
Submitted:
15 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
Free-of-charge HCV screening in some key populations and in 1969–1989 birth cohorts have been funded in Italy as the first step to diagnosing individuals unaware of their infection.
The aim of this study is to use available in-hospital routine screening data to understand the inpatients HCV screening in a region of North Italy.
A retrospective search of in-hospital patients tested for HCV-antibody (HCV-Ab) from January 2017 to the end of December 2022, was conducted according to age categories (older than 76 years, birth group 1947-1968; birth group1969-1989 and two other categories with patients younger than 33 years) using the TriNetX network.
Of 42,805 in-hospital patients tested, 1,297 (3.03%) resulted HCV-Ab positive.
The proportion decreased from 2017 to 2022 (from 2.03% to 0.36%) years). The higher prevalence of HCV-Ab was in patients older than 76 years (5.3%) while, the lowest was in the younger birth cohort (2000-2022, 0.16%). Of 1,297 patients found HCV-Ab positive, only 198 (15.3%) were tested for the presence of HCV RNA. Although the birth cohort 1969-1989 had a lower seroprevalence (1.5%), they represented the most affected age group with 44.4% of HCV RNA positivity. The in-hospital HCV screening including birth cohort 1947-1989 could be a valuable option respect to the screening for birth group 1969-1989 in the general population. Since a high proportion of patients were not tested for HCV RNA during hospitalization, reflex testing promptly ascertaining an active infection could facilitate linkage to care to stop the burden of HCV.
Keywords:
HCV
; antibodies
; in-hospital screening
; birth cohort
; prevalence
1. Introduction
Chronic hepatitis C virus (HCV) infection is a serious public-health problem, with an estimated global prevalence of 0.7% (0.7–0.9%), corresponding to approximately 56.8 million HCV infections [1]. Over the past two decades, 48% of global hepatitis-related mortality is attributable to hepatitis C virus infection [2].
The estimation of people with HCV chronic active infection in Italy consisted in 2020 of about 280,000 persons who are potentially asymptomatic, and additionally about 120,000 persons with advanced liver fibrosis/cirrhosis with an uncured HCV infection [3]. The World Health Organization presented the following aims regarding all hepatitis viruses by the year 2030: a 90% reduction in incidence, a 65% reduction in mortality, a 90% rate of diagnosing chronic cases, and an 80% treatment rate of individuals with chronic hepatitis [4]. To achieve the HCV elimination goal by 2030, the general-population screening of 1948–1988 birth cohorts and of those with risk factors for HCV infection independent of their age has been recommended in Italy [5,6]. Very recently, free-of-charge HCV screening in some key populations and in 1969–1989 birth cohorts have been funded in Italy as the first step to diagnosing individuals who are infected but asymptomatic (https://www.salute.gov.it/). Preliminary data in Lombardy showed 0.5% of HCV seroprevalence by screening about 150.000 people in the birth group 1969-1989, representing 5% of the overall targeted population.
Since a specific roadmap for each region, is of paramount importance to achieve the high effectiveness of this intervention nationwide, we investigated the seroprevalence for HCV by retrieving data obtained by in-hospital HCV screening in a tertiary hospital in Milan, Lombardy.
Our findings could be useful for supporting the regional level’s decision-making process to define screening and possibly linkage-to-care.
2. Materials and Methods
2.1. Study Design
This study was conducted with data obtained from TriNetX, LLC (“TriNetX), a global federated health research network that provides access to electronic medical records (EMRs) from health-care organizations (HCOs) worldwide. HCOs leverage their EMRs data via TriNetX Platform to build patient cohort level queries to understand patient populations and outcomes analysis. The analyses were conducted utilizing the network “Ospedale San Raffaele”, an HCO self-network. TriNetX is compliant with all Data Protection laws applicable to the contributing HCOs, including the EU Data Protection Law Regulation 2016/679, the General Data Protection Regulation on the protection of natural persons with regard to the processing of personal data. Any data displayed on the TriNetX Platform is in aggregated form, therefore, anonymized data. TriNetX is ISO 27001:2013 certified and maintains a robust IT security program that protects both personal data and health care data.
The retrospective cohort analysis included patients (PTs) hospitalized at Ospedale San Raffaele between year 2017 and 2022. The positivity of HCV antibodies (HCV-Ab) was identified using the LOINC code 16128-1 Hepatitis C Ab [Presence] in Serum within a month since hospitalization. The positivity of HCV RNA testing was identified using the LOINC code 11259-9 Hepatitis C virus RNA [Presence] in Serum or Plasma by nucleic acid amplification (NAA) with probe detection. The patients with an HCV infection (identified with ICD-10-CM codes B17.1 Acute hepatitis C, B18.2 Chronic viral hepatitis C and B19.20 Unspecified viral hepatitis C without hepatic coma, as well as with the positive HCV RNA before the screening were excluded from the study. Sub-cohorts of PTs were created based on the year of birth, defining the following birth control ranges: before 1947, 1947-1968, 1969-1989, 1990-2000 and 2001-2022.
