
Submitted:
28 November 2023
Posted:
29 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: COVID-19 is currently one of the most important medical challenges as it affects the entire population with children being infected as easily as adults. Objective: The study evaluated the mortality of under 17-year-olds and compare the frequency with that of adults in a cohort of 8986 COVID-19 positive patients hospitalized in a single care center. Design: retrospective clinical trial, all hospitalizations of COVID-19 positive patients as diagnosed by RT-qPCR were analyzed by revisiting their medical records. Setting: 8986 COVID-19 positive patients hospitalized in a Hospital de Base and the Infant and Maternal Hospital of São Jose do Rio Preto, SP, Brazil (HB/HCM) being these totals of 383 COVID-19 positive under 17-patients. Patients: patients COVID-19 positive under 17-year-olds were grouped by age and evaluated by analyzing their medical records. They were categorized as Group I, children, and adolescents under 19 years old and Group II, adults over 19 years. Results: Overall mortality in under 19-year-olds was 12 deaths, that is, 3.13% of the patients in this age group and 0.55% of the overall mortality from COVID-19. Mortality in the group of adults was 2197 equivalent to 24.45% of the hospitalized adults and 99.45% of overall deaths. Mortality was significantly higher for adults than for under 19-year olds (p-value < 0.0001). Regarding the different ages of children and adolescents, the number of deaths of under 1-year olds was 2/123 (1.62%), of 1-4 years it was 4/95 (2.11%), of 5-9 years it was 1/47 (2.13%), of 10-14 years it was 1/40 (2.5%) and of 15-19 years it was 4/78 (5.13%). There were no statistical differences between the different age groups ( p-value = 0.3). Conclusion: Mortality from COVID-19 in children and adolescents was lower than in adults and generally associated with other comorbidities with the main association being with heart disease.
Keywords:
COVID-19
; children
; mortality
1. Introduction
COVID-19 is currently one of the most important medical challenges as it affects the entire population with children being infected as easily as adults are; they often remain asymptomatic or have mild complaints due to their immature immune systems [1]. Most children with COVID-19 have mild disease, however coagulopathies have been associated with multisystem inflammatory syndrome in children (MIS-C), a postinfectious complication [2].
A study in England reported that 1408 (4.0%) of 35,200 tests performed in under 16-year-old children were positive for SARS-CoV-2 compared to 19.1%-34.9% in adults [3]. A review of pregnant women with COVID-19 reported that nineteen of 444 (4.27%) newborns were positive for RNA of SARS-CoV-2 at birth. Elevated levels of IgM and IgG serum antibodies were reported in one case, but the swab test was negative [4]. Mortality in children is higher in those with comorbidities compared to those without comorbidities [5].
Regarding the prognosis, metabolic acidosis, hyperlactatemia, hyperglycemia, altered liver function parameters and hypoproteinemia are biochemical markers associated with the severe form of the disease in SARS-CoV-2 infected children. The presence of anemia, and ketoacidosis are important risk factors for death in pediatric patients with SARS-CoV-2 infection [6]. Gastrointestinal (GI) involvement is common in children hospitalized for acute COVID-19 infection and multisystem inflammatory syndrome, but GI involvement is not associated with critical illness, length of hospital stays, or mortality in acute cases of COVID-19 [7].
Reinforcing, in relation to the risk factors associated with the disease, we highlight the presence of comorbidities and the age group (under 2 years old). In this context, the following stand out: congenital heart disease, Down syndrome, obesity, and asthma. Furthermore, there is a greater morbidity and mortality related to regional disparities, especially in countries with low economic resources, as for example in the case of our country, Brazil, with a higher proportion related to the economically less favored North and Northeast regions.
It is also worth highlighting regarding COVID-19 and prolonged symptoms, notably: fatigue, headaches, drowsiness, difficulty concentrating. We noticed an important impact of social isolation with psychosocial disorders and school delays with a major impact on children's education [8,9].
An American study reports that pediatric patients with recent relapse of cancer have a higher chance of all-cause mortality in the scenario of COVID-19 [10].
The objectives of the current study were to evaluate the mortality of under 17-year-olds and compare the frequency with that of adults in a cohort of 8986 COVID-19 positive patients hospitalized in a single care center (university hospital complex), grouping the 383 children by age.
