Submitted:
05 December 2023
Posted:
07 December 2023
You are already at the latest version
Abstract
Vascular endothelial growth factors (VEGFs) are regarded as the key vasculogenic mediators in the human body, of which VEGF-A is considered as one of the important types. It is the major growth factor possessing increasing vascular permeability as well as angiogenesis properties. This article provides intuition into the different effects of VEGF-A on vessels in ovarian hyper stimulation syndrome (OHSS) which is defined as a complication of in-vitro fertilization for infertility treatment, and obesity, a universally health problem. These are two dissimilar pathways outcomes for VEGF-A effects, thereby This article reviews updated information about the mentioned disorders and reveals that how this kind of growth factor yields different results on vasculature by activating distinct intracellular signaling in endothelial cells.
Keywords:
obesity
; VEGF-A
; vascular permeability
; ovarian hyper stimulation syndrome
; adipose tissue
; angiogenesis
; adipocytes
; endothelial cell
; IVF
; infertility
1. Introduction
Currently, a vast number of people suffer from infertility [1]. In the Unites States, around 12.1% of reproductive-age women have this problem [2]. It is defined as an individual’s inability to conceive after one year (or longer) through a natural process. Infertility is classified as primary (lack of history of pregnancy in the past) and secondary infertility (failure to repeat pregnancy after at least one conception) [3]. There are several risk factors for infertility including, genital infections, congenital uterine abnormalities, prolonged oral contraception, hormonal disorders, sociocultural factors, etc. Moreover, due to increasing life style factors attributed, in part, to smoking, sexual transmitted diseases (STDs), obesity, alcohol use, and lake of physical activity, the prevalence rate of infertility has grown [4]. Therefore, assisted reproductive technologies (ARTs) are utilized to help those infertile couples in treatment of this multifactorial disorder [5].
The uses of ARTs have increased during recent years. ARTs are defined as all procedures for commencing conception, which consist of numerous types such as in-vitro fertilization (IVF), intrauterine insemination (IUI), intracytoplasmic sperm injection (ICSI), gamete and embryo cryopreservation, preimplantation genetic screening, preimplantation diagnosis, and/or the use of fertility medication. Among these different kinds of ART, IVF is the most predominant type [6].
IVF procedure is categorized in 4 basic steps. To clarify, high- dose gonadotropins are used for controlled ovarian hyper stimulation (COH) in the first step. Additionally, patients are triggered by using such drugs as human Chorionic Gonadotropin (hCG) after reaching desired count /size of ovarian follicles so as to initiate the ovulatory cascade, yielding the final follicle maturation process. Afterwards, oocytes are retrieved from the ovaries in surgery rooms and are transferred to special laboratories to achieve fertilization. In step three, embryos are cultured in equipped mediums for a few days in order to prime the embryos for transfer (3 days to reach the eight-cell stage or 5 days to reach the developed embryo in blastocyst stage). In the final step, embryos are transferred into the uterus, which is known as Fresh-ET, and/or frozen for the future transfer [6]. In spite of the fact that IVF is beneficial for most of infertile couples, ovarian hyper stimulation syndrome (OHSS) can occur as one of its complications [2,6,7].
2. OHSS
OHSS is an important iatrogenic condition during IVF procedure, which has the potential to be life-threatening in its severe forms [5,6,7,8]. In other words, OHSS often develops as the consequence of gonadotropins (mostly hCG) administration which facilitates oocytes maturation and is released during IVF treatment [1,2]. There are several risk factors for OHSS, which almost most of them have been summed up in Table 1. For better perception, researchers categorized OHSS risk factors into two different groups: 1) primary risk factors and 2) secondary risk factors. Primary risk factors include past history of OHSS, low body mass index (BMI), PCOS (which is also a risk factor for infertility), high antral follicle count (AFC) > 8, age < 30 years (even though the chance of conception for women aged under 30 years is around 71%, and women > 35 years old are at high risk of infertility), and high amounts of basal anti-mullerian hormone (AMH) > 3.36 ng/ml (high specifity and sensitivity (81.3%, 90.5%)). On the other hand, secondary risk factors are associated with ovarian response to COH, and they consist ofsmall follicle counts > 14 with the diameter of around 11mm (8-12 mm) in the triggering day, rapid elevation in serum estradiol concentration > 2500 pg/ml, and large retrieved oocytes count >20 [3,4,9,10,11,12,13]. Furthermore, hCG a complex heterodimeric glycoprotein hormone, is regarded as one of the main risk factors for OHSS development [14,15]. In 2020, one study reported that patients with dyslipidemia are in the higher risk for development of OHSS [11]. Along with different types for categorization of these risk factors, numerous attempts have been carried out to classify OHSS.
Two sorts of classifications have been determined for this potentially lethal complication: 1) based on timing presentation in which two forms have been described: early and late. Early OHSS is commonly trigger-related. It happens within 10 days of induced ovulation. On the other hand, late OHSS is mainly pregnancy-related because of excessive amounts of endogenous hCG from a developing pregnancy, and it appears after ≥ 10 days following oocyte retrieval [8,12,14,16]. 2) Based on clinical, imaging plus laboratory features, in which OHSS is categorized into 4 stages: mild, moderate, severe, and critical. The milder form is the most prevalent among other stages of OHSS [2]. According to the second classification type, OHSS appears with various features related to severity.
There are an extensive range of clinical presentation for OHSS from mild to critical although these stages are not purely separated from each other. OHSS manifestations appear because of bilateral cystic enlargement of exceedingly luteinized ovaries [13]. Mild ovarian enlargement (ovarian diameter: 5-12 cm) makes the mild form of OHSS. Initial clinical presentations of mild OHSS are commonly associated with abdominal distention, which include mild abdominal pain, poor appetite, nausea, vomiting, mild diarrhea, and bloating [1,2,8,12,13] even though The symptoms of this stage might be imperceptible. In moderate OHSS, detectable ascites on ultrasound is added to the diagnostic criteria, and an apparent clinically ascites (grade 2) plus other more severe manifestations are revealed in the severe form. Indeed, clinical presentations in the severe forms include severe abdominal discomfort, severe shortness of breath (SOB), rapid weight gain around > 1 kg in a day, severe nausea and vomiting, venous thrombosis, oliguria, pleural effusion (signs: tachypnea, crackle upon auscultation), intra-abdominal hypertension (IAH) which is defined as intra-abdominal pressure (IAP) > 12 mmHg, hemodynamic changes and so on. Also, the critical form manifestations include arterial thrombosis, anuria, thromboembolism, pericardial effusion, acute respiratory distress syndrome (ARDS), massive hydrothorax, sepsis, shock, and maybe even death [8,13,14,17].
