Submitted:
08 December 2023
Posted:
11 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Radiological imaging is essential for acute patient management in Intensive Care Units (ICUs); however, it introduces the risk of exposure to ionizing radiation. This review synthesizes research on radiation exposure in intensive care unit (ICU) settings, highlighting its rise during the COVID-19 pandemic and repetitive imaging. Our analysis extends to radiation safety thresholds, revealing that some ICU patients exceed annual occupational limits, emphasizing the need to balance diagnostic utility against potential long-term risks, such as cancer. Prospective studies have demonstrated an increase in the median Cumulative Effective Dose (CED) in patients with trauma over time, prompting calls for improved awareness and monitoring. Moreover, innovative dose-reduction strategies and optimized protocols, especially in neuro-ICU units, promise to mitigate these risks. This review highlights the essential but risky role of radiological imaging in critical care. It advocates rigorous radiation management protocols to safeguard patient health, while ensuring the continuity of high-quality medical care.
Keywords:
Radiological Imaging
; Radiation exposure
; ICU patients
; COVID-19
; Optimization strategies
; Cancer risk
; Cumulative Effective Dose
Key Points
- Radiological imaging is essential in ICU patients; however, it increases ionizing radiation exposure, necessitating balanced diagnostic benefits against potential long-term health risks.
- Research indicates that ICU patients, especially those with COVID-19 and trauma, often exceed the recommended radiation safety thresholds, highlighting the importance of minimizing exposure to reduce future cancer risks.
- Implementation of dose-reduction strategies and advanced imaging protocols in neuro ICUs demonstrates significant potential for reducing radiation exposure while maintaining care quality.
Abbreviations:
- • ICU: Intensive Care Unit
- • CT: Computed Tomography
- • CED: Cumulative Effective Dose
- • NICU: Neurological Intensive Care Unit
- • LAR: Lifetime Attributable Risk
- • CTDI_vol: Volumetric CT Dose Index
- • ARDS: Adult Respiratory Distress Syndrome
1. Introduction
Radiological imaging has become an indispensable tool in the modern healthcare landscape, particularly in Intensive Care Units (ICUs).[1], [2] These specialized units are dedicated to the care of patients with critical conditions, where timely and accurate diagnoses are often a matter of life and death. Radiological imaging, including radiography and computed tomography (CT), serves as a lifeline for physicians in these high-stress settings, offering crucial insights into patients' conditions and aiding continuous health monitoring. [1]–[3] However, this invaluable resource comes with a consequential caveat: the potential risk of ionizing radiation exposure. The technology that enables healthcare providers to make rapid and informed decisions also carries the inherent risk of triggering radiation-related health concerns, including cancer development. [2], [4], [5]This review delves deeply into the intricate relationship between radiological imaging and radiation exposure in the ICU. We examined the radiation exposure faced by COVID-19 patients in ICUs[6], [7], the risks associated with repetitive imaging in ICU patients[8], and varying degrees of radiation exposure in different patient populations. [2], [9], [10]
The findings of this review emphasize the need for a meticulous approach to radiological practice, guided by the principles of justification, optimization, and strict adherence to dose limits, as advocated by the International Commission on Radiological Protection. [11], [12]Striking the delicate equilibrium between the benefits of diagnostic imaging and the potential hazards of radiation exposure is a continuous challenge, particularly when caring for critically ill adults.
Methodology
We searched PubMed[13], Scopus[14], and Web of Science [15]for articles on radiation exposure in ICUs published between 1995 and 2023. The search parameters were "Cumulative Radiation Exposure,” “X-ray,” “Oncogenic,” “Intensive Care Unit, “Critically ill patients, “and “Risk,“” Cancer,” and were limited to articles in English. The final review excluded duplicate studies and articles that did not specifically address radiation exposure in ICU. We included evidence from case studies, editorials, observational studies, and randomized controlled trials.
