
Submitted:
23 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
Magnesium alloy stents have been extensively studied in the field of biodegradable metal stents due to their exceptional biocompatibility, biodegradability and excellent biomechanical properties. Nevertheless, the specific in vivo service environment causes magnesium alloy stents to degrade rapidly and fail to provide sufficient support for certain time. This paper presents an overview of the development history and protection strategies for magnesium alloy stents. Alloying, optimizing stent structure and preparing protective coating have improved the corrosion resistance of magnesium alloy stents. Based on the corrosion mechanism of magnesium alloy stents, as well as their deformation during use and environmental characteristics, we present some novel solution strategies aiming at reducing the corrosion rate of magnesium alloys and enhancing the comprehensive performance of magnesium alloy stents. These strategies include adapting protective coatings for the deformation of the stents, preparing rapid endothelialization coatings to enhance the service environment of the stent, and constructing coatings with self-healing functions. It is hoped that this review can help to understand the development of magnesium alloy cardiovascular stents and solve the problems related to magnesium alloy stents in clinical applications at the early implantation stage.
Keywords:
Magnesium alloy
; Cardiovascular stent
; Corrosion resistance
; Protective coating
; Rapid endothelialization
1. Introduction
Cardiovascular diseases (CVDs) are the leading cause of death globally, taking an estimated 17.9 million lives each year[1]. The application of vascular stents for the treatment of the associated coronary and peripheral artery disease has become one of the most effective and rapidly adopted medical interventions[2]. The entire evolution of vascular stents includes the first-generation of bare-metal stents, the second-generation of drug-eluting stents, and the third-generation of biodegradable drug-eluting stents (Figure 1).
The bare-metal stents (BMS) were invented and used in clinical settings firstly. In 1987, the clinical implantation of stainless steel stent into human coronary artery was firstly reported[3]. BMS could provide arterial support and significantly improve the clinical and angiographic outcomes in patients[4]. However, implantation of bare metal stents (BMS) might result in symptoms including in-stent restenosis (ISR) and stent thrombosis (ST)[5,6]. In order to address the issues of ISR and ST associated with BMS, drug-eluting stents (DES) were developed, which could load and deliver drugs such as sirolimus and paclitaxel through a polymer coating on the surface of the bare metal stents[7,8]. However, as a permanent implant in the vasculature, DES still brought the potential risks of thrombogenicity, delayed re-endothelialization, mismatches in mechanical behavior, long-term endothelial dysfunction, and chronic inflammatory local reactions[9,10].
To construct innovative stent systems to resolve the above clinical issues, bioabsorbable polymer and metal stents have attracted increasing attention due to their favorable biodegradability and biocompatibility[11]. The most commonly used bioabsorbable polymer material is poly-L-lactic acid (PLLA), and the PLLA-based bioabsorbable polymer stents have achieved promising clinical results. The bioabsorbable everolimus-eluting stent system (Absorb; Abbott Vascular, Santa Clara, CA, USA) is made of a bioabsorbable polylactic acid backbone which is coated with a more rapidly absorbed polylactic acid layer carrying the antiproliferative drug, everolimus (Novartis, Basel, Switzerland)[12]. The first bioabsorbable polymer stent was designed to provide comparable radial strength and anti-restenosis efficacy comparable to the metallic drug-eluting stents[13]. Whereas PLLA may need 24 months or more to degrade, mismatching the ideal implanting process of integrity for the first 6–12 months and full degradation after 12–24 months[2]. The issue of reduced stent area and stent malapposition is a challenge for the polymeric stent, which may initially lack sufficient radial force, resulting in subsequent recoil and malapposition of the stent as bioabsorption is further decreased[14]. Due to the lower radial strength, a thicker strut size is necessary for these polymer stents compared to the majority of metal stents. Clinical trials have demonstrated that bioresorbable vascular stents (BVS) were associated with increased rates of composite device-oriented and patient-oriented adverse events at 2 years postoperative follow-up[15]. The leading mechanism underlying very late stent thrombosis was the stent discontinuity, which suggested an unfavorable resorption-related process, followed by malapposition and neoatherosclerosis[16]. Abbott Vascular called a halt to sales of the Absorb bioresorbable vascular stent on September 14, 2017[17].
Degradable metal stents possess higher mechanical strength and biocompatibility compared to polymer stents. The bioabsorbable metal stents include magnesium alloy stents, iron alloy stents and zinc alloy stents. Iron alloy stent possesses good mechanical properties, high elastic modulus and high radial strength, which can well satisfy the mechanical requirements of stent. Meanwhile, the hemolysis rate of pure iron is less than 5%, and there is no sign of thrombosis, indicating that iron-based stent has good hemocompatibility[18]. However, the complete biodegradation time of iron alloy stent is still too long as it far exceeds the time required for arterial remodeling and healing (6-12 months)[19]. In general, the alloy corrodes slowly for stenting applications and accumulates a large amount of corrosion product that repels surrounding cells and biological matrix and does not appear to be excreted or metabolized at an appreciable rate, so future research on iron alloy stents should focus on improving the efficiency of absorption, conversion, metabolism, and elimination of the degradation products[20]. As an essential element in the human body, zinc has a suitable degradation rate, making it one of the choices for biodegradable metal stents[21,22]. The present results revealed that there was no stent thrombosis in the preclinical study. However, zinc-based stent exposed significant “strain-softening” effect that can lead to a limited uniform deformation. This kind of non-uniform deformation is detrimental to the zinc alloy stents, which could possibly lead to unexpected failure[20]. Currently there have been attempts to solve the strain softening problem through some material processing techniques, such as equal-channel angular pressing.
Magnesium alloy stents were the first biodegradable metal stents having been used in clinical applications due to their excellent biocompatibility, biodegradability and favorable mechanical properties. Mg alloy stents could be degraded and completely absorbed in vivo, thus avoiding the neointimal hyperplasia and stenosis caused by long-term foreign body reaction. Compared to bioabsorbable polymer stents, Mg alloys permit rapid expansion and have stable mechanical strength and ductility, which provides better radial support for vessels and facilitates stent processing and crimp-expansion deformation[23]. However, the rapid degradation and localized degradation of Mg alloy stents constrain their clinical application, and rapid degradation of stents may lead to restenosis and loss of mechanical integrity. Based on the computational modelling of the corrosion process, it was found that the heterogeneous corrosion leads to a significant reduction in the supporting performance of stent, but slight reduction in mass loss compared to the homogeneous corrosion[24]. In addition, the degradation of magnesium alloys could cause an elevation of local pH and an accumulation of hydrogen, which may lead to obstruction of blood circuits and tissue necrosis[25]. Rapid degradation can generate high concentrations of Mg ions in a local environment, which may induce coagulation or inflammation, and delay the process of vascular remodeling[26]. Therefore, how to effectively control the degradation behavior of magnesium alloys is of great significance in promoting the clinical application of magnesium alloy stents. This is also the key research issue for biodegradable magnesium alloy stents at present.
To solve this bottleneck problem of rapid degradation of magnesium alloy stents, many studies have been conducted on material composition, structural optimization for stent and protective coating of magnesium alloys, etc. These studies have promoted the forward the development of magnesium alloy stents to various degrees. The first application of biodegradable magnesium alloy stent was a milestone in time[27], marking the incorporation of biodegradable vascular stents into the time coordinates of stent development. Late postoperative follow-up showed that the magnesium alloy stent exhibited certain advantages over the bioabsorbable PLA stent. However, a relatively high incidence of device-oriented composite endpoint (DOCE) was found during the follow-up[28].
This article reviews the development history of magnesium alloy stents, summarizes the protection strategies for the stents, and prospects the future development trend of the stent protection. Focusing on solving the problems of rapid degradation and short-term strut fracture of magnesium alloy stents, unique solution strategies are discussed and proposed, which are expected to create new ways to reduce the degradation rate of magnesium alloys and then improve the comprehensive performance of magnesium alloy stents.
2. Development history of magnesium alloy stents
BIOTRONIK in Germany is dedicated to the research and development of biodegradable magnesium alloy stents, and has developed several generations of products, including Lekton Magic (AMS), DREAMS 1G, Magmaris (DREAMS 2G), and DREAMS 3G, achieving good results in the research[29,30], as shown in Figure 2.
The study of the biodegradable magnesium alloy stent was firstly reported in 2003, using a non-commercial magnesium alloy, AE21 (containing 2 % aluminum and 1 % rare earths), which was implanted into the coronary artery of domestic pigs. There was no stent experienced major problems or initial signs of fracture during implantation, and no significant thrombosis occurred[27]. Waksman et al.[31] compared the safety and efficacy of biodegradable magnesium alloy stents with stainless steel stents in porcine coronary arteries. At 28 days, the magnesium alloy stent began to show signs of degradation. At 28 days and 3 months, the magnesium alloy stent had a significantly smaller area of neointima than the stainless steel stent. However, the reduction in neointimal formation didn't translate into a larger vessel lumen. This could be caused by under-expansion of the stent at deployment, early or late recoil, or all of the above. Within 3 months, the magnesium alloy stents had completely degraded or were in an advanced stage of degradation in porcine vessels. There was a modest degree of neointimal formation, which did not increase between 30 and 90 days. This indicated that the primary reason for restenosis after implantation of biodegradable magnesium alloy stents was an early recoil. This issue could be solved by slowing down the pace of stent degradation[32].
As the first biodegradable magnesium alloy stent, Lekton Magic (Biotronik, Bulach, Switzerland) stent was implanted in 20 patients for the treatment of critical lower limb ischemia[33]. No adverse event was reported during the procedures. Postprocedural color Doppler flow and magnetic resonance demonstrated accurate positioning and expansion of the stents and no early recoil. At 1 month post-operation, no patient showed any symptom of allergic or toxic reactions to the stent material. The primary clinical patency rate at 3 months postoperatively was 89.5%. All patients had no amputation and the limb retention rate was 100%[34]. Afterwards, the stent was evaluated in human coronary arteries by the PROGRESS-AMS study (Clinical Performance and Angiographic Results of Coronary Stenting with Absorbable Metal Stents)[35]. It was demonstrated that biodegradable magnesium alloy stents could be delivered and expanded at high pressure within atherosclerotic coronary arteries, furnishing reliable mechanical supporting and accomplishing a lumen enlargement comparable to the immediate lumen gain attained with customary metal stents. The absence of raised creatine kinase (CK) and ischemic episodes suggested the absence of embolization of stent material in the early phases of stent degradation, indirectly confirming that the degradation of the alloy occurred within the vessel wall, with rapid re-endothelialization and strut coverage. Angiography at 4 months post-operation showed an increased diameter stenosis of 48.4%. Intravascular ultrasound (IVUS) examination of biodegradable metal stents in human coronary arteries revealed that the early recoil significantly contributed to the restenosis within 4 months[36].
To extend vessel support and minimize the neointimal growth, the biodegradable metal stent has been redesigned and layered with a biodegradable poly(lactide-co-glycolide) polymer matrix (PLGA) that contains the anti-proliferative drug paclitaxel[37]. It has comparable efficacy and healing properties to paclitaxel-eluting permanent metal stents in a porcine coronary artery. A multicenter, first-in-human trial (BIOSOLVE-I) of drug-eluting absorbable metallic stents (DREAMS) was undertaken[38]. At 12 months of implantation, DREAMS had a better result of clinical driven target lesion revascularization compared to bare absorbable metal stents (4.7% vs. 26.7%)[35], while maintaining an excellent biosafety. The incidence of target lesion failure for DREAMS at 6 and 12-month periods was comparable to the contemporary drug-eluting stents and the Absorb bioresorbable everolimus-eluting coronary stent systems. Nevertheless, the late lumen loss of DREAMS was not as impressive as those of the other stents.
The DREAMS 2G, also known as Magmaris, was the second generation of drug-eluting absorbable metallic stents. It was coated with a bioabsorbable poly-L-lactic acid (PLLA) carrying sirolimus. Animal tests indicated that the Magmaris had a favorable safety profile[39]. After 12 months post-operation, DREAMS 2G had almost completely degraded in porcine coronary arteries. Strut discontinuities were uncommon at 28 days and increased rapidly up to 90 days, with almost complete degradation of the stent at one year[40].
In order to evaluate the safety and performance of Magmaris in patients with de novo coronary artery lesions, the BIOSOLVE-II and BIOSOLVE-III studies were performed[41,42]. Compared to DREAMS 1G, Magmaris had a more flexible and robust stent structure design, higher bending flexibility, and higher radial force. Sirolimus-loaded PLLA as a drug-eluting coating was more effective on inhibiting the neointima formation. The angiographic performance of Magmaris stents showed that no definite or probable stent thrombosis occurred after 12 months implantation. The late lumen loss of Magmaris has been improved, maintaining a favorable clinical and safety profile. The 30 days and 1 year follow-up data showed that the primary endpoints (death from cardiac causes, myocardial infarction, stent thrombosis) as well as the incidence of target lesions were significantly lower for Magmaris than the Absorb. Biodegradable magnesium alloy stents have presented a more satisfactory safety profile and more favorable clinical outcomes[43]. The Magmaris has gained CE-mark in June 2016[42]. BIOSOLVE-IV verified the safety and efficacy of the Magmaris in a significant sample size of individuals, combined with a highly satisfactory safety profile up to 12 months in a low-risk cohort[44].
However, Bossard et al.[28] found a relatively high incidence of device-oriented composite endpoints (DOCE) and even observed stent collapse and uncontrolled dismantling in the follow-up of patients treated with Magmaris. Most adverse events occurred within 24 months of implantation, with target lesion failure (TLF) occurring rarely thereafter. Signs of stent collapse and stent dismantling were found in the long-term follow-up of patients implanted with Magmaris. As shown in Figure 3(a), the optical coherence tomography (OCT) image shows a collapsed stent, which appears to be a "free-floating" strut (arrow) that is no longer embedded in the coronary artery wall. In addition, there appears to be restenosis of the inner lumen with significant luminal irregularities and tissue protrusion. Figure 3(b) demonstrates uncontrolled dismantling of stent with strut residuals protruding into the vessel lumen (arrows). In addition, the intima appears partially irregular (1-5 o'clock).
Corrosion of the strut is a unique phenomenon of magnesium alloy stents. The corrosion rate of strut may vary among different individuals, and may be accelerated by stent malapposition, focal low pH between the vessel wall and the magnesium alloy stent struts and also by substantial hinging forces[45]. The rapid degradation rate with a loss of radial strength, combined with a potential accelerated healing response at the dilated stenosis, might contribute to the occurrence of restenosis[46]. A certain degree of late stent disruption might also lead to the development of restenosis[47].
The development of the third-generation of drug-eluting magnesium alloy stent (DREAMS 3G) has used a new magnesium alloy, which endows the stent with higher mechanical properties, thinner struts, while maintaining the same resorption time. A new marker concept and an increased size portfolio were adopted by DREAMS 3G, which showed favorable safety and performance outcomes comparable to the contemporary drug-eluting stents[30].
3. Corrosion mechanism of magnesium alloys and stents
In order to solve the problems of short-term collapse and rapid attenuation of support force of magnesium alloy stents in vivo, it is necessary to investigate the most direct reasons leading to the corrosion and fracture of magnesium alloy stents from the corrosion mechanisms of magnesium alloys and stents in order to find effective ways to solve the problems fundamentally.
3.1. Corrosion mechanism of magnesium alloys
Magnesium (Mg) has advantages such as low density and high specific strength, but its chemical activity makes it highly susceptible to corrosion, thus limiting its applications in industry, medical devices and other fields. Corrosion of Mg is essentially an electrochemical process in which Mg is oxidized to MgO and Mg(OH)2, which is a highly susceptible spontaneous reaction. The reaction is as in Equation (1):
The generated MgO layer improves the corrosion resistance of Mg in the dry environment. In a moist environment, the layer formed on the Mg surface contains Mg(OH)2 and MgO. Due to the decomposition of water molecules to form H+ and OH-, leading to the surface hydroxylation of the MgO. At lower water vapor concentrations (greater than 1 ppm H2O), the reaction of magnesium oxide in solid state with water may result in the formation of solid magnesium hydroxide[48].
Liu et al.[49] found that a two-layer film existed on the surface of Mg exposed to water, consisting of an internal MgO layer near the Mg metal and an external porous Mg(OH)2 layer. Mg undergoes electrochemical corrosion in an aqueous environment and the overall reaction is as follows.
