Submitted:
19 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
Background
The incidence of congenital cholesteatoma (CC) has rarely been discussed, particularly from the demographic viewpoint. Therefore, we conducted an epidemiological study of CC using local medical characteristics.
Materials and methods
The participants were 100 patients (101 ears) who underwent initial surgical treatment at university hospitals in two rural prefectures between 2006 and 2022. Sixty-eight percent of the patients were males and 32% were females, with a median age of 5 years. We reviewed the medical records for the date of birth, date of surgery, stage of disease, and first symptom of the disease.
Result
The total incidence of CC was calculated to be 26.44 per 100,000 births and tended to increase. No significant difference was found between the incidences in the two prefectures. The number of surgeries performed was higher in the second half of the study period. No difference in the stage of progress was observed based on age.
Conclusion
The incidence of CC was estimated to be 26.44 per 100,000 new-born births. The number of patients with CC has tended to increase; however, this can be attributed to an increase in the detection rate rather than the incidence.
Keywords:
congenital cholesteatoma
; epidemiology
; incidence
Introduction
Congenital cholesteatoma (CC) is a white retrotympanic mass associated with a normal tympanic membrane without a history of otorrhea, perforation, or otologic surgery [1]. The incidence of various congenital diseases has been demonstrated in epidemiological studies; however, the incidence of CC has rarely been discussed, even though it is a congenital disease. Some reports mention the incidence, in which the comparison and ratio with the number of surgeries performed have been discussed for acquired cholesteatoma [2,3,4]. Therefore, we aimed to study the epidemiology of CC in Japan based on the demographics.
Materials and Methods
This study was approved by the ethics committees of the Oita University and Miyazaki University (approval number: 2487).
A total of 101 ears of 100 patients who underwent initial surgical treatment for CC at the Oita and Miyazaki University Hospitals between January 2006 and December 2022 were recruited for this retrospective study. The participants were limited to those born in the respective prefecture. We reviewed the medical records for age, sex, laterality, date of birth, date of surgery, disease stage, and first symptoms of the disease. Disease was diagnosed based on the 2015 JOS classification criteria [5]. This study comprised 69 males (68%) and 31 females (32%). Regarding the affected side, 51 ears were in the right ear and 50 ears were in the left. Mean age of patients at the surgery was 6.7±4.6 years and median age was 5 years.
These participants were analyzed regarding the following items.
1. Incidence of CC per newborn births
The number of newborn births per year in Oita and Miyazaki Prefectures was obtained from the data available on their websites (https://www.pref.oita.jp/uploaded/attachment/2008926.pdf, https://statdb.me/births/45000/). In this incidence analysis, the lag between birth and surgery may have compromised the accuracy of the results. Therefore, we calculated the incidence in patients born between 2001 and 2017, i.e., 5 years backward with the median age at surgery during this research period. Patients were divided by year of birth from 2001–2017, and the incidence per 100,000 births was calculated for each year. The figures for each prefecture and total incidence rates for both prefectures were also calculated. In addition, the transition of the incidence was analyzed by measuring the correlation coefficients between the number of patients and year of birth.
2. Number of surgeries by year
The number of surgeries performed between 2006 and 2022 was calculated, and the patients’ age at the time of surgery were sorted. Subsequently, changes in the number of surgeries and age at the time of surgery were measured.
3. First opportunity for medical examination
Most patients were suspected to have CC when they initially visited a nearby clinic and were referred to the respective University hospital. Opportunities for medical examinations led to the diagnosis of the disease and were divided into the following four categories:
- Otitis Media: the symptom of otitis media including otalgia and otorrhea.
- Routine examination: A white mass was found on the eardrum by routine examinations when the patient was examined for symptoms other than those of the ear.
- Hearing loss: Patients who became aware of hearing impairment or whose hearing loss was noted during a medical checkup.
- Others.
Four patients with unknown background were excluded.
In addition, the age at that time were also divided into four categories: 0–2 years (before entering kindergarten), 3–5 years (kindergarten), 6–9 years (lower grades of elementary school), and 10 years and above (upper grades of elementary school and above).
4. Disease progression
Disease staging was classified according to the JOS classification criteria [5]. One patient with unknown progression was excluded from the analysis. We also examined the correlation between the age at surgery and disease progression.
Statistical analyses were performed using EZR ver. 1.61 (Saitama Medical Center, Jichi Medical University, Saitama, Japan). Statistical significance was set at p<0.05.
