
Submitted:
28 December 2023
Posted:
28 December 2023
You are already at the latest version
Abstract
Germline mutations in Breast cancer susceptibility gene 1 and 2 (BRCA1 and BRCA2) cause breast, ovarian and other cancers, and the chemotherapeutic drug doxorubicin (Dox) is widely used to treat these cancers. However, Dox use is limited by latent induction of severe cardiotoxicity known as Dox-induced cardiomyopathy, for which there are no specific treatments currently available. Dox is administered into the systemic circulation, where it readily translocates into sub-cellular compartments, and disrupts the integrity of DNA. Accumulating evidence indicates that oxidative stress, DNA damage, inflammation and apoptosis all play a central role in Dox-induced cardiomyopathy. The BRCA1 and BRCA2 proteins are distinct as they perform crucial yet separate roles in the homologous recombination repair of DNA double-strand breaks, thereby maintaining genomic integrity. Additionally, both BRCA1 and BRCA2 mitigate oxidative stress and apoptosis in both cardiomyocytes and endothelial cells. Accordingly, BRCA1 and BRCA2 are essential regulators of pathways that are central to the development of cardiomyopathy induced by Doxorubicin. Despite extensive investigations, there exists a gap in knowledge about the role of BRCA1 and BRCA2 in Doxorubicin-induced cardiomyopathy. Here, we review the previous findings and associations about the expected role and associated mechanisms of BRCA1 and 2 in Dox-induced cardiomyopathy and future perspectives.
Keywords:
BRCA2
; BRCA1
; doxorubicin
; breast cancer
; heart failure
Doxorubicin (Dox), an anthracycline antibiotic derived from Streptomyces peucetius var. caesius, is a potent geno- and cytotoxic medication used to treat various cancers. Dox is commonly prescribed with strict regime for, including but not limited to, breast, lung, and ovarian cancers [1]. Approximately 75% administered Dox circulate in blood via binding to plasma proteins [2]. Dox’s average terminal half-life is 20-48 hours [3,4]. Upon clearance, ~ 50% of the administered dose is eliminated from the body unchanged, with 5-12% appear in urine and 40% in bile within a week. Notably, men have higher Dox clearance compared to women, indicating higher vulnerability to Dox effects in women vs. men [5]. Dox is designed to target rapidly dividing cells, but the cytotoxicity induced by Dox is wide-scale, devastating virtually all cellular growth, survival, and proliferating processes. The drug's potent cytotoxic mechanisms are mainly summarized as two tiers: 1) DNA impairment and 2) Inducing oxidative stress. Accordingly, multiple novel mechanisms of these categories have recently emerged to substantiate Dox's potent toxicity in the recipients [6]. The genomic impacts of Dox are more specific to the drug's effects and encompass torsional stress, bombarding DNA strand breaks, and impairing replication, topoisomerase's activity, DNA repair and gene expression, ultimately inducing cell cycle arrest and apoptosis.
Although the oxidative impact is less specific to Dox's pharmacodynamic, Dox-induced oxidative stress is a common feature of the drug's cytotoxicity, featuring a notable excessive and devastating promotion of reactive oxygen species (ROS) and ROS-associated radicals, such as reactive nitrogen species (RNS), superoxide anions, hydrogen peroxide, etc. For instance, Dox-induced apoptosis results in the assembly of micronuclei, which are clusters of genomic fragments known to activate the cGAS-STING pathway that upregulates the inflammatory machinery and, thereby, ROS production [7]. In other cases, as elaborated later, Dox itself upregulates bioactivities of radicals. While the cells innately metabolize and neutralize radicals via antioxidant enzymes, such as catalase and superoxide dismutase, adverse phenotypes typically indicate that radical accumulation has overwhelmed the antioxidant's mechanisms. Typical sequala of Dox-induced oxidative stress include cellular injuries characterized by the destruction of cellular components at all biomolecular levels (e.g., membrane damage, lipid peroxidation, DNA damage, and oxidized protein aggregates) [8].
Notably, the body metabolizes Dox into doxorubicinol that can undergo spontaneous reduction to form doxorubicin-deoxyaglycone and then quinone-methide, which potently produce radicals from covalently binding to DNA. Moreover, Dox is also metabolized into doxorubicin-semiquinone radical by enzymes including cytochrome p450, xanthine oxidase, NADPH oxidases (NOX) and NO synthases (NOS) [7,8]. In addition to being a source of ROS, accumulating radicals can re-oxidize the semiquinone radicals back to doxorubicin, amplifying the drug's cytotoxicity [9].
In this notion, Dox’s cytotoxicity is non-specific, and the adverse clinical implications of Dox's molecular mechanisms remain a subject of intensive research. Indeed, Dox has been associated with increased risk of secondary malignancies, reproductive organs toxicity, and infertility. Most notable are complications in women, which includes amenorrhea, premature menopause, fetal harm in administered pregnant women, and birth defects such as prepubertal growth failure and gonadal impairment [6,10]. Among a conglomeration of reported adverse events, Dox-induced cardiotoxicity is the most concerning complication as it is relatively common and lead to cardiovascular dysfunction. For this reason, Dox is excluded for patients with poor heart function, and treatments are discontinued once the maximally tolerated cumulative dose is reached [8].
Dox Induced Cardiotoxicity
Dox-induced cardiotoxicity (DIC) is notably common in patients receiving Dox treatment and typically manifest as cardiomyocytes injuries subjected to the mechanisms of Dox that were meant for neoplastic cells. Clinically, DIC are either acute or chronic depending on the dosing regimen, age, and cardiovascular health of the patients. Recent incidence rate of acute DIC is ~30% and typically detected 2-3 days after DOX administration, with ~50% mortality after 1-year diagnosis. Acute DIC is reversible and often manifest with tachycardia, and ventricular premature beats shortly following administration. Histological features of acute DIC in the myocardium include interruption of myofibrils, cytoplasmic vacuolation and sparsity in cardiomyocytes [11]. The incidence of chronic DIC is ~2-20% and typically manifests as a complication of breaching Dox dosage tolerance after weeks or months of administration, featuring irreversible cardiomyopathy, prominent left ventricular enlargement, and heart failure [10,12,13]. The mechanisms of DIC are summarized in Figure 1.
Intercalation of DNA and Topoisomerase II inhibition:
It has been generally established that free radical-associated DNA damage is more likely to occur when Dox concentration breaches the tolerance dosage [14]. Instead, Dox-associated cytotoxic impact on the cell's genome is often attributed to DNA intercalation and Dox-dependent topoisomerase II inhibition [15,16]. Notably, considering the highly oxidative environment subjected to cardiac tissues by default, both mechanisms likely damage genomic integrity by a similar degree of significance in DIC.
The drug's potent mechanism is DNA intercalation, achieved via its anthraquinone ring. Dox inserts itself between DNA bases and stabilizes the interaction through hydrogen bonding, facilitated by its hydroxyl and daunosamine sugar's amino groups. Dox-DNA complexes induce torsional stress in the DNA's superhelical structures, leading to double-strand breaks and apoptosis. In addition, Dox can bind and inhibit DNA and RNA polymerases, disrupting replication, transcription, and DNA repair [16].
An additional Dox-associated cytotoxic impact on the cell's genome is topoisomerase II inhibition [15]. Topoisomerase II (TopoII) is a well-characterized enzyme that functions in replication (TopoIIa) or DNA repair and gene transcription (TopoIIb). Typically, it is recruited to associate with the DNA strand and induce coordinated DNA double-strand breaks as a response to alleviate torsional stress, relaxing positive supercoils, unlinking intertwined strands, in turn stabilizing the DNA's superhelical state. TopoII inhibition is also a Dox’s mechanism designed for rapidly proliferating cells. Dox binds and inhibits both TopoIIa and IIb during their actions, forming Dox-TopoII-DNA complexes that induce unaccounted-for double-strand breaks, hindering replication and gene expression, and resulting in cell death [15]. Indeed, Dox efficacy is dependent on TopoII concentration in the cells [2]. Dox-TopoII-DNA complexes can be reversed by the dissociation of Dox upon turnover, suggesting that Dox exposure duration is a key factor of Dox cytotoxicity [17].
The genomic impacts of Dox are typically observed at 0.01-5 μM Dox concentrations and followed by p53 upregulation [2]. p53 is constitutively expressed and preferably suppressed in cells. Its activation regulatory competes with various cell growth and DNA repair pathways; hindrance in the cell's growth/survival (e.g., downregulated E2F, the growth transcription factor) and/or improper DNA repair promote p53 activation [18,19]. Activated p53 facilitates cell cycle arrest and programmed cell death [20]. While Dox is designed to tarnish cellular replication and prompt p53's pro-apoptotic action in the neoplastic cell population, in DIC, Dox-treated cardiac tissues demonstrate impaired vital gene expression, DNA damages and dysregulated p53, among other complications [21,22]. In this notion, genetic and pharmacologic inhibition of p53 have been shown to attenuate acute DIC [23,24,25,26,27]; however, disrupted p53 activity has been associated with exacerbated cardiac dysfunction in animal models [22] and is also a feature of Dox-resistant tumor cells [28], suggesting a selectivity challenge for p53 targeting therapeutic strategies.
Moreover, in DIC, while cardiomyocytes are non-dividing cells, they preferentially express TopoIIb over TopoIIa. This expression is adopted by both the cardiomyocytes’ genomes and mitochondria. A single cardiomyocyte can have between 5,000 and 8,000 mitochondria, and mitochondria are vital for cardiac function, regulating essential lipid oxidation and redox balance [29]. Therefore, Dox’s inhibiting TopoIIb and the formation of Dox-TopoIIb-DNA complexes in cardiomyocytes promote DNA damages and oxidative stress as a feature of DIC.
NADPH Oxidases, Nitric Oxide Synthases, and Xanthine Oxidase:
DIC’s oxidative stress has been well characterized by three enzymes, NADPH oxidases (NOXs), nitric oxide synthases (NOSs), and xanthine oxidase (XOs), which were previously mentioned as metabolizer of Dox into semiquinone radicals. In addition to metabolizing Dox into radical intermediates, these enzymes pathologically contribute to oxidative stress by facilitating the production of oxidative radicals [30,31,32]. However, targeting these enzymes clinically remains under consideration due to conflicting observations attributed to their physiological oxidative significance. For instance, as XO mediates oxygen radical generation and exacerbates DIC in Dox-treated mice [33], febuxostat, an inhibitor of XO that reduces ROS production in the myocardium, has yet to be used clinically [34,35]. The NOXs enzymes are significant source of superoxide production, with NOX2 and NOX4 being the primary contributors to Dox-induced oxidative stress [36]; antioxidant treatments irisin and osteocrin inhibit NOX2 and NOX4, respectively, and result in the attenuation of DOX-induced oxidative stress in the heart [37,38]. However, NOXs’ inhibitors have yet to be considered clinically as their oxidative roles have physiological significance [39]; NOX2-deficient mice under high-fat diets developed severe glucose metabolism disorders, suggesting that the NOX enzymes maybe a sensitive target to modulate Dox cardiotoxicity [40].
Nitric oxide (NO) derived from NOS enzymes can interact with concurrent radicals to produce more radicals, such as peroxynitrite anion (ONOO-). Indeed, available antioxidant treatments for Dox-induced cardiotoxicity involves altering NOSs expression, such as levosimendan [41] and vitamin C [42]. Dox-treated cardiomyocytes show increased inducible NOS (iNOS) expression, and iNOS-deficient mice show attenuated DOX-induced generation of ONOO- [43]. However, studies have also shown that the lack of NO bioavailability exacerbates DOX-induced cardiotoxicity [44]. Notably, endothelial NOS (eNOS) catalyzes the biological synthesis of NO that is an essential regulator of endothelial function and vasotone [45]. Indeed, eNOS-deficient and -overexpressing mice showed reduced and increased susceptibility to Dox-induced oxidative stress, respectively [46]. On the other hand, Dox has been shown to impair eNOS activation while facilitating ROS-mediated oxidative stress [47]. Moreover, eNOS-deficient female mice were shown with aggravated DOX-induced oxidative stress and cellular damage [48].
Overall, it appears that by engaging in oxidation and Dox metabolism, NOX, NOS and XO may undesirably exacerbate Dox-induced oxidative stress. However, whether Dox induces the activities of these enzymes requires further investigation, and conflicting results have yet to point out a clear implication for modulating these enzymes as strategies to protect against DIC.
Antioxidants in Dox-induced Cardiotoxicity:
Relatively, cardiac tissues engage in an overall highly oxidative metabolic environment to sustain their essential systemic function. Approximately 70% of the energy in the heart are derived from the oxidation of fatty acids within the mitochondria and peroxisomes, which rely heavily on lipid-trafficking mechanisms [49]. Naturally, cardiomyocytes express sensitive levels of endogenous antioxidant enzymes (e.g., superoxide dismutase, glutathione peroxidase, glutathione S-transferase, heme oxygenase-1, catalase, etc.) [50]. Tipping the redox balance, as in antioxidant deficiency, easily renders cardiac tissues vulnerable to oxidative stress. Indeed, Dox impairs the antioxidants’ bioavailability in cardiomyocytes dependent on the duration and dosage of Dox exposure [51]. Conversely, increasing antioxidants’ activity enhances the cells’ redox capacity, obstructs free radical-related injury to DNA, and attenuates DIC [52,53]. However, adjusting antioxidants bioavailability remains a challenge in the clinical setting for DIC. For instance, apigenin, which enhances antioxidants in cardiomyocytes, has yet to be considered for clinical practice [54]. Nrf2, a transcription factor regulating antioxidant enzymes, is downregulated in DIC, such is rescued by the yet-to-be clinically implemented irisin, a benefit additional to the drug’s inhibition of NOX2 that mitigate oxidative DIC [55].
Peroxisomes in Dox-induced Cardiotoxicity:
Cellular peroxisomes are organelles that maintain redox and lipid homeostasis via fatty acids β-oxidation and detoxification of metabolic byproducts, such as hydrogen peroxide (H2O2), polyamines, glyoxylate, as well as several xenobiotics [56]. Notable peroxisomal enzymes include catalase and peroxidases, such as the peroxiredoxins, that process various oxidative radicals into water and oxygen, thereby maintaining oxidative balance. Dysfunctional peroxisomes, as in developing Niemann-Pick type C disease [57], lead to radical accumulation, oxidative stress, and downstream risk of multiple-organ failures. Indeed, aging cells, which become progressively peroxisomal inefficient, feature elevated ROS levels [58]. Conversely, overexpressing peroxiredoxin-1 attenuates oxidative stress and DIC in cardiomyocytes [59,60].