Laboratory findings are different related to the severity of the disease. For instance, in the mild stage, there is no significant laboratory change most of the times. In the moderate form of OHSS, laboratory findings are such as white blood cells (WBC) > 15000/ ml, hematocrit (HCT) > 41%, and hypoproteinemia [17]. In the severe stage, the laboratory changes get more serious, including HCT> 55%, WBC > 25000/ ml, Na < 135 meq/ml, K > 5 meq/ml, serum creatinine (Cr) > 1.6 mg/dl, increasing liver enzymes, and clearance of Cr < 50 ml/min. In the critical stage, the laboratory parameters become more deteriorated [17]. To summarize, a number of most important clinical and laboratory findings in OHSS have been shown below (Figure 1). These manifestations of OHSS specially in the severe forms, predominantly are caused by fluid shifting into the third space of the body (mostly in peritoneal compartment, less frequently in pleural and pericardial space) [2,18].
2.1. Third Spacing Phenomenon
Third spacing in OHSS is the result of increased vascular permeability. There are two main proposed models for increased vascular permeability: first, formation of vesiculo-vacuolar organelles (VVOs) which are a kind of trans-endothelial channels generated from vesicles or vacuoles. The next model which is deserved to be taken into account is transient dissolving of endothelial junctions [19]. For more explanation, endothelial cells are the bulk of the innermost layer of vessels; they are actually simple squamous cells. Three sorts of endothelial cell junctions have been discovered: gap, tight, and adherence junctions. Each of these different cell junctions possess their own constituents. For instance, in gap junctions, connexins are participated as the junction generators. Nevertheless, in tight junctions, some other molecules are involved such as claudins, nectin, occluding, and so on. The constituents of adherence junctions are such as nectin, VE-cadherin, etc. Furthermore, inner side of endothelial cells are covered by glycocalyx which is made up of two layers of fiber matrix and full of proteoglycans. The glycocalyx layer is bound to the membrane of endothelial cells and contributes to the modulating of vascular permeability so that damaged glycocalyx may be also associated with increased permeability of vessels [20]. Plasma possesses three principle macromolecules, including globulins, fibrinogen, and albumin. They are in charge of different tasks like maintaining the pressure balance between blood and interstitial space. In addition, inflammatory cells adhere to endothelial cells so as to pass through endothelial junctions or via the thin endothelial cells directly [19]. Somehow the same probably occurs in OHSS.
In OHSS, the increased capillary permeability is fundamentally the main pathophysiologic feature of massive luteinization of enlarged-ovarian granulosa cells due to high dose hCG (exogenous or endogenous). In addition, some proinflammatory and vasoactive factors have directly or indirectly been involved in this process, resulting in shifting of intravascular fluid into extravascular compartment which is known as third space. The vasoactive factors include interleukin (IL)-1β, transforming growth factor (TGF)-α, TGF-β, endothelin-1, insulin-like growth factor 1 (IGF-1), epidermal growth factor (EGF), von Willebrand factor (VWF), prostaglandin, basic problast growth factor (BPGF), inhibin, prolactin, estrogen, histamine, serotonin, renin-angiotensin-aldosterone system, and most importantly, vascular endothelial growth factor (VEGF) [1,13,21,22,23,24,25]. Among the factors mentioned above, a few of them are not strongly evidenced to approve themselves as key mediators for increasing vascular permeability in OHSS, despite of being supposed as possible factors for enhancing vascular permeability in the past [17]. Therefore, we try to explain more about common recent proved mediators affecting vascular permeability, of which VEGF is the most principle.
2.1.1. VEGF
VEGFs also called vascular permeability factors (VPFs), are signal proteins accompanied by angiogenesis as well as vasculogenesis properties. Indeed, they are the member of the platelet-derived growth factor family of cysteine-knot growth factors. There are 7 types of VEGF, including VEGF-A (i.e. VEGF), VEGF-B, VEGF-C, VEGF-D, the placental growth factor (PlGF), the viral genome-derived VEGF-E, and VEGF-F which is encoded in the venom of some snakes [26,27,28,29,30]. Moreover, there are 3 types of VEGF receptor (VEGFR). To clarify, VEGFR-1 is the receptor for VEGF- A, B, PlGF. VEGFR-2 is the receptor for types A, E, C, and D and VEGFR-3 is the receptor for VEGF-C and D. In humans, VEGFRs are encoded by the FLT genes such as FLT-1 which encodes VEGFR-1, and FLT-4 which encodes VEGFR-3. VEGF- C/D are essential for the regulation of lymph-angiogenesis plus angiogenesis at an early embryogenesis less importantly [29,30,31,32]. VEGF-B is involved in embryonic angiogenesis (specifically, myocardial tissue) [33]. In addition, PlGF plays a main role in pathological angiogenesis (like retinopathy especially those with diabetes retinopathy) and inflammation [34]. Among different kinds of VEGF, type A was discovered initially and is the most responsible type of VEGF playing an important role in this disorder.
