
Submitted:
29 December 2023
Posted:
30 December 2023
You are already at the latest version
Abstract
Rapid haemostasis during surgery is essential when one wants to reduce the duration of opera-tions, reduce the need for transfusions, and above all when one wants to achieve better patient management. The use of haemostatic agents, sealants and adhesives improves the haemostatic process by offering several advantages, especially in vascular surgery. These agents vary widely in their mechanism of action, composition, ease of application, adhesion to wet or dry tissue, im-munogenicity and cost. The most used are cyanoacrylate-based glues (Glubran 2) or polysaccharide hydrogel-microsphere powder (AristaTMAH). This work is based on a retrospective study carried out on a sample of patients with different vascular diseases (FAV, pseudoaneurysm and PICC application) in which two different haemostatic sealants were used. The aim was to assess the safety, the advantages and the ability of both sealants to activate the haemostatic process at the affected site, also in relation to their chemical-physical characteristics. The obtained results showed that the application of Glubran 2 and AristaTMAH as surgical wound closure systems is effective and safe as the success achieved was ≥94% on anastomoses of FAV; 100% on stabilization of Picc catheters; ≤95% on pseudoaneurysms.
Keywords:
tissue adhesive
; cyanoacrylate-based glues
; polysaccharide hydrogel-microsphere powder
; vascular application-
1. Introduction
The tissue adhesives are biomaterials used in the treatment of hemostasis, wound closure and tissue repair [1]. Compared to sutures, the advantages of using these adhesives relate to their ability to polymerize in situ, to adapt to complex wound contours and dimensions (sufficient mechanical flexibility), to be biocompatible, to possess adequate mechanical and physical properties (such as burst strength, tensile strength and shear strength and shear resistance), to have high bond strength to moist tissue or organs, and finally to be easily applied [2,3]. They fall into two categories: (i) tissue adhesives based on natural polymers (fibrin, albumin and gelatin); (ii) synthetic tissue glues, based on cyanoacrylate, poly(ethylene glycol) (PEG), catechol and methacrylic anhydride [4,5,6]. The design of an effective tissue adhesive is related to a careful tissue-adhesive interface that includes an adhesion layer, where the adhesive makes intimate contact with the tissue, and an adhesive matrix, which consists of the polymer network of the substances that make up the adhesive. The adhesion layer anchors to the underlying tissue through chemical, physical or covalent and non-covalent bonds; while the adhesive matrix provides structural support to the adhesion layer and determines the chemical and physical characteristics of the adhesive [7]. From the 1950s onwards, cyanoacrylate glue was only used for wound closure; in 2000 it was finally approved its use for internal use in the treatment of arteriovenous malformations as a liquid gel embolic system [6]. Cyanoacrylate comes in four forms: methyl-2-cyanoacrylate (2-MCA),ethyl-2-cyanoacrylate (2-ECA), n-butyl-2-cyanoacrylate (nBCA) isobutyl-cyanoacrylate (ICA) and 2-octyl-cyanoacrylate (2-OCA). The short-chain forms (2-MCA, 2-ECA) are rarely used due to their rapid degradation and toxic effects; whereas the long-chain forms (nBCA, 2-OCA) are the most widely used in industry and medicine because they provide a strong and rigid bond in contact with tissues [8]. In fact, having a consistency like that of a liquid gel at room temperature, when it comes into contact with basic substances (such as water, blood, body tissue or moisture) or negatively charged ions, it undergoes an exothermic polymerization that hardens it into a solid adhesive film [9,10]. The cyanoacrylate glue used in this work is Glubran 2, a CE-certified Class III surgical medical device for internal and endovascular use [11,12]. This device has undergone preclinical and clinical testing to assess its safety. In particular, it has undergone biocompatibility testing, performance testing and animal studies (depending on the application). Biocompatibility tests are trained according to Good Laboratory Practice (GLP; 21 CFR 58) in accordance with International Organization for Standardization (ISO) 10993. Laboratory tests demonstrating safety and efficacy prior to animal studies include the following: cytotoxicity - International Organization for Standardization (ISO10993-5), sensitization and irritation (ISO 10993-10), implantation (ISO 10993-6), pyrogenicity, acute, subchronic, and chronic toxicity (ISO10993-11), hemolysis (ISO 10993-4), genotoxicity (ISO 10993-3). Animal studies for specific applications of Glubran have been conducted on sheep, dogs, rats, mice and pigs. In addition to these tests, as bioadhesives in contact with blood degrade with time, degradation studies and blood-compatibility studies are performed on them [13]. In particular, in the case of Glubran 2, several models were developed to mimic different clinical situations. For example, the ascending pharyngeal artery in the pig serves as a model for arteriovenous malformations (AVMs). Aneurysms, including aortic aneurysms, have been created in rabbits and pigs and arteriovenous fistulas in dogs [14].
This device has a high adhesive capacity in a humid environment (viable tissue) with haemostatic, sealing and bacteriostatic (barrier) properties, high elasticity and tensile strength for waterproof and breathable bonding, a low polymerization temperature (45°C) that starts on contact with the tissue (1-2 seconds) and is complete in 60-90 seconds [15,16]. It also possesses high biocompatibility and slow biodegradability, does not cause release of toxic products and the minimum use quantity is 1 ml T20 cm2 . The film formed after application of this glue can be easily punctured by suture needles and the glue when mixed with Lipiodol® can be opacified and its rate of polymerization can be altered and favoring the formation of a less uniform and more flocculent polymer with a gel-like consistency (embolizing agent) [17]. Glubran 2 is commercially available as ready-to-use disposable applicator devices, formulated as a clear liquid in single-dose bottles of 0.25; 0.50; 1 ml to be stored between 2 and 8°C. Blood vessels that are subjected to Glubran 2 injection are embolized via three mechanisms: (1) cast and thrombus formation [18,19], (2) the adhesion to the inner vascular wall [20], and (3) damage to the vascular endothelium caused by an inflammatory response [21]. Another device used in the vascular field with hemostatic action is the AristaTMAH an absorbable topical hemostatic that uses hydrophilic polysaccharide hemosphere (MPH) technology to help control blood loss [22]. The product is derived from purified vegetable starch and is supplied as a powder substance with a variety of applicators. Starch is an abundant hydrophilic natural biopolymer composed of anhydroglucose units that have hydrophilicity, biodegradability, biocompatibility, and similarity to skin extracellular matrix, making them useful for various biomedical applications. Hydrophilicity and biodegradability are two crucial properties of starch granules that belong to the passive hemostats class and act as a ‘‘molecular sieve’’ by extracting fluids and blood [23,24]. Instead, the AristaTMAH haemostatic activity is activated when, upon meeting the liquid components of the blood, they are absorbed by the polysaccharide hydrogel-hemospheres and are concentrated to form a molecular network (gel) that allows efficient thrombus formation through natural coagulation (Figure 1). In fact, in situ gelling polymeric systems having functional groups that can react with functional groups present in tissue, have been found to be adhesive in nature [25]. This device has been approved by the FDA precisely because it enhances the biological process of coagulation through the formation of a natural haemostatic plug. Also in the case of AristaTMAH, clinical and preclinical tests to assess its safety are based on biocompatibility tests, performance tests and animal studies. Animal studies are mainly carried out on 6-8 week old Sprague-Dawley rat models in which the surgical site is performed in the abdominal area. Tests showed no signs of inflammation at any time after application of the powder [26]. The aim of this work was to evaluate the effectiveness and safety of the two devices in the surgical field by differentiating their application based on the pathology treated and the hemostasis mechanism exerted on it.
2. Materials and Methods
2.1. Study design
One surgical glues e one powder for internal use were tested: Glubran 2 (supplied by General Enterprise Marketing GEM s.r.l, Viareggio, Lucca, Italy) and AristaTMAH (C. R. Bard, Inc. - Davol, Warwick, RI).This study is an analysis of data collected retrospectively at the Cosenza Hospital (Cosenza, Italy) of patients who underwent open/endovascular surgical treatments requiring the use of Glubran 2 and in a given sample of patients, AristaTMAH powder was applied at the site of anastomosis instead of glue, and a comparison of the two devices was carried out to test their stability and effectiveness at that site of action between January 2023 and September 2023. Specifically, these devices were effective in promoting surgical site closure by inducing hemostasis processes through different mechanisms.
Inclusion criteria were: 1) echo-guided venous access for endovascular placement of catheter for drug infusion (sheath size 4Fr, Maxflo expert Vygon, Padova, Italy); 2) surgical access for arteriovenous fistula packing for hemodialysis; 3) surgical access for emptying and exclusion of iatrogenic pseudo-aneurysm; 4) age over 18 years.