1. Radiation Dose Assessment in ICU Patients Amidst COVID-19 and Beyond
Radiation Exposure During the COVID-19 Pandemic
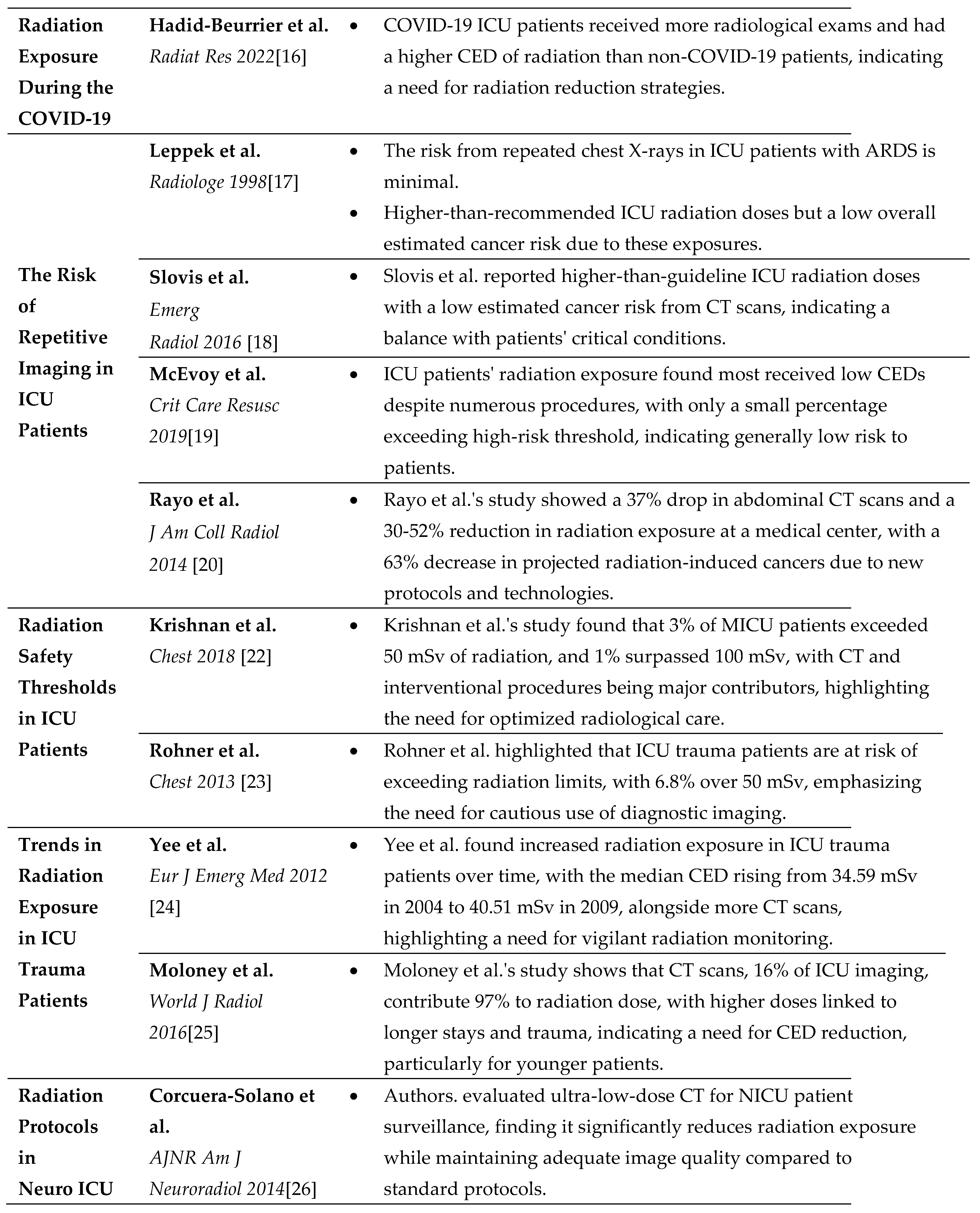
Hadid-Beurrier et al. conducted a study to assess radiation doses from medical imaging in COVID-19 ICU patients compared to non-COVID-19 critically ill patients. They performed a descriptive cohort study on 90 successive ICU patients with COVID-19 between March and May 2020, and 90 non-COVID-19 ICU patients from the same month in 2019. Cumulative effective dose (CED) was calculated from all radiological examinations. Authors found that COVID-19 patients underwent more radiological examinations, with a median of 12.0, compared to 4.0 in non-COVID-19 patients. The CED over four months was significantly higher for COVID-19 patients at 4.2 mSv versus 1.2 mSv for non-COVID-19 patients. Among survivors, a higher proportion of COVID-19 patients had a CED greater than 1 mSv. There was a significant correlation between CED, length of hospitalization, and number of radiographic examinations. The authors found that critically ill COVID-19 patients underwent more medical imaging and thus had a higher CED than non-COVID-19 ICU patients, suggesting the need for strategies to reduce radiation exposure in the future.[16]
The Risk of Repetitive Imaging in ICU Patients
Recent studies have examined radiation exposure risks in ICU patients. Leppek et al. [17] evaluated the morbidity risk associated with repeated bedside chest radiography in ICU patients, particularly those undergoing long-term ventilation for Adult Respiratory Distress Syndrome (ARDS).[9] Surface and gonadal doses were measured for each patient, revealing that the mean surface dose per patient ranged from 0.31 mGy to 0.56 mGy. Gonadal exposure was less than 0.03 mGy per radiograph, with a mean effective dose per exposure of approximately 0.15 mSv. The CED varied between 2.49 mSv and 14.09 mSv, corresponding to an estimated increase in individual cancer risk between 0.01% and 0.07%. The study concluded that when considering the poor prognosis of critically ill, long-term ventilated patients, the additional risk of morbidity due to bedside chest radiographs is minimal and should be considered negligible.
Slovis et al. focused on radiation exposure from CT scans in ICU patients and the associated lifetime attributable risk (LAR) of cancer. Conducted via an electronic chart review from January 2007 to December 2011, this study calculated the CED for each CT scan and predicted the LAR for each patient. The average radiation exposure was 22.2 mSv with a mean LAR of 0.1%, although the median was higher at 0.6%, ranging from less than 0.001% to 3.4%. The research found that radiation doses in the ICU were higher than those recommended by the guidelines, which could justify the critical condition of the patients. Overall, the estimated cancer risk due to radiation exposure in the ICU patient cohort was considered low.[18]