The data were extracted on May 10th, 2023.
Biochemistry included liver enzymes [aspartate aminotransferase, AST (normal values <35 IU/L); alanine aminotransferase, ALT (normal value <59 IU/L); gamma glutamyl transpeptidase, GGT (normal value <68 IU/L)] platelets count (normal value 130-400 x 109/L), alkaline phosphatase, ALP (normal value < 129 IU/L and total bilirubin (normal value <1.1mg/dL).
2.2. Statistical Analysis
All analyses were generated using TriNetX Platform. Demographics information of the cohorts included age and sex (males and females). Continuous variables are expressed as mean values and standard deviation, categorial data were represented as frequencies and percentages. We ran an incidence analysis to calculate the HCV-Ab positivity among the tested PTs over the years, from 2017 to 2022. Incidence proportion calculation method in TriNetX assumes an analysis ran on EHR-data [7]. For a given time window, the incidence proportion denominator (PTs at risk) includes the PTs of the cohort whose fact record overlaps the time window by at least one day and whose fact record does not contain the event of interest before the given time window. The incidence numerator (Incident Cases) includes all those PTs who are in the denominator and whose record includes the event of interest on a date within the time window.
3. Results
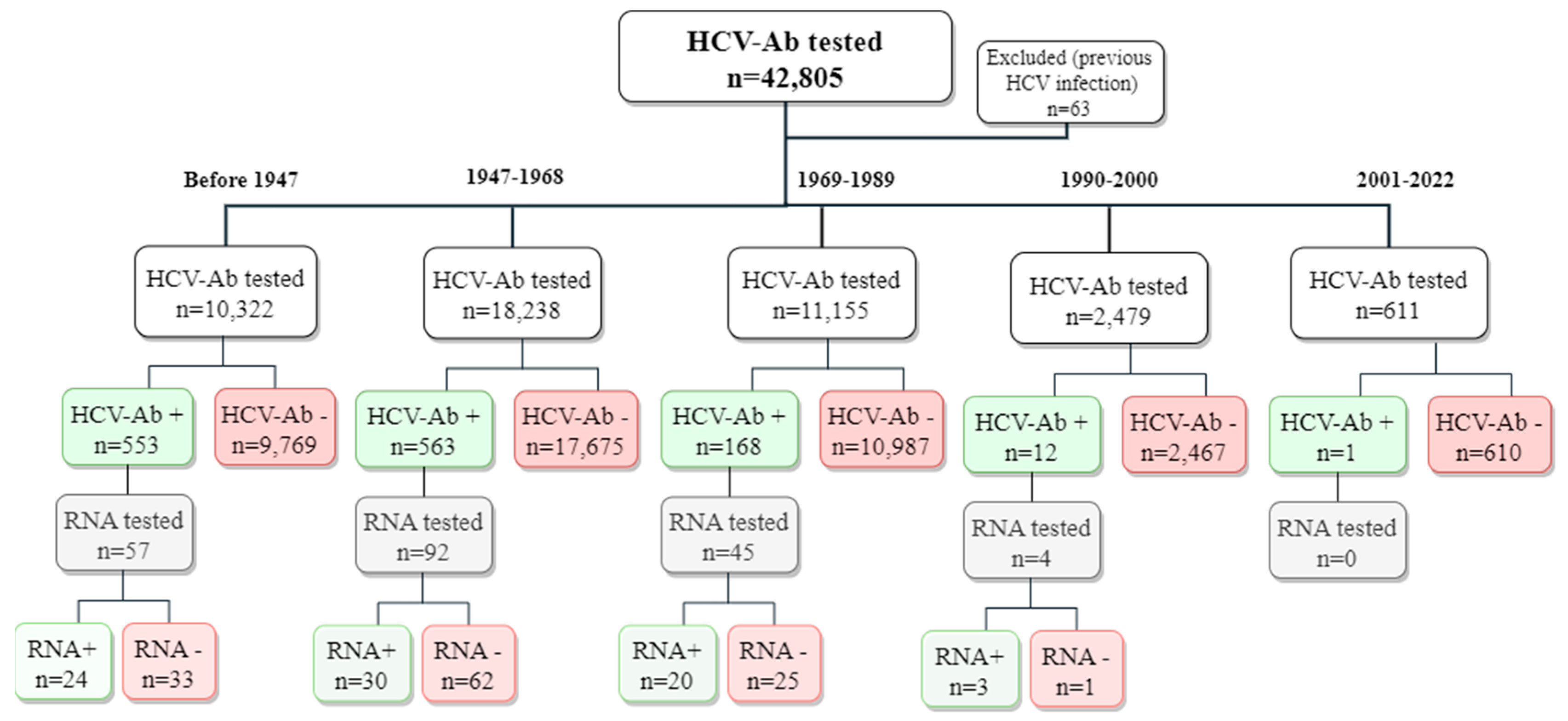
From January 2017 to the end of December 2022, 181,869 PTs were hospitalized at the Scientific Institute San Raffaele, Milan, Italy. During the study period, 42,868 were HCV-Ab tested. Among these, 63 had a previous HCV infection and were excluded from the analysis.
