
Submitted:
16 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
The use of miniplates for stabilizing bones after orthognathic surgeries, has become increasingly popular for their effectiveness in ensuring stability and promoting swift recovery. However, the post-surgical fate of these miniplates remains a subject of contention among surgeons. Some advocate for their removal, while others suggest leaving them in place. The aims of this study, is to evaluate the incidence, causes, and potential risk factors associated with the removal of miniplates in orthognathic surgeries. A comprehensive meta-analysis was conducted by reviewing studies from various databases like PubMed, Google Scholar, Research Gate, Embase, and Scopus, focusing on publications from 1989 to 2023. Ten studies encompassing a total of 1603 patients which conformed to the inclusion criteria were selected and included in the meta-analysis. With M:F ratio range from 4:1 to 109:141. Total number of miniplates inserted was 5595, and total number of miniplates removed were 294 (5.3%). The most common reasons for miniplates removal were, infection was reported in 161 cases (2.9%), followed by miniplates exposure (34 cases, 0.6%) and palpable plates (23 cases 0.4%). Other indications included pain, patient’s preference, and temperature sensitivity. Relatively less common reasons that resulted in miniplates removal include, sinusitis, second surgery and dental pathology. The mean duration of miniplates removal was 5.5 months with the majority of miniplates (56.1%) were removed from the mandible compared to maxilla. In conclusion, this meta-analysis underscores the importance of miniplate removal in cases where hardware causes diverse complications and physical discomfort. The primary reasons for miniplates removal were infections and plates exposure, with the mandible being the most common site for removal. These findings emphasize the need for continued monitoring to assess the fate of miniplates in orthognathic surgery and provide valuable insights for future clinical decision-making.
Keywords:
Complications
; Orthognathic surgery
; Osteosynthesis
; Miniplate
; Titanium
; Mataanalysis
1. Introduction
Orthognathic surgery, also known as corrective jaw surgery, plays a critical role in the correction of dentofacial deformities and related functional issues. This surgical procedure aims to enhance both the aesthetic appearance and functionality of the patient's face and jaw. Orthognathic surgery has evolved significantly over the years, modern techniques and advances in technology have made orthognathic surgery safer and more precise, with a focus on achieving not only functional but also aesthetic outcomes. Following these procedures, bone segments are immobilized using fixation plates and screws to establish osteosynthesis, with titanium miniplates and screws being the preferred choice [1,2].
Titanium miniplates and screws have become a standard method for rigid fixation in these surgeries. Traditionally, these miniplates were removed after bone healing, often within 3 months of the surgery [3,4,5,6]. Surgeons' opinions on removal varied, with some recommending routine removal and others suggesting it only when necessary. However, the use of titanium, known for its biocompatibility and inertness, has weakened the argument for their routine removal as foreign bodies [3,7,8,9].
The rates of miniplate removal post-orthognathic surgery have been reported with a significant range, between 3.2% and 27.5% [3,8,10,11,12]. Commonly reported reasons for removal include infection, exposure of the miniplate, and patient-reported irritation or discomfort. This wide variation in removal rates can lead to confusion and potentially misleading information for patients during orthognathic surgery consultations and consent processes. Contributing to this variation are factors such as flawed study designs, the amalgamation of orthognathic and trauma surgery data, small or non-consecutive sample sizes, and the involvement of multiple surgeons. Only a limited number of studies have minimized sampling bias by focusing solely on consecutive orthognathic surgery patients. The decision to remove miniplates following orthognathic surgery, once healing has taken place, lacks consensus, primarily due to the associated risks like infection, morbidity, and cost. The aims of this study, is to evaluate the incidence, causes, and potential risk factors associated with the removal of miniplates in orthognathic surgeries and the common complications associated with miniplate removal.
2. Materials and Methods
This study constitutes a systematic review and meta-analysis. We formulated the research protocol by following the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) and registered it under PROSPERO registration number CRD42023399232.
2.1. Eligibility Criteria
Inclusion criteria:
- Full-text available
- Population: patients who underwent orthognathic surgery.
- Intervention: fixation using miniplates.
- Outcome: number/percent of miniplates removed.
- Study design: clinical trials, controlled trials, retrospective studies, and case series.
Exclusion
- Animal or in vitro studies
- Studies not mentioning miniplate numbers.
- Duplicate publication
- Editorial letters, case reports, and review articles.
- Articles without complete demographic information of patient.
- Follow-up less than 12 months.
2.2. Selection of Studies
Initial database search retrieved 239 articles. There were 45 duplicates, and 64 articles were excluded. Remaining 130 articles’ titles and abstracts were scanned, leading to exclusion of 92 articles. Retrieval of the 38 remaining potentially eligible articles was attempted, and only 34 were retrieved. After a second round of full text screening, 10 articles fit the eligibility criteria and were included in this systematic review and meta-analysis (Figure 1).
Data extracted from each selected study such as study population, study design, sample size, age range, gender, number of miniplates placed and removed, site of miniplate placement and removal, type of miniplates, reasons for removal, and duration between insertion and removal.
2.3. Information Sources
Following the guidelines outlined in the PRISMA statement, we conducted an electronic search of various databases, including PubMed, Google Scholar, ResearchGate, Embase, and Scopus. We also performed a search for grey literature using OpenGrey version 1 and manually checked the references in the articles we found. We included studies published from 1989 to 2023 in our meta-analysis.