2. Material and Method
2.1. Casuistry and Local
Patients hospitalizations of COVID-19 positive patients as diagnosed by RT-qPCR were analyzed by revisiting their medical records admitted to the Hospital de Base-Funfarme and the Infant and Maternal Hospital of São Jose do Rio Preto, SP, Brazil (HB/HCM) between March 2020 and July 2023.
2.2. Inclusion Criteria
The inclusion criterion was all COVID-19 positive patients diagnosed by reverse transcription quantitative polymerase chain reaction (RT-qPCR) admitted to these hospitals.
2.3. Exclusion Criteria
Patients hospitalized for other illnesses and without positivity for Covid 19 during this period.
2.4. Study Design
Retrospective observational study analyzing mortality in all hospitalizations for Covid 19 at Hospital de Base (HB) and Hospital de Criança e Maternidade de São José do Rio Preto-SP-Brazil (HCM), from 2020 to 2023 for analyzed by revisiting their medical records.
2.5. Hypotheses
Children and adolescents hospitalized with positive COVID-19 and who died had other associated comorbidities.
2.6. Development
They were categorized as Group I, children and adolescents under 19 years old and Group II, adults over 19 years. Furthermore, Group I was subdivided by age: < 1 year, 1-4 years, 5-9 years, 10-14 years and 15-19 years. The monthly occurrence of COVID-19 was evaluated for under 19-year-olds from March 2020 to July 2023 and mortality in children and adolescents was compared to deaths in adults. The causes of mortality and the occurrence of viral diseases were identified in the COVID-19 positive under 19-year-olds over the same period.
2.7. Ethical Aspects
The study was approved by the Ethics Committee of the Faculdade de Medicina de São Jose do Rio Preto-FAMERP number 6.086,468- 2023.
For the study, the assistance institution requested and permitted the analysis of these records, where a document was signed guaranteeing the use of data only for this research protocol and absolute confidentiality during the collection and use of data. Safe safeguards are taken to collect data from medical records in the institution's own archiving location, not leaving that location in any way.
Data was collected by date (annual) and an alphabetical classification system was created, A: medical record data beginning February 2020; B medical records from 2021; C medical record data until March 2023 and sequenced numbers (1,2,3...) for each medical record that allows names not to be identified.
2.8. Patient Consent for Publication
Not required. The signed consent form was authorized by this ethics committee to be waived because they were medical records and the impossibility of contacting family members and deaths. Thus, the authors guaranteed the privacy and confidentiality of the data obtained, fully preserving the anonymity of the participants in accordance with Declaration of Helsinki.
2.9. Statistical Analysis
Microsoft Excel was used for data collection with statistical analysis being performed using StatsDirect 3 (StatsDirect Ltd Wirral, UK Company number: 04399867). Descriptive statistics, Fisher's exact test, the Chi-square test and Odds Ratio were utilized considering an alpha error of 5% (p-value ≤ 0.05).
3. Results
A total of 8986 COVID-19 positive patients were hospitalized between March 2020 and July 2023, 383 (4.26%) of whom were under 19 years old and 8603 (95.74%) were over 19 years old (Figure 1). Overall mortality in under 19-year-olds was 12 deaths, that is, 3.13% of the patients in this age group and 0.55% of the overall mortality from COVID-19. Mortality in the group of adults was 2197 equivalent to 24.45% of the hospitalized adults and 99.45% of overall deaths. Mortality was significantly higher for adults than for under 19-year-olds (Yates-corrected Chi-square test = 98.127501; p-value < 0.0001).
Regarding the different ages of children and adolescents, the number of deaths of under 1-year olds was 2/123 (1.62%) of 1-4 years it was 4/95 (2.11%), of 5-9 years it was 1/47 (2.13%), of 10-14 years it was 1/40 (2.5%) and of 15-19 years it was 4/78 (5.13%). There were no statistical differences between the different age groups (Fisher's exact test: p-value = 0.3; Table 1 and Figure 2). Figure 3 shows the main viral infections of the COVID-19 positive patients in the two hospitals, emphasizing the importance of this disease. Table 2 shows the main causes of mortality of the 12 children who died from COVID-19.
