Wolff H. Bilateral areolar and periareolar pityriasis versicolor. J Ger Soc Dermatol. 2010 Aug;8(8):617-8. [CrossRef]
- O'Grady TCSahn EE Investigation of asymptomatic tinea pedis in children. J Am Acad Dermatol. 1991;24660- 661.
- Al Hasan M, Fitzgerald SM, Saoudian M, Krishnaswamy G. Dermatology for the practicing allergist: Tinea pedis and its complications. Clin Mol Allergy. 2004 Mar 29;2(1):5. [CrossRef]
- Flores CR, Martín Díaz MA, Prats Caelles I, de Lucas Laguna R. Tinea manuum inflamatoria. An Pediatr (Barc) 2004;61(4):344-52 3.
- Balighi K, Lajevardi V, Barzegar M, Sadri M. Extensive tinea corporis with photosensivity. Indian J Dermatol. 2009;54(5):57–9.
- Dai, Y., Xia, X. & Shen, H. Multiple abscesses in the lower extremities caused by Trichophyton rubrum. BMC Infect Dis 19, 271 (2019). [CrossRef]
- Heibel HD, Ibad S, Chao Y, Patel KK, Hutto J, Redd LE, Nussenzveig DR, Laborde KH, Cockerell CJ, Shwin K. Scurvy and TineaCorporisSimulatingLeukocytoclasticVasculitis. Am J Dermatopathol. 2021 Dec 1;43(12):e230-e233. [CrossRef]
- Sarojini PA, Dharmaratnam AD, Pavithran K, Gangadharan C. Concentric rings simulating tinea imbricata in secondary syphilis. A case report. Br J Vener Dis. 1980 Oct;56(5):302-3. [CrossRef]
- Hong JS, Lee DW, Suh MK, Ha GY, Jang TJ, Choi JS. Tinea Corporis Caused by Trichophyton verrucosum Mimicking Nummular Dermatitis. J Mycol Infect 2019; 24(1): 32-34. [CrossRef]
- Gupta AK, Bluhm R, Summerbell R. Pityriasis versicolor. Journal of the European Academy of Dermatology and Venereology 2002;16(1):19-33. [CrossRef]
- Merad Y, Merad S, Belkacemi M, Belmokhtar Z, Merad Z, Metmour D. Extensive Pityriasis Versicolor Lesions in an Immunocompetent Parking Attendant: An Occupational Disorder? CMOR 05(08), 1327-1331 (2022). [CrossRef]
- Rehamnia Y, L Senhadji L, D Matmour D, MA Boumelik MA, Belmokhtar Z, and al. Tinea Versicolor Disguised as Pityriasis Alba: How to Deal with Confusing Skin Hypopigmentation. Journal of Current Medical Research and Opinion 6 (12), 1962-1968, 2023.
- Nakabayashi A, Sei Y, Guillot J. Identification of Malassezia species isolated from patients with seborrhoeic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Medical Mycology. 2000 Oct;38(5):337-41.
- Akaberi AA. Amini SS, Hajihosseini H. An Unusual Form of Tinea Versicolor: A Case Report. Iranian Journal of Dermatology, Vol 12, No 3 (Suppl), Autumn 2009.
- Hall J, Perry VE. Tinea nigra palmaris: differentiation from malignant melanoma or junctional nevi. Cutis 1998;62:45–46. 77.
- Haliasos EC, Kerner M, Jaimes-Lopez N, et al. Dermoscopy for the pediatric dermatologist. Part I: dermoscopy of pediatric infectious and inflammatory skin lesions and hair disorders. Pediatr Dermatol 2013;30:163–171. [CrossRef]
- Mendez J, Sanchez A, Martinez JC. Urticaria associated with dermatophytosis. Allergol Immunopathol (Madr). 2002 Nov-Dec;30(6):344-5. [CrossRef]
- Veraldi S, Gorani A, Schmitt E, Gianotti R. Case report. Tinea corporis purpurea. Mycoses 1999; 42: 587–9. [CrossRef]
- Hsu S, LE EH, Khoshevis MR. Differential Diagnosis of Annular Lesions. Am Fam Physician. 2001;64(2):289-297.
- Kalkan G, Demirseren DD, Güney CA, Aktaş A. A case of tinea incognito mimicking subcorneal pustular dermatosis. Dermatology Online Journal. 2020, 26(2):13. [CrossRef]
- Terragni L, Marelli MA, Oriani A, Cecca E. Tinea corporis bullosa. Mycoses 1993; 36: 135–7.
- Veraldi S, Scarabelli G, Oriani A, Vigo GP. Tinea corporis bullosa anularis. Dermatology 1996; 192: 349–50. [CrossRef]
- Karakoca Y, Endoğru E, Erdemir AT, Kiremitçi U, Gürel MS, Güçin Z. Generalized Inflammatory Tinea Corporis. J Turk Acad Dermatol 2010; 4 (4): 04402c.