2.4. Search Strategy
To identify studies related to orthognathic surgery, we used three terms: “corrective jaw surgery”, “orthognathic surgery”, and “jaw surgery”. For plate removal, we employed the following terms: “plate removal”, “plates removal”, “plate failure”, “plates failure”, “titanium miniplates”, “screws”, “complications”, and “removal”. We used Boolean operators: “OR” to broaden the search, and “AND” to combine different areas. The search equations for each database were as follows:
Search strategy for identifying studies in primary electronic databases:
- PubMed: (“corrective jaw surgery” OR “orthognathic surgery”,) AND (“plate removal” OR “plates removal” OR “plate failure” OR “plates failure”)
- Scopus: (“corrective jaw surgery” OR “orthognathic surgery”,) AND (“plate removal” OR “plates removal” OR “plate failure” OR “plates failure”)
- Embase: (“corrective jaw surgery” OR “orthognathic surgery”,) AND (“plate removal” OR “plates removal” OR “plate failure” OR “plates failure”)
- Google Scholar: (“corrective jaw surgery” OR “orthognathic surgery”,) AND (“plate removal” OR “plates removal” OR “plate failure” OR “plates failure”)
- ResearchGate: (“corrective jaw surgery” OR “orthognathic surgery”,) AND (“plate removal” OR “plates removal” OR “plate failure” OR “plates failure”)
The selected studies for analysis were those that reported on the outcomes of using miniplates in orthognathic surgery, including details on complications and removal rates.
2.5. Selection
Two independent reviewers, NA and MH, assessed the titles and abstracts of all the works found in the initial search. If abstracts did not provide sufficient information, the reviewers examined the full text to determine whether to include or exclude the work. They then reviewed the full texts of all remaining articles. Any discrepancies in the results between reviewers were resolved through consensus, and if agreement could not be reached, a third researcher (MJ) was consulted.
2.6. Data Collection Process
We reviewed all research papers centered on the removal of miniplates in patients undergoing orthognathic surgery. Two separate assessors collected the following data from articles meeting the inclusion criteria: author names, publication year, study design, the number of patients and plates inserted, average patient age, gender ratio, the location of miniplate placement (mandible or maxilla), reasons for miniplate removal, and the average follow-up duration in months. To assess the level of agreement between these assessors, the kappa statistic, applying the same criteria used during the study selection phase, was utilized. In cases of discrepancies, the assessors resolved them through discussion. If a consensus could not be reached, a third evaluator (MJ) was consulted to provide an assessment.
2.7. Study Risk of Bias Assessment
The review incorporated 10 articles that met our inclusion criteria, published between 1989 and 2023. We utilized the Newcastle–Ottawa Scale (NOS) to assess the quality of the selected studies, categorizing them as “Good”, “Fair”, or “Poor”. Good quality studies received 3 or 4 stars in the selection domain, 1 or 2 stars in the comparability domain, and 2 or 3 stars in the outcome/exposure domain. Fair quality studies received 2 stars in the selection domain, 1 or 2 stars in the comparability domain, and 2 or 3 stars in the outcome/exposure domain. Poor quality studies received 0 or 1 star in the selection domain, 0 stars in the comparability domain, or 0 or 1 star in the outcome/exposure domain. The resulting classification (Good, Fair, or Poor) reflected the overall study quality, based on these criteria. One study [15] was categorized as “Fair”, while all the remaining studies were deemed to be of “Good” quality, as summarized in (Table 1).
2.8. Statistical Analysis
Data was run through the comprehensive meta-analysis software (CMA-V4). Using the random-effects model to estimate the pooled prevalence and the 95% confidence intervals (CI’s). Heterogeneity among studies was assessed using the Cochran’s Q statistics, I2 statistic, which describes the total variation percentage across included studies due to heterogeneities, as well as the tau square (T2) test.
To further interpret the results of the meta-analysis, we also performed a sensitivity analysis by removing one study at a time and evaluating the impact on the overall results. This analysis helps to assess the robustness of the findings and the potential influence of any individual study on the overall effect estimate. The sensitivity analysis showed that the overall effect estimate was not significantly affected by the removal of any individual study. The results remained consistent, and the effect size was within the range of the overall estimate.
Additionally, we assessed the heterogeneity of the included studies using a chi-squared test and the I-squared statistic. The chi-squared test result was significant (p<0.001), indicating significant heterogeneity among the studies. To explore the possible sources of heterogeneity, we conducted a subgroup analysis based on the type of indication for plate removal.
3. Results
A total of 239 articles were identified, of which 229 were excluded, 10 remaining articles satisfied our inclusion criteria and were included in our review (Figure 1). A risk of bias assessment was done following New Castel Ottawa Scale (Table 1).
Ten studies were included in the meta-analysis, and a total of 1603 patients were assessed. With M:F ratio range from 4:1 (O’Connell et al, [6]) to 109:141 (Ulker et al, [18]). Most of the studies were retrospective in nature, with the largest study including 533 patients (Alpha et al., [2]) (Table 2). Total number of miniplates inserted was 5595, and total number of miniplates removed were 294 (5.3%). The most common reasons for miniplates removal were, infection was reported in 161 cases (2.9%), followed by miniplates exposure (34 cases, 0.6%) and palpable plates (23 cases 0.4%). Other indications included pain (19 cases, 0.3%), patient’s preference (16 cases, 0.3%), and temperature sensitivity (14 cases, 0.2%). Other relatively less common reasons that resulted in miniplates removal include, sinusitis, second surgery and dental pathology (Table 3).