4. Discussion
The present study reports on the general mortality of under 19-year-olds and adult patients in a single care center (university hospital complex) from March 2020 to July 2023 grouped by age. Of the 8986 patients hospitalized with COVID-19, 383 were children and adolescents attended in the Children's Hospital. Deaths in this age group represented 0.55% of all deaths from COVID-19 in the institution and 3.13% of all hospitalized under 19-year-olds. No difference was detected in mortality between the age groups of children and adolescents. A multicenter study in Latin America reported a mortality rate of 14% in 210 children with 67% of those who died being treated in an intensive care unit [10].
Observational studies in the pediatric population have shown that the presence of comorbidities is a risk factor for severe disease. Obesity, genetic disorders (such as sickle cell anemia), neurological, hematological, and congenital heart diseases, diabetes, chronic kidney disease, asthma and other lung diseases are pathologies that have already been associated with the severity of COVID-19 in some studies [12]. In the present study, heart disease was the main disorder associated with mortality of children.
Regarding age of children and adolescents, there is no consensus on which age group has a highest or lowest severity risk. Under one-year-old children have been identified by some studies as being at greater risk, while other authors have reported the neonatal or adolescent age groups as having greater risks of contamination and severity, so there is no consensus [13]. In the current study, no significant differences were detected between age groups, however the number of patients is too small to arrive at any definite conclusion.
In North America, mortality was higher in children younger than one year old and then in adolescents between 15 and 19 years of age [14]. In 2021 and 2022, another study in Java, Indonesia analyzed 6441 under 18-year-old patients positive for COVID-19 and reported 2.7% of deaths with other associated factors [15].
Regarding mortality since the beginning of the pandemic, newborns, children and adolescents are less prone to this emerging condition compared to adults. Most of them suffer mild symptoms; hospitalization and death of pediatric patients are rare, with deaths usually being explained by associated complications [16].
The United States of America had a significant number of victims. A study in the period from August 2021 to July 2022 informed crude pediatric mortality rates due to COVID-19 considering five age groups: the deaths reported were under 1-year olds 4.3/100,000 inhabitants; 1-4 years old 0.6/100,000; 5-9 years old 0.4/100,000; 10-14 years old 0.5/100,000; and 15-19 years 1.8/100,000 inhabitants [14].
In Ecuador, a study on mortality from 2020 to 2021 reported that out of 34,001 confirmed cases of COVID-19, 258 were children and adolescents aged between 0 and 19 years and that 127 died due to COVID-19. In the same period, this study found that most deaths occurred in children aged 0 to 1 year, representing 44% (n = 114) of total deaths reported. of the total number of hospitalized under 19-year-olds [17].
In Brazil, in 2020, there were 14,638 children with SARS, with 1180 (8.06%) deaths. Younger than two years old was a risk factor for which higher hospitalization and mortality rates were described [18]. In 2021, an increase in the number of cases of pediatric patients was noted. According to data from the Ministry of Health, in 2021 there were 17,644 occurrences of SARS-CoV-2 with 1263 (7.15%) deaths. This rise is related to greater knowledge of the disease, a simpler diagnosis, the larger quantity of diagnostic tests performed and the emergence of new variants (Delta and Omicron) [19]. Patients with comorbidities are at higher risk for hospitalization and mortality. Among the reported comorbidities, the following should be highlighted: Down syndrome, asthma, obesity, immunosuppression, and heart disease. Morbidity and mortality due to COVID-19 are not similar to other etiologies of acute respiratory distress syndrome (ARDS). This is because fulminant activation of coagulation can occur resulting in widespread microvascular thrombosis and the consumption of clotting factors [18,19,20,21,22]. It appears that inflamed lung tissues and pulmonary endothelial cells may result in the formation of microthrombi that contribute to the high incidence of thrombotic complications such as deep vein thrombosis, pulmonary embolism, and arterial thrombotic complications.
Another important factor that must be highlighted is the possibility of presenting long-term symptoms such as fatigue, headaches, drowsiness, and difficulty concentrating, instigating implications in social and educational spheres with important concern regarding the impact of the pandemic on future early childhood education.
Another point to be considered is related to the risk of the long-term effects of COVID-19 on the health of the general population. Post-COVID coronary changes and the presence of multisystem inflammatory syndrome were identified in some pediatric patients.
Therefore, although children and adolescents represent a low percentage of COVID-19 cases in Latin America and worldwide, major social, economic, and cultural implications are linked to the disease in this population. In true COVID-19 has disrupted all spheres of life, including country risk regarding the exposure of economies to multi-dimensional risk drivers.
