Submitted:
29 December 2023
Posted:
04 January 2024
You are already at the latest version
Abstract
We performed electronic research for articles published in PubMed, MEDLINE, and ScienceDirect databases from January 2004 to January 2023. The systematic review of twenty (20) peer-reviewed articles about dosimetric parameters and eight (8) articles about clinical outcomes confirmed the dosimetric advantages of ART through better target coverage and Organs at Risk (OARs) sparing, with subsequent benefits on decreased toxicity and improved clinical outcome, specifically local control of the disease. ART replanning is a sustainable strategy for minimizing toxicity by improving normal tissue sparing. Furthermore, it enhances target volume coverage by correctly determining the specific amount of dose to be delivered to the tumor. In conclusion, this review confirms that ART benefits dosimetric, clinical/therapeutic, and toxicity outcomes.
Keywords:
head and neck cancer
; adaptive radiotherapy
; intensity-modulated radiation therapy
; anatomic changes
; dosimetric changes
; time of adaptation
; clinical outcomes
2 Radiation Oncology Dept, University Hospital of Larissa, Faculty of Medicine, School of Health Sciences, University of Thessaly, Larissa, Greece
3 Radiation Oncology Dept, Metropolitan Hospital, Piraeus, Greece
4 Medical Physics Dept, University Hospital of Larissa, Faculty of Medicine, School of Health Sciences, University of Thessaly, Larissa, Greece
Introduction
Head and Neck Cancers (HNC) still represent some of the most common malignancies in developing countries, accounting for 5% of all cancers, both in males and females, with over 800,000 new cases reported worldwide each year, being responsible for more than 400,000 deaths annually [1,2]. The incidence of HNC exhibits significant regional variations, with higher prevalence in South and Southeast Asia and certain parts of Europe [3,4].
HNC encompasses various cancer types, including those affecting the oral cavity, pharynx, larynx, nasal cavity, paranasal sinuses, and salivary glands [5]. The primary risk factors include tobacco and alcohol use, but in recent years, human papillomavirus (HPV) infection has also emerged as a significant risk factor, especially for oropharyngeal cancer [6,7,8,9]. Men face a higher risk of developing HNC than women, and the likelihood of diagnosis increases with age, with most cases occurring in individuals over the age of 40. Treatments for HNC usually involve surgery, radiation therapy (RT), chemotherapy, or a combination of these approaches, with the specific treatment plan tailored to the cancer's stage and location [10].
Survival rates vary based on several factors, mainly the stage at diagnosis and the tumor's location, but in general, the 5-year survival rate is around 60% [11].
Most studies and statistics show that more than 65% of HNC patients have locoregionally advanced disease at diagnosis [12]. Chemoradiotherapy with systemic administration of a platinum-based regimen in combination with fractionated radiotherapy to a dose of 63–70 Gy is the standard of care for locoregional organ-sparing therapy of head-and-neck squamous cell carcinoma. Modern radiotherapy practice evolves imaging techniques, such as computer tomography during treatment, to accurately deliver high curative radiation doses to the tumors [13]. In this direction, the transition from two-dimensional conventional radiotherapy (2D-RT) to three-dimensional conformal radiotherapy (3D-CRT) and, nowadays, to intensity-modulated radiation therapy (IMRT) contributed the most to achieving the maximum therapeutic effect [14].
Apart from the significant therapeutic results, the issue of adverse acute effects of chemoradiotherapy treatment schedule for head and neck cancer is still substantial. Chemotherapy, radiotherapy, and the combination of these two can cause several acute but also delayed adverse effects, such as weight loss and anxiety. Significant acute radiation-induced toxicities include severe mucositis, dermatitis, xerostomia, and dysphagia, which may require a feeding tube. Significant late or chronic toxicities include xerostomia, dysphagia, and fatigue, which have been shown to impact quality of life years after treatment [15,16].
HNC poses a significant challenge in the field of RT due to the complex and dynamic anatomical structures, proximity to critical organs, and inter-fractional variations in the tumor and surrounding healthy tissues [17]. However, in the contemporary practice for HNC RT, it is often usual that radiation oncologists carry out the treatment plan without accounting for the actual anatomical changes that may result from swelling of the irradiated areas, the daily normal-tissue volume alterations, the tumor shrinkage, and the loss of body mass and weight [18,19]. All these changes can displace the target and the organs at risk (OARs) from their original position, affecting the accuracy of the radiation dose delivered without avoiding and protecting surrounding healthy tissues. Progress in image-guided RT has shown that volumetric changes to target volumes and OARs are often seen during intensity-modulated radiation therapy for HNC patients [19]. Moreover, the changes may result in an ill-fitting immobilization mask [13].
Although weight loss or reduction of nodular volume may be apparent on physical examination, these changes have resulted in unintended (or, at the very least, unmonitored) deviation from the initial planning geometry. Clinical target volume (CTV) undercoverage and/or organ at risk (OAR) overdosing may occur despite the application of isocentric image-guided alignment [20,21,22].
Therefore, adaptive radiotherapy (ART), with its ability to dynamically adjust the treatment plan in response to the patient's anatomical changes and deviations, has emerged as a promising solution to enhance target volume coverage in tumor size, shape, and position, guaranteeing that the tumor receives the intended radiation dose and minimize radiation-induced toxicity, improving the patient's quality of life during and after treatment. Additionally, ART offers the opportunity for optimal dose escalation when clinically indicated, potentially increasing the likelihood of tumor control without increasing the risk of damage to healthy tissues. Furthermore, ART can minimize treatment interruptions, as it quickly adjusts the treatment plan to accommodate sudden changes in anatomy, such as those caused by weight loss during treatment. ART considers each patient's unique anatomical changes as a highly personalized approach, leading to better treatment outcomes [23]. This individualized treatment can improve therapeutic outcomes and provide a more customized treatment experience [18,24].
ART for HNC can typically be employed to assess and correct tumor response and weight loss. Radiation oncologists are expected to utilize image-guided scans as the basis for treatment to help enhance adaptation planning for treatment response [25,26].
Therefore, ART is implemented to correct all morphological variations by actively adapting the treatment plans into three different timeframes: between therapy sessions (Offline Adaptive), immediately before a therapy session (Online Adaptive), and during a therapy session (Real-time Adaptive) [27].
With all the principles mentioned above, this review article focuses on exploring the impact of Adaptive Radiotherapy on dosimetry, clinical, and toxicity outcomes. Additionally, it will help evaluate whether Adaptive Radiotherapy improves the target volume coverage and/or normal tissue sparing.
Methods and Materials
We performed an electronic search of articles published in PubMed/MEDLINE and Science Direct from January 2004 (2007) to January 2020 (2023). The search was accomplished according to PRISMA GUIDELINES, using the following keywords: ART, HNC, parotid gland, and target volume. Additionally, reference lists were screened for studies with topics relevant to the current review. Retrospective and prospective studies were both included.
Articles were selected based on the relevance of the project studied. The eligibility criteria for the current review include:
- ■
- Report on dosimetric/anatomic changes.
- ■
- studies with ≥10 patients
All included studies were reviewed to collect the following data: number of patients, therapy practice, number of replans, anatomic and dosimetric variations, and dosimetric and clinical benefits of ART. Studies with a limited number of <10 patients were excluded. The flow chart diagram of the literature review is shown in Figure 1.