2.1.1.1. VEGF-A; Increasing Vascular Permeability
VEGF-A (Figure 2) Actually gets involved in capillary permeability and pro-angiogenic activity. Indeed, it is made by those cells underwent stress conditions, such as endothelial cells. It is expressed during female reproductive cycle remodeling as well as atherosclerosis and cancer [26,31]. VEGF-A like other types of human VEGFs, alternatively spliced so as to generate numerous isoforms accompanied by different properties. Several sorts of VEGF-A isoforms are generated by alternative MRNA splicing from 8-exon VEGF-A gene. According to 8-exon of VEGF gene (terminal exon), the isoforms are categorized in to two different groups: 1) proximal splice site (denoted VEGF×××a) or 2) distal splice site (denoted VEGF×××b). The proximal splice site is expressed in angiogenesis, which causes the proteins get pro-angiogenic, and the distal splice site is expressed in normal tissues, which causes the proteins become anti-angiogenic. Furthermore, inclusion vs. exclusion of exons 6 and 7 enhances VEGF ability to bind plus actuate VEGFRs, due to mediating interactions with neuropilin co-receptors and heparan sulfate proteoglycans (HSPGs) on the cell surface [35]. During OHSS, VEGF-A after getting released into the blood circulation, binds to its specific receptor on the cell surface to exert its effects on the body (Figure 3).
For more specific explanation, endothelial cells connect to each other tightly by some protein complexes which are known as adherens junctional proteins (AJ proteins). There are several kinds of AJ proteins like β-catenin, VE-cadherin, α-catenin, and p 120-catenin. These proteins maintain vascular integrity so as to make a vascular barrier. The barrier is able to breakdown due to some reasons such as endocytosis, phosphorylation, S-nitrosylation, and/or cleavage of these proteins. The vascular barrier integrity is dynamically modulated by VEGFR signaling. As a matter of fact, VEGF enhances VE-cadherin and β-catenin tyrosine (Y)-phosphorylation, followed by capillary leak. Also, it is recently evident that a kind of kinase known as Src-family protein-tyrosine kinase (PTK), is activated by VEGF and plays an important role in promoting AJ phosphorylation. Src-family PTK is also able to get actuated by integrin receptors which cross-talk with VEGF in vascular permeability controlling. To clarify, VE-cadherin phosphorylation at Y658, Y731 or β-catenin phosphorylation at Y654, both by Src mediation, induce complicated AJ stability regulation. Moreover, β-catenin phosphorylation at Y142 disrupts α-catenin binding. In spite of the fact that in-vitro phosphorylation of β-catenin at Y142 by PTK6 has been demonstrated, the modulating of this kind of AJ protein phosphorylation remains unknown in-vivo. There is another type of PTK, called focal adhesion kinase (FAK) which is actuated by both integrins and VEGF. When FAK binds to paxilin, followed by its localization to cell adhesions, and a FAK/αvβ5 integrin signaling structure formation, actin-myosin tension is generated and cell motility increases [29,35,36,37]. Consequently, VEGF-A binds to VEGFR and activates the receptor so that cell signaling induces phosphorylation of AJ proteins resulting in vascular barrier breakdown and increased vascular permeability.
As mentioned above, VEGF-A holds two important impacts on vasculature. First, the increase in vascular permeability, which was explained in the previous paragraphs by the description of OHSS as an example. The next role that should be taken into account is that VEGF-A also plays a principal role in physiological and pathological angiogenesis which occurs in obesity as an instance [29,30,38].
3. Obesity
Obesity incidence is aggregating over the last few decades, leading to be one of the main health problems worldwide [39,40]. According to WHO, approximately 20% of adult population around the world, will suffer from obesity by 2025 [40,41]. To clarify the concept of obesity, we should state that the imbalance between energy intake and energy consumption underlies obesity and overweight. [42,43,44,45,46]. The next thing which is deserved to be pay attention is that changes in diet quality might also cause obesity [47]. Obesity is in fact a complex chronic disorder, which is specified as three sorts; generalized obesity (BMI ≥ 30 kg/m2), extreme obesity (BMI > 40 kg/m2), and central obesity in which the abdomen fat gets accumulated excessively [44,48,49]. There are a number of factors such as epigenetic changes, increasing the risk of obesity. Epigenetics is in fact a phenomenon in which some variables like nutrition and lifestyle lead to make some alterations in gene expression in terms of histone modification, non-coding RNA, and DNA methylation, without any changes in DNA sequence [50,51]. Other predisposing factors include genetic factors, inadequate physical activity, socioeconomic status, excess caloric consumption, sleep deprivation, medical conditions like hypothyroidism and insolinoma, psychosocial stress and mental disorders [43,44,52,53]. Furthermore, it would be such an interesting point that researchers categorized the genetic type into three groups: first, monogenic obesity which is caused by a mutation of a single gene that is involved in the leptin-melanocortin pathway that regulates energy homeostasis. In this type, the major characteristically feature is hyperplasia: secondly, polygenic obesity which results from the occurrence of multiple gene variants concurrently; third, syndromic obesity which is accompanying other signs of developmental diseases such as, Bardet-Biedel, MOMO, Cohen, and Prader will syndrome [49,52,54,55,56]. For management of genetic obesity, a combination treatment is required, including administering medicine, rectifying patients’ lifestyles, plus bariatric surgeries [49]. Scholars demonstrated that obesity particularly causes several adverse health consequences for human body. As a matter of fact, obesity promotes some undesirable outcomes attributed, in part, to type two diabetes mellitus, hypertension, sleep apnea, endometriosis, liver cirrhosis, dyslipidemia, PCOS, infertility, metabolic syndrome, arthritis, cardiovascular diseases, etc. [52,53,54,57]. Evidence demonstrates that obesity is able to elevate the risk of some pregnancy-related complications, such as pregnancy loss, gestational hypertension, gestational diabetes, miscarriage, maternal death, and so on [58,59]. Moreover, obesity, as a systemic inflammatory condition, adversely increases the risk of some types of cancers which are related to vascular dysfunctioning, including liver and gastrointestinal cancers [39,44,45,51,54]. As get informed, Obesity has been revealed as a metabolic state in which excess in storage of triglycerides in adipose tissues occurs gradually [46,59].