- Barbé J, Clerc G, Bonhomme A. Granulome de Majocchi pubien : une entité clinique de localisation inhabituelle. Annales de Dermatologie et de Vénérologie, Volume 145, Issue 12, Supplement, 2018, S287-S288,. [CrossRef]
- Inaoki M, Nishijima C, Miyake M, Asaka T, Hasegawa Y, Anzawa K, Mochizuki T. Case of dermatophyte abscess caused by Trichophyton rubrum : a case report and review of the literature. Mycoses, Vol. 58, Issue 5, p. 318-3232, 2015. [CrossRef]
- Yonebayashi K, Yasuda E, Sakatani S, Kusakabe H, Kiyokane K. A case of granuloma trichophyticum associated with relapsing polychondritis. Skin Research 1998;40:394-8.
- Matsuzaki Y, Ota K, Sato K, Nara S, Yagushi T, Nakano H, Sawamura D. Deep pseudocystic dermatophytosis caused by Trichophyton rubrum in a patient with myasthenia gravis. Acta Derm Venereol. 2023 May. [CrossRef]
- Colwell AS, Kwaan MR, Orgill DP. Dermatophytic pseudomycetoma of the scalp. Plast Reconstr Surg. 2004;113(3):1072-1073. [CrossRef]
- Toussaint F, Sticherling M. Multiple Dermal Abscesses by Trichophyton rubrum in an Immunocompromised Patient. Frontiers in Medicine, Volume 6 - 2019. [CrossRef]
- Kim SH, Jo IH, Kang J, Joo SY, Choi JH. Dermatophyte abscesses caused by Trichophyton rubrum in a patient without pre-existing superficial dermatophytosis: a case report. BMC Infect Dis. 2016 Jun 17;16:298. [CrossRef]
- Schlesinger P, Rottman A. Trichophyton species as the Cause of A Diabetic Deep Plantar Foot Abscess: A Case Report. Podiatry Today 2021. [CrossRef]
- Hironaga M, Okazaki N, Saito K, Watanabe S. Trichophyton mentagrophytes granulomas. Unique systemic dissemination to lymph nodes, testes, vertebrae, and brain. Arch Dermatol 1983; 119: 482–90.
- Parmar NV, Asir GJ, Rudramurthy SM. Atypical Presentation of Majocchi's Granuloma in an Immunocompetent Host. Am J Trop Med Hyg. 2017 Jan 11;96(1):1-2.
- Hironaga M, Okazaki N, Saito K, Watanabe S. Trichophyton mentagrophytes granulomas. Unique systemic dissemination to lymph nodes. Testes, vertebrae, and brain. Arch. Dermatol. 1983, 119,482-490.
- Fukushiro R. Dermatophytes abscess . In: Fukushiro R (ed. Color Atlas of Dermatophytoses. Tokyo: Kanehara Co. 1999:89-95.
- Marconi VC, Kradin R, Marty FM, Hospenthal DR, Kotton CN. Dessiminated dermatophytosis in a patient with hereditary hemochromatosis and hepatic cirrhosis: case report and review of the literature. Medical Mycology, Vol 48, Issue 3, May 2010, p 518-527.
- Zheng, Yy., Li, Y., Chen, My. et al. Majocchi’s granuloma on the forearm caused by Trichophyton tonsurans in an immunocompetent patient. Ann Clin Microbiol Antimicrob 19, 39 (2020). [CrossRef]
- Jakob Lillemoen Drivenes, Mette Ramsing, Anette Bygum; Majocchi’s Granuloma – The Great Mimicker: A Case Report. Case Rep Dermatol 21 December 2023; 15 (1): 190–193.
- Toyoki M, Hase M, Hiradawa Y et al. A giant dermatophyte abscess caused by Trichophyton rubrum in an immunocompromised patient. Med. Mycol. J. 58E, E63-E66, 2017. [CrossRef]
- Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in humandisease. ClinicalMicrobiologyReviews, vol. 13, no. 2, pp. 236–301, 2000.
- Kyung-Ran K, Hwanhee P, Door-Ri K, Yoonsunn Y, Chiman J, Saanghoon L, So-Young L, Ji-Hye K, Yae-Jean K. Kerion Celsi caused by Trichophyton verrucosum mimicking a hypervascular tumor in a pediatric patient: a case report. Pediatric Infection & Vaccine;118-123,2022.
- Yun, SK., Lee, SK., Park, J. et al. Deeper Dermal Dermatophytosis by Trichophyton rubrum Infection Mimicking Kaposi Sarcoma. Mycopathologia (2022). [CrossRef]
- Tookey P, Gale J, pKazmi A, Ligaj M, Hawthorne M, Jeetle S, Fhogartaigh CN, M. Stodell, Moir G, Khurram M, Harwood C. BI02: Melanized (dematiaceous) fungal infections simulating skin cancer in African organ transplant recipients, British Journal of Dermatology, Volume 185, Issue S1, 1 July 2021, Pages 142–143.
Figure 1.
A) unexpected otomycosis after self-induced trauma in schizophrenic patient, B) Aspergillus flavus macroscopy after ear swab culture.
Figure 1.
A) unexpected otomycosis after self-induced trauma in schizophrenic patient, B) Aspergillus flavus macroscopy after ear swab culture.