Results
1. Incidence of the CC per newborn births
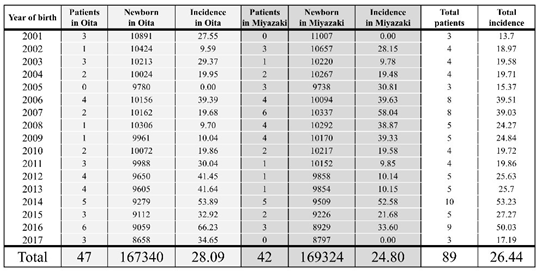
Table 1. shows the number of newborn births, number of patients with CC, and incidence rate per 100,000 newborn births each year. The number of newborn births in both the Oita and Miyazaki prefectures has been declining almost every year, with a 20% decrease from 2001–2017. Forty-seven patients with CC were born in the Oita Prefecture and 42 in the Miyazaki Prefecture during this period. The mean incidence rate per 100,000 newborn births was 28.09 and 24.80 in the Oita and Miyazaki Prefectures, respectively. Consequently, the total disease incidence rates in both prefectures during the study period was calculated to be 26.44. There was no statistically significant difference in incidence rates between the two prefectures (p=0.414). There was a significant positive correlation between the year of birth and total disease incidence. Spearman’s rank correlation coefficient was 0.53 (p=0.03) (Figure 1). Therefore, its incidence increased from 2001–2017.
Each point represents the incidence of patients born in that year. These values are significantly positively correlated (R=0.53, P=0.03), indicating trend in incidence over this period.
2. Number of surgeries by year
During the study period, the total number of surgeries performed at the two facilities ranged from 1–11 per year (Figure 2). Comparing before and after 2014, the number of surgeries in each year was significantly higher in the latter half (p<0.001). Patients’ age at surgery ranged from 1–25 years. Figure 3 shows the patients’ age divided by the year of surgery during the study period. There was no significant correlation between the year of surgery and mean age of patients (R > -0.1, p= 0.099). Five of the relatively older patients (12–25 years) had ossicular malformations. The age at the time of surgery of cases with ossicular malformations were significantly higher than in those without (p<0.01).
The number of surgeries increased significantly in the latter half of the period, starting in 2014.
Each point represents patient’s age who underwent surgery in that year. There was not any correlation between the two items. (R >-0.1, P=0.099)
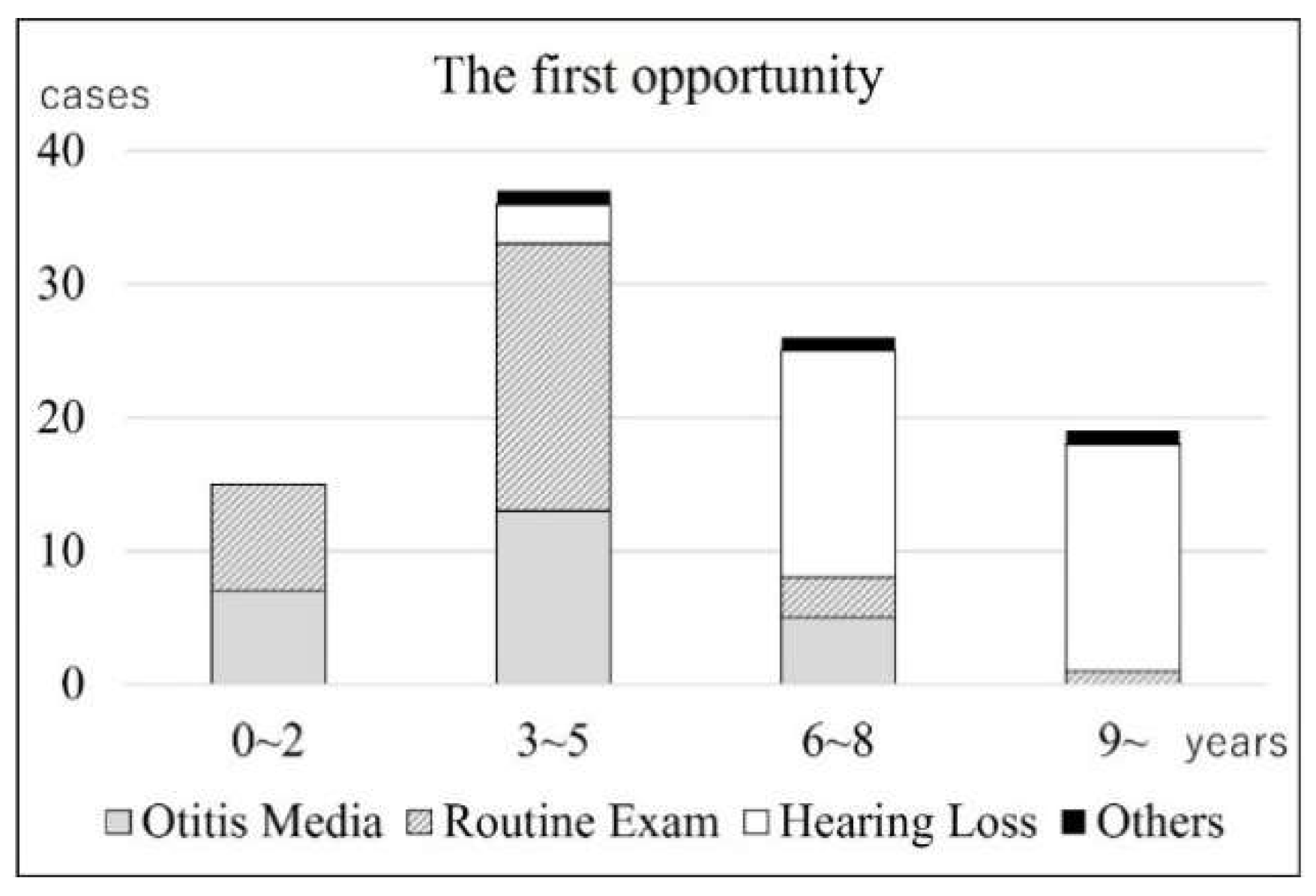