Therefore, in total 42,805 PTs were considered for the analysis. The flowchart of the study cohort is shown in Figure 1.
Characteristics of PTs according to birth cohort are described in Table 1.
Overall, there was a preponderance of males (52% of males vs. 48% of females). Concerning liver enzymes, mean aspartate aminotransferase (AST) levels were found slightly increased in the study cohort (including all birth cohorts). The other biochemical parameters were invariably within the normal range.
Among 42,805 PTs tested for the presence of HCV-Ab, 1297 (3.03%) were found HCV-Ab positive. Overall, the incidence of seroprevalence was higher in men (3.5%) respect to women (2.67%) and yearly incidence proportion decreased from year 2017 to 2022 in males as well as in females (Figure 2).
| 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | ||
| Overall | Incident cases | 335 | 279 | 261 | 190 | 184 | 33 |
| Patients at risk | 16,468 | 18,843 | 19,440 | 17,278 | 15,443 | 9,046 | |
| Incidence proportion | 2.03% | 1.48% | 1.34% | 1.10% | 1.19% | 0.36% | |
| Males | Incident cases | 184 | 159 | 151 | 115 | 111 | 20 |
| Patients at risk | 8325 | 9343 | 9671 | 8533 | 7557 | 4414 | |
| Incidence proportion | 2.21% | 1.70% | 1.56% | 1.35% | 1.47% | 0.45% | |
| Females | Incident cases | 151 | 120 | 110 | 75 | 73 | 13 |
| Patients at risk | 8143 | 9500 | 9769 | 8745 | 7886 | 4632 | |
| Incidence proportion | 1.85% | 1.26% | 1.13% | 0.86% | 0.93% | 0.28% |
The prevalence of an active infection assessed by HCV RNA positivity in HCV-Ab positive PTs, according to birth cohort, are depicted in Figure 3. The prevalence of HCV-Ab decreased from older to younger age with a higher proportion (5.1 %) in PTs older than 76 years and the lower prevalence in birth cohort 2001-2022 (0.16%) (Figure 3). Of 1,297 PTs only 198 (15.3%) were tested for the presence of HCV RNA.
Among HCV-Ab positive PTs, tested for HCV RNA we found 42.1% of active infection in those older than 76 years, 32.6% in the 1947-1968 birth cohort, and 44% in the 1969-1989 birth cohort (Figure 3). In the younger age groups (birth cohort 1990-2000 and 2001-2022) the seroprevalence was very low (0.48% and 0.16%, respectively) and only 4 PTs in the age group 1990-2000 were investigated for the presence of HCV RNA (Figure 3).
Biochemical parameters of PTs with HCV-Ab positivity are described in Table 2.
Considering PTs with HCV-Ab, the sex male was prevalent (57.6%). This data was confirmed also according to birth cohort (Table 2). Concerning liver enzymes, mean AST levels were higher than normal values in older PTs (including PTs older than 76 years and birth cohorts 1947-1968, 1969-1989) while ALT levels were found higher than normal values only in birth cohort 1969-89. The other variables evaluated in different groups of PTs were within the normal range.
Biochemical parameters of PTs with active HCV infection are described in Table 3. There was a preponderance of males (68%) among PTs with active HCV infection. Concerning liver enzymes, mean AST, ALT and GGT levels were found higher than normal values (AST, about 2.5-fold the normal levels; ALT and GGT about 2- and 1.5 -fold the normal levels, respectively). Bilirubin levels were slightly increased. The other parameters were within the normal range.
4. Discussion
The number of newly diagnosed hepatitis C cases reported from Countries across Europe remains at high level with considerable variation between Country specific rate. According to a recent systematic review an estimated 3.9 milion individuals are chronically infected with HCV in EU/EEA Countries with national estimates of HCV prevalence ranging from 0.1 to 5.9%, and Italy has been considered amongst Countries with the highest HCV-Ab prevalence (5.9%) according to the 2016 ECDC report [8].
As of April 1, 2021, WHO reported data indicating 1.34% seroprevalence for HCV in European Country4, while reported data by the ECDC in 2020 indicate that HCV is an infection that predominantly affects people aged 25-44 years that is consistent with the demographic profile of injecting drug use, the main route of transmission reported for chronic case [9]. In Italy the reported cases from 2016 to 2019 was invariably 0.3% with a lower rate in 2020 (0.1%) that could be the result of a combination of changes in healthcare-seeking behaviours and testing practices during the COVID-19 pandemic10. The finding of significant lower prevalence in our Country respect to that reported in previous reports is likely the consequence of harm reduction programmes and, more recently, treatment with new direct-acting antiviral drugs in Italy [8,9,11,12].
Considering the regional distribution of HCV-Ab in Italy, it has been recently estimated that nearly 48.000 individuals living in Lombardy are HCV-Ab positive, corresponding to a seroprevalence of approximately 0.48% [13].