As oxidative stress and inflammation typically occur together, peroxisomal functions are closely linked to the inflammatory response. Likewise, chronic inflammation also features elevated ROS and oxidative cellular injuries. Moreover, peroxisomal enzymes also facilitate the degradation of pro-inflammatory mediators (e.g., prostaglandins, thromboxanes, leukotrienes, prostacyclins) and the biogenesis of anti-inflammatory metabolites (e.g., omega-3 fatty acids) [61]. Notably, omega-3 fatty acids are precursors of potent anti-inflammatory factors such as resolvins, maresins, and protectins [62]; enhancing the conversion of omega-3 fatty acids to these molecules is a feature non-steroidal anti-inflammatory drugs (NSAIDs), such as aspirin [63].
Mitigating DIC approaches from peroxisome functions have heavily focused on the peroxisome proliferator-activated receptors (PPARs). The PPARs are a family of nuclear transcription factors that, upon activation, upregulate peroxisome proliferators, which induce increase in cellular peroxisomes number, size and functions [64]. In humans, three closely related PPAR subtypes have been identified. PPAR-δ is expressed ubiquitously and at higher levels than the other two. PPAR-γ is mainly found in adipose tissues and, to a lesser extent, immune cells (monocytes, macrophages, etc.). PPAR-α is rich in hepatocytes, cardiomyocytes, skeletal muscles, and other peripheral tissues with active lipid oxidation. Notably, of the three, PPAR-α exert the highest affinity for lipids, regulating the escorts of unsaturated and saturated fatty acids via cytosolic fatty-acid binding proteins to the peroxisomes and mitochondria for lipids β-oxidation [65].
Dox inhibits PPARγ in adipose tissues of mice, leading to loss of storing of blood glucose and lipid, thereby causing hyperglycemia and hyperlipidemia, which are high risk factors for insulin resistance, atherogenesis, and cardiovascular diseases [66]. PPAR-α-null mice exhibit loss of fatty acid oxidative capacity, leading to increased lipid accumulation, reduced ketone bodies, and lack of gluconeogenesis and of metabolic switching to fatty acid usage in the heart during starvation. These culminate in cardiac dysfunction, myocardial damage and fibrosis [67]. The heart of tumor-bearing Dox-treated mice also showed inhibited PPARα but such is absent in their tumors; conversely, the same paper demonstrates that fenofibrate (FENO) treatment, an agonist of PPARα, and overexpression of PPARα in these mice enhanced cardiac function and salvaged DIC without affecting tumor progression [68]. Notably, FENO was shown to attenuate DIC in mice by improving endothelial function and upregulating eNOS expression and activation via Akt [69]. Outside of modulating the PPARs, there are little to no studies addressing the role of peroxisomes more directly for clinical applications against DIC [60].
Sirtuins Deacetylation in Dox-induced Cardiotoxicity:
The Sir2 and Sir2-like proteins, together referred to as sirtuins (SIRTs), are NAD-dependent deacetylase enzymes that make up the evolutionarily conserved class III histone-deacetylases in humans [70]. A distinct NAD/FAD-binding domain characterizes the class III HDACs. In humans, seven sirtuins have been reported and localized: nucleus (SIRT1, SIRT2, SIRT3, SIRT6, SIRT7), cytoplasm (SIRT1, SIRT2), and mitochondria (SIRT3, SIRT4, SIRT5) [70].
The SIRTs have been reported to regulate aging, metabolism, inflammation, apoptosis, and maintaining redox balance in cardiac cells [71]. SIRT1 has been linked to cardiovascular diseases [72]. SIRT3, 6 and 7 regulate ageing, apoptosis and oxidative stress in cardiomyocytes and are linked to cardiac hypertrophy [73,74,75]. The roles of SIRT4 and 5 in the heart remain under-investigated.
SIRT3 deacetylase is expressed abundantly in cardiomyocytes and plays a crucial role in regulating mitochondrial function, proliferation, and maintenance of mitochondrial genome, all of which are essential for cardiac metabolism. The mitochondria also engage in lipid oxidation similar to peroxisomes, regulating the redox balance. Notably, ~20% of mitochondrial proteins are regulated via reversible lysine acetylation [76], and the mitochondria contain high levels of NAD and NADH [77]. Mitochondrial acyl-CoA dehydrogenase and synthase facilitates long-chain fatty acid oxidation, and thereby lipid metabolism in cardiomyocytes [78]. SIRT3 regulates these enzymes and also those of the tricarboxylic acid cycle, electron transport chain subunits, and ATP synthase [79]. SIRT3 also regulates mitochondrial ROS formation, via the antioxidant SOD2 [80], and Ku70, a factor of the non-homologous end joining DNA repair pathway [81]. SIRT3 knock-down animals exhibit high risk for cardiac hypertrophy, oxidative stress, diminished cardiac ATP, and increased mitochondrial fragmentation [82,83,84]. Dox-treated cardiomyocytes exhibit mitochondrial dysfunction that contributes to oxidative stress and impaired lipid metabolism featured in DIC [85]. Resveratrol, which activates SIRT3, in co-treatment with Dox attenuates mitochondrial ROS production [86,87].
Cardiomyocytes adopt protein acetylation/deacetylation in metabolic regulation. Deacetylation of p53 prompts its ubiquitination and subsequent degradation, thereby promoting survival, and class III deacetylases also regulate several antioxidant enzymes. Dox significantly suppressed several SIRT deacetylases in the myocardium, abolishing antioxidants and exacerbating ROS production and apoptosis [88]. Upregulating the SIRT enzymes restores p53 ubiquitination, reduces caspase-3 activation, promotes Nrf2 and antioxidant enzymes, attenuates Dox-induced oxidative stress and salvages DIC [88,89,90]. Interestingly, endothelial cells also highly express the SIRT enzymes [91]. Overall, the SIRT enzymes regulate cardiomyocytes' metabolism, redox, and genomic integrity, all of which are aspects impaired in Dox-induced cardiotoxicity. Despite these findings, there remains a lack of SIRT activators developed for clinical therapy.
Dox Impairs Autophagy:
2-Hydroxypropyl-β-cyclodextrin (HPβCD), a proposed treatment for Niemann-Pick type C disease characterized by impaired lipid metabolism, is an activator of the transcription factor TFEB that upregulates autophagy [92]. Co-treatment of HPβCD in Dox-treated neurons, thereby activating autophagy, attenuates peroxisome-associated ROS accumulation, reducing neurotoxicity [93].
All cells continually engage in autophagy ("self-eating"), an essential process that encompasses encapsulation of the cell's own macromolecules and organelles in the cytoplasm, followed by the lysosomal digestion of these biowastes into metabolic materials (e.g., amino acids, nucleic acids, phospholipids, etc.) [94,95]. Biowastes of autophagy include mRNAs, turnover proteins, toxic misfolded aggregates, desensitized receptors, and dysfunctional organelles such as abnormally proliferated mitochondria and peroxisomes. Disruption of autophagy leads to accumulating cytotoxicity, resulting in dysfunction, and rapidly incapacitates metabolically stressed cells. As apoptosis is an energy-demanding process, this resulting cytotoxicity likely prompts necrosis and tissue inflammation, culminating in organ failures [96,97].
Autophagy is an emerging field in DIC research. Dox impairs autophagic flux at all stages. Dox inhibits various stress response factors that inhibit mTOR [98], thereby inhibiting autophagy. Dox-treated myocardium shows reduced numbers of autophagosomes and autolysosomes. On the other hand, Dox can also inhibit mTOR itself or modulate intermediate mediators, leading to excessive autophagosomes and autolysosomes, thereby dysregulating autophagy [87,99]. Dox-induced ROS accumulation also impairs lysosomal acidification and enzyme activity, resulting in the accumulation of autolysosomes [87]. Dysregulated autophagy, in turn, leads to mitochondrial dysfunction, impaired cellular metabolism, and apoptosis.
Dox induces Sarcoplasm Leakage:
Under Dox exposure, the myocardium exhibits cellular swelling, cytoplasmic vacuolation and myofibrils disruption, and other characteristics of cardiac dysfunction [100]. Most notable is the severe dilation of the sarcoplasm (SR), followed by Ca+2 leakage into the cytoplasm, upsetting the cells ion-tonicity, impairing contractility and potentiating ROS production [101]. In cardiomyocytes, Dox can increase CaMKII phosphorylation, which promotes the opening of RyR2 clusters on the SR, enabling Ca+2 leakage [102].
Dox-induced endotheliotoxicity (DIE):
The heart is a complex multicellular organ, comprising of cardiomyocytes - the main parenchymal cells behind cardiac pace-making and atrial/ventricular blood pumping, ECs (5% lymphatic, 95% vascular), vascular smooth muscle cells, fibroblasts, and pericytes. Cardiac ECs lining the endocardium and coronary vessels are known to establish regulatory cross-talk with the other cell type populations to regulate vasomotor tone, blood flow, and angiogenesis [103], thereby are subjected to high-energy oxidative metabolic environment, mitochondrial and peroxisomal redox regulation and lipid oxidation and influence cardiac function [104,105].
Virtually all cytotoxic aspects through which cardiomyocytes are subjected Dox’s cytotoxicity also apply for endothelial cells (ECs). Since the ratio of ECs to cardiomyocytes in cardiac tissues is ~1.5:1, ECs are about 1.5-fold more susceptible to Dox’s genomic and oxidative impacts than cardiomyocytes [106]. Therefore, a comprehensive understanding of the mechanisms that alter EC function leading to DIC is warranted.
Recent findings have linked Dox-induced endothelial dysfunction, or Dox-induced endotheliotoxicity (DIE), to susceptibility and severity of DIC. In this notion, both DIE and DIC may in fact contribute cumulatively to cardiovascular failure (Figure 2). Moreover, ECs are the first surface to interact with all circulatory entities, thereby the first to interact with Dox following systemic administration [107].
The Endothelium:
ECs comprise the endothelium, which is the simple squamous specialized epithelia that lines the inner luminal walls of blood vessels, such as those in the endocardium, coronary arteries and veins. The endothelium adopts systemic structural and functional heterogeneity, reflecting the various functions through which different organ systems interact with the circulatory system. Structurally, ECs can be continuous, fenestrated, and discontinuous, establishing the organ’s system unique permeability to blood (e.g., blood-brain barrier vs. spleen ECs) [108]. Other heterogenous structural features include ECs endocytic patterns (e.g., clathrin-based or caveolin-based) and junction types (e.g., tight junction, cadherin-based, gap-junction, etc.). Notably, hemodynamic stress and vasoactive agents (e.g., NO, ET-1, histamine, etc.) can modulate endothelial permeability via influencing ECs tight junctions. Functionally, ECs adopt extensive regulatory capacities that vary across organ systems and strictly determines vascular homeostasis. Endothelial functions oversee production of signaling agents that control or maintain vasotone (vasodilation vs. vasoconstriction) and vessel compliance, barrier/exchange permeability, blood fluidity, inflammation, wound healing, angiogenesis, and thrombosis [108].
Endothelial Dysfunction:
Physiologically, ECs maintains a non-thrombogenic and non-inflammatory blood–tissue interface with regulated selective permeability. ECs also maintain redox balance in their vasotone regulation through nitric oxide production. Upon stressful physical, chemical, or infectious stimuli (e.g., hemodynamic or oxidative stresses, advanced glycation end products, pathogens, metabolic insults, etc.), the injured ECs become activated toward a state of increased permeability and oxidative stress, pro-inflammation, thrombosis, and vasoconstriction—a reversible process referred to as endothelial activation [109]. Endothelial activation notably encompasses vasoconstriction, hemostasis, permeable blood-tissue barrier, and ECs secretion of inflammatory cytokines, growth and coagulative factors, upregulating inflammation, proliferation, angiogenesis, and thrombosis [110,111]. These processes, under prolonged or severe endothelial activation, can introduce irreversible injuries and progression toward endothelial dysfunction. Endothelial dysfunction, in addition to hypercholesterolemia, is the key mechanism behind atherosclerosis and cardiovascular diseases [112]. It is defined as the functional impairment of ECs in regulating vascular homeostasis and characterized by several aspects at the levels of activated ECs: impaired permeability (“leaky endothelium”); pro-inflammatory; proliferative; hypercoagulability; enhanced apoptosis and presences of free radicals and oxidative stress; dysregulated production and activities of vasoactive factors (e.g., NO, ET-1) and, thus, impaired vasotone [112].
Dox-induced Endothelial Dysfunction, Endotheliotoxicity, and Cardiotoxicity:
Recently, endothelial dysfunction has emerged as a novel mechanism contributing to DIC. As mentioned previously, ECs to cardiomyocytes amount ratio in the heart is ~1.5:1, suggesting higher vulnerability of cardiac ECs to Dox in various aspects compared to myocardiocytes. Moreover, Dox likely induce endothelial dysfunction as its cytotoxic mechanisms appear to impair crucial components of endothelial function (Figure 2).
ECs express both TopoIIa and IIb as they are proliferative in comparison to terminally differentiated non-proliferative cardiomyocytes, especially during stress-induced endothelial activation, wound healing, and angiogenesis [113]. Therefore, they are more vulnerable to Dox-inhibition of TopoII in addition to Dox-induced DNA intercalation and micronuclei generation. Cytoplasmic micronuclei signal the cGAS-STING pathway that promotes the pro-inflammatory and apoptotic IFN/TNFa signaling [63,114]. In addition, stressed and activated ECs also upregulate inflammation. Therefore, Dox-induced DNA damages in ECs can exacerbate inflammatory cardiac tissue injury. Indeed, the amount of micronuclei in ECs correlates directly with increasing Dox concentration and inversely with EC survival following Dox treatment [115]. Additionally, endothelial tight junction proteins such as zona occludens-1 (ZO-1) make the cardiac endothelium impermeable to prevent exposure of cardiomyocytes to harmful compounds. Dox inhibits ZO-1 expression in coronary ECs, leading to a leaky endothelium, increasing accesses of Dox to cardiomyocytes [107].