McEvoy et al. investigated CED exposure in ICU patients, considering the medical benefits against associated risks. Conducted as a retrospective audit in a South Australian tertiary care ICU, the study included 526 long-stay patients over a year, from April 2015 to 2016. The audit revealed that these patients underwent 4331 procedures, resulting in a total of 5688.45 mSv of radiation. Despite 82% of the procedures, chest X-rays contributed to only 1.2% of the CED. In contrast, although only 3.6% of the procedures were performed, abdominal and pelvic CT scans accounted for 68% of CED. Over half of the patients received a CED of less than one mSv, 6% received > 50 mSv, and 1.3% exceeded 100 mSv. Patients with trauma and longer ICU stays had higher CEDs. This conclusion indicates that most ICU patients receive a low CED, with the majority staying under the public exposure limit of 1 mSv, suggesting that the risk to patients is relatively low. These findings serve to inform clinicians about radiation exposure levels in ICU settings.[19]
Rayo et al. evaluated the impact of reduced CT scan volume and dose reduction strategies on radiation exposure in patients at a Midwestern academic medical center from 2008 to 2012. The focus was on CT scans of the abdomen, head, sinus, and lumbar spine. Data collected for general medicine and ICU patients were used to assess the CT volume, rate, effective dose, radiation exposure, and estimated cancer risk annually. The results showed a significant 37% reduction in abdominal CT scan volume and a 30%–52% decrease in radiation exposure due to dose reduction strategies. No volume reduction was observed in the head or lumbar spine CT scans, and only a minimal decrease was observed in the sinus scans. The combined strategies led to a 63% reduction in the estimated number of radiation-induced cancers. The conclusion emphasizes that the institution successfully reduced ionizing radiation exposure through fewer CT procedures and lower doses per procedure, primarily owing to the adoption of new protocols and technologies. These changes appear to have had the most substantial impact on reducing future cancer risk associated with CT radiation.[20] These studies collectively underline the importance of balancing medical benefits against the potential risks of radiation in critical care settings.