3. First opportunity for medical examination (Figure 4)
Of the 97 ears, 25 (25.8%) had otitis media, 32 (33.0%) underwent routine examination, 37 (38.1%) had hearing loss, and 3 (3.1%) had other reasons as the first opportunity for the diagnosis of CC. Before entering elementary school, otitis media and routine examination accounted for most cases (92.3%); however, after entering elementary school, most cases were due to hearing loss (75.6%). In addition, the proportion of cases due to hearing loss increased further with age (89.5%). The other cases were found incidentally on computed tomography images.
In the age group under 5 years, otitis media and routine examination were most common, but in the age group 6 years and above, hearing loss was the most common.
Figure 4.
The first opportunity for medical examination.
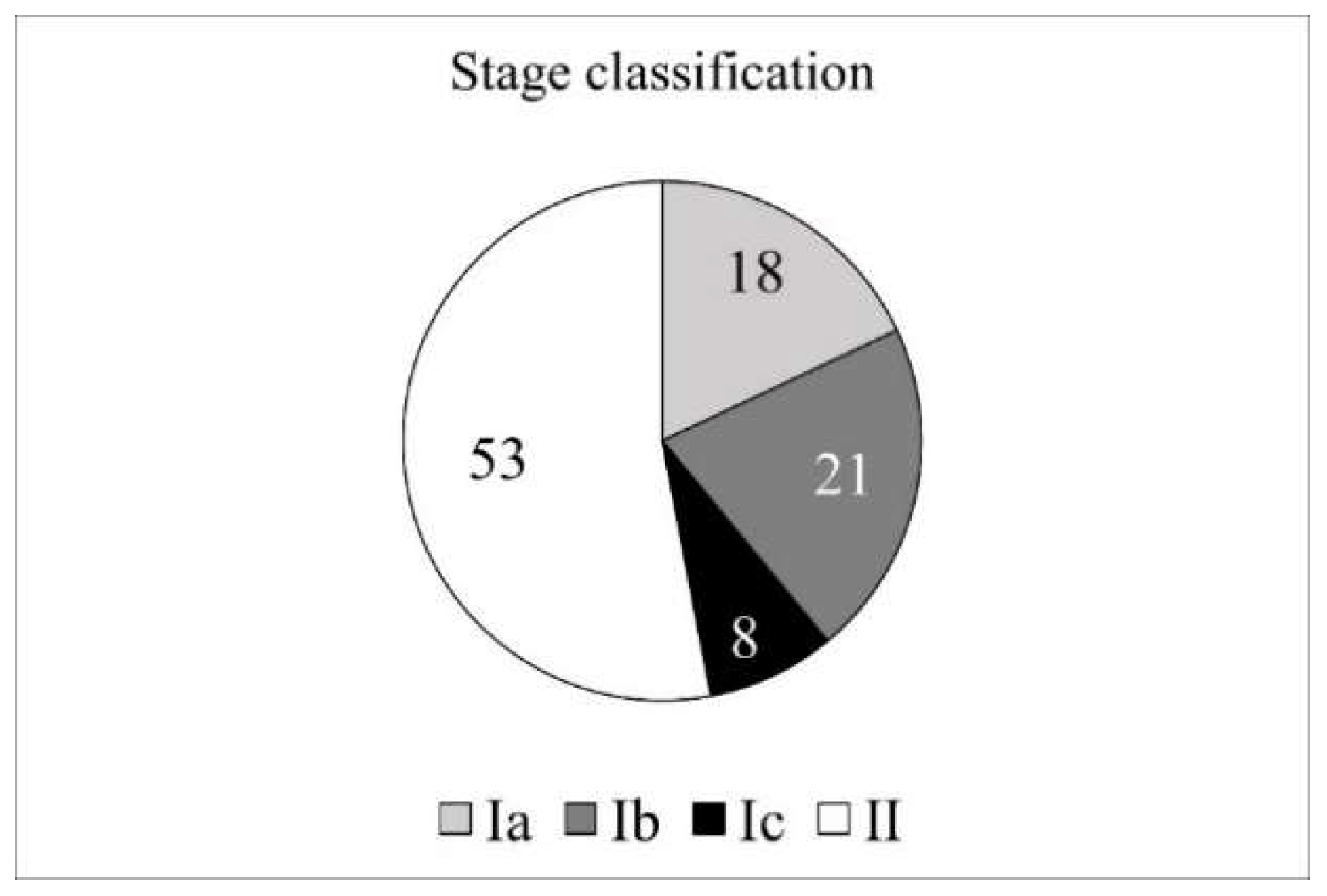
4. Disease progression (Figure 5)
Fifty-seven ears were classified as stage I (Ia, 18 ears; Ib, 21 ears; Ic, 8 ears), and 53 ears as stage II. No cases were classified as stage III (inner ear or facial nerve complications) or IV (intracranial complications). The average age by stage was 6.8 years for stage Ⅰ and 6.6 years for stage Ⅱ, with no significant difference between the two groups (p=0.39).
Stage classification by JOS staging system. There were no stage Ⅲ and Ⅳ cases.
Figure 5.
Stage classification.
Discussion
Komori [2] reported that CC accounted for 13% of all cholesteatoma cases, including adult cases, in a Japanese nationwide study, and Kazahaya [4] reported that CC was 2–5% of all cholesteatoma cases. Denoyelle [1] reported that the proportion of CC in pediatric cholesteatoma is 1–5%. However, these numbers cannot be used directly to estimate the incidence of CC, as there seems to be a difference in the rate of surgical treatment between congenital and acquired cases. Kazahaya reported that it was difficult to determine the actual incidence of CC [4]. As mentioned above, the reason for the difficulty in discussing the incidence of CC is that it is impossible to examine the tympanic membrane of all newborns, and there are no other screening methods, such as blood tests or hearing screening. Only Tos [6] reported the incidence of CC using