Exclusion criteria were: 1) age under 18 years; 2) pregnancy; 3) last hemodialysis session at least 36 h distant; 4) bleeding risk higher than the recommendations of the CIRSE Standards of Practice on the management of peri-operative anticoagulation [27]; 5) presence of arterial thrombosis of the pseudoaneurysm and absence of echocolour and internal flowmetry; 6) history of superficial or deep vein thrombosis of the upper limb or ongoing thrombosis (PICC); 7) INR values >1.5; platelet count <70,000; 8) HB values <8.0 g/dl; 9) white blood cell count >12,000; 10) had Thromboplastine Partial Time values Activated (a-PTT) values > 40 sec; 11) positive Covid Sars-19 nasopharyngeal swab.
2.2. Data collections and procedure
All patients underwent pre-treatment evaluation with bed-side ambulatory ultrasound using a SIEMENS S2000 ultrasound scanner (7.5 Mhz linear probe) repeated peri-operatively in the operating room using a SONOSITE ultrasound scanner (7.5 Mhz linear probe) with transducer coverage under sterile conditions. In patients with iatrogenic arterial pseudoaneurysm, CT angiography (CTA) was performed. The choice of tissue adhesive depended on the operator's preference according to the access technique used (endovascular and/or surgical), the site to be treated and the type of material required to activate a haemostatic process at the site concerned. The surgical procedure for packing an arteriovenous fistula for hemodialysis was always performed in the operating theatre [28,29]. Having identified the site of anastomosis between the vein and the artery (radius cephalic/humeral basilic) by ultrasound, local anaesthetic was infiltrated with an incision of the skin at the level of the distal part of the left forearm. The cephalic vein was identified and isolated, which appeared to be of normal calibre (3-5 mm), and the radial artery was isolated (Figure 2).
After systemic heparinization by the anaesthesiologist with 2.000 I.U. of sodium heparin, proximal and distal clamping of the radial artery was performed, the radial artery was tomified and the termo-lateral anastomosis was made with pro-lene 7.0. At declamping, blending bleeding from the anastomosis on the arterial side due to arterial calcifications was noted; therefore, Glubran 2 was applied to the anastomosis site at the arterial suture passage points (Figure 3A).In a sample of patients, AristaTMAH powder was applied at the site of anastomosis instead of glue, and a comparison of the two devices was carried out to test their stability and effectiveness at that site of action (Figure 3B).
The procedure for stabilization and fixation of the PICCs (Peripherally Inserted Central Catheters) took place in the angiography room after identification by ultrasound of the endovascular access site and exclusion of in situ thrombosis [30,31] (Figure 4). If the identified site is affected by venous thrombosis, one goes to the other arm.
In most cases the catheter and venipuncture is performed in the middle third of the right arm, above the elbow crease to identify the brachial or basilic vein. Under radioscopic guidance, the catheter was led up to the superior vena cava. When venipuncture on the forearm is not possible, it is necessary to use the veins on the back of the hand.No antibiotic therapy is administered as the ultrasound-guided procedure is with percutaneous access. The indication for the implantation of PICCs indicated if patients must be given therapy for an infusion time of more than 6 days. The use of these devices has brought many benefits in addition to improving the quality of life of cancer patients as it decreases pain and anxiety during the infusion of chemotherapy drugs, ensures greater safety in the administration of antiblastic drugs, and a significant reduction in repeated venipuncture of patients and the consequent reduction in skin lesions and superficial phlebitis (chemical phlebitis). To stabilize the device and fix it at the percutaneous insertion point, Glubran 2 surgical glue was applied around the catheter (Figure 5a) and the Picc was stabilized (Figure 5b).
The procedure for exclusion and emptying of the pseudoaneurysm took place in the operating theatre after ultrasound identification of the radial artery and the periarterial blood collection site (Figure 6).
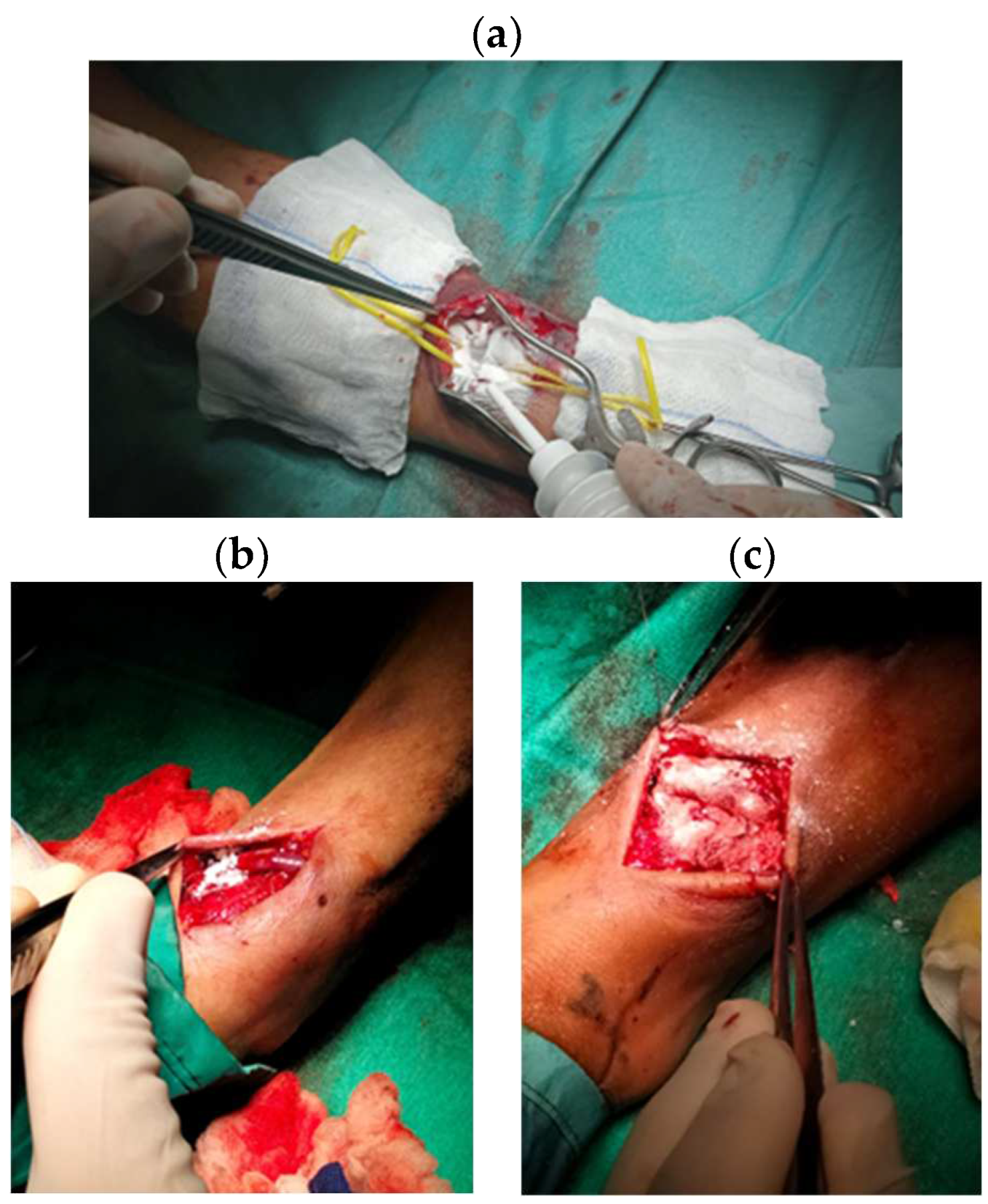
After anaesthesia, an incision was made distal to the right forearm along the anatomical course of the artery [32,33]. Next, the radial artery upstream and downstream of the pseudoaneurysm was isolated, the pseudo-aneurysm was isolated from the surrounding tissues (Figure 7a) and incised to evacuate it (Figure 7b).
After emptying abundant clot, the iatrogenic lesions on the radial artery wall were in-divided and Glubran 2 haemostatic adhesive was applied (Figure 8).