The main corrosion products are Mg2+, OH- and H2. The electrochemical theory shows that the corrosion rate of Mg is determined by both anodic and cathodic reactions. The anodic reaction is:
And the cathodic reaction is:
In acidic and neutral aqueous solutions, the surface layer of Mg fails to protect the metal substrate beneath it. When the hydroxide layer dissolves in the aqueous solution, the pH of the solution increases, which leads to the precipitation of Mg(OH)2. It has been shown that the dissolution of the MgO layer is converted to Mg(OH)2 precipitation, which is the corrosion mechanism of Mg. The precipitation of Mg(OH)2 reduces the thickness of the surface MgO layer, which exacerbates the corrosion[48].
Physicochemical characters such as impurity content and alloying elements, microstructures (e.g., grain size and second phases, segregation and intracrystalline orientation errors), plastic deformation and internal stress determine the electrode potentials, oxide features and galvanic corrosion tendency in magnesium alloys[50]. Therefore, the corrosion resistance of magnesium alloys can be improved by changing the alloy composition and constituent phases in magnesium alloys, surface coating protection, and adding corrosion inhibitor.
3.2. Corrosion mechanism of magnesium alloy stents
Compared with magnesium alloy substrate, magnesium alloy stents not only need to withstand media corrosion, but also need to undergo the complex deformation during the compression grip-expansion-pulsation process in the implantation, and the mechanism of corrosion is more complex. The study found that about 95 % of the stent was degraded within 12 months after implantation of magnesium alloy stent[51]. The degradation and absorption of the stent occur in two stages. Initially, the magnesium alloy is converted into hydrated magnesium oxide. Subsequently, the magnesium oxide is converted into magnesium phosphate, which is further replaced by amorphous calcium phosphate. During this process, the metallic Mg is removed from the amorphous matrix via diffusion and is absorbed by the body. The amorphous calcium phosphate, along with the other elements in the alloy and markers as well, remains in the tissue[41].
The stent should undergo both uniform corrosion and stress corrosion. Corrosion product is going to form and cover the entire exposed surface of the stent in a "layer-by-layer" pattern during the uniform corrosion. However, the stress corrosion is prone to occur at the place with high residual stress, which would cause the stent ring shatter quicker than the other locations[52]. The residual stress is generated during the grip and expansion of the stent for implantation, and the presence of stress would accelerate the rate of degradation and the attenuation of the supporting properties[53]. Since the integrity of the stent is usually destroyed firstly at the location of stress concentration, it can be estimated that the stress corrosion should play a major role for the stent failure[54].
Aside from the residual stress generated, the protective coating on the surface of the stent may crack as the stent deforms. Compared with the bare magnesium alloy stents, the HF-treated stents showed excellent corrosion resistance without deformation. However, small fragments and cracks presented on the surface of the HF-treated magnesium alloy stent after deformation, which accelerated corrosion of the stent [55]. During the corrosion process, hydrogen may escape locally, pushing away the polymer coating and weakening the adhesion of the outer polymer coating to the stent, which would subsequently accelerate the degradation of magnesium alloy stent[56].
The other reason leading to the premature failure of magnesium alloy stent is the cyclic loading applied by arterial pulses. Magnesium alloys were found to have greater corrosion rates under cyclic loading, and the corrosion rate increases with increasing the cyclic loading. In a corrosive environment with cyclic loading, corrosion pits could cause crack initiation with release of the stress concentration[57]. The mechanism of fracture failure was explored by Chen et al. [58]. This study implanted 18 drug-eluting biodegradable AZ31B stents into porcine coronary arteries, showing a large number of fractures leading to the loss of structural integrity. During the crack formation, there was no degradation product on the cracks. However, the degradation products on the cracks increased as the implantation time increased. It was inferred that the loss of structural integrity of the AZ31B stent might be the result of stress concentration, degradation and microstructural change. Shen et al.[59] published the first paper on numerical simulation of the corrosion fatigue behavior of magnesium alloy stents under cyclic loading in the physiological environment. A numerical continuum damage mechanics model was developed using the finite element method to explain the corrosion fatigue of magnesium alloys and the application in coronary stents. The total mass loss of the stent was caused by both the corrosion damage and the fatigue damage. The fatigue loading or cyclic stress accelerated the degradation of the stent, potentially leading to premature the stent failure.
4. Traditional strategy for protection of magnesium alloy stents
According to the corrosion mechanisms of both magnesium alloys and stents, different strategies for protection of magnesium alloy stents were attempted. Alloying is an effective way to improve the mechanical properties of metallic materials, and the addition of alloying elements can affect the corrosion behaviors of materials. So how to balance the mechanical property and corrosion resistance is very important. In addition, the structure optimization for magnesium alloy stent could reduce the maximum residual stress by lowering the concentration of residual stress, thereby reducing the degree of stress corrosion. The last and most important strategy is preparation of protective coating on magnesium alloy stents. The protective coating is as a physical barrier against the penetration of corrosive media, and its effectiveness is particularly important for magnesium alloy stents that need to undergo complex deformation.
Above three aspects have improved the corrosion resistance of magnesium alloy stents at certain extent. Next, the related research progresses of these three aspects are introduced one by one.
4.1. Alloying design for magnesium alloy stents
Commonly employed alloying elements in magnesium alloys consist of basic metal elements such as Al, Zn, Mn, Zr, Li and rare earth elements, each alloying element has its own effect. Aluminum (Al) is a crucial element in magnesium alloys as it enhances their corrosion resistance and strength. Aluminum can form the β-phase (Mg17Al12) in magnesium alloys. Increasing its content in the basal phase facilitates the creation of highly corrosion resistant surface layer with a substantial aluminum content[60]. As the aluminum content increases, the β-phase increases and more β-phase precipitates along the grain boundaries, protecting the magnesium alloy matrix. By micro-alloying zinc (Zn) in the magnesium matrix, there is a decrease in the stacking fault energy and an increase in the plastic deformation capacity by effectively activating the non-basal slip. Zirconium (Zr) acts as a significant refining agent for the grains and elevates the toughness of magnesium alloy[26]. The Mg-Li (lithium) alloy is a newly developed system with ultra-high ductility and potential applications in vascular stents. However, the presence of Li causes a reduction in mechanical strength of the alloy. Rare-earth elements are added into magnesium alloys that can play the roles of solid solution strengthening by forming intermetallic phases and improvement of the corrosion resistance of magnesium alloys. Based on the specific alloying effects of each alloying element, three series of magnesium alloys have been attempted to be applied to the vascular stent at present. They are AZ series alloys (AZ31 and AZ91), rare-earth series alloys (WE43[33], Mg-Zn-Y-Nd (ZE21B)[61], Mg-Nd-Zn-Zr (JDBM)[62]), and Mg-Li series alloy[63] (Figure 4).
The effect and existing problems of different series of magnesium alloys used for vascular stents are reviewed below. AZ series magnesium alloys as a traditional commercially used material possess excellent and stable comprehensive properties. In the previous study[58], 18 drug-eluting biodegradable AZ31B alloy stents were implanted into porcine coronary arteries, and there were a large number of fractures formed on the stent strut leading to a loss of structural integrity. Despite some recoil and lumen loss, the lumen remained unobstructed after 3 months implantation. The occurrence of fracture was related to the strong stress corrosion of the alloy.
Hence, rare-earth series magnesium alloys were designed and prepared, including WE43 (used as the first-in-men magnesium alloy stent by Biotronik), Mg-Zn-Y-Nd (ZE21B) alloy developed by Zhengzhou University, China, and Mg-Nd-Zn-Zr (JDBM) alloy developed by Shanghai Jiao Tong University, China.
Mg-Y-Gd-Nd alloy (WE43) is a commonly used material for manufacturing biodegradable magnesium alloy stents, and Y(yttrium) and Nd (neodymium) as alloying elements can improve the corrosion resistance of the alloy. Meanwhile, studies have shown that Y, Nd and Gd (gadolinium) are not cytotoxic[64]. The WE43 alloy stent was implanted in patients for the treatment of severe lower limb ischemia[33]. No adverse events were reported during the procedure, and no patients showed any symptoms of allergic or toxic reactions to the stent material. Magmaris (formerly known as DREAMS 2G), based on WE43 alloy, is a balloon-expandable, sirolimus-eluting, biodegradable metal stent mounted on a rapid exchange delivery system[51]. This was the pioneer product for biodegradable metal stents, which received CE approval in June 2016. It has exhibited promising clinical outcomes so far.
Mg-Zn-Y-Nd alloy (ZE21B) was developed with low levels of zinc and yttrium by Zhengzhou University, China, in 2010[61]. Zinc is known to improve the corrosion resistance of magnesium alloys, leading to the cast Mg-Zn-Y-Nd alloy exhibiting a higher corrosion potential (-1.76 V) as compared to the cast Mg-Y-Gd-Nd alloy (-1.95 V). The Mg-Zn-Y-Nd alloy was prepared through a sub-rapid solidification process, exhibiting superior corrosion resistance in a dynamic SBF. The mechanical properties and corrosion resistance of Mg-Zn-Y-Nd alloy can be further improved by different processing techniques and heat treatments, for example, cyclic extrusion compression (CEC)[65]. The findings demonstrated that the grain size in the alloy was refined to 1µm with CEC treatment. Furthermore, the second phase distributed in a grid shape along the grain boundaries, and the nano-particles uniformly distributed within the grain, leading to a significant improvement in mechanical properties of the alloy. The alloy also displayed uniform corrosion. The corrosion current density of the alloy was observed to decrease from 2.8 × 10-4 A/cm2 to 6.6 × 10-5 A/cm2. In 2018, Wang et al.[66] processed tube blanks of Mg-Zn-Y-Nd alloy by hot extrusion. The annealed and drawn fine tubes exhibited superior mechanical properties. Moreover, the fine tubes demonstrated uniform corrosion in the simulated body fluid and exhibited excellent corrosion resistance. In 2021, Du et al.[67] processed fine tubes of Mg-Zn-Y-Nd alloy by a HTHE (long-time and high-temperature heat treatment, large-reduction-ratio hot extrusion) process, obtaining a refinement of the coarse secondary phase uniformly distributed in the matrix of fine tubes.
Mg-Nd-Zn-Zr (JDBM) alloy was designed by Shanghai Jiao Tong University (SJTU) for biomedical applications[62]. Nd was used as the main alloying element for strengthening, which was revealed by diminishing the stacking fault energy of the basal plane and producing a pinning effect on the base slip[26]. Additionally, Zr serves as a potent grain refiner in magnesium alloys with better biocompatible[68]. The extruded JDBM alloy exhibited superior corrosion resistance with slight uniform corrosion. It was found that the corrosion rate of JDBM alloy in Hank's solution was significantly slow at 0.28 mm/year compared to AZ31 alloy at 1.02 mm/year[69], covered by a more compact and protective layer preventing the pitting corrosion at the early stage of immersion. Furthermore, bare JDBM stents were implanted into the common carotid artery of New Zealand white rabbits to evaluate the safety, efficacy and degradation behavior of the stent[70]. The results indicated that the bare JDBM stent was effective and safe, and complete re-endothelialization occurred within 28 days. The majority of the JDBM stent struts underwent in situ replacement by degradation products in 4 months.
Besides these, the Mg-Li alloy was developed through mechanisms such as solid solution strengthening, grain refinement and dispersion strengthening, showing superior corrosion resistance at the meanwhile. Bian et al.[71] used a high ductility (>40%) Mg-8.5Li (wt.%) alloy (without rare earth metals and aluminum) to fabricate the stent. Finite element analysis verified the impact of plastic deformation and residual stress, arising from the expansion process, on the degradation of this stent. While the stent showed a favorable degradation rate in vitro (0.15 mm/year), different results were found in vivo (>0.6 mm/year). Further, the stents were well-tolerated by the adjacent tissues in pigs, and no thrombosis was reported. Furthermore, a range of Mg-Li based alloys have been developed, for examples, Mg-Li-Zn ternary alloy[72] and Mg-Li-Al-Zn quaternary alloy[73]. The current research on Mg-Li alloys in cardiovascular stents mainly focuses on the mechanical properties and corrosion resistance, and the toxicity and biocompatibility still need to be further verified.
Above all, the addition of alloying elements has improved the mechanical property and corrosion resistance at a certain extent, but it has not well met the clinical demand for magnesium alloy stent. So other methods should be adopted.
4.2. Optimization of magnesium alloy stent structure
Generally, the radial strength, recoil and non-uniform expansion (a reduced dog-boning effect) during expansion as well as the in-stent restenosis of the stents are influenced by the structures of the stents[74]. For magnesium alloy stent, the structure optimization is another way to improve its corrosion resistance, due to the decrease of the stress concentration and stress corrosion. Finite element analysis (FEA), a simple and efficient method, has been widely used in recent years for structural design and optimization of magnesium alloy stents. Wu et al.[54] found that the width of the strut was increased by roughly 48%, resulting in improved safety performance (specifically a 29% decrease in maximum principal stress after tissue recoil and a 14% decrease in maximum principal strain during expansion) and a 24% increase in scaffolding ability. The strut width in the final optimized design was not uniform: the mass of the inner straight parts was decreased more while the mass of the outer curved parts was added, which lowered the maximum strain and produced a more uniform strain distribution. Both decrease in maximum principal strain and more uniform stress distribution should result in a slower stress corrosion. Whereafter, a three-dimensional (3D) FEA model combined with a degradable material model was proposed[75], which was used to analyze three different stent designs made from the AZ31 alloy, crimped and expanded in arterial vessels, through the ABAQUS explicit solver. It was verified that the expectation that the design for magnesium alloy stent with more mass and optimized mechanical properties could increase the stenting time. In addition, Wu et al.[52] compared the corrosion resistance of AZ31B alloy stent samples with two designs (an optimized one[54] and a conventional one), which were underwent balloon expansion and subsequently immersed in D-Hanks' solution for a 14-day degradation test. It indicated that the optimized designed stents exhibited superior corrosion resistance than these of the conventional design, due to the less stress distribution in the former ones. The congruity between numerical simulation and experimental data demonstrated the efficiency of the FEA numerical modelling tool in the design optimization of novel biodegradable magnesium alloy stents.
Increasing the strut size (e.g., larger strut width) and decreasing the uniformly distributed principal stress are two effective ways of improving the mechanical properties of magnesium alloy stents. Although augmented strut width could offer adequate radial support to prolong uniform corrosion time, it might also escalate the maximum principal stress during stent expansion and after recoil, which could lead to the stress corrosion. Degradation failure of magnesium alloy stents typically occurs first at the location of stress concentration. Therefore, the initial phase in designing an optimized stent structure is to decrease the maximum principal stress or strain. Conventional stent design usually maintains constant stent width. For stents with low ductility materials, changing the mass distribution of the stent is also an effective way to optimize the performance of the stent.
4.3. Protective coating on magnesium alloy stents
Making protective coating is an important strategy to improve the corrosion resistance and biocompatibility of magnesium alloy stents. There have been many kinds of coatings on magnesium alloys. Although a single coating typically does not attain these objectives simultaneously, composite coatings comprising various single-layer coatings can present fresh perspectives for investigations on magnesium alloy stents. When preparing a coating on magnesium alloy stent for the surface modification, a chemical conversion film is commonly used to enhance corrosion resistance of the substrate and improve the adhesion between the substrate and the coating. An outer polymer coating is then prepared to covered the chemical conversion film to further enhance the corrosion resistance and biocompatibility.
4.3.1. Inner chemical conversion coating
Chemical conversion treatment can create a protective layer of metal oxides or other compounds on the surface of magnesium alloys, which acts as a physical barrier to effectively separate the magnesium substrate from the corrosive medium. This treatment improves the adhesion of the final deposited coating to the substrate, and then enhances the corrosion resistance and biocompatibility. The commonly used chemical conversion coatings to protect magnesium alloy stents include micro-arc oxidation coating, phosphate conversion coating, magnesium hydroxide coating and magnesium fluoride coating.
Micro-arc oxidation (MAO), also known as plasma electrolytic oxidation (PEO), is an electrochemical technique in which the metal materials are oxidized in a controlled way to obtain the surfaces with specific morphology, thickness and composition, improving the corrosion resistance and biological properties of the metal materials[76]. MAO coating is usually composed of one inner layer and one outer layer. The compact and uniform inner layer could act as a simple barrier, partially preventing the access of the solution to the substrate. The presence of oxygen bubbles during coating growth and thermal stress due to the rapid solidification of the molten oxide in the relatively cold electrolyte could result in a rough outer layer with micro-pores and microcracks[77]. Therefore, while the inner compact layer of the MAO coating could improve the corrosion resistance, the outer layer would allow more corrosive electrolyte to adsorb into the MAO coating, thus decreasing the corrosion resistance of the coating[78].
