
Submitted:
01 December 2023
Posted:
05 December 2023
You are already at the latest version
Abstract
Haemolytic anaemia represents a risk factor for the development of pulmonary hypertension (PH), currently classified as World Health Organization group 5 PH and data regarding appropriate therapeutic strategy are limited. A total of 28 patients, 85.7% with thalassemia and 14,3% with sickle cell disease, with a diagnosis of PH confirmed by right heart catheterization, were included in the study. The patients were divided into three groups according to haemodynamics and overall diagnostic approach: 42,9% had precapillary PH (Pulmonary Arterial Hypertension -PAH group), 25% post-capillary PH and 32.1% Chronic Thromboembolic PH (CTEPH) (29% of b-thalassemia and 50% of SCD patients). The therapeutic approach in each group and its impact on the outcome and haemodynamics was recorded. PAH-specific drug therapy received 82.1% of patients and Balloon Pulmonary Angioplasty (BPA) was performed in 6 patients with CTEPH. There were statistically significant differences in baseline mPAP and PVR values between the CTEPH-haemolytic anaemia group and other groups. PAH-specific drug therapy resulted in haemodynamic improvement for PAH-group. Patients who underwent BPA improved Pulmonary Haemodynamics. Median survival time was 162 months and the survival rate was 1yr-100%, 2,3,4,5,6 years 96%, 9yrs 90% and 13yrs 78%. In patients with haemolytic anaemia, the wide spectrum of induced PH highlights the importance of a correct diagnosis. BPA in CTEPH patients and specific-PAH drug therapy for PAH patients represent potential therapeutic strategies, however the management should be offered in expert PH centers under patients’ individualized approach.
Keywords:
Pulmonary Hypertension
; Haemolytic anemia
; Haematological Disorders
; Chronic Thromboembolic Pulmonary Hypertension
; Pulmonary Arterial Hypertension
; Balloon Pulmonary Angioplasty
1. Introduction
Hereditary Hemoglobin disorders affecting the globin chain synthesis, thalassemia syndromes and Sickle cell disease (SCD) represent common genetic diseases as around of 7% of the world population carries genes for these disorders [1,2]. Pulmonary Hypertension (PH) is a major complication, due to increased Pulmonary Vascular Resistance (PVR), leading to Right Ventricular Dysfunction and Right Heart Failure, representing a major cause of mortality and morbidity in chronic haemolytic anaemias [3,4]. PH is defined as an increase in mean pulmonary arterial pressure (mPAP) of more than 20mmHg at rest assessed by Right Heart Catheterization (RHC); in all PH forms Pulmonary Arterial Wedge Pressure (PAWP) is lower than 15mmHg (Precapillary PH) except Group II PH due to Left Heart Disease (PH-LHD) characterized by PAWP more than 15mmHg (postcapillary PH) [5]. he pathogenesis of PH in haemolytic anaemia patients has not been fully clarified, however accumulating evidence indicates that haemolysis, reduced nitric oxide bioavailability, increased endothelin-1 mediated responses, arginine metabolism dysregulation, compromised oxygenation and chronic hypoxia as also hypercoagulability play crucial roles in the development of the disease [6]. A variety of underlying mechanisms can lead to different forms of PH [7,8] as Pulmonary Arterial Hypertension (PAH), Chronic Thromboembolic PH (CTEPH), or PH due to Left Heart Disease (PH-LHD). Thus, haemolytic Anaemias are included in group 5 PH according to the latest guidelines [5], group defined as PH with unclear and multifactorial mechanisms. This classification does not permit a widely accepted standard therapeutic strategy for PH haemolytic anaemia patients and highlights the importance of prompt diagnosis. Considering the unmet goal of the appropriate therapeutic approach for those patients, we retrospectively studied our haemolytic anaemia population.
2. Materials and Methods
2.1. Patient selection
This single-center, retrospective observational study was approved by the Institutional Review Board of Onassis Cardiac Surgery Center (approval number 2020-686). The need for written informed consent was waived because of the retrospective nature of the study. A total of 28 consecutive patients, 24 (85.7%) with thalassemia and 4 patients (14.3%) with SCD suffering from PH were included. The diagnosis of PH was established by Right Heart Catheterization according to the proposed definition of 2015 guidelines for the diagnosis and treatment of PH. Haemodynamic and echocardiographic parameters were studied. The patients were divided in three groups based on haemodynamics and overall diagnostic approach, according to 2015 ESC/ERS guidelines [6] (Figure 1). CTEPH diagnosis was verified via Lung Ventilation Perfusion Scanning and invasive Pulmonary Angiography. Precapillary PH (PAH-like group) was identified in 12 patients (42.9%), 7 patients (25%) had post-capillary PH (Group II-PH) and 9 patients (32.1%) were classified in group IV PH as CTEPH was diagnosed (29% of b-thalassemia and 50% of SCD patients). For the SCD group, 50% (2 patients) were diagnosed with CTEPH, one patient with Group II PH and the last one with PAH-like PH. Eleven among 24 (45.8%) b-thalassemia patients had PAH-like PH, 6 (25%) were classified as Group II PH and 7 (29.2%) patients with CTEPH.
2.2. Data collection
Data concerning medical history, medication, and comorbidities were obtained from medical records. Echocardiographic parameters (right ventricular fractional area change (RVFAC), right atrial area (RAA) and tricuspid annular plane systolic excursion (TAPSE)/pulmonary arterial systolic pressure (PASP)), and hemodynamic parameters (mPAP, PASP, PAWP, right atrial pressure (RAP), cardiac output estimated by Fick method, and pulmonary vascular resistance [PVR]) were collected at baseline and at the last available follow-up visit.