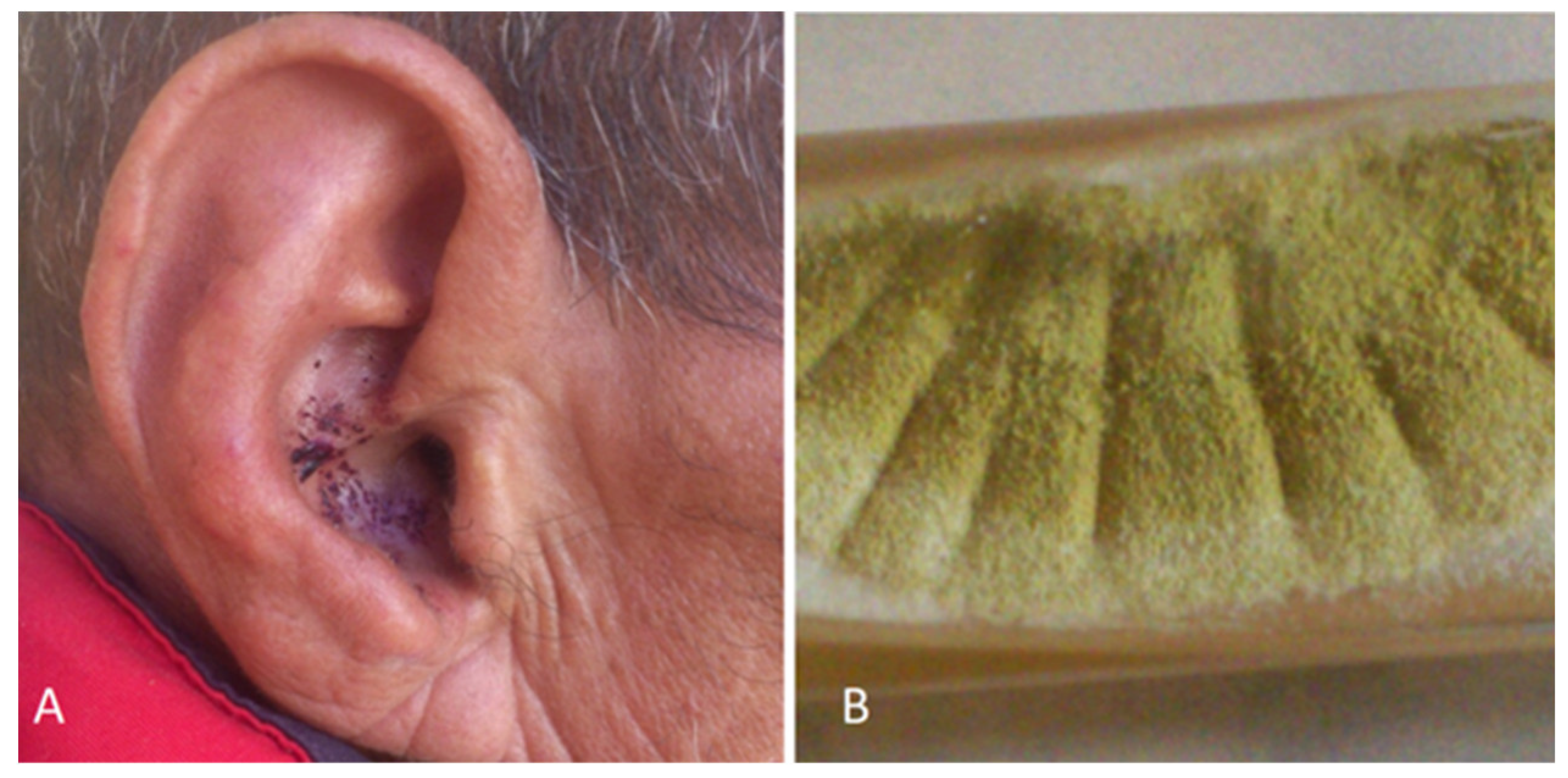
Figure 2.
A) Onycholyse associated to exudate and oedema in a patient under Docetaxel chemotherapy, B) Budding yeast and creamy white colonies of Candida guillermondii on SDA.
Figure 2.
A) Onycholyse associated to exudate and oedema in a patient under Docetaxel chemotherapy, B) Budding yeast and creamy white colonies of Candida guillermondii on SDA.

Figure 3.
A) Microsporum canis tinea corporis in HIV female at day 7 after hospitalization for cryptococcus neuromeingitis, B) macroscopic aspect of skin scraping culture.
Figure 3.
A) Microsporum canis tinea corporis in HIV female at day 7 after hospitalization for cryptococcus neuromeingitis, B) macroscopic aspect of skin scraping culture.