It is known that socio-economic and political conditions directly interfere in health conditions and directly affect a pandemic and the application of resources directly to immediate health care. Studies analyzing the influence of demographic, economic and political conditions in different countries and continents show a significant difference between countries with a lower Human Development Index (HDI) than those with a higher HDI. And this has influenced and continues to directly influence human health care [23,24].
It should be remembered that the dynamics of infections and deaths related to COVID-19 differs from country to country and is constantly changing throughout Latin America. Management requires political leadership, financial resources, and social equality, as well as the existence of informal and regional economies with emphasis on disadvantaged populations that traditionally have limited access to health services. In the present study, COVID-19 was the most common viral infection identified in this period, with variations between the different months. Mortality from COVID-19 in children and adolescents was lower than in adults and generally associated with other comorbidities with the main association being with heart disease.
Our study showed results consistent with our hypothesis and with the presentation of some studies in Medline literature. Like this, to predict the outcome of COVID-19 is of vital clinical importance to better allocate medical resources and provide individualized treatment for patients. The availability of clinical characteristics and parameters with potential prognostic implications will be of value for effective prevention and intervention methods.
5. Conclusions
Mortality from COVID-19 in children and adolescents was lower than in adults and generally associated with other comorbidities with the main association being with heart disease.
Conflict Interest
The authors declare no have conflict interesting.
Financial Support
No have.
Authors contributions
Concept and design: Godoy ACP, Bestetti RB; Acquisition of data: Godoy ACP, Bestetti RB; Analysis and interpretation of data: Godoy ACP, Bestetti RB; Drafting the article: Godoy ACP, Bestetti RB; Revising it critically for important intellectual content: Godoy ACP, Bestetti RB; Final approval of the version to be Published: Godoy ACP, Bestetti RB.
Data availability
All data generated or analyzed during this study are included within the article.
References
- Frenkel, L.D.; Gomez, F.; Bellanti, J.A. COVID-19 in children: Pathogenesis and current status. Allergy Asthma Proc. 2021 Jan 3;42(1):8-15. [CrossRef] [PubMed]
- Whitworth, H.; Sartain, S.E.; Kumar, R.; Armstrong, K.; Ballester, L.; Betensky, M.; et al Rate of thrombosis in children adolescents hospitalized with COVID-19 or, M.I.S.-C. Blood. 2021 Jul 15;138(2):190-198. [CrossRef]
- Ladhani SN, Amin-Chowdhury Z, Davies HG, Aiano F, Hayden I, Lacy J, Sinnathamby M, et al. COVID-19 in children: analysis of the first pandemic peak in England. Arch Dis Child. 2020 Dec;105(12):1180-1185. [CrossRef]
- Di Toro F, Gjoka M, Di Lorenzo G, De Santo D, De Seta F, Maso G, et al. Impact of COVID-19 on maternal and neonatal outcomes: a systematic review and meta-analysis. Clin Microbiol Infect. 2021 Jan;27(1):36-46. [CrossRef]
- Tsankov, B.K.; Allaire, J.M.; Irvine, M.A.; Lopez, A.A.; Sauvé, L.J.; Vallance, B.A.; Jacobson, K. Severe COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int J Infect Dis. 2021 Feb;103:246-256. [CrossRef]
- Belu A, Trandafir LM, Țarcă E, Cojocaru E, Frăsinariu O, Stârcea M, et al. Variations in Biochemical Values under Stress in Children with SARS-CoV-2 Infection. Diagnostics (Basel). 2022 ;12(5):1213. [CrossRef]
- Sayed IA, Bhalala U, Strom L, Tripathi S, Kim JS, Michaud K, et al. VIRUS Investigators. Gastrointestinal Manifestations in Hospitalized Children With Acute SARS-CoV-2 Infection and Multisystem Inflammatory Condition: An Analysis of the VIRUS COVID-19 Registry. Pediatr Infect Dis J. 2022. [CrossRef]