2. Long-Term Studies on Radiation Exposure in ICU Settings
Radiation Safety Thresholds in ICU Patients
The implications of radiation exposure in critical care settings have been a growing concern, particularly as doses may approach or exceed established safety limits.
Krishnan et al. evaluate patients' radiation exposure in the medical ICU (MICU), hypothesizing that some may exceed US federal occupational health standards. This retrospective observational study at an academic medical center analyzed all adult admissions to the MICU in 2013, totaling 4,155 patients, to calculate their CED from radiological studies. The results showed that 3% of admissions accrued a CED of ≥50 mSv, and 1% exceeded 100 mSv, with a median CED of 0.72 mSv. Higher APACHE III scores[21], longer MICU stay, sepsis, and gastrointestinal issues were associated with higher CEDs. CT and interventional radiology procedures were the most significant contributors to CED. The study concluded that a notable proportion of MICU patients receive radiation doses exceeding the annual occupational limits, with some surpassing 100 mSv. There is a clear need to justify and optimize radiological studies to minimize exposure while delivering essential medical care.[22]
Rohner et al. discussed the concern regarding the safety limits of radiation exposure to minimize the risk of radiation-induced cancer. Occupational exposure limits were set at 20 mSv/year over five years, with a cap of 50 mSv per year. However, the average radiation dose in the US has increased over the past 30 years, mainly because of medical imaging. The study hypothesized that patients in a surgical ICU, particularly trauma patients, might approach or exceed these exposure limits owing to frequent diagnostic imaging. The study involved prospective observation of patients in a level I trauma center's SICU over 30 days. Radiation doses were calculated using Huda's method for all imaging procedures. The study found that 6.8% of the patients exceeded the 50 mSv mark. Higher radiation doses were associated with trauma, extended hospital stay, and more frequent use of CT and fluoroscopy. Multivariable analysis indicated that the number of CT scans and fluoroscopy duration significantly influenced increased radiation exposure. This finding emphasizes the need for careful radiological imaging to avoid excessive radiation exposure. Healthcare providers must balance the diagnostic benefits with the risks of CED in critically ill and injured patients.[23]
Trends in Radiation Exposure in ICU Trauma Patients
Yee et al. assessed the CED of radiation received by mechanically ventilated trauma patients in the Emergency Department and ICU during two periods. A retrospective analysis was conducted on two cohorts of 45 adult patients each, starting from January 1, 2004, and January 1, 2009, in a regional non-urban ICU. Data on radiological examinations, demographics, and clinical information were collected from various databases. The findings indicated an increase in the median CED per patient from 34.59 mSv (IQR 9.08-43.91) in 2004 to 40.51 mSv (IQR 22.01-48.87) in 2009, with a significant p-value of 0.045. There was also an increase in CT examinations per patient over time, from an average of 2.11 in 2004 to 2.62 in 2009. The conclusion drawn was that radiation exposure in ICU trauma patients requiring mechanical ventilation has increased, emphasizing the need for prospective monitoring and awareness among staff of the heightened risk due to this shift in clinical practice.[24]
Moloney et al. quantified the CED of radiation from diagnostic imaging performed in ICU patients. Conducted prospectively in the ICU of a tertiary referral and level 1 trauma center, the study gathered demographic and clinical data from all patients admitted for over one year. CED was calculated based on the UK National Radiation Protection Board's reference effective dose. Of the 421 patients, 2737 studies were conducted, resulting in a total CED of 1704 mSv. The median CED was 1.5 mSv. In the pediatric subgroup, the total CED was 74.6 mSv, with a median of 0.07 mSv. Chest radiography, although the most common, accounted for only 2.7% of the total CED, while CT scans, only 16% of the studies, contributed 97% of the CED. Patients with trauma had a significantly higher CED than those with medical or surgical trauma. This study found that the length of ICU stay was an independent predictor of receiving a CED > 15 mSv. This conclusion highlights that trauma patients and those with extended ICU stays are at higher risk of elevated CEDs. This study advocates minimization of CED, particularly in younger patients.[25] These studies underscore the urgent need to balance the necessity of diagnostic imaging in critically ill patients with the potential long-term risks of radiation exposure.