Right-heart catheterization was performed at the beginning of each BPA procedure. For the post-treatment analysis of haemodynamics the catheterization performed before the last BPA procedure was used, except for one patient where a follow-up catheterization after the end of treatment was available. BPA was performed in a series of staged procedures at several intervals depending on patients’ preference. The target of BPA was to achieve an mPAP < 30 mmHg with concomitant cessation of oxygen therapy.
The follow-up period for analyses of survival data for the study population ended in September 2023.
2.3. Statistical Analysis
Data are presented as mean ± standard deviation for continuous variables with normal distribution, and as median and interquartile range for non-normally distributed variables. Differences in continuous variables before and after treatment were compared using the paired t-test for normally distributed variables and the Wilcoxon paired test for non-normally distributed variables. The normality was assessed with the Shapiro-Wilk test. Categorical variables are expressed as number and percentage and are compared using the χ2 test for independence or Fisher’s exact test. Kruskal-Wallis test or one-way ANOVA with post hoc analysis were used as appropriate for comparisons between groups. Receiver operating characteristic analyses were used to determine cut-off values for selected variables. The Kaplan–Meier method was used to estimate overall survival and differences between survival curves were assessed using the log-rank test. For the survival analysis, the date of PH diagnosis was used as the start point to determine length of survival. The cut-off date was October 12, 2023. The Kaplan–Meier curve was supplemented by the proportion surviving at analyzed times. A p-value < 0.05 was considered statistically significant in this study. Data were analyzed using the SPSS version 16.0. (IBM SPSS Statistics for Windows, Version 16.0. Armonk, NY, USA).
3. Results
3.1. Baseline Haemodynamic and Echocardiographic Characteristics
The age at PH diagnosis was 48±9 years (33-65) and 15 patients (53.6%) were females. Three patients had a history of Pulmonary Embolism, 9 patients had atrial fibrillation and 3 patients had Diabetes mellitusFor the whole group, mean Pulmonary Arterial Pressure (mPAP) was 41.0±9.8 mmHg, PAWP 13.2±4.7 mmHg, Cardiac Index (C.I.) 2.7±0.7 l/min/m2, Pulmonary Vascular Resistance (PVR) 6.3±3.0 WU, venous Oxygen Saturation (SVO2) 63.5±9.8%, Pulmonary Arterial Compliance (PAC) 1.69±1.3, Right Atrial Pressure (RAP) 10.4±4.9 mmHg and Systolic Pulmonary Arterial Pressure (PASP) 65.5±17.7 mmHg. Patients were also studied by echocardiography. Right Ventricular Fractional Area (RVFAC) was 41.9±4%, Tricuspid Annulus Plane Systolic Excursion (TAPSE) /PASP 0.47±0.16 and Right Atrial Area (RA area) 16.1±4 cm2.
Haemodynamic characteristics show some significant differences among the 3 groups population (Table 1). CTEPH group was more severely compromised according to their haemodynamic parameters than the two other groups in terms of PASP, mPAP, PVR and SvO2 (p< 0.05).
CTEPH patients had more severe PH compared to patients with PAH, as mPAP was 50.4±6.2 vs 36±7.6 mmHg (p: 0.01), PVR 8.5±2.4 vs 5.7±3 WU (p=0.038) and SVO2 52.5±10% vs 68.3±5.9% (p<0.01) (Table 2). Apart from haemodynamic parameters, the burden of CTEPH patients is also reflected in echocardiographic indices of right ventricular function such as Right Ventricular Fractional Area Change (RVFAC) and Tricuspid Annulus Plane Systolic Excursion (TAPSE) /PASP, parameters significantly lower compared to patients with precapillary PH (RVFAC 30±2.5 vs 42.8±5%, p<0.01 and TAPSE/SPAP 0.27±0.05 vs 0.5±0.17, p=0.05, respectively). RVFAC was also significantly lower in CTEPH patients compared to postcapillary group -Group II PH (38.3±3.8%, p=0.013), while no differences were noticed in these indices between pre and postcapillary patients. Patients with precapillary PH classified as PAH-group had significant lower RAP 7.7±4 vs 13.5±3.7 mmHg (p=0.029) and PAWP 10.8±4 vs 19±1 mmHg (<0.01) compared to patients with postcapillary PH. No differences were noted in other haemodynamic parameters between these two groups.
3.2. Therapeutic approach
PAH-specific drug therapy was prescribed in 23 (82.1%) patients (Table 2). Endothelin Receptor Antagonist (ERA) was prescribed in 15 (65.2%) patients (ambrisentan in 39.1%, bosentan in 17.4% and macitentan in 8.7%), Phosphodiesterase-5 inhibitors (PDE-5) in 6 (26%) patients and Riociguat in 8 (34.5%) of patients. Considering SCD group, three patients received Riociguat and a patient combination therapy with ERA and Selexipag. Sixteen patients received monotherapy and 7 patients double PAH drug therapy. One patient with precapillary PH did not receive drug therapy as mild PH was identified (mPAP 26mmHg). The majority of patients with postcapillary PH (57.1%) did not receive specific PAH drugs.
3.3. Hemodynamic Parameters at follow up
3.3.1. PAH-like group
Nine out of 12 PAH group patients had baseline and post-treatment available haemodynamic parameters. An improvement was noted in PASP, PVR and PAC for patients who received PAH specific drugs (Table 3). Furthermore, in 10 patients studied by echocardiography before and after treatment, a significant improvement in TAPSE/PASP was noticed (0.47±0.16 vs 0.69±0.22, p=0.039).
3.3.2. PH Group II (PH-LHD)
Five out of 7 patients with postcapillary PH had a follow-up catheterization and among all aforementioned haemodynamic parameters, only RAP was significantly improved(14.2±3.3 vs 9.4±2.0 mmHg, p=0.026) (Table 4). Three patients received PAH-specific drug therapy. Patients 1, 2 and 3 had mPAP 39mmHg, 32mmHg and 56 mmHg respectively and PVR 3.1, 4.3 and 7.9 WU respectively. The rest of the patients had PVR < 4.1 WU. No difference was noted between patients who received PAH specific drug therapy and those who did not receive. Patient No 3 with the most severe haemodynamicaly defined PH, improved PVR to 3.9WU and mPAP to 37mmHg after drug therapy.