Results
Radiotherapy Planning
Over the past 20 years, the standard of care for radiotherapy of HNC has transitioned from 2D RT to 3D-conformal radiotherapy (3D-CRT) and eventually to intensity-modulated radiation therapy (IMRT) [28]. Initially, conventional radiotherapy approaches were rigid, delivering a fixed dose to the tumor and surrounding tissues. IMRT has demonstrated its superiority with its ability to decrease adverse effects on normal tissues, such as reducing xerostomia without compromising the therapeutic dose of radiation to target volumes of both primary and lymph nodes [29]; however, because of the unique features of IMRT, such as inverse planning procedures, any anatomical changes in patients resulting from weight loss or tumor shrinkage can substantially impact the radiation dose delivered. For this reason, the ART concept was introduced, offering improved precision, reduced toxicities, and improved patient outcomes [30,31].
Further innovations in modern radiotherapy practice include apart from intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), stereotactic body radiotherapy (SBRT), image-guided radiotherapy (IGRT), and protons or heavy ions [30,32].
The standard 3D-CRT approach, until the late 90s, involved the employment of 6 MV photon beams and a technique known as the three-field method. This method utilizes two lateral fields opposite each other to irradiate the primary tumor and cervical lymph nodes in the upper and lower neck regions. Additionally, a third anterior field irradiates the supraclavicular lymph nodes. The two lateral and anterior fields share the same isocenter to ensure precise radiation delivery. They are carefully aligned at this isocenter level, preventing any overlap of radiation fields at the junction line. It is also important to periodically adjust the junction line during treatment to ensure a gradual transition in the dose distribution to minimize adverse effects. This three-field technique involved several sequential dose boosts associated with specific prescription doses [31,33].
In contrast to the “older” three-field treatment approach, IMRT employs varying beam intensities and segments to deliver radiation that conforms to the tumor's shape and results in a steep dose drop-off at the tumor-normal tissue boundary. IMRT is well-suited for head and neck cancer (HNC) due to its complex tumor geometry and proximity to critical structures, as well as minimal organ movement. Two standard IMRT planning techniques for HNC are split-field and extended-field IMRT. The split-field approach treats the primary tumor and upper neck with IMRT, using a conventional anterior field for the lower neck and supraclavicular regions. Extended-field IMRT treats all tumor volumes simultaneously but requires attention to avoid overdosing to the larynx. For treating bilateral tumors, a standard setup involves nine coplanar 6 MV photon beams evenly positioned around the patient at angles of 0°, 40°, 80°, 120°, 160°, 200°, 240°, 280°, and 320°. In unilateral tumors, seven coplanar beams are utilized, angled from the side of the cancer. Care is taken to avoid directing the radiation laterally and, when necessary, to adjust the gantry angle slightly to prevent the beam from passing through the shoulder. The treatment's isocenter is typically chosen at the central point within the area to be irradiated, given that head and neck treatments often involve relatively large treatment fields.
The delineation of target volumes is further improved with functional imaging and the fusion of 18F-fluorodeoxyglucose positron emission tomography (18FDG-PET) scans with CT scans, although variability in delineation remains a challenge. IMRT planning has transitioned from manual planning to computer-based inverse planning, which offers better dose distribution to tumor volumes and improved sparing of critical structures [34,35,36,37].
VMAT, an advanced version of IMRT, further improves treatment by optimizing treatment delivery. In traditional IMRT, the treatment plan involves numerous small radiation fields created using the multileaf collimator (MLC). This can be done by sequentially positioning the MLC leaves to form these fields and then delivering radiation (the step-and-shoot method) or by continuously adjusting the MLC leaves while the radiation beam is on (the sliding window method). In contrast, VMAT allows for simultaneous motion of the MLC and gantry, adjusting factors like MLC leaf speed, gantry speed, and dose rate, all during real-time treatment. VMAT has become a popular choice for treating head and neck cancers due to the region's complex anatomy. A typical VMAT plan includes 2-3 full or partial arcs, depending on whether the treatment addresses bilateral or unilateral targets. VMAT plans utilize a more significant number of beam angles, resulting in a more precise dose distribution within the target area when compared to traditional IMRT. VMAT plans maintain similar target coverage as fixed gantry IMRT but offer improved uniformity. Notably, the delivery time for VMAT plans is significantly shorter, taking about 5 minutes, whereas fixed gantry IMRT plans typically require 10-15 minutes. Figure 4 provides a comparison of dose distributions between a two-arc VMAT plan and a nine-beam IMRT plan for a patient with laryngeal cancer and bilateral cervical lymph node involvement. VMAT and IMRT effectively cover the target volumes with comparable organ-at-risk (OAR) sparing. Occasionally, VMAT may enhance the sparing of contralateral OARs [38,39,40].
Fractionation
Radiation treatment schedules for head and neck cancers are not universally standardized. Typically, standard radiation therapy refers to daily doses of 1.8 to 2 Gy, given five days a week in 33 to 35 fractions, delivering a therapeutic dose of 70 Gy. However, to enhance the outcomes of head and neck cancer treatments, different radiation schedules have been developed. Over the past twenty years, two primary altered fractionation schedules, hyperfractionation and accelerated fractionation, have been extensively studied.
Hyperfractionation usually involves delivering two smaller doses of radiation daily in more fractions while maintaining or slightly shortening the overall treatment duration. This approach provides a higher biologically effective dose to the tumors and increases the tolerance of late-responding normal tissues. Several randomized trials have demonstrated that hyperfractionation significantly improves the control of tumors in both local and regional areas and enhances survival rates compared to standard fractionation. It's worth noting that hyperfractionation can lead to more severe acute mucositis, but the incidence of late complications remains within the range observed with conventional fractionation schedules.
Accelerated fractionation, on the other hand, reduces the overall treatment duration while keeping the number of dose fractions, total dose, and individual fraction sizes mostly unchanged or slightly reduced. The fundamental concept behind accelerated fractionation is that by shortening the treatment duration, there's less time for tumor cells to regenerate or repopulate during the treatment course. Clinical research on accelerated fractionation has demonstrated a significant improvement in local and regional control and survival rates. These accelerated schedules can also result in severe acute mucositis, but they do not appear to increase the risk of late complications.
Both hyperfractionation and accelerated fractionation schedules necessitate a minimum interval of 4.5 hours between fractions to allow normal tissues to repair after sublethal radiation injuries. Fractionation in radiotherapy is a critical factor significantly affecting treatment effectiveness [30,41,42,43,44].
A meta-analysis by Bourhis and colleagues [45], which reviewed 15 trials comparing conventional radiotherapy with hyperfractionation and accelerated radiotherapy for squamous cell carcinoma (SCC) patients, concluded that altered fractionation radiotherapy led to better tumor control and improved survival compared to conventional therapy. Additionally, research by Fu and colleagues indicated that both hyperfractionation and accelerated fractionation were more effective than conventional fractionation for locally advanced cancer [46,47].
Daily Imaging
Modern radiation therapy practice requires frequent imaging, which is necessary to improve treatment precision and outcomes. Daily imaging is essential, specifically during ART for head and neck cancer, for several key reasons:
- Anatomical Variability: The head and neck region experiences significant anatomical changes, including weight loss, tumor regression, and patient positioning shifts. Daily imaging, often via cone-beam computed tomography (CBCT), detects these changes and ensures precise tumor targeting while sparing critical structures.
- Patient Positioning: Accurate patient setup is essential for effective radiation therapy. Daily imaging verifies patient positioning, minimizing the risk of radiation toxicity to normal tissues.
- Dose Escalation: Daily imaging enables safe dose escalation by adapting treatment plans to current anatomy. This can improve local control and overall treatment outcomes.
- Reduced Margins: Smaller treatment margins, made possible by daily imaging, minimize radiation exposure to nearby healthy tissues, which is crucial in the head and neck region where critical structures are close to the tumor.