The duration of miniplates removal varies between studies, with some authors reporting a mean duration of 5.5 months, while others reported up to 72 months. For example, Theodossy et al. [11] reported a mean duration of 5.5 months, while Cubuk et al. [17] reported a mean duration of 6 years.
The site of miniplates removal also varied, with some studies reporting a higher incidence of removal in the mandible (147 6.5%), compared to the maxilla (115 4.5 (Table 4).
Meta-analysis of the selected articles:
The analysis is based on ten studies. The effect size index is the event rate. The random-effects model was employed for the analysis. The studies in the analysis are assumed to be a random sample from a universe of potential studies, and this analysis was used to make an inference to that universe. The mean effect size is 0.053 with a 95% confidence interval of 0.036 to 0.078. The mean effect size in the universe of comparable studies could fall anywhere in this interval. The I-squared statistic is 90%, which indicate that some 90% of the variance in observed effects reflects variance in true effects rather than sampling error (Table 5). The meta-analysis revealed the odds in favor of removing miniplates is 0.053 times the odds in favor of retaining miniplates (Figure 2). The terms "Favors Retention" and "Favours Removal" imply that lower event rates may be preferable for retention, while higher rates favor removal.
The funnel plot, which measure the study size (usually standard error or precision) on the vertical axis as a function of effect size on the horizontal axis. Large studies appear toward the top of the graph, and tend to cluster near the mean effect size. Smaller studies appear toward the bottom of the graph, and (since there is more sampling variation in effect size estimates in the smaller studies) will be dispersed across a range of values (Figure 3).
Miniplates removal in the Mandible and the Maxilla
This analysis is based on five studies. The effect size index is the odds ratio (OR). The random-effects model was employed for the analysis. The studies in the analysis are assumed to be a random sample from a universe of potential studies, and this analysis was used to make an inference to that universe.
The Q-statistic provides a test of the null hypothesis that all studies in the analysis share a common effect size. The Q-value is 5.873 with 4 degrees of freedom and p = 0.209. Using a criterion alpha of 0.100, we cannot reject the null hypothesis that the true effect size is the same in all these studies (Table 6). The meta-analysis revealed the odds in favor of removing miniplates in the mandible is 2.169 times more than the odds in favor of removing miniplates in the maxilla with acceptable heterogeneity of 32% based on I-squared statistics (Figure 4).
The forest plot also suggests that, on average, the event rate for miniplates removal is low, with both fixed and random-effects models showing less than 10% of such events, which statistically favors retention of the miniplates.
4. Discussion
The utilization of miniplates for stabilizing bones has gained popularity due to their efficacy in achieving stability and promoting swift recovery, but they present several challenges. These include growth inhibition, the palpable presence of plates and screws, difficulties with imaging and radiotherapy, temperature sensitivity, titanium particle dispersion in lymph nodes, bone stress due to the system's rigidity, and a potential risk of causing genetic mutations. Consequently, about one-third of these systems are removed, leading to increased costs and additional burdens [1,2,3,4,5,6,7,8].
In this study, we evaluated a total of 1603 patients spanning different age groups, with a predominance of female participants. 5595 miniplates were inserted in mandible and maxilla, and we observed a 5.3% incidence of miniplate removal following orthognathic surgeries.
The selected ten studies were conducted in various countries, potentially reflecting divergent healthcare practices and patient demographics. The inconsistency in literature regarding the influence of patient age on the necessity for miniplate removal suggests a complex interplay of factors that may impact surgical outcomes [11,19]. In this study, we found higher removal rates among patients under 40 years old, differing from other reports that indicated higher removal rates among those under 30 years old [11,13,19].
We observed gender-based differences, with females more likely to have miniplates removed. This may be due to behavioral or physiological differences affecting post-surgical recovery and the need for further procedures. Manor et al. suggested that this might be due to females more readily seeking medical attention for symptoms like pain, sensitivity, and palpability [19].
This study didn't analyze the impact of medical comorbidities on miniplate removal due to insufficient details in the selected studies, highlighting the need for more comprehensive research. The strong advice against smoking before orthognathic surgery is based on the increased infection risk in smokers, who are significantly more likely to need miniplate removal [11,12,19,20]. This finding underscores the importance of adhering to preoperative instructions to reduce post-surgical complications and ensure optimal healing.
In this study, infection and exposure of miniplates emerged as the most prevalent causes for their removal, aligning with findings from other studies that also pinpoint infection as the leading reason for miniplate extraction [2,3,11,12]. Miniplates, situated in the sensitive submucosal tissues, are vulnerable to external trauma and masticatory forces. These factors can destabilize the miniplates, leading to screw loosening, inflammation, and heightened infection risk. Additionally, improper suturing techniques and insufficient bone cooling during the preparation of screw holes have been associated with miniplate failures due to infections [2,3,11,12].
Variations in other reported reasons for miniplate removal across different studies [2,3,6,8,9,10,11,12,13], like pain, plate exposure, growth restriction, and prosthetic rehabilitation needs, reflect the complex nature of orthognathic surgeries. These variations emphasize how patient-specific factors influence the decision to remove plates. Moreover, these differences highlight the critical need for comprehensive patient evaluations and tailored approaches in these surgical procedures [1,6,21,22,23].