The phosphate conversion coating has shown high biocompatibility, excellent and robust adhesion, reduced degradation rate and inhibited negative side effects for magnesium alloy implants in animal models[79]. Phosphate conversion coatings such as magnesium phosphate[80], zinc phosphate[81,82] and calcium phosphate[83,84] have been reported in many studies on corrosion resistance of magnesium alloys, as an environmentally friendly surface modification technique. Zai et al.[85] compared the corrosion resistance and biocompatibility of various phosphate conversion coatings, including magnesium phosphate (Mg-P), calcium phosphate (comprising Ca-P, CaMg-P) and zinc phosphate (comprising Zn-P, ZnMg-P, ZnCa-P and ZnCaMg-P). Magnesium alloy substrates, as well as magnesium phosphate and calcium phosphate conversion coatings, showed a mixed form of corrosion involving filiform and pitting during extended immersion in Hanks' solution. Conversely, the primary form of corrosion in zinc phosphate conversion coating was pitting. ZnMg-P provided superior anti-corrosion performance than the other coatings due to its highly stable structure effectively inhibiting the propagation of filiform corrosion. Based on the results of the cell viability test, calcium phosphate conversion coating displayed superior biocompatibility compared to zinc phosphate and magnesium phosphate conversion coatings as well as the bare magnesium alloy substrate. Mao et al.[86] prepared a uniform Mg3(PO4)2 coating on the surface of JDBM alloy by chemical transformation method in a mixed phosphate solution of 5% NaH2PO4 and 3% Na3PO4 with a ratio of 1:1, which improved both corrosion resistance and biocompatibility of the alloy. The phosphate coating with a lamellar structure showed excellent affinity for cells by supporting cell adhesion and spreading. It was found that the magnesium phosphate conversion coating consisted of a precipitated outer layer and an in situ grown inner layer[87].
The degradation product of magnesium in the human body, Mg(OH)2, exhibits superb biocompatibility without toxicity. The hydrothermal method[88,89] can be used to prepare a uniform and compact hydroxide layer on the surface of magnesium alloys, which has a strong adhesion with the matrix and greatly reduce the degradation rate of magnesium alloys. However, as the degradation process of magnesium alloy advances, it results in the formation of porous Mg(OH)2 on the surface. Mg(OH)2 coating contains micro-pores and microcracks that function as transport channels for corrosive media. Therefore, these coatings do not provide long-term and effective protection for magnesium alloys. In order to improve the corrosion resistance of hydroxide coating, the layered double hydroxides (LDH) coating was further developed. The Mg-Al LDH has been considered as an effective agent to retard the corrosion reaction. Its atomic structure consists of brucite-like octahedral layers and these layers are charged positively by the replacement of some Mg2+ with Al3+ ions[90]. The carbonate-based Mg–Al LDH enabled to trap Cl− anion in a corrosive environment in the interlayer of the LDH, allowing the layer to protect the magnesium alloy against the corrosion[91]. The Mg-Al LDH coating on magnesium alloys showed favorable corrosion resistance both in vitro and in vivo, with significant cell adhesion, migration and proliferation [89]. The layered double hydroxide (LDH)/poly-dopamine (PDA) composite coating prepared on the surface of AZ31 alloy could significantly improve the corrosion resistance of the alloy[92]. However, it was found that the LDH coating was not always superior to the single hydroxide coating. Zhang et al.[93] fabricated three kinds of hydroxide coatings with nano-sheet structures, Mg(OH)2, Mg-Fe LDH and FeOOH, on the surface of a PEO-treated magnesium alloy, which completely closed the micro-pores formed during the PEO treatment process. Compared with PEO-treated magnesium alloy, the corrosion resistance and biocompatibility of the magnesium alloy with hydroxide coating was significantly enhanced, and the trend was as follows: FeOOH > Mg-Fe LDH > Mg(OH )2 > PEO coatings. The FeOOH coating can be used as a novel potential coating for the surface modification of magnesium alloy implants. Above coatings all can improve the corrosion resistance of magnesium alloys, but whether they can undergo the deformation of magnesium alloy stents during the implantation can be suspected.
The fluoride conversion coating, which possesses uniform and controllable thickness and relatively high density, has a potential to considerably enhance the corrosion resistance and inhibit degradation of magnesium alloys. Mao et al.[94] prepared a uniform and compact MgF2 film by chemical conversion on the surface of JDBM using hydrofluoric acid (HF). The MgF2 film could effectively improve the corrosion resistance of JDBM, while significantly decreasing the hemolysis rate of the alloy. In order to reduce the pollution of HF to the laboratory environment, Mao et al.[95] developed an eco-friendly and simple method to prepare nano-scale MgF2 film on JDBM through chemical conversion treatment of the alloy in a 0.1 M potassium fluoride (KF) solution. The film had a uniform and dense physical structure that significantly reduced the corrosion rate. Whereafter JDBM stents coated with MgF2 film were implanted into rabbit abdominal aorta, which confirmed the excellent tissue compatibility without thrombosis or restenosis. Li et al.[96] investigated the degradation and the related mechanism of AZ31B alloy with fluoride conversion coating. After the alloy with fluoride conversion coating was immersed in Hank’s solution, MgF2 in the coating dissolved into F ions and Mg ions. Owning to the low solubility of MgF2, formation rate of Mg(OH)2 was slow, giving rise to an even corrosion resistant coating. Upon penetration of H2O and Cl- into the alloy substrate, the alloy began to degrade, forming Mg(OH)2 and H2. The degradation of the magnesium alloy with fluoride conversion coating proceeded gradually, migrating inward layer by layer. The HF-treated magnesium alloy stents exhibited excellent corrosion resistance without expansion compared to the bare stents. However, after stent expansion, small fragments and cracks appeared on the surface of HF-treated magnesium alloy stents, leading to an accelerated corrosion rate[55]. Cardiovascular stents are constantly subjected to the cyclic loading due to heartbeats, and microcracks on the surface of the stent severely affect implantation stability. So, the fluoride conversion coating still could not satisfy the high requirement for the corrosion resistance of magnesium alloy stents, and further treatment is still needed to improve the corrosion resistance and biosafety of the magnesium alloy stents. The inorganic base layer has been utilized as a pretreatment coating to form a composite coating with polymer, which can improve the corrosion resistance and biocompatibility of magnesium alloy stents.
4.3.2. Outer polymer coating
Compared with the inner inorganic coating, polymer coatings could endow magnesium alloy stent with superior corrosion resistance and biocompatibility. At the same time, polymer coatings can serve as a drug delivery platform, fulfilling various medical functional requirements. However, when a polymer protective coating is prepared on the surface of magnesium alloy directly, the corrosion medium permeated through the polymer coating would lead to rapid corrosion of magnesium matrix and hydrogen release. It could lead to gas accumulation underneath the coating, causing the coating to crack and failure[56,97]. Therefore, magnesium alloys often need to be pre-treated before the polymer coating preparation, which provides a physical barrier to the substrate and at the same time improve the bonding between the substrate and the outer polymer coating. There are a large number of polymer coatings for magnesium alloy stents, owning excellent deformability.
- Polylactic acid (PLA) coating
Polylactic acid is a hydrophobic aliphatic polyester, which is a thermoplastic, biodegradable, and biocompatible synthetic polymer with exceptional strength and modulus. It is classified as generally recognized as safe (GRAS) by the Food and Drug Administration (FDA) of United States and is already used in industrial packaging and many medical devices[98,99].
The PLA coating significantly reduces the degradation rate of magnesium alloy stent, thus providing radial support to the vascular wall over a 6-month period[100]. However, the bonding between PLA and magnesium alloy is weak, and the surface of the alloy is usually treated with fluorination to improve the adhesion[55]. The MgF2 layer on the surface of magnesium alloys is smooth and compact, but with some micro-pores. Preparation of PLLA coatings by ultrasonic atomization spraying could well cover these pores and provide a good physical barrier[101]. The fluoride-treated magnesium alloy stents could remain unchanged in the neutral axis direction after crimping and dilating with a balloon catheter, while the coating appeared brittle and flaky at the deformed radius. In contrast, the PLLA coating prepared outside the fluoride-treated magnesium alloy stents had a homogeneous and pinhole-free appearance on the surface and did not show cracks even after curling and dilation. Animal experiments also showed that fluoride-treated magnesium alloy stents with PLLA coating exhibited better corrosion resistance and longer supports compared to the fluoride-treated magnesium alloy stents, while also exhibiting excellent biocompatibility[102]. The composite coating prevented the penetration of erosion ions into the magnesium matrix to improve the corrosion resistance and reduce the corrosion rate. The PLA coating could eliminate the prior porous defects through a critical re-melting treatment, which significantly improved the corrosion resistance of the magnesium alloy stents[103].
It has been found that the addition of certain specific nanoparticles to PLA coatings could improve the corrosion resistance and show better biocompatibility. Shi et al.[104] added 2 % Mg(OH)2 particles to PLLA coatings to improve protective ability of the coating. The incorporation of Mg(OH)2 particles decreased the hydrophobicity and enhanced the water absorption of the PLLA. As a result of polymer swelling induced by water ingress, numerous defects/channels were created in the polymer coating due to the expansion of the coating volume during the swelling process. Consequently, H2 was able to diffuse through the composite coating more easily than through the compact PLLA coating. Therefore, H2 did not accumulate to create gas pockets beneath the coating, which prevented the coating from peeling on the substrate. Taking a similar strategy, Park et al.[105] integrated silica nanoparticles that were surface-functionalized with hexadecyltrimethoxysilane (mSiNP) into a PLLA coating (Figure 5). The mSiNPs that were exposed contributed to the hydrophobicity of the coating, which could interfere with initial water penetration; in addition, the embedded particles could extend the water transport path to increase the time delay to contact with the magnesium alloy substrate. The delay hindered the degradation of the magnesium alloy, leading to a small amount of evolved hydrogen gas and a low concentration of the released magnesium ions. Meanwhile, the released silicon ions were considered to be a driving factor of angiogenesis by activating the synthesis of vascular endothelial growth factor (VEGF) and its receptor (VEGF receptor 2), resulting in increased proliferation, migration, motility and differentiation of endothelial cells.
However, the PLA coating is relatively hard and brittle, and the coating could peel and crack on the surface after the stent expands, causing serious localized corrosion and deeper pits[106].
- Poly (lactic-co-glycolic acid) (PLGA) coating
PLGA is another protective coating for magnesium alloys to reduce the degradation rate and enhance the cell adhesion[107], which is approved by the FDA and European Medicine Agency (EMA) in various drug delivery systems for humans[108].
As a single protective coating, PLGA may not effectively improve the corrosion resistance of magnesium alloy as expected, which is related to the bulk erosion of PLGA[109]. As corrosion medium is easy to diffuse into and through PLGA coating, both PLGA and magnesium alloy begin to degrade simultaneously. Once bulk erosion has started, by-products of polymer degradation can react with the corroded magnesium ions or magnesium hydroxide, forming soluble magnesium lactates or magnesium glycolates. These can prevent the formation and growth of a dense and thick layer of corrosion protective magnesium hydroxide, and the polymer may provide little or no protection for the following time[97]. When the PLGA coating was applied to magnesium alloy stent alone, there were several wrinkles, creases and partial detachment appeared after expansion process, which could not provide good protection for the stent[110].
- Polycaprolactone (PCL) coating
Polycaprolactone is an aliphatic polyester consisting of hexanoic repeat units. Its wide applicabilities and interesting properties (controlled degradability, miscibility with other polymers, biocompatibility and potential to be made from monomers derived from renewable sources) make it a very useful polymer[111]. PCL inhibits gas evolution on the base metal and is a promising candidate as a coating material for controlling degradation rate and mechanical strength of magnesium alloys[98]. PCL has been approved by FDA for use in a wide range of biomedical products such as drug delivery, bone graft substitution and tissue engineering applications[112,113,114].
The glass transition temperature (Tg) of PCL was measured by differential scanning calorimetry (DSC) to be (-64.5 ± 3.9°C)[106], which implies that the PCL coating is in a rubbery and flexible state in the biological environment, and the coating maintains its macroscopic integrity after deformation of the stent and does not undergo localized corrosion. The dense coating exerts a long-lasting decelerating impact on corrosion by establishing diffusion barriers and autoinhibition of the corrosion process[115]. Compared to the PLA-coated high purity magnesium (HPM), the PCL-coated HPM showed a higher Ecorr and lower Icorr[56]. The PCL coating could improve the cell adhesion and tissue growth around the magnesium alloy implant by decreasing its corrosion rate[114,116].
- Poly (trimethylene carbonate) (PTMC) coating
PTMC is commonly used as a soft material in the scaffold application for soft tissue regeneration and as a hydrophobic segment of amphiphilic block copolymers for drug delivery[117]. The degradation process of PTMC is slower than that of PLLA and other aliphatic polyesters. The study showed that the enzymatic degradation played a crucial role in the surface erosion[118]. Meanwhile, PTMC possesses elasticity and softness, so it can be used as a surface coating material for magnesium alloy stents.
It has been found that a uniform thin PTMC on magnesium alloys eroded from the surface to the interior when exposed to the biological environments[119]. As a result, it created a protective pathway that impeded the electrolyte diffusion from the blood to the magnesium alloy, thus minimizing substrate corrosion. PTMC hydrolysis is a nearly neutral ionic process and maintains a physiological pH during degradation. PTMC allows a minimal amount of electrolyte penetration through the coating to interact with the magnesium alloy substrate beneath. The remaining PTMC preserves the stability of this thin corrosion layer, regardless of whether the product layer is Mg(OH)2 or MgH2, to prevent further corrosion and dissolution (Figure 6). The addition of graphene oxide (GO) into PTMC coatings could improve the water barrier property of the composite coatings through the two dimension structure of GO, lengthen the penetration path of the solution through the labyrinth effect, and further inhibit the accumulation of hydrogen underneath the polymer layer to improve the corrosion resistance[120,121].
PTMC coated samples showed good cytocompatibility and hemocompatibility, with very few platelets adhering on the surface. Compared with PLGA, PTMC coatings have a more stable and sustained drug release capacity and can inhibit the proliferative of HUVSMCs for a long period of time, due to the much slower surface erosion behavior and degradation rate[122]. Atorvastatin calcium (ATVC) was loaded into the PTMC delivery coating on the magnesium alloy surface, which was able to promote rapid endothelialization of HUVECs and regulate growth of HUVSMCs, further preventing the endothelial hyperplasia and inflammatory responses[123]. However, PTMC lacks functional groups, which limits further functional modifications such as conjunction of bioactive components as well as immobilization on the metal surfaces. Chen et al.[124] developed amino-grafted PTMC polymers that were immobilized on the surface of magnesium alloys through the reaction of amino and carboxyl groups, and the immobilized polymeric coatings might be more resistant to detachment in the clinical delivery process including stent dilatation.
- Polyurethanes (PU) coating
The polyurethane is an elastic polymer, and the highly polar urea groups in the polyurethane urea provide enhanced hydrogen bonding in the hard segments, which act as strong physical crosslinkers. The high molecular weight, low crystallinity, and low glass transition temperature (Tg<-46℃) endow the solid polyurethane coatings with good elastomeric mechanical properties[125], making them a potentially biodegradable polymer coating for magnesium alloy stents. Gu et al.[126] investigated the dynamic degradation behavior, hemocompatibility and drug release of poly(carbonate urethane) urea (PCUU) and poly(ester urethane) urea (PEUU) coating on magnesium alloy stents. Compared with PEUU-coated, PLGA-coated and bare magnesium alloy stents, the PCUU-coated stents showed better corrosion resistance and reduced the thrombotic deposition. Compared to the PLGA coating, Arg-PEUU and Arg-Leu-PEUU have better bonding to magnesium alloys while exhibiting better corrosion resistance and biocompatibility[127,128]. The advantage of corrosion resistance could be attributed to the surface degradation nature of the amino acid based polyester urea urethane family[129], which resulted in a slow degradation rate in the simulated body fluid. Arg-PEUU and Arg-Leu-PEUU coatings reduced both platelet adhesion and hemolysis rate, had better cell adhesion to HUVEC, stimulated NO release from HUVEC, and had the ability to delay the thrombosis and restenosis.