- Luo X, Lv M, Zhang X, Estill J, Yang B, Lei R, Ren M, Liu Y, Wang L, Liu X, Wang Q, Meng M, Chen Y; COVID-19 evidence and recommendations working group. Clinical manifestations of COVID-19: An overview of 102 systematic reviews with evidence mapping. J Evid Based Med. 2022 Sep;15(3):201-215. [CrossRef]
- Souza IV, Scodro RB de Lima, Siqueira VLD, Cardoso RF 2, Ferracioli KRC. Comorbidities And Deaths By Covid-19 In Brazil. Uningá Journal 2021; 58: eUJ4054. 4054. [CrossRef]
- Quast, T.; Andel, R.; Gregory, S.; Storch, E.A. Years of life lost associated with COVID-19 deaths in the USA during the first 2 years of the pandemic. J Public Health (Oxf). 2022 :fdac057. [CrossRef]
- Dominguez-Rojas JÁ, Vásquez-Hoyos P, Pérez-Morales R, Monsalve-Quintero AM, Mora-Robles L, Diaz-Diaz A, et al. Association of Cancer Diagnosis and Therapeutic Stage With Mortality in Pediatric Patients With COVID-19, Prospective Multicenter Cohort Study From Latin America. Front Pediatr. 2022 ;10:885633. [CrossRef]
- Pathak, E.B.; Salemi, J.L.; Sobers, N.; Menard, J.; Hambleton, I.R. COVID-19 in Children in the United States: Intensive Care Admissions, Estimated Total Infected, and Projected Numbers of Severe Pediatric Cases in 2020. J Public Health Manag Pract. 2020 Jul/Aug;26(4):325-333. [CrossRef]
- de Siqueira Alves Lopes A, Fontes Vieira SC, Lima Santos Porto R, Santana Santos V, Fontes Leite DC, Eduardo Cuevas L, et al. Coronavirus disease-19 deaths among children and adolescents in an area of Northeast, Brazil: why so many? Trop Med Int Health. 2021 Jan;26(1):115-119. [CrossRef]
- Flaxman S, Whittaker C, Semenova E, Rashid T, Parks RM, Blenkinsop A, et al. Assessment of COVID-19 as the Underlying Cause of Death Among Children and Young People Aged 0 to 19 Years in the US. JAMA Netw Open. 2023 Jan 3;6(1):e2253590. [CrossRef]
- Efendi F, Haryanto J, Has EMM, Makhfudli M, Indarwati R, Kuswanto H, et al. Predictors of Mortality Among Children with Confirmed and Suspected Cases of COVID-19 in East Java, Indonesia. J Multidiscip Healthc. 2023 Feb 7;16:355-362. [CrossRef]
- Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review. JAMA Pediatr. 2020;174:882-9. 1467. [CrossRef]
- Ortiz-Prado E, Izquierdo-Condoy JS, Fernandez-Naranjo R, Vasconez J, Dávila Rosero MG, Revelo-Bastidas D, et al. The deadly impact of COVID-19 among children from Latin America: The case of Ecuador. Front Pediatr. 2023 Apr 21;11:1060311. [CrossRef]
- Brazil – Ministério da Saúde [homepage on the Internet]. SRAG 2020 - Banco de Dados de Síndrome Respiratória Aguda Grave - incluindo dados da COVID-19 - Conjuntos de dados - Open Data [cited 2021 Oct 19]. Available from: https://opendatasus.saude.gov.br/dataset/bd-srag-2020.
- Sousa, B.L.A.; Silva, C.A.; Ferraro, A.A. An update on the epidemiology of pediatric COVID-19 in Brazil Editorial Rev. Paul. Pediatr. 2022; 40. [CrossRef]
- Mucalo L, Brandow AM, Dasgupta M, Mason SF, Simpson PM, Singh A, et al. Comorbidities are risk factors for hospitalization and serious COVID-19 illness in children and adults with sickle cell disease. Blood Adv. 2021 Jul 13;5(13):2717-2724. [CrossRef]
- Trapani S, Rubino C, Lasagni D, Pegoraro F, Resti M, Simonini G,et al. Thromboembolic complications in children with COVID-19 and MIS-C: A narrative review. Front Pediatr. 2022 Aug 11;10:944743. [CrossRef]
- Conway EM, Mackman N, Warren RQ, Wolberg AS, Mosnier LO, Campbell RA, et al. Understanding COVID-19-associated coagulopathy. Nat Rev Immunol 2022; 22: 639–649. [CrossRef]
- Renzaho, A.M.N. The Need for the Right Socio-Economic and Cultural Fit in the COVID-19 Response in Sub-Saharan Africa: Examining Demographic, Economic Political, Health, and Socio-Cultural Differentials in COVID-19 Morbidity and Mortality. Int J Environ Res Public Health. 2020 ;17(10):3445. [CrossRef]
- Heo, M.H.; Kwon, Y.D.; Cheon, J.; Kim, K.B.; Noh, J.W. Association between the Human Development Index and Confirmed COVID-19 Cases by Country. Healthcare (Basel). 2022 Jul 29;10(8):1417. [CrossRef]
Figure 1.