3.3.3. CTEPH group
CTEPH patients improved PASP, mPAP and PVR after treatment. Balloon Pulmonary Angioplasty (BPA) was performed in 6 (66.7%) among 9 patients with CTEPH as all of them had distal disease; all CTEPH patients were receiving specific PAH drug therapy. BPA in Greece has become available since 2017 and one patient among the 3 who did not undergo BPA died before that year; the second one was diagnosed 11 years before starting BPA program and died two years after the initiation of the program without consenting to undergo evaluation for BPA eligibility, and the third one has been considered ineligible due to extremely severe disease with very hard lesions extending to distal vasculature and an unfavorable risk to benefit ratio. Baseline and follow-up haemodynamic data were available for patients who underwent BPA (Table 5)
The improvement in haemodynamics for patients undergoing BPA is anticipated to be more pronounced if the treatment could be continued to reach treatment goals. Among these six patients, one patient died after accident and subsequent pulmonary embolism before completion of therapy and after only two sessions, two other patients did not consent to the continuation of interventions due to significant clinical improvement despite not reaching the target of mPAP< 30 mmHg (both with 32 mmHg before the last BPA), one patient became normal (mPAP from 56 to 18 mmHg) and the last two patients continue interventions.
3.3.4. Haemodynamic Indices to predict the relevant PH diagnosis
All haemodynamic indices were further analyzed for their ability to predict the PH Group that patients were ultimately included in, and especially to differentiate CTEPH from the other two groups, using receiver operating characteristics (ROC) curves with corresponding area under the ROC curves (AUCs); mPAP had the highest AUC to predict CTEPH diagnosis (0.895, p: 0.001) and PVR had AUC of 0.833 (p:0.0050). The optimal cut-off values for mPAP and PVR were 42mmHg, with a sensitivity of 100% and specificity of 79% and 5.3 WU with a sensitivity of 89% and specificity of 74% in predicting CTEPH diagnosis, respectively.
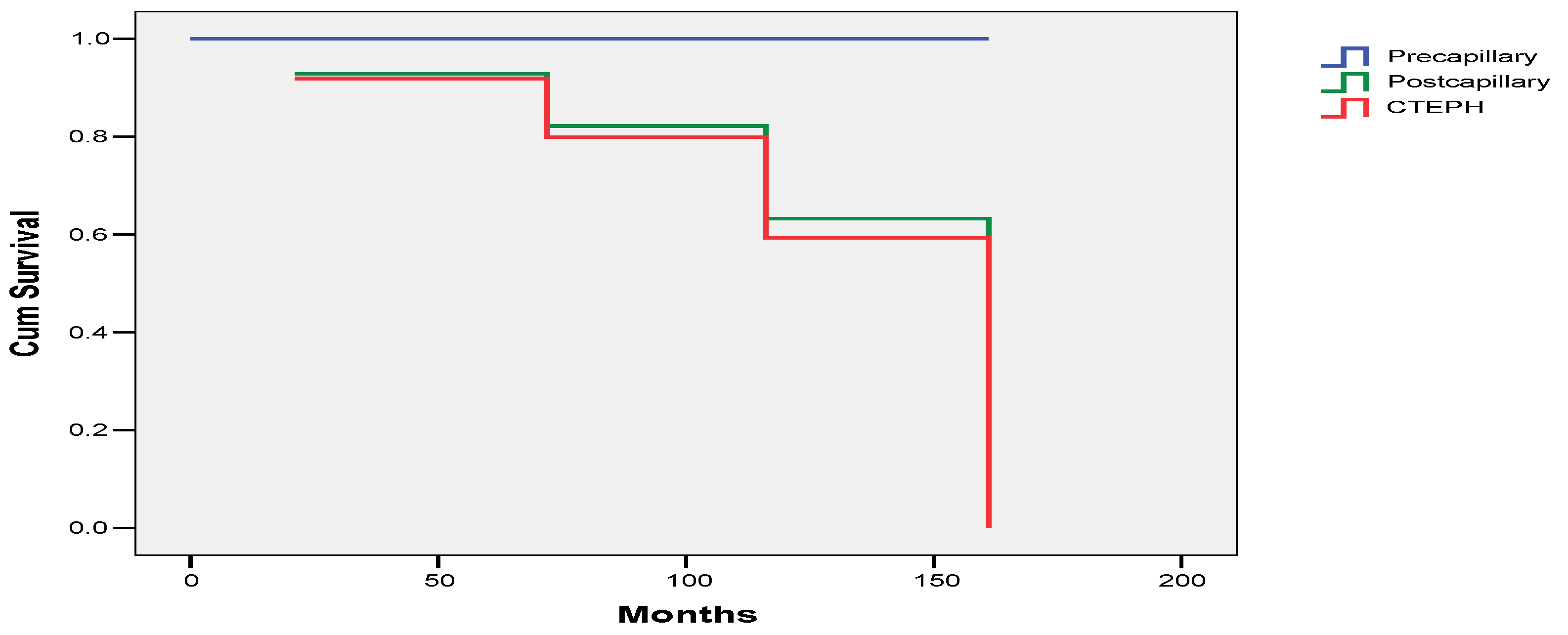
3.4. Survival
Overall survival at 1-y was 100%, at 2, 3, 4, 5 and 6 years 96%, 9yrs 96%, and 13years 78%. The median survival time was 162 months (Figure 1). From the whole study group four patients died, one with postcapillary PH and the other 3 with CTEPH. The survival rates between patients with postcapillary PH and CTEPH were similar (p=0.916) but there was a trend for worst survival rate for patients with postcapillary PH and CTEPH as compared with patients with precapillary PH (p=0.068 and p=0.061, respectively).