Dox inhibits and dysregulates the bioactivities of eNOS and endothelin-1, disrupting vascular tones and inducing RNS-mediated oxidative stress [116]. The restoration of cardiac NO levels preserve heart function in Dox-treated mice [117]. Dox also hinders the pro-growth factor neuregulin-1, which is expressed in ECs and cardiomyocytes and play crucial roles in cellular stress responses [118,119]. Likewise, ECs express and regulate NOS, eNOS, and XO, which are the sources of oxidative radical productions following Dox-treatment [120,121,122]. Additionally, PPARα, PPARβ/δ, and PPARγ expression have been found in ECs and are crucial in endothelial function, regulating cell proliferation, angiogenesis, inflammation, thrombosis, and coagulation [123]. As Dox is known to inhibit PPARy and PPARα, the drug, therefore, potently induces endothelial dysfunction; this notion, however, remains novel [47].
ECs express multiple SIRT family members that are also involved in endothelial function [124]. For instance, endothelial SIRT1 expression is positively associated with eNOS; overexpressing endothelial SIRT1 enhances vasorelaxation [72,125]. ECs’ SIRT1 also deacetylate and inhibit p53 [126]. Endothelial SIRT1 and 4 inhibit pro-inflammatory signaling of NF-κB, ICAM-1 and VCAM-1 [127,128]. Endothelial SIRT3-dependent antioxidant preserves mitochondrial function and endothelial redox balance [129]. Notably, downregulated endothelial SIRT1 is associated with oxidative stress, inflammation, and hypertension [130]. Moreover, loss of endothelial SIRT1 leads to MMP-14 downregulation, which normally inhibit the collagen-crosslinking enzyme transglutaminase-2 [131], suggesting that Dox-inhibition of SIRT1 in ECs and cardiomyocytes may give rise to cardiac fibrosis.
Autophagy in ECs strictly determines endothelial function for their metabolic implication. Indeed, loss of autophagy induces endothelial dysfunction; interestingly, aging-associated loss of autophagy closely correlate with loss of eNOS regulation and endothelial function [94]. As Dox impairs autophagy in various stages in cardiomyocytes, ECs likely incur similar damages, suggesting that Dox may also induce endothelial dysfunction through impairing endothelial autophagy. However, this research remains novel. A recent finding by Graziani 2022, demonstrated autophagy upregulation in ECs upon Dox treatment, indicated by increased LC3II-LC3I ratio even under the autophagy inhibitor chloroquine [132]; while they did not measure Dox’s effects on crucial ATG proteins and p62, which would indicate whether complete and functional autophagy occurred, Dox was shown to induce the aberrant inhibition of mTOR, thereby sustaining autophagy, and the suppression of VEGFR2, which are receptors for VEGFa, an essential endothelial function regulator that also regulates autophagy [133]. Ultimately, Graziani 2022 reinforces that Dox induces endothelial dysfunction and impair endothelial autophagy. Additionally, another recently published article shows that endothelial cell-specific loss of autophagy exacerbates Dox-induced cardiac dysfunction in mice [134]; suggesting an essential role of endothelial autophagy in DIC.
Overall, Dox-induced endothelial dysfunction appears to be a crucial factor in developing DIC, and ECs functional alterations, as under Dox treatment, can have significant implications for cardiac health. Therefore, a better understanding of the mechanisms underlying the susceptibility of ECs to Dox-induced endotheliotoxicity is essential for treating DIC in cancer patients undergoing chemotherapy with Dox. The mechanism of Dox-induced endotheliotoxicity is summarised in Figure 2.
Breast Cancer Gene 1 & 2:
Breast cancer is the most common cancer among Canadian women, and by 2020, it is the most common cancer globally [135]. Breast cancers are largely sporadic, with tumorigenesis often attributable to combined effects of genetic and environmental factors. On the other hand, 5-10% of breast cancers are familial that are often due to mutations in the BReast-CAncer (BRCA) genes, i.e., BRCA1 and/or BRCA2 genes. The BRCA mutations carriers are predisposed to known increased lifetime risks for mainly breast and ovarian cancer, along with various other cancers such as prostrate or colorectal cancer [136]. Identifying BRCA mutations forms the diagnosing basis of the hereditary breast and ovarian cancer (HBOC) syndrome [137], and the genes’ association to cancer development risk have prompted intensive investigation into the roles of BRCA1 and 2 in cancer and health.
BRCA1 and BRCA2 are tumor suppressor genes encoding for two critical and non-redundant mediators of the homologous recombination DNA damage repair pathway [138]. BRCA1 and BRCA2 are completely distinct genes as BRCA1 is located on chromosome 17q21, contains 24 exons and spans 100 kilobases, while BRCA2 is on chromosome 13q12.3 with 27 exons spanning ~ 70 kilobases. BRCA1 (220 kDa) and BRCA2 (384 kDa) proteins are also completely distinct in structures and functions; they have different direct and indirect protein partners and, thereby, engaging in unique roles in the DNA Damage Response (DDR) pathway [138]. Cells are constantly exposed to DNA damage due to exogenous (e.g., radiation) and endogenous (e.g., metabolite byproduct such as ROS) stressors that, if unaccounted for, would otherwise rapidly compromise their genomic integrity and stability. Genomic impairments are known to underlie cancer, neurodegenerative diseases, premature aging, autoimmune disorders, and cardiovascular diseases [139,140]. In sustaining constant and rapidly arising DNA damage, most cells conduct the DDR pathway, a complex and dynamically fine-tuned error-free signaling package of DNA repair pathways [141,142].
Among the various types of DNA damages, double-strand breaks (DSBs) are the most harmful and require the most energy to repair; several factors regulating DSB repairs also regulate the cell-cycle and apoptosis [143]. In DSB repair, DDR's sensors- ATM and ATR kinases- detect the lesion, promote the phosphorylation of local histone H2AX, and induce a unique chromatin modification that recruits and activates MDC1, which then recruits the initiators of DSB repairs. In addition, activated ATM and ATR interact with the CHK proteins to stabilize p53, which upregulates cell cycle inhibitors and checkpoint activators. If DSBs are not repaired, p53's continuous activity will eventually upregulate the molecular trigger of apoptosis- BAX, BAM, and PUMA (28). The DDR package devote two separate repair mechanisms for DSBs. Non-homologous end joining (NHEJ) and Homologous Recombination (HR).
Non-homologous end joining (NHEJ) does not use a homologous chromosomal copy, and therefore, cannot recover the genetic information lost to DSBs; therefore, it is an error-prone method for DNA repair. However, NHEJ is a more immediate response that operates throughout all cell cycle phases, aiming to quickly resolve DSBs and preventing apoptosis or genotypic aberrations due to deletion. The initiator of NHEJ is 53BP1, which mediates the binding of the Ku70-Ku80 heterodimer (Ku) to the DSB lesion, followed by stabilizing the broken ends, alignment by DNA-PK, and ligation by DNA ligase IV-XRCC4-XLF-PAXX complex. Notably, Ku70 is regulated by SIRT3 deacetylation, which is impaired by Dox treatment [144]. Moreover, DNA-PK facilitates p53's upregulation should NHEJ fail in its goal [145,146,147,148,149].
Homologous Recombination (HR) is restricted to late S or G2 phases, requiring an available completely replicated ‘homologous’ sister chromatid. Compared to NHEJ, it is more sophisticated, time- and energy-consuming. The initiator of HR repair is BRCA1 (Figure 3). Upon activation by the DSB detection complex, BRCA1 mediates the binding of the MRN complex to broken ends. The MRN complex then produces the unique 5′ to 3’ resection and 3’-overhangs; these formations also replace any binding Ku proteins with RPA heterotrimers, inhibiting NHEJ. Indeed, BRCA1 is also known to antagonize 53BP1 [150], and BRCA1’s bioavailability relative to 53BP1 determines whether NHEJ or HR is executed to repair DSBs [151]. Next, PALB2, with the help of BRC1, mediates BRCA2’s disassembling of RAD51 heptamers and loading their monomers onto the 3’-end overhangs and the resected regions, replacing the RPAs. BRCA2 then 1) guide the invasion of the RAD51-single strand formation to the correct copied regions on the homologous sister chromatid, and 2) mediates the homologous template-dependent strand extension to re-synthesize the lost base-pairs (Figure 3). Similar to NHEJ’s DNA-PK, BRCA1 also regulate p53 in dictating apoptosis based on the result of repair [152,153,154].
Moreover, BRCA1 also complexes with several factors to regulate the activation of cell cycle checkpoints. In the G1/S-checkpoint, activated ATM phosphorylates BRCA1, which requires complexing with BARD1 to facilitate the stabilization of p53, in turn inducing p21, a cell cycle inhibitor. During S-phase, BRCA1 also interacts with TopoII via the BRCA1–BRIP1–DNA topoisomerase 2-binding protein 1 (TOPBP1) complex to regulate replication. The G2/M checkpoint requires BRCA1 complexing with RAP80, Abraxas, and BARD1 [155].
The broader range of functions of BRCA1 implies that it is the more critical counterpart, albeit it is an entirely distinct protein relative to BRCA2 [138], and they only overlap in HR repairs. Accordingly, more severe genomic instability is found in tumors associated with defective BRCA1 than in those with faulty BRCA2 [156], which may explain the higher lifetime risks for developing cancers (breast and ovarian cancers) in women carrying BRCA1 mutations. Interestingly, while this is the case in women, recent patient studies suggest that in men, higher cancer risk (breast, pancreas and prostate cancers) is associated with BRCA2 mutation carriers instead, although the phenotypical connection BRCA2’s function remains to be investigated [157,158]. Considering the current state of what is known about BRCA2 vs. BRCA1, and that BRCA2 is essential for proper HR repair and, thereby, the cells’ cycle and genomic integrity, this excitingly suggests that there is still a vacuum of BRCA2’ important mechanisms to be unearthed.
Breast Cancer Gene, Doxorubicin and Cardiovascular Implications and Prospects:
Considering the essential roles of BRCA1 and BRCA2 in determining cellular survival and genomic integrity and the wide-scale detrimental cytotoxic mechanisms of Dox, there remains a critical lack of investigation into the effects of BRCA1 and BRCA2 functions on Dox-induced cytotoxicity and DIC.
Moreover, current diagnosing approach for identifying BRCA mutations lacks consideration for haplo-insufficiency in either BRCA genes, whereby the BRCA-haplo-insufficient individuals carry a malfunctional BRCA-related phenotypes. This has led to a considerable oversight in clinical examination for the implications related to impaired BRCA functions. For instance, as Dox’s genomic impacts encompass DNA intercalation and TopoII inhibition, thereby impairing replication, gene expression and DNA repair, it is still currently not known how Dox affects the BRCA’s related pathways. Moreover, the SIRT proteins are Class III deacetylases and, therefore, important regulators of epigenetics and histone modifications. While Dox is known to inhibit SIRT3 and indirectly impair the Ku proteins, thereby NHEJ, still little is known about Dox affecting any of the factors related to HR repair other than suppressing DNA synthesis.
In addition, as HBOC diagnosis is directed toward examining risk of cancers in BRCA mutation carriers, the current clinical approach on BRCA mutations largely overlook non-neoplastic implications of haploinsufficiency in BRCA gene. Notably, BRCA haploinsufficiency can be caused by multiple factors (transcription factors, genetic modifiers, hormonal regulation, SNPs in promoter/5’UTR) independent of BRCA mutations. This is reinforced by the fact that the estimated general population prevalence of high cancer risk BRCA1/2 mutations is 1 in 400 [159], and HBOC only accounts for ~6 in 100 cases of breast and ovarian cancers [160]. In other words, not all BRCA1/2 mutation carriers will develop cancer, and most breast and ovarian cancers are not due to HBOC. Therefore, the clinical prospect of compromised BRCA genes in an individual’s health and pathophysiology remains vague outside the focus of cancer, especially in assessing non-specific Dox’s cytotoxicity.
Interestingly, a single clinical retrospective study in 2009 found a noticeably higher risk of mortality associated with carriers of BRCA mutation in the absence of cancers [161]. This notion is further elaborated by the fact that the roles of BRCA are commonly studied in the context of a general non-specific eukaryotic cell. The latest update on BRCA expression pattern from The Human Protein Atlas indicates a global expression trend in the human body; a majority of organ systems express BRCA1 and 2 [162]. Likewise, 58% of deaths in breast cancer patients are due to complications related to organ dysfunction; leading causes include pulmonic insufficiency, infection, and hepatic insufficiency [163]. Notably, cancer patients have recently been characterized by higher cardiovascular risk [164].
BRCA1 and 2 maintain genomic integrity, regulate cell cycle, metabolism and function, while Dox targets and impair all the same aspects. This is summarised in Figure 4 and suggests that the mechanisms of Dox may conflict with the essential pathways regulate by BRCA1 and 2. Yet despite intensive research have reveal a vast multitude of cellular functions impaired by Dox, particularly in the heart, there remains a critical lack of investigation on Dox’s functional connection to BRCA1 and BRCA2.
Nevertheless, recent research has begun to demonstrate the essential roles of BRCA genes in endothelial and cardiac function. For instance, markedly greater cardiac dysfunction has been observed in left ventricular sections of Dox-treated cardiomyocyte-specific BRCA2 knock-out mice compared to vehicle-treated controls. Cardiac samples from these Dox-treated mice also exhibit enhanced apoptosis, elevated phosphorylated histone H2Ax (DSB markers), increased expression and activities of p53, PUMA, and Bax, which are pro-apoptotic proteins, and increased cytochrome C release, a marker of mitochondrial dysfunction and apoptosis. Notably, the samples also show reduced RAD51 formation, suggesting that Dox impacts BRCA2’s related DNA repair pathway [165].