Infections associated with miniplates can arise from oral cavity bacteria or from improper sterile practices during surgery. Sometimes, these infections are linked to dental damage during the fixation procedure or a reduced blood flow in the mandible. However, if the infection does not involve the bone, it's possible to retain the miniplates by administering antibiotics, excising infected tissue, and tackling the infection's root cause. Studies suggest that smaller plates can become reservoirs for bacteria, leading to persistent inflammation and discomfort, indicating an increased risk of infection the longer a plate is left in the body [21,22,23]. In research conducted by Alpha et al. [2], 6.5% of the plates (70 out of 1066) were removed due to symptoms like erythema, fistula, granulation tissue, hematoma, or wound dehiscence, which were categorized as "disturbances in healing". Similarly, Mohamed et al. [16] noted plate removals due to infection, with patients displaying various signs like sinus tracts, localized swelling, sinusitis, and superficial infections. Theodossy et al. [11] observed a 15.6% removal rate, with all the removed plates being attributed to infections, manifesting as pain, swelling, wound dehiscence, and pus discharge.
While titanium-based alloy miniplates are generally recognized for their benefits in osteosynthesis, uncertainties persist regarding their long-term effects. Recent research has focused on evaluating the tissue around removed titanium materials to assess potential impacts. Although removal of titanium devices has mainly been limited to cases of infection or exposure, concerns exist about the local cellular effects of metallic particles, which can infiltrate nearby tissue and even migrate through the lymphatic system to other organs. Studies have indicated local reactions and immune-inflammatory responses in fibrous connective tissue deposits, with titanium inducing oxidative stress and allergic reactions, moreover, instances of facial eczema have been reported [24,25,26].
In our study, pain accounted for 0.3% (19 cases) of miniplate removals. Retained miniplates might cause discomfort or pain, particularly when situated near facial muscles, nerves, or tendons. Such discomfort can significantly impact the patient's quality of life, especially if the miniplate is visible, such as in the cheek or jawbone [27]. Pain can arise from various sources, including nerve damage, plate migration, or cold intolerance. In a study by Brown et al. [13], several patients complained of pain in the area surrounding the plates placed, and symptom relief occurred when the plates were removed (4%). Similarly, Little et al. [10] reported that patients who complained of pain did not have an associated infection or plate exposure to explain the pain, and 4 plates were removed in their study due to pain. Schmidt et al. [15] found that pain was the most common reason for removal in their study, either occurring alone or with other symptoms.
Miniplates can sometimes be visible under the skin or cause scarring, raising cosmetic concerns for certain patients and prompting them to opt for removal. Plate exposure occurs when the miniplate becomes visible through the skin or mucosa due to inadequate wound closure, insufficient tissue coverage, or suboptimal plate positioning. Cheung et al. [14] found that plate exposure rates for titanium miniplates were 1.02%, with 2 plates removed due to exposure, mainly in the posterior maxilla and mandibular premolar region, attributed to the thin mucosa and Le Fort I cut. Mohamed et al. [16] indicated that the primary reason for removal was plate exposure (11 out of 31 plates), with no pain or infection accompanying the exposure. Schmidt et al. [15] found that plates placed in the maxillary buttress region were removed due to palpation. They recommended using lower-profile plates in these regions to reduce palpability and suggested the use of absorbable plates as an alternative. Sinusitis may occur as a rare complication following Le Fort I osteotomy, related to disturbance of sinus mucosa due to plate placement, as reported by Schmidt et al. [15]. Little et al. [10] and Ulker et al. [18] reported only 1 and 2 plates removed due to sinus infection, respectively.
Other reported reasons for miniplates removal includes, prosthetic rehabilitation involving dental implants, miniplate fractures resulting from improper plate placement or excessive stress, loose fixation devices due to suboptimal plate placement, improper screw positioning, patient requests, poor aesthetics, nerve impairment, and cancer concerns. Some studies also reported patients experiencing temperature sensitivity in the region around the plates, particularly intolerance to cold. For example, Cubuk et al. [17] described patients experiencing discomfort during cold weather, leading to plate removal for symptom relief and Cubuk et al. [17] documented cases of patients requiring the removal of maxillary plates as they were undergoing additional surgical procedures like rhinoplasty and a sinus lift.
The timing of miniplate removal varies, with most cases occurring within one year of initial surgery. Existing literature suggests that removals often happen between 6 months and 1-year post-fixation, with some cases even removed within less than 3 months. Typically, miniplates are removed after confirming bone healing, usually within 6 months to a year. The varied range of removal times identified in this study is influenced by patient-specific factors, fracture characteristics, surgical techniques, healing rates, and potential complications. Customized patient care and continuous assessment are essential for determining the optimal removal timing. Operating time as a risk factor remains debated, with extremes of less than 100 and over 190 minutes cited as increasing risks [9]. Shorter times might indicate rushed surgeries with poor miniplate placement, while longer times could mean prolonged exposure to oral microflora [10,19].
The majority of miniplates (56.1%) were removed from the mandible. The mandible's relatively dense cortical bone structure and the risks associated with surgical interventions likely contribute to this pattern. Additionally, the intraoral mucosa's thickness during surgical approaches increases the likelihood of plate exposure. In the case of the mandible, which endures greater biomechanical forces than the maxilla [27,28], issues such as screw loosening and inflammation are more prevalent, especially in osteotomies lacking interfragmentary stability [29]. The distinct vascular supply and structure of the mandible can also impact the effectiveness of these fixation systems [29].