Online and Offline Adaptive Planning in Radiation Therapy
The two primary approaches to ART are offline and online adaptive radiotherapy. Online adaptive planning, often called "real-time" adaptive planning, is a technique where treatment plans are adjusted daily during therapy. This approach is particularly relevant in situations where anatomical changes, such as tumor shrinkage or variations in patient positioning, occur frequently and necessitate immediate action.
Offline adaption, or "inter-fractional" adaptive planning, is suitable for systematic or slow progressive changes (e.g., tumor regression, weight loss). The treatment team can decide to apply an adaption based on an observed deviation in anatomy (on imaging or visible physical alterations) or follow a protocol with predefined action levels and/or surveillance scans [18,25,26,46,48].
Table 1 Provides an overview of the main differences between online and offline adaptive radiotherapy, highlighting their strengths and weaknesses in various clinical contexts. The choice between these approaches depends on the specific needs of the patient and the clinical circumstances.
The frequency of CT scans for replanning therapy, is a critical consideration to maximize the benefits of this adaptive approach. The timing and frequency of CT scans for replanning in head and neck cancer treatment vary, with some advocating for daily scans while others perform scans depending on patient responses and clinical protocols. Typically, these scans occur at critical points during treatment, such as the start and specific intervals, to assess anatomical changes and adjust treatment plans. The goal is to precise tumor targeting while minimizing side effects and radiation exposure to healthy structures [19].
Dosimetric Considerations
Several studies have collectively investigated the dosimetric benefits of ART in head and neck cancer treatment. Various imaging methods, timing of evaluation, and frequencies of replanning were utilized in these studies. Expected dosimetric outcomes included volume shrinkage in target structures and changes in radiation doses to organs at risk (OARs) [20,21,49,50,51,52,53,54,55,56,57,58,59,60,61].
Volume Shrinkage
All studies reported varying degrees of volume shrinkage in target structures, such as the gross tumor volume (GTV), clinical target volume (CTV), and planning target volume (PTV). The extent of volume reduction ranged from approximately 11% to over 80%, with differences likely related to individual patient responses and tumor characteristics.
Dose Improvement to OARs
Multiple studies demonstrated improvements in radiation doses to OARs, particularly the parotid glands. Dose reductions in parotid glands ranged from approximately 3% to over 25%, reducing xerostomia and other side effects. Spinal cord and brainstem doses were also lowered, enhancing treatment safety.
Replanning Strategies
The studies utilized various strategies for ART, including daily cone-beam computed tomography (CBCT), weekly CT scans, and different timing for evaluation. Some studies performed multiple replans, showing adaptability in the ART process. One study applied an online ART approach, offering real-time adaptability.
Quality Assurance (QA)
Ensuring the accuracy and reliability of ART is paramount. Comprehensive quality assurance procedures, encompassing imaging, contouring, plan adaptation, and dose calculation, are essential to maintain the integrity of ART. Rigorous QA programs help guarantee safe and effective treatment delivery [19].
Table 2 summarizes the dosimetric benefits of online ART in terms of target coverage and the sparing of critical OARs in various replanning strategies for HNC patients.
These studies have explored the advantages of online ART, considering factors such as total dose, imaging method, timing of evaluation, the number of replanning events, volume shrinkage, and benefits to OARs. Duma et al. [62] conducted a study with 11 patients, demonstrating parotid gland sparing with minimal spinal cord dose variation. Two studies underscore the significant dosimetric advantages of online ART in enhancing target coverage for HNC patients. Jensen et al. [63] conducted a comprehensive investigation involving 72 patients who underwent 15 replanning events. Their findings revealed a substantial improvement in target coverage, suggesting that online ART can dynamically adapt to changes in patient anatomy and ensure more precise irradiation of the tumor volume. Similarly, Schwartz et al. [64] reported increased target coverage and improved dose homogeneity in a cohort of 22 patients. These results further emphasize that online ART can adapt to anatomical variations and optimize target coverage and dose distribution.

Table 2.
Dosimetric Benefits of ART in Target Covering and OAR’s Sparing.
| REPLANNING STRATEGIES | DOSIMETRIC BENEFITS | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author (year) | Pts No | TOTAL DOSE (Gy) |
Imaging method | Time of evaluation |
No of Replanning |
Volume Shrinkage | Parotid (Dmean/V26) |
Spinal Cord/Brainstem (Dmax) |
Benefit from ART |
| Zhao (2011) [65] | 33 | 37.5 Gy (20 – 50 Gy) | CT | 1st at 15th (+/-5) fr 2nd at 12th (+/- 4) fr 3rd after 15th fr |
1 | GTVp: - 13.9%; GTVn: - 71.9%; CTV: - 3.5%; | Decreased mean dose (p <0.05) | NR | Decreased PG dose |
| Capelle (2012) [49] | 20 | 66 Gy (54-60 nodes; 66 Gy primary) |
CT | 15TH fr | 1 | Median Volume Loss: PTV60/66 = -16% (0-45%); PTV54 = - 6.8 (-1.2 – 19%); GTV = -28.8% (-1.6 – 60%); CTV60 = - 4.1% (-0.1 – 10%); PG = 17.5% (-1 – 46%) | CohA Adjuvant CRT: PG: Dmean = -1.2 Gy/V26 = -6.3% CohB Definitive CRT: PG: Dmean = -1.2 Gy/V26 = -6.3% |
SC: Dmax = 1.2 Gy | 15/23 Pts improved TV dose coverage |
| Duma (2012) [62] | 11 | 64 postop 70 radical |
MVCT | 16th fr (9th – 21rst) | 1 | NR | PG: no variation of dose | SC: -0.14 Gy | --- |
| Jensen (2012) [63] | 72 15 replanned |
70.4 | Weekly CT | Weekly | 2-4 | NR | CPG: - 11.5% | NR | 8% Improvement of coverage |
| Schwartz (2013) [64] | 22 | 70 | 16th and 22nd Fr |
1-2 | NR | -0.7 Gy | NR | Increase coverage and dose homogeneity |
|
| Bhandari (2014) [21] | 15 | NR | CT | 3rd week of treatm Between 18th and 20th fr |
1 (HP vs AP) | Mean Volume Loss: GTV = -44.32 cc; CTV = 82.2 cc; PTV = -149.83 cc | RPG Dmean= +5.56+/-4.99 Gy (p<0.04); LPG Dmean =+3.28+/-3.32 Gy (p<0.003); | SC Dmax = +1.25+/-2.14 (p=0.04) BS Dmax = +3.88+/-3.22 (p<0.02) |
TV and OARs |
| Lu J (2014) [50] | 12 | 66 to Primary GTV (D95) | CT | 25th fr | 1 (HP vs AP) | Mean Volume Change: PGTV = -16.4 +/- 27.3; PTV1 = +3.8+/-6.3; PTV2 = -8.8+/-12.0 cc; rPG = -24.6+/-11.9; IPG = -35.1+/-20.1 | RPG = -24.6+/-11.9; LPG =-35.1+/-20.1 | SC and BS: 8/12 No-ART Pts exceeded the constraint without replanning |