In vivo, overexpressing BRCA1 in ECs protects against Dox-induced inflammation in association with reduced ROS levels, upregulated eNOS and VEGFa in vitro [166]. On the other hand, silencing endothelial BRCA1 aggravates inflammation under Dox treatment. From the same study, EC-specific BRCA1-overexpressing ApoE-null mice subjected to hind-limb ischemia, a model of endothelial activation, exhibit improved capillary density and better vascular recovery compared to controls. Under Western diets, modeling atherogenesis, BRCA1-overexpressing mice show less aortic plaque lesions, reduced macrophage infiltration and less oxidative stress vs. controls. In contrast, BRCA1-null mice demonstrated greater inflammation, apoptosis and impaired endothelial function in lung and aortic sections. Lastly, the study also observed suppressed BRCA1 expression in the plaque region of human atherosclerotic carotid artery samples compared with the adjacent plaque-free area [166]. Similarly, endothelial cell-specific loss of BRCA2 exacerbated oxidative stress-induced DNA damage, apoptosis and endothelial dysfunction [109].
Final remarks
In conclusion, doxorubicin is a cytotoxic cancer medication with devastating cardiotoxicity side effects that have been well characterized for two modes: genomic impairment and oxidative stress. The molecular mechanisms of Dox remain a subject of intensive research, with novel mechanisms being discovered that fortify the drug’s potency as well as its roles in DIC. In addition to impairing cardiomyocytes' genomic integrity, redox balance, autophagy and metabolism, recent research on Dox’s impacts in the endothelia of cardiac tissues have suggested the critical roles of endotheliotoxicity in DIC. Moreover, the impact of Dox on the functions of BRCA1 and BRCA2 remains largely unexplored. The current diagnostic approach for identifying BRCA mutations lacks consideration for haploinsufficiency, leading to compulsory oversights on the clinical implications related to impaired BRCA functions. Recent studies have shown the essential roles of BRCA genes in endothelial and cardiac function, and the dysregulation of these genes lead to cardiovascular and non-neoplastic implications. Accordingly, there are conflicting reports about the role of BRCA in an increased risk for cardiovascular diseases, most importantly regarding DIC [167,168] . Given the noticeable overlap in the mechanisms governing the loss-of BRCA-associated phenotype and DIC further investigation into the functional connections between Dox and BRCA1/2 is warranted to better understand the mechanisms of Dox-induced cardiotoxicity and endotheliotoxicity in order to promote personalized therapy to in BRCA-mutant cancer patients.
Funding
This research was funded by Heart and Stroke Foundation, grant number G-22-0032104.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sritharan, S.; Sivalingam, N. A Comprehensive Review on Time-Tested Anticancer Drug Doxorubicin. Life Sci 2021, 278, 119527. [Google Scholar] [CrossRef]
- Nicoletto, R.E.; Ofner, C.M. Cytotoxic Mechanisms of Doxorubicin at Clinically Relevant Concentrations in Breast Cancer Cells. Cancer Chemother Pharmacol 2022, 89, 285–311. [Google Scholar] [CrossRef]
- Gustafson, D.L.; Rastatter, J.C.; Colombo, T.; Long, M.E. Doxorubicin Pharmacokinetics: Macromolecule Binding, Metabolism, and Excretion in the Context of a Physiologic Model. J Pharm Sci 2002, 91, 1488–1501. [Google Scholar] [CrossRef]
- Speth, P.A.; van Hoesel, Q.G.; Haanen, C. Clinical Pharmacokinetics of Doxorubicin. Clin Pharmacokinet 1988, 15, 15–31. [Google Scholar] [CrossRef]
- Dobbs, N.A.; Twelves, C.J.; Gillies, H.; James, C.A.; Harper, P.G.; Rubens, R.D. Gender Affects Doxorubicin Pharmacokinetics in Patients with Normal Liver Biochemistry. Cancer Chemother. Pharmacol. 1995, 36, 473–476. [Google Scholar] [CrossRef]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An Update on Anticancer Molecular Action, Toxicity and Novel Drug Delivery Systems. Journal of Pharmacy and Pharmacology 2013, 65, 157–170. [Google Scholar] [CrossRef]
- Thorn, C.F.; Oshiro, C.; Marsh, S.; Hernandez-Boussard, T.; McLeod, H.; Klein, T.E.; Altman, R.B. Doxorubicin Pathways: Pharmacodynamics and Adverse Effects. Pharmacogenet Genomics 2011, 21, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.-Y.; Guo, Z.; Song, P.; Zhang, X.; Yuan, Y.-P.; Teng, T.; Yan, L.; Tang, Q.-Z. Underlying the Mechanisms of Doxorubicin-Induced Acute Cardiotoxicity: Oxidative Stress and Cell Death. Int J Biol Sci 2022, 18, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Minotti, G.; Recalcati, S.; Mordente, A.; Liberi, G.; Calafiore, A.M.; Mancuso, C.; Preziosi, P.; Cairo, G. The Secondary Alcohol Metabolite of Doxorubicin Irreversibly Inactivates Aconitase/Iron Regulatory Protein-1 in Cytosolic Fractions from Human Myocardium. FASEB J 1998, 12, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Sheibani, M.; Azizi, Y.; Shayan, M.; Nezamoleslami, S.; Eslami, F.; Farjoo, M.H.; Dehpour, A.R. Doxorubicin-Induced Cardiotoxicity: An Overview on Pre-Clinical Therapeutic Approaches. Cardiovasc Toxicol 2022, 22, 292–310. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Khedr, M.M.; Morsy, M.H.; Badae, N.M.; Elatrebi, S. A Comparative Study of the Cardioprotective Effect of Metformin, Sitagliptin and Dapagliflozin on Isoprenaline Induced Myocardial Infarction in Non-Diabetic Rats. Bulletin of the National Research Centre 2022, 46, 123. [Google Scholar] [CrossRef]
- Aloss, K.; Hamar, P. Recent Preclinical and Clinical Progress in Liposomal Doxorubicin. Pharmaceutics 2023, 15, 893. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, C.W.; Turissini, C.; Asnani, A. Doxorubicin Cardiotoxicity: Pathophysiology Updates. Curr Treat Options Cardio Med 2020, 22, 52. [Google Scholar] [CrossRef]
- Carvalho, C.; Santos, R.X.; Cardoso, S.; Correia, S.; Oliveira, P.J.; Santos, M.S.; Moreira, P.I. Doxorubicin: The Good, the Bad and the Ugly Effect. Curr Med Chem 2009, 16, 3267–3285. [Google Scholar] [CrossRef]
- Zhu, H.; Sarkar, S.; Scott, L.; Danelisen, I.; Trush, M.A.; Jia, Z.; Li, Y.R. Doxorubicin Redox Biology: Redox Cycling, Topoisomerase Inhibition, and Oxidative Stress. React Oxyg Species (Apex) 2016, 1, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Agudelo, D.; Bourassa, P.; Bérubé, G.; Tajmir-Riahi, H.-A. Intercalation of Antitumor Drug Doxorubicin and Its Analogue by DNA Duplex: Structural Features and Biological Implications. International Journal of Biological Macromolecules 2014, 66, 144–150. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, X.; Bawa-Khalfe, T.; Lu, L.-S.; Lyu, Y.L.; Liu, L.F.; Yeh, E.T.H. Identification of the Molecular Basis of Doxorubicin-Induced Cardiotoxicity. Nat Med 2012, 18, 1639–1642. [Google Scholar] [CrossRef]
- Engeland, K. Cell Cycle Regulation: P53-P21-RB Signaling. Cell Death Differ 2022, 29, 946–960. [Google Scholar] [CrossRef]
- Polager, S.; Ginsberg, D. P53 and E2f: Partners in Life and Death. Nat Rev Cancer 2009, 9, 738–748. [Google Scholar] [CrossRef]
- Aubrey, B.J.; Kelly, G.L.; Janic, A.; Herold, M.J.; Strasser, A. How Does P53 Induce Apoptosis and How Does This Relate to P53-Mediated Tumour Suppression? Cell Death Differ 2018, 25, 104–113. [Google Scholar] [CrossRef]
- Zhu, W.; Soonpaa, M.H.; Chen, H.; Shen, W.; Payne, R.M.; Liechty, E.A.; Caldwell, R.L.; Shou, W.; Field, L.J. Acute Doxorubicin Cardiotoxicity Is Associated with P53-Induced Inhibition of the Mammalian Target of Rapamycin Pathway. Circulation 2009, 119, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, P.-Y.; Long, N.A.; Zhuang, J.; Springer, D.A.; Zou, J.; Lin, Y.; Bleck, C.K.E.; Park, J.-H.; Kang, J.-G.; et al. P53 Prevents Doxorubicin Cardiotoxicity Independently of Its Prototypical Tumor Suppressor Activities. Proc Natl Acad Sci U S A 2019, 116, 19626–19634. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Zhang, W.; Shou, W.; Field, L.J. P53 Inhibition Exacerbates Late-Stage Anthracycline Cardiotoxicity. Cardiovascular Research 2014, 103, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Sin, T.K.; Tam, B.T.; Yung, B.Y.; Yip, S.P.; Chan, L.W.; Wong, C.S.; Ying, M.; Rudd, J.A.; Siu, P.M. Resveratrol Protects against Doxorubicin-Induced Cardiotoxicity in Aged Hearts through the SIRT1-USP7 Axis. J Physiol 2015, 593, 1887–1899. [Google Scholar] [CrossRef]
- Zheng, W.; Lu, Y.-B.; Liang, S.-T.; Zhang, Q.-J.; Xu, J.; She, Z.-G.; Zhang, Z.-Q.; Yang, R.-F.; Mao, B.-B.; Xu, Z.; et al. SIRT1 Mediates the Protective Function of Nkx2.5 during Stress in Cardiomyocytes. Basic Res Cardiol 2013, 108, 364. [Google Scholar] [CrossRef]
- Wu, S.; Lan, J.; Li, L.; Wang, X.; Tong, M.; Fu, L.; Zhang, Y.; Xu, J.; Chen, X.; Chen, H.; et al. Sirt6 Protects Cardiomyocytes against Doxorubicin-Induced Cardiotoxicity by Inhibiting P53/Fas-Dependent Cell Death and Augmenting Endogenous Antioxidant Defense Mechanisms. Cell Biol Toxicol 2023, 39, 237–258. [Google Scholar] [CrossRef]
- Hori, Y.S.; Kuno, A.; Hosoda, R.; Horio, Y. Regulation of FOXOs and P53 by SIRT1 Modulators under Oxidative Stress. PLOS ONE 2013, 8, e73875. [Google Scholar] [CrossRef]
- Guo, Y.; Tang, Y.; Lu, G.; Gu, J. P53 at the Crossroads between Doxorubicin-Induced Cardiotoxicity and Resistance: A Nutritional Balancing Act. Nutrients 2023, 15, 2259. [Google Scholar] [CrossRef]
- Li, A.; Gao, M.; Jiang, W.; Qin, Y.; Gong, G. Mitochondrial Dynamics in Adult Cardiomyocytes and Heart Diseases. Frontiers in Cell and Developmental Biology 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Begum, R.; Thota, S.; Abdulkadir, A.; Kaur, G.; Bagam, P.; Batra, S. NADPH Oxidase Family Proteins: Signaling Dynamics to Disease Management. Cell Mol Immunol 2022, 19, 660–686. [Google Scholar] [CrossRef] [PubMed]
- Förstermann, U.; Sessa, W.C. Nitric Oxide Synthases: Regulation and Function. Eur Heart J 2012, 33, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Baek, B.S.; Song, S.H.; Kim, M.S.; Huh, J.I.; Shim, K.H.; Kim, K.W.; Lee, K.H. Xanthine Dehydrogenase/Xanthine Oxidase and Oxidative Stress. Age (Omaha) 1997, 20, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, D.L.; Swanson, J.D.; Pritsos, C.A. Role of Xanthine Oxidase in the Potentiation of Doxorubicin-Induced Cardiotoxicity by Mitomycin C. Cancer Commun 1991, 3, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Febuxostat Ameliorates Doxorubicin-Induced Cardiotoxicity in Rats - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26036690/ (accessed on 18 November 2023).