3.1. Adipose Tissue
Adipose tissue is distinguished as an endocrine organ [42,45,54]. It comprises of mixtures various adipocytes which are covered by stromal vascular cells, as well as fibroblasts and macrophages. These vasculature yields a condensed network of blood capillaries around the adipocytes [42,54,60]. Additionally, scholars recognized that there are different kinds of adipocytes in their functions despite of similar morphology. For instance, thermogenic adipocytes which conserve core body temperature. This kind of adipocyte exists around central organs. Some other examples include perivascular, mesenteric, and subcutaneous adipocytes. the latter instance is regarded as the largest depot and is capable of getting expanded as a reaction to excess food intake [60]. If we take a more totally look at adipose tissues, we realize that they comprise two types in human body; white adipose tissue (WAT), and brown adipose tissue (BAT). Researchers found out some different features between these two kinds. WAT is assigned for energy storage in the form of triglycerides. Moreover, WAT works as an endocrine organ, secreting some hormones such as gerlin and leptin, which are called adipokines. Nevertheless, BAT is specialized for thermogenesis in addition to energy expenditure due to mitochondria function which exist in this sort of adipocytes at high concentrated levels plus high density vasculature [38,54,61,62,63]. Overall, adipose tissue has the capability to get expanded by some triggering situations which include fasting and excess food intake. During the former condition, the body attains benefits from the adipose tissue expansion due to providing the ability to store fuels for using. The latter situation actually brings some drawbacks for the body so that causes obesity plus in turn its comorbidities [60]. The adipose tissue expansion can occur through two distinct mechanisms which consist of hypertrophic expansion (increase in size of adipocytes) and hyperplastic expansion (formation of new adipose cells) [54,59,62,64]. Both of these mechanisms are able to happen in adults, specifically hypertrophy which sets out to get generated by excess caloric intake [60,62]. During hypertrophy in adipose tissues, angiogenesis occurs because of overexpression of VEGF-A [54,60].
3.1.1. VEGF-A, Angiogenesis
As described above, overfeeding leads to hypertrophy of adipocytes eventually. The increase in size of adipocytes yields several negative impacts on the adipose tissues which include tissue hypoxia [51,54,62,63]. Indeed, adipose tissue dysfunctions contribute to adiposopathy for which there are two parts (anatomic & functional). For more explanation, the anatomic changes of adiposopathy are such as adipose tissue expansion and augmented levels of fat deposition in organs of the body. Nevertheless, functional changes include adipose tissue dysfunctions through endocrine and immunology responses, increased amounts of reactive oxygen species, tissue hypoxia, etc. [42,64]. actually, some researchers state that these results especially adipocyte hypoxia might be because of either the compression effect of large adipocytes on vasculature by creating a niche or impairing capillary function through depressing capability of vessels to eliminate extracellular fatty acids. Furthermore, some other researchers hypothesized that the event of hypoxia in adults’ adipose tissues following adipocytes hypertrophy occurs due to the impacts of excess calories on both vasculature function and adipocytes [42,60,65]. Anyway, after generating tissue hypoxia in which the tissue receives inadequate blood flow, in turn the adipose tissue function gets disrupted and here is an alarm for the body, since hypoxia finally can lead to endothelial cells death. Therefore, the endothelial cells begin to overexpression of cytokines and angiogenic factors such as VEGF-A [29,60,66]. It should be emphasized that the VEGF-A is able to yield both angiogenesis and anti-angiogenesis on the capillaries [38,60]. This against effect on endothelial cells comes from conversed effects of receptors on the cells. As a matter of fact, when VEGF-A locates on VEGFR 1, the anti-angiogenic property starts to happen. Nevertheless, when VEGFR 2 gets activated by VEGF-A, it shows angiogenic features [30,31,38]. As hypoxia is one of the stimulators of endothelial cells due to capillary rarefaction, the aim of releasing high amounts of VEGF-A would consequences angiogenesis in order to take the adequate blood flow to the tissue [29,42,63,65]. For more explanation, VEGF-A sits on VEGFR 2 on endothelial cell wall. The mentioned receptor gets phosphorylated and is activated to generate intra cellular signaling such as PLC (phosphoinositide phospholipase C)- dependent pathway. This pathway consists of two mechanisms, including NOS-dependent signaling and mitogen-activated protein kinase (MAPK) cascade that both of them Finally, induce gene expression, mitogenesis, cell proliferation, and cell survival, thereby angiogenesis [29,31,67]. To clarify, VEGFR-2 activated leads tyrosine phosphorylation of PLCγ1 for which the activity of Src- family kinases are the requirements. phosphorylated PLCγ1 aggregates the level of inositol triphosphate (IP3) plus Ca2+ inside the endothelial cells which in turn leads to increased production of NO. Additionally, phosphorylated PLCγ1 activates MAPK cascades. Both NOS and MAPK cascade result in endothelial cells proliferation [29,31]. Then the basement membrane of the capillaries gets cleaved, allowing proliferated endothelial cells to incur into the adipose tissue stroma and make a lumen by endothelial cells migration. The following results include arranging extended blood capillaries which makes a dense network of vasculature in the adipose tissue [30,54,65].