Gareb and co-workers [29] compared the long-term clinical performance of titanium and biodegradable plates in fixation of maxillary, mandibular, and bimaxillary osteotomies and concluded that there were no notable differences in the frequency of symptomatic plates removal among these types. But, there was a tendency to prefer biodegradable osteosyntheses for maxillary osteotomies, while titanium systems were more common for mandibular and bimaxillary osteotomies. This suggests that biodegradable options might be more appropriate for maxillary osteotomies, potentially due to lower symptomatic plates removal rates. Future research considerations might include the impact of factors like skeletal movement distances, oral hygiene, and proximity to incision sites on miniplates removal. Likewise, Ueki et al, [30] from a randomized controlled trial reported that 25% of patients with titanium osteosyntheses developed issues with TMJ-function a year after surgery, with some experiencing long-term mandibular function impairment, thus, future studies are advised to include TMJ-function evaluations using validated questionnaires for a thorough assessment.
Cost considerations also play a significant role in the question of whether to remove miniplates after orthognathic surgery healing, with substantial variations in removal costs among different countries. Van Bakelen et al. [31] conducted a randomized controlled trial (RCT) and assessed the overall financial burden on patients admitted for titanium miniplates removal and found that the average total costs were significantly high at the 2-year follow-up mark. These costs were attributed to a range of factors including perioperative expenses, costs of additional medical procedures, travel expenses, and the economic impact due to absence from work. This detailed cost evaluation offers a broader understanding of the economic impact associated with the use of titanium osteosynthesis systems in orthognathic surgeries.
Despite the systematic approach used in the review, based on registered protocol and adherence to the PRISMA statement, some limitations persisted. The thorough and updated literature search was limited by the inability to retrieve some data, which was not included in the review. This gap underscores the importance of comprehensive data reporting in clinical studies. The heterogeneity observed in the studies was attributed to differences in the types of osteosynthesis systems used, variations in surgical procedures, differences in operative displacement. Therefore, future research is encouraged to follow strict protocols, focusing on well-defined inclusion and exclusion criteria and specific endpoints to minimize reporting bias. Longer follow-up periods are also recommended to better assess symptomatic device removal and skeletal stability. Clear definitions and adherence to indications for device removal are crucial to reduce detection bias.
In conclusion, this meta-analysis underscores the importance of miniplate removal in cases where hardware causes diverse complications and physical discomfort. The primary reasons for miniplates removal were infections and plates exposure, with the mandible being the most common site for removal. These findings emphasize the need for continued monitoring to assess the fate of miniplates in orthognathic surgery and provide valuable insights for future clinical decision-making.
Author Contributions
Conceptualization, M.J., and N.A.; methodology, M.H., N.A., and A.M.E.-A.; formal analysis, M.H. and M.J.; investigation, M.H. and A.M.E.-A.; writing—original draft preparation, N.A. and M.J; writing—review and editing, M.H., A.M.E.-A., and M.J.; supervision, M.J. and M.H.; project administration, M.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Althagafi:, Dr.M.Y. and Korayem, Dr. M. Dentofacial Deformity: Treated with Combined Orthodontic and Orthognathic Surgery Treatment. Saudi J Oral Dent Res 2020, 5, 254–261. [Google Scholar] [CrossRef]
- Alpha, C.; O'Ryan, F.; Silva, A.; Poor, D. The incidence of postoperative wound healing problems following sagittal ramus osteotomies stabilized with miniplates and monocortical screws. J Oral Maxillofac Surg. 2006, 64, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Kuhlefelt, M.; Laine, P.; Suominen-Taipale, L.; Ingman, T.; Lindqvist, C.; Thorén, H. Risk factors contributing to symptomatic miniplate removal: a retrospective study of 153 bilateral sagittal split osteotomy patients. J Oral Maxillofac Surg. 2010, 39, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Champy, M.; Loddé, J. P.; Schmitt, R.; Jaeger, J. H.; Muster, D. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J Oral Maxillofac Surg. 1978, 6, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Cawood J., I. Small plate osteosynthesis of mandibular fractures. Br J Oral Maxillofac Surg. 1985, 23, 77–91. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.; Murphy, C.; Ikeagwuani, O.; Adley, C.; Kearns, G. The fate of titanium miniplates and screws used in maxillofacial surgery: A 10 year retrospective study. Int. J Oral Maxillofac Surg. 2009, 38, 731–735. [CrossRef]