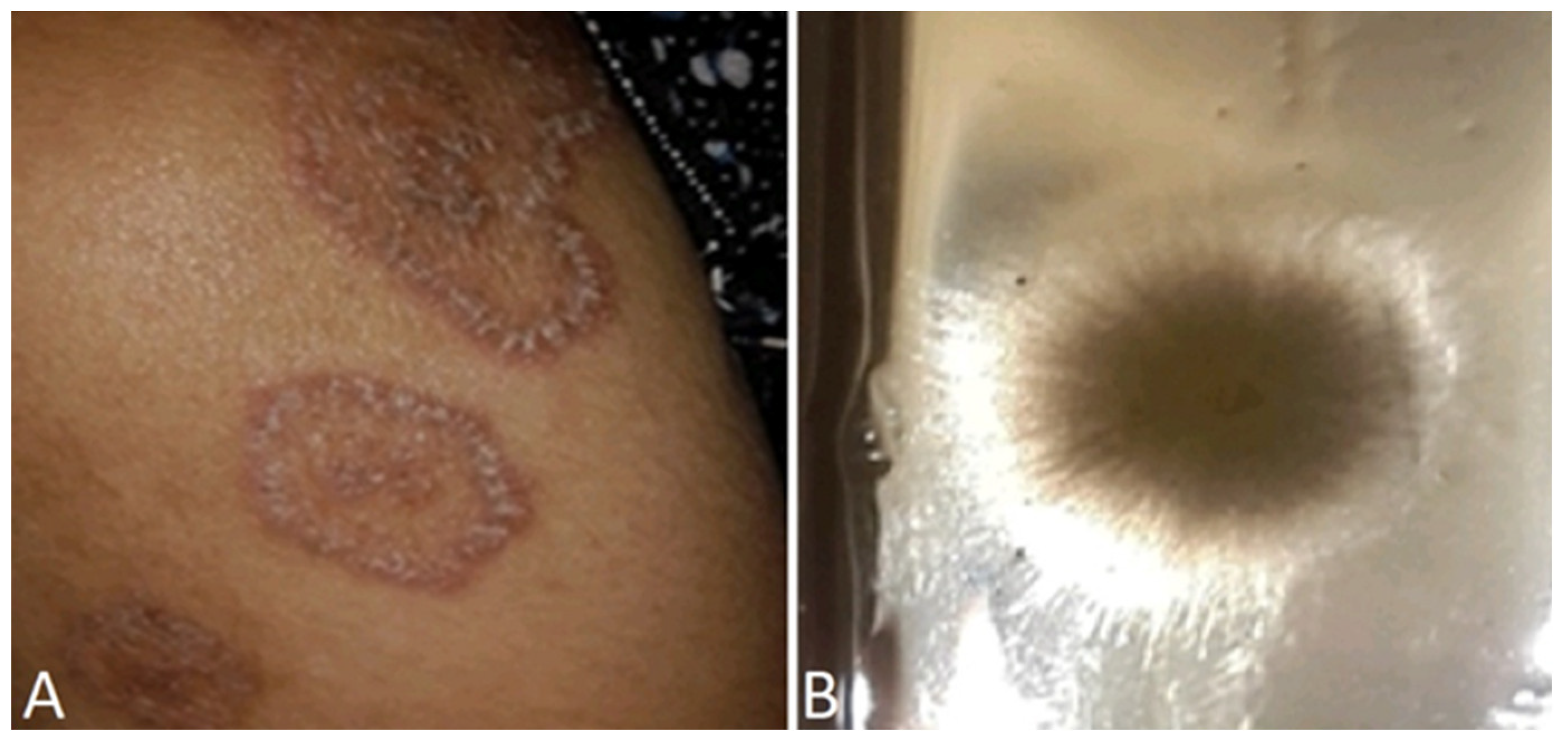
Figure 6.
A) unexpected tinea faciei in Acromegaly patient under corticosteroids B) Trichophyton mentagrophytes culture after skin scraping.
Figure 6.
A) unexpected tinea faciei in Acromegaly patient under corticosteroids B) Trichophyton mentagrophytes culture after skin scraping.