4. Conclusion
We reviewed the different results of VEGF-A overexpression on blood vessels during two distinct situations; OHSS is one of the important IVF complications; leads to secretion of some mediators like VEGF, cytokines, renin-angiotensin system substances, etc. Among these vasoactive mediators, VEGF is considered as the main factor resulting in vascular permeability increase. In order to achieve this goal, VEGF-A binds to its receptor. Then, VEGFR2 activation generates a cell signaling which includes AJ protein phosphorylation. Since AJ stability underlies tight endothelial cell junction, the vascular barrier breakdown occurs due to phosphorylation of AJ proteins. Therefore, vascular permeability increases and intravascular fluid simply shifts into third space. On the other hand, during obesity something different occurs by VEGF-A; obesity prevalence has been increased during recent years due to environmental, genetic factors and so on. Due to adipose tissue expansion, tissue hypoxia occurs thereby cytokines and angiogenic factors such as VEGF-A release in order to repair capillary rarefaction. During this process, VEGF-A locate on VEGFR2, thereby activates NOS-dependent signaling and MAPK cascade by phosphorylation of PLCγ1. This event results in endothelial proliferation which then migrate and create denser network of capillaries in adipose tissue.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Farkas B, Boldizsar F, Bohonyi N, Farkas N, Marczi S, Kovacs GL, et al. Comparative analysis of abdominal fluid cytokine levels in ovarian hyperstimulation syndrome (OHSS). Journal of Ovarian Research. 2020;13(1):1-8. [CrossRef]
- Timmons D, Montrief T, Koyfman A, Long B. Ovarian hyperstimulation syndrome: a review for emergency clinicians. The American journal of emergency medicine. 2019;37(8):1577-84. [CrossRef]
- Hazlina NHN, Norhayati MN, Bahari IS, Arif NANM. Worldwide prevalence, risk factors and psychological impact of infertility among women: a systematic review and meta-analysis. BMJ open. 2022;12(3):e057132. [CrossRef]
- Sharma R, Biedenharn KR, Fedor JM, Agarwal A. Lifestyle factors and reproductive health: taking control of your fertility. Reproductive biology and endocrinology. 2013;11(1):1-15. [CrossRef]
- Zhu Y, Fu Y, Tang M, Yan H, Zhang F, Hu X, et al. Risk of Higher Blood Pressure in 3 to 6 Years Old Singleton Born From OHSS Patients Undergone With Fresh IVF/ICSI. Frontiers in Endocrinology. 2022;13. [CrossRef]
- Chen M, Heilbronn L. The health outcomes of human offspring conceived by assisted reproductive technologies (ART). Journal of developmental origins of health and disease. 2017;8(4):388-402. [CrossRef]
- Fang L, Yu Y, Li Y, Wang S, He J, Zhang R, et al. Upregulation of AREG, EGFR, and HER2 contributes to increased VEGF expression in granulosa cells of patients with OHSS. Biology of reproduction. 2019;101(2):426-32. [CrossRef]
- Christ J, Herndon CN, Yu B. Severe ovarian hyperstimulation syndrome associated with long-acting GnRH agonist in oncofertility patients. Journal of Assisted Reproduction and Genetics. 2021;38(3):751-6. [CrossRef]
- Akalewold M, Yohannes GW, Abdo ZA, Hailu Y, Negesse A. Magnitude of infertility and associated factors among women attending selected public hospitals in Addis Ababa, Ethiopia: a cross-sectional study. BMC Women's Health. 2022;22(1):1-11. [CrossRef]
- Jahromi BN, Parsanezhad ME, Shomali Z, Bakhshai P, Alborzi M, Vaziri NM, et al. Ovarian hyperstimulation syndrome: a narrative review of its pathophysiology, risk factors, prevention, classification, and management. Iranian journal of medical sciences. 2018;43(3):248.
- Liu F, Jiang Q, Sun X, Huang Y, Zhang Z, Han T, et al. Lipid metabolic disorders and ovarian hyperstimulation syndrome: a retrospective analysis. Frontiers in Physiology. 2020;11:491892. [CrossRef]
- Humaidan P, Nelson S, Devroey P, Coddington C, Schwartz L, Gordon K, et al. Ovarian hyperstimulation syndrome: review and new classification criteria for reporting in clinical trials. Human Reproduction. 2016;31(9):1997-2004. [CrossRef]
- Sun B, Ma Y, Li L, Hu L, Wang F, Zhang Y, et al. Factors associated with ovarian hyperstimulation syndrome (OHSS) severity in women with polycystic ovary syndrome undergoing IVF/ICSI. Frontiers in endocrinology. 2021;11:615957. [CrossRef]
- Abbara A, Islam R, Clarke S, Jeffers L, Christopoulos G, Comninos A, et al. Clinical parameters of ovarian hyperstimulation syndrome following different hormonal triggers of oocyte maturation in IVF treatment. Clinical endocrinology. 2018;88(6):920-7. [CrossRef]
- Bergandi L, Canosa S, Carosso AR, Paschero C, Gennarelli G, Silvagno F, et al. Human recombinant FSH and its Biosimilars: clinical efficacy, safety, and cost-effectiveness in controlled ovarian stimulation for in vitro fertilization. Pharmaceuticals. 2020;13(7):136. [CrossRef]
- Braam S, de Bruin J, Mol B, van Wely M. The perspective of women with an increased risk of OHSS regarding the safety and burden of IVF: a discrete choice experiment. Human reproduction open. 2020;2020(2):hoz034. [CrossRef]
- Pakhomov S, Orlova V, Verzilina I, Sukhih N, Nagorniy A, Matrosova A. Risk Factors and Methods for Predicting Ovarian Hyperstimulation Syndrome (OHSS) in the in vitro Fertilization. Archives of Razi Institute. 2021;76(5):1461-8. [CrossRef]
- Li S, Qian Y, Pei Y, Wu K, Lu S. Coagulation and Fibrinolysis Biomarkers as Potential Indicators for the Diagnosis and Classification of Ovarian Hyperstimulation Syndrome. Frontiers in Medicine. 2021:1430. [CrossRef]
- Claesson-Welsh, L. Vascular permeability—the essentials. Upsala journal of medical sciences. 2015;120(3):135-43. [CrossRef]
- Wautier J-L, Wautier M-P. Vascular Permeability in Diseases. International Journal of Molecular Sciences. 2022;23(7):3645. [CrossRef]
- Liu K, Yang W, Hu M, Xie W, Huang J, Cui M, et al. Exosomal miR-27 negatively regulates ROS production and promotes granulosa cells apoptosis by targeting SPRY2 in OHSS. Journal of cellular and molecular medicine. 2021;25(8):3976-90. [CrossRef]
- Elchalal U, Schenker JG. The pathophysiology of ovarian hyperstimulation syndrome--views and ideas. Human reproduction (Oxford, England). 1997;12(6):1129-37. [CrossRef]
- Morris RS, Wong IL, Do YS, Hsueh WA, Lobo RA, Sauer MV, et al. The Pathophysiology of Ovarian Hyperstimulation Syndrome (OHSS). Tissue Renin-Angiotensin Systems. 1995:391-8. [CrossRef]
- Elmahal M, Lohana P, Anvekar P, Menda MK. Hyponatremia: An Untimely Finding in Ovarian Hyper-Stimulation Syndrome. Cureus. 2021;13(7). [CrossRef]
- Medicine PCotASfR. Ovarian hyperstimulation syndrome. Fertility and sterility. 2008;90(5):S188-S93. [CrossRef]
- Bates DO. Vascular endothelial growth factors and vascular permeability. Cardiovascular research. 2010;87(2):262-71. [CrossRef]
- Yamazaki Y, Matsunaga Y, Tokunaga Y, Obayashi S, Saito M, Morita T. Snake venom Vascular Endothelial Growth Factors (VEGF-Fs) exclusively vary their structures and functions among species. Journal of Biological Chemistry. 2009;284(15):9885-91. [CrossRef]
- Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS, Dvorak HF. Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science. 1983;219(4587):983-5. [CrossRef]
- Claesson-Welsh L, Welsh M. VEGFA and tumour angiogenesis. Journal of internal medicine. 2013;273(2):114-27. [CrossRef]
- Bokhari SMZ, Hamar P. Vascular endothelial growth factor-D (VEGF-D): An angiogenesis bypass in malignant tumors. International Journal of Molecular Sciences. 2023;24(17):13317. [CrossRef]
- Shibuya M. Vascular endothelial growth factor (VEGF) and its receptor (VEGFR) signaling in angiogenesis: a crucial target for anti-and pro-angiogenic therapies. Genes & cancer. 2011;2(12):1097-105. [CrossRef]
- Shibuya M, Yamaguchi S, Yamane A, Ikeda T, Tojo A, Matsushime H, et al. Nucleotide sequence and expression of a novel human receptor-type tyrosine kinase gene (flt) closely related to the fms family. Oncogene. 1990;5(4):519-24.