- Jaber, M.; Abouseif, N.; Ibrahim, N.; Hassan, M.; El-Ameen, A.M. Reasons for Removal of Miniplates Used in Fixation of Maxillofacial Bone Fractures: Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 11899. [Google Scholar] [CrossRef]
- Widar, F.; Afshari, M.; Rasmusson, L.; Dahlin, C.; Kashani, H. Incidence and risk factors predisposing plate removal following orthognathic surgery. Oral Surg, Oral Med, Oral Pathol and Oral Radiol 2017, 124, 231–239. [Google Scholar] [CrossRef]
- Posnick, J. C.; Choi, E.; Chavda, A. Method of osteotomy fixation and need for removal following bimaxillary orthognathic, osseous genioplasty, and intranasal surgery: a retrospective cohort study. Int J Oral Maxillofac Surg. 2017, 46, 1276–1283. [Google Scholar] [CrossRef]
- Little, M.; Langford, R. J.; Bhanji, A.; Farr, D. Plate removal following orthognathic surgery. J Cranio-maxillofa Surg. 2015, 43, 1705–1709. [Google Scholar] [CrossRef]
- Theodossy, T.; Jackson, O.; Petrie, A.; Lloyd, T. Risk factors contributing to symptomatic plate removal following sagittal split osteotomy. Int J Oral Maxillofac Surg. 2006, 35, 598–601. [Google Scholar] [CrossRef]
- Cousin, A. S.; Bouletreau, P.; Giai, J.; Ibrahim, B.; Louvrier, A.; Sigaux, N. Severity and long-term complications of surgical site infections after orthognathic surgery: a retrospective study. Sci Reports 2020, 10, 12015. [Google Scholar] [CrossRef]
- Brown, J.S.; Trotter, M.; Cliffe, J.; Ward-Booth, R.P.; Williams, E.D. The fate of miniplates in facial trauma and orthognathic surgery: A retrospective study. Br. J. Oral. Maxillofac. Surg. 1989, 27, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L. K.; Chow, L. K.; Chiu, W. K. A randomized controlled trial of resorbable versus titanium fixation for orthognathic surgery. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, and Endod. 2004, 98, 386–397. [Google Scholar] [CrossRef]
- Schmidt, B. L.; Perrott, D. H.; Mahan, D.; Kearns, G. The removal of plates and screws after Le Fort I osteotomy. J Oral Maxillofac Surg.. 1998, 56, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, N. H.; Murugesan, R.; Soh, C. L.; Singh, J. A 7-Year Retrospective Analysis of Titanium Plates Removal Following Orthognathic Surgery. J Oral Maxillofac Surg. 2022, 21, 743–746. [Google Scholar] [CrossRef]
- Çubuk, S.; Kaya, B.; Bayram, B.; Uckan, S. The prevalence of removal of miniplates used in orthognathic surgery: A retrospective study with long-term follow-up. 7tepeklinik. 2022, 18, 44–49. [Google Scholar] [CrossRef]
- ÜLKER, Ö.; DEMİRBAŞ, A. E.; KÜTÜK, N.; KILIC, E.; Alkan, A. INCIDENCE AND CAUSES OF OSTEOSYNTHESIS TITANIUM MINIPLATE REMOVAL FOLLOWING ORTHOGNATHIC SURGERY. Sağlık Bilimleri Dergisi 2022, 31, 390–394. [Google Scholar] [CrossRef]
- Manor, Y.; Chaushu, G.; Taicher, S. Risk factors contributing to symptomatic plate removal in orthognathic surgery patients. J Oral Maxillofac Surg. 1999, 57, 679–682. [Google Scholar] [CrossRef]
- Kuhlefelt, M.; Laine, P.; Suominen, A. L.; Lindqvist, C.; Thorén, H. Smoking as a significant risk factor for infections after orthognathic surgery. J Oral Maxillofac Surg. 2012, 70, 1643–1647. [Google Scholar] [CrossRef]
- Haraji, A.; Motamedi, M. H.; Moharamnejad, N. Causes and incidence of miniplate removal following Le Fort I osteotomy. Eplasty 2009, 9, e45. [Google Scholar]
- Falter, B.; Schepers, S.; Vrielinck, L.; Lambrichts, I.; Politis, C. Plate removal following orthognathic surgery. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, and Endod. 2011, 112, 737–743. [Google Scholar] [CrossRef]
- Francel, T.J.; Birely, B.C.; Ringelman, P.R.; Manson, P.N. The Fate of Plates and Screws after Facial Fracture Reconstruction. Plas and Recon Surg. 1992, 90, 568–573. [Google Scholar] [CrossRef]
- Riviș, M.; Roi, C.; Roi, A.; Nica, D.; Văleanu, A.; Rusu, L.-C. The Implications of Titanium Alloys Applied in Maxillofacial Osteosynthesis. Appl. Sci. 2020, 10, 3203. [Google Scholar] [CrossRef]
- Thomas, P.; Iglhaut, G.; Wollenberg, A.; Cadosch, D.; Summer, B. Allergy or tolerance: Reduced inflammatory cytokine response and concomitant IL-10 production of lymphocytes and monocytes in symptom-free titanium dental implant patients. BioMed Res. Int. 2013, 2013, 539834. [Google Scholar] [CrossRef]
- Armencea, G.; Gheban, D.; Onisor, F.; Mitre, I.; Manea, A.; Trombitas, V.; Lazar, M.; Baciut, G.; Baciut, M.; Bran, S. Histological Change in Soft Tissue Surrounding Titanium Plates after Jaw Surgery. Materials 2019, 12, 3205. [Google Scholar] [CrossRef]
- Van, Eijden, T. Biomechanics of the mandible. Crit Rev Oral Biol Med. 2000, 11, 123–36. [Google Scholar] [CrossRef]
- Huang, S-F., L,o L-J., Lin, C-L. Biomechanical interactions of different mini-plate fixations and maxilla advancements in the Le Fort I Osteotomy: a finite element analysis. Comput Methods Biomech Biomed Engin 2016,, 19, 1704–1713. [CrossRef]
- Gareb, B., Van, Bakelen., NB., Buijs, GJ., Jansma, J., De Visscher, J. Hoppenreijs, T. et al. Comparison of the long-term clinical performance of a biodegradable and a titanium fixation system in maxillofacial surgery: a multicenter randomized controlled trial. PLoS One 2017, 12, 1–12.