demographic statistics. As there were 13 cases over 30 years of age in the medical field of 350,000 people, he calculated the annual incidence rate to be one case per one million people. The Oita and Miyazaki Prefectures are neighbors located in the eastern area of Kyushu Island, Japan. Each prefecture contains 1% of the national population, and can be depicted as ‘rural areas’ in Japan. In addition to geographical proximity, both prefectures are rural areas with little population movement and have a medical system in which all patients with CC are concentrated at the only university hospital in the prefecture. We conducted this study focusing on the fact that this ‘closed’ environment is even more advantageous for epidemiological investigations of CC.
Regarding the demographics of the participants, 68% were males and 32% were females. The male-to-female ratio was 2:1 in both Japanese nationwide research [2,7] and a systematic review of English literature [8], which was similar to the ratio in our study, with a predominance of males. The average age of the patients at surgery (6.7 years) was almost the same as that in the systematic review [8] (6.6 years). The average age in the nationwide research [7] was higher at 8.2 years, but the median age was 6.0 years, suggesting that some adult patients included in the study may have elevated the average age.
The incidence of CC was calculated to be 26.44 cases per 100,000 newborn births. No significant difference existed between the incidence in each prefecture (Oita: 28.09; Miyazaki: 24.80) ensuring the reliability of these values. There was a significant positive correlation between the year of birth and incidence from 2001–2017, indicating that the incidence has been increasing. However, it is unlikely that the incidence of congenital diseases will increase over such a short period, which is more likely an increase in the detection rate than in the incidence. As Im et al. [9] and Morita et al. [10] mentioned, the development of the ENT endoscopic system and expanding recognition of the disease may have contributed to the elevation of the detection rate. Hence, it is believed that this incidence will reach its upper limit before long or it has already been reached.