In the present study we showed that in-hospital screening including people born in the years 1947-1989 seems more effective than opportunistic screening in the general population targeted in the birth cohort 1969-1989.
Our data showed cumulative prevalence of HCV-Ab of 3.03 % measured along 5 years, in PTs hospitalized for other comorbidities, with a higher prevalence in older age groups, particularly in PTs older than 76 years (5.3%) and in birth cohort 1947-68 (3.1%). The prevalence was lower in younger PTs with 1.5% in birth group 1969-1989, that dramatically decreased in PTs younger than 33 years confirming the decreasing HCV-infection risk in younger populations in Italy, known as the cohort effect [11,14,15]. In a previous study investigating by a mathematical model the seroprevalence for HCV in Lombardy, the prevalence was estimated approximately 2.65% lower than what we have found in the present study, and according to birth cohort, they found approximately 0.07 % seroprevalence in individuals aged 51-70 years, while we found in people aged 54-75 years 3.12% of seroprevalence that is considerably higher respect to the prevalence estimated by the mathematical model in their report13. Considering also older members in their cohort (aged 71-100 years) the seroprevalence remained lower (about 0.04%) than what we found in our older age groups.
We also assessed the incidence of HCV-Ab during five 5 of observation, showing an incidence proportion of 2.2% in year 2017 that progressively decreased during years 2018-2022, confirming that a large proportion of people in Lombardy have already undergone HCV testing and commenced new efficient and safe therapies against hepatitis C. Interestingly, we observed a small wave of HCV-Ab positivity in year 2021. It is possible that this small increase in the rate of HCV seroprevalence was consequent to hospitalization of older PTs and/or people suffering of other comorbidities during the COVID-19 pandemia. Hepatic manifestations are the common consequences of COVID-19 and PTs with chronic liver diseases are at a higher risk for severe disease and death from COVID-19 [16,17]. Therefore, we hypothesized that a special vigilance was adopted during COVID-19 pandemia to screen and treat COVID-19-associated liver injury. On the contrary, in year 2022 a significant decrease of seroprevalence was observed (0.36%). We have not a clear explanation for this result. It could be the consequence of a decline in testing volumes adopted in our hospital, rather than a true epidemiological finding. Regarding biochemistry, we did not find liver enzymes altered in the initial cohort of 42,805 PTs tested for HCV-Ab, while in the HCV-Ab positive cohort consisting of 1297 PTs, transaminases were found abnormal in some birth cohorts. In all age groups apart those younger than 23 years, AST levels were found abnormally high, while ALT were found altered in the birth cohort 1969-1989. Unfortunately, information on alcohol intake that could be responsible for higher increase of AST respect to ALT, was not available in our cohort. Liver enzymes were found within the normal range in the younger group (birth cohort 1990-2000) where the prevalence of HCV-Ab was very low (0.42%). Finally, altered transaminases were found in PTs with active HCV infection indicating liver damage, despite the different reasons for the hospital admission (Table 3).
Concerning the economical costs, examples of economic analyses of HCV screening programmes in Europe were performed on pregnant women or high-risk populations only [18,19,20,21]. So, peculiar aspects of the national health systems, the target population and the cost per treatment in each context should be considered in terms of low generalizability of the results.
Previous studies showed that age of the target population to be screened and prevalence were main drivers of cost-effectiveness [22,23]. Kondily et al., showed that hepatitis C virus screening strategies by birth cohort in the general population in Italy may have a cost of 6 bilion in direct medical costs by 2031[24]. We identified in-hospital screening as a good option for revealing HCV infection. However, we did not calculate the costs of such a screening.
We could hypothesize that the in-hospital screening could be cost-effective respect to opportunistic screening in the general population, firstly because we identified a higher seroprevalence, secondly, because differently from previous reports [25,26,27] in the present study were involved in-hospital human resurces, and HCV screening was included within biochemical routine test.
Thus, the discussion should be re-opened as to whether the hepatitis screening should be implemented by adding in the screening programme the group 1947-1968, and if the in-hospital rather than opportunistic screening in the general population should be a better strategy for revealing HCV active infection.
In conclusion, to achieve HCV elimination in Italy, broader screening strategies are required.
The HCV-Ab screening including at least birth cohort 1947-1969 could be of interest in hospitalized PTs. Since a high proportion of PTs were not tested for HCV RNA during hospitalization, reflex testing permitting the one-step confirmation of the HCV active infection in individuals unaware of their infection status, should be recommended in hospital settings followed by the immediate engagement and cure of individuals diagnosed with an active HCV infection.
List of Abbreviations
| HCVAb | HCV-antibody; |
| HCOs | health-care organizations; |
| EMRs | electronic medical records |
| PTs | patients; |
| AST | aspartate aminotransferase; |
| ALT | alanine aminotransferase; |
| GGT | gamma glutamyl transpeptidase; |
| ALP | Alkaline phosphatase; |
| SD | standard deviation; |
References
- Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol. 2022;7(5):396-415. [CrossRef]
- World Health Organization. Combating Hepatitis B and C to reach elimination by 2030. WHO; Geneva, Switzerland, 2016.