3. Optimizing Radiological Practices in Neuro ICU Units
Evaluating Radiation Protocols in Neuro ICU Surveillance
Corcuera-Solano et al. focused on the radiation exposure of patients in the neurosurgical ICU (NICU) who underwent multiple head CT scans. The objective of this study was to evaluate the effectiveness of an ultra-low-dose CT protocol for NICU surveillance, comparing it to standard low-dose CT and traditional standard-dose CT protocols. A retrospective analysis of 54 head CT examinations of 22 NICU patients was conducted. The examinations were categorized into ultra-low-dose (22), low-dose (12), and standard-dose (20). The ultra-low-dose and low-dose CTs used a sinogram-affirmed iterative reconstruction technique on a Siemens AS+128 scanner. In contrast, standard-dose CTs use filtered back-projection on a Somatom Sensation 64 scanner. Image quality and radiation dose were assessed both qualitatively and quantitatively. The results showed that ultra-low-dose CT had a 68% lower dose index volume than standard-dose CT but maintained similar image quality and signal-to-noise ratio (SNR). Low-dose CT has better image quality than standard-dose CT, with a 24% lower dose index volume. Although ultra-low-dose CT has a lower SNR than low-dose CT, it is still clinically acceptable. The study concluded that the ultralow-dose CT protocol significantly reduced radiation exposure while preserving adequate image quality for surveillance in NICU patients.[26]
Radiation Exposure in Neuro ICU Patients
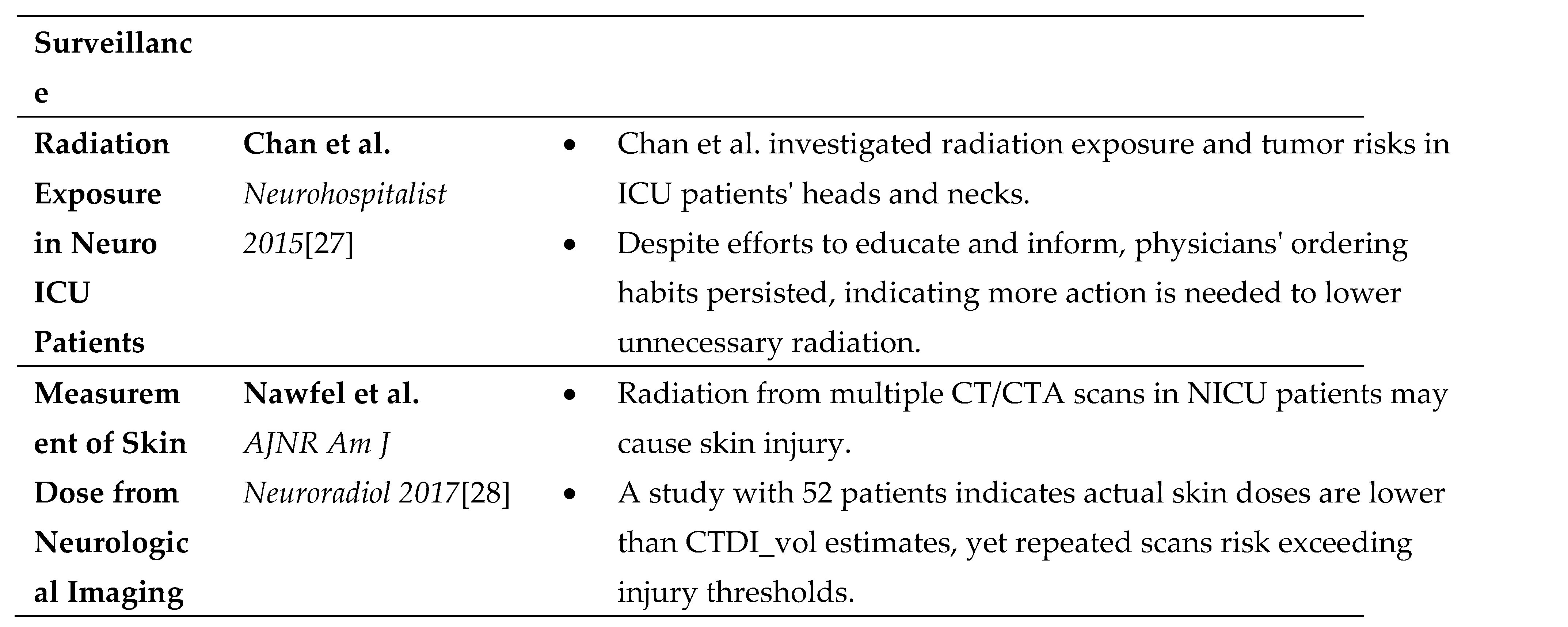
Chan et al. examined CED from diagnostic studies in patients with primary neurological disorders in an ICU. This study aimed to quantify the radiation doses and assess the risk of radiation-induced tumors in the head and neck regions. This retrospective cohort study was conducted in a single institution's neuroscience ICU (NICU), with radiation doses converted to estimated effective doses in mSv using published formulas. An educational initiative was implemented to inform physicians about patient radiation exposure, with a focus on treating acute subarachnoid hemorrhage. Data on radiation exposure were posted at patients' bedsides to determine whether it would influence physician ordering practices. From July 2010 to March 2011, 641 patients who underwent head CT scans were identified, with an average exposure of 18.4 mSv. Patients with subarachnoid hemorrhage had the highest average exposure at 37.1 mSv, although