According to the calculation method of Tos [6], the combined population of both prefecture was 2.3 million people, and there were 89 patients in the 17 years of the target period, with an annual incidence of 2.3 cases per million population. Although it is uncertain whether there are differences in the incidence of CC among ethnic groups, this number was approximately twice as that reported by Tos. However, his research period was 30 years, starting from 1965, so there may not be a big difference between each result, considering the recent improvement in the detection rate.
Accompanied by an increasing incidence, the number of surgeries performed increased significantly in the latter half of 2014. Denoyelle et al. [1] also reported that the incidence of CC tends to increase with more effective screening. Similar to the incidence, surgery is likely to reach an upper limit. Some reports have pointed out that the age at disease detection is decreasing [9,10]; however, there was no significant change in the age at detection during our study period.
The first opportunity for a medical examination varies with age. Particularly, the proportion of patients with ‘hearing loss’ significantly increased after the patients entered elementary school. There may be individual factors, such as the patients becoming less susceptible to otitis media or becoming more aware of their own hearing loss as they grow up, and the disease factor, which is the progression of hearing loss accompanied by the growth of cholesteatoma. Morita et al. [10] reported that 52% of patients had a lesion during routine examination of their ears, and 42% were informed of hearing loss during their medical examinations. Gilberto et al. [8] reported that 34% of patients were asymptomatic, 26% had hearing loss, and 23% had a history of otitis media with effusion or acute otitis media. As mentioned above, in addition to individual and disease factors, school screening can be a major factor in disease detection, and its importance has been emphasized.
In this staging study according to the JOS classification criteria, 47% were stage I, 53% were stage II, and there were no cases of stage III or IV neurological or intracranial complications. This is almost similar to that reported by Morita et al. [7] (stage I, 46%; stage II, 52%; and stage III, 2%), and the complication rate is lower than that of acquired cholesteatoma. Kazahaya [4] and Gilberto [1] reported that cholesteatoma size increased and staging progressed with patient’s age according to the Potsic classification [11]. However, no relationship between disease progression and patient's age was observed in this study. This may be due to the difference between the JOS and Potsic classifications.
A limitation of this study is that some patients may not have been included; for example, patients who moved out before being diagnosed (since this study was conducted in a rural area, there must be more people moving out than moving in), patients who were referred to hospitals in other larger cities, and patients whose disease progressed undiagnosed and could no longer be distinguished from acquired cholesteatoma. In addition, there have been reports of cases in which CC disappeared spontaneously [12]; therefore, there is a possibility that latent patients may be cured without being diagnosed or treated. In any case, the calculated incidence of CC may be considered lower than the actual number, as the number of cases may be underestimated but not overestimated.
Conclusion
We conducted a research on the epidemiology of CC utilizing the characteristics of the medical system in rural areas. The incidence of CC was 26.44 per 100,000 newborns. The incidence of CC tended to increase; however, more precisely, it can be considered as an increase in the detection rate. This number is expected to reach a plateau in the near future. Further, hearing loss accounted for most opportunities for medical examinations after entering elementary school.
Author Contributions
Conceptualization, Y.K.; Methodology, Y.K.; Validation, S.I., T.N. and T.O.; Formal Analysis, H.S. and T.H.; Investigation, S.I. and T.O.; Resources, S.I. and T.N.; Data Curation, Y.K. and S.I.; Writing – Original Draft Preparation, Y.K.; Writing – Review & Editing, Y.K. and T.H.; Visualization, Y.K. and H.S.; Supervision, Y.K., K.T. and M.S.; Project Administration, Y.K and T.H.; Funding Acquisition, Y.K, T.H and M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the ethics committees of the Oita University and Miyazaki University (approval number: 2487).