Figure 2.
Overall survival according to the different PH groups in the study population.
4. Discussion
PH associated with haemolytic anaemia had been classified as Group I PH (PAH) during the 4th PH World Congress, however at the 2013 5th World Symposium on PH, reclassification in Group V PH was proposed by the Task Force, due to the multifactorial pathogenesis of haemolytic anaemia resulting in different PH forms. Chronic Haemolysis leads to free haemoglobin resulting in inactivation and reduced NO synthesis, alteration of L-arginine metabolism contributing to smooth muscle proliferation and vascular remodelling. Furthermore, Haemolytic disorders increase plasma endothelin-1 levels leading to vasoconstriction. These proposed mechanisms represent underlying mechanisms for the development of precapillary PH [9,10]. Moreover, red cell destruction can provoke platelet and tissue factors activation and thrombin generation leading to obliteration. Splenectomy, endothelial dysfunction and red cell pre-coagulant surface are considered as causes of thromboembolic complications resulting in Thromboembolic Disease and subsequently PH. Iron overload and high cardiac output state are major causes of Left Heart Dysfunction, so patients with haemolytic anaemia can ultimately develop PH due to Left Heart Disease [10,11]. Iron overload mostly present in transfusion-dependent patients with b-thalassemia may induce interstitial pulmonary fibrosis leading to PH due to lung disease (Group III PH) [12]. A combination of these abnormalities in several patients can lead to mixed PH cases, however Right heart Catheterization is mandatory to distinguish precapillary and postcapillary PH. Echocardiography does not seem to provide accurate pulmonary pressures in haemolytic anaemia cohorts, according to the literature [13]. In our cohort, all symptomatic haemolytic anaemia patients with intermediate and high echocardiographic probability for PH underwent RHC. They were classified into three groups as follows: Patients with PAWP>15mmHg as group II PH (PH-LHD), those with precapillary PH, positive lung V/Q scan and thrombi in invasive Pulmonary Angiography as CTEPH and when precapillary PH without thromboembolic disease was present, haemolytic-anemia patients were considered suffering from PAH. None of our patients had severe parenchymal disease according to High Resolution Chest Computed Tomography, Pulmonary Function Tests or blood gas analysis, mandatory steps in diagnostic PH algorithm, to exclude PH due to Lung Disease diagnosis.
According to the literature, thrombotic lesions are a major component of PH related to SCD [2] and precapillary PH has an important impact on survival, with an overall mortality rate of 5.3% in 18 months [1]. In b-thalassemia, precapillary PH appears in 2.1% of cases, while postcapillary in 0.3% [4]. Among our patients with thalassemia, 45.6% had PAH phenotype, 25% postcapillary PH and 29.4% CTEPH. Based on haemodynamic characteristics, CTEPH patients are more severely compromised compared to the other two groups. Furthermore, the level of PVR and mPAP are identified as indices to predict CTEPH diagnosis. This finding could differentiate diagnosis between precapillary PH with thromboembolic disease versus without. So, during a diagnostic approach, a value of mPAP or PVR more than 42mmHg and 5.3WU respectively, necessitates CTEPH exclusion via a lung V/Q scan. In case V/Q scan is positive, invasive pulmonary angiography is a cornerstone for CTEPH verification, emerging the assessment for possible invasive therapeutic approach, ameliorating patients’ outcomes.
Prompt PH classification is mandatory for the most appropriate therapeutic approach. There are no specific management guidelines for patients with PH associated with Haemolytic anaemia [5], however it is of paramount importance for them to be treated with Oxygen supplementation when hypoxia is present as also with blood transfusion and iron chelation according to the severity of underlying haemolytic anaemia disease. Specific PAH-drugs including ERA’s, PDE5, Riociguat, Prostacyclin Receptor agonists such as Selexipag, and prostanoids have been studied in a small number of patients and there is a lack of data supporting their use in haemolytic anaemia patients [14]. PDE-5 were tried in few small case series with positive results concerning 6Minute Walk Distance, NYHA functional class and decreased tricuspid regurgitation velocity [14,15]. A multi-centre randomized double-blind trial [15] (walk-PHaSST trial) was early terminated because of increased hospitalization rates of pain for SCD patients treated with Sildenafil. This is the reason, PDE-5 has been avoided in this cohort. A clinical trial with fourteen SCD patients treated with ERAs, showed improvement in mPAP [17]. Acute administration of intravenous epoprostenol in patients withSCD-ph has shown decrease of PVR and increase in cardiac output, resulting in hyperdynamic state worsening and heart failure [14]. Our study reveals haemodynamic improvement for patients treated with PAH specific drug therapy when classified as precapillary PH. Furthermore, the effectiveness of specific PAH drugs in these patients is also reflected in the excellent survival they showed in contrast to the survival of patients suffering from several forms of group 1 PH, as patients with Idiopathic PAH or PAH associated with Connective Tissue Disorders. In our cohort, the precapillary group had 100% survival for more than 12 years, when the 7-years survival in the drug era for PAH patients is only 49% according to REVEAL registry [18]. The best survival for chronic haemolytic anaemia patients classified as suffering with PAH differs substantially from PAH patients included in registries. The reason is the compensatory high cardiac output state haemolytic anaemia patients present, due to persistent hypoxia. A careful PAH drug initiation with regular follow-up and re-catheterization in 3-6 months is appropriate. In SCD patients, due to adverse effects reported in literature, regular follow-up every month is proposed for the first year after PAH drugs initiation. The role of PAH-specific drug treatment is not well established, however prompt evaluation related to a correct diagnosis and classification could improve hemodynamic parameters and prolong survival.