TV and OARs |
| REPLANNING STRATEGIES | DOSIMETRIC BENEFITS | ||||||||
| Author (year) | Pts No |
TOTAL DOSE (Gy) |
Imaging method | Time of evaluation |
No of Replanning |
Volume Shrinkage |
Parotid benefit (Dmean/V26) |
Spinal Cord/Brainstem (Dmax) |
Benefit from ART |
| Olteanu (2014) [51] | 10 | 70.2 Gy | PET-CT | 10th, 20th and last day of treatm for dose sum | 2 (11th-20th fr and 21st – 30th) | Reduced GTV volumes (18.6-93.3%) after 18th fr | PG: reduced median dose 4.6-7.1% (p>0.05) | OARs: dose-differences from -7.1to 7.1% | TV and OARs |
| Reali (2014) [52] | 10 | 68.4 – 70.2 Gy | CT | Weeks 3, 5, and 7 of treatm |
1 | PTVs mean relative shift = 0.1 cm (not taken in consideration for replan); PG volume decreased mainly for Ipsilateral PG | NR | SC mean relative shift = 0 cm | PGs |
| Castelli (2015) [53] | 15 | 70 Gy | Weekly CT | Weekly | Weekly replanning | CTV70 decreased by a mean value of 31% (ranging 3% to −13%) PG volumes decreased by a mean value of 28.3% (ranging from 0.0 to 63.4% |
PG Dmean: -4.8 Gy (67% Pts) and -3.9 Gy (33% Pts) Median contralateral PG dose-decrease: -2.0 Gy. (from 27.9 to 25.9 Gy) |
NR | PG reduced dose |
| Zhang (2016) [54] | 13 | 70 | Weekly CT | Weekly | 6 weekly replans | Mean Volume Reduction CTV70=24.43% | With standard IMRT: Mean PG overdose of 4.1 Gy vs planned dose. In Replan: PG mean dose -3.1 Gy compared planned dose |
NR | PG Benefit >4 Gy (34% one PG – 15% both PGs) |
| Van Kranen (2016) [55] | 19 | 70 | Daily CBCT | 10th fr | 1 (10th fr or max in 2nd week of treat) | In 5th week: decreased CTVn & CTVnboost <-10% |
Margin reduction and improvement in OAR dose ≈ 1 Gy/mm | NR | PGs: improved D99% with – at least - 3 Gy |
| Dewan (2016) [56] | 30 | GTV= 70 Gy; CTV = 66 Gy; PTV = 60 Gy | Weekly CT | 20th fr | 1 (+ 1 hybrid) |
Shrinkage: GTV: 47.62%; CTV: 43.76%; PTV: 39.69%. IPG: 33.65%; CPG: 31.06% | Mean dose to ipsilateral parotid was significantly reduced with replanning by 26.04+29.14 % (p= 0.001). | SC: Replanning reduced mean Dmax, D2% and D1% by 28.26 + 10.27%, 30.87+ 12.83% and 31.20 + 13.09% respectively as compared to delivered dose (p<0.01) | TV and OARs |
| Deng (2017) [57] |
20 | 66 – 71.6 Gy | CT | 5th and 15th frs | 2 replans + 2 hybrid replans (5th and 15th fr) | Increase in V95; PTVnx: Decreased Vmax and V110 | Left PGs: Dmean = 3.67 Gy; V30 = 3.66 Gy | In ART plans: SC: Dmax decreased by 2.42 Gy; BS: Dmax decreased by 2.42 Gy | TV and OARs |
| Surucu (2017) [19] | 51 | 70.2 Gy | CT and CBCT | After median dose of 37.8 Gy (27 - 48.6) | 1 (in 34/51 pts) | Median TVRR: 35.2% (-18.8 – 79.6%) | IPG Dmean = – 6.2%; CPG Dmean = -2.5%; | SC Dmax = -4.5% BS Dmax = -3.0% |
TV and OARs |
| REPLANNING STRATEGIES | DOSIMETRIC BENEFITS | ||||||||
| Author (year) | Pts No |
TOTAL DOSE (Gy) |
Imaging method |
Time of evaluation |
No of Replanning |
Volume Shrinkage |
Parotid benefit (Dmean/V26) |
Spinal Cord/Brainstem (Dmax) |
Benefit from ART |
| Castelli (2018) [58] | 37 | 70 Gy | Weekly CT | weekly | Weekly replanning | NR | Median contralateral PG dose-decrease: -2.0 Gy. (from 27.9 to 25.9 Gy) | NR | PGs: reduced dose in 89% of Pts; CTV: increased dose in 67% of Pts; Both benefits: in 56% of Pts |
| Aly (2018) [20] | 10 | 70 Gy | CT | Mainly in 10th fr and 15th fr |
Mean 2 (range 0-5) | Volume Reductions: GTVp = 25%; CTVp = 18%; GTVn = 44%; CTVn = 28%; PTV70 = 11%; PTV60 no signific change | PG volume decrease 28% during treatment | NR | Improved coverage of PTV70 and PTV60 |
| Hay (2020) [60] | 20 | 65 Gy | CT and CBCT | At fraction 16th | 1 (19th fr) | NR | NR | SC: 3 Pts exceed max dose without replan | Benefit in OARs |
| Mnejja (2020) [59] | 20 | 69.96 Gy | CT | At dose 38 Gy | 1 (19th fr) | Reduction in TV: 58.56% (GTVnodes); 29.52% (GTVtumor) | NR | NR | Deterioration of Tumor Coverage in no-ART Pts |
| Avkshtol (2023) [61] |
21 | NR | CT and CBCT | Frequency of adapts at the discretion of treat physician | 1-5 Median 13.5th and 19th fr |
NR | IPG: -13.2 (node+ pts) -11.24% (T3/4 disease pts) CPG: - 3.78 (node+ pts) -1.68 (T3/4 disease pts) |
SC Dmax: -9.65 (node+ pts) -9.32 (T3/4 disease pts) BS Dmax: -6.41 (node+ pts) -5.38 (T3/4 disease pts) |
PTV coverage PTV dose homogeneity OARs |
Clinical Considerations
Table 3 summarizes the clinical outcomes of ART for head and neck cancer across different tumor sites, demonstrating the potential benefits of ART in improving locoregional control, survival rates, and toxicity profiles. The studies collectively support the utility of ART in enhancing the therapeutic landscape for head and neck cancer patients.
Regarding Nasopharyngeal Cancer (NPC), two fundamental studies explain the potential benefits of ART in improving clinical outcomes. Zhao et al. [65] evaluated clinical results in a cohort of 33 patients who received ART compared to 66 patients who underwent a non-ART treatment. Their results indicated a 3-year locoregional failure-free survival (LRFS) of 72.7% for the ART group compared to 68.1% for the non-ART group. Notably, the ART approach showed even non-significant reduced xerostomia and mucosal issues, particularly in N2 and N3 patients, underlining the potential benefits of ART in improving patient comfort and quality of life. Yang et al. [66] conducted a study involving 86 patients with NPC, of which 43 received non-ART treatment. Their findings demonstrated significant improvements in clinical outcomes for the ART group, with a 2-year locoregional control (LRC) rate of 97.2% compared to 82.2% in the non-ART group. Additionally, the ART group's 2-year overall survival (OS) rate was 89.8%, while the non-ART group had an OS rate of 82.2%.
Similar studies for Oropharyngeal Cancer (OPC), like the study from Schwartz [64], examined ART in 22 OPC patients, and their results revealed an impressive 2-year local-regional control rate of 95%. Notably, this study highlighted a favorable toxicity profile, indicating that most patients either maintained or achieved complete preservation or functional recovery of speech and eating within a relatively short period of 20 months.
In locally advanced head and neck cancer (LAHNC), two critical studies, Chen's study [67] and Mostafa's study [68], collectively underscore the potential benefits of ART in LAHNC, showing improved disease control without a significant increase in acute toxicity, which can ultimately translate into enhanced survival rates for patients. The variation in clinical endpoints between the two studies highlights the multifaceted nature of ART's impact on LAHNC, demonstrating that this approach can be tailored to individual patient needs while striving for improved therapeutic efficacy and quality of life.