the risk of carcinogenesis was deemed low. The educational initiative did not result in a reduction in the effective dose per patient. The study concluded that while it is possible to accurately report estimated effective doses to physicians, more than an educational initiative alone was needed to alter ordering behaviors. These findings suggest that additional strategies are necessary to mitigate unnecessary radiation exposure in the NICU.[27]
Direct Measurement of Skin Dose from Neurological Imaging
Nawfel's research addresses the concerns that radiation exposure from multiple CT and CTA scans in neurological ICU(NICU) patients can reach levels high enough to cause deterministic skin injury. This study aimed to measure head CT and CTA peak skin doses directly, evaluate their correlation with the volumetric CT dose index (CTDI_vol), and assess whether CED from multiple scans could exceed thresholds for skin injury. From to 2011-2013, a prospective study involving 52 patients measured peak skin doses using nanoDot optically stimulated luminescence dosimeters across two CT scanners. Patient and phantom data were collected to ensure accuracy. The study found that CTDI_vol often overestimated the peak skin dose 1.4 or 1.9 times. The CED for patients who underwent multiple scans ranged from 1.9 4.5 Gy. In conclusion, the directly measured skin doses from head CT and CTA scans were lower than those estimated by CTDI_vol. However, the CED from multiple examinations may surpass the deterministic threshold for skin damage in NICU patients, indicating the potential risk of injury from repeated imaging.[28]
Conclusion
This comprehensive review underscores the complexity of managing radiation exposure in ICU settings, especially with increased reliance on imaging for critical care diagnostics. Studies have shown that, particularly during the COVID-19 pandemic, ICU patients are subject to higher radiation doses, raising concerns about the long-term risks of cancer. These studies collectively indicate a need for meticulous radiation management, emphasizing dose minimization and adherence to safety thresholds, especially for vulnerable populations, such as trauma patients. Optimization of imaging protocols, as seen in neuro ICU practices, and educational initiatives on radiation risk are crucial steps. Ultimately, the balance between the diagnostic benefits and radiation risks must be carefully monitored to ensure patient safety while delivering essential care.