- Claesson-Welsh, L. VEGF-B taken to our hearts: specific effect of VEGF-B in myocardial ischemia. Am Heart Assoc; 2008. p. 1575-6. [CrossRef]
- Van Bergen T, Etienne I, Cunningham F, Moons L, Schlingemann RO, Feyen JH, et al. The role of placental growth factor (PlGF) and its receptor system in retinal vascular diseases. Progress in retinal and eye research. 2019;69:116-36. [CrossRef]
- Chen XL, Nam J-O, Jean C, Lawson C, Walsh CT, Goka E, et al. VEGF-induced vascular permeability is mediated by FAK. Developmental cell. 2012;22(1):146-57. [CrossRef]
- Adam AP, Sharenko AL, Pumiglia K, Vincent PA. Src-induced Tyrosine Phosphorylation of VE-cadherin Is Not Sufficient to Decrease Barrier Function of Endothelial Monolayers*♦. Journal of Biological Chemistry. 2010;285(10):7045-55. [CrossRef]
- Abedi H, Zachary I. Vascular endothelial growth factor stimulates tyrosine phosphorylation and recruitment to new focal adhesions of focal adhesion kinase and paxillin in endothelial cells. Journal of Biological Chemistry. 1997;272(24):15442-51. [CrossRef]
- Elias I, Franckhauser S, Bosch F. New insights into adipose tissue VEGF-A actions in the control of obesity and insulin resistance. Adipocyte. 2013;2(2):109-12. [CrossRef]
- Tzenios, N. OBESITY AS A RISK FACTOR FOR DIFFERENT TYPES OF CANCER. EPRA International Journal of Research and Development (IJRD). 2023;8(2):97-100. [CrossRef]
- Lobstein T, Brinsden H, Neveux M. World obesity atlas 2022. 2022.
- Wen X, Zhang B, Wu B, Xiao H, Li Z, Li R, et al. Signaling pathways in obesity: mechanisms and therapeutic interventions. Signal Transduction and Targeted Therapy. 2022;7(1):298. [CrossRef]
- AlZaim I, de Rooij LP, Sheikh BN, Börgeson E, Kalucka J. The evolving functions of the vasculature in regulating adipose tissue biology in health and obesity. Nature Reviews Endocrinology. 2023:1-17. [CrossRef]
- Kim C, Fryar C, Ogden CL. Epidemiology of obesity. Handbook of epidemiology: Springer; 2023. p. 1-47. [CrossRef]
- Hu FB. Obesity in the USA: diet and lifestyle key to prevention. The Lancet Diabetes & Endocrinology. 2023;11(9):642-3. [CrossRef]
- Organization WH. WHO European regional obesity report 2022: World Health Organization. Regional Office for Europe; 2022.
- Elkhawaga SY, Ismail A, Elsakka EG, Doghish AS, Elkady MA, El-Mahdy HA. miRNAs as cornerstones in adipogenesis and obesity. Life Sciences. 2023:121382. [CrossRef]
- Mozaffarian, D. Perspective: Obesity—an unexplained epidemic. The American Journal of Clinical Nutrition. 2022;115(6):1445-50. [CrossRef]
- Purnell, JQ. Definitions, classification, and epidemiology of obesity. Endotext [Internet]. 2023.