The last category of studies encompasses a mixed head and neck cancer population. In the survey from Zhou et al. 2022 [69], in a substantial cohort of 290 patients who received ART, investigators compared their clinical outcome to 147 patients who underwent non-ART treatment. The findings were particularly promising, with ART demonstrating an impressive 8-year locoregional failure-free survival (LRFS) of 87.4%, compared to 75.6% in the non-ART group. Notably, ART was associated with a reduction in xerostomia, with a notably favorable rate of Grade I-II and a lower rate of Grade III-IV xerostomia compared to the non-ART approach [19,64,65,66,67,68,69,70].
Conclusions
In conclusion, our review paper reveals a comprehensive and evolving landscape in adaptive radiotherapy in HNC. The primary goal of radiotherapy in HNC is to enhance local control while maintaining patients' quality of life.
Adaptive radiotherapy, with its ability to modify treatment plans in response to anatomical changes during therapy, has shown great promise in improving the therapeutic outcomes for HNC patients. Studies consistently demonstrate that adaptive radiotherapy provides better target volume coverage and conformality, resulting in enhanced dose delivery to the tumor while minimizing radiation exposure to adjacent healthy tissues. This is particularly critical in HNC treatment, where precision is vital to balance therapeutic efficacy with patient well-being.
The clinical implications of adaptive radiotherapy are promising. Enhanced target coverage and reduced toxicity improve local control and overall survival rates. Additionally, adapting treatment plans in real-time or periodically allows for individualized patient care, addressing the unique challenges of head and neck cancers, such as anatomical changes due to weight loss, tumor shrinkage, or edema. Reduced radiation exposure to surrounding normal tissues translates into a lower incidence of acute and chronic side effects. Patients undergoing adaptive radiotherapy experience fewer instances of xerostomia, dysphagia, and other debilitating complications. This improves the quality of life during and after treatment and enables patients to tolerate fully prescribed courses of radiotherapy better.
However, the successful implementation of adaptive radiotherapy is contingent on several factors, including robust imaging techniques, skilled staff, and resource availability. Furthermore, large-scale prospective clinical trials are needed to solidify the existing evidence and establish guidelines for the broader application of adaptive radiotherapy in head and neck cancer treatment.
In summary, adaptive radiotherapy has the potential to revolutionize head and neck cancer treatment by optimizing target volume coverage and sparing normal tissues. With its dosimetric and clinical benefits, adaptive radiotherapy is promising for enhancing the therapeutic outcomes and overall well-being of head and neck cancer patients. Further research, technological advancements, and clinical standardization will continue to refine the role of adaptive radiotherapy in managing this challenging disease.
Abbreviations
HNC: Head and Neck Cancer, RT: Radiation Therapy, CT: Computed Tomography, 3DCRT: Three-Dimentional Conformal Radiation Therapy, OARs: Organs at Risk, IMRT: Intensity-Modulated Radiation Therapy, IMPT: Intensity-modulated Proton Therapy, IGRT: Image-Guided Radiation Therapy, ART: Adaptive Radiation Therapy, R-ART: Response-Adapted Radiation Therapy, A-ART: Anatomy-adapted Radiation Therapy, CBCT: Cone Beam Computed Tomography, PET: Positron-Emission Tomography, GTV: Gross Tumor Volume, CTV: Clinical Tumor Volume, PTV: Planning Tumor Volume.
References
- Poonam, J.; Dutta, S.; Chaturvedi, P.; Nair, S. Head and Neck Cancers in Developing Countries. Cancer of the oral cavity. Ram Maimonides Med J., 2014;5 (2) . [CrossRef]
- Siegel, R.;, Miller, K.; Wagle, N.; Jemal, A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48.
- Marur, S.; Forastiere, A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin Proc. 2016;91(3):386 – 96.
- Dhull, K.; Atri, R.; Dhankhar, R.; Chauhan, A.; Kaushal, V. Major Risk Factors in Head and Neck Cancer: A Retrospective Analysis of 12-Year Experiences. World J Oncol. 2018 Jun; 9(3): 80–84. [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer Available from http://globocan.iarc.fr. 2012.
- Gregory, T.; Scott, M.; George, E.; Waun, K. In: Cancer Medicine. James FH, Emil FN, Robert CB, Donald WK, Donald LM, Ralph RW, editors. Philadelphia: Lea and Febiger; 1993. Head and neck cancer; pp. 1211–1274.
- Cogliano, V.; Baan, R.; Straif, K.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V. et al. Preventable exposures associated with human cancers. J Natl Cancer Inst. 2011;103(24):1827–1839. [CrossRef]
- Zygogianni, A.; Kyrgias, G.; Karakitsos, P.; Psyrri, A.; Kouvaris, J.; Kelekis, N.; Kouloulias, V. Oral Squamous Cell Cancer: Early Detection and the Role of Alcohol and Smoking. Head Neck Oncol.2011;3(2) . [CrossRef]
- Zygogianni, A.; Kyrgias, G.; Mystakidou, K.; Antypas, C.; Kouvaris, J.; Papadimitriou, C.; Armonis, V.; Alkati, H.; Kouloulias, V. Potential Role of the Alcohol and Smoking in the Squamous-Cell Carcinoma of the Head and Neck: Review of the Current Literature and New Perspectives. Asian Pac J Cancer. 2011;12(2):339-344.
- Machiels, J.; Rene Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. et al. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(11):1462–75. [CrossRef]
- Vokes, E. In Harrison's Principles of Internal Medicine. Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Maltin JB, Kasper DL, et al., editors. Vol. 16. New York: McGraw Hill; 2005. Head and neck cancer; pp. 503–506.
- Pai, S.; Westra, W.; Molecular pathology of Head and Neck cancer: implications for diagnosis, prognosis, and treatment. Annu Rev Pathol. 2009;4:49-70.
- Mali, SB. Adaptive Radiotherapy for Head Neck Cancer. Journal Of Maxillofacial and Oral Surgery. 2016;15(4): 549-554. [CrossRef]
- Kouloulias, V.;Thalassinou, S.; Platoni, K.; Zygogianni, A.; Kouvaris, J.; Antypas, C.; Efstathopoulos, E.; Kelekis, N. The treatment outcome and radiation-induced toxicity for patients with head and neck carcinoma in the IMRT era: a systematic review with dosimetric and clinical parameters. Biomed Res Int. 2013:401261. [CrossRef]
- Ackerstaff, A.; Rasch, C.; Balm, A.; de Boer, J.; Wiggenraad, R.; Rietveld, D. et al. Five-year quality of life results of the randomized clinical phase III (RADPLAT) trial, comparing concomitant intra-arterial versus intravenous chemoradiotherapy in locally advanced head and neck cancer. Head Neck. 2012;34(7):974–80.
- Langendijk, J.; Doornaert, P.; Verdonck-de Leeuw, I.; Leemans, C.; Aaronson, N.; Slotman, B. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J Clin Oncol. 2008;26(22):3770–3776 . [CrossRef]
- Yeh Shyh-An. Radiotherapy for Head and Neck Cancer. Semin Plast Surg. 2010; 24(2): 127–136.