- Kondo, M.; Imanishi, M.; Fukushima, K.; Ikuto, R.; Murai, Y.; Horinouchi, Y.; Izawa-Ishizawa, Y.; Goda, M.; Zamami, Y.; Takechi, K.; et al. Xanthine Oxidase Inhibition by Febuxostat in Macrophages Suppresses Angiotensin II-Induced Aortic Fibrosis. Am J Hypertens 2019, 32, 249–256. [Google Scholar] [CrossRef]
- Cappetta, D.; De Angelis, A.; Sapio, L.; Prezioso, L.; Illiano, M.; Quaini, F.; Rossi, F.; Berrino, L.; Naviglio, S.; Urbanek, K. Oxidative Stress and Cellular Response to Doxorubicin: A Common Factor in the Complex Milieu of Anthracycline Cardiotoxicity. Oxid Med Cell Longev 2017, 2017, 1521020. [Google Scholar] [CrossRef]
- Zhuo, C.; Xin, J.; Huang, W.; Zhang, D.; Yan, X.; Li, R.; Li, H.; Lan, J.; Lin, L.; Li, L.; et al. Irisin Protects against Doxorubicin-Induced Cardiotoxicity by Improving AMPK-Nrf2 Dependent Mitochondrial Fusion and Strengthening Endogenous Anti-Oxidant Defense Mechanisms. Toxicology 2023, 494, 153597. [Google Scholar] [CrossRef]
- Hu, C.; Zhang, X.; Zhang, N.; Wei, W.-Y.; Li, L.-L.; Ma, Z.-G.; Tang, Q.-Z. Osteocrin Attenuates Inflammation, Oxidative Stress, Apoptosis, and Cardiac Dysfunction in Doxorubicin-Induced Cardiotoxicity. Clin Transl Med 2020, 10, e124. [Google Scholar] [CrossRef]
- Lassègue, B.; San Martín, A.; Griendling, K.K. Biochemistry, Physiology, and Pathophysiology of NADPH Oxidases in the Cardiovascular System. Circulation Research 2012, 110, 1364–1390. [Google Scholar] [CrossRef]
- Henriquez-Olguin, C.; Meneses-Valdes, R.; Raun, S.H.; Gallero, S.; Knudsen, J.R.; Li, Z.; Li, J.; Sylow, L.; Jaimovich, E.; Jensen, T.E. NOX2 Deficiency Exacerbates Diet-Induced Obesity and Impairs Molecular Training Adaptations in Skeletal Muscle. Redox Biology 2023, 65, 102842. [Google Scholar] [CrossRef]
- Efentakis, P.; Varela, A.; Chavdoula, E.; Sigala, F.; Sanoudou, D.; Tenta, R.; Gioti, K.; Kostomitsopoulos, N.; Papapetropoulos, A.; Tasouli, A.; et al. Levosimendan Prevents Doxorubicin-Induced Cardiotoxicity in Time- and Dose-Dependent Manner: Implications for Inotropy. Cardiovasc Res 2020, 116, 576–591. [Google Scholar] [CrossRef]
- Akolkar, G.; Bagchi, A.K.; Ayyappan, P.; Jassal, D.S.; Singal, P.K. Doxorubicin-Induced Nitrosative Stress Is Mitigated by Vitamin C via the Modulation of Nitric Oxide Synthases. Am J Physiol Cell Physiol 2017, 312, C418–C427. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yao, L.; Wu, X.; Guo, Q.; Sun, S.; Li, J.; Shi, G.; Caldwell, R.B.; Caldwell, R.W.; Chen, Y. Protection against Doxorubicin-Induced Cardiotoxicity through Modulating iNOS/ARG 2 Balance by Electroacupuncture at PC6. Oxidative Medicine and Cellular Longevity 2021, 2021, e6628957. [Google Scholar] [CrossRef] [PubMed]
- Sangweni, N.F.; van Vuuren, D.; Mabasa, L.; Gabuza, K.; Huisamen, B.; Naidoo, S.; Barry, R.; Johnson, R. Prevention of Anthracycline-Induced Cardiotoxicity: The Good and Bad of Current and Alternative Therapies. Frontiers in Cardiovascular Medicine 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.; Garcia, T.; Aniqa, M.; Ali, S.; Ally, A.; Nauli, S. Endothelial Nitric Oxide Synthase (eNOS) and the Cardiovascular System: In Physiology and in Disease States. Am J Biomed Sci Res 2022, 15, 153–177. [Google Scholar] [PubMed]
- Neilan, T.G.; Blake, S.L.; Ichinose, F.; Raher, M.J.; Buys, E.S.; Jassal, D.S.; Furutani, E.; Perez-Sanz, T.M.; Graveline, A.; Janssens, S.P.; et al. Disruption of Nitric Oxide Synthase 3 Protects against the Cardiac Injury, Dysfunction, and Mortality Induced by Doxorubicin. Circulation 2007, 116, 506–514. [Google Scholar] [CrossRef]
- He, H.; Wang, L.; Qiao, Y.; Zhou, Q.; Li, H.; Chen, S.; Yin, D.; Huang, Q.; He, M. Doxorubicin Induces Endotheliotoxicity and Mitochondrial Dysfunction via ROS/eNOS/NO Pathway. Front Pharmacol 2020, 10, 1531. [Google Scholar] [CrossRef]
- Zeglinski, M.; Premecz, S.; Lerner, J.; Wtorek, P.; Dasilva, M.; Hasanally, D.; Chaudhary, R.; Sharma, A.; Thliveris, J.; Ravandi, A.; et al. Congenital Absence of Nitric Oxide Synthase 3 Potentiates Cardiac Dysfunction and Reduces Survival in Doxorubicin- and Trastuzumab-Mediated Cardiomyopathy. Can J Cardiol 2014, 30, 359–367. [Google Scholar] [CrossRef]
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Myocardial Substrate Metabolism in the Normal and Failing Heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef]
- Marzoog, B.A.; Vlasova, T.I. Myocardiocyte Autophagy in the Context of Myocardiocytes Regeneration: A Potential Novel Therapeutic Strategy. Egyptian Journal of Medical Human Genetics 2022, 23, 41. [Google Scholar] [CrossRef]
- Afonso, A.I.; Amaro-Leal, Â.; Machado, F.; Rocha, I.; Geraldes, V. Doxorubicin Dose-Dependent Impact on Physiological Balance—A Holistic Approach in a Rat Model. Biology (Basel) 2023, 12, 1031. [Google Scholar] [CrossRef]
- Dallons, M.; Schepkens, C.; Dupuis, A.; Tagliatti, V.; Colet, J.-M. New Insights About Doxorubicin-Induced Toxicity to Cardiomyoblast-Derived H9C2 Cells and Dexrazoxane Cytoprotective Effect: Contribution of In Vitro 1H-NMR Metabonomics. Front Pharmacol 2020, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Qiao, X.; Van Der Zanden, S.Y.; Wander, D.P.A.; Borràs, D.M.; Song, J.-Y.; Li, X.; Van Duikeren, S.; Van Gils, N.; Rutten, A.; Van Herwaarden, T.; et al. Uncoupling DNA Damage from Chromatin Damage to Detoxify Doxorubicin. Proc. Natl. Acad. Sci. U.S.A. 2020, 117, 15182–15192. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, P.; Shikha, D.; Thakur, M.; Aneja, A. Functionality of Apigenin as a Potent Antioxidant with Emphasis on Bioavailability, Metabolism, Action Mechanism and in Vitro and in Vivo Studies: A Review. J Food Biochem 2022, 46, e13950. [Google Scholar] [CrossRef] [PubMed]
- Huo, C.-J.; Yu, X.-J.; Sun, Y.-J.; Li, H.-B.; Su, Q.; Bai, J.; Li, Y.; Liu, K.-L.; Qi, J.; Zhou, S.-W.; et al. Irisin Lowers Blood Pressure by Activating the Nrf2 Signaling Pathway in the Hypothalamic Paraventricular Nucleus of Spontaneously Hypertensive Rats. Toxicol Appl Pharmacol 2020, 394, 114953. [Google Scholar] [CrossRef] [PubMed]
- He, A.; Dean, J.M.; Lodhi, I.J. Peroxisomes as Cellular Adaptors to Metabolic and Environmental Stress. Trends Cell Biol 2021, 31, 656–670. [Google Scholar] [CrossRef]
- Schedin, S.; Sindelar, P.J.; Pentchev, P.; Brunk, U.; Dallner, G. Peroxisomal Impairment in Niemann-Pick Type C Disease. J Biol Chem 1997, 272, 6245–6251. [Google Scholar] [CrossRef]
- Kawałek, A.; Lefevre, S.D.; Veenhuis, M.; Klei, I.J. van der Peroxisomal Catalase Deficiency Modulates Yeast Lifespan Depending on Growth Conditions. Aging 2013, 5, 67–83. [Google Scholar] [CrossRef]
- Han, Y.-H.; Lian, X.-D.; Lee, S.-J.; Li, W.-L.; Sun, H.-N.; Jin, M.-H.; Kwon, T. Regulatory Effect of Peroxiredoxin 1 (PRDX1) on Doxorubicin-Induced Apoptosis in Triple Negative Breast Cancer Cells. Applied Biological Chemistry 2022, 65, 63. [Google Scholar] [CrossRef]
- Jiang, L.; Gong, Y.; Hu, Y.; You, Y.; Wang, J.; Zhang, Z.; Wei, Z.; Tang, C. Peroxiredoxin-1 Overexpression Attenuates Doxorubicin-Induced Cardiotoxicity by Inhibiting Oxidative Stress and Cardiomyocyte Apoptosis. Oxid Med Cell Longev 2020, 2020, 2405135. [Google Scholar] [CrossRef] [PubMed]
- Wanders, R.J.A.; Waterham, H.R. Peroxisomal Disorders: The Single Peroxisomal Enzyme Deficiencies. Biochimica et Biophysica Acta (BBA) - Molecular Cell Research 2006, 1763, 1707–1720. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Chiang, N.; Dalli, J.; Levy, B.D. Lipid Mediators in the Resolution of Inflammation. Cold Spring Harb Perspect Biol 2014, 7, a016311. [Google Scholar] [CrossRef] [PubMed]
- Endres, S.; Ghorbani, R.; Kelley, V.E.; Georgilis, K.; Lonnemann, G.; van der Meer, J.W.; Cannon, J.G.; Rogers, T.S.; Klempner, M.S.; Weber, P.C. The Effect of Dietary Supplementation with N-3 Polyunsaturated Fatty Acids on the Synthesis of Interleukin-1 and Tumor Necrosis Factor by Mononuclear Cells. N Engl J Med 1989, 320, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Reddy, J.K.; Hashimoto, T. Peroxisomal Beta-Oxidation and Peroxisome Proliferator-Activated Receptor Alpha: An Adaptive Metabolic System. Annu Rev Nutr 2001, 21, 193–230. [Google Scholar] [CrossRef]
- Kersten, S. Peroxisome Proliferator Activated Receptors and Lipoprotein Metabolism. PPAR Res 2008, 2008, 132960. [Google Scholar] [CrossRef]
- Arunachalam, S.; Tirupathi Pichiah, P.B.; Achiraman, S. Doxorubicin Treatment Inhibits PPARγ and May Induce Lipotoxicity by Mimicking a Type 2 Diabetes-like Condition in Rodent Models. FEBS Letters 2013, 587, 105–110. [Google Scholar] [CrossRef]
- Lin, Y.; Liu, R.; Huang, Y.; Yang, Z.; Xian, J.; Huang, J.; Qiu, Z.; Lin, X.; Zhang, M.; Chen, H.; et al. Reactivation of PPARα Alleviates Myocardial Lipid Accumulation and Cardiac Dysfunction by Improving Fatty Acid β-Oxidation in Dsg2-Deficient Arrhythmogenic Cardiomyopathy. Acta Pharm Sin B 2023, 13, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Fang, Q.; Zhang, Z.; Wang, D.; Wu, L.; Wang, Y. PPARα Ameliorates Doxorubicin-Induced Cardiotoxicity by Reducing Mitochondria-Dependent Apoptosis via Regulating MEOX1. Front Pharmacol 2020, 11, 528267. [Google Scholar] [CrossRef]
- Huang, W.-P.; Yin, W.-H.; Chen, J.-S.; Huang, P.-H.; Chen, J.-W.; Lin, S.-J. Fenofibrate Attenuates Doxorubicin-Induced Cardiac Dysfunction in Mice via Activating the eNOS/EPC Pathway. Sci Rep 2021, 11, 1159. [Google Scholar] [CrossRef]
- North, B.J.; Verdin, E. Sirtuins: Sir2-Related NAD-Dependent Protein Deacetylases. Genome Biol 2004, 5, 224. [Google Scholar] [CrossRef]
- Matsushima, S.; Sadoshima, J. The Role of Sirtuins in Cardiac Disease. American Journal of Physiology-Heart and Circulatory Physiology 2015, 309, H1375–H1389. [Google Scholar] [CrossRef]
- Ministrini, S.; Puspitasari, Y.M.; Beer, G.; Liberale, L.; Montecucco, F.; Camici, G.G. Sirtuin 1 in Endothelial Dysfunction and Cardiovascular Aging. Frontiers in Physiology 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Murugasamy, K.; Munjal, A.; Sundaresan, N.R. Emerging Roles of SIRT3 in Cardiac Metabolism. Front Cardiovasc Med 2022, 9, 850340. [Google Scholar] [CrossRef] [PubMed]
- Saiyang, X.; Deng, W.; Qizhu, T. Sirtuin 6: A Potential Therapeutic Target for Cardiovascular Diseases. Pharmacol Res 2021, 163, 105214. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, S.; Izumiya, Y.; Araki, S.; Nakamura, T.; Kimura, Y.; Hanatani, S.; Yamada, T.; Ishida, T.; Yamamoto, M.; Onoue, Y.; et al. Cardiomyocyte Sirt (Sirtuin) 7 Ameliorates Stress-Induced Cardiac Hypertrophy by Interacting With and Deacetylating GATA4. Hypertension 2020, 75, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.A.; Hirschey, M.D. Mitochondrial Protein Acetylation Regulates Metabolism. Essays Biochem 2012, 52, 10–1042. [Google Scholar] [CrossRef]
- Stein, L.R.; Imai, S. The Dynamic Regulation of NAD Metabolism in Mitochondria. Trends Endocrinol Metab 2012, 23, 420–428. [Google Scholar] [CrossRef]
- Zhang, Y.; Bharathi, S.S.; Beck, M.E.; Goetzman, E.S. The Fatty Acid Oxidation Enzyme Long-Chain Acyl-CoA Dehydrogenase Can Be a Source of Mitochondrial Hydrogen Peroxide. Redox Biol 2019, 26, 101253. [Google Scholar] [CrossRef]
- Parodi-Rullán, R.M.; Chapa-Dubocq, X.R.; Javadov, S. Acetylation of Mitochondrial Proteins in the Heart: The Role of SIRT3. Front Physiol 2018, 9, 1094. [Google Scholar] [CrossRef]
- Dikalova, A.E.; Itani, H.A.; Nazarewicz, R.R.; McMaster, W.G.; Flynn, C.R.; Uzhachenko, R.; Fessel, J.P.; Gamboa, J.L.; Harrison, D.G.; Dikalov, S.I. Sirt3 Impairment and SOD2 Hyperacetylation in Vascular Oxidative Stress and Hypertension. Circ Res 2017, 121, 564–574. [Google Scholar] [CrossRef]
- Sundaresan, N.R.; Samant, S.A.; Pillai, V.B.; Rajamohan, S.B.; Gupta, M.P. SIRT3 Is a Stress-Responsive Deacetylase in Cardiomyocytes That Protects Cells from Stress-Mediated Cell Death by Deacetylation of Ku70. Mol Cell Biol 2008, 28, 6384–6401. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Cantrell, A.C.; Chen, J.-X.; Gu, W.; Zeng, H. SIRT3 Deficiency Enhances Ferroptosis and Promotes Cardiac Fibrosis via P53 Acetylation. Cells 2023, 12, 1428. [Google Scholar] [CrossRef]
- Li, Z.; Lu, G.; Lu, J.; Wang, P.; Zhang, X.; Zou, Y.; Liu, P. SZC-6, a Small-Molecule Activator of SIRT3, Attenuates Cardiac Hypertrophy in Mice. Acta Pharmacol Sin 2023, 44, 546–560. [Google Scholar] [CrossRef]