2.3. Outcomes
The primary objective of this study was to evaluate the efficacy, safety and benefits of using Glubran 2 and AristaTMAH in favouring the activation of haemostatic processes applied to the surgeon's wift closure of arteriovenous fistulas and the repair of iatrogenic damage in patients undergoing surgical and endovascular treatment for the treatment of arteriodosis. Iatrogenic arterial pseudoaneurysm, arteriovenous fistula for hemodialysis and stabilization and fixation of the Picc catheter. Primary technical success was defined by adequate hemostasis obtained in the peri-operative phase within a time frame of less than 5 minutes (in the case of AristaTMAH) and 2 minutes (in the case of Glubran 2) from the time of application of the product and temporary closure of the surgical site with minimal manual compression with sterile gauze. Secondary technical success was defined as hemostasis achieved after the above scheme or after a second subsequent period of manual compression with sterile gauze on the surgical site. Clinical success was defined by the absence of hematoma or bleeding-related peri-lesional collections at follow-up and the absence of peripheral neuropathy. Complications were classified according to SVS (Society for Vascular Surgery clinical practice guidelines) reporting standards and bibliography can be found here [34].
Postoperative hematoma was defined as a palpable mass equal to or greater than 5 cm confirmed by ultrasound, failure to close arterial damage or anastomosis confirmed by echocolordoppler examination and supported by level II imaging ( TC scan).
The diagnosis of neuropathy (radial nerve for radiocephalic fistula, median nerve for humerus basilic fistula, brachial nerve for PICC accesses) requires a specialized neurological consultation.
2.4. Hemostasis Evaluation
After removing the gauze, each lesion was qualitatively assessed for hemostasis at 2, 3, 4, 5, 6, 7 and 10 minutes after application using the validated bleeding scale. After the 10 min hemostasis assessment, the lesions were irrigated with saline and visually assessed to remove excess material not incorporated into the blood clot (AristaTMAH) (Figure 9).In the case of Glubran2 each lesion was qualitatively assessed for hemostasis at 2,3,4,5 min after application using the validated bleeding scale. the operator assessed the patency of the artery by appreciating the flow downstream of the site of use to avoid 'STOP' to blood flow should the haemostatic device migrate into the artery at the site of hemostasis or should the anastomosis become excessively 'stiff' due to the use of the adhesive.
2.5. Statistical analysis
Statistical analyses were conducted on all recruited patients who underwent clinical and ultrasound examinations 1 day and 3 days after surgery, who responded to the telephone interview 30 days after surgery, and who were still alive. The statistical significance threshold for the above tests was set at *P < 0.05.
3. Results
3.1 Study population
During the interval (January 2023-September 2023), 60 patients (n=28 picc, n= 10 with radial or femoral pseudoaneurysms, and n= 22 for arteriovenous fistula packing for hemodialysis) were subjected to Glubran2 and AristaTMAH haemostatic agent application. The mean age of the patients was about 70 years, the mean INR was 1.3 and 56% of the patients were on antiplatelet or anticoagulant therapy (cardioaspirin + xarelt, cardirene, duoplavin), 20% on anticoagulant therapy (low molecular weight heparin or New Oral Anticoagulants or NAO) and 24% on single antiplatelet therapy (Table 1).
3.2 Procedure data
The most used surgical access for hemodialysis fistula placement is the cephalic radius to be performed (for the same vein calibre) on the arm least used by the patient (if right-handed, left-handed, right-handed) (DX 70% of patients, SX 30% of patients). The major site of pseudoaneurysm is the left radial artery (site of interventional cardiologist access) and right femoral artery (site of endovascular access for major endovascular procedures - EVAR aneurysms or carotid artery CAS). In most cases of pseudoaneurysm formation the most frequently used introducer was the 6 Fr (68% of cases) on common femoral artery and proximal radial artery and 7 Fr common femoral artery and distal radial artery (22% of cases) and 10 Fr (10% of cases) on common femoral artery. For patients to undergo arteriovenous fistula in the operating room, antihypertensive (catapresan used) was administered to maintain adequate pressures to open the artery and pack the fistula, sodium heparin to avoid clots during clamping of the artery and preoperative antibiotic as per protocol to avoid infection. For patients undergoing pseudoaneurysm exclusion pre-operative antibiotic and antihypertensive for the same reason as before. Both patients are monitored with continuous electrocardiogram (ECG) and continuous saturation through devices in the anaesthetist's charge. Patients with Peripherally Inserted Central Catheters (PICC) application the procedure does not require systemic antibiotic, instead it requires ECG monitoring to recognize P-wave variation during catheter placement, sealed gown for angio-suite procedure with Rx exposure or only operator sterility if only ultrasound guided. All three procedures require Local Anaesthetic (Lidocaine). The choice of sealant for closure of a lesion was site specific; therefore, in this study Glubran 2 was chosen to ensure hemostasis on arterial lesions with high-pressure blood flow (∼120 mmHg) typical of a declamped artery and to prevent the occurrence of infection related to the presence of Picc between different layers of skin. Gluing made exclusively with glue must effectively resist the physiological loads that tend to pull the tissues away from each other, thus ensuring an even distribution of loads in all affected areas, without compromising the elastic properties of natural fabrics. Glubran 2 glue was found to have a broad spectrum activity against Gram-positive and Gram-negative bacteria, yeast and fungi. The deformation and mechanical pressure exerted by the vascular tissue emphasize the importance of the adhesive's fatigue strength. The choice to use AristaTMAH was made considering the ability of this sealant to act on larger tissue lesions with tassel bleeding, that is, when profuse bleeding occurs at low pressure on an iatrogenic lesion of a parenchymatous tissue. In addition is completely degraded within 24-48 h in vivo.
3.3 Outcomes and follow-up
In the use of Glubran 2, the primary success resulting from the application of this sigillant was ≥94% on anastomoses of arteriovenous fistulas; equal to 100% on stabilization of catheters from Picc; ≤95% on pseudo-aneurysms. Failures, on the other hand, were related to active bleeding after 3 minutes or secondary bleeding in bedside drainage as a result of heparin overload (≥5,000 I.U.) or use of antiplatelet/anticoagulants (not discontinued by the patient before the procedure). In the use of AristaTMAH, the success resulting from its use has been ≥96% on anastomoses of arteriovenous fistulas, demonstrating that, unlike glue, the powder's large specific surface area, high porosity, and exceptional water absorption rate are more effective.
Specifically a suction drainage was applied to all patients undergoing FAV and pseudo aneurysm surgery for continuous monitoring of the surgical site and any blood loss. This drain has been used in dialysis and non-dialysis patients, in treatment with or without NAO and/or EBPM, in treatment with or without antiplatelet. The device is equipped with a lateral centimetric guide for the exact quantification of any blood loss. The nurses note at 1,3,6,24 h the amount present as shown in Table 2 and 3, which if less than 10cc is indicative of no bleeding. The results showed that 96% of patients treated with AristaTMAH after FAV surgery were discharged after 24 h due to absence of bleeding from the surgical site (Table 2); 94% of patients treated with Glubran 2 after FAV surgery were discharged after 24h due to absence of bleeding (Table 2). Other outcome measures in FAV patients treated with AristaTMAH or Glubran 2 were the presence of hematoma at the surgical site and the wound closure process. The results in Table 2 show that 50 % of patients at 24h had hematoma at the surgical site in both treatments, only 10 % had it at 7 days. Healing with follow-up of the surgical wound at 7 days occurred in 95 % of the cases. No patients experienced any adverse effects in both procedures.
In the case of patients undergoing pseudo-aneurysm treatment, the success rate obtained is relative to the use of Glubran 2 alone. Again, patients on dialysis and off-dialysis, treated with or without NAO and/or EBPM, treated with or without antiplatelet were taken into account. After emptying the pseudoaneurysm, a 6-mm PVC drain was applied under suction to monitor postoperative blood loss (Ulmer PVC drainage catheter without needle guide). The results shown in Table 3. show that 93% of the patients treated with Glubran 2 were discharged after 24 hours due to the absence of bleeding from the surgical site (≤ 10 cc), all patients had a hematoma at the surgical site, of which 50% maintained it at 7 days (antiplatelet and NAO/EBPM Therapy patients), while at the 30-day follow-up it had disappeared in all patients. The type of suture used (Vycril or Metal clips) was also taken into account in the follow-up of wound closure and stitch removal. In 95% of the patients in whom a vycril suture was applied, healing occurred at 7 days after the operation, only in 5% no healing occurred (anti-clotting and NAO/EBPM Therapy patients). In 90% of patients with metal clips, healing occurs 7 days after surgery, only 10% without healing (anti-clotting and NAO/EBPM Therapy patients).