- Mahmoud R, Kimonis V, Butler MG. Genetics of obesity in humans: A clinical review. International Journal of Molecular Sciences. 2022;23(19):11005. [CrossRef]
- Mahmoud, AM. An overview of epigenetics in obesity: The role of lifestyle and therapeutic interventions. International Journal of Molecular Sciences. 2022;23(3):1341. [CrossRef]
- Lazarus E, Bays HE. Cancer and obesity: an obesity medicine association (OMA) clinical practice statement (CPS) 2022. Obesity Pillars. 2022;3:100026. [CrossRef]
- Masood B, Moorthy M. Causes of obesity: a review. Clinical Medicine. 2023;23(4):284. [CrossRef]
- Sørensen TI, Martinez AR, Jørgensen TSH. Epidemiology of obesity. From Obesity to Diabetes: Springer; 2022. p. 3-27. [CrossRef]
- Nijhawans P, Behl T, Bhardwaj S. Angiogenesis in obesity. Biomedicine & Pharmacotherapy. 2020;126:110103. [CrossRef]
- Martin WP, Le Roux C. Obesity is a disease. Bariatric Surgery in Clinical Practice. 2022. [CrossRef]
- Loos RJ, Yeo GS. The genetics of obesity: from discovery to biology. Nature Reviews Genetics. 2022;23(2):120-33. [CrossRef]
- Venkatesh SS, Ferreira T, Benonisdottir S, Rahmioglu N, Becker CM, Granne I, et al. Obesity and risk of female reproductive conditions: A Mendelian randomisation study. PLoS medicine. 2022;19(2):e1003679. [CrossRef]
- Langley-Evans SC, Pearce J, Ellis S. Overweight, obesity and excessive weight gain in pregnancy as risk factors for adverse pregnancy outcomes: a narrative review. Journal of Human Nutrition and Dietetics. 2022;35(2):250-64. [CrossRef]
- Creanga AA, Catalano PM, Bateman BT. Obesity in pregnancy. New England Journal of Medicine. 2022;387(3):248-59. [CrossRef]
- Corvera S, Solivan-Rivera J, Yang Loureiro Z. Angiogenesis in adipose tissue and obesity. Angiogenesis. 2022;25(4):439-53. [CrossRef]
- Lustig RH, Collier D, Kassotis C, Roepke TA, Kim MJ, Blanc E, et al. Obesity I: Overview and molecular and biochemical mechanisms. Biochemical Pharmacology. 2022;199:115012. [CrossRef]
- Horwitz A, Birk R. Adipose Tissue Hyperplasia and Hypertrophy in Common and Syndromic Obesity—The Case of BBS Obesity. Nutrients. 2023;15(15):3445. [CrossRef]
- Lemoine AY, Ledoux S, Larger E. Adipose tissue angiogenesis in obesity. Thrombosis and haemostasis. 2013;110(10):661-9. [CrossRef]
- Fitch AK, Bays HE. Obesity definition, diagnosis, bias, standard operating procedures (SOPs), and telehealth: an Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022. Obesity Pillars. 2022;1:100004. [CrossRef]
- Corvera S, Gealekman O. Adipose tissue angiogenesis: impact on obesity and type-2 diabetes. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease. 2014;1842(3):463-72. [CrossRef]
- Zhou W, Liu K, Zeng L, He J, Gao X, Gu X, et al. Targeting VEGF-A/VEGFR2 Y949 signaling-mediated vascular permeability alleviates hypoxic pulmonary hypertension. Circulation. 2022;146(24):1855-81. [CrossRef]
- Herold J, Kalucka J. Angiogenesis in adipose tissue: the interplay between adipose and endothelial cells. Frontiers in physiology. 2021;11:624903. [CrossRef]
Figure 1.
The most important clinical presentations and laboratory features of OHSS divided into 4 stages. HCT; hematocrit, WBC; white blood cell, SOB; shortness of breath, ARDS; acute respiratory distress syndrome, N/V; nausea/vomiting, IAH; intra-abdominal hypertension, ACS; abdominal compartment syndrome.
Figure 1.
The most important clinical presentations and laboratory features of OHSS divided into 4 stages. HCT; hematocrit, WBC; white blood cell, SOB; shortness of breath, ARDS; acute respiratory distress syndrome, N/V; nausea/vomiting, IAH; intra-abdominal hypertension, ACS; abdominal compartment syndrome.
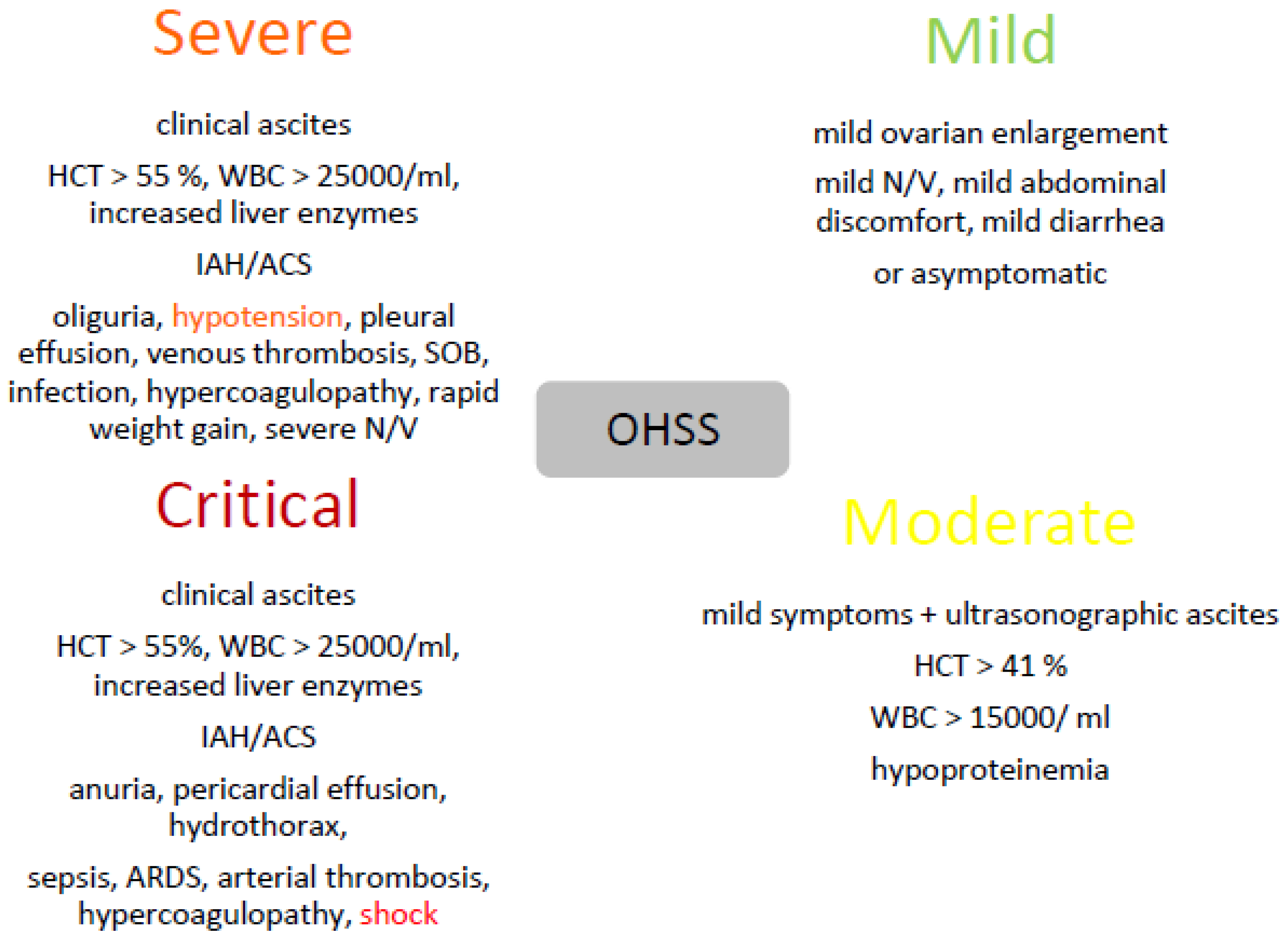
Figure 2.