- Kondili LA, Andreoni M, Alberti A, et al. A mathematical model by route of transmission and fibrosis progression to estimate undiagnosed individuals with HCV in different Italian regions. BMC Infect. Dis. 2022;22(1):58. [CrossRef]
- WHO: Global health sector strategy on viral hepatitis 2016-2021, 2016-2021. https://apps.who.int/iris/han-dle/10665/246177.
- Kondili LA, Gamkrelidze I, Blach, S, et al. Optimization of hepatitis C virus screening strategies by birth cohort in Italy. Liver Int. 2020;40(7):1545–1555. [CrossRef]
- Kondili LA, Aghemo A, Andreoni M, et al. Milestones to reach Hepatitis C Virus (HCV) elimination in Italy: From free-of-charge screening to regional roadmaps for an HCV-free nation. Dig. Liver Dis. 2022;54(2):237–242. [CrossRef]
- Rassen JA, Bartels DB, Schneeweiss S, Patrick AR, Murk W. Measuring prevalence and incidence of chronic conditions in claims and electronic health record databases. Clin Epidemiol. 2018;11:1-15. [CrossRef]
- European Centre for disease prevention and control (ECDC). Systematic review on hepatitis B and C prevalence in the EU/EEA. Stockholm: ECDC. Nov 2016.
- European Centre for disease prevention and control ((ECDC). Hepatitis B and C in the EU neighbourhood: prevalence burden of disease and screening policies. Stockolm: ECDC; 2010.
- European Centre for disease prevention and control (ECDC). Annual epidemiological report 2020.
- Stroffolini, T, Menchinelli, M, Taliani, G, et al. High prevalence of hepatitis C virus infection in a small central Italian town: Lack of evidence of parenteral exposure. Ital. J. Gastroenterol. 1995;27(5):235–238.
- Guadagnino, V, Stroffolini, T, Rapicetta M, et al. Prevalence, risk factors, and genotype distribution of hepatitis C virus infection in the general population: A community-based survey in southern Italy. Hepatology 1997;26(4):1006–1011. [CrossRef]
- Kondili L. L’infezione cronica da virus dell’epatite C (HCV) in Lombardia. Infez. Med. 2021, S2.
- Di Stefano R, Stroffolini T, Ferraro D, et al. Endemic hepatitis C virus infection in a Sicilian town: Further evidence for iatrogenic transmission. J. Med. Virol. 2002;67(3): 339–344. [CrossRef]
- Rosato V, Kondili LA, Nevola R, et al. Elimination of hepatitis C in Southern Italy: A model of HCV screening and linkage to care among hospitalized patients at different hospital divisions. Viruses 2022;14(5):1096. [CrossRef]
- Roshanshad R, Roshanshad A, Fereidooni R, Hosseini-Bensenjan M. COVID-19 and liver injury: Pathophysiology, risk factors, outcome and management in special populations. World J Hepatol. 2023;15(4):441-459. [CrossRef]
- Nawghare P, Jain S, Chandnani S, et al. Predictors of severity and mortality in chronic liver disease patients with COVID-19 during the second wave of the pandemic in India. Cureus. 2022;14(1):e20891. [CrossRef]
- Eijsink JFH, Al Khayat MNMT, Boersma C, et al. Cost-effectiveness of hepatitis C virus screening, and subsequent monitoring or treatment among pregnant women in the Netherlands. Eur J Health Econ. 2021;22(1):75-88. [CrossRef]
- McCormick CA, Domegan L, Carty P, et al. Routine screening for hepatitis C in pregnancy is cost effective in a large urban population in Ireland: a retrospective study. BJOG. 2021;129(2):322-327. [CrossRef]
- Ward Z, Mafirakureva N, Stone J, et al. Cost-effectiveness of mass screening for hepatitis C virus among all inmates in an Irish prison. Int J Drug Policy 2021;96:103394. [CrossRef]
- Mohamed Z, Scott N, Al-Kurdi D, et al. Cost-effectiveness of strategies to improve HCV screening, linkage-to-care and treatment in remand prison settings in England. Liver Int. 2020 ;40(12):2950-2960. [CrossRef]
- Coretti S, Romano F, Orlando V, et al. Economic evaluation of screening programs for hepatitis C virus infection: evidence from literature. Risk Manag Healthc Policy 2015; 8:45-54. [CrossRef]
- Ruggeri M, Coretti S, Gasbarrini A, Cicchetti A. Economic assessment of an anti-HCV screening program in Italy. Value Health. 2013;16(6):965-972. [CrossRef]
- Kondili LA, Gamkrelidze I, Blach S et al; PITER collaborating group. Optimization of hepatitis C virus screening strategies by birth cohort in Italy. Liver Int. 2020;40(7):1545-1555. [CrossRef]
- Coppola C, Kondili LA, Staiano L, et al. Hepatitis C virus micro-elimination plan in Southern Italy: The "HCV ICEberg" project. Pathogens 2023; 12(2):195. [CrossRef]
- Morisco F, Loperto I, Stroffolini T, et al. Prevalence and risk factors of HCV infection in a metropolitan area in southern Italy: Tail of a cohort infected in past decades. J. Med. Virol. 2017;89(2):291–297. [CrossRef]
- D’Ambrosio R, Rizzardini G, Puoti M, et al. Implementation of HCV screening in the 1969-1989 birth-cohort undergoing COVID-19 vaccination. Liver Int. 2022; 42(5):1012-1016. [CrossRef]
Figure 2.