Both adhesives did not induce thrombosis within the arterious or venious vessels with which they have come into contact at the treatment site (artery or vein for FAV or vein for Picc apposition or artery as in the case of the pseudoaneurysm). This result emerges after intra-operative postoperative echocolordoppler performed with a Linear L7-11 Mhz probe covered by a sterile protective device applied on it.
3.4 Hemostasis Evaluation
At the end of the 10-minute observation period, the haemostatic success of lesions treated with AristaTMAH was 94%. In most cases of AristaTMAH failure, blood leaked from under a contiguous gel mass or occurred in patients with minimal INR alteration or use of antiplatelets (not discontinued prior to surgery) or anticoagulants. Controlling for differences in the level of pre-treatment bleeding, the median time to hemostasis for AristaTMAH was approximately 5 minutes after its use combined with gentle manual compression by the surgeon. At the end of the 10-minute observation period, the haemostatic success of lesions treated with Glubran 2 was 98%. In the majority of cases of Glubran2 failure, blood leaked between two or more Prolene stitches at the suture site in patients with non-discontinued anticoagulant therapy (NAO) in favor of low molecular weight heparin (EBPM). Controlling for differences in pre-treatment bleeding levels, the median time to hemostasis for Glubran 2 was about 2 minutes after its use with a 5-minute observation time (p≤0.05).

Table 4.
Hemostasis Evaluation of AristaTMAH and Glubran 2.
 
|
3.5 Statistical analysis
The collected data were stored in a Microsoft Excel spreadsheet (Microsoft Inc., Redmond, WA, USA). Statistical analyses were conducted on the number of patients who underwent surgery for FAV, pseudoaneurysm and PICC, who underwent clinical and ultrasound examinations 1 day and 3 days after surgery, who responded to the telephone interview 30 days after surgery and who were still alive. Statistically significant differences were observed in Table 5. To perform these analyses, the unpaired Student's t-test was used and a p-value<0.001 and p≤0.05 was considered statistically significant.
4. Discussion
An ideal sealant, in order to guarantee effective hemostasis in all types of patients undergoing vascular procedures, should be used individually, be a-traumatic without foreign bodies or mechanisms that alter the site it acts on, but above all it should be easy to use, have a success rate of ≥95% and be cost-effective. In this retrospective study, we have focused the attention on the application and the efficacy of two sealants in three differents typologies vascular surgery and in a specific category of patients selected (Scheme 1.) The obtained results show us that the two hemostatics Glubran 2 and AristaTMAH prove to be closure systems with an efficacy of ≥96-99% in the case studies described above. Underlying these positive values is above all the ability of these adhesive fabrics to activate a haemostatic process by exploiting their chemical-physical characteristics. In particular, in the case of Glubran 2, the monomeric structure of cyanoacrylate, consisting of a double-carbon ethylene group with two electro-active reactive functions (cyano-CN and ester-COOR), reacting with the anions or radicals present in human blood or plasma (hydroxyl ions of H2O) through Michael addition reactions, would lead to the formation of a reactive carbanion or radical. The reaction continues until all accessible monomers are exhausted, or until the acid species stop the polymer growth. During polymerization, tissue amines can be added to the polymer chains as a Michael-type initiator, resulting in covalent bonds between the cyanoacrylates and the tissue. This would form a polymeric film that would adhere well to the body tissue, hold the wound edges together and stop bleeding. This would result in a significant reduction of the local activated partial thromboplastin time (APTT), which is favorable with regard to the desired hemostasis as the shortening of the APTT leads to a haemostatic effect and contributes to glue-induced tissue adhesion. The results obtained in operational and 3-day follow-up of patients after treatment show no significant changes in prothrombin activity, fibrinogen, platelet count, total and differential leucocyte count after treatment with Glubran 2. In vivo applications of Glubran 2 also revealed its excellent haemostatic and adhesive properties, in particular in binding biological tissues to each other or to prosthetic implants; the adhesion appeared tenacious immediately after application and consolidated its strength during the completion of the polymerization process in various chemical-physical phases (liquid, gel-like, film), guaranteeing rapid and effective results in vascular surgery. The results obtained from the use of AristaTMAH showed that the porous hydrogel microspheres constituting the powder, once dispersed at the wound site, act as a molecular sieve, capable of contacting and activating platelets, leading to rapid hemostasis through the absorption of water and the concentration of coagulation factors. The powder's powerful osmotic action dehydrates and turns blood into gel, accelerating the normal coagulation process. Evidence from applications of these sealants in the surgical environment has shown that both are safe and effective both as closure devices and as substances capable of stimulating the haemostatic process. Specifically in the surgical cases analyzed, it was observed that Glubran 2 is a device particularly suitable for treating lesion sites where there is high blood pressure (pseudo aneurysm) or where the risk of infection is high (Picc stabilization); while AristaTMAH is a device particularly useful for sealing lesion sites with low blood pressure such as FAVs as it helps control venous, capillary and arteriolar bleeding in general. The failures that occurred in the patient samples examined were related more to complications of the procedure than to the use of sealants. Specifically in the case of FAVs, the discrepancies in luminal diameters between artery and vein (the vein calibre considered 'minimum' for packing the fistula for hemodialysis is at least 3 mm) can cause the anastomosis on the distal radial artery to predispose to ischaemia of the hand (so-called artery steal). The risk is particularly high in elderly and diabetic patients (approx. 5% of our cases = 1 case) due to the parietal sclerosis of the arterial vessel being poorly compensated by the ulnar artery, which is also affected by atherosclerosis of the intima. One of the manouvres to optimize flow in a fistula is to avoid acute angles when the vessels are anastomosed, but when the radial artery is sclerosed acute angles cannot be consistently avoided. it is therefore preferred to perform a terminolateral anastomosis. Another failure that may occur is venous thrombosis at the arterial branch of the fistula (o% of cases in our study). In the application of the PICC, catheter occlusion occurred on average 16 days after catheter placement in an average of 15% of patients (n=4 patients). It is assumed that healthcare workers did not always follow the instructions for the prevention of catheter obstruction and perhaps did not pay attention to the warning signs requiring timely preventive measures; or the patient did not adequately comply with the recommended drug therapy (low molecular weight heparin) or did not carry out impermissible mechanical maneuvres (physical exertion, lifting weight,). Regarding infections, we found a PICC-related BSI rate of 0.42 per 1000 PICC days, which is lower than that reported in the literature. This could be related to the application of Glubran 2, which seals the catheter insertion site by isolating it from the external environment. With regard to the pseudoaneurysm, no arterial occlusion was ever found in the 10 patients treated (0% arterial occlusion) and wound dehiscence with edge infection and fibrin formation in 2% of the cases (2 patients), thought to be due to the excessive weakness of the skin which was punctured, then stretched by the pseudoaneurysm and then incised in the operating theatre and sutured.
No adverse reactions related to the occurrence of haemorrhage and/or allergic reactions have been reported in the literature from in vitro tests and in vivo application of AristaTMAH, as also demonstrated by the clinical cases we analyzed. At discharge and 7-day follow-up, no patients reported systemic allergic reactions (no tearing or itchy eyes, no nasal discharge, no rhinorrhoea, no sneezing) or local allergic reactions (urticaria, itchy skin). With regard to the clinical cases we considered for the application of Glubran 2, it can be stated that no distal leakage of glue or thrombotic material occurred during or after the procedure. No haemorrhage, non-targeted glue embolization, stenosis or thrombosis, allergic reaction, infection, skin ischaemia or rupture of the pseudo-aneurysm (Glubran 2) occurred. All these were assessed with intraoperative echocolordoppler, postoperatively 1 day after the procedure and then at discharge after 7 days.
5. Conclusions
The results of the present investigation show that the application of Glubran 2 and AristaTMAH as surgical wound closure systems is effective and safe in achieving hemostasis of the affected site in patients undergoing surgical treatment. The success achieved was ≥94% on anastomoses of arteriovenous fistulas; 100% on stabilization of Picc catheters; ≤97% on pseudoaneurysms. This allowed us to appreciate the versatility of these devices as sealants in vascular surgery.
Author Contributions
All authors conceptualized and designed this study; F.C. writing—review and editing, R.C., S.T. and P.P. drafting and revision of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Department of Pharmacy and Health and Nutrition Sciences Department of Excellence L. 232/2016 and by PON R&I 2014-2020—ARS01_00568—SI.F.I.PA.CRO.DE.—Development and Industrialization of Innovative Drugs for Personalized Molecular Therapy PA.CRO.DE. .
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The patient provided informed consent for publication according to D.Lgs. 196/2003.