- Heukelom, J.; Fuller, C. Head and Neck Cancer Adaptive Radiation Therapy (ART): Conceptual Considerations for the Informed Clinician. Semin Radiat Oncol. 2019; 29(3): 258–273. [CrossRef]
- Surucu, Murat.; Shah, K.; Roeske, J.; Choi, M.; Small, W.; Emami, B. Adaptive Radiotherapy for Head And Neck Cancer. Technol Cancer Res Treat. 2017; 16(2): 218-223. [CrossRef]
- Aly, F.; Miller, A.; Jameson, M.; et al. A prospective study of weekly intensity modulated radiation therapy plan adaptation for head and neck cancer: improved target coverage and organ at risk sparing. Australas Phys Eng Sci Med. 2019; 42:43–51 . [CrossRef]
- Bhandari, V.; Patel, P.; Gurjar, O.; Lal Gupta, K. Impact of repeat computerized tomography replan in the radiation therapy of head and neck cancers. J Med Phys. 2014; 39(3):164-168. [CrossRef]
- Mahmoud, O.; Reis, I.; Samuels, M.; Elsayyad, N.; Bossart, E.; Both, J.; et al. Prospective Pilot Study Comparing the Need for Adaptive Radiotherapy in Unresected Bulky Disease and Postoperative Patients With Head and Neck Cancer. Technol Cancer Res Treat. 2017; 16(6); 1014-1021. [CrossRef]
- Glide-Hurst, C.; Lee, P.; Yock, A.; Olsen, J.; Cao, M.; et al. Adaptive radiation therapy (ART) strategies and technical considerations: A state of the ART review from NRG Oncology. Int J Radiat Oncol Biol Phys. 2021; 109(4): 1054–1075. [CrossRef]
- Alfouzan Afnan. Radiation therapy in head and neck cancer. Saudi Med J. 2021;42(3): 247–254.
- Figen, M.; Oksuz, D.; Duman, E.; et al. Radiotherapy for Head and Neck Cancer: Evaluation of Triggered Adaptive Replanning in Routine Practice. Front Oncol. 2020; 10: 579917. [CrossRef]
- Nasser, N.; Yang, G.; Koo, J.; Bowers, M.; Greco, K. et al. A head and neck treatment planning strategy for a CBCT-guided ring-gantry online adaptive radiotherapy system. J Appl Clin Med Phys. 2023; e14134. [CrossRef]
- Glide-Hurst, C.; Lee, P.; Yock, A.; Olsen, J.; Cao, M.; Siddiqui, F.; Parker, W.; et al. Adaptive Radiation Therapy (ART) Strategies and Technical Considerations: A State-of-the-ART Review From NRG Oncology. Int J Radiat Oncol Biol Phys. 2021; 109(4):1054-1075. [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers, Version 2.2020. J Natl Compr Canc Netw. 2020;18(7):873-898.
- Nutting, C.; Morden, J.; Harrington, K.; Urbano, J.; Bhide, S.; et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomized controlled trial. Lancet Oncol. 2011;12(2):127-136.
- Shang, Q.; Liu Shen, Z.; Ward, M.; Joshi, N.; Koyfman, S.; Xia, P. Evolution of treatment planning techniques in external-beam radiation therapy for head and neck cancer. Applied Radiat Oncol 2015; 4(3):18-25. [CrossRef]
- Connell, P.; Hellman, S. Advances in radiotherapy and implications for the next century: a historical perspective. Cancer Res 2009; 69: 383–392. [CrossRef]
- de Arruda, F.; Puri, D.; Zhung, J.; et al. Intensity-modulated radiation therapy for treating oropharyngeal carcinoma: the Memorial Sloan-Kettering Cancer Center experience. Int J Radiat Oncol Biol Phys. 2006;64(2):363-373.
- Mallick, I.; Waldron, J.; Radiation therapy for head and neck cancers. Semin Oncol Nurs 2009; 25: 193–202.
- Ghosh, A.; Gupta, S.; Johny, D.; Bhosale, V.; Negi, M. A Study to Assess the Dosimetric Impact of the Anatomical Changes Occurring in the Parotid Glands and Tumour Volume during Intensity Modulated Radiotherapy using Simultaneous Integrated Boost (IMRT-SIB) in Head and Neck Squamous Cell Cancers. Cancer Med. 2021;10:5175–5190. [CrossRef]
- Burela, N.; Soni, T.; Patni, N.; Natarajan, T.; Adaptive intensity-modulated radiotherapy in head-and-neck cancer: A volumetric and dosimetric study. J. Cancer Res. Ther. 2019;15:533–538.
- Lee, C., Langen, K., Lu, W., Haimerl, J., Schnarr, E., Ruchala, K., Olivera, G., Meeks, S., Kupelian, P., Shellenberger, T., et al. Assessment of parotid gland dose changes during head and neck cancer radiotherapy using daily megavoltage computed tomography and deformable image registration. Int J Radiat Oncol Biol Phys. 2008;71:1563–1571. [CrossRef]
- Thomson, D., Beasley, W., Garcez, K., Lee, L., Sykes, A., Rowbottom, C., Slevin, N. Relative plan robustness of step-and-shoot vs rotational intensity–modulated radiotherapy on repeat computed tomographic simulation for weight loss in head and neck cancer. Med Dosim. 2016;41:154–158. [CrossRef]
- Buciuman, N.; Marcu, L. Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy. J Pers Med. 2022; 12(5):668. [CrossRef]
- Nicosia, L.; Sicignano, G.; Rigo, M.; Figlia, V.; Cuccia, F.; De Simone, A.; Giaj-Levra, N.; Mazzola, R.; Naccarato, S.; Ricchetti, F.; et al. Daily dosimetric variation between image-guided volumetric modulated arc radiotherapy and MR-guided daily adaptive radiotherapy for prostate cancer stereotactic body radiotherapy. Acta Oncol. 2021, 60, 215–221. [CrossRef]
- Lee, V.; Schetllno G., Nisbet, A. UK adaptive radiotherapy practices for head and neck cancer patients. BJR Open. 2020; 11;2(1):20200051. [CrossRef]
- Barker, J.; Garden, A.; Ang, K.; et al. Quantifying volumetric and geometric changes occurring during fractionated radiotherapy for head-and-neck cancer using an integrated CT/linear accelerator system. Int J Radiat Oncol Biol Phys. 2004;59(4):960-970.