Informed Consent Statement
The requirement for written informed consent from the patients was waived because the study retrospectively used anonymous data from patients’ medical records.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Denoyelle, F.; Simon, F., International Pediatric Otolaryngology Group (IPOG) Consensus Recommendations: Congenital Cholesteatoma. Otol Neurotol 2020, 41 (3), 345-351. [CrossRef]
- Komori, M.; Morita, Y., Nationwide survey of middle ear cholesteatoma surgery cases in Japan: Results from the Japan Otological society registry using the JOS staging and classification system. Auris Nasus Larynx 2021, 48 (4), 555-564. [CrossRef]
- Richards, E.; Muzaffar, J., Congenital Mastoid Cholesteatoma. J Int Adv Otol 2022, 18 (4), 308-314. [CrossRef]
- Kazahaya, K.; Potsic, W. P., Congenital cholesteatoma. Curr Opin Otolaryngol Head Neck Surg 2004, 12 (5), 398-403. [CrossRef]
- Tono, T.; Sakagami, M., Staging and classification criteria for middle ear cholesteatoma proposed by the Japan Otological Society. Auris Nasus Larynx 2017, 44 (2), 135-140. [CrossRef]
- Tos, M., A new pathogenesis of mesotympanic (congenital) cholesteatoma. Laryngoscope 2000, 110 (11), 1890-7. [CrossRef]
- Morita, Y.; Tono, T., Nationwide survey of congenital cholesteatoma using staging and classification criteria for middle ear cholesteatoma proposed by the Japan Otological Society. Auris Nasus Larynx 2019, 46 (3), 346-352. [CrossRef]
- Gilberto, N.; Custódio, S., Middle ear congenital cholesteatoma: systematic review, meta-analysis and insights on its pathogenesis. Eur Arch Otorhinolaryngol 2020, 277 (4), 987-998. [CrossRef]
- Im, G. J.; Han, K., Rate of chronic otitis media operations and cholesteatoma surgeries in South Korea: a nationwide population-based study (2006-2018). Sci Rep 2020, 10 (1), 11356. [CrossRef]
- Morita, Y.; Yamamoto, Y., Pediatric middle ear cholesteatoma: the comparative study of congenital cholesteatoma and acquired cholesteatoma. Eur Arch Otorhinolaryngol 2016, 273 (5), 1155-60. [CrossRef]
- Potsic, W. P.; Samadi, D. S., A staging system for congenital cholesteatoma. Arch Otolaryngol Head Neck Surg 2002, 128 (9), 1009-12. [CrossRef]
- Kodama, K.; Hara, M., Two cases of spontaneous regression of congenital cholesteatomas. Int J Pediatr Otorhinolaryngol 2012, 76 (1), 142-4. [CrossRef]
Figure 1.
The transition in the incidence of CC.
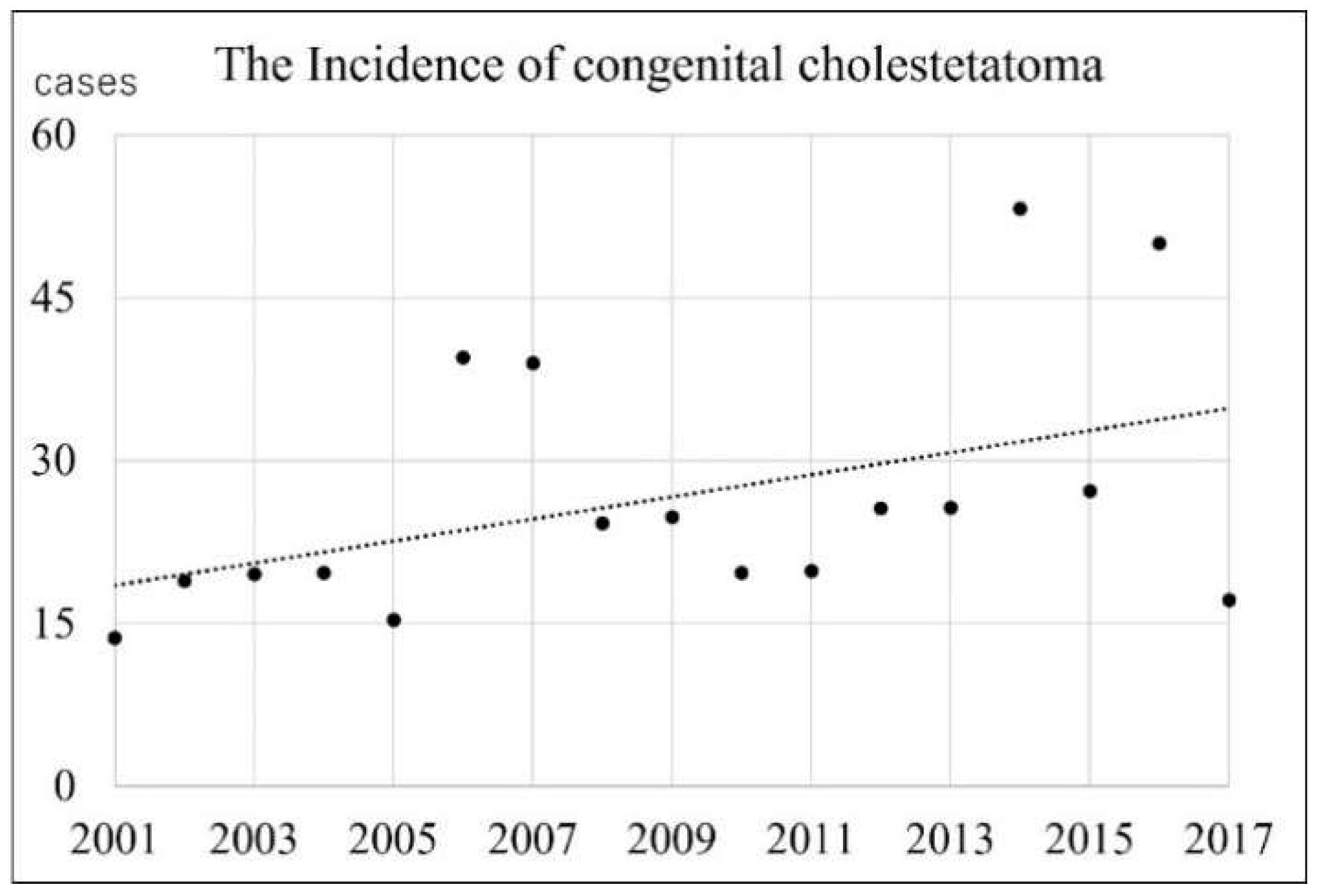
Figure 2.