Data Availability Statement
Not Applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bao Z., Gao M., Sun Y., Nian R., Xian M. The recent progress of tissue adhesives in design strategies, adhesive mechanism and applications. Materials Science & Engineering C, (2020), 111 110796.
- Bal-Ozturk A., Cecen B., Avci-Adali M., Topkaya S.N., Alarcin E., Yasayan G., et al. Tissue adhesives: from research to clinical translation. Nano Today 2021;36:101049. [CrossRef]
- Trombino, S. , Sole R., Curcio F., Cassano R. Polymeric Based Hydrogel Membranes for Biomedical Applications. Membranes 2023, 13, 576. [Google Scholar] [CrossRef] [PubMed]
- Trombino, S. , Curcio F., Cassano R., Curcio M., Cirillo G., Iemma F. Polymeric Biomaterials for the Treatment of Cardiac Post-Infarction Injuries Pharmaceutics 2021, 13, 1038. [CrossRef]
- Cassano R., Curcio F., Sole R., Trombino S.. Hydrogel based on hyaluronic acid. Polysaccharide Hydrogels for Drug Delivery and Regenerative Medicine. Chapter 3, (2023), Pages 35-46.
- Serini S., Trombino S., Curcio F., Sole R., Cassano R. * and Calviello G. (Hyaluronic Acid-Mediated Phenolic Compound Nano-Delivery for Cancer Targeting. Pharmaceutics, (2023). 15.
- Cassano R., Perri P., Esposito A., Intrieri F., Sole R., Curcio F., Trombino S. Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports. Membranes (2023)13 (2), 240. [CrossRef]
- Sungmin Nam and David Mooney. Polymeric Tissue Adhesives. Chem. Rev. 2021, 121, 11336−11384.
- Dey A., Bhattacharya P.,Neogi S. Bioadhesives in Biomedical Applications: A Critical Review. In: Progress in Adhesion and Adhesives, Author: K.L. Mittal, Scrivener Publishing LLC ed. 2021, Volume 6, (131–154).
- Athavale A., Thao M., Sassaki V.S., Lewis M., Chandra V., Fukaya E. Cyanoacrylate glue reactions: A systematic review, cases, and proposed mechanisms. Journal of Vascular Surgery: Venous and Lymphatic Disorders, (2023)11, 4.
- Allotey J.K., King A.H., MS, Kumins N.H, Wong V.L.,. Harth K.C., Cho J.S., Kashyap V.S. Systematic review of hemostatic agents used in vascular surgery, Journal of Vascular 2021 73,6.
- https://www.gemitaly.it/prodotti/glubran-2/.
- Dhandapani V. Saseedharan P. Groleau D. Vermette P. Overview of approval procedures for bioadhesives in the United States of America and Canada., J Biomed Mater Res. 2022;110:950–966.
- Guillen, K.; Comby, P.-O.; Chevallier, O.; Salsac, A.-V.; Loffroy, R. In Vivo Experimental Endovascular Uses of Cyanoacrylate in Non-Modified Arteries: A Systematic Review. Biomedicines 2021, 9, 1282. [CrossRef]
- Zheng K., Gu Q. , Zhou D. , Zhou M. , Lei Zhang L. Recent progress in surgical adhesives for biomedical applications. Smart Materials in Medicine. 2022, 3, 41-65.
- Malik A., Ur Rehman F., Ullah Shah K., Naz S.S., Sara Qaisar S. Hemostatic strategies for uncontrolled bleeding: A comprehensive update.J Biomed Mater Res. 2021;109:1465–1477.
- CombyP., Guillen K., Chevallier O., Lenfant M., Pellegrinelli J. ,Falvo N., Midulla M., Loffroy R. Endovascular Use of Cyanoacrylate-Lipiodol Mixture for Peripheral Embolization: Properties, Techniques, Pitfalls, and Applications,J. Clin. Med. 2021, 10(19), 4320. [CrossRef]
- Asada Y., Yamashita A., Sato Y., Hatakeyama K. Pathophysiology of atherothrombosis: Mechanisms of thrombus formation on disrupted atherosclerotic plaques. Pathology International 2020, 70. [CrossRef]
- Brass L.F. , Tomaiuolo M., Welsh J.,Poventud-Fuentes I. , Zhu L. , L. Diamond S.L., Stalker T.J. Hemostatic Thrombus Formation in Flowing Blood. Platelets 2019, 371-391. [CrossRef]
- Krüger-Genge A., Blocki A., Franke R.P., Jung F. Vascular Endothelial Cell Biology: An Update. Int. J. Mol. Sci. 2019, 20(18), 4411. [CrossRef]
- Kang S., Kishimoto T. Interplay between interleukin-6 signaling and the vascular endothelium in cytokine storms. Experimental & Molecular Medicine (2021) 53:1116–1123.
- LIT-0057 Rev E Arista®AH Absorbable Hemostatic Particles Microporous Polysaccharide Hemosphere (MPH) Technology. Medafor, Inc.; 2.
- Biranje S.S., Sun J., Shi Y.,. Yu S., Jiao H., Zhang M., Wang Q., Wang J. Polysaccharide-based hemostats: recent developments, challenges, and future perspectives. Cellulose 202128(14):1-39.
- Miller K.J., Cao W., Ibrahim M.M., Levinson H. The effect of microporous polysaccharide hemospheres on wound healing and.
- scarring in wild-type and Db/Db mice. J Adv Skin Wound Care. 2017;30:170–180. [CrossRef]
- Balakrishnan B., Payanam U., Laurent A., Wassef M., Jayakrishna A. Efficacy evaluation of an in situ forming tissue adhesive hydrogel as sealant for lung and vascular injury. Biomedical Materials, 2021, 16, 4. [CrossRef]
- Capella-Monsonı´s H., Shridhar A., Chirravuri B., Figucia M., Learn G., Greenawalt K., Badylak S.F. A Comparative Study of the Resorption and Immune Response for Two Starch-Based Hemostat Powders. journal of surgical research. 2023 (282) 210 e224.
- Hadi, M.; Walker, C.; Desborough, M.; Basile, A.; Tsetis, D.; Hunt, B.; Müller-Hüllsbeck, S.; Rand, T.; van Delden, O.; Uberoi, R. CIRSE Standards of Practice on Peri-Operative Anticoagulation Management During Interventional Radiology Procedures. Cardiovasc. Interv. Radiol. 2021, 44, 523–536. [Google Scholar] [CrossRef]
- Prasad R., Israrahmed A., . Yadav R.R., Singh S., Behra M.R., Khuswaha R.S., Narayan PrasadN.,Lal H. Endovascular Embolization in Problematic Hemodialysis Arteriovenous Fistulas: A Nonsurgical Technique Indian.J Nephrol. 2021 31(6): 516–523.
- Bertagna G., Adami D., Del Corso S. Percutaneous glue embolization of arteriovenous fistula of in situ saphenous vein bypass graft: Case report and literature review. Vascular 2022, 30, 4, 759 – 763. [CrossRef]
- Zhang, Sheng; Lingle, Bethany S.; Phelps, Shannon A Revolutionary, Proven Solution to Vascular Access Concerns: A Review of the Advantageous Properties and Benefits of Catheter Securement Cyanoacrylate Adhesives.Journal of Infusion Nursing2022, 45, 3, 154-164(11). [CrossRef]
- Bergua-Lorente A., J Farrero-Mena J., Escolà-Nogués A., Llauradó-Mateu M., Serret-Nuevo C., Bellon F. Effectiveness of cyanoacrylate glue in the fixation of midline catheters and peripherally inserted central catheters in hospitalized adult patients: Randomised clinical trial. SAGE Open Medicine. 2023,11.
- Del Corso A.,Vergaro G. Percutaneous Treatment of Iatrogenic Pseudoaneurysms by Cyanoacrylate-Based Wall-Gluing, Cardiovasc Intervent Radiol (2013) 36:669–675. [CrossRef]
- HakanKar. Treatment of iatrogenic pseudoaneurysms. Turkish Journal of Vascular Surgery 2019;28(3):174-179.
- Ferrante G. , Rao S.V., Jüni P. , Da Costa B.R. , Reimers B. , Condorelli G. , Anzuini A. , S Jolly S.S. , Bertrand O.F., Krucoff M.W. , Windecker S. , Valgimigli M. Radial Versus Femoral Access for Coronary Interventions Across the Entire Spectrum of Patients With Coronary Artery Disease: A Meta-Analysis of Randomized Trials. JACC Cardiovasc Interv. 2016, 25;9(14):1419-34.