- Silane coating
Silane coatings for magnesium alloys have been found to be valid, ecofriendly, and economical. Liu et al.[130] investigated a one-step reaction in which a cross-linked 3-amino-propyltrimethoxysilane (APTES) silane physical barrier layer was introduced onto the surface of a ZE21B alloy prior to electrostatic spraying of the rapamycin-eluting PLGA coating. Solid polysiloxane networks with exposed amine functional groups were formed by in situ APTES polycondensation, providing an effective physical barrier and strong bonding function. The APTES-treated magnesium alloy showed very favorable compatibility with HUVECs and HUVSMCs. Animal experiments confirmed that APTES-treated Mg-Zn-Y-Nd stents implanted into porcine coronary arteries for 6 months showed excellent tissue compatibility and re-endothelialization capacity without severe sign of injury, thrombosis, or restenosis of the vascular wall. After that, a simple two-step reaction was used to introduce anticorrosive silane pre-treatment on ZE21B alloy before coating with PLGA[131] (Figure 7). The first step was to immerse the NaOH-activated ZE21B alloy in bistriethoxysilylethane (BTSE) to form a cross-linked silane coating layer with enhanced corrosion resistance, and the second step was to treat the BTSE-modified ZE21B alloy with APTES to immobilize the amino functional groups so that to form hydrogen bonds with the outer PLGA coating. Compared to APTES pretreatment, the cross-linked bilayer BTSE-APTES pretreatment showed better corrosion protection and biocompatibility.
There have been a large number of researches on the polymer coating prepared on the magnesium alloy stents, which indicated that each polymer with its own characteristics was hard to meet the clinical requirements of magnesium alloy stent with surface protection separately. We should make full use of the performance advantages of various coatings to integrate magnesium alloy stents with excellent corrosion resistance. On this basis, new protective strategies should be sought to further improve the clinical safety and effectiveness of magnesium alloy stent.
5. Research trend and outlook of magnesium alloy stents
5.1. Research trend of magnesium alloy stents
Based on the corrosion mechanism of magnesium alloy stents, together with their deformation during usage and features of the service environment, further comprehensive exploration and study are necessary on magnesium alloy stents. This calls for adapting protective coatings to the deformation of the stents, preparing rapid endothelialization coatings to enhance the service environment of the stent, and constructing coatings with self-healing functions, with the aim of developing bioabsorbable magnesium alloy stents with controlled degradation (Figure 8).
5.1.1. Study of protective coatings adapted to the deformation mechanics of stents
Biodegradable magnesium alloy stents are currently delivered mainly through balloon-expandable catheter systems during implantations. However, the surface coating of the stent may crack or even peel off from the substrate due to the deformation after balloon expansion, indicating that the protective coating is not compatible with the deformation mechanics of the stent. The incompatibility of the surface coating with magnesium alloy stents may expedite the local corrosion of the stent platform. Consequently, the corrosion of the stent quickens, leading to the speedy loss of radial support. Thus, a protective coating aligns with the deformation mechanics of the stent is crucial.
In order to reduce the stress concentration distribution of the stent after deformation, the structure of the magnesium alloy stent should be optimized using the FEA method. Furthermore, it is essential to select a polymer with higher elasticity that is specifically tailored to the deformation of magnesium alloy stent when creating the protective coating. This can prevent damage to the coating caused by the deformation of the stent, which will reduce the corrosion rate of magnesium alloy stent. In addition, it is crucial to pay a close attention to the corrosion pattern of the polymer coating and the bonding strength between the substrate and the polymer coating. Shi et al.[132] coated magnesium alloy discs and stents with a relatively high plasticity polymer, poly(butyl acrylate) (PBA), through dip-coating method and ultrasonic spraying system, respectively. Compared with poly-D,L-lactic acid(PDLLA), the PBA polymer coating exhibited excellent mechanical properties without any noticeable damage during the expansion of the stent, indicating that this coating has the ability to withstand the deformation. The PBA coating maintained the structural integrity of magnesium alloy stent with slightly corrosion after 21 days of service. Whereafter, poly(butylene-co-adipate-terephthalate) (PBAT) was selected for reliable protection of HF-treatment magnesium alloys, due to its high elongation at break (>200%)[133]. The PBAT polymer coating is more suitable for the surface protection of magnesium alloy stents due to its excellent ability to hinder the electrolyte permeation and withstand the complex deformation. In the long term, PBAT-F coating showed significantly better protective property than the PDLLA coating, and the magnesium alloy stent with PBAT-F coating showed homogeneous corrosion as shown in Figure 9.
The quantitative study on the compatibility of protective coatings on the stents with deformation should be further carried out. The finite element simulation method has been used to optimize the structure of stent, which should be expansively used to establish a model of magnesium alloy stent with protective coating. Based on it, the effects of compression and expansion on the coating integrity and binding performance of the protective coating on the surface of the stent need to be studied. These can provide theoretical basis and data support for screening protective coating for magnesium alloy stents, which is an important research direction in the future.
5.1.2. Rapid endothelialization coating on magnesium alloy stents
Most traditional methods to decrease the corrosion rate of magnesium alloy stents have been concentrated on enhancing the corrosion resistance of the stent material or the protective property of the coating. However, less attention has been paid to the influence of the implantation surroundings on the degradation rate of magnesium alloy stents. A strategy is proposed like this: the more rapidly the stent is covered by the endothelium post-implantation, the lower the incidence of restenosis and thrombosis occur on the stent. Furthermore, the nascent endothelium quickly covers the magnesium alloy stents after implantation, shortening the cycles of flushing by blood. This also results in a change from the initial-stage blood corrosion to the tissue-fluid exchange corrosion, further reducing the corrosion rate of the magnesium alloy stents from the perspective of improving the in vivo service environment.
Conventional medications carried on the surface of stent, such as rapamycin, paclitaxel and sirolimus, are utilized to inhibit the in-stent restenosis. However, they have inhibitory effects on both endothelial cells and smooth muscle cells, which can lead to a delayed endothelialization and prolonged exposure time of the stent in the blood. Thus, to develop a functional coating with the properties of enhancing endothelial cell proliferation and suppressing smooth muscle cell proliferation is a crucial area for the future research of magnesium alloy stents.
PDA coatings can be used directly to control the behavior of cells on the stent surface and are able to solve the problems associated with re-endothelialization and restenosis of the stents. It can enhance the attachment and proliferation of human umbilical vein endothelial cells (HUVECs) [134,135]. In addition, the PDA coating has the ability to effectively inhibit the adhesion and proliferation of human umbilical vascular smooth muscle cells (HUVSMCs)[136]. Arg-Glu-Asp-Val (REDV) is a fibronectin-derived peptide, and when synthetic peptides containing this sequence are immobilized on otherwise cell non-adhesive substrates, endothelial cells adhere and spread, but fibroblasts, vascular smooth muscle cells and platelets do not[137]. Currently, studies related to the preparation of functionalized coatings on magnesium alloys containing REDV have been carried out[138,139,140]. However, the current studies are mainly focused on the in vitro study, and the animal experiments of magnesium alloy stents with functionalized REDV coatings should be the next research focus.
The copper (Cu)-bearing metals (including 316L stainless steel and cobalt-based alloy) developed by Ke Yang's team at the Institute of Metal Research, Chinese Academy of Sciences, exhibited excellent properties of promoting endothelialization, inhibiting smooth muscle cells proliferation and thrombosis as a novel platform material for the future vascular stents[141]. Inspired by this, the copper-containing coating was further investigated[142], and the preliminary results showed excellent biofunctional properties, the implanted magnesium alloy stent with copper-loaded coating was covered by endothelium within 7 days, indicating that the copper-loaded coated magnesium alloy has an application prospect. Based on the same strategy, Li et al. [143] developed a facile copper-incorporated coating system through nonaqueous phase synthesis of PDA to facilitate Cu2+ capture along with robust film deposited on easily corrodible magnesium, which subsequently enabled a sustained Cu2+ elution (Figure 10). The generated Cu2+ integrated Mg remarkably promoted HUVECs growth and endogenetic NO release, while simultaneously inhibited HUVSMCs. In vivo implantation studies further confirmed that the Cu2+ released magnesium alloy stent could improve stenting durability, promote rapid re-endothelialization, and alleviate neointimal hyperplasia, without obvious injure, inflammation, or thrombosis.
The potential biofunctional coatings with superb pro-endothelial effect should be further explored, which should be suitable for magnesium alloy stents to promote the biocompatibility and biosafety.
5.1.3. Introduction of self-healing mechanism into coating on magnesium alloy stents
The corrosion fracture of magnesium alloy stent is essentially attributed to the stress corrosion and fatigue corrosion of magnesium alloy. According to the characteristics of the use and service process of magnesium alloy stent, stress, deformation and damage of the stent are inevitable. If a material with self-healing property is introduced into the magnesium alloy or the coating, the damage formed during the service process of the stent can be repaired in real time, thus reducing the degradation rate of the magnesium alloy stent and prolongating the fracture cycle of the stent. It is a promising surface protection strategy for magnesium alloy stents. How to construct a self-healing coating on surface of magnesium alloy stents is another research direction in the future.
5.2. Outlook
Magnesium alloy stent is one of the three types of biodegradable metal stents developed at present, and it is the earliest biodegradable metal stent applied in clinic. Clinical results have shown long-term biosafety, but the physical support performance of the stent in the acute stage after surgery is not stable enough. It is necessary to further optimize the mechanical properties of the stent platform, the short-term protective effect of the protective coating, the rapid endothelialization function of the endothelialization promoting coating, and the self-healing function in the stent, so as to realize the effective support of magnesium alloy stents at the initial stage of implantation, and a gradual loss of support after 3-6 months of implantation, that is, controllable degradation.
References
- Cardiovascular Diseases. Available online: https://www.who.int/health-topics/cardiovascular-diseases (accessed on 31 July 2023).
- Qi, P.; Yang, Y.; Maitz, F.M.; Huang, N. Current Status of Research and Application in Vascular Stents. Chin. Sci. Bull. 2013, 58, 4362–4370. [Google Scholar] [CrossRef]
- Sigwart, U.; Puel, J.; Mirkovitch, V.; Joffre, F.; Kappenberger, L. Intravascular Stents to Prevent Occlusion and Re-Stenosis after Transluminal Angioplasty. N Engl J Med 1987, 316, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.; Dejaegere, P.; Kiemeneij, F.; Macaya, C.; Rutsch, W.; Heyndrickx, G.; Emanuelsson, H.; Marco, J.; Legrand, V.; Materne, P.; et al. A Comparison of Balloon-Expandable-Stent Implantation with Balloon Angioplasty in Patients with Coronary-Artery Disease. N. Engl. J. Med. 1994, 331, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Mintz, G.; Dussaillant, G.; Popma, J.; Pichard, A.; Satler, L.; Kent, K.; Griffin, J.; Leon, M. Patterns and Mechanisms of In-Stent Restenosis - A Serial Intravascular Ultrasound Study. CIRCULATION 1996, 94, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Claessen, B.E.; Henriques, J.P.S.; Jaffer, F.A.; Mehran, R.; Piek, J.J.; Dangas, G.D. Stent Thrombosis. JACC: Cardiovascular Interventions 2014, 7, 1081–1092. [Google Scholar] [CrossRef]
- Morice, M.-C.; Hayashi, E.B.; Guagliumi, G. A Randomized Comparison of a Sirolimus-Eluting Stent with a Standard Stent for Coronary Revascularization. The New England Journal of Medicine 2002. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.; Ellis, S.; Cannon, L.; Mann, J.; Greenberg, J.; Spriggs, D.; O’Shaughnessy, C.; DeMaio, S.; Hall, P.; Popma, J.; et al. Comparison of a Polymer-Based Paclitaxel-Eluting Stent with a Bare Metal Stent in Patients with Complex Coronary Artery Disease - A Randomized Controlled Trial. JAMA-JOURNAL OF THE AMERICAN MEDICAL ASSOCIATION 2005, 294, 1215–1223. [Google Scholar] [CrossRef]
- Joner, M.; Finn, A.V.; Farb, A.; Mont, E.K.; Kolodgie, F.D.; Ladich, E.; Kutys, R.; Skorija, K.; Gold, H.K.; Virmani, R. Pathology of Drug-Eluting Stents in Humans. Journal of the American College of Cardiology 2006, 48, 193–202. [Google Scholar] [CrossRef]
- Erne, P.; Schier, M.; Resink, T.J. The Road to Bioabsorbable Stents: Reaching Clinical Reality? Cardiovasc Intervent Radiol 2006, 29, 11–16. [Google Scholar] [CrossRef]
- Sotomi, Y.; Onuma, Y.; Collet, C.; Tenekecioglu, E.; Virmani, R.; Kleiman, N.S.; Serruys, P.W. Bioresorbable Scaffold: The Emerging Reality and Future Directions. Circ Res 2017, 120, 1341–1352. [Google Scholar] [CrossRef]
- Ormiston, J.A.; Serruys, P.W.; Regar, E.; Dudek, D.; Thuesen, L.; Webster, M.W.; Onuma, Y.; Garcia-Garcia, H.M.; McGreevy, R.; Veldhof, S. A Bioabsorbable Everolimus-Eluting Coronary Stent System for Patients with Single de-Novo Coronary Artery Lesions (ABSORB): A Prospective Open-Label Trial. The Lancet 2008, 371, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Yang, Y.; Han, Y.; Huo, Y.; Chen, J.; Yu, B.; Su, X.; Li, L.; Kuo, H.-C.; Ying, S.-W.; et al. Bioresorbable Vascular Scaffolds Versus Metallic Stents in Patients With Coronary Artery Disease. Journal of the American College of Cardiology 2015, 66, 2298–2309. [Google Scholar] [CrossRef] [PubMed]
- Bonan, R.; Asgar, A.W. Biodegradable Stents - Where Are We in 2009? US Cardiology 2009;6(1):81–4, 2009. [Google Scholar] [CrossRef]
- Ali, Z.A.; Serruys, P.W.; Kimura, T.; Gao, R.; Ellis, S.G.; Kereiakes, D.J.; Onuma, Y.; Simonton, C.; Zhang, Z.; Stone, G.W. 2-Year Outcomes with the Absorb Bioresorbable Scaffold for Treatment of Coronary Artery Disease: A Systematic Review and Meta-Analysis of Seven Randomised Trials with an Individual Patient Data Substudy. The Lancet 2017, 390, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Yamaji, K.; Ueki, Y.; Souteyrand, G.; Daemen, J.; Wiebe, J.; Nef, H.; Adriaenssens, T.; Loh, J.P.; Lattuca, B.; Wykrzykowska, J.J.; et al. Mechanisms of Very Late Bioresorbable Scaffold Thrombosis. Journal of the American College of Cardiology 2017, 70, 2330–2344. [Google Scholar] [CrossRef] [PubMed]
- No More Absorb BVS: Abbott Puts a Stop to Sales | Tctmd.Com. Available online: https://www.tctmd.com/news/no-more-absorb-bvs-abbott-puts-stop-sales (accessed on 9 October 2023).