The number of surgeries by year.
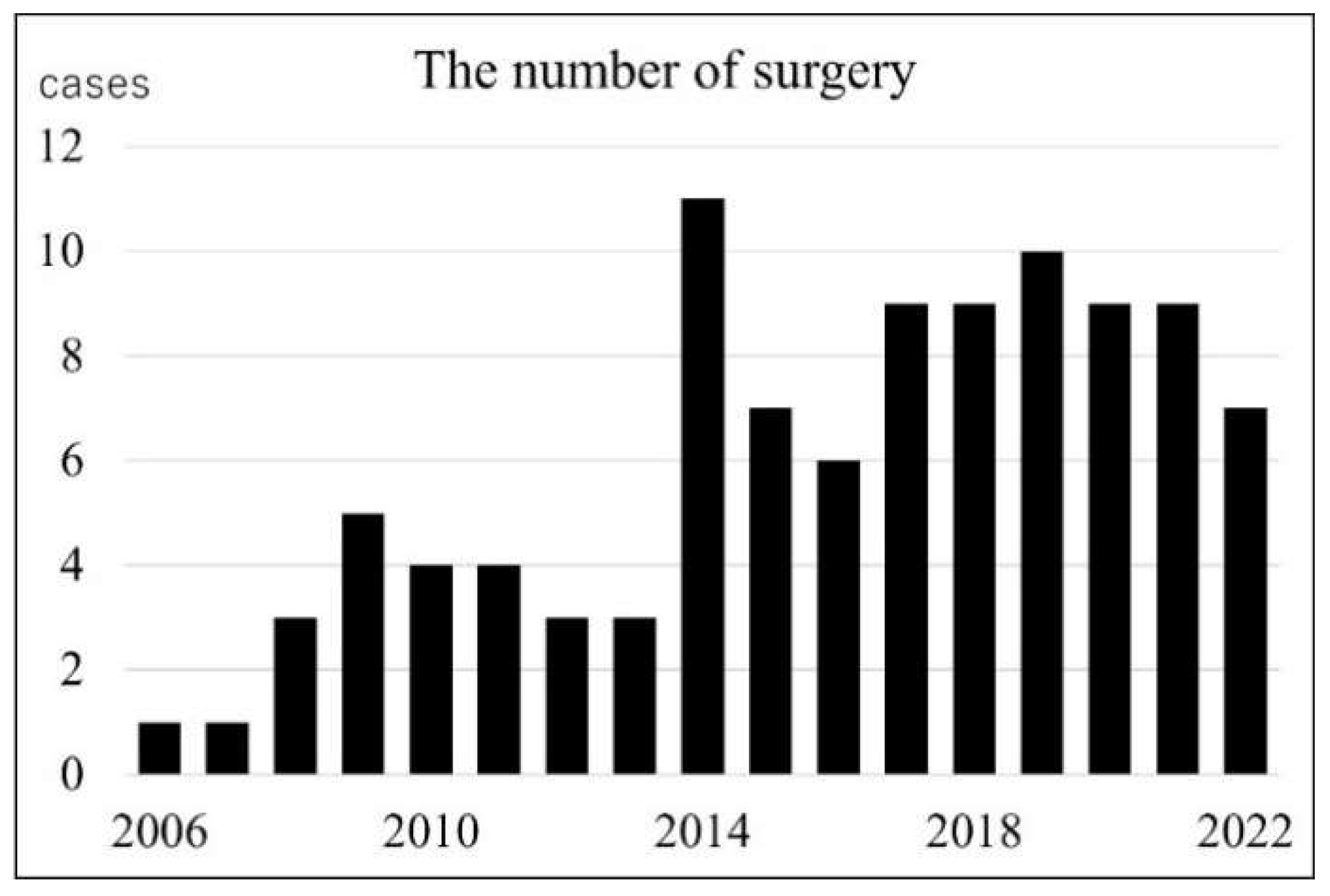
Figure 3.