Figure 1.
Sealant application in vascular surgery

Figure 2.
Radial artery and cephalic vein identification and isolation

Figure 3.
Glubran 2 (A) and AristaTMAH (B) application to the anastomosis site at the arterial suture passage points.
Figure 3.
Glubran 2 (A) and AristaTMAH (B) application to the anastomosis site at the arterial suture passage points.
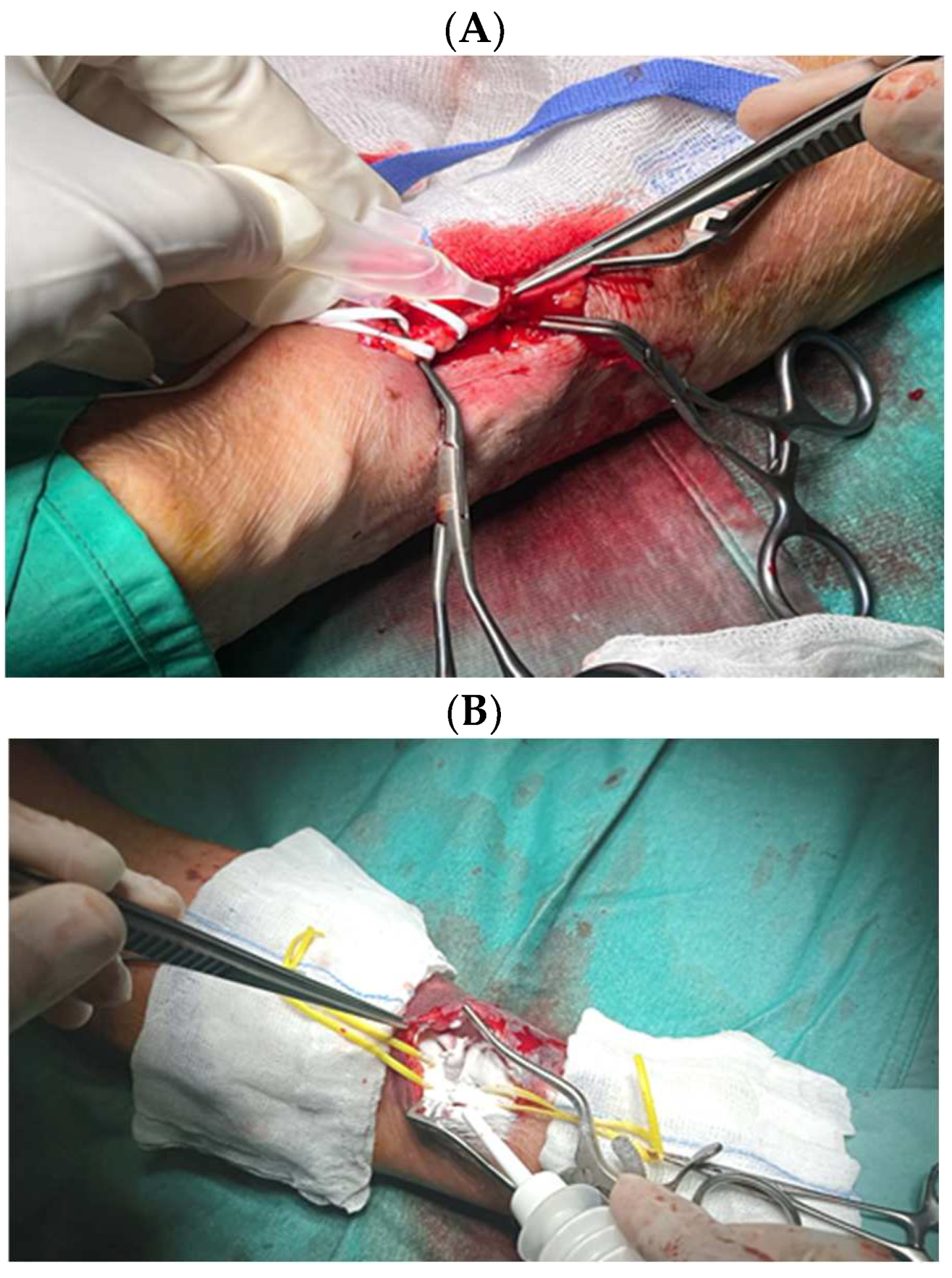
Figure 4.
Ultrasound identification of the endovascular access site for Picc stabilization.
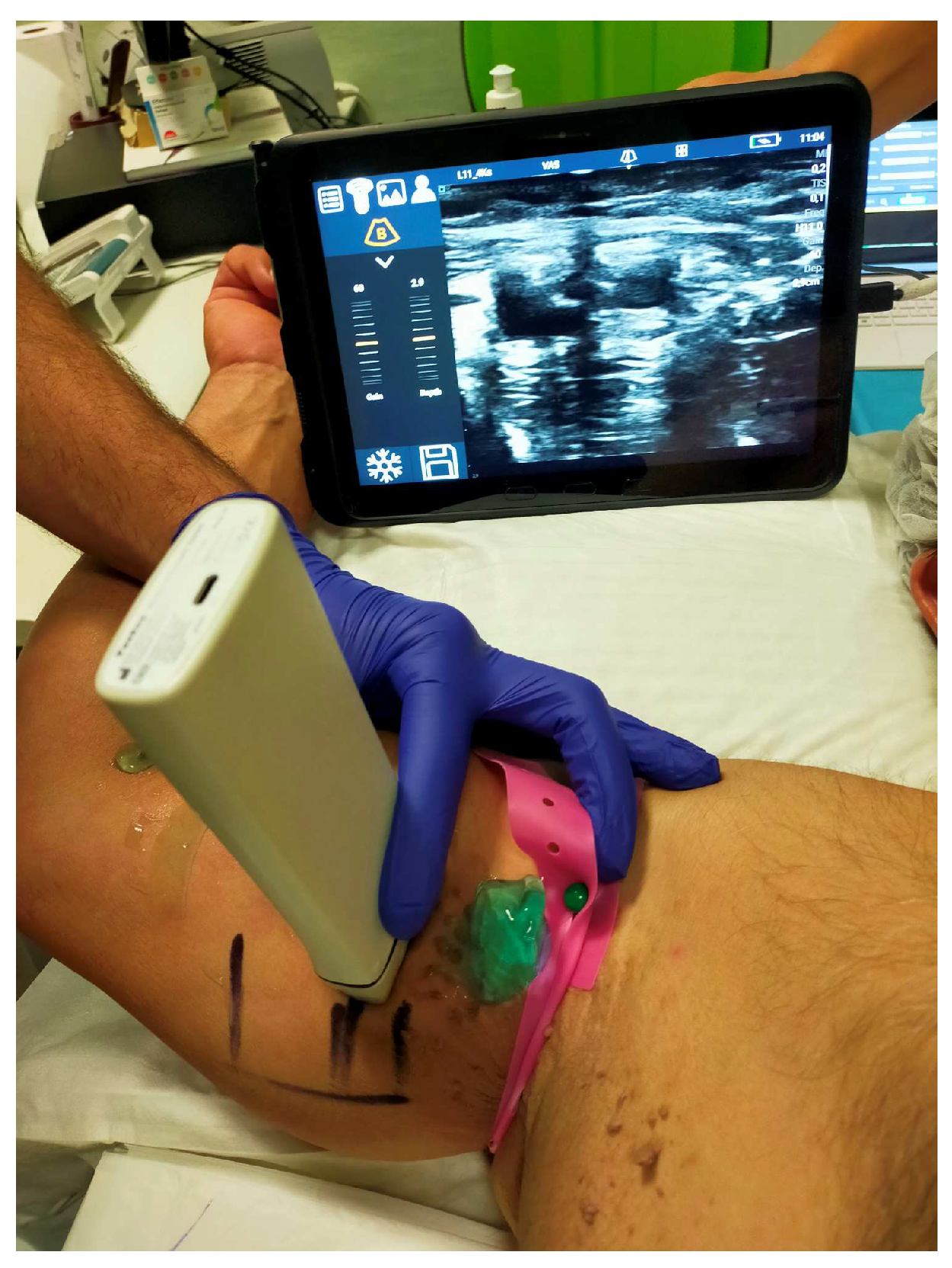
Figure 5.
Glubran 2 surgical glue application (a)and Picc catheter stabilization (b).