Incidence of HCV-Ab from year 2017 to 2022 in the cohort tested for HCV-Ab overall and according to gender (males vs. females).
Figure 2.
Incidence of HCV-Ab from year 2017 to 2022 in the cohort tested for HCV-Ab overall and according to gender (males vs. females).
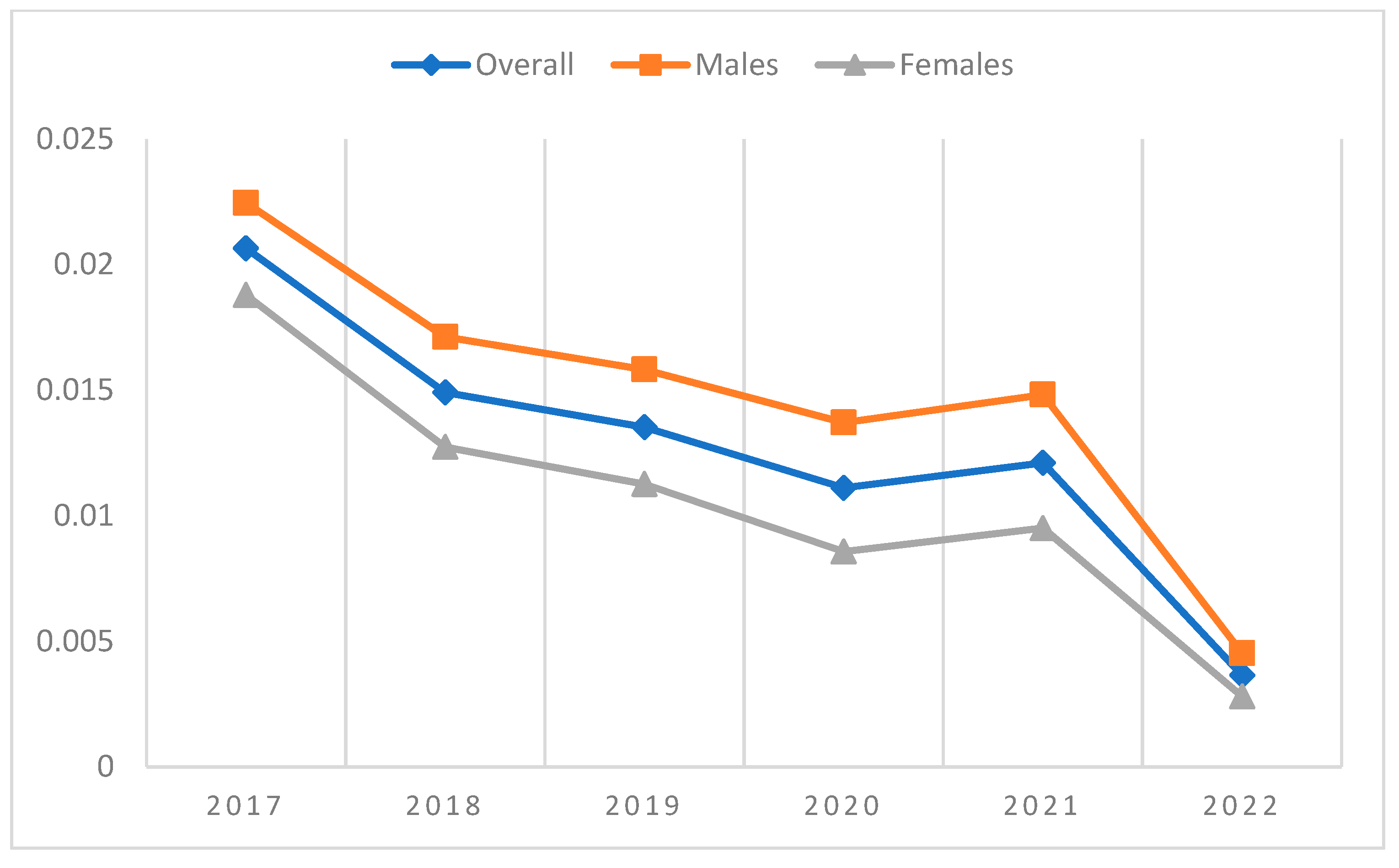
Figure 3.