- Wang, M.; Ding, Y.; Hu, Y.; Li, Z.; Luo, W.; Liu, P.; Li, Z. SIRT3 Improved Peroxisomes-Mitochondria Interplay and Prevented Cardiac Hypertrophy via Preserving PEX5 Expression. Redox Biology 2023, 62, 102652. [Google Scholar] [CrossRef] [PubMed]
- Ling, G.; Wang, X.; Tan, N.; Cao, J.; Li, W.; Zhang, Y.; Jiang, J.; Sun, Q.; Jiang, Y.; Wang, W.; et al. Mechanisms and Drug Intervention for Doxorubicin-Induced Cardiotoxicity Based on Mitochondrial Bioenergetics. Oxidative Medicine and Cellular Longevity 2022, 2022, e7176282. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Shen, T.; Lian, J.; Deng, K.; Qu, C.; Li, E.; Li, G.; Ren, Y.; Wang, Z.; Jiang, Z.; et al. Resveratrol Reduces ROS-Induced Ferroptosis by Activating SIRT3 and Compensating the GSH/GPX4 Pathway. Molecular Medicine 2023, 29, 137. [Google Scholar] [CrossRef] [PubMed]
- Christidi, E.; Brunham, L.R. Regulated Cell Death Pathways in Doxorubicin-Induced Cardiotoxicity. Cell Death Dis 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yang, Y.; Wang, S.; He, X.; Liu, M.; Bai, B.; Tian, C.; Sun, R.; Yu, T.; Chu, X. Role of Acetylation in Doxorubicin-Induced Cardiotoxicity. Redox Biol 2021, 46, 102089. [Google Scholar] [CrossRef] [PubMed]
- Nagasaka, M.; Miyajima, C.; Aoki, H.; Aoyama, M.; Morishita, D.; Inoue, Y.; Hayashi, H. Insights into Regulators of P53 Acetylation. Cells 2022, 11, 3825. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, S.; Zhang, B.; Liu, J. SIRT3 as a Potential Therapeutic Target for Heart Failure. Pharmacological Research 2021, 165, 105432. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-N.; Dai, Y.; Zhang, C.-H.; Omondi, A.M.; Ghosh, A.; Khanra, I.; Chakraborty, M.; Yu, X.-B.; Liang, J. Sirtuins Family as a Target in Endothelial Cell Dysfunction: Implications for Vascular Ageing. Biogerontology 2020, 21, 495–516. [Google Scholar] [CrossRef]
- Song, W.; Wang, F.; Lotfi, P.; Sardiello, M.; Segatori, L. 2-Hydroxypropyl-β-Cyclodextrin Promotes Transcription Factor EB-Mediated Activation of Autophagy: Implications for Therapy. J Biol Chem 2014, 289, 10211–10222. [Google Scholar] [CrossRef]
- Moruno-Manchon, J.F.; Uzor, N.-E.; Kesler, S.R.; Wefel, J.S.; Townley, D.M.; Nagaraja, A.S.; Pradeep, S.; Mangala, L.S.; Sood, A.K.; Tsvetkov, A.S. Peroxisomes Contribute to Oxidative Stress in Neurons during Doxorubicin-Based Chemotherapy. Mol Cell Neurosci 2018, 86, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Bu, S.; Joseph, J.J.; Nguyen, H.C.; Ehsan, M.; Rasheed, B.; Singh, A.; Qadura, M.; Frisbee, J.C.; Singh, K.K. MicroRNA miR-378-3p Is a Novel Regulator of Endothelial Autophagy and Function. Journal of Molecular and Cellular Cardiology Plus 2023, 3, 100027. [Google Scholar] [CrossRef]
- Bu, S.; Singh, K.K. Epigenetic Regulation of Autophagy in Cardiovascular Pathobiology. Int J Mol Sci 2021, 22, 6544. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Cui, T.; Wang, X. The Interplay Between Autophagy and Regulated Necrosis. Antioxid Redox Signal 2023, 38, 550–580. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.K.; Lovren, F.; Pan, Y.; Quan, A.; Ramadan, A.; Matkar, P.N.; Ehsan, M.; Sandhu, P.; Mantella, L.E.; Gupta, N.; et al. The Essential Autophagy Gene ATG7 Modulates Organ Fibrosis via Regulation of Endothelial-to-Mesenchymal Transition. J Biol Chem 2015, 290, 2547–2559. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wei, X.; Zhang, H.; Wu, Y.; Jing, J.; Huang, R.; Zhou, T.; Hu, J.; Wu, Y.; Li, Y.; et al. Doxorubicin Downregulates Autophagy to Promote Apoptosis-Induced Dilated Cardiomyopathy via Regulating the AMPK/mTOR Pathway. Biomedicine & Pharmacotherapy 2023, 162, 114691. [Google Scholar] [CrossRef]
- Koleini, N.; Kardami, E. Autophagy and Mitophagy in the Context of Doxorubicin-Induced Cardiotoxicity. Oncotarget 2017, 8, 46663–46680. [Google Scholar] [CrossRef]
- Mitry, M.A.; Edwards, J.G. Doxorubicin Induced Heart Failure: Phenotype and Molecular Mechanisms. Int J Cardiol Heart Vasc 2015, 10, 17–24. [Google Scholar] [CrossRef]
- Radu, R.I.; Bold, A.; Pop, O.T.; Mălăescu, D.G.; Gheorghişor, I.; Mogoantă, L. Histological and Immunohistochemical Changes of the Myocardium in Dilated Cardiomyopathy. Rom J Morphol Embryol 2012, 53, 269–275. [Google Scholar]
- Hanna, A.D.; Lam, A.; Tham, S.; Dulhunty, A.F.; Beard, N.A. Adverse Effects of Doxorubicin and Its Metabolic Product on Cardiac RyR2 and SERCA2A. Mol Pharmacol 2014, 86, 438–449. [Google Scholar] [CrossRef]
- Chia, P.Y.; Teo, A.; Yeo, T.W. Overview of the Assessment of Endothelial Function in Humans. Front Med (Lausanne) 2020, 7, 542567. [Google Scholar] [CrossRef]
- Dye, B.; Lincoln, J. The Endocardium and Heart Valves. Cold Spring Harb Perspect Biol 2020, 12, a036723. [Google Scholar] [CrossRef] [PubMed]
- Harris, I.S.; Black, B.L. Development of the Endocardium. Pediatr Cardiol 2010, 31, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Dewing, J.M.; Saunders, V.; O’Kelly, I.; Wilson, D.I. Defining Cardiac Cell Populations and Relative Cellular Composition of the Early Fetal Human Heart. PLOS ONE 2022, 17, e0259477. [Google Scholar] [CrossRef]
- Luu, A.Z.; Chowdhury, B.; Al-Omran, M.; Teoh, H.; Hess, D.A.; Verma, S. Role of Endothelium in Doxorubicin-Induced Cardiomyopathy. JACC Basic Transl Sci 2018, 3, 861–870. [Google Scholar] [CrossRef]
- Félétou, M. Multiple Functions of the Endothelial Cells. In The Endothelium: Part 1: Multiple Functions of the Endothelial Cells—Focus on Endothelium-Derived Vasoactive Mediators; Morgan & Claypool Life Sciences, 2011.
- Singh, S.; Nguyen, H.; Michels, D.; Bazinet, H.; Matkar, P.N.; Liu, Z.; Esene, L.; Adam, M.; Bugyei-Twum, A.; Mebrahtu, E.; et al. BReast CAncer Susceptibility Gene 2 Deficiency Exacerbates Oxidized LDL-Induced DNA Damage and Endothelial Apoptosis. Physiol Rep 2020, 8, e14481–e14481. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Ji, W.; Yang, H.; Chen, S.; Zhang, W.; Duan, G. Endothelial Activation and Dysfunction in COVID-19: From Basic Mechanisms to Potential Therapeutic Approaches. Signal Transduct Target Ther 2020, 5, 293. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Bu, S.; Nikfarjam, S.; Rasheed, B.; Michels, D.C.R.; Singh, A.; Singh, S.; Marszal, C.; McGuire, J.J.; Feng, Q.; et al. Loss of Fatty Acid Binding Protein 3 Ameliorates Lipopolysaccharide-Induced Inflammation and Endothelial Dysfunction. J Biol Chem 2023, 299, 102921. [Google Scholar] [CrossRef]
- Sun, H.-J.; Wu, Z.-Y.; Nie, X.-W.; Bian, J.-S. Role of Endothelial Dysfunction in Cardiovascular Diseases: The Link Between Inflammation and Hydrogen Sulfide. Front Pharmacol 2020, 10, 1568–1568. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, L.; Li, W.; Wang, L.; Jia, Q.; Shi, F.; Li, K.; Liao, L.; Shi, Y.; Wu, S. The Role of TOP2A in Immunotherapy and Vasculogenic Mimicry in Non-Small Cell Lung Cancer and Its Potential Mechanism. Sci Rep 2023, 13, 10906. [Google Scholar] [CrossRef]
- Hopfner, K.-P.; Hornung, V. Molecular Mechanisms and Cellular Functions of cGAS–STING Signalling. Nat Rev Mol Cell Biol 2020, 21, 501–521. [Google Scholar] [CrossRef]
- Lovitt, C.J.; Shelper, T.B.; Avery, V.M. Doxorubicin Resistance in Breast Cancer Cells Is Mediated by Extracellular Matrix Proteins. BMC Cancer 2018, 18, 41. [Google Scholar] [CrossRef] [PubMed]
- Rawat, P.S.; Jaiswal, A.; Khurana, A.; Bhatti, J.S.; Navik, U. Doxorubicin-Induced Cardiotoxicity: An Update on the Molecular Mechanism and Novel Therapeutic Strategies for Effective Management. Biomedicine & Pharmacotherapy 2021, 139, 111708. [Google Scholar] [CrossRef]
- Mu, H.; Liu, H.; Zhang, J.; Huang, J.; Zhu, C.; Lu, Y.; Shi, Y.; Wang, Y. Ursolic Acid Prevents Doxorubicin-Induced Cardiac Toxicity in Mice through eNOS Activation and Inhibition of eNOS Uncoupling. J Cell Mol Med 2019, 23, 2174–2183. [Google Scholar] [CrossRef] [PubMed]
- Bian, Y.; Sun, M.; Silver, M.; Ho, K.K.L.; Marchionni, M.A.; Caggiano, A.O.; Stone, J.R.; Amende, I.; Hampton, T.G.; Morgan, J.P.; et al. Neuregulin-1 Attenuated Doxorubicin-Induced Decrease in Cardiac Troponins. Am J Physiol Heart Circ Physiol 2009, 297, H1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Q.; Yang, M.; Duan, C.H.; Su, G.B.; Wang, J.H.; Liu, Y.F.; Zhang, J. Protective Role of Neuregulin-1 toward Doxorubicin-Induced Myocardial Toxicity. Genet Mol Res 2014, 13, 4627–4634. [Google Scholar] [CrossRef] [PubMed]
- Frey, R.S.; Ushio-Fukai, M.; Malik, A.B. NADPH Oxidase-Dependent Signaling in Endothelial Cells: Role in Physiology and Pathophysiology. Antioxid Redox Signal 2009, 11, 791–810. [Google Scholar] [CrossRef] [PubMed]
- Daiber, A.; Xia, N.; Steven, S.; Oelze, M.; Hanf, A.; Kröller-Schön, S.; Münzel, T.; Li, H. New Therapeutic Implications of Endothelial Nitric Oxide Synthase (eNOS) Function/Dysfunction in Cardiovascular Disease. International Journal of Molecular Sciences 2019, 20, 187. [Google Scholar] [CrossRef]
- Landmesser, U.; Spiekermann, S.; Preuss, C.; Sorrentino, S.; Fischer, D.; Manes, C.; Mueller, M.; Drexler, H. Angiotensin II Induces Endothelial Xanthine Oxidase Activation: Role for Endothelial Dysfunction in Patients with Coronary Disease. Arterioscler Thromb Vasc Biol 2007, 27, 943–948. [Google Scholar] [CrossRef]
- Bishop-Bailey, D.; Swales, K.E. The Role of PPARs in the Endothelium: Implications for Cancer Therapy. PPAR Res 2008, 2008, 904251–904251. [Google Scholar] [CrossRef]
- Fang, Z.; Wang, X.; Sun, X.; Hu, W.; Miao, Q.R. The Role of Histone Protein Acetylation in Regulating Endothelial Function. Frontiers in Cell and Developmental Biology 2021, 9. [Google Scholar] [CrossRef]
- Man, A.W.C.; Li, H.; Xia, N. The Role of Sirtuin1 in Regulating Endothelial Function, Arterial Remodeling and Vascular Aging. Front Physiol 2019, 10, 1173. [Google Scholar] [CrossRef]
- Yang, K.; Dong, W. SIRT1-Related Signaling Pathways and Their Association With Bronchopulmonary Dysplasia. Frontiers in Medicine 2021, 8. [Google Scholar] [CrossRef]
- Stein, S.; Schäfer, N.; Breitenstein, A.; Besler, C.; Winnik, S.; Lohmann, C.; Heinrich, K.; Brokopp, C.E.; Handschin, C.; Landmesser, U.; et al. SIRT1 Reduces Endothelial Activation without Affecting Vascular Function in ApoE-/- Mice. Aging (Albany NY) 2010, 2, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Yu, S.; Chao, M.; Wang, Y.; Xiong, J.; Lai, H. SIRT4 Suppresses the PI3K/Akt/NF-κB Signaling Pathway and Attenuates HUVEC Injury Induced by oxLDL. Mol Med Rep 2019, 19, 4973–4979. [Google Scholar] [CrossRef]
- Martino, E.; Balestrieri, A.; Anastasio, C.; Maione, M.; Mele, L.; Cautela, D.; Campanile, G.; Balestrieri, M.L.; D’Onofrio, N. SIRT3 Modulates Endothelial Mitochondrial Redox State during Insulin Resistance. Antioxidants (Basel) 2022, 11, 1611. [Google Scholar] [CrossRef]
- Hwang, J.; Yao, H.; Caito, S.; Sundar, I.K.; Rahman, I. Redox Regulation of SIRT1 in Inflammation and Cellular Senescence. Free Radic Biol Med 2013, 61, 95–110. [Google Scholar] [CrossRef]
- Liu, Z.-H.; Zhang, Y.; Wang, X.; Fan, X.-F.; Zhang, Y.; Li, X.; Gong, Y.-S.; Han, L.-P. SIRT1 Activation Attenuates Cardiac Fibrosis by Endothelial-to-Mesenchymal Transition. Biomed Pharmacother 2019, 118, 109227. [Google Scholar] [CrossRef] [PubMed]
- Graziani, S.; Scorrano, L.; Pontarin, G. Transient Exposure of Endothelial Cells to Doxorubicin Leads to Long-Lasting Vascular Endothelial Growth Factor Receptor 2 Downregulation. Cells 2022, 11, 210. [Google Scholar] [CrossRef] [PubMed]
- Spengler, K.; Kryeziu, N.; Große, S.; Mosig, A.S.; Heller, R. VEGF Triggers Transient Induction of Autophagy in Endothelial Cells via AMPKα1. Cells 2020, 9, 687. [Google Scholar] [CrossRef] [PubMed]
- Luu, A.Z.; Luu, V.Z.; Chowdhury, B.; Kosmopoulos, A.; Pan, Y.; Al-Omran, M.; Quan, A.; Teoh, H.; Hess, D.A.; Verma, S. Loss of Endothelial Cell-Specific Autophagy-Related Protein 7 Exacerbates Doxorubicin-Induced Cardiotoxicity. Biochem Biophys Rep 2021, 25, 100926. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J. BRCA Mutations and Breast Cancer Prevention. Cancers (Basel) 2018, 10, 524. [Google Scholar] [CrossRef] [PubMed]
- BRCA1 and BRCA2: Cancer Risks and Management (PDQ®) - PDQ Cancer Information Summaries - NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK589498/ (accessed on 13 October 2023).