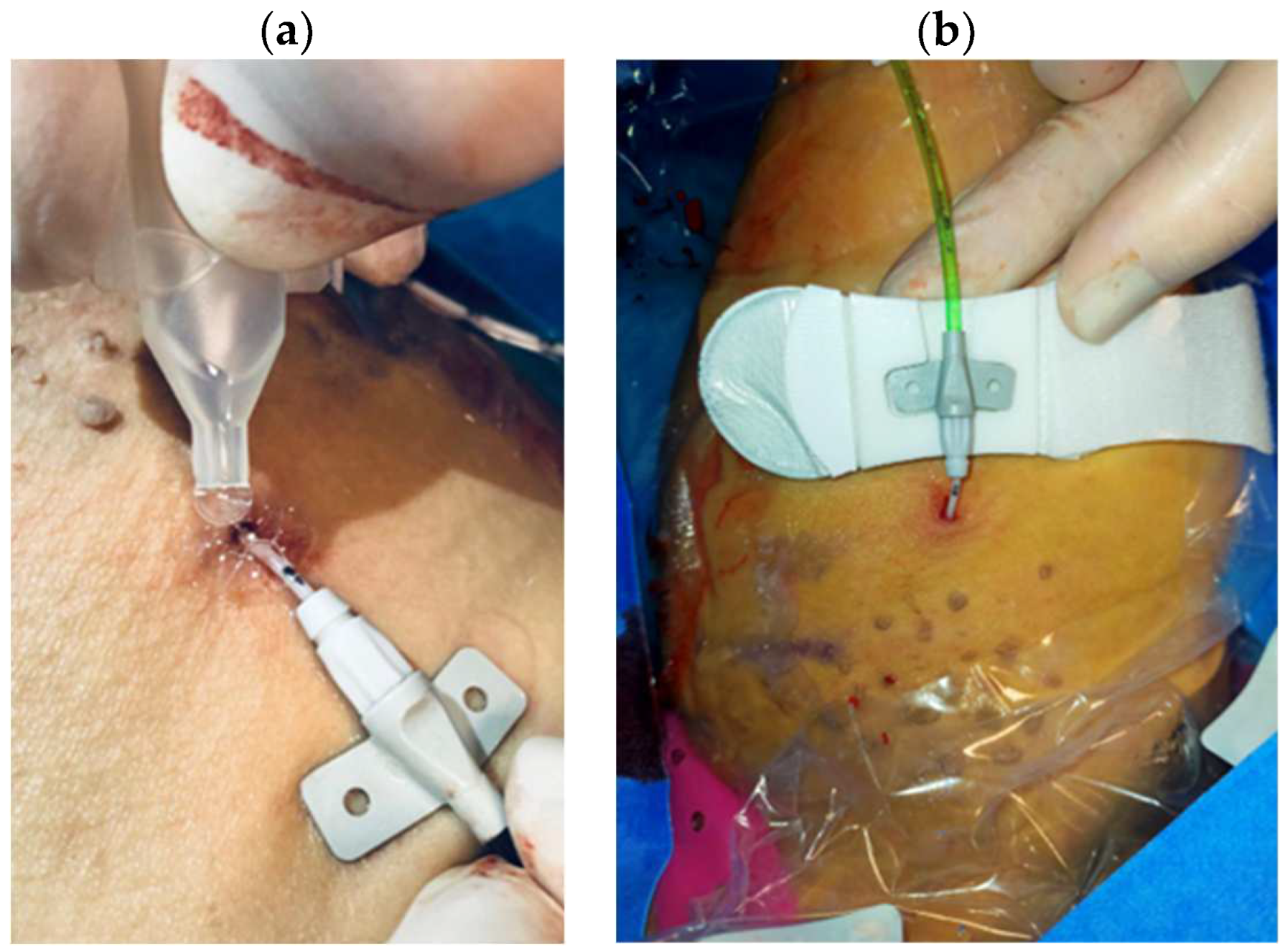
Figure 6.
Pseudoaneurysm identification.

Figure 7.
Pseudo-aneurysm isolation (a) and evacuation (b).
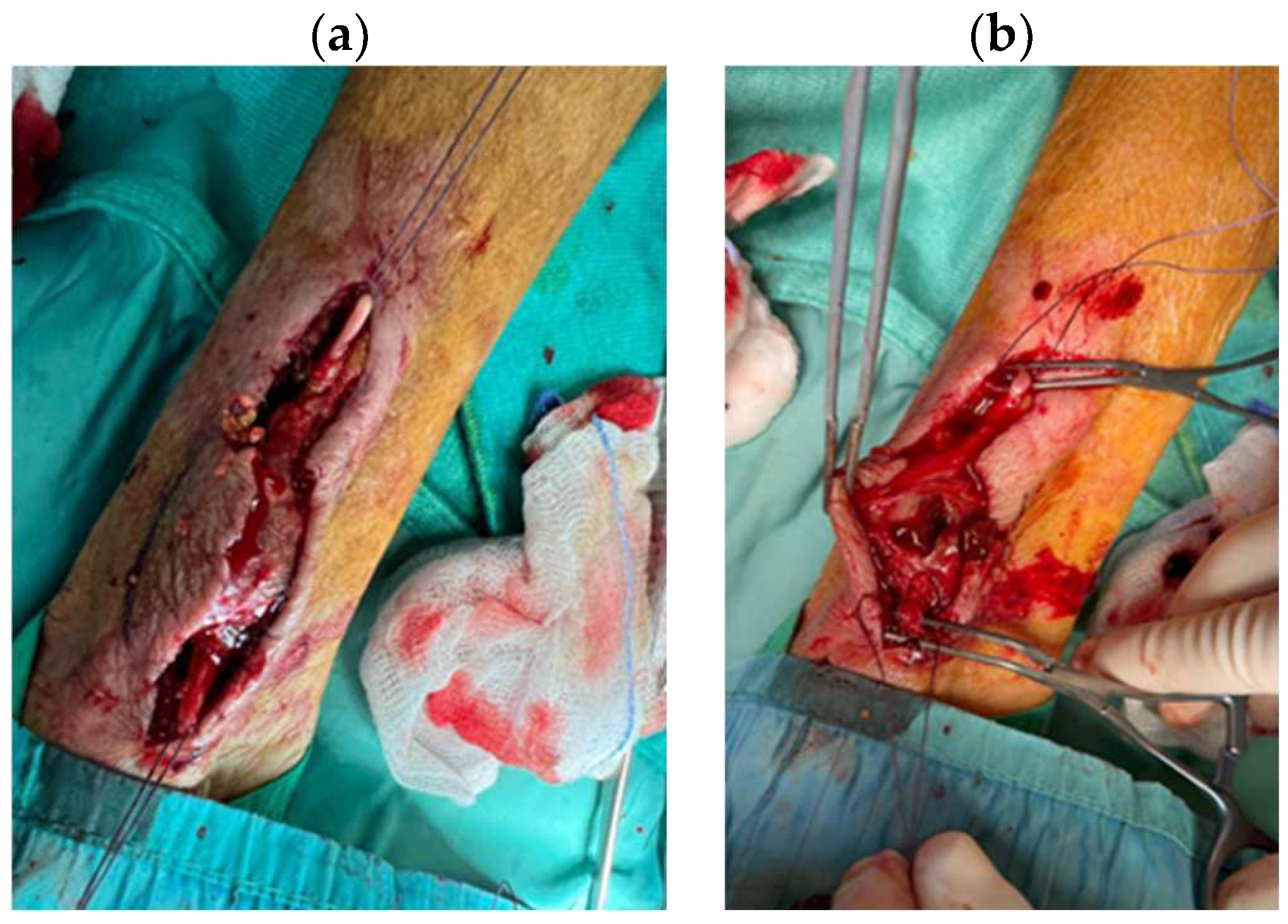
Figure 8.
Glubran 2 hemostatic adhesive application.

Figure 9.
Hemostasis evaluation at 2 min (A), 5 min (B), and 10 min (C) after AristaTMAH application.
Figure 9.
Hemostasis evaluation at 2 min (A), 5 min (B), and 10 min (C) after AristaTMAH application.
Scheme 1.