- Liu, B.; Zheng, Y.F. Effects of Alloying Elements (Mn, Co, Al, W, Sn, B, C and S) on Biodegradability and in Vitro Biocompatibility of Pure Iron. Acta Biomaterialia 2011, 7, 1407–1420. [Google Scholar] [CrossRef] [PubMed]
- Moravej, M.; Mantovani, D. Biodegradable Metals for Cardiovascular Stent Application: Interests and New Opportunities. IJMS 2011, 12, 4250–4270. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Chang, R.; Liu, H.; Zhang, L.; Zheng, Y. Moving Research Direction in the Field of Metallic Bioresorbable Stents-A Mini-Review. Bioactive Materials 2023, 24, 20–25. [Google Scholar] [CrossRef]
- Tapiero, H.; Tew, K.D. Trace Elements in Human Physiology and Pathology: Zinc and Metallothioneins. Biomedicine & Pharmacotherapy 2003, 57, 399–411. [Google Scholar] [CrossRef]
- Bowen, P.K.; Drelich, J.; Goldman, J. Zinc Exhibits Ideal Physiological Corrosion Behavior for Bioabsorbable Stents. Advanced Materials 2013, 25, 2577–2582. [Google Scholar] [CrossRef]
- Schmidt, W.; Behrens, P.; Brandt-Wunderlich, C.; Siewert, S.; Grabow, N.; Schmitz, K.-P. In Vitro Performance Investigation of Bioresorbable Scaffolds – Standard Tests for Vascular Stents and Beyond. Cardiovascular Revascularization Medicine 2016, 17, 375–383. [Google Scholar] [CrossRef]
- Grogan, J.A.; O’Brien, B.J.; Leen, S.B.; McHugh, P.E. A Corrosion Model for Bioabsorbable Metallic Stents. Acta Biomaterialia 2011, 7, 3523–3533. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Dou, J.; Wang, Z.; Hu, C.; Yu, H.; Chen, C. Research Progress of Biodegradable Magnesium-Based Biomedical Materials: A Review. Journal of Alloys and Compounds 2022, 923, 166377. [Google Scholar] [CrossRef]
- Niu, J.; Huang, H.; Pei, J.; Jin, Z.; Guan, S.; Yuan, G.; Gy; Jn; Sg; Jn; et al. Research and Development Strategy for Biodegradable Magnesium-Based Vascular Stents: A Review. Biomater Transl 2021, 2, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Heublein, B. Biocorrosion of Magnesium Alloys: A New Principle in Cardiovascular Implant Technology? Heart 2003, 89, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Madanchi, M.; Avdijaj, D.; Attinger-Toller, A.; Cioffi, G.M.; Seiler, T.; Tersalvi, G.; Kobza, R.; Schüpfer, G.; Cuculi, F. Long-Term Outcomes After Implantation of Magnesium-Based Bioresorbable Scaffolds—Insights From an All-Comer Registry. Frontiers in Cardiovascular Medicine 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Onuma, Y.; Ormiston, J.; Abizaid, A.; Waksman, R.; Serruys, P. Bioresorbable Scaffolds: Rationale, Current Status, Challenges, and Future. European Heart Journal 2014, 35, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Haude, M.; Wlodarczak, A.; Van Der Schaaf, R.J.; Torzewski, J.; Ferdinande, B.; Escaned, J.; Iglesias, J.F.; Bennett, J.; Toth, G.; Joner, M.; et al. Safety and Performance of the Third-Generation Drug-Eluting Resorbable Coronary Magnesium Scaffold System in the Treatment of Subjects with de Novo Coronary Artery Lesions: 6-Month Results of the Prospective, Multicenter BIOMAG-I First-in-Human Study. eClinicalMedicine 2023, 59, 101940. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R.; Pakala, R.; Kuchulakanti, P.K.; Baffour, R.; Hellinga, D.; Seabron, R.; Tio, F.O.; Wittchow, E.; Hartwig, S.; Harder, C.; et al. Safety and Efficacy of Bioabsorbable Magnesium Alloy Stents in Porcine Coronary Arteries. Cathet. Cardiovasc. Intervent. 2006, 68, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Slottow, T.L.P.; Pakala, R.; Okabe, T.; Hellinga, D.; Lovec, R.J.; Tio, F.O.; Bui, A.B.; Waksman, R. Optical Coherence Tomography and Intravascular Ultrasound Imaging of Bioabsorbable Magnesium Stent Degradation in Porcine Coronary Arteries. Cardiovascular Revascularization Medicine 2008, 9, 248–254. [Google Scholar] [CrossRef]
- Di Mario, C.; Griffiths, H.; Goktekin, O.; Peeters, N.; Verbist, J.; Bosiers, M.; Deloose, K.; Heublein, B.; Rohde, R.; Kasese, V.; et al. Drug-Eluting Bioabsorbable Magnesium Stent. Journal of Interventional Cardiology 2004, 17, 391–395. [Google Scholar] [CrossRef]
- Peeters, P.; Bosiers, M.; Verbist, J.; Deloose, K.; Heublein, B. Preliminary Results After Application of Absorbable Metal Stents in Patients With Critical Limb Ischemia. Journal of Endovascular Therapy 2005, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Erbel, R.; Mario, C.D.; Bartunek, J.; Bonnier, J.; de Bruyne, B.; Eberli, F.R.; Erne, P.; Haude, M.; Heublein, B.; Horrigan, M.; et al. Temporary Scaffolding of Coronary Arteries with Bioabsorbable Magnesium Stents: A Prospective, Non-Randomised Multicentre Trial. 2007; 369. [Google Scholar]
- Waksman, R.; Erbel, R.; Di Mario, C.; Bartunek, J.; De Bruyne, B.; Eberli, F.R.; Erne, P.; Haude, M.; Horrigan, M.; Ilsley, C.; et al. Early- and Long-Term Intravascular Ultrasound and Angiographic Findings After Bioabsorbable Magnesium Stent Implantation in Human Coronary Arteries. JACC: Cardiovascular Interventions 2009, 2, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Wittchow, E.; Adden, N.; Riedmüller, J.; Savard, C.; Waksman, R.; Braune, M. Bioresorbable Drug-Eluting Magnesium-Alloy Scaffold: Design and Feasibility in a Porcine Coronary Model. EuroIntervention 2013, 8, 1441–1450. [Google Scholar] [CrossRef] [PubMed]
- Haude, M.; Erbel, R.; Erne, P.; Verheye, S.; Degen, H.; Böse, D.; Vermeersch, P.; Wijnbergen, I.; Weissman, N.; Prati, F.; et al. Safety and Performance of the Drug-Eluting Absorbable Metal Scaffold (DREAMS) in Patients with de-Novo Coronary Lesions: 12 Month Results of the Prospective, Multicentre, First-in-Man BIOSOLVE-I Trial. The Lancet 2013, 381, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R.; Zumstein, P.; Pritsch, M.; Wittchow, E.; Haude, M.; Lapointe-Corriveau, C.; Leclerc, G.; Joner, M. Second-Generation Magnesium Scaffold Magmaris: Device Design and Preclinical Evaluation in a Porcine Coronary Artery Model. EuroIntervention 2017, 13, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Joner, M.; Ruppelt, P.; Zumstein, P.; Lapointe-Corriveau, C.; Leclerc, G.; Bulin, A.; Castellanos, M.I.; Wittchow, E.; Haude, M.; Waksman, R. Preclinical Evaluation of Degradation Kinetics and Elemental Mapping of First- and Second-Generation Bioresorbable Magnesium Scaffolds. EuroIntervention 2018, 14, e1040–e1048. [Google Scholar] [CrossRef] [PubMed]
- Haude, M.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; von Birgelen, C.; Christiansen, E.H.; Wijns, W.; Neumann, F.-J.; Kaiser, C.; et al. Safety and Performance of the Second-Generation Drug-Eluting Absorbable Metal Scaffold in Patients with de-Novo Coronary Artery Lesions (BIOSOLVE-II): 6 Month Results of a Prospective, Multicentre, Non-Randomised, First-in-Man Trial. The Lancet 2016, 387, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Haude, M.; Ince, H.; Kische, S.; Abizaid, A.; Tölg, R.; Alves Lemos, P.; Van Mieghem, N.M.; Verheye, S.; von Birgelen, C.; Christiansen, E.H.; et al. Safety and Clinical Performance of a Drug Eluting Absorbable Metal Scaffold in the Treatment of Subjects with de Novo Lesions in Native Coronary Arteries: Pooled 12-month Outcomes of BIOSOLVE-II and BIOSOLVE-III. Catheter Cardiovasc Interv 2018, 92, E502–E511. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Włodarczak, A.; Łanocha, M.; Barycki, M.; Szudrowicz, M.; Kulczycki, J.J.; Jaroszewska-Pozorska, J.; Gosiewska, A.; Woźnica, K.; Lesiak, M.; et al. Outcomes of the Two Generations of Bioresorbable Scaffolds (Magmaris vs. Absorb) in Acute Coronary Syndrome in Routine Clinical Practice. Cardiology Journal 2022, 0. [Google Scholar] [CrossRef]
- Verheye, S.; Wlodarczak, A.; Montorsi, P.; Torzewski, J.; Bennett, J.; Haude, M.; Starmer, G.; Buck, T.; Wiemer, M.; Nuruddin, A.A.B.; et al. BIOSOLVE-IV-Registry: Safety and Performance of the Magmaris Scaffold: 12-Month Outcomes of the First Cohort of 1,075 Patients. Catheterization and Cardiovascular Interventions 2021, 98, E1–E8. [Google Scholar] [CrossRef]
- Cubero-Gallego, H.; Vandeloo, B.; Gomez-Lara, J.; Romaguera, R.; Roura, G.; Gomez-Hospital, J.A.; Cequier, A. Early Collapse of a Magnesium Bioresorbable Scaffold. JACC: Cardiovascular Interventions 2017, 10, e171–e172. [Google Scholar] [CrossRef] [PubMed]
- Barkholt, T.Ø.; Neghabat, O.; Terkelsen, C.J.; Christiansen, E.H.; Holm, N.R. Restenosis in a Collapsed Magnesium Bioresorbable Scaffold. Circ: Cardiovascular Interventions 2017, 10, e005677. [Google Scholar] [CrossRef] [PubMed]
- García-Blas, S.; Miñana, G.; Sanchis, J. Optical Coherence Tomography of Magnesium Bioresorbable Scaffold Restenosis. Revista Española de Cardiología (English Edition) 2018, 71, 1069. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.V.S.; Prasad, S.B.; Verma, K.; Mishra, R.K.; Kumar, V.; Singh, S. The Role and Significance of Magnesium in Modern Day Research-A Review. Journal of Magnesium and Alloys 2022, 10, 1–61. [Google Scholar] [CrossRef]
- Liu, M.; Zanna, S.; Ardelean, H.; Frateur, I.; Schmutz, P.; Song, G.; Atrens, A.; Marcus, P. A First Quantitative XPS Study of the Surface Films Formed, by Exposure to Water, on Mg and on the Mg–Al Intermetallics: Al3Mg2 and Mg17Al12. Corrosion Science 2009, 51, 1115–1127. [Google Scholar] [CrossRef]
- Lin, X.; Saijilafu; Wu, X.; Wu, K.; Chen, J.; Tan, L.; Witte, F.; Yang, H.; Mantovani, D.; Zhou, H.; et al. Biodegradable Mg-Based Alloys: Biological Implications and Restorative Opportunities. International Materials Reviews, 2022; 1–39. [Google Scholar] [CrossRef]
- Rapetto, C.; Leoncini, M. Magmaris: A New Generation Metallic Sirolimus-Eluting Fully Bioresorbable Scaffold: Present Status and Future Perspectives. Journal of Thoracic Disease 2017, 9. [Google Scholar] [CrossRef]
- Wu, W.; Chen, S.; Gastaldi, D.; Petrini, L.; Mantovani, D.; Yang, K.; Tan, L.; Migliavacca, F. Experimental Data Confirm Numerical Modeling of the Degradation Process of Magnesium Alloys Stents. Acta Biomaterialia 2013, 9, 8730–8739. [Google Scholar] [CrossRef]
- Tao, J.; Cheng, J.; Zhao, G.; Hu, X.; Gu, X.; Su, J. Computational Modeling of the Corrosion Process and Mechanical Performance of Biodegradable Stent. J. Phys.: Conf. Ser. 2021, 1888, 012019. [Google Scholar] [CrossRef]
- Wu, W.; Petrini, L.; Gastaldi, D.; Villa, T.; Vedani, M.; Lesma, E.; Previtali, B.; Migliavacca, F. Finite Element Shape Optimization for Biodegradable Magnesium Alloy Stents. Ann Biomed Eng 2010, 38, 2829–2840. [Google Scholar] [CrossRef]
- Xu, W.; Sato, K.; Koga, Y.; Sasaki, M.; Niidome, T. Corrosion Resistance of HF-Treated Mg Alloy Stent Following Balloon Expansion and Its Improvement through Biodegradable Polymer Coating. J Coat Technol Res 2020, 17, 1023–1032. [Google Scholar] [CrossRef]
- Chen, Y.; Song, Y.; Zhang, S.; Li, J.; Zhao, C.; Zhang, X. Interaction between a High Purity Magnesium Surface and PCL and PLA Coatings during Dynamic Degradation. Biomed. Mater. 2011, 6, 025005. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.N.; Zhou, W.R.; Zheng, Y.F.; Cheng, Y.; Wei, S.C.; Zhong, S.P.; Xi, T.F.; Chen, L.J. Corrosion Fatigue Behaviors of Two Biomedical Mg Alloys – AZ91D and WE43 – In Simulated Body Fluid. Acta Biomaterialia 2010, 6, 4605–4613. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhang, B.; Zhang, B.; Lin, H.; Yang, H.; Zheng, F.; Chen, M. Assessment of Structure Integrity, Corrosion Behavior and Microstructure Change of AZ31B Stent in Porcine Coronary Arteries. Journal of Materials Science & Technology 2019, 39. [Google Scholar] [CrossRef]