PAH- specific drug therapy is furthermore recommended in CTEPH patients as micro-vasculopathy is implicated in pathogenesis. Riociguat and Treprostinil are indicated according to RCT’s [19,20] however, to manage the increased PVR, medical therapies are usually used off-label, according to uncontrolled studies and/or regional approvals [5]. The CTEPH management includes a multimodal approach of a combination of Pulmonary Endarterectomy (PEA), BPA, and medical therapies and all patients should be evaluated for possible Pulmonary Endarterectomy [5,21]. The initial evaluation is targeted at identifying patients who udergo mechanical treatment via PEA to remove chronic obstructive material, reducing pulmonary vascular resistance, so PEA represents the gold standard of treatment and BPA remains the alternative option for those who deemed to be inoperable or when thrombi do not appear in the main or segmental pulmonary arterial branches. When thrombotic material appears in the distal pulmonary vascular bed, BPA seems to represent the most appropriate invasive therapeutic strategy. Data from RACE trial [22] demonstrated that for patients who underwent BPA, pre-treatment with Riociguat was associated with a lower complication rate (14% vs 42% of patients). There are not much data on PEA or BPA in chronic haemolytic anaemia. According to Papworth’s experience, 19 patients with haemoglobinopathy of congenital haemolytic anaemia underwent PEA [23]. The results of PEA in this complex patient group were satisfactory under expert haematological advice and exchange blood transfusions. Immediately postoperatively, there was a significant improvement in PVR, so the researchers concluded that the presence of abnormal haemoglobin does not contraindicate PEA surgery. In our patients, the thromboembolic disease was distal in the pulmonary vascular bed, so BPA, an established treatment for selected CTEPH patients, seemed to be the proper therapeutic management. Data regarding the application of BPA in haemolytic anaemia patients are extremely scarce. For thalassemia patients, there is a case report [24] in the literature and the published Hellenic (HOPE) registry where CTEPH patients with haemolytic anaemia were included [2,25,26]. On the other hand, regarding SCD patients, there is also one case report [27], and except for the HOPE registry there is a published study comprising 58 consecutive SCD patients with pre-capillary PH, where three of them were treated by BPA suggesting that this technique remains a viable option to consider in SCD- CTEPH [2]. In our study, these patients were treated with PAH specific drug therapy and most of them with BPA. Haemodynamic improvement was achieved with a survival of 60% in 162 months. So, BPA and PAH drug therapy seems to lead to hemodynamic improvement in patients with haemolytic anaemia, management applied in expert PH centers in close collaboration with haematological advice.
5. Conclusion
PH is a complication in chronic Haemolytic Anaemia patients and its multifactorial pathogenesis is responsible for multiple phenotypes, ultimately classified in different PH groups. The heterogeneity of patient phenotypes and the wide spectrum of disease necessitates a prompt diagnosis based on right heart catheterization and the whole diagnostic approach according to current guidelines recommendation. Chronic thromboembolic phenotype seems to be the most severe but also has the better results from the currently available therapies. The optimal disease-directed therapeutic approach according to PH classification can be beneficial in hemodynamic parameters, improving right heart function and outcomes. Given the complexity of Haemolytic anaemia and PH therapy and the rapidly changing landscape, these patients should be monitored and regularly be under follow up in Thalassemic and PH expert centers.
References
- Gladwin MT, Sachdev V, Jison ML, Shizukuda Y, Plehn JF, Minter K, et al. Pulmonary hypertension as a risk factor for death in patients with sickle cell disease. N Engl J Med 2004, 350, 886–895. [CrossRef]
- Savale L, Habibi A, Lionnet F, Maitre B, Cottin V, Jais X, et al. Clinical phenotypes and outcomes of precapillary pulmonary hypertension of sickle cell disease. Eur Respir J 2019, 54, 1900585. [CrossRef]
- Sutton LL, Castro O, Cross DJ, Spencer JE, Lewis JF. Pulmonary hypertension in sickle cell disease. Am J Cardiol 1994, 74, 626–628. [CrossRef]
- Derchi G, Galanello R, Bina P, Cappellini MD, Piga A, Lai ME, et al. Prevalence and risk factors for pulmonary arterial hypertension in a large group of beta-thalassemia patients using right heart catheterization: a Webthal study. Circulation 2014, 129, 338–345. [CrossRef]
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, Ferreira DS, Ghofrani HA, Giannakoulas G, Kiely DG, Mayer E, Meszaros G, Nagavci B, Olsson KM, Pepke-Zaba J, Quint JK, Rådegran G, Simonneau G, Sitbon O, Tonia T, Toshner M, Vachiery JL, Vonk Noordegraaf A, Delcroix M, Rosenkranz S; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022, 43, 3618–3731.
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M; ESC Scientific Document Group.2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016, 37, 67–119.
- D T Kremastinos, D P Tsiapras, G A Tsetsos, E I Rentoukas, H P Vretou, P K Toutouzas. Left ventricular diastolic Doppler characteristics inbeta-thalassemia major. Circulation 1993, 88, 1127–1135. [CrossRef] [PubMed]
- A Aessopos, G Stamatelos, V Skoumas, G Vassilopoulos, M Mantzourani, D Loukopoulos Pulmonary hypertension and right heart failure inpatients with beta-thalassemia intermedia. Chest 1995, 107, 50–53. [CrossRef] [PubMed]
- Anastasia Anthi, Stylianos E Orfanos, Apostolos Armaganidis. Pulmonary hypertension in β thalassaemia. Lancet Respir Med 2013, 1, 488–496.