- Ueki, K, Nakagawa, K., Marukawa, K., Takazakura, D., Shimada, M., Takatsuka, S., et al. Changes in condylar long axis and skeletal stability after bilateral sagittal split ramus osteotomy with poly-l-lactic acid or titanium plate fixation. Int J Oral Maxillofac Surg 2005, 34, 627–634. [CrossRef] [PubMed]
- Van, Bakelen, N.B., Vermeulen, K.M., Buijs, G.J., Jansma, J., De, Visscher, J.G.A., Hoppenreijs, T., et al. Cost-effectiveness of a biodegradable compared to a titanium fixation system in maxillofacial surgery: a multicenter randomized controlled trial. PLoS One 2015, 10, 1–16.
Figure 1.
PRISMA flow diagram.
Figure 2.
Forest plot of all selected studies showing the event rate of miniplates removal in both maxilla and mandible.
Figure 2.
Forest plot of all selected studies showing the event rate of miniplates removal in both maxilla and mandible.
Figure 3.
Funnel Plot of all selected studies showing the event rate of miniplates removal in both maxilla and mandible.
Figure 3.
Funnel Plot of all selected studies showing the event rate of miniplates removal in both maxilla and mandible.
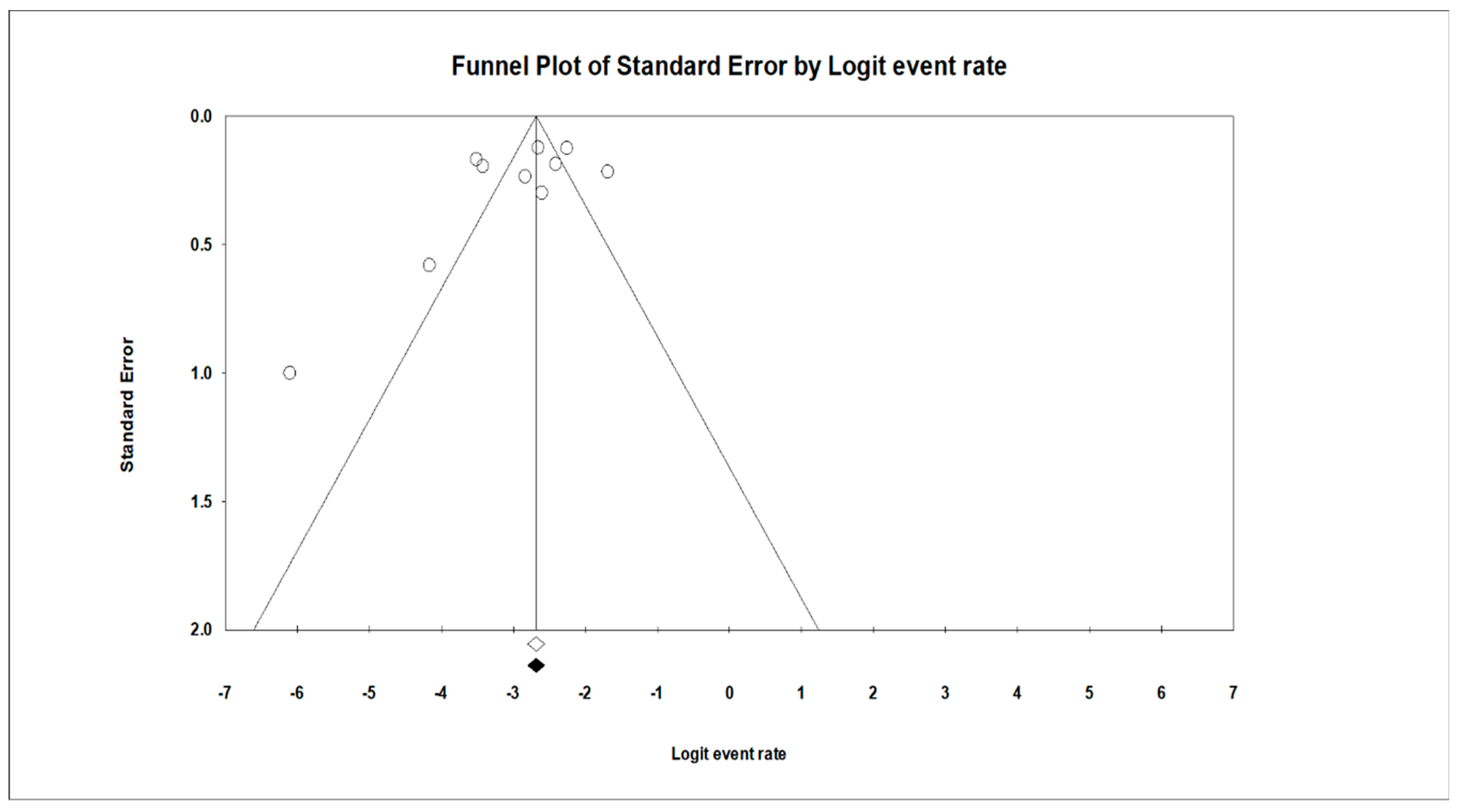
Figure 4.
Forest plot of five selected studies showing the event rate of miniplates removal comparing maxillary to mandibular arches (odds > 1 favor removal of miniplates in the mandibular arch more than maxillary arch).
Figure 4.
Forest plot of five selected studies showing the event rate of miniplates removal comparing maxillary to mandibular arches (odds > 1 favor removal of miniplates in the mandibular arch more than maxillary arch).