Patients hospitalized with COVID-19 by age group and by year.
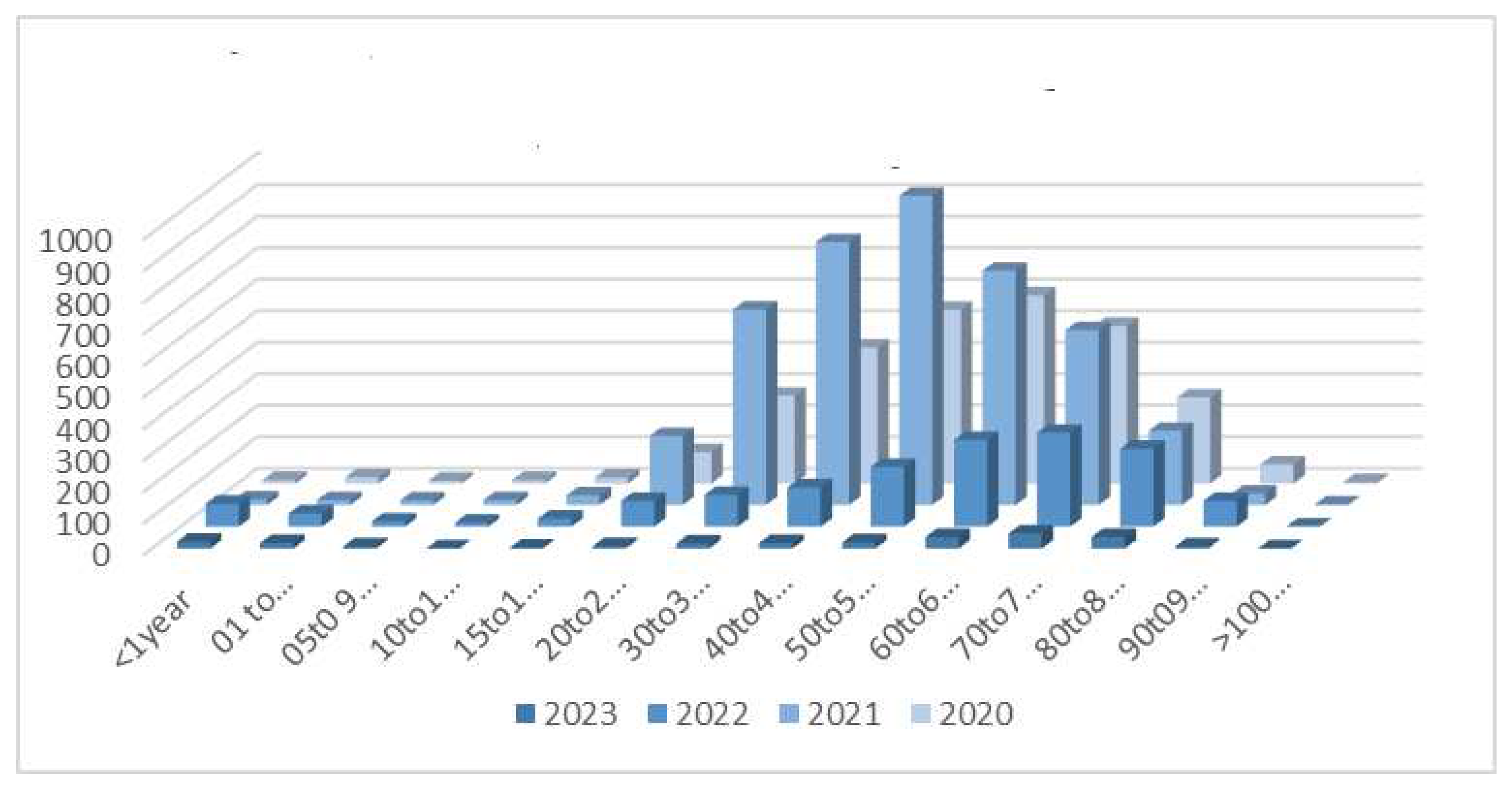
Figure 2.