- Shen, Z.; Zhao, M.; Zhou, X.; Yang, H.; Liu, J.; Guo, H.; Zheng, Y.; Yang, J.-A. A Numerical Corrosion-Fatigue Model for Biodegradable Mg Alloy Stents. Acta Biomaterialia 2019, 97, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Guangling Song. Corrosion Protection of magnesium alloys; Chemical Industry Press: Beijing, CHN, 2006. [Google Scholar]
- Wang, J.; Wang, L.; Guan, S.; Zhu, S.; Ren, C.; Hou, S. Microstructure and Corrosion Properties of as Sub-Rapid Solidification Mg–Zn–Y–Nd Alloy in Dynamic Simulated Body Fluid for Vascular Stent Application. J Mater Sci: Mater Med 2010, 21, 2001–2008. [Google Scholar] [CrossRef]
- Zhang, X.; Yuan, G.; Mao, L.; Niu, J.; Ding, W. Biocorrosion Properties of As-Extruded Mg–Nd–Zn–Zr Alloy Compared with Commercial AZ31 and WE43 Alloys. Materials Letters 2012, 66, 209–211. [Google Scholar] [CrossRef]
- Leeflang, M.A.; Dzwonczyk, J.S.; Zhou, J.; Duszczyk, J. Long-Term Biodegradation and Associated Hydrogen Evolution of Duplex-Structured Mg–Li–Al–(RE) Alloys and Their Mechanical Properties. Materials Science and Engineering: B 2011, 176, 1741–1745. [Google Scholar] [CrossRef]
- Witte, F.; Kaese, V.; Haferkamp, H.; Switzer, E.; Meyer-Lindenberg, A.; Wirth, C.J.; Windhagen, H. In Vivo Corrosion of Four Magnesium Alloys and the Associated Bone Response. Biomaterials 2005, 26, 3557–3563. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Zhu, S.; Wang, L.; Liu, Q.; Yue, G.; Wang, J.; Guan, S. The Microstructure and Properties of Cyclic Extrusion Compression Treated Mg–Zn–Y–Nd Alloy for Vascular Stent Application. Journal of the Mechanical Behavior of Biomedical Materials 2012, 8, 1–7. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, Y.; Yang, Z.; Zhu, S.; Wang, L.; Guan, S. Processing and Properties of Magnesium Alloy Micro-Tubes for Biodegradable Vascular Stents. Materials Science and Engineering: C 2018, 90, 504–513. [Google Scholar] [CrossRef]
- Du, P.; Mei, D.; Furushima, T.; Zhu, S.; Wang, L.; Zhou, Y.; Guan, S. In Vitro Corrosion Properties of HTHEed Mg-Zn-Y-Nd Alloy Microtubes for Stent Applications: Influence of Second Phase Particles and Crystal Orientation. Journal of Magnesium and Alloys 2022, 10, 1286–1295. [Google Scholar] [CrossRef]
- Ye, X.; Chen, M.; Yang, M.; Wei, J.; Liu, D. In Vitro Corrosion Resistance and Cytocompatibility of Nano-Hydroxyapatite Reinforced Mg–Zn–Zr Composites. J Mater Sci: Mater Med 2010, 21, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Zong, Y.; Yuan, G.; Zhang, X.; Mao, L.; Niu, J.; Ding, W. Comparison of Biodegradable Behaviors of AZ31 and Mg–Nd–Zn–Zr Alloys in Hank’s Physiological Solution. Materials Science and Engineering: B 2012, 177, 395–401. [Google Scholar] [CrossRef]
- Zhang, J.; Li, H.; Wang, W.; Huang, H.; Pei, J.; Qu, H.; Yuan, G.; Li, Y. The Degradation and Transport Mechanism of a Mg-Nd-Zn-Zr Stent in Rabbit Common Carotid Artery: A 20-Month Study. Acta Biomaterialia 2018, 69, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Bian, D.; Zhou, X.; Liu, J.; Li, W.; Shen, D.; Zheng, Y.; Gu, W.; Jiang, J.; Li, M.; Chu, X.; et al. Degradation Behaviors and In-Vivo Biocompatibility of a Rare Earth- and Aluminum-Free Magnesium-Based Stent. Acta Biomaterialia 2021, 124, 382–397. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, Y.; Bian, D.; Gao, S.; Leeflang, S.; Guo, H.; Zheng, Y.; Zhou, J. Study on the Mg-Li-Zn Ternary Alloy System with Improved Mechanical Properties, Good Degradation Performance and Different Responses to Cells. Acta Biomaterialia 2017, 62, 418–433. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhao, D.; Lee, B.; Roy, A.; Yao, R.; Chen, S.; Dong, Z.; Heineman, W.R.; Kumta, P.N. Effect of Lithium and Aluminum on the Mechanical Properties, In Vivo and In Vitro Degradation, and Toxicity of Multiphase Ultrahigh Ductility Mg–Li–Al–Zn Quaternary Alloys for Vascular Stent Application. ACS Biomater. Sci. Eng. 2020, 6, 1950–1964. [Google Scholar] [CrossRef] [PubMed]
- Pang, T.Y.; Kwok, J.S.; Nguyen, C.T.; Fox, K. Evaluating Magnesium Alloy WE43 for Bioresorbable Coronary Stent Applications. MRS Advances 2021, 6, 54–60. [Google Scholar] [CrossRef]
- Wu, W.; Gastaldi, D.; Yang, K.; Tan, L.; Petrini, L.; Migliavacca, F. Finite Element Analyses for Design Evaluation of Biodegradable Magnesium Alloy Stents in Arterial Vessels. Materials Science and Engineering: B 2011, 176, 1733–1740. [Google Scholar] [CrossRef]
- Echeverry-Rendon, M.; Duque, V.; Quintero, D.; Harmsen, M.C.; Echeverria, F. Novel Coatings Obtained by Plasma Electrolytic Oxidation to Improve the Corrosion Resistance of Magnesium-Based Biodegradable Implants. Surface and Coatings Technology 2018, 354, 28–37. [Google Scholar] [CrossRef]
- Lu, P.; Cao, L.; Liu, Y.; Xu, X.; Wu, X. Evaluation of Magnesium Ions Release, Biocorrosion, and Hemocompatibility of MAO/PLLA-Modified Magnesium Alloy WE42. J. Biomed. Mater. Res. 2011, 96B, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Tian, P.; Liu, X.; Zhou, B. In Vitro Degradation, Hemolysis, and Cytocompatibility of PEO/PLLA Composite Coating on Biodegradable AZ31 Alloy: PEO/PLLA Composite Coating on Biodegradable AZ31 Alloy. J. Biomed. Mater. Res. 2015, 103, 342–354. [Google Scholar] [CrossRef] [PubMed]
- Rahim, M.I.; Tavares, A.; Evertz, F.; Kieke, M.; Seitz, J.-M.; Eifler, R.; Weizbauer, A.; Willbold, E.; Jürgen Maier, H.; Glasmacher, B.; et al. Phosphate Conversion Coating Reduces the Degradation Rate and Suppresses Side Effects of Metallic Magnesium Implants in an Animal Model. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2017, 105, 1622–1635. [Google Scholar] [CrossRef] [PubMed]
- Van PHUONG, N.; Gupta, M.; Moon, S. Enhanced Corrosion Performance of Magnesium Phosphate Conversion Coating on AZ31 Magnesium Alloy. Transactions of Nonferrous Metals Society of China 2017, 27, 1087–1095. [Google Scholar] [CrossRef]
- Li, G.Y.; Lian, J.S.; Niu, L.Y.; Jiang, Z.H.; Jiang, Q. Growth of Zinc Phosphate Coatings on AZ91D Magnesium Alloy. Surface and Coatings Technology 2006, 201, 1814–1820. [Google Scholar] [CrossRef]
- Niu, L.Y.; Jiang, Z.H.; Li, G.Y.; Gu, C.D.; Lian, J.S. A Study and Application of Zinc Phosphate Coating on AZ91D Magnesium Alloy. Surface and Coatings Technology 2006, 200, 3021–3026. [Google Scholar] [CrossRef]
- Su, Y.; Su, Y.; Lu, Y.; Lian, J.; Li, G. Composite Microstructure and Formation Mechanism of Calcium Phosphate Conversion Coating on Magnesium Alloy. J. Electrochem. Soc. 2016, 163, G138–G143. [Google Scholar] [CrossRef]
- Su, Y.; Guo, Y.; Huang, Z.; Zhang, Z.; Li, G.; Lian, J.; Ren, L. Preparation and Corrosion Behaviors of Calcium Phosphate Conversion Coating on Magnesium Alloy. Surface and Coatings Technology 2016, 307, 99–108. [Google Scholar] [CrossRef]
- Zai, W.; Zhang, X.; Su, Y.; Man, H.C.; Li, G.; Lian, J. Comparison of Corrosion Resistance and Biocompatibility of Magnesium Phosphate (MgP), Zinc Phosphate (ZnP) and Calcium Phosphate (CaP) Conversion Coatings on Mg Alloy. Surface and Coatings Technology 2020, 397, 125919. [Google Scholar] [CrossRef]
- Mao, L.; Zhu, H.; Chen, L.; Zhou, H.; Yuan, G.; Song, C. Enhancement of Corrosion Resistance and Biocompatibility of Mg-Nd-Zn-Zr Alloy Achieved with Phosphate Coating for Vascular Stent Application. Journal of Materials Research and Technology 2020, 9, 6409–6419. [Google Scholar] [CrossRef]
- Zai, W.; Su, Y.; Man, H.C.; Lian, J.; Li, G. Effect of pH Value and Preparation Temperature on the Formation of Magnesium Phosphate Conversion Coatings on AZ31 Magnesium Alloy. Applied Surface Science 2019, 492, 314–327. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, G.; Zhang, Y.-H.; Zhao, Q. Growth and Characterization of Mg(OH)2 Film on Magnesium Alloy AZ31. Applied Surface Science 2011, 257, 6129–6137. [Google Scholar] [CrossRef]
- Peng, F.; Li, H.; Wang, D.; Tian, P.; Tian, Y.; Yuan, G.; Xu, D.; Liu, X. Enhanced Corrosion Resistance and Biocompatibility of Magnesium Alloy by Mg–Al-Layered Double Hydroxide. ACS Appl. Mater. Interfaces 2016, 8, 35033–35044. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, N.; Panomsuwan, G.; Yamamoto, E.; Sudare, T.; Saito, N.; Ishizaki, T. Effect of Treatment Time in the Mg(OH)2/Mg–Al LDH Composite Film Formed on Mg Alloy AZ31 by Steam Coating on the Corrosion Resistance. Surface and Coatings Technology 2016, 286, 172–177. [Google Scholar] [CrossRef]
- Lin, J.; Hsia, C.; Uan, J. Characterization of Mg,Al-Hydrotalcite Conversion Film on Mg Alloy and Cl− and CO32- Anion-Exchangeability of the Film in a Corrosive Environment. Scripta Materialia 2007, 56, 927–930. [Google Scholar] [CrossRef]
- Li, H.; Peng, F.; Wang, D.; Qiao, Y.; Xu, D.; Liu, X. Layered Double Hydroxide/Poly-Dopamine Composite Coating with Surface Heparinization on Mg Alloys: Improved Anticorrosion, Endothelialization and Hemocompatibility. Biomater. Sci. 2018, 6, 1846–1858. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Tan, J.; Du, H.; Qian, S.; Liu, X. Comparison Study of Mg(OH)2, Mg-Fe LDH, and FeOOH Coatings on PEO-Treated Mg Alloy in Anticorrosion and Biocompatibility. Applied Clay Science 2022, 225, 106535. [Google Scholar] [CrossRef]
- Mao, L.; Yuan, G.; Niu, J.; Zong, Y.; Ding, W. In Vitro Degradation Behavior and Biocompatibility of Mg–Nd–Zn–Zr Alloy by Hydrofluoric Acid Treatment. Materials Science and Engineering: C 2013, 33, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Shen, L.; Chen, J.; Wu, Y.; Kwak, M.; Lu, Y.; Xue, Q.; Pei, J.; Zhang, L.; Yuan, G.; et al. Enhanced Bioactivity of Mg–Nd–Zn–Zr Alloy Achieved with Nanoscale MgF 2 Surface for Vascular Stent Application. ACS Appl. Mater. Interfaces 2015, 7, 5320–5330. [Google Scholar] [CrossRef]
- Li, Q.; Zhu, P.; Chen, S.; Zhang, B.; Yang, K. In Vitro Study on Degradation of AZ31B Magnesium Alloy with Fluoride Conversion Coating. Materials Technology 2017, 32, 409–414. [Google Scholar] [CrossRef]
- Ostrowski, N.J.; Lee, B.; Roy, A.; Ramanathan, M.; Kumta, P.N. Biodegradable Poly(Lactide-Co-Glycolide) Coatings on Magnesium Alloys for Orthopedic Applications. J Mater Sci: Mater Med 2013, 24, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Li, L.-Y.; Cui, L.-Y.; Zeng, R.-C.; Li, S.-Q.; Chen, X.-B.; Zheng, Y.; Kannan, M.B. Advances in Functionalized Polymer Coatings on Biodegradable Magnesium Alloys – A Review. Acta Biomaterialia 2018, 79, 23–36. [Google Scholar] [CrossRef]
- Farah, S.; Anderson, D.G.; Langer, R. Physical and Mechanical Properties of PLA, and Their Functions in Widespread Applications — A Comprehensive Review. Advanced Drug Delivery Reviews 2016, 107, 367–392. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhang, X.; Niu, J.; Shi, Y.; Zhu, Z.; Dai, D.; Chen, C.; Pei, J.; Yuan, G.; Zhang, R. Biosafety and Efficacy Evaluation of a Biodegradable Magnesium-Based Drug-Eluting Stent in Porcine Coronary Artery. Sci Rep 2021, 11, 7330. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Chen, Y.; Fan, H.; Chen, S.; Wang, H.; Song, X. A Novel PLLA/MgF2 Coating on Mg Alloy by Ultrasonic Atomization Spraying for Controlling Degradation and Improving Biocompatibility. Materials 2023, 16, 682. [Google Scholar] [CrossRef]
- Menze, R.; Wittchow, E. In Vitro and in Vivo Evaluation of a Novel Bioresorbable Magnesium Scaffold with Different Surface Modifications. J Biomed Mater Res B Appl Biomater 2021, 109, 1292–1302. [Google Scholar] [CrossRef]