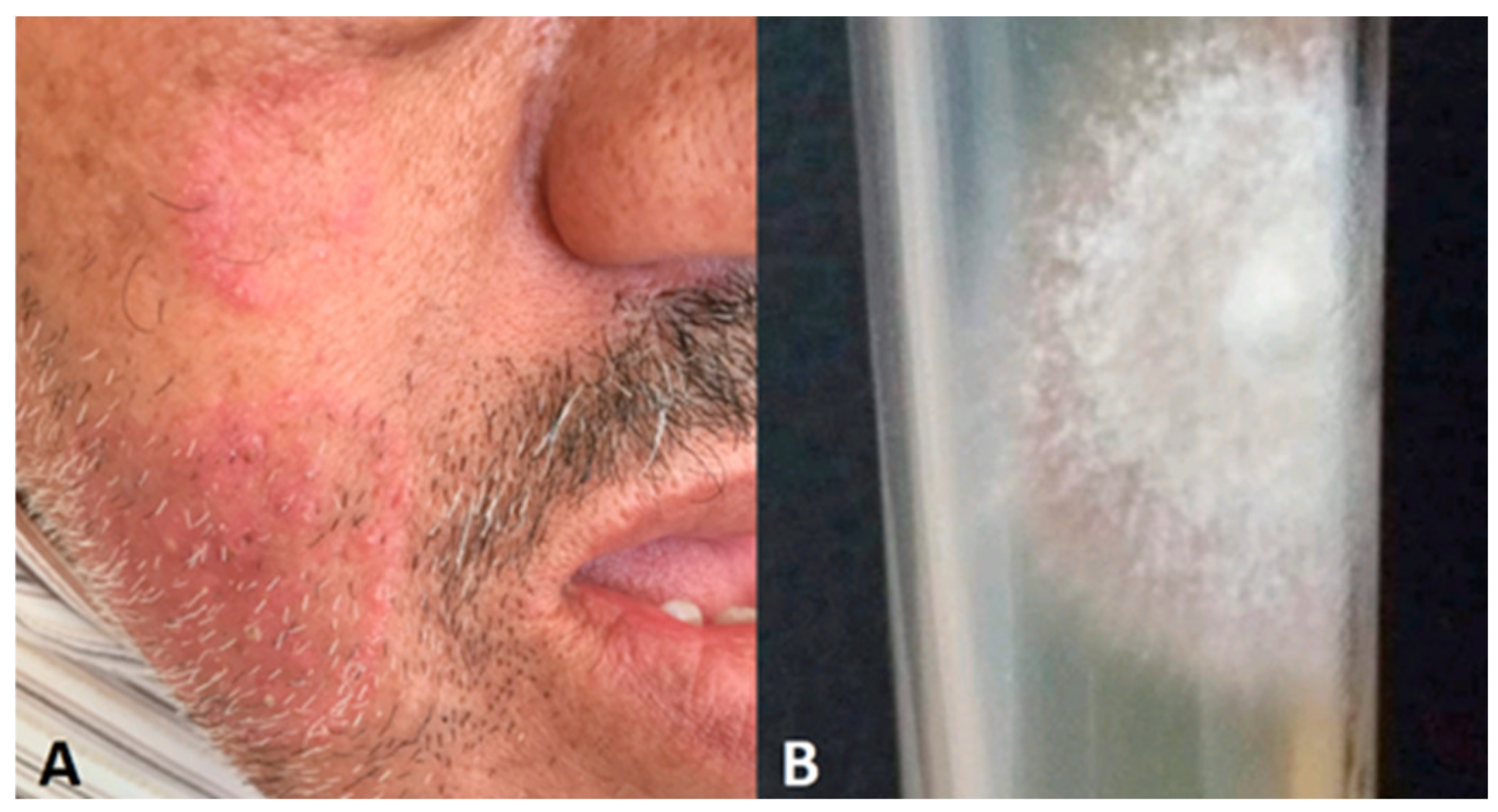
Figure 7.
A) Candida albicans breast hyperkeratosis and discharge, B) Creamy white colonies of Candida albicans.
Figure 7.
A) Candida albicans breast hyperkeratosis and discharge, B) Creamy white colonies of Candida albicans.
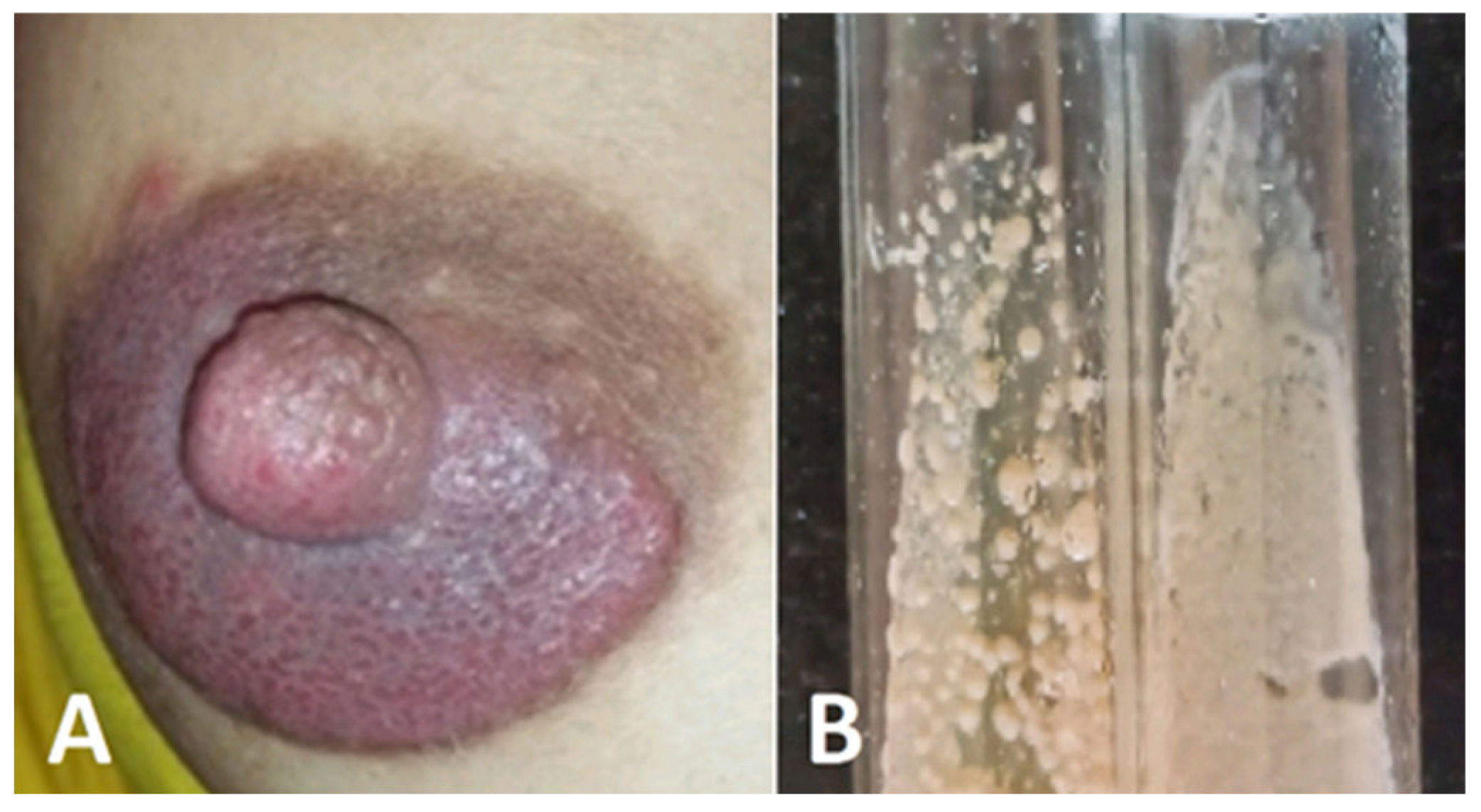