Shows hospitalizations and mortality in children and adolescents.

Figure 3.
Distribution of the percentage of hospitalized cases for COVID-19, Influenza and Respiratory syncytial virus (RSV) infection at FUNFARME according to month and etiological agent from Oct 21 to 7/24/2023.
Figure 3.
Distribution of the percentage of hospitalized cases for COVID-19, Influenza and Respiratory syncytial virus (RSV) infection at FUNFARME according to month and etiological agent from Oct 21 to 7/24/2023.
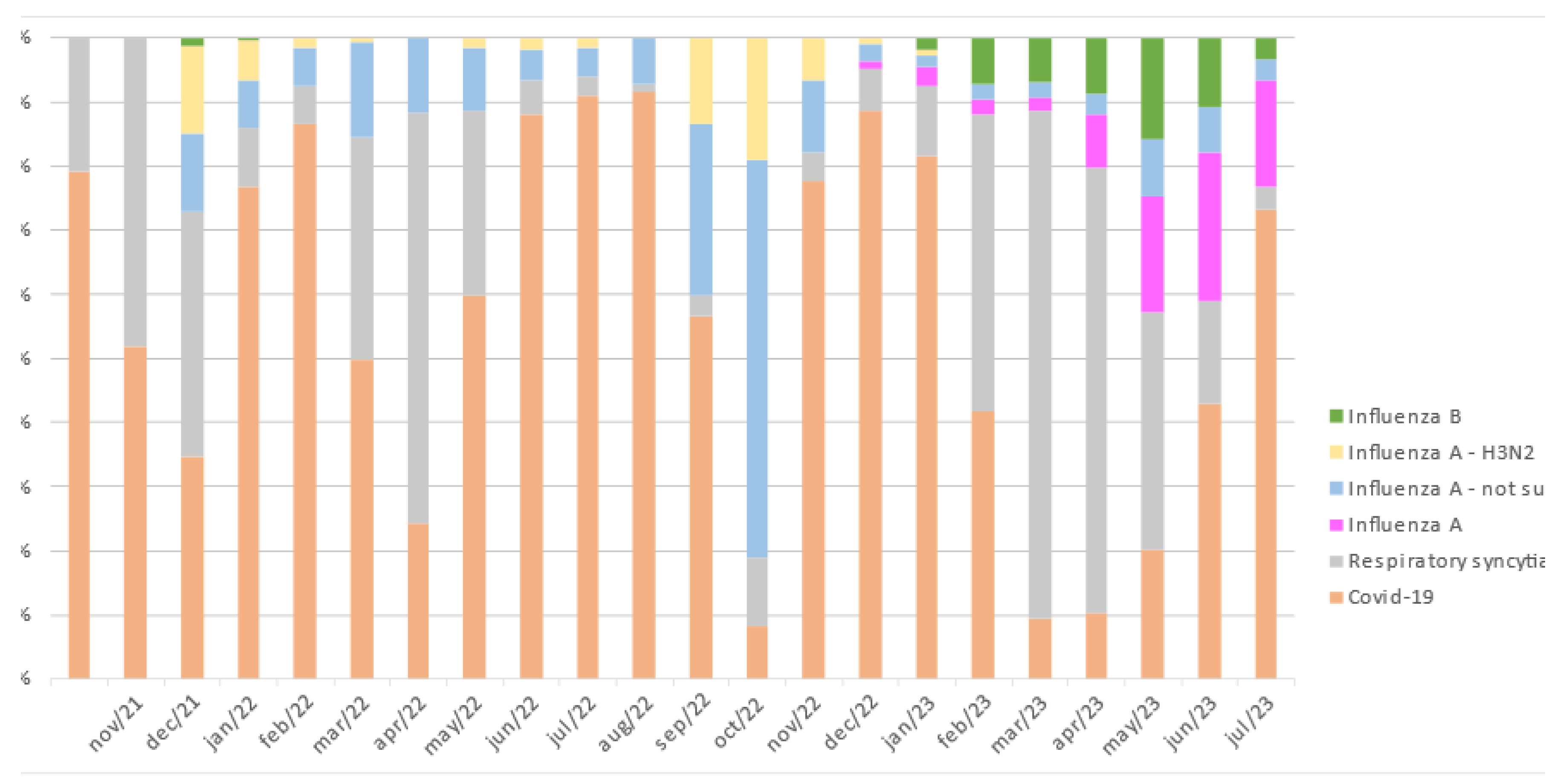

Table 1.