Table 1.
Intensive care unit studies.
References
- D. Toy, M. D. Siegel, and A. N. Rubinowitz, “Imaging in the Intensive Care Unit,” Semin Respir Crit Care Med, vol. 43, no. 06, pp. 899–923, Dec. 2022. [CrossRef]
- S. Rajsic, R. Breitkopf, M. Bachler, and B. Treml, “Diagnostic Modalities in Critical Care: Point-of-Care Approach,” Diagnostics, vol. 11, no. 12, p. 2202, Nov. 2021. [CrossRef]
- B. Trotman-Dickenson, “Radiology in the Intensive Care Unit (Part I),” J Intensive Care Med, vol. 18, no. 4, pp. 198–210, Jul. 2003. [CrossRef]
- E. Soo and A. J. Edey, “The role of thoracic imaging in the intensive care unit,” Br J Hosp Med, vol. 73, no. 11, pp. 612–619, Nov. 2012. [CrossRef]
- B. Trotman-Dickenson, “Radiology in the Intensive Care Unit (Part 2),” J Intensive Care Med, vol. 18, no. 5, pp. 239–252, Sep. 2003. [CrossRef]
- F. Crimì et al., “High resolution computed tomography texture analysis identifies patients at risk of pulmonary fibrosis after COVID-19 pneumonia,” Quant Imaging Med Surg, vol. 12, no. 3, pp. 2199–2202, Mar. 2022. [CrossRef]
- G. Cabrelle, C. Zanon, F. Crimì, and E. Quaia, “Can chest computed tomography findings be compared between outpatient and hospitalized COVID-19 patients?,” J Med Imaging Radiat Sci, vol. 53, no. 1, pp. 184–185, Mar. 2022. [CrossRef]
- C. Zanon, G. Cabrelle, F. Crimì, and E. Quaia, “Correlation among semiquantitative High-Resolution Computed Tomography severity scores and clinical and biochemical parameters in COVID-19, is it really effective?,” Clin Respir J, vol. 17, no. 2, pp. 122–123, Feb. 2023. [CrossRef]
- S. Inui et al., “The role of chest imaging in the diagnosis, management, and monitoring of coronavirus disease 2019 (COVID-19),” Insights Imaging, vol. 12, no. 1, p. 155, Dec. 2021. [CrossRef]
- F. Crimì, G. Cabrelle, C. Zanon, and E. Quaia, “Chest computed tomography in COVID-19 infection,” Clin Transl Imaging, vol. 9, no. 6, pp. 649–650, Dec. 2021. [CrossRef]
- R. Najjar, “Radiology’s Ionising Radiation Paradox: Weighing the Indispensable Against the Detrimental in Medical Imaging,” Cureus, Jul. 2023. [CrossRef]
- https://www.icrp.org/publication.asp?id=ICRP%20Publication%20103%20(Users%20Edition), “https://www.icrp.org/publication.asp?id=ICRP%20Publication%20103%20(Users%20Edition)”.
- https://pubmed.ncbi.nlm.nih.gov/, “https://pubmed.ncbi.nlm.nih.gov/”.
- https://www.scopus.com/home.uri, “https://www.scopus.com/home.uri”.