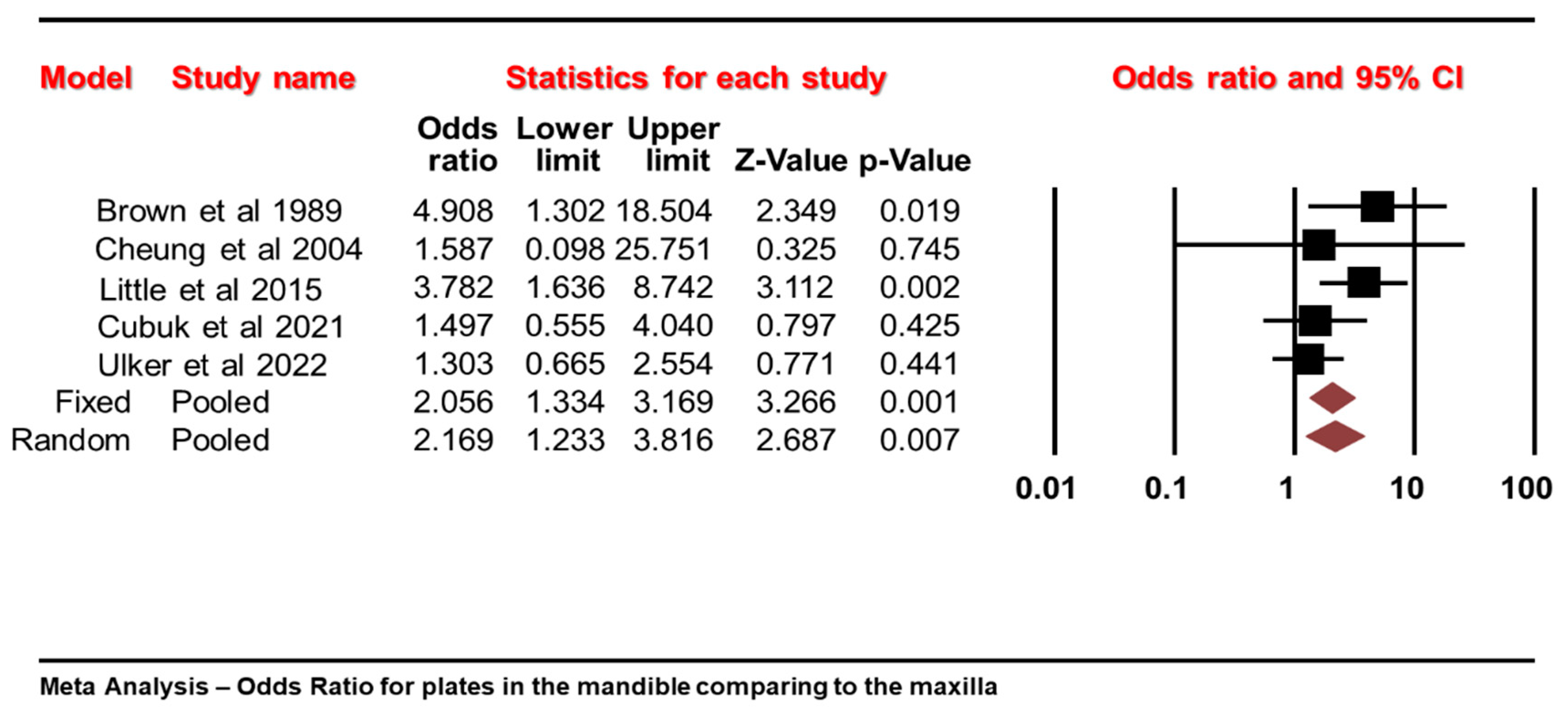

Table 1.
Quality of the selected studies on the Newcastle–Ottawa Scale (NOS).
| Author/Year | Selection | Comparability | Outcomes | Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort |
Selection of the Non-Exposed Cohort |
Ascertainment of Exposure |
Demonstration That Outcome of Interest Was Not Present at Start of Study |
Comparability of Cohorts on the Basis of the Design or Analysis |
Assessment of Outcome |
Was Follow-Up Long Enough for Outcomes to Occur |
Adequacy of Follow-Up of Cohorts |
||
| Brown et al, 1989 [13] |
★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9 |
| Schmidt et al., 1998 [15] | ★ | ☆ | ☆ | ★ | ★☆ | ★ | ★ | ★ | 6 |
| Cheung et al., 2004 [14] | ★ | ★ | ★ | ★ | ★☆ | ★ | ☆ | ★ | 7 |
| Alpha et al., 2006 [2] | ★ | ☆ | ★ | ★ | ☆☆ | ★ | ★ | ★ | 7 |
| Theodossy et al., 2006 [11] | ★ | ★ | ★ | ★ | ★☆ | ★ | ★ | ★ | 8 |
| O’Connell et al., 2009 [6] | ☆ | ★ | ★ | ★ | ★☆ | ★ | ★ | ★ | 7 |
| Little et al., 2015 [10] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9 |
| Mohamed et al., 2020 [16] | ★ | ★ | ★ | ☆ | ★☆ | ★ | ★ | ★ | 8 |
| Cubuk et al., 2021 [17] | ★ | ☆ | ★ | ★ | ★☆ | ★ | ★ | ★ | 7 |
| Ulker et al., 2022 [18] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9 |
The Newcastle–Ottawa Scale.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