Hospitalizations and deaths for different age groups from March 2020 to July 2023.
| Age | 2020 | 2021 | 2022 | 2023 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| years | Hospital | Deaths | Hospital | Deaths | Hospital | Deaths | Hospital | Deaths | Hospital | Deaths | |
| < 1 | 11 | 0 | 18 | 1 | 73 | 1 | 21 | 0 | 123 | 2 | |
| 1-4 | 20 | 1 | 16 | 1 | 42 | 2 | 17 | 0 | 95 | 4 | |
| 5-9 | 9 | 0 | 15 | 1 | 17 | 0 | 6 | 0 | 47 | 1 | |
| 10-14 | 11 | 1 | 16 | 0 | 13 | 0 | 0 | 0 | 40 | 1 | |
| 15-19 | 19 | 2 | 31 | 0 | 26 | 2 | 2 | 0 | 78 | 4 | |
| 20-29 | 100 | 8 | 219 | 20 | 82 | 4 | 7 | 1 | 408 | 33 | |
| 30-39 | 279 | 13 | 620 | 76 | 101 | 8 | 14 | 2 | 1014 | 99 | |
| 40-49 | 431 | 27 | 834 | 125 | 125 | 11 | 17 | 3 | 1407 | 166 | |
| 50-59 | 551 | 85 | 981 | 241 | 190 | 23 | 19 | 3 | 1741 | 352 | |
| 60-69 | 597 | 147 | 744 | 287 | 275 | 71 | 34 | 11 | 1650 | 516 | |
| 70-79 | 500 | 187 | 555 | 257 | 298 | 90 | 47 | 11 | 1400 | 545 | |
| 80-89 | 273 | 141 | 236 | 136 | 247 | 94 | 34 | 6 | 790 | 377 | |
| 90-99 | 61 | 43 | 37 | 22 | 82 | 28 | 6 | 0 | 186 | 93 | |
| >100 | 4 | 3 | 2 | 1 | 1 | 0 | 0 | 0 | 7 | 4 | |
| TOTAL | 2866 | 658 | 4324 | 1168 | 1572 | 334 | 224 | 37 | 8986 | 2197 | |
Table 2.
Comorbidities associated with COVID-19 that led to death.
| Age | Sex | Comorbidity | Infect | ATB | Image | VAD | MV | ICU | DS | HS |
|---|---|---|---|---|---|---|---|---|---|---|
| Years | ||||||||||
| 19 | F | Hodgkin’s lymphoma | Y | Y | TC 25% compromised (frost glass) | Y | Y | Y | Y | 45 |
| 14 | F | Down Syndrome | Y | Y | TC - 70% | Y | Y | Y | Y | 12 |
| 2 | M | Down Syndrome, heart disease | Y | Y | Rx | Y | Y | Y | Y | 5 |
| 19 | F | Down Syndrome, schizophrenia, | Y | Y | TC - 50% compromised | Y | Y | Y | Y | 5 |
| asthma, corrected heart disease | ||||||||||
| 0 | M | None | Y | Y | Rx - infiltrated | Y | Y | Y | Y | 5 |
| 2 | M | encephalopathy | Y | Y | Rx | Y | Y | Y | Y | 24 |
| 5 | M | Renal transplant | Y | Y | TC > 50% infiltrated (frosted glass) | Y | Y | Y | N | 20 |
| 3 | M | Congenital heart disease | Y | Y | Rx | Y | Y | Y | N | 3 |
| 16 | F | Tumor CNS | Y | Y | TC > 50% infiltrated (frosted glass) | Y | Y | Y | Y | 10 |
| 17 | F | Lupus | Y | Y | TC < 25% | Y | Y | Y | N | 55 |
| 3 | F | Hydranencephaly | Y | Y | Rx | N | Y | Y | Y | 1 |
| 1 | F | Congenital heart disease | N | N | Rx | Y | Y | N | N | 1 |
ATB: Antibiotics; VAD: vasoactive drugs; MV: Mechanical ventilation; ICU: Intensive care unit; DS: Dialysis support; HS: Hospitalization stay; CNS: Central nervous system; F:Female; M:Male Y:Yes; N:No.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