- Abdelhafiz, N.; Mahmoud, D.; Gad, M.; Essa, H.; Morsy, A. Effect of definitive hypo-fractionated radiotherapy concurrent with weekly cisplatin in locally advanced squamous cell carcinoma of the head and neck. J Med Life. 2023;16(5):743-750. [CrossRef]
- Baujat, B.; Borhis, J.; Blanchard, P.; et al. Hyperfractionated or accelerated radiotherapy for head and neck cancer. Cochrane Database Syst Rev. 2010;2010(12): CD002026. [CrossRef]
- Lacas, B.; Bourhis, J.; Overgaard, J.; et al. Role of radiotherapy fractionation in head and neck cancers (MARCH): an updated meta-analysis. Lancet Oncol. 2017; 18(9):1221-1237. [CrossRef]
- Bourhis, J.; Overgaard, J.; Audry, H.; et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006; 368(9538):843-854. [CrossRef]
- Bertholet, J.; Anastasi, G.; Noble, D.; Bel, A.; van Leeuwen, R.; Roggen, T.; et al. Patterns of practice for adaptive and real-time radiation therapy (POP-ART RT): part II offline and online plan adaption for interfractional changes. Radiother Oncol.2020; 33:333–338. [CrossRef]
- Fu, K.; Pajak, T.; Trotti, A.; et al. A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys 2000;48(1):7-16. [CrossRef]
- Bobić, M.; Lalonde, A.; Nesteruk, K.; et al. Large anatomical changes in head-and-neck cancers – A dosimetric comparison of online and offline adaptive proton therapy. Clin Transl Radiat Oncol. 2023; 40:100625. [CrossRef]
- Capelle, L.; Mackenzie, M.; Field, C.; Parliament, M.; Ghosh, S.; Scrimger, R. Adaptive radiotherapy using helical tomotherapy for head and neck cancer in definitive and postoperative settings: initial results. Clin Oncol (R Coll Radiol). 2012; 24(3):208-215. [CrossRef]
- Lu, J.; Ma, Y.; Chen, J.; Wang, L.; et al. Assessment of anatomical and dosimetric changes by a deformable registration method during the course of intensity-modulated radiotherapy for nasopharyngeal carcinoma. J Radiat Res. 2014;55(1):97–104. [CrossRef]
- Olteanu, L.; Berwoutz, D.; Madani, I.; et al. Comparative dosimetry of three-phase adaptive and non-adaptive dose-painting IMRT for head-and-neck cancer. Radiother Oncol. 2014; 111(3): 348–353. [CrossRef]
- Reali, A.; Anglesio, S.; Mortellaro, G.; et al. Volumetric and positional changes of planning target volumes and organs at risk using computed tomography imaging during intensity-modulated radiation therapy for head–neck cancer: an ‘‘old’’ adaptive radiation therapy approach. La Radiologia Medica. 2014; 119:714–720. [CrossRef]
- Castelli, J.; Simon, A.; Louvel, G.; Henry, O.; Chajon, E.; et al. Impact of head and neck cancer adaptive radiotherapy to spare the parotid glands and decrease the risk of xerostomia. Radiat Oncol. 2015; 10:6. [CrossRef]
- Zhang, P.; Simon, A.; Rigaud, B.; Castelli, J.; Ospina Arango, J.; et al. Optimal adaptive IMRT strategy to spare the parotid glands in oropharyngeal cancer. Radiother Oncology. 2016;120 (1): 41–47. [CrossRef]
- van Kranen, S.; Hamming-Vrieze, O.; wolf, A.; et al. Head and Neck Margin Reduction With Adaptive Radiation Therapy: Robustness of Treatment Plans Against Anatomy Changes. Intern J Radiat Oncol Biol Phys. 2016; 96(3):653-660. [CrossRef]
- Dewan, A.; Sharma, S.; Dewan, A.; et al. Impact of Adaptive Radiotherapy on Locally Advanced Head and Neck Cancer - A Dosimetric and Volumetric Study. Asian Pac J Cancer Prev. 2016; 17 (3): 985-992. [CrossRef]
- Deng, S.; Liu, X.; Lu, H.; Huang, H.; Shu, L.; et al. Three-Phase Adaptive Radiation Therapy for Patients With Nasopharyngeal Carcinoma Undergoing Intensity-Modulated Radiation Therapy: Dosimetric Analysis. Technol Cancer Res Treat.2017; 16(6): 910–916.
- Castelli, J.; Simon, A.; Laford, C.; Perichon, N.; Rigaud, B.; Chajon, E.; et al. Adaptive radiotherapy for head and neck cancer. Acta Oncologica. 2018; 57(10): 1284-1292. [CrossRef]
- Mnejja, W.; Daoud, H.; Fourati, N.; Sahnoun, T.; Siala, W.; Farhat, L.; Daoud, J.; et al. Dosimetric impact on changes in target volumes during intensity-modulated radiotherapy for nasopharyngeal carcinoma. Rep Pract Oncol Radiother. 2020; 25(1); 41-45. [CrossRef]
- Hay, L.; Paterson, C.; McLoone, P.; Miguel-Chumacero, E.; Valentine, R.; et al. Analysis of dose using CBCT and synthetic CT during head and neck radiotherapy: A single centre feasibility study. Tech Innov Patient Support Radiat Oncol. 2020;23(14):21-29. [CrossRef]
- Avkshtol, V.; Meng, B.; Shen, C.; Choi, B.; Okoroafor, C.; et al. Early Experience of Online Adaptive Radiation Therapy for Definitive Radiation of Patients With Head and Neck Cancer. Advances in Radiat Oncol. 2023; 8. 101256. [CrossRef]
- Duma, M.; Kamper, S.; Schuster, J.; Winkler, C.; Geinitz, H. Adaptive radiotherapy for soft tissue changes during helical tomotherapy for head and neck cancer. Strahlenther Onkol. 2012; 188(3):243–247. [CrossRef]
- Jensen, A.; Nill, S.; Huber, P.; Bendl, R.; Debus, J.; Munter, M. A clinical concept for interfractional adaptive radiation therapy in the treatment of head and neck. Int J Radiat Oncol Biol Phys. 2012; 82(2): 590-596. [CrossRef]
- Schwartz, D.; Garden, A.; Shah, S.; Chronowski, G.; Sejpal, S.; et al. Adaptive radiotherapy for head and neck cancer - Dosimetric results from a prospective clinical trial. Radiother Oncology. 2013; 106 (1): 80–84. [CrossRef]
- Zhao, L.; Wan, Q.; Zhou, Y.; Deng, X.; Xie, C.; Wu, S. The role of replanning in fractionated intensity modulated radiotherapy for nasopharyngeal carcinoma. Radiother Oncology. 2011; 98 (1): 23–27. [CrossRef]
- Yang, H.; Hu, W.; Wang, W.; Chen, P.; Ding, W.; Luo, W. Replanning During Intensity Modulated Radiation Therapy Improved Quality of Life in Patients With Nasopharyngeal Carcinoma. Int J Radiat Oncol Biol Phys. 2013; 85(1):e47-54. [CrossRef]
- Chen, A.; Daly, M.; Cui, J.; Mathai, M.; Benedict, S.; Pardy, J. Clinical outcomes among patients with head and neck cancer treated by intensity-modulated radiotherapy with and without adaptive replanning. Head Neck. 2014; 36(11): 1541-1546. [CrossRef]
- Mostafa El-Shahat, M.; Elshishtawy, W.; Al-Agamawi, A. Evaluation of Adaptive Radiation Therapy in Treatment of Locally Advanced Head and Neck cancers. Al-Azhar Intern Med J. 2021; 2(12): 51-58. [CrossRef]
- Zhou, X.; Wang, W.; Zhou, C.; Zhu, J.; Ding, W. et al. Long-term outcomes of replanning during intensity-modulated radiation therapy in patients with nasopharyngeal carcinoma: An updated and expanded retrospective analysis. Radiother Oncol. 2022; 170:136–142. [CrossRef]
- Kataria, T.; Gupta, D.; Goyal, S.; Bisht, S.; Basu, J. et al. Clinical outcomes of adaptive radiotherapy in head and neck cancers. Br J Radiol. 2016; 89: 20160085. [CrossRef]
Figure 1.
Flow chart diagram.