Figure 8.
A) black nail discoloration in vegetable vendor, B) Aspergillus niger culture after nail’s debris culture.
Figure 8.
A) black nail discoloration in vegetable vendor, B) Aspergillus niger culture after nail’s debris culture.
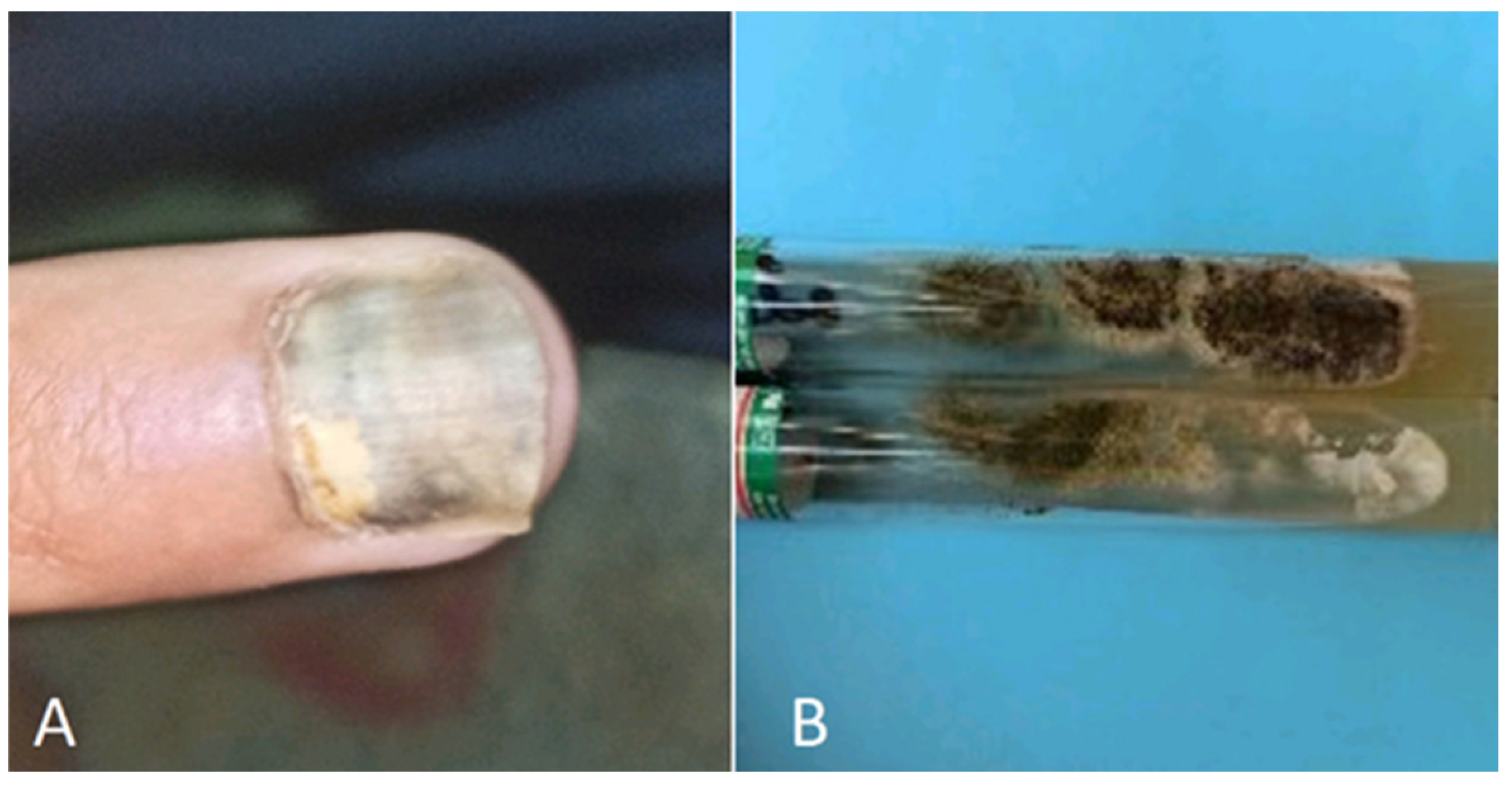
Figure 9.