Patient’s age at the surgery.
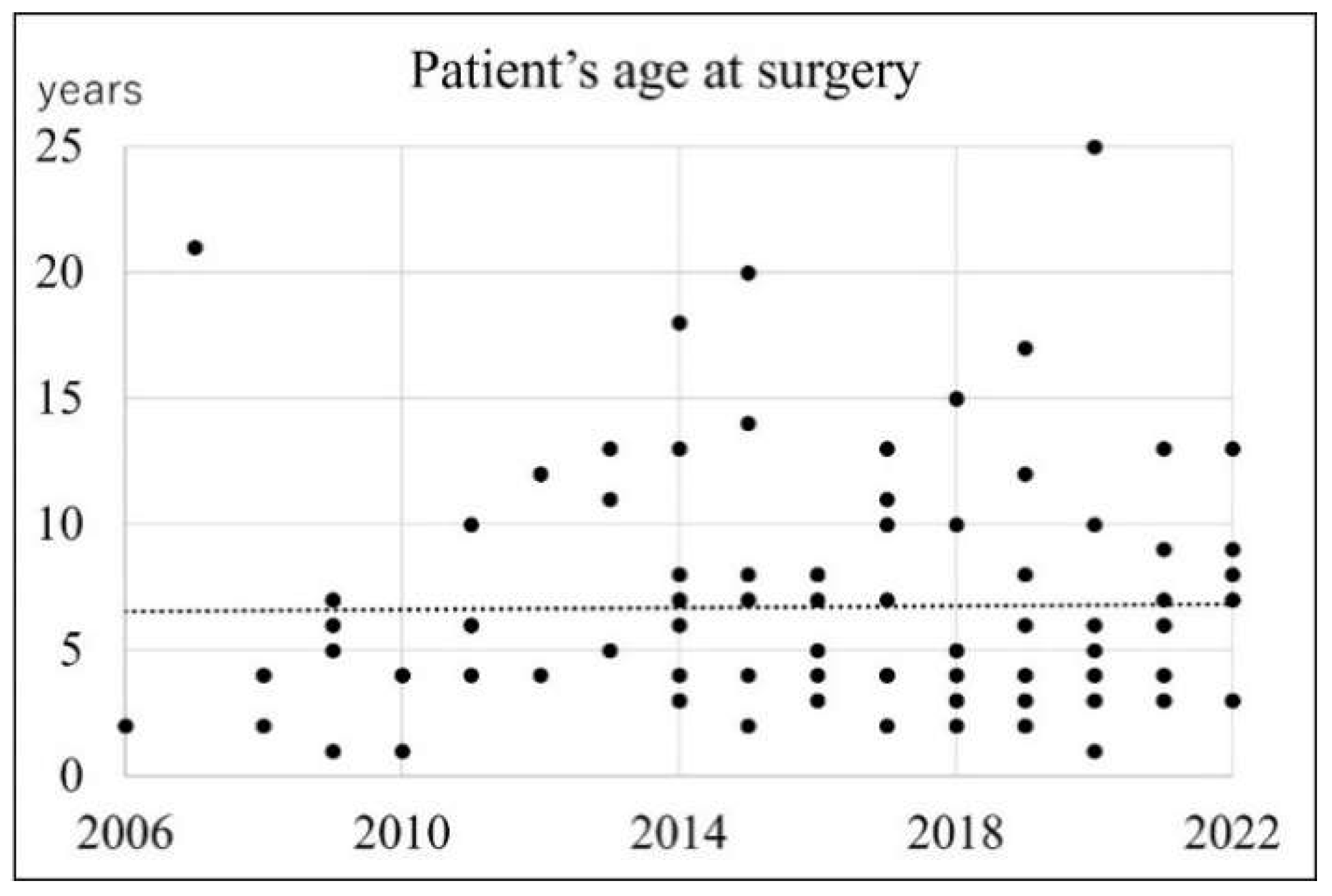

Table 1.
Number of CC patients, newborn births and incidence.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