- Roy, R.; Chun, J.; Powell, S.N. BRCA1 and BRCA2: Different Roles in a Common Pathway of Genome Protection. Nat Rev Cancer 2011, 12, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Griendling, K.K.; FitzGerald, G.A. Oxidative Stress and Cardiovascular Injury: Part II: Animal and Human Studies. Circulation 2003, 108, 2034–2040. [Google Scholar] [CrossRef]
- Robert, G.; Wagner, J.R. ROS-Induced DNA Damage as an Underlying Cause of Aging. Advances in Geriatric Medicine and Research 2020, 4. [Google Scholar] [CrossRef]
- Giglia-Mari, G.; Zotter, A.; Vermeulen, W. DNA Damage Response. Cold Spring Harb Perspect Biol 2011, 3, a000745. [Google Scholar] [CrossRef]
- Luijsterburg, M.S.; van Attikum, H. Chromatin and the DNA Damage Response: The Cancer Connection. Mol Oncol 2011, 5, 349–367. [Google Scholar] [CrossRef]
- Hegde, M.L.; Hazra, T.K.; Mitra, S. Early Steps in the DNA Base Excision/Single-Strand Interruption Repair Pathway in Mammalian Cells. Cell Res 2008, 18, 27–47. [Google Scholar] [CrossRef]
- Luo, K.; Huang, W.; Tang, S. Sirt3 Enhances Glioma Cell Viability by Stabilizing Ku70-BAX Interaction. Onco Targets Ther 2018, 11, 7559–7567. [Google Scholar] [CrossRef]
- Gupta, A.; Hunt, C.R.; Chakraborty, S.; Pandita, R.K.; Yordy, J.; Ramnarain, D.B.; Horikoshi, N.; Pandita, T.K. Role of 53BP1 in the Regulation of DNA Double-Strand Break Repair Pathway Choice. Radiat Res 2014, 181, 1–8. [Google Scholar] [CrossRef]
- Dimitrova, N.; Chen, Y.-C.M.; Spector, D.L.; de Lange, T. 53BP1 Promotes Non-Homologous End Joining of Telomeres by Increasing Chromatin Mobility. Nature 2008, 456, 524–528. [Google Scholar] [CrossRef]
- Wu, Q.; Liang, S.; Ochi, T.; Chirgadze, D.Y.; Huiskonen, J.T.; Blundell, T.L. Understanding the Structure and Role of DNA-PK in NHEJ: How X-Ray Diffraction and Cryo-EM Contribute in Complementary Ways. Prog Biophys Mol Biol 2019, 147, 26–32. [Google Scholar] [CrossRef]
- Mao, Z.; Bozzella, M.; Seluanov, A.; Gorbunova, V. DNA Repair by Nonhomologous End Joining and Homologous Recombination during Cell Cycle in Human Cells. Cell Cycle 2008, 7, 2902–2906. [Google Scholar] [CrossRef]
- Achanta, G.; Pelicano, H.; Feng, L.; Plunkett, W.; Huang, P. Interaction of P53 and DNA-PK in Response to Nucleoside Analogues: Potential Role as a Sensor Complex for DNA Damage. Cancer Res 2001, 61, 8723–8729. [Google Scholar]
- Xu, Y.; Ning, S.; Wei, Z.; Xu, R.; Xu, X.; Xing, M.; Guo, R.; Xu, D. 53BP1 and BRCA1 Control Pathway Choice for Stalled Replication Restart. Elife 2017, 6, e30523. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.R.; Taylor, M.R.G.; Boulton, S.J. Playing the End Game: DNA Double-Strand Break Repair Pathway Choice. Mol Cell 2012, 47, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Heyer, W.-D. Homologous Recombination in DNA Repair and DNA Damage Tolerance. Cell Res 2008, 18, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Friedman, L.S.; Ostermeyer, E.A.; Szabo, C.I.; Dowd, P.; Lynch, E.D.; Rowell, S.E.; King, M.C. Confirmation of BRCA1 by Analysis of Germline Mutations Linked to Breast and Ovarian Cancer in Ten Families. Nat Genet 1994, 8, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Godin, S.K.; Sullivan, M.R.; Bernstein, K.A. Novel Insights into RAD51 Activity and Regulation during Homologous Recombination and DNA Replication. Biochem Cell Biol 2016, 94, 407–418. [Google Scholar] [CrossRef]
- MacLachlan, T.K.; El-Deiry, W. Functional Interactions Between BRCA1 and the Cell Cycle; Landes Bioscience, 2013.
- Petrucelli, N.; Daly, M.B.; Pal, T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. In GeneReviews®; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington, Seattle: Seattle (WA), 1993. [Google Scholar]
- Nyberg, T.; Frost, D.; Barrowdale, D.; Evans, D.G.; Bancroft, E.; Adlard, J.; Ahmed, M.; Barwell, J.; Brady, A.F.; Brewer, C.; et al. Prostate Cancer Risks for Male BRCA1 and BRCA2 Mutation Carriers: A Prospective Cohort Study. Eur Urol 2020, 77, 24–35. [Google Scholar] [CrossRef]
- Ibrahim, M.; Yadav, S.; Ogunleye, F.; Zakalik, D. Male BRCA Mutation Carriers: Clinical Characteristics and Cancer Spectrum. BMC Cancer 2018, 18, 179. [Google Scholar] [CrossRef] [PubMed]
- Abul-Husn, N.S.; Soper, E.R.; Odgis, J.A.; Cullina, S.; Bobo, D.; Moscati, A.; Rodriguez, J.E.; CBIPM Genomics Team; Regeneron Genetics, Center; Loos, R.J.F.; et al. Exome Sequencing Reveals a High Prevalence of BRCA1 and BRCA2 Founder Variants in a Diverse Population-Based Biobank. Genome Med 2019, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, R. Hereditary Breast and Ovarian Cancer (HBOC): Review of Its Molecular Characteristics, Screening, Treatment, and Prognosis. Breast Cancer 2021, 28, 1167–1180. [Google Scholar] [CrossRef] [PubMed]
- Mai, P.L.; Chatterjee, N.; Hartge, P.; Tucker, M.; Brody, L.; Struewing, J.P.; Wacholder, S. Potential Excess Mortality in BRCA1/2 Mutation Carriers beyond Breast, Ovarian, Prostate, and Pancreatic Cancers, and Melanoma. PLoS One 2009, 4, e4812. [Google Scholar] [CrossRef] [PubMed]
- BRCA1 Protein Expression Summary - The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000012048-BRCA1 (accessed on 12 July 2022).
- Hagemeister, F.B.; Buzdar, A.U.; Luna, M.A.; Blumenschein, G.R. Causes of Death in Breast Cancer: A Clinicopathologic Study. Cancer 1980, 46, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Florido, R.; Daya, N.R.; Ndumele, C.E.; Koton, S.; Russell, S.D.; Prizment, A.; Blumenthal, R.S.; Matsushita, K.; Mok, Y.; Felix, A.S.; et al. Cardiovascular Disease Risk Among Cancer Survivors: The Atherosclerosis Risk In Communities (ARIC) Study. J Am Coll Cardiol 2022, 80, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.K.; Shukla, P.C.; Quan, A.; Desjardins, J.-F.; Lovren, F.; Pan, Y.; Garg, V.; Gosal, S.; Garg, A.; Szmitko, P.E.; et al. BRCA2 Protein Deficiency Exaggerates Doxorubicin-Induced Cardiomyocyte Apoptosis and Cardiac Failure. J Biol Chem 2012, 287, 6604–6614. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.K.; Shukla, P.C.; Quan, A.; Al-Omran, M.; Lovren, F.; Pan, Y.; Brezden-Masley, C.; Ingram, A.J.; Stanford, W.L.; Teoh, H.; et al. BRCA1 Is a Novel Target to Improve Endothelial Dysfunction and Retard Atherosclerosis. The Journal of Thoracic and Cardiovascular Surgery 2013, 146, 949–960.e4. [Google Scholar] [CrossRef]
- Sajjad, M.; Fradley, M.; Sun, W.; Kim, J.; Zhao, X.; Pal, T.; Ismail-Khan, R. An Exploratory Study to Determine Whether BRCA1 and BRCA2 Mutation Carriers Have Higher Risk of Cardiac Toxicity. Genes (Basel) 2017, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Pearson, E.J.; Nair, A.; Daoud, Y.; Blum, J.L. The Incidence of Cardiomyopathy in BRCA1 and BRCA2 Mutation Carriers after Anthracycline-Based Adjuvant Chemotherapy. Breast Cancer Res Treat 2017, 162, 59–67. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Illustrated summary of all doxorubicin’s mechanisms of cytotoxicity up to date. Red arrows indicate direct actions of doxorubicin. ROS = Reactive oxygen species; RNS = Reactive nitrogen species; NOX = NADPH oxidase; NOS = Nitric oxide synthase; XO = Xanthine oxidase; PPAR = Peroxisome proliferator-activated receptors; NRF2 = Nuclear factor erythroid 2-related factor 2; SIRTs = Sirtuin-like proteins; Topo2A/B = Topoisomerase 2A/B; BRCA = Breast cancer gene; TNFa = Tumor necrosis factor alpha.
Figure 1.
Illustrated summary of all doxorubicin’s mechanisms of cytotoxicity up to date. Red arrows indicate direct actions of doxorubicin. ROS = Reactive oxygen species; RNS = Reactive nitrogen species; NOX = NADPH oxidase; NOS = Nitric oxide synthase; XO = Xanthine oxidase; PPAR = Peroxisome proliferator-activated receptors; NRF2 = Nuclear factor erythroid 2-related factor 2; SIRTs = Sirtuin-like proteins; Topo2A/B = Topoisomerase 2A/B; BRCA = Breast cancer gene; TNFa = Tumor necrosis factor alpha.
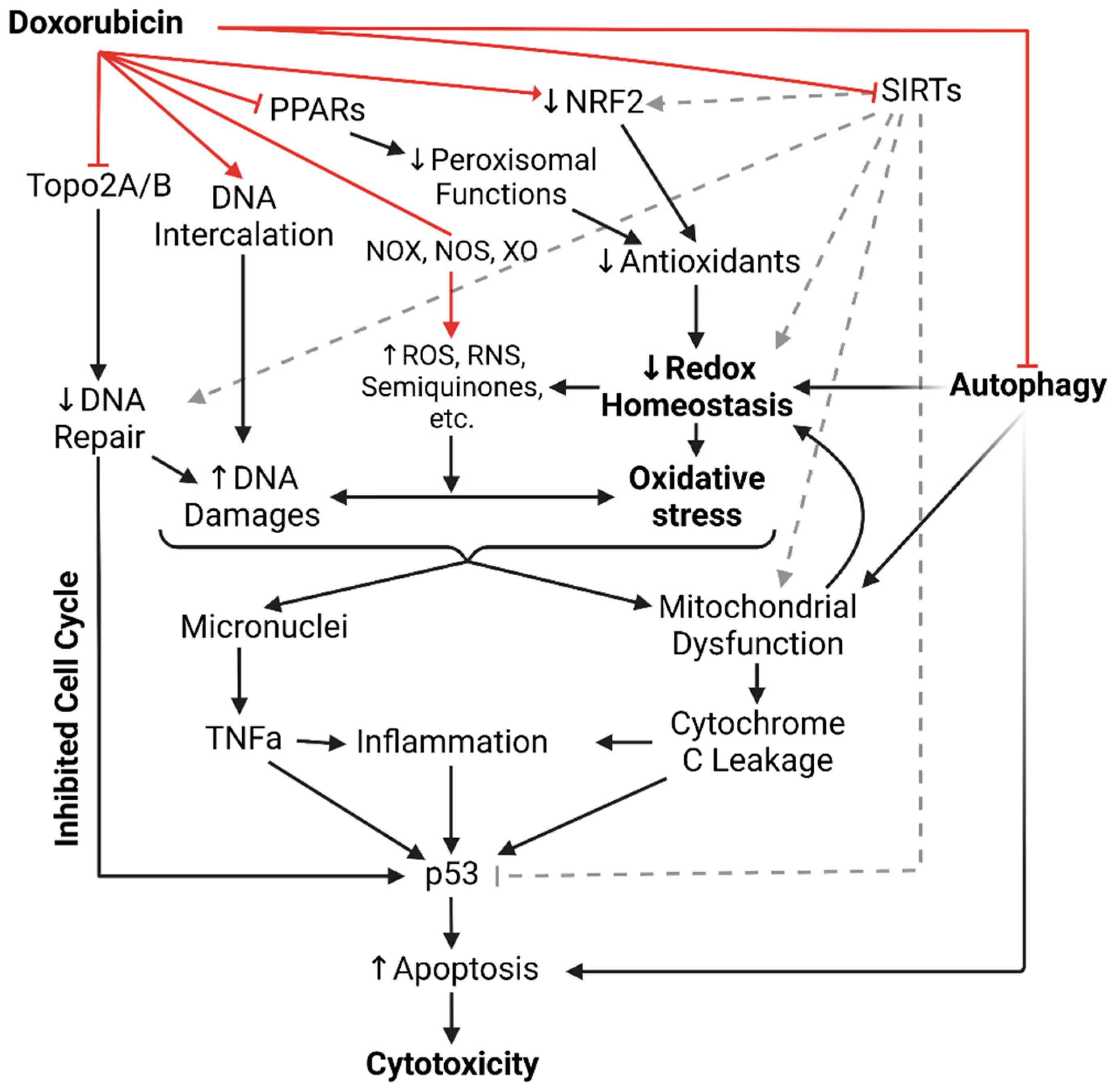
Figure 2.