HCV-Ab prevalence (A) and proportion (B) of HCV RNA positivity by birth cohort. Data concerning HCV RNA positivity are shown in birth groups where at least 10 PTs were tested.
Figure 3.
HCV-Ab prevalence (A) and proportion (B) of HCV RNA positivity by birth cohort. Data concerning HCV RNA positivity are shown in birth groups where at least 10 PTs were tested.
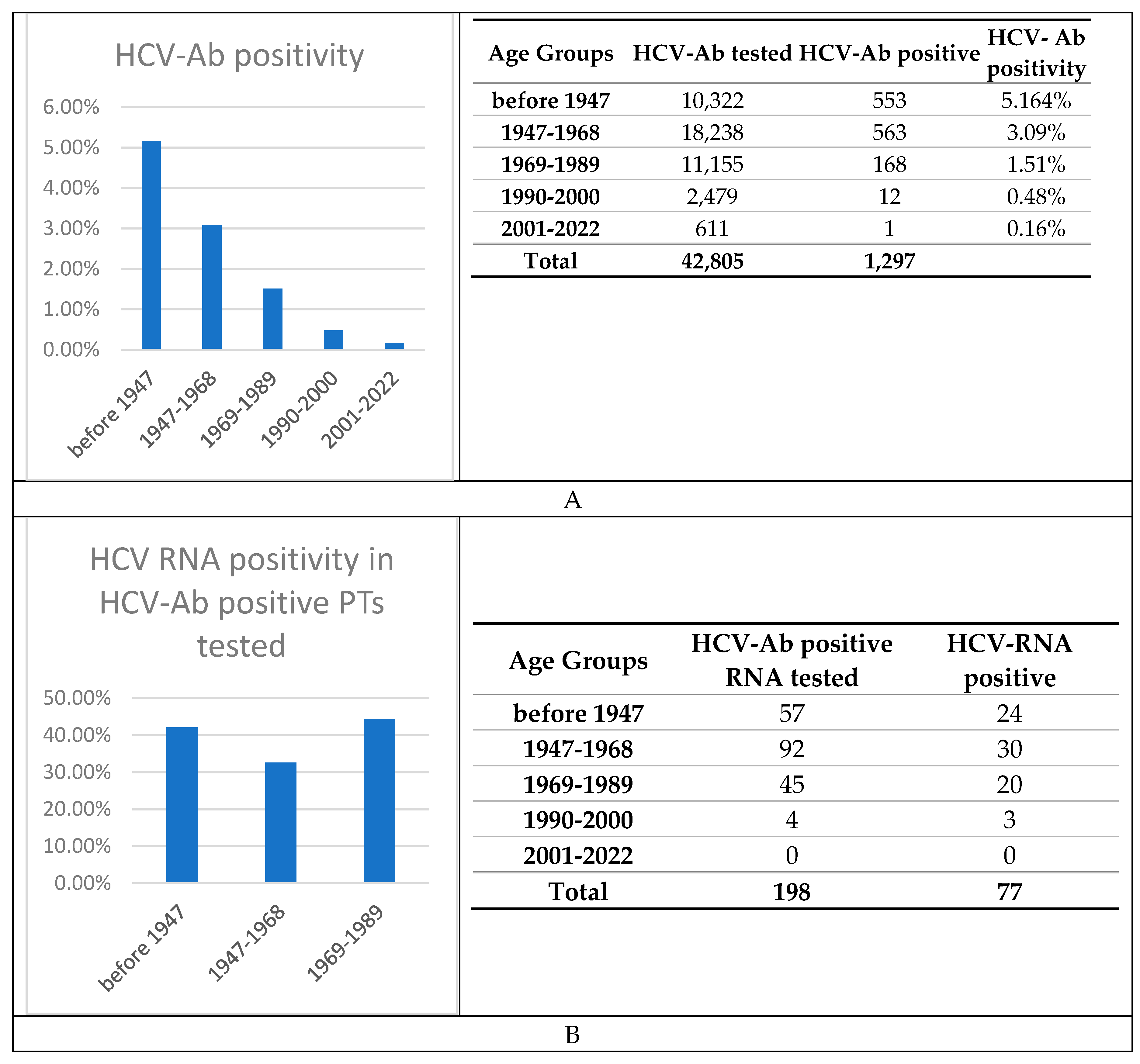

Table 1.
Main clinical characteristics of the study cohort including 42,805 PTs tested for the presence of HCV-Ab.
Table 1.