- Alem Mehari, Elizabeth S Klings. Chronic Pulmonary Complications of Sickle Cell Disease. Chest 2016, 149, 1313–1324. [CrossRef]
- Valeria Maria Pinto, Khaled M Musallam, Giorgio Derchi, Giovanna Graziadei, Marianna Giuditta, Raffaella Origa, Susanna Barella, Gavino Casu, Annamaria Pasanisi, Filomena Longo et al. Mortality in β-thalassemia patients with confirmed pulmonary arterial hypertension on right heart catheterization. Blood 2022, 139, 2080–2083.
- Parent F, Bachir D, Inamo J, et al. A hemodynamic study of pulmonary hypertension in sickle cell disease. N Engl J Med 2011, 365, 44–53. [CrossRef] [PubMed]
- Anthi, D. Tsiapras, P. Karyofyllis, V. Voudris, A. Armaganidis, S. Orfanos. The wide spectrum of β-thalassaemia intermedia-induced pulmonary hypertension: two case reportson the possible role of specific pulmonary arteri-alhypertension therapy. Pulm Circ 2021, 11, 20458940211030490.
- Derchi G, Forni GL, Formisano F, Cappellini MD, Galanello R, D’Ascola G, et al. Efficacy and safety of sildenafil in the treatment of severe pulmonary hypertension in patients with hemoglobinopathies. Haematologica 2005, 90, 452–458.
- Machado RF, Martyr S, Kato GJ, Barst RJ, Anthi A, Robinson MR,et al. Sildenafi l therapy in patients with sickle cell disease and pulmonary hypertension. Br J Haematol 2005, 130, 445–453. [CrossRef]
- Minniti CP, Machado RF, Coles WA, Sachdev V, Gladwin MT, Kato GJ. Endothelin receptor antagonists for pulmonary hypertension in adult patients with sickle cell disease. Br J Haematol 2009, 147, 737–743. [CrossRef]
- Castro O, Hoque M, Brown BD. Pulmonary hypertension in sickle cell disease: Cardiac catheterization results and survival. Blood 2003, 101, 1257–1261. [CrossRef] [PubMed]
- Raymond L Benza, Dave P Miller, Robyn J Barst, David B Badesch, Adaani E Frost, Michael D McGoon. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest 2012, 142, 448–456. [CrossRef] [PubMed]
- Ghofrani HA, D’Armini AM, Grimminger F, Hoeper MM, Jansa P, Kim NH, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N Engl J Med 2013, 369, 319–329. [CrossRef]
- Sadushi-Kolici R, Jansa P, Kopec G, Torbicki A, Skoro-Sajer N, Campean IA, et al. Subcutaneous treprostinil for the treatment of severe non-operable chronic thromboembolic pulmonary hypertension (CTEPH): a double-blind, phase 3, randomised controlled trial. Lancet Respir Med 2019, 7, 239–248. [CrossRef]
- Ghofrani HA, Simonneau G, D’Armini AM, Fedullo P, Howard LS, Jais X, et al. Macitentan for the treatment of inoperable chronic thromboembolic pulmonary hypertension (MERIT-1): results from the multicentre, phase 2, randomised, double-blind, placebo-controlled study. Lancet Respir Med 2017, 5, 785–794.
- Xavier Jaïs 1, Philippe Brenot 2, Hélène Bouvaist 3, Mitja Jevnikar 4, Matthieu Canuet 5, Céline Chabanne 6, Ari Chaouat 7, Vincent Cottin 8, Pascal De Groote 9, Nicolas Favrolt 10, Delphine Horeau-Langlard 11, Pascal Magro 12, Laurent Savale 4, Grégoire Prévot 13, Sébastien Renard 14, Olivier Sitbon 4, Florence Parent 4, Romain Trésorier 15, Cécile Tromeur 16, Céline Piedvache 17, Lamiae Grimaldi 18, Elie Fadel 19, David Montani 4, Marc Humbert 4, Gérald Simonneau 4 Balloon pulmonary angioplasty versus riociguat for the treatment of inoperable chronic thromboembolic pulmonary hypertension (RACE): a multicentre, phase 3, open-label, randomised controlled trial and ancillary follow-up study. Lancet Respir Med 2022, 10, 961–971.
- Balakrishnan Mahesh, Martin Besser, Antonio Ravaglioli, Joanna Pepke-Zaba, Guillermo Martinez, Andrew Klein, Choo Ng, Steven Tsui, John Dunning, David P. Jenkins Author Notes Pulmonary endarterectomy is effective and safe in patients with haemoglobinopathies and abnormal red blood cells: the Papworth experience. European Journal of Cardio-Thoracic Surgery 2016, 50, 537–541.
- Panagiotis Karyofyllis 1, Dimitris Tsiapras 2, Varvara Papadopoulou 3, Michael D Diamantidis 4, Paraskevi Fotiou 4, Eftychia Demerouti 2, Vassilis Voudris Balloon pulmonary angioplasty is a promising option in thalassemic patients with inoperable chronic thromboembolic pulmonary hypertension. Case Reports J Thromb Thrombolysis 2018, 46, 516–520.
- Demerouti E, Karyofyllis P, Voudris V, Boutsikou M, Anastasiadis G, Anthi A, Arvanitaki A, Athanassopoulos G, Avgeropoulou A, Brili S, Feloukidis C, Frantzeskaki F, Karatasakis G, Karvounis H, Konstantonis D, Mitrouska I, Mouratoglou S, Naka KK, Orfanos SE, Panagiotidou E, Pitsiou G, Pitsis A, Stamatopoulou V, Stanopoulos I, Thomaidis A, Tsangaris I, Tsiapras D, Giannakoulas G, Manginas A, On Behalf Of The Hellenic Society For The Study Of Pulmonary Hypertension Hssph. Epidemiology and Management of Chronic Thromboembolic Pulmonary Hypertension in Greece. Real-World Data from the Hellenic Pulmonary Hypertension Registry (HOPE). J Clin Med. 2021, 10, 4547.