A) Tinea versicolor misdiagnosed as Pityriasis alba, B).
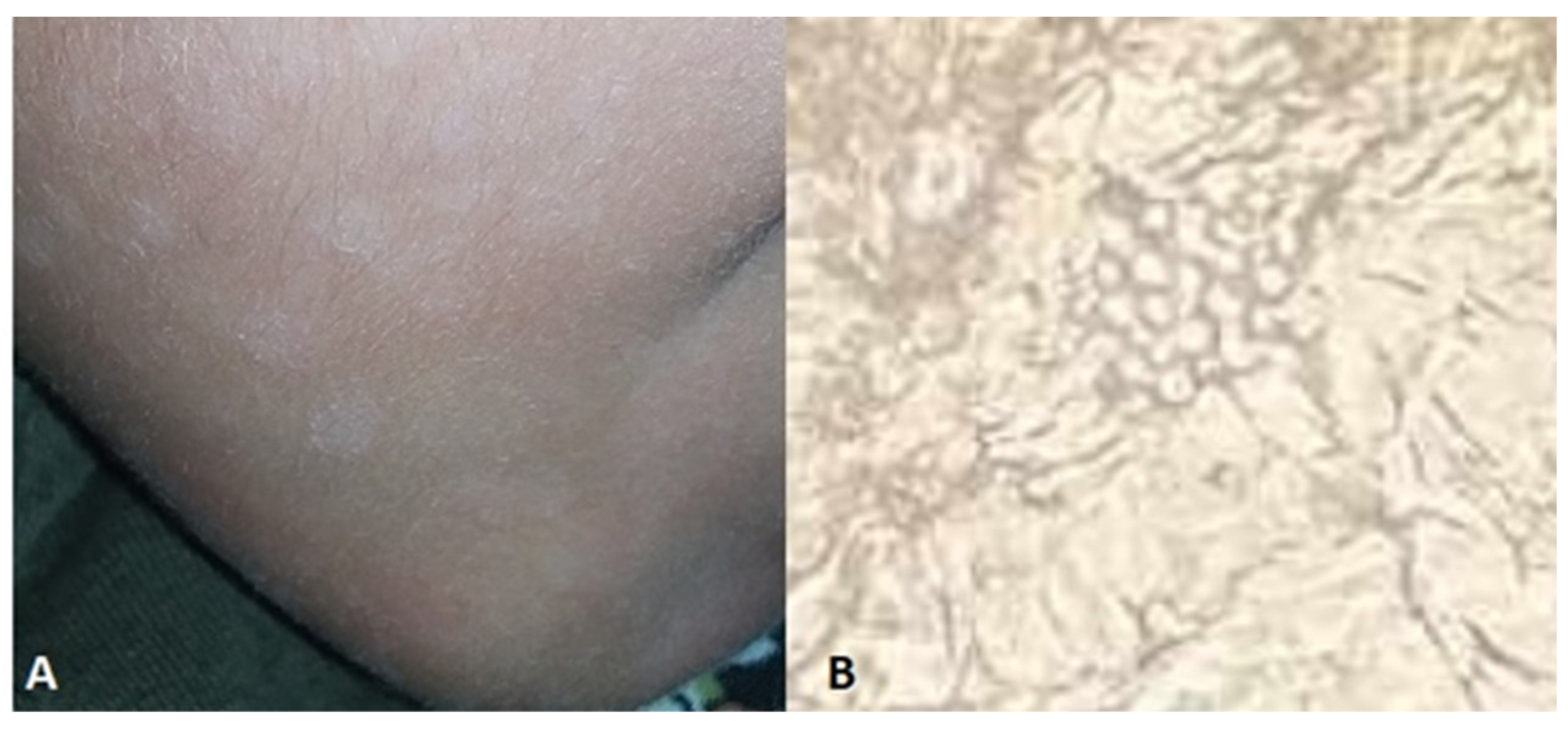
Figure 10.
A) Granular atypical dermatophytosis lesion before treatment, B) the healing lesion after Terbinafine treatment.
Figure 10.
A) Granular atypical dermatophytosis lesion before treatment, B) the healing lesion after Terbinafine treatment.