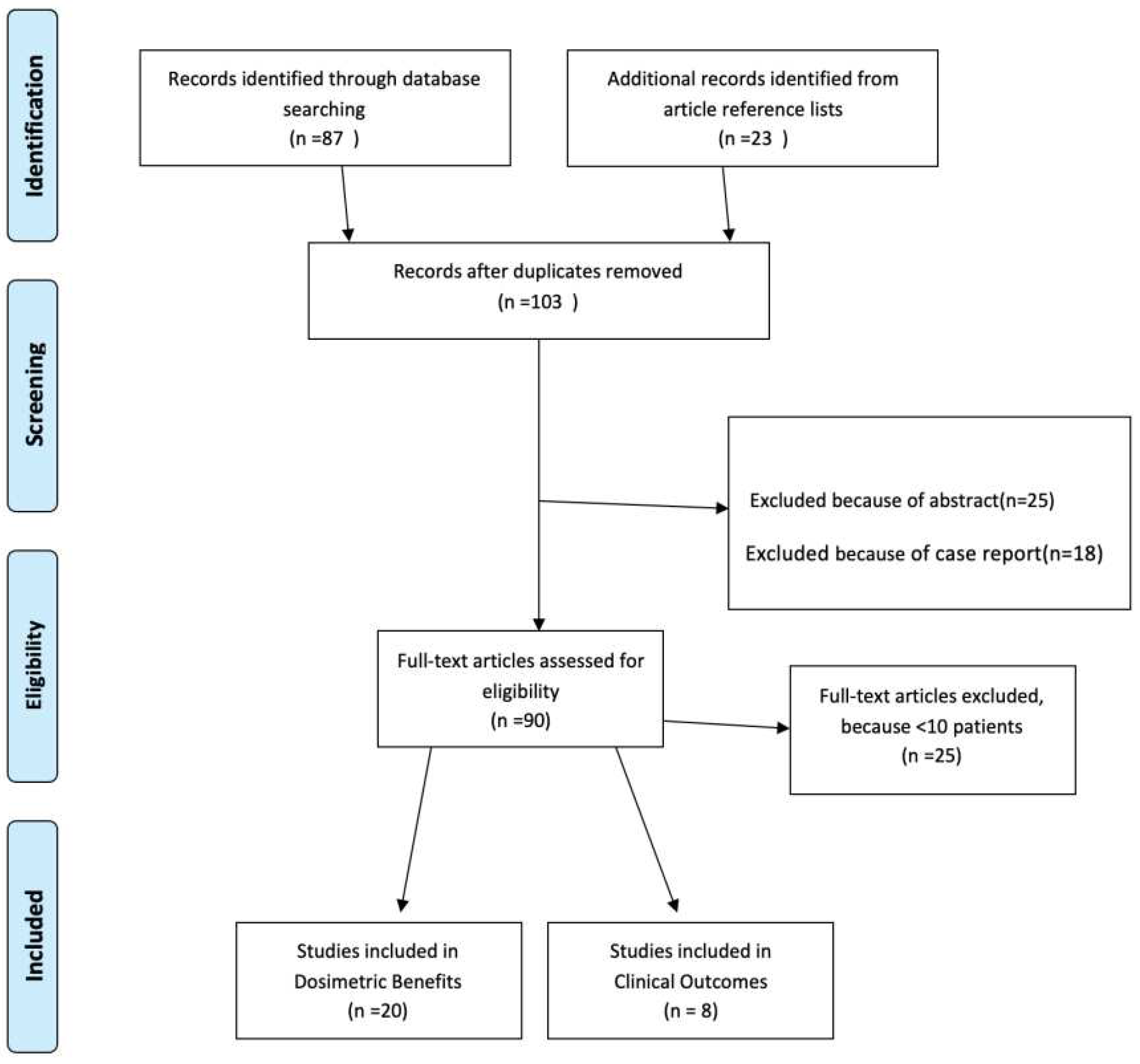
Table 1.
Main differences between Online ART and Offline ART.
| Aspects | Online ART | Offline ART |
|---|---|---|
| Timing of Plan Adaptation | Real-time, daily or even intra-fractional | Periodic, often weekly or bi-weekly |
| Imaging Frequency | Daily, often using CBCT | Periodic, less frequent imaging (e.g., weekly) |
| Adaptation Response Time | Immediate | Delayed, typically days to weeks |
| Treatment Efficiency | Time-consuming, may extend treatment duration | Less time-consuming, may minimize treatment interruptions |
| Anatomical Changes | Continuously monitored | Assessed periodically |
| Resource Requirements | Requires significant resources, including advanced imaging equipment | Requires fewer resources, often relies on conventional imaging |
| Precision in Tumor Targeting | High, allowing rapid response to changes | Good, with adaptations at intervals |
| Patient Comfort and Experience | Potential for longer treatment times | Potential for more consistent treatment times |
| Handling of Clinical Uncertainties | Offers real-time adaptation to uncertainties | May not address uncertainties as quickly |
| Clinical Applications | Applicable in dynamic or rapidly changing clinical scenarios | Suited for more stable anatomical conditions |
Table 3.
ART Studies - CLINICAL OUTCOMES.
| No PTS | REPLANNING STRATEGIES | CLINICAL ENDPOINT | |||||||
| Author (year) | ART (NO ART) |
TUMOR SITE |
TOTAL DOSE (Gy) |
No of Replanning |
Timing (fraction) |
Follow-up (months) |
LOCOREGIONAL CONTROL and SURVIVAL | ACUTE TOXICITY (%) |
LATE TOXICITY |
| Zhao (2011) | 33 (66) |
NPC | 70 | 1 | 15th (+/- 5) | 38 | 3-year LRFS 72.7% (ART); 68.1% (No-ART) p = 0.3 | NR | Less xerostomia and mucosal with ART for N2 and N3 pts |
| Schwartz (2012) | 22 (0) |
OPC | 66-70 | 1 or 2 | 16th and 22nd | 31 | 2-year LRC=95% | G III mucositis: 100%, G II xerostomia: 55% G III xerostomia: 5% | Full preservation or functional recovery of speech and eating at 20 months |
| Yang (2013) | 86 (43) |
NPC | 70-76 | 1 or 2 | 15th and/or 25th Fr |
29 | 2-year LRC = 97.2% (ART); 82.2% (No-ART) p =0.04 2-year OS = 89.8% (ART); 82.2% (No-ART) p=0.47 | NR | Improvement in OoL with ART |
| Chen (2014) | 51 (266) |
LAHNC | 60 b 70 μ |
1 | 40 Gy (10-58 Gy) |
30 | 2-year LRC = 88% (ART); 79% (No-ART) p =0.01 2-year OS = 73% (ART); 79% (No-ART) p=0.55 | G III : 39% (ART) 30% (No-ART) P = .45 |
G III =14% (ART) 19% (No-ART) P = .71 |
| Kataria (2016) | 36 (0) |
LAHNC | 70 | 1 | 54 Gy | ----- | 2-year DFS = 72%. 2-year OS = 75% | G II-III mucositis=100% | – G II xerostomia = 8% – G II mucosal = 11%. – No G III toxicity |
| Surucu (2017) | 51 (17) |
LAHNC | 70.2 | 1 | 37.8 Gy (47 – 48.6) | 17.6 mos | Median DFS: 14.8 (0.9 – 57.5) mos Median OS: 21.1 (4.5 – 61.4) mos Residual Disease: 11.8 % Locoregional Control: 64.7% Metastatic disease: 23.5% |
Mucositis 35.3% Xerostomia NA Dysphagia 41.2% |
Mucositis NA Xerostomia 3.3% Dysphagia 20% |
| Mostafa (2021) | 49 (0) |
LAHNC | 70 | 1 | 42 Gy (37-44.1) | median 18 months (6.5 – 31) |
1-year PFS 89.7%; 2-year PFS 70.2% 1-year OS 89%; 2-year OS 83 % |
G II-III mucositis: 32.6 – 36.7 % G II-III Xerostomia: 44.9 - 16.3% | --------- |
| Zhou (2022) | 290 (147) |
NPC | NA | 1-2 | 15th-25th Fr | median (months) 104 ART; 96 no-ART |
8-year LRFS ART 87.4%; No-ART 75.6% 8-year DMFS ART 82.3%; No-ART 76.8% OS: 60.9 % (ART) / 59.4 % (no-ART) |
NR | G I-II Xerostomia: ART 96.5% - no-ART 90.5% G III-IV Xerostomia: ART 3.5% - no-ART 9.5% |
Nb pts: number of patients; LAHNC: locally advanced head and neck cancer; OPC: oropharynx cancer; NPC: nasopharyngeal carcinoma; Nb: number; ART: adaptive radiotherapy; Fr: fraction; LRC: loco-regional control;LRFS: loco-regional free survival; DFS: disease-free survival; OS: overall survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