- Karyofyllis P, Demerouti E, Giannakoulas G, Anthi A, Arvanitaki A, Athanassopoulos G, Feloukidis C, Iakovou I, Kostelidou T, Mitrouska I, Mouratoglou SA, Orfanos SE, Pappas C, Pitsiou G, Tsetika EG, Tsiapras D, Voudris V, Manginas A; Hellenic Society for the Study of Pulmonary Hypertension HSSPH. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension in Greece: Data from the Hellenic Pulmonary Hypertension Registry. J Clin Med. 2022, 11, 2211.
- Panagiotis Karyofyllis, Dimitrios Tsiapras, Eftychia Demerouti, Iakovos Armenis, Varvara Papadopoulou, Vassilis Voudris Sickle cell disease related chronic thromboembolic pulmonary hypertension: challenging clinical scenario. J Thromb Thrombolysis 2022, 53, 467–470. [CrossRef] [PubMed]
Figure 1.
Study flowchart of participants showing the patients whole group and their allocation according to diagnostic approach.
Figure 1.
Study flowchart of participants showing the patients whole group and their allocation according to diagnostic approach.
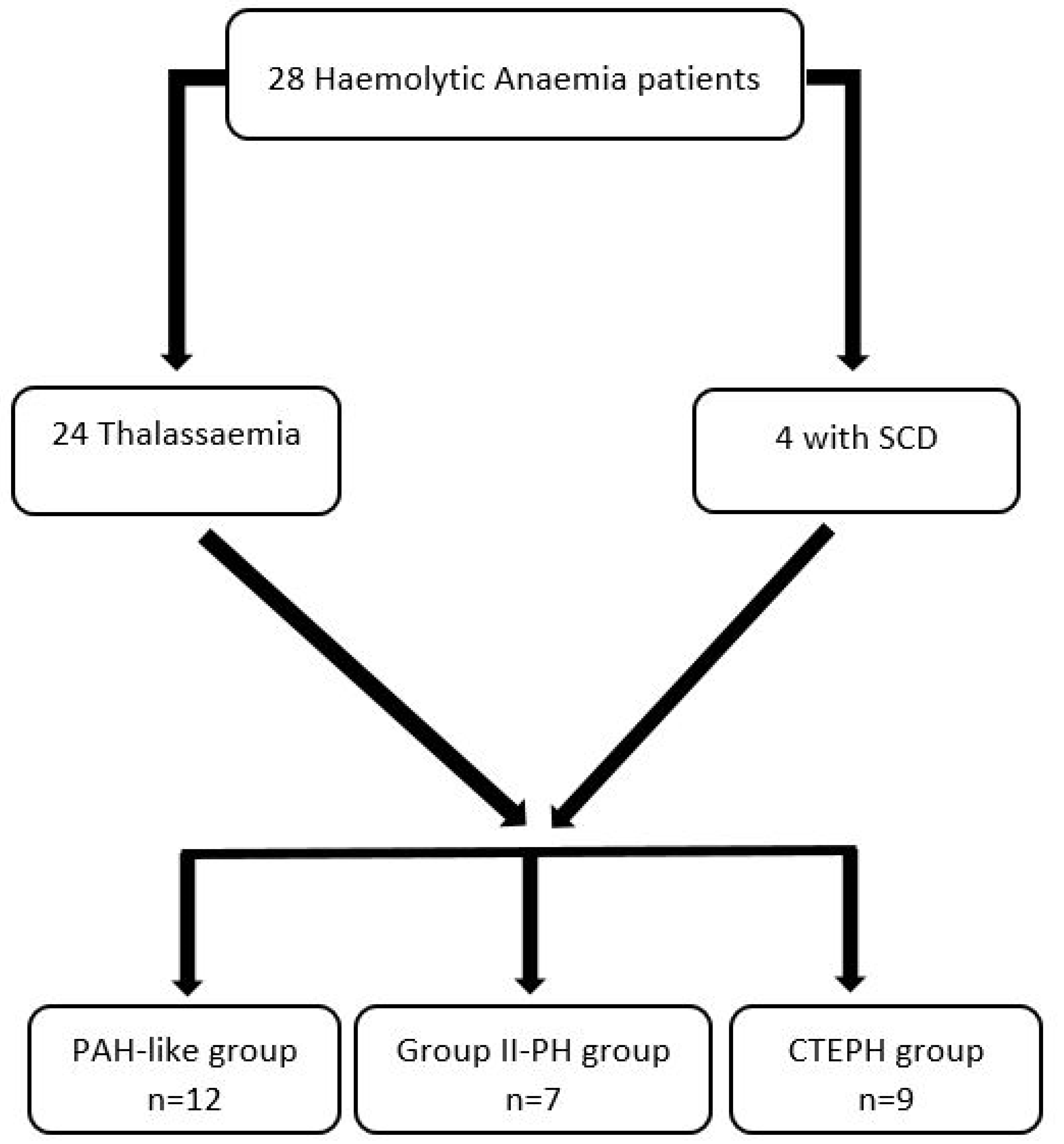

Table 1.