- Chen, S.; Wan, P.; Zhang, B.; Eren Erişen, D.; Yang, H.; Yang, K. A Novel Polymer Critical Re-Melting Treatment for Improving Corrosion Resistance of Magnesium Alloy Stent. Journal of Materials Science & Technology 2019, 35, 19–22. [Google Scholar] [CrossRef]
- Shi, Y.; Pei, J.; Zhang, J.; Niu, J.; Zhang, H.; Guo, S.; Li, Z.; Yuan, G. Enhanced Corrosion Resistance and Cytocompatibility of Biodegradable Mg Alloys by Introduction of Mg(OH)2 Particles into Poly (L-Lactic Acid) Coating. Sci Rep 2017, 7, 41796. [Google Scholar] [CrossRef]
- Park, S.; Lee, H.; Kim, H.-E.; Jung, H.-D.; Jang, T.-S. Bifunctional Poly (l-Lactic Acid)/Hydrophobic Silica Nanocomposite Layer Coated on Magnesium Stents for Enhancing Corrosion Resistance and Endothelial Cell Responses. Materials Science and Engineering: C 2021, 127, 112239. [Google Scholar] [CrossRef]
- Xu, W.; Yagoshi, K.; Koga, Y.; Sasaki, M.; Niidome, T. Optimized Polymer Coating for Magnesium Alloy-Based Bioresorbable Scaffolds for Long-Lasting Drug Release and Corrosion Resistance. Colloids and Surfaces B: Biointerfaces 2018, 163, 100–106. [Google Scholar] [CrossRef]
- Li, J.N.; Cao, P.; Zhang, X.N.; Zhang, S.X.; He, Y.H. In Vitro Degradation and Cell Attachment of a PLGA Coated Biodegradable Mg–6Zn Based Alloy. J Mater Sci 2010, 45, 6038–6045. [Google Scholar] [CrossRef]
- Danhier, F.; Ansorena, E.; Silva, J.M.; Coco, R.; Le Breton, A.; Préat, V. PLGA-Based Nanoparticles: An Overview of Biomedical Applications. Journal of Controlled Release 2012, 161, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Burkersroda, F. von; Schedl, L.; Göpferich, A. Why Degradable Polymers Undergo Surface Erosion or Bulk Erosion. Biomaterials 2002, 23, 4221–4231. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.-H.; Cheon, K.-H.; Jo, K.-I.; Ahn, J.-H.; Kim, H.-E.; Jung, H.-D.; Jang, T.-S. An Asymmetric Surface Coating Strategy for Improved Corrosion Resistance and Vascular Compatibility of Magnesium Alloy Stents. Materials & Design 2020, 196, 109182. [Google Scholar] [CrossRef]
- Labet, M.; Thielemans, W. Synthesis of Polycaprolactone: A Review. Chem. Soc. Rev. 2009, 38, 3484. [Google Scholar] [CrossRef] [PubMed]
- Dash, T.K.; Konkimalla, V.B. Polymeric Modification and Its Implication in Drug Delivery: Poly-ε-Caprolactone (PCL) as a Model Polymer. Mol. Pharmaceutics 2012, 9, 2365–2379. [Google Scholar] [CrossRef] [PubMed]
- Yazdimamaghani, M.; Razavi, M.; Vashaee, D.; Tayebi, L. Surface Modification of Biodegradable Porous Mg Bone Scaffold Using Polycaprolactone/Bioactive Glass Composite. Materials Science and Engineering: C 2015, 49, 436–444. [Google Scholar] [CrossRef]
- Wong, H.M.; Yeung, K.W.K.; Lam, K.O.; Tam, V.; Chu, P.K.; Luk, K.D.K.; Cheung, K.M.C. A Biodegradable Polymer-Based Coating to Control the Performance of Magnesium Alloy Orthopaedic Implants. Biomaterials 2010, 31, 2084–2096. [Google Scholar] [CrossRef] [PubMed]
- Knigge, S.; Mueller, M.; Fricke, L.; Schilling, T.; Glasmacher, B. In Vitro Investigation of Corrosion Control of Magnesium with Degradable Polycaprolactone Coatings for Cardiovascular Grafts. Coatings 2023, 13, 94. [Google Scholar] [CrossRef]
- Xu, L.; Yamamoto, A. Characteristics and Cytocompatibility of Biodegradable Polymer Film on Magnesium by Spin Coating. Colloids and Surfaces B: Biointerfaces 2012, 93, 67–74. [Google Scholar] [CrossRef]
- Fukushima, K. Poly(Trimethylene Carbonate)-Based Polymers Engineered for Biodegradable Functional Biomaterials. Biomater. Sci. 2016, 4, 9–24. [Google Scholar] [CrossRef]
- Zhang, Z.; Kuijer, R.; Bulstra, S.K.; Grijpma, D.W.; Feijen, J. The in Vivo and in Vitro Degradation Behavior of Poly(Trimethylene Carbonate). Biomaterials 2006, 27, 1741–1748. [Google Scholar] [CrossRef]
- Wang, J.; He, Y.; Maitz, M.F.; Collins, B.; Xiong, K.; Guo, L.; Yun, Y.; Wan, G.; Huang, N. A Surface-Eroding Poly(1,3-Trimethylene Carbonate) Coating for Fully Biodegradable Magnesium-Based Stent Applications: Toward Better Biofunction, Biodegradation and Biocompatibility. Acta Biomaterialia 2013, 9, 8678–8689. [Google Scholar] [CrossRef]
- Zhao, Z.; Zong, L.; Liu, C.; Wang, C.; Qi, C.; Wang, N.; Chen, H.; Wang, J.; Jian, X. Dual Strengthened Corrosion Control of Biodegradable Coating on Magnesium Alloy for Vascular Stent Application. Progress in Organic Coatings 2023, 174, 107297. [Google Scholar] [CrossRef]
- Zhao, Z.; Zong, L.; Liu, C.; Ding, W.; Zhu, L.; Qi, C.; Wang, C.; Shao, S.; Wang, J.; Jian, X. Strengthened Corrosion Control of Biodegradable Poly(Trimethylene Carbonate) Coating on Bioabsorbable Mg Alloy by Introducing Graphene Oxide. Surface and Coatings Technology 2022, 451, 129052. [Google Scholar] [CrossRef]
- Tang, H.; Li, S.; Zhao, Y.; Liu, C.; Gu, X.; Fan, Y. A Surface-Eroding Poly(1,3-Trimethylene Carbonate) Coating for Magnesium Based Cardiovascular Stents with Stable Drug Release and Improved Corrosion Resistance. Bioactive Materials 2022, 7, 144–153. [Google Scholar] [CrossRef]
- Ye, C.; Wang, J.; Zhao, A.; He, D.; Maitz, M.F.; Zhou, N.; Huang, N. Atorvastatin Eluting Coating for Magnesium-Based Stents: Control of Degradation and Endothelialization in a Microfluidic Assay and In Vivo. Adv. Mater. Technol. 2020, 5, 1900947. [Google Scholar] [CrossRef]
- Chen, Y.; Ye, S.; Zhu, Y.; Gu, X.; Higuchi, S.; Wan, G.; Wagner, W.R. Covalently-Attached, Surface-Eroding Polymer Coatings on Magnesium Alloys for Corrosion Control and Temporally Varying Support of Cell Adhesion. Adv. Mater. Interfaces 2020, 7, 2000356. [Google Scholar] [CrossRef]
- Hong, Y.; Guan, J.; Fujimoto, K.L.; Hashizume, R.; Pelinescu, A.L.; Wagner, W.R. Tailoring the Degradation Kinetics of Poly(Ester Carbonate Urethane)Urea Thermoplastic Elastomers for Tissue Engineering Scaffolds. Biomaterials 2010, 31, 4249–4258. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Mao, Z.; Ye, S.-H.; Koo, Y.; Yun, Y.; Tiasha, T.R.; Shanov, V.; Wagner, W.R. Biodegradable, Elastomeric Coatings with Controlled Anti-Proliferative Agent Release for Magnesium-Based Cardiovascular Stents. Colloids and Surfaces B: Biointerfaces 2016, 144, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, P.; Chu, C.-C.; Xi, T. A Novel Biodegradable and Biologically Functional Arginine-Based Poly(Ester Urea Urethane) Coating for Mg–Zn–Y–Nd Alloy: Enhancement in Corrosion Resistance and Biocompatibility. J. Mater. Chem. B 2017, 5, 1787–1802. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, P.; Chu, C.-C.; Xi, T. Arginine-Leucine Based Poly (Ester Urea Urethane) Coating for Mg-Zn-Y-Nd Alloy in Cardiovascular Stent Applications. Colloids and Surfaces B: Biointerfaces 2017, 159, 78–88. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Chu, C.-C. A New Family of Functional Biodegradable Arginine-Based Polyester Urea Urethanes: Synthesis, Chracterization and Biodegradation. Polymer 2013, 54, 4112–4125. [Google Scholar] [CrossRef]
- Liu, J.; Zheng, B.; Wang, P.; Wang, X.; Zhang, B.; Shi, Q.; Xi, T.; Chen, M.; Guan, S. Enhanced in Vitro and in Vivo Performance of Mg–Zn–Y–Nd Alloy Achieved with APTES Pretreatment for Drug-Eluting Vascular Stent Application. ACS Appl. Mater. Interfaces 2016, 8, 17842–17858. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xi, T. Enhanced Anti-Corrosion Ability and Biocompatibility of PLGA Coatings on MgZnYNd Alloy by BTSE-APTES Pre-Treatment for Cardiovascular Stent. Journal of Materials Science & Technology 2016, 32, 845–857. [Google Scholar] [CrossRef]
- Shi, L.; Chen, S.; Zheng, F.; Liu, M.; Yang, H.; Zhang, B. Corrosion Resistance Evaluation of Biodegradable Magnesium Alloy Vascular Stents Optimized by Mechanical Adapted Polymer Coating Strategy. Colloids and Surfaces A: Physicochemical and Engineering Aspects 2023, 658, 130664. [Google Scholar] [CrossRef]
- Shi, L.; Chen, s. s; Shahzad, M.B.; Wei, Z.; Leng, B. Enhanced Corrosion Resistance and Biocompatibility of an Elastic Poly (Butyleneadipate-Co-Terephthalate) Composite Coating for AZ31 Magnesium Alloy Vascular Stents. Progress in Organic Coatings 2022, 172, 107138. [Google Scholar] [CrossRef]
- Ku, S.H.; Park, C.B. Human Endothelial Cell Growth on Mussel-Inspired Nanofiber Scaffold for Vascular Tissue Engineering. Biomaterials 2010, 31, 9431–9437. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-L.; Ren, K.-F.; Chang, H.; Jia, F.; Li, B.-C.; Ji, Y.; Ji, J. Direct Adhesion of Endothelial Cells to Bioinspired Poly(Dopamine) Coating Through Endogenous Fibronectin and Integrin A5β1. Macromolecular Bioscience 2013, 13, 483–493. [Google Scholar] [CrossRef]
- Yang, Z.; Tu, Q.; Zhu, Y.; Luo, R.; Li, X.; Xie, Y.; Maitz, M.F.; Wang, J.; Huang, N. Mussel-Inspired Coating of Polydopamine Directs Endothelial and Smooth Muscle Cell Fate for Re-Endothelialization of Vascular Devices. Advanced Healthcare Materials 2012, 1, 548–559. [Google Scholar] [CrossRef]
- Hubbell, J.A.; Massia, S.P.; Desai, N.P.; Drumheller, P.D. Endothelial Cell-Selective Materials for Tissue Engineering in the Vascular Graft Via a New Receptor. Nat Biotechnol 1991, 9, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, J.; Wang, S.; Zhu, S.; Zhu, C.; Zheng, B.; Yang, G.; Guan, S. Surface Modification of the Biodegradable Cardiovascular Stent Material Mg–Zn–Y–Nd Alloy via Conjugating REDV Peptide for Better Endothelialization. J. Mater. Res. 2018, 33, 4123–4133. [Google Scholar] [CrossRef]
- Bai, L.; Wang, Y.; Chen, L.; Wang, J.; Li, J.; Zhu, S.; Wang, L.; Guan, S. Preparation of Functional Coating on Magnesium Alloy with Hydrophilic Polymers and Bioactive Peptides for Improved Corrosion Resistance and Biocompatibility. Journal of Magnesium and Alloys 2022, 10, 1957–1971. [Google Scholar] [CrossRef]
- Zhang, Z.-Q.; Tong, P.-D.; Wang, L.; Qiu, Z.-H.; Li, J.-A.; Li, H.; Guan, S.-K.; Lin, C.-G.; Wang, H.-Y. One-Step Fabrication of Self-Healing Poly(Thioctic Acid) Coatings on ZE21B Mg Alloys for Enhancing Corrosion Resistance, Anti-Bacterial/Oxidation, Hemocompatibility and Promoting Re-Endothelialization. Chemical Engineering Journal 2023, 451, 139096. [Google Scholar] [CrossRef]
- Jin, S.; Qi, X.; Wang, T.; Ren, L.; Yang, K.; Zhong, H. In Vitro Study of Stimulation Effect on Endothelialization by a Copper Bearing Cobalt Alloy. Journal of Biomedical Materials Research Part A 2018, 106, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Ma, J.; Kang, S.; Chen, S. Copper-Loaded Chitosan Coating for Improved in-Vitro Corrosion Resistance and Endothelialization of Magnesium Alloy Stents. Materials Chemistry and Physics 2023, 305, 127931. [Google Scholar] [CrossRef]
- Li, L.-Y.; Yang, Z.; Pan, X.-X.; Feng, B.-X.; Yue, R.; Yu, B.; Zheng, Y.-F.; Tan, J.-Y.; Yuan, G.-Y.; Pei, J. Incorporating Copper to Biodegradable Magnesium Alloy Vascular Stents via a Cu(II)-Eluting Coating for Synergistic Enhancement in Prolonged Durability and Rapid Re-Endothelialization. Advanced Functional Materials 2022, 32, 2205634. [Google Scholar] [CrossRef]
Figure 1.
Timeline of progress in the development of stents.
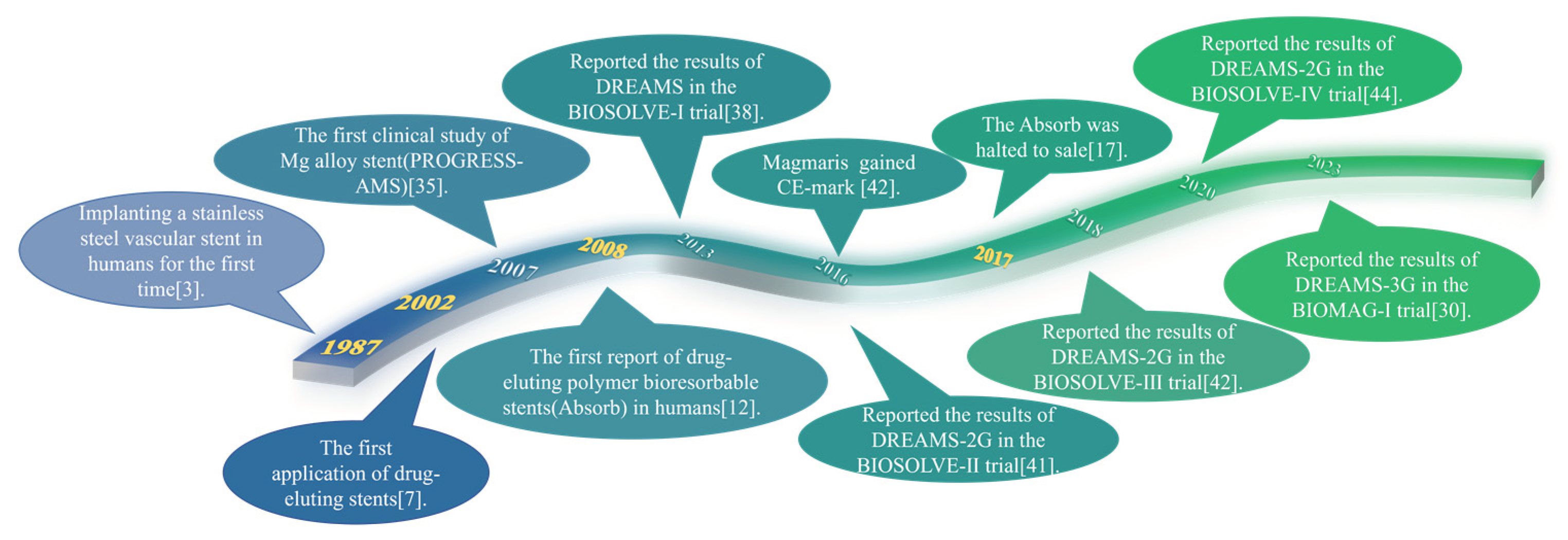
Figure 2.
The characteristics of biodegradable magnesium alloy stents made by Biotronik.
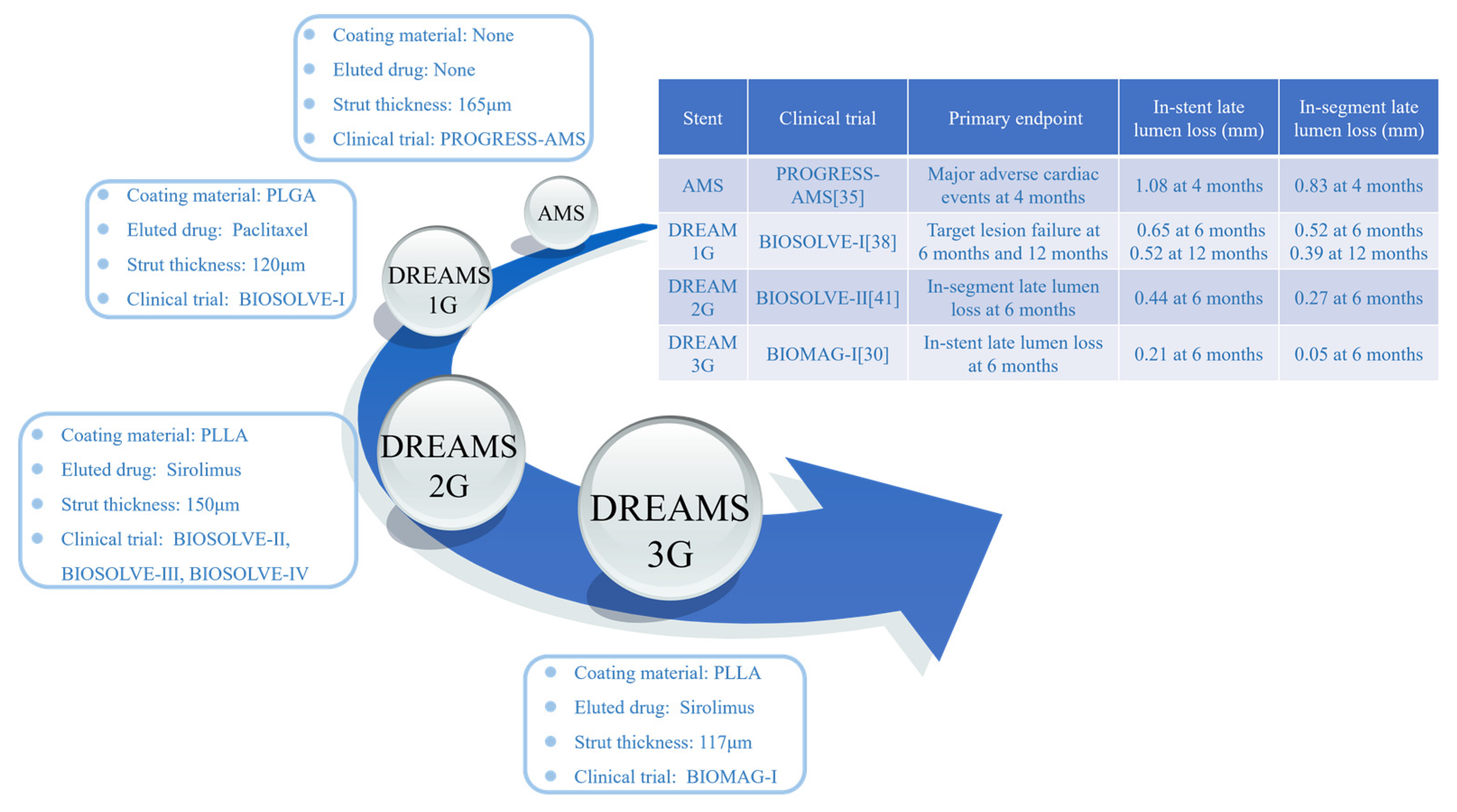
Figure 3.
Hallmark OCT findings encountered in patients with the Magmaris-related target lesion failures: (a) stent collapse; (b) uncontrolled device dismantling[28].
Figure 3.
Hallmark OCT findings encountered in patients with the Magmaris-related target lesion failures: (a) stent collapse; (b) uncontrolled device dismantling[28].
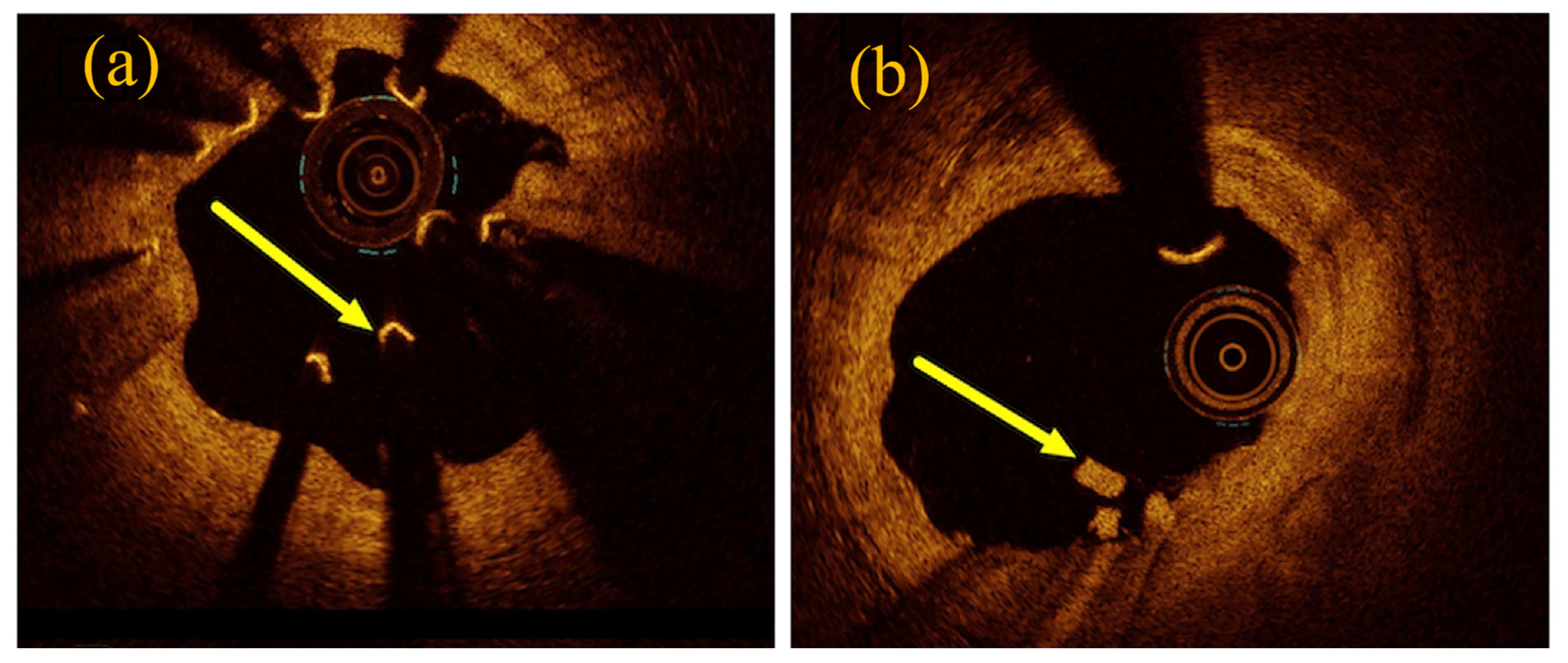
Figure 4.