Main clinical characteristics of the study cohort including 42,805 PTs tested for the presence of HCV-Ab.
| Birth cohort | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Overall | Before 1947 | 1947-1968 | 1969-89 | 1990-2000 | 2001-2022 |
| Number | 42,805 | 10,322 | 18,238 | 11,155 | 2,479 | 611 |
| Age | 57.8 (± 18) | 78.9 (± 4.7) | 62.5 (± 6.46) | 40.1 (± 6.29) | 25.6 (± 3.45) | 12.1 (± 6.62) |
| Males | 22,141 (52) | 6,179 (60) | 11,103 (61) | 3,856 (35) | 712 (29) | 291 ≡(48) |
| AST levels, IU/L | 50.1 (± 373) | 50 (± 324) | 52.9 (± 422) | 43.4 (± 219) | 39.6 (± 201) | 56.4 (± 228) |
| ALT levels, IU/L | 44.3 ± 197 | 38.1 (± 158) | 42.3 (± 167) | 49.2 (± 230) | 42.2 (± 166) | 59.7 (± 163) |
| PLTs count, x109/L | 232 (± 84.8) | 218 (± 85.8) | 233 (± 85.3) | 242 (± 80.3) | 239 (± 78.6) | 268 (± 119) |
| GGT levels, IU/L | 61.6 (± 149) | 58.8 (± 124) | 65.9 (± 157) | 55.5 (± 123) | 36.9 (± 65.7) | 32.9 (± 64.1) |
| Total bilirubin, mg/dL | 0.88 (± 1.69) | 0.912 (± 1.76) | 0.975 (± 2.02) | 0.754 (± 1.35) | 0.638 (± 0.601) | 0.573 (± 0.702) |
| ALP levels, IU/L | 91.4 (± 97.4) | 92.9 (± 102) | 95.4 (± 108) | 78.4 (± 74.3) | 68 (± 47.1) | 176 (± 109) |
Results described by mean (standard deviation, SD) or frequency (%). Abbreviations: AST= aspartate aminotransferase (normal values <35 IU/L); ALT= alanine aminotransferase (normal value <59 IU/L); GGT= gamma glutamyl transpeptidase (normal value <68 IU/L); PLTs=Platelets count (normal amount 130-400 x 109/L), ALP=alkaline phosphatase (normal value < 129 IU/L); bilirubin (normal value <1.1mg/dL).
Table 2.
Main clinical characteristics of the 1,297 patients with HCV-Ab positivity.
| Characteristics | Overall | Before 1947 | 1947-68 | 1969-89 |
|---|---|---|---|---|
| Number | 1,297 | 553 | 563 | 168 |
| Age | 66.7 (± 14.5) | 79.7 (± 4.9) | 62.1 (± 6.74) | 42.7 (± 6.09) |
| Males | 747 (57.6) | 282 (51) | 356 (63.2) | 103 (61.3) |
| AST levels, IU/L | 75.7 (± 602) | 80.9 (± 826) | 77 (± 400) | 57.5 (± 117) |
| ALT levels, IU/L | 52.3 (± 193) | 45.2 (± 239) | 54 (± 149) | 71.6 (± 157) |
| PLTs count, 109/L | 196 (± 91.3) | 186 (± 87.1) | 195 (± 89.5) | 225 (± 101) |
| GGT levels, IU/L | 70.3 (± 123) | 55.4 (± 95.5) | 83 (± 138) | 86.5 (± 153) |
| Bilirubin, mg/dL | 1.08 (± 2.19) | 0.994 (± 2.25) | 1.13 (± 1.94) | 1.26 (± 2.8) |
| ALP levels, IU/L | 94.7 (± 87.8) | 89.6 (± 57.6) | 97.6 (± 97.7) | 103 (± 134) |
*Data in birth group 1990-2000 and 2001-2022 regarding less than 10 PTs were not extracted due to privacy policies. Results are described by mean (standard deviation, SD) or frequency (%). Abbreviations: AST= aspartate aminotransferase (normal values <35 IU/L); ALT= alanine aminotransferase (normal value <59 IU/L); GGT= gamma glutamyl transpeptidase (normal value <68 IU/L); PLTs=Platelets count (normal amount 130-400 x 109/L), ALP=alkaline phosphatase (normal value < 129 IU/L and bilirubin (normal value <1.1mg/dL).
Table 3.
Characteristics of patients with active HCV infection.
| Patients | % of Cohort | |||
|---|---|---|---|---|
| Demographics | Age | 59.3 (± 18.6) | 77 | 100 |
| Males | - | 52 | 68 | |
| Females | - | 25 | 32 | |
| Biochemistry | AST levels, IU/L | 89.8 (± 185) | 72 | 94 |
| ALT levels, IU/L | 119 (± 233) | 72 | 94 | |
| Alkaline phosphatase levels, IU/L | 101 (± 69.1) | 56 | 73 | |
| GGT levels, IU/L | 108 (± 153) | 61 | 79 | |
| Platelets count x109/L | 192 (± 79.1) | 76 | 99 | |
| Total bilirubin, mg/dL | 1.15 (± 2.38) | 66 | 86 |
Results are described by mean (standard deviation, SD) or frequency (%). Abbreviations: AST= aspartate aminotransferase (normal values <35 IU/L); ALT= alanine aminotransferase (normal value <59 IU/L); GGT= gamma glutamyl transpeptidase (normal value <68 IU/L); PLTs=Platelets count (normal amount 130-400 x 109/L), ALP=alkaline phosphatase (normal value < 129 IU/L and bilirubin (normal value <1.1mg/dL).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