Haemodynamic characteristics in the three groups of study population.
| PAH GROUP (group 1) | PH-LHD (group 2) | CTEPH GROUP (group 4) | p-value | |
| RAP (mmHg) | 7.7±0.4 | 13.5±3.7 | 11.5±5.3 | 0.029 (group 1 vs 2) |
| PASP (mmHg) | 57.6±12.8 | 55.8±15.5 | 83.6±10.5 | ≤ 0.01 (group 4 vs 1,2) |
| mPAP (mmHg) | 36±7.6 | 37.1±8.6 | 50.4±6.2 | ≤ 0.04 (group 4 vs 1,2) |
| PAWP (mmHg) | 10.8±4 | 19±1.4 | 11.9±3.2 | <0.01 (group 2 vs 1,4) |
| CI (L/min/m2) | 2.82±0.78 | 2.67±0.62 | 2.60±0.7 | ns |
| PVR (WU) | 5.7±3 | 4.3±1.9 | 8.5±2.4 | ≤ 0.038 (group 4 vs 1,2) |
| PAC (ml/mmHg) | 1.78±0.68 | 2.31±2.36 | 1.09±0.39 | 0.023 (group 2 vs 4) |
| SVO2 (%) | 68.3±5.9 | 66.4±6.1 | 52.5±10 | ≤ 0.01(group 4 vs 1,2) |
PAH: Pulmonary Arterial Hypertension, CTEPH: Chronic Thromboembolic Pulmonary Hypertension, PH-LHD: Left Heart Disease related Pulmonary Hypertension, RAP: Right Atrial Pressure, PASP: Systolic Pulmonary Arterial Pressure, mPAP: mean Pulmonary Arterial Pres-sure, PAWP: Pulmonary Arterial Wedge Pressure, PVR: Pulmonary Vascular Resistance, PAC: Pulmonary Arterial Compliance, SVO2: Venus Oxygen Saturation.
Table 2.
Specific PH treatment among the three different groups of PH in the study patients.
| Specific PH treatment n=23/28(82.1) | ERA 15(65.2) | PDE5 6(26) | RIO 8(34.5) | SELEX 1(4.3) | Monotherapy 16(69.5) | Double therapy 7(30.4) | No specific PH treatment 5(17.9) |
| Precapillary PH n=11/12 | 9(75) | 3(25) | 1(8.3) | 0 | 9(75) | 2(16.7) | 1(8.3) |
| Postcapillary PH n=3/7 | 1(14.3) | 1(14.3) | 2(28.6) | 0 | 2(28.6) | 1(14.3) | 4(57.1) |
| CTEPH n=9/9 | 5(55.6) | 2(22.2) | 5(55.6) | 1(11.1) | 5(55.6) | 4(44.4) | 0 |
PH: Pulmonary Hypertension, ERA: Endothelin Receptor Antagonist, PDE5: Phosphodiesterase Inhitor5, RIO: Riociguat, SELEX: Selexipag, CTEPH: Chronic Thromboembolic Pulmonary Hypertension.
Table 3.
RHC parameters at baseline and after PAH-specific drug treatment in PAH-like group.
| N=9 | Baseline | Post treatment | p-value |
| RAP (mmHg) | 8.1±4.6 | 7.6±2.8 | 0.807 |
| PASP (mmHg) | 62.6±10.1 | 51±9.6 | 0.019 |
| mPAP (mmHg) | 38.8±6.8 | 33±6.5 | 0.083 |
| CI (L/min/m2) | 2.92±0.87 | 3.49±0.91 | 0.145 |
| PVR (WU) | 6.4±3.2 | 4±1.9 | 0.005 |
| PAC (ml/mmHg) | 1.58±0.55 | 2.75±1.67 | 0.044 |
| SVO2 (%) | 67.5±6 | 71.4±6.5 | 0.094 |
RAP: Right Atrial Pressure, PASP: Systolic Pulmonary Arterial Pressure, mPAP: mean Pulmonary Arterial Pressure, CI: Cardiac Index, PVR: Pulmonary Vascular Resistance, PAC: Pulmonary Arterial Compliance, SVO2: Venus Oxygen Saturation, WU: Woods Units.
Table 4.
Right Heart Catheterization parameters at baseline and at follow-up in postcapillary PH group.
Table 4.
Right Heart Catheterization parameters at baseline and at follow-up in postcapillary PH group.
| Baseline | Last RHC | p-value | |
| RAP (mmHg) | 14.2±3.3 | 9.4±2 | 0.026 |
| PASP (mmHg) | 56.8±18.9 | 55±11 | 0.841 |
| mPAP (mmHg) | 38±10.1 | 34.6±5.5 | 0.482 |
| CI (L/min/m2) | 2.85±0.64 | 2.76±0.75 | 0.821 |
| PVR (WU) | 4.1±2.3 | 4.2±1.5 | 0.983 |
| PAC (ml/mmHg) | 2.71±2.77 | 2.01±0.78 | 0.594 |
| SVO2 (%) | 69.8±1.2 | 66.1±4.3 | 0.159 |
RAP: Right Atrial Pressure, PASP: Systolic Pulmonary Arterial Pressure, mPAP: mean Pulmonary Arterial Pressure, CI: Cardiac Index, PVR: Pulmonary Vascular Resistance, PAC: Pulmonary Arterial Compliance, SVO2: Venus Oxygen Saturation.
Table 5.
Haemodynamic parameters at baseline and after therapeutic approach in CTEPH patients.
| N=6 | Baseline | Post treatment | p-value |
| RAP (mmHg) | 11.5±5.3 | 7.1±1.4 | 0.149 |
| PASP (mmHg) | 85.2±7.4 | 56.3±21 | 0.02 |
| mPAP (mmHg) | 51.7±6.1 | 34±10.2 | 0.029 |
| CI (L/min) | 2.33±0.35 | 2.79±0.42 | 0.063 |
| PVR (WU) | 9.5±1.6 | 4.5±2.9 | 0.020 |
| PAC (ml/mmHg) | 0.94±0.18 | 2.51±2 | 0.122 |
| SVO2 (%) | 51.6±10.9 | 61.1±8.4 | 0.138 |
RAP: Right Atrial Pressure, PASP: Systolic Pulmonary Arterial Pressure, mPAP: mean Pulmonary Arterial Pressure, CI: Cardiac Index, PVR: Pulmonary Vascular Resistance, PAC: Pulmonary Arterial Compliance, SVO2: Venus Oxygen Saturation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