Retrospective study summary
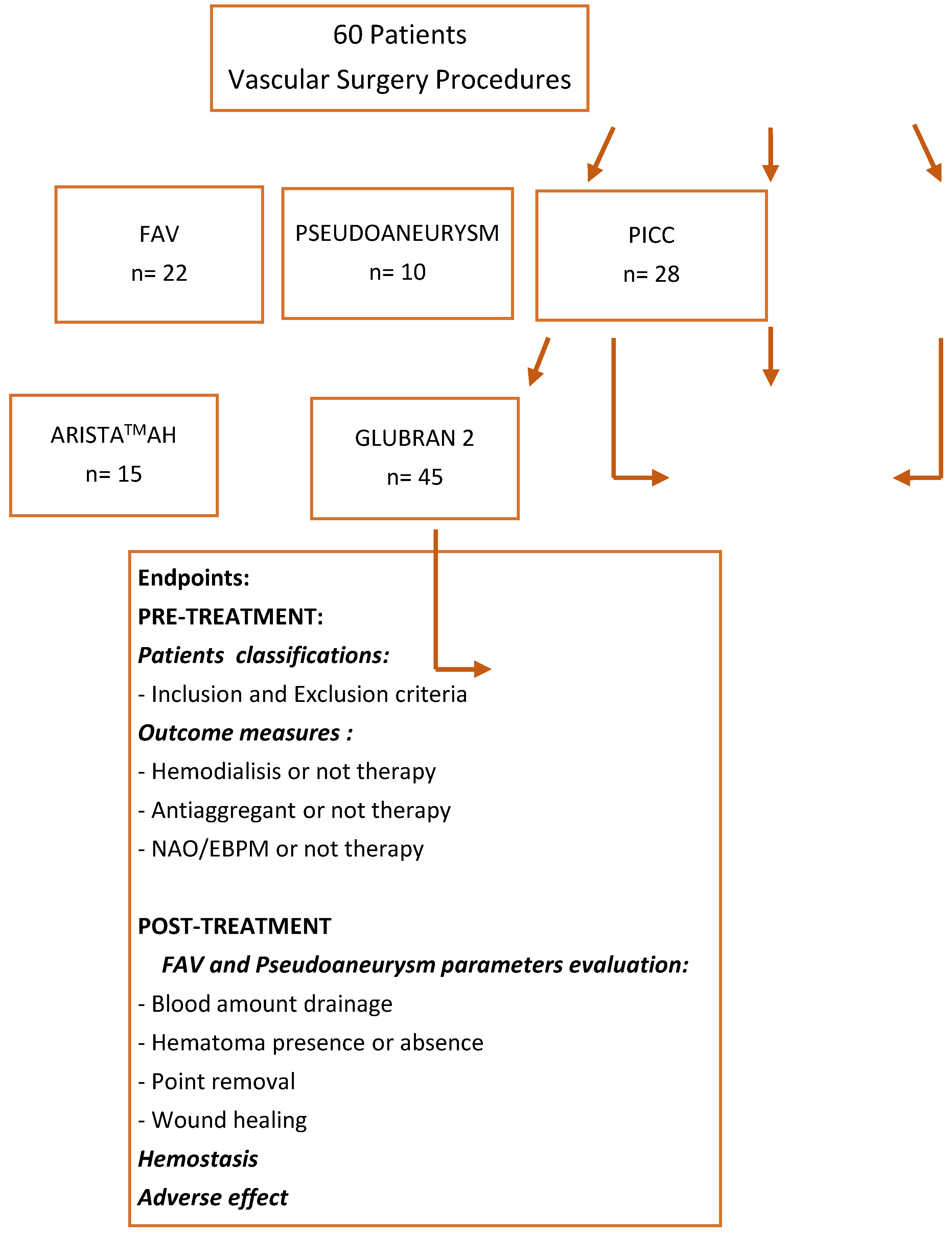
Table 1.
Population data.
| Variables |
Picc Patients (n=28) |
FAV Patients (n=22) |
PseudoaneuriysmPatients (n=10) |
|---|---|---|---|
| Ages (years) Sex (%M/%F) |
68 70 (F)/30 (M) |
71 68 (F)/ 32 (M) |
77 20 (F)/ 80 (M) |
| INR* | 0.92 | 1.18 | 1.06 |
| aPTT** (s) | 27 | 35 | 32 |
| Platelet count (x106/ml) | 260 | 340 | 290 |
| Hemoglobin (g/dL)) | 14 | 8 | 13 |
| Creatinine (mg/dl) | 0.9 | 4.9 | 1.3 |
| Anticoagulant therapy (%) | 7 | 25 | 20 |
| Antiplatelet therapy | (%) 18 | 65 | 50 |
| Haemodialysis therapy (%) | 0 | 50 | 20 |
* International Normalized Ratio** Activated partial thromboplastin time
Table 2.
Evaluation outcome and follow-up in patients with FAV.
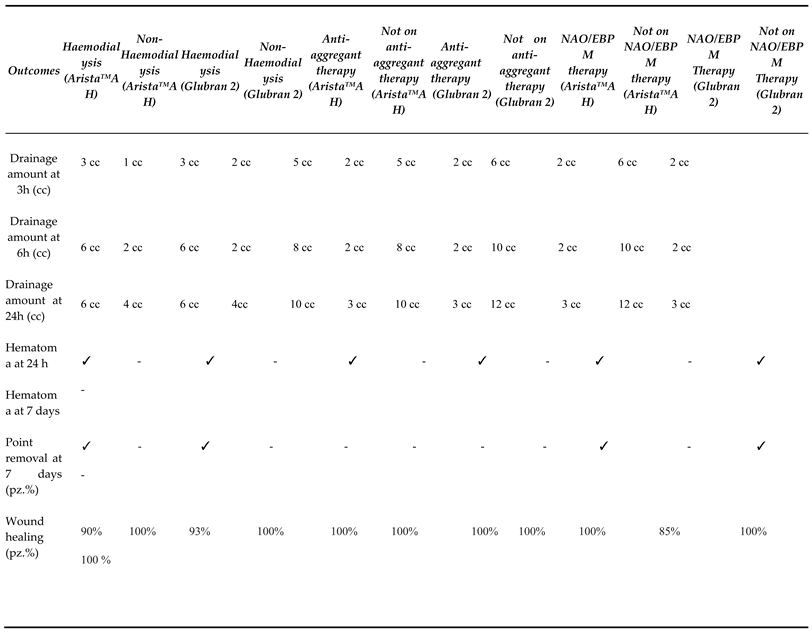 |
Table 3.
Evaluation outcome and follow-up patients with pseudoaneurysm.
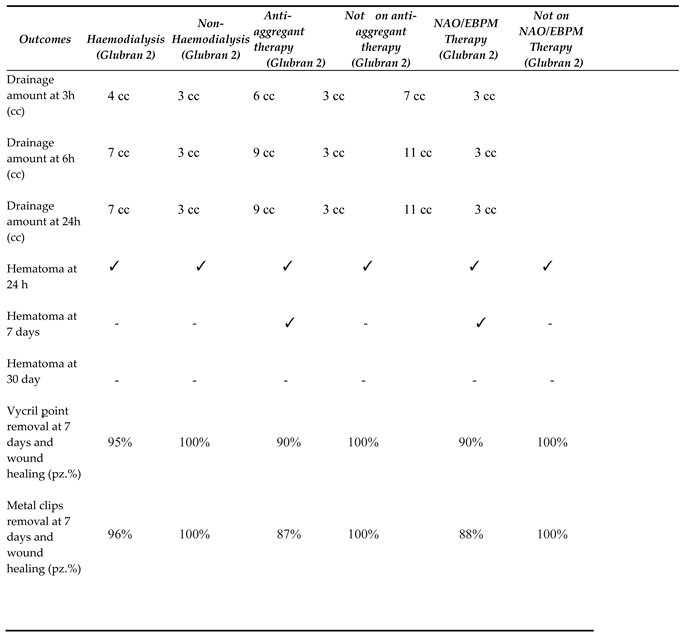 |
Table 5.
Comparison of data between Patients with Picc, pseudoaneurysm and FAV.
| Echocolordoppler control at 1 day | Echocolordoppler control at 3 day | Hematoma presence at 24 h | Hematoma presence at 7 day | Hematoma presence at 30 day | Wound healing Metal clips | Wound healing Vycryl | Collateral effect | Still alive | p-value | |
| Patients with Picc (n=28) | 0 0 | 0 | 0 | 0 | 0 | 0 | 0 | 28 | 2,77x10-7 | |
| Patients with pseudoaneurysm (n=10) | 0 0 | 10(100%) | 6(55%) | 0 | 8(88%) | 9(90%) | 0 | 10(100%) | 9,6x10-5 | |
| Patients with FAV (n=22) | 0 0 | 11(50%) | 7(10%) | 0 | 0 | 22(100%) | 0 | 22(100%) | 2,057x10-3 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