- https://clarivate.com/products/scientific-and-academic-research/research-discovery-and-workflow-solutions/webofscience-platform/, “https://clarivate.com/products/scientific-and-academic-research/research-discovery-and-workflow-solutions/webofscience-platform/”.
- L. Hadid-Beurrier et al., “Cumulative Radiation Exposure in Covid-19 Patients Admitted to the Intensive Care Unit,” Radiat Res, vol. 197, no. 6, Mar. 2022. [CrossRef]
- R. Leppek, S. S. Bertrams, W. Höltermann, and K. J. Klose, “Strahlenexposition durch Röntgenthoraxaufnahmen auf der Intensivstation Dosiskumulation und Strahlenkrebsrisiko bei Langzeittherapie,” Radiologe, vol. 38, no. 9, pp. 730–736, Sep. 1998. [CrossRef]
- B. H. Slovis et al., “Significant but reasonable radiation exposure from computed tomography-related medical imaging in the ICU.,” Emerg Radiol, vol. 23, no. 2, pp. 141–6, Apr. 2016. [CrossRef]
- J. H. McEvoy, S. Bihari, A. M. Hooker, and D.-L. Dixon, “Cumulative radiation in critically ill patients: a retrospective audit of ionising radiation exposure in an intensive care unit.,” Crit Care Resusc, vol. 21, no. 3, pp. 212–219, Sep. 2019.
- M. F. Rayo, E. S. Patterson, B. W. Liston, S. White, and N. Kowalczyk, “Determining the Rate of Change in Exposure to Ionizing Radiation From CT Scans: A Database Analysis From One Hospital,” Journal of the American College of Radiology, vol. 11, no. 7, pp. 703–708, Jul. 2014. [CrossRef]
- M. A. Matthay et al., “Acute respiratory distress syndrome,” Nat Rev Dis Primers, vol. 5, no. 1, p. 18, Mar. 2019. [CrossRef]
- S. Krishnan et al., “Radiation Exposure in the Medical ICU,” Chest, vol. 153, no. 5, pp. 1160–1168, May 2018. [CrossRef]
- D. J. Rohner et al., “Cumulative Total Effective Whole-Body Radiation Dose in Critically Ill Patients,” Chest, vol. 144, no. 5, pp. 1481–1486, Nov. 2013. [CrossRef]
- M. V. Yee, R. A. Barron, T. A. Knobloch, U. Pandey, C. Twyford, and R. C. Freebairn, “Radiation exposure of ventilated trauma patients in intensive care,” European Journal of Emergency Medicine, vol. 19, no. 4, pp. 231–234, Aug. 2012. [CrossRef]
- F. Moloney et al., “Cumulative radiation exposure from diagnostic imaging in intensive care unit patients,” World J Radiol, vol. 8, no. 4, p. 419, 2016. [CrossRef]
- I. Corcuera-Solano, A. H. Doshi, A. Noor, and L. N. Tanenbaum, “Repeated Head CT in the Neurosurgical Intensive Care Unit: Feasibility of Sinogram-Affirmed Iterative Reconstruction–Based Ultra-Low-Dose CT for Surveillance,” American Journal of Neuroradiology, vol. 35, no. 7, pp. 1281–1287, Jul. 2014, doi: 10.3174/ajnr.A3861.
- S. Chan, S. A. Josephson, L. Rosow, and W. S. Smith, “A Quality Assurance Initiative Targeting Radiation Exposure to Neuroscience Patients in the Intensive Care Unit,” Neurohospitalist, vol. 5, no. 1, pp. 9–14, Jan. 2015. [CrossRef]
- R. D. Nawfel and G. S. Young, “Measured Head CT/CTA Skin Dose and Intensive Care Unit Patient Cumulative Exposure,” American Journal of Neuroradiology, vol. 38, no. 3, pp. 455–461, Mar. 2017. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