Structure of the VEGFA protein. Based on PyMOL rendering of PDB 1bj1. Source: Wikimedia Commons. URL: https://commons.wikimedia.org/wiki/user:Emw.
Figure 2.
Structure of the VEGFA protein. Based on PyMOL rendering of PDB 1bj1. Source: Wikimedia Commons. URL: https://commons.wikimedia.org/wiki/user:Emw.
Figure 3.
VEGFRs and cell signaling; after binding VEGF-A to VEGFR-2, a special cell signaling sets out to degrade AJ proteins between endothelial cells so that yields increased vascular permeability. PlGF; placental growth factor, FAK; focal adhesion kinase.
Figure 3.
VEGFRs and cell signaling; after binding VEGF-A to VEGFR-2, a special cell signaling sets out to degrade AJ proteins between endothelial cells so that yields increased vascular permeability. PlGF; placental growth factor, FAK; focal adhesion kinase.
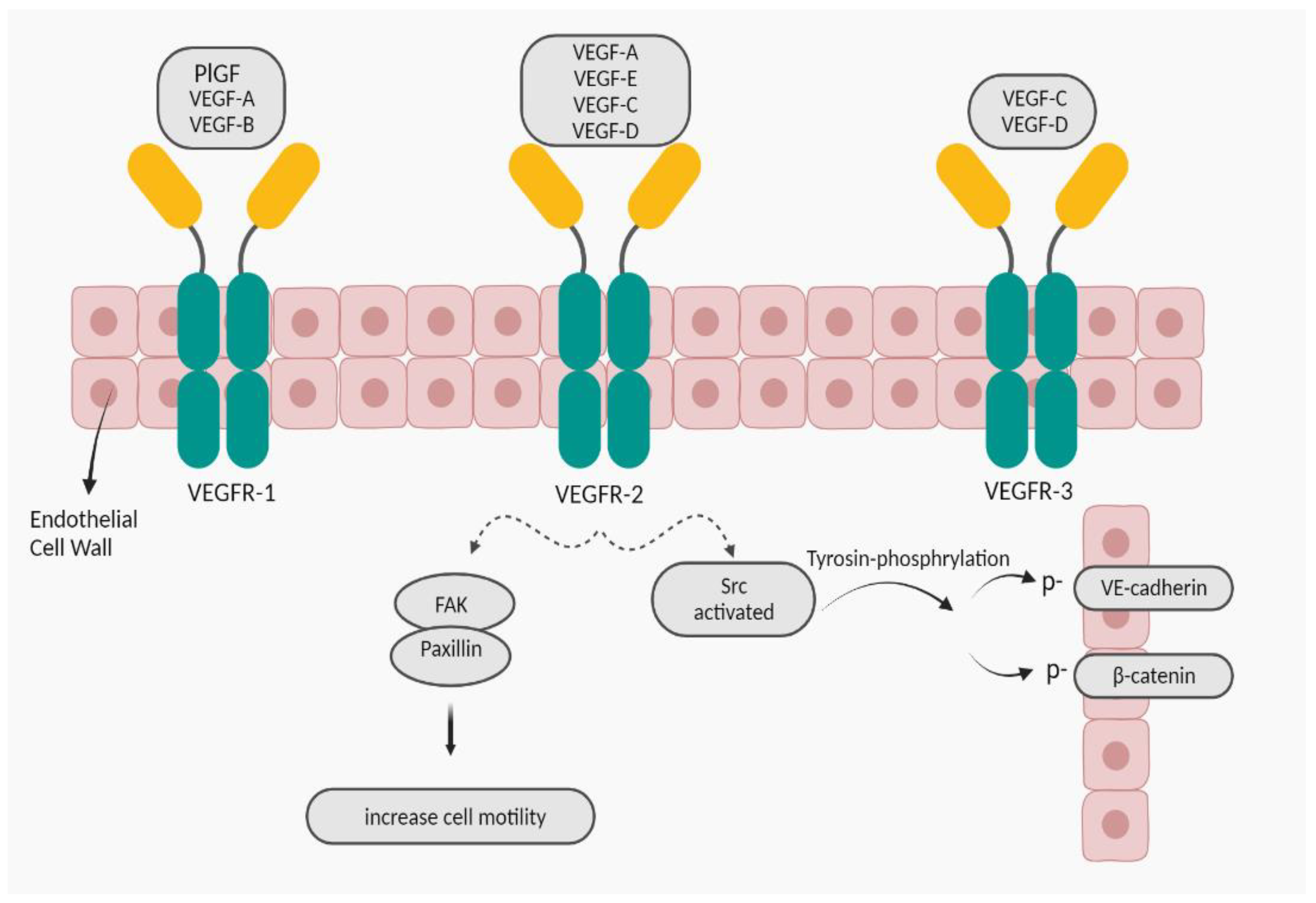

Table 1.
The most common risk factors for OHSS.
| PCOS |
| AFC > 8 |
| Age < 30 |
| AMH > 3.36 ng/ml |
| Low BMI |
| Previous OHSS |
| Serum estradiol levels > 2500 pg/ml during COH |
| Small ovarian follicle count > 14 |
| A large number of retrieved oocytes > 20 |
| hCG administration |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