Doxorubicin’s induced endotheliotoxicity exacerbate cardiotoxicity.
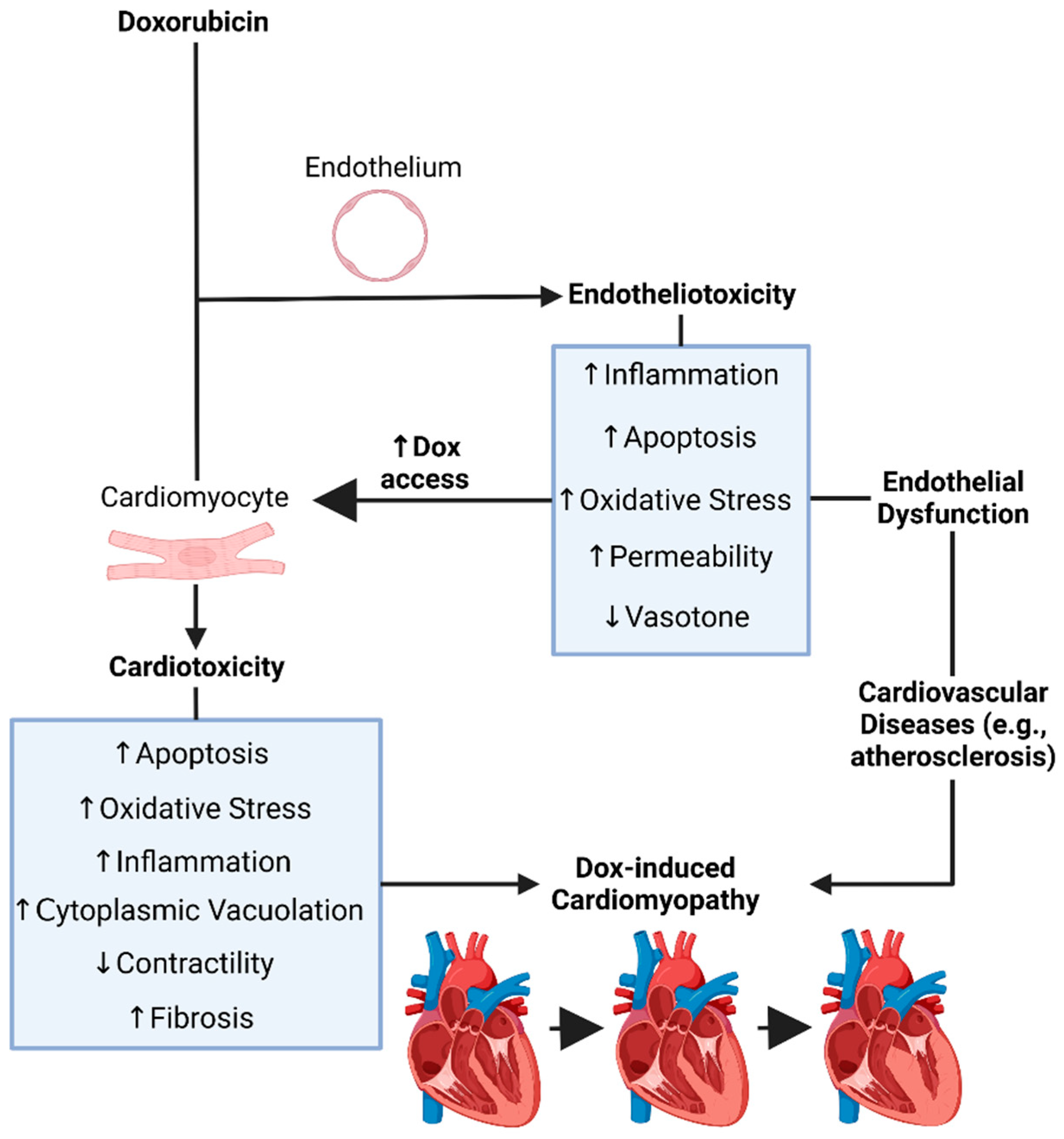
Figure 3.
Roles of BRCA1 and BRCA2 in Homologous Recombination Repair of double-strand breaks. MRN complex = Mre11, Rad50 and Nbs1 complex; BRCA1/2 = Breast cancer gene 1/2; BARD1 = BRCA1-associated RING domain protein 1; TOPBP1 = DNA topoisomerase 2-binding protein 1; RPA = Replication protein A; PALB2 = Partner And Locator of BRCA2; RAD51 = RAD51 Recombinase; RAP80 = Receptor-Associated Protein 80.
Figure 3.
Roles of BRCA1 and BRCA2 in Homologous Recombination Repair of double-strand breaks. MRN complex = Mre11, Rad50 and Nbs1 complex; BRCA1/2 = Breast cancer gene 1/2; BARD1 = BRCA1-associated RING domain protein 1; TOPBP1 = DNA topoisomerase 2-binding protein 1; RPA = Replication protein A; PALB2 = Partner And Locator of BRCA2; RAD51 = RAD51 Recombinase; RAP80 = Receptor-Associated Protein 80.
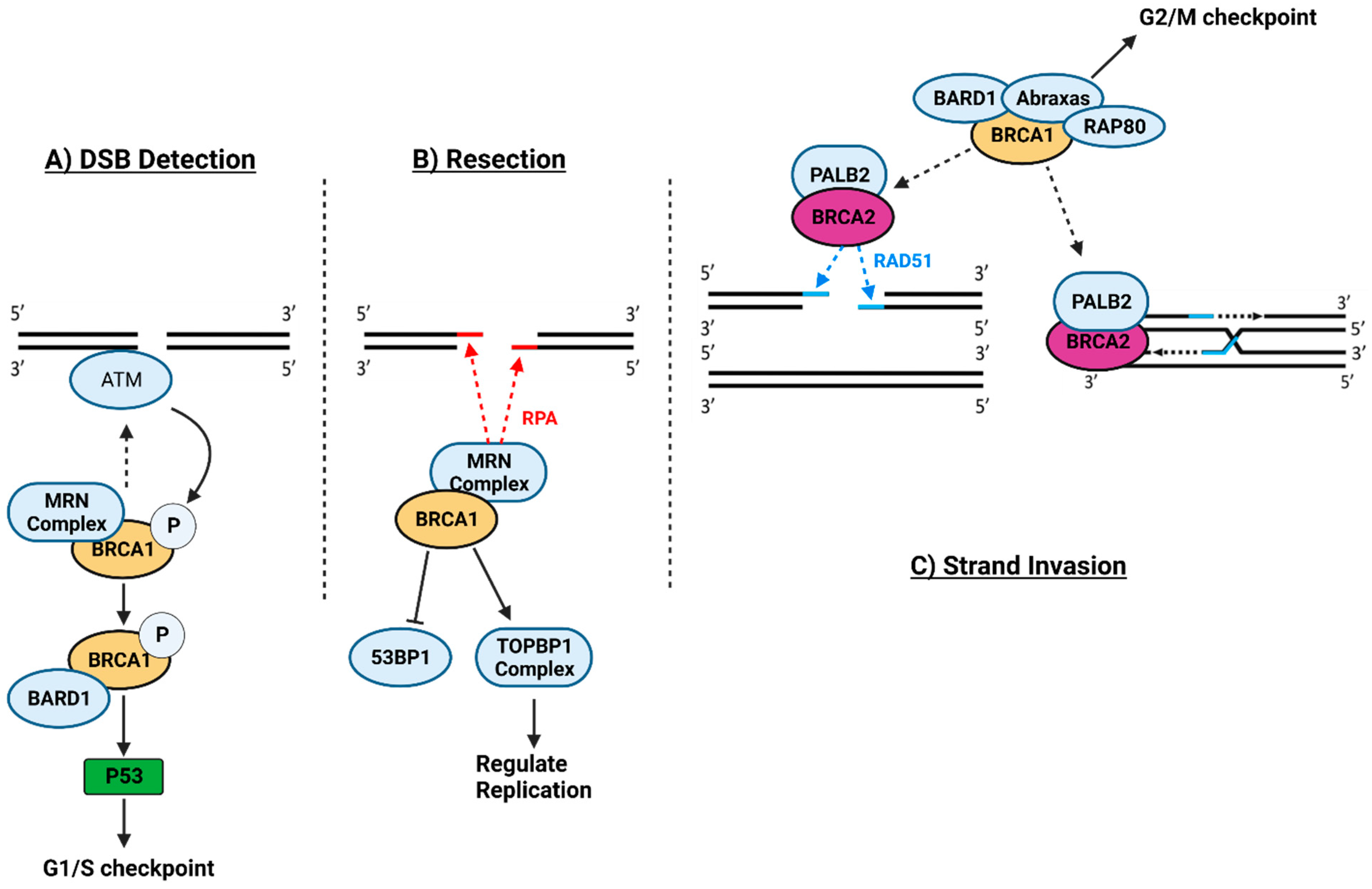
Figure 4.
Comparison between Doxorubicin’s mechanism of cytotoxicity (A) vs. that of loss of BRCA1/2 functions (B). ROS = Reactive oxygen species; RNS = Reactive nitrogen species; NOX = NADPH oxidase; NOS = Nitric oxide synthase; XO = Xanthine oxidase; NRF2 = Nuclear factor erythroid 2-related factor 2; Topo2A/B = Topoisomerase 2A/B; BRCA = Breast cancer gene; TNFa = Tumor necrosis factor alpha.
Figure 4.
Comparison between Doxorubicin’s mechanism of cytotoxicity (A) vs. that of loss of BRCA1/2 functions (B). ROS = Reactive oxygen species; RNS = Reactive nitrogen species; NOX = NADPH oxidase; NOS = Nitric oxide synthase; XO = Xanthine oxidase; NRF2 = Nuclear factor erythroid 2-related factor 2; Topo2A/B = Topoisomerase 2A/B; BRCA = Breast cancer gene; TNFa = Tumor necrosis factor alpha.
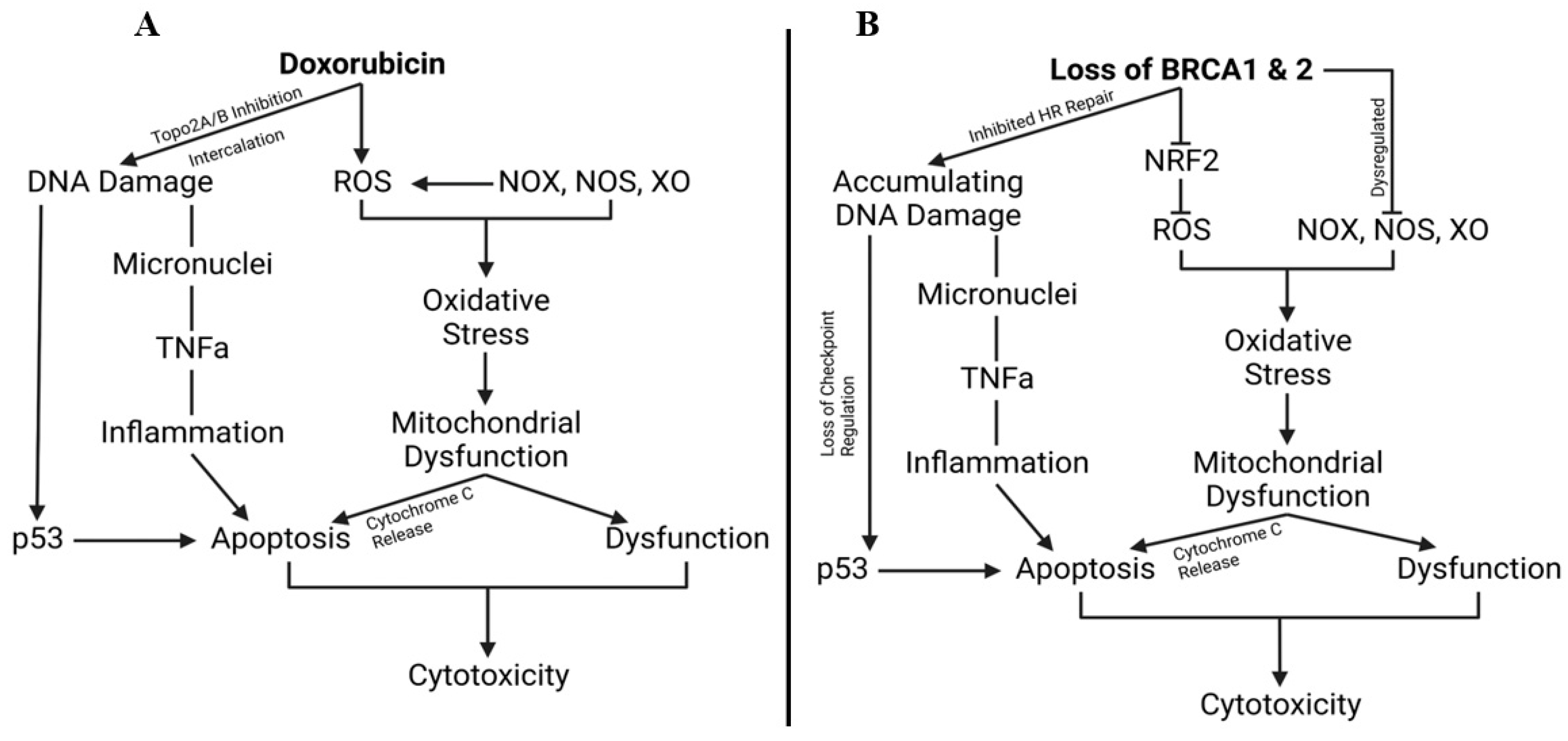
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