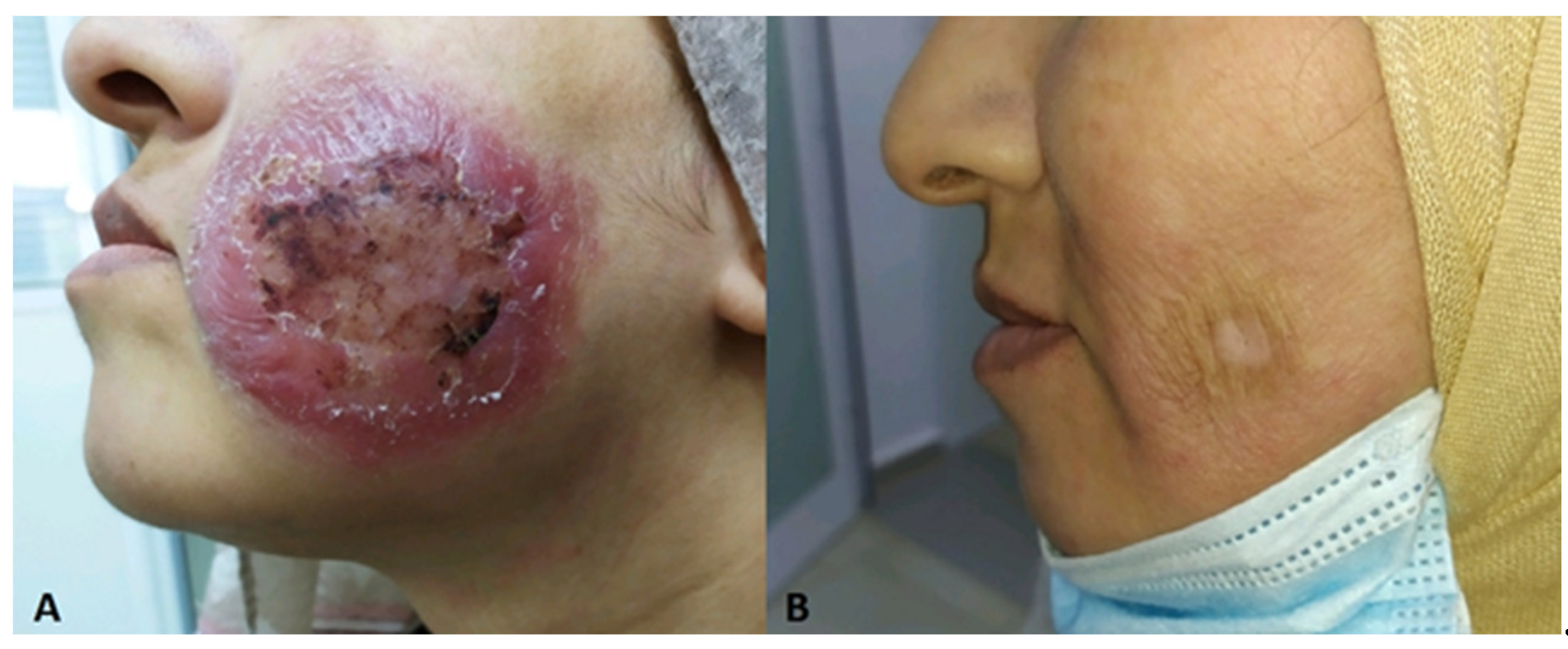
Table 4.
examples of atypical abscessed dermatophytoses.
| Localisation | Sex/age | Culture | Underlying disease | Country | References | |
| Lip | F/40 | T. rubrum | - | India | [128] | |
| Hand | F/52 | T.rubrum | Polychodritis | Japan | [189] | |
| Extremities, trunk, face | F/44 | T.rubrum | Myasthenia gravis | Japan | [190] | |
| Leg | M/54 | T.rubrum | None | Japan | [188] | |
| Thigh | F/24 | T.mentagrophytes | None | USA | [82] | |
| Scalp | F/19 | M.canis | None | [192] | ||
| Upper extremities | M/52 | T.rubrum | Immunosuppresive therapy | France | [193] | |
| Malleolus | F /68 | T.rubrum | - | Korea | [194] | |
| Foot | M/39 | Trichophyton sp | Type-2 diabetes | USA | [195] |
Table 5.
Examples of atypical nodular dermatophytoses.
| Localisation | Sex/age | Culture | Underlying disease | Country | References | |
| Leg, trunk | M/28 | T. verrucosum | Nephrotic syndrme | Japan | [198] | |
| Groin | M/58 | T.rubrum | Nephrotic syndrome | Japan | [199] | |
| Extremities, truck, face | M/45 | T.rubrum | Haemochromatosis | USA | [200] | |
| Forearm | F/62 | T.tonsurans | - | China | [201] | |
| Breast | F/28 | T.violaceum | India | [162] | ||
| genitoinguinal | M/54 | - | - | Danemark | [202] | |
| Forearm | M/53 | T.rubrum | Spain | [116] | ||
| Buttock | M/73 | T.rubrum | Suppressive drugs | Japan | [203] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