Magnesium alloys for stents and functions of alloying elements.
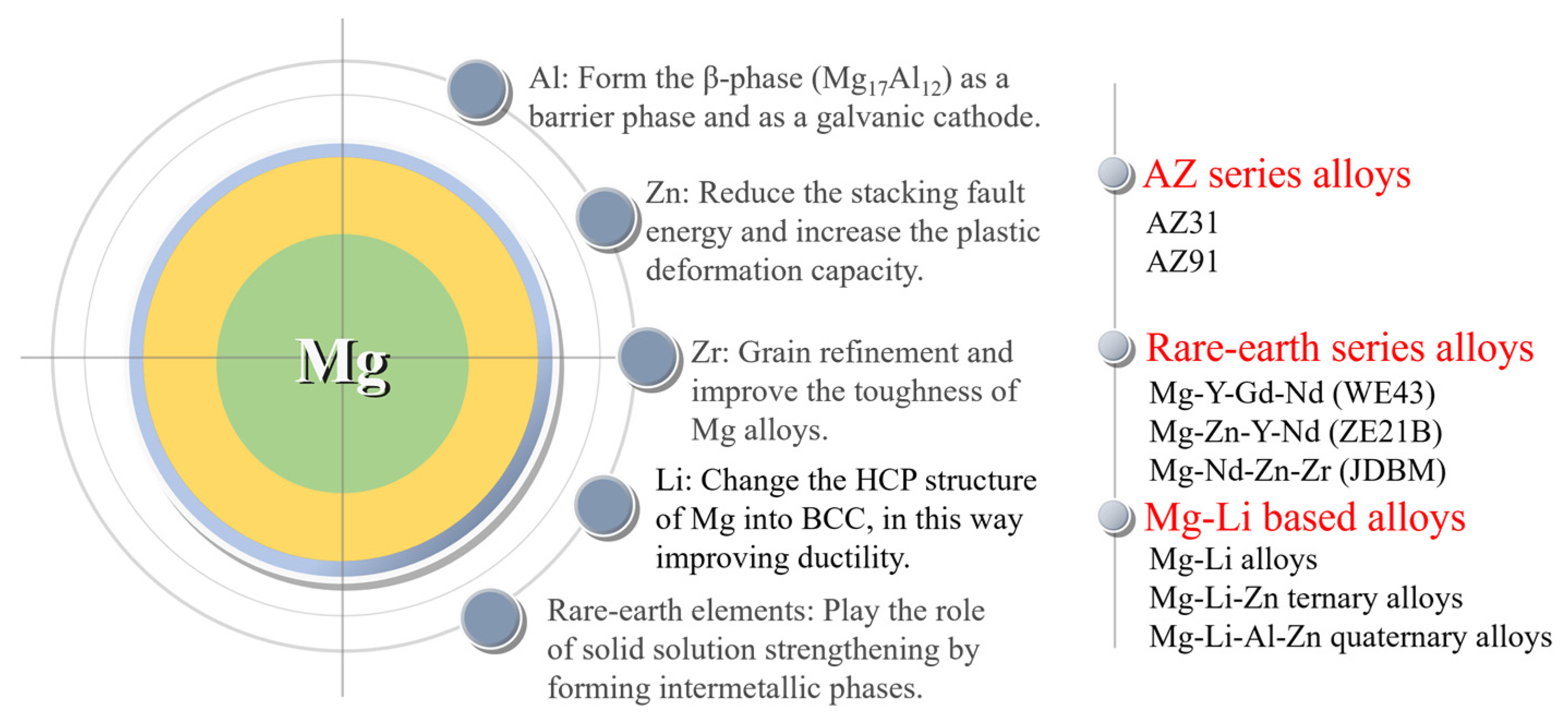
Figure 1.
Schematic illustration of biofunctional PLLA/mSiNP nanocomposite coating on the surface of magnesium alloy stent[105].
Figure 1.
Schematic illustration of biofunctional PLLA/mSiNP nanocomposite coating on the surface of magnesium alloy stent[105].
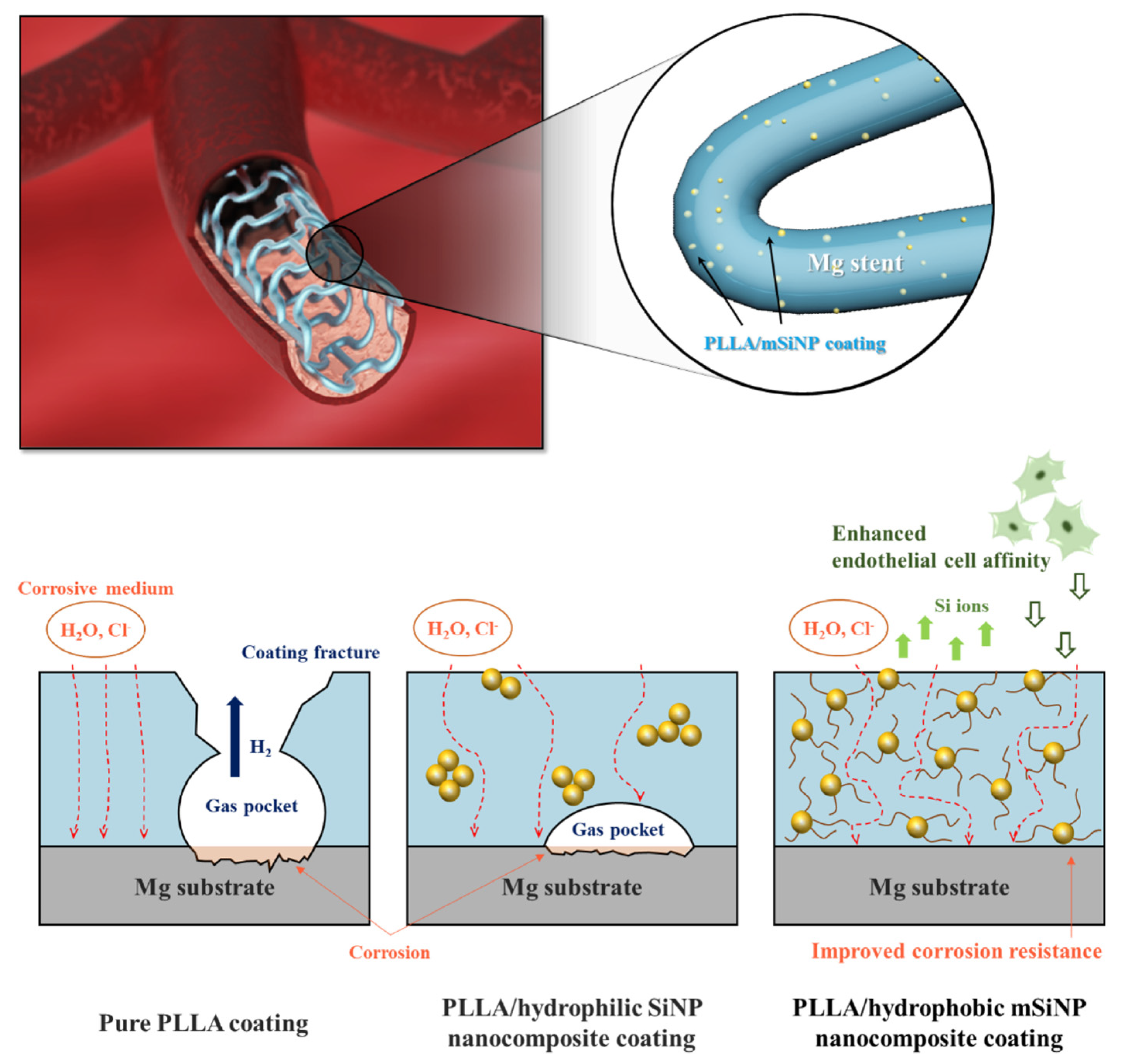
Figure 6.
Schematic diagram of surface and bulk erosions as a function of time[119].
Figure 6.
Schematic diagram of surface and bulk erosions as a function of time[119].
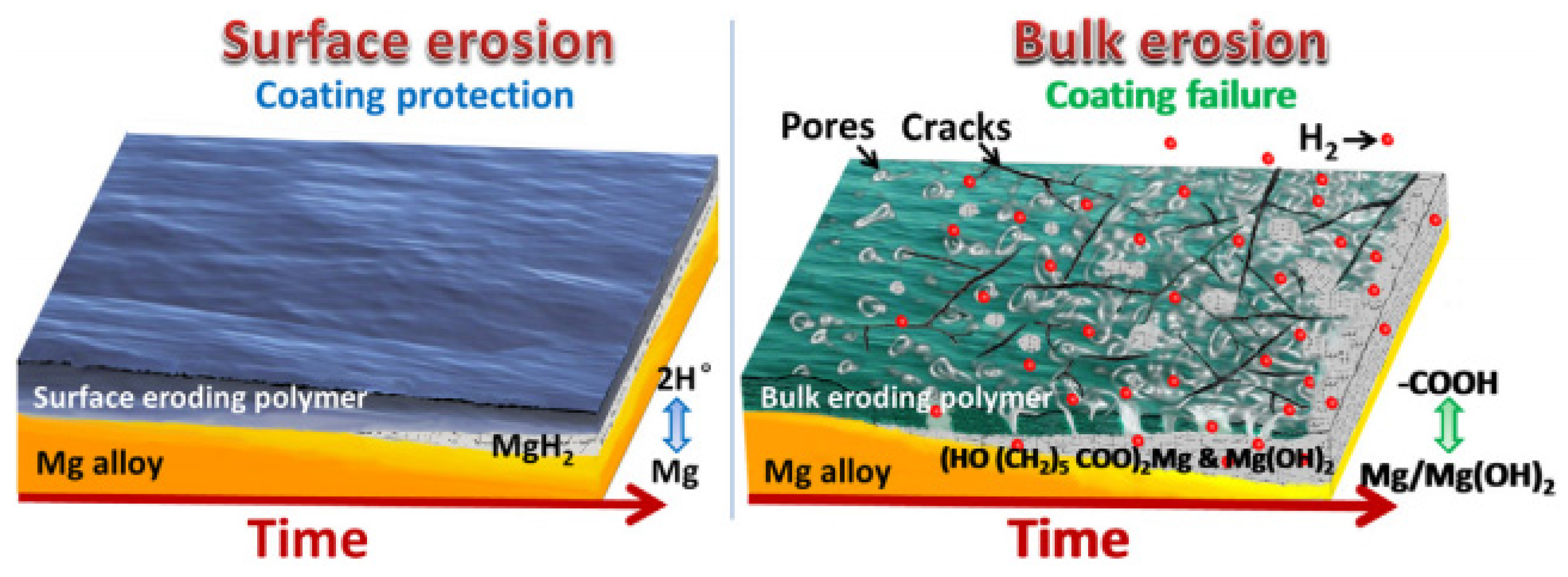
Figure 7.
Chemical structure of BTSE (a) and APTES (b); (c) surface modification procedure on ZE21B alloy[131].
Figure 7.
Chemical structure of BTSE (a) and APTES (b); (c) surface modification procedure on ZE21B alloy[131].
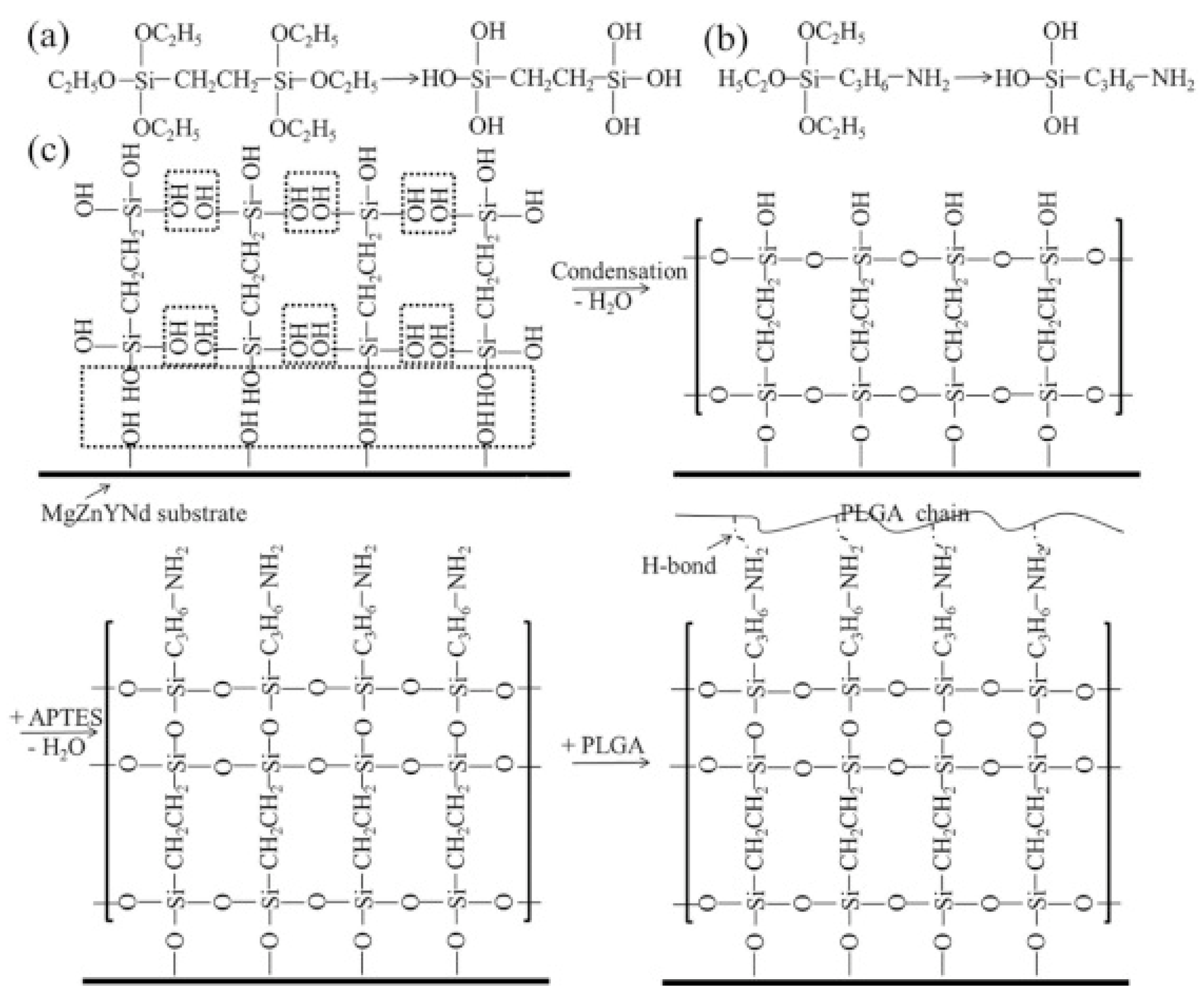
Figure 2.
Further exploration and study of magnesium alloy stents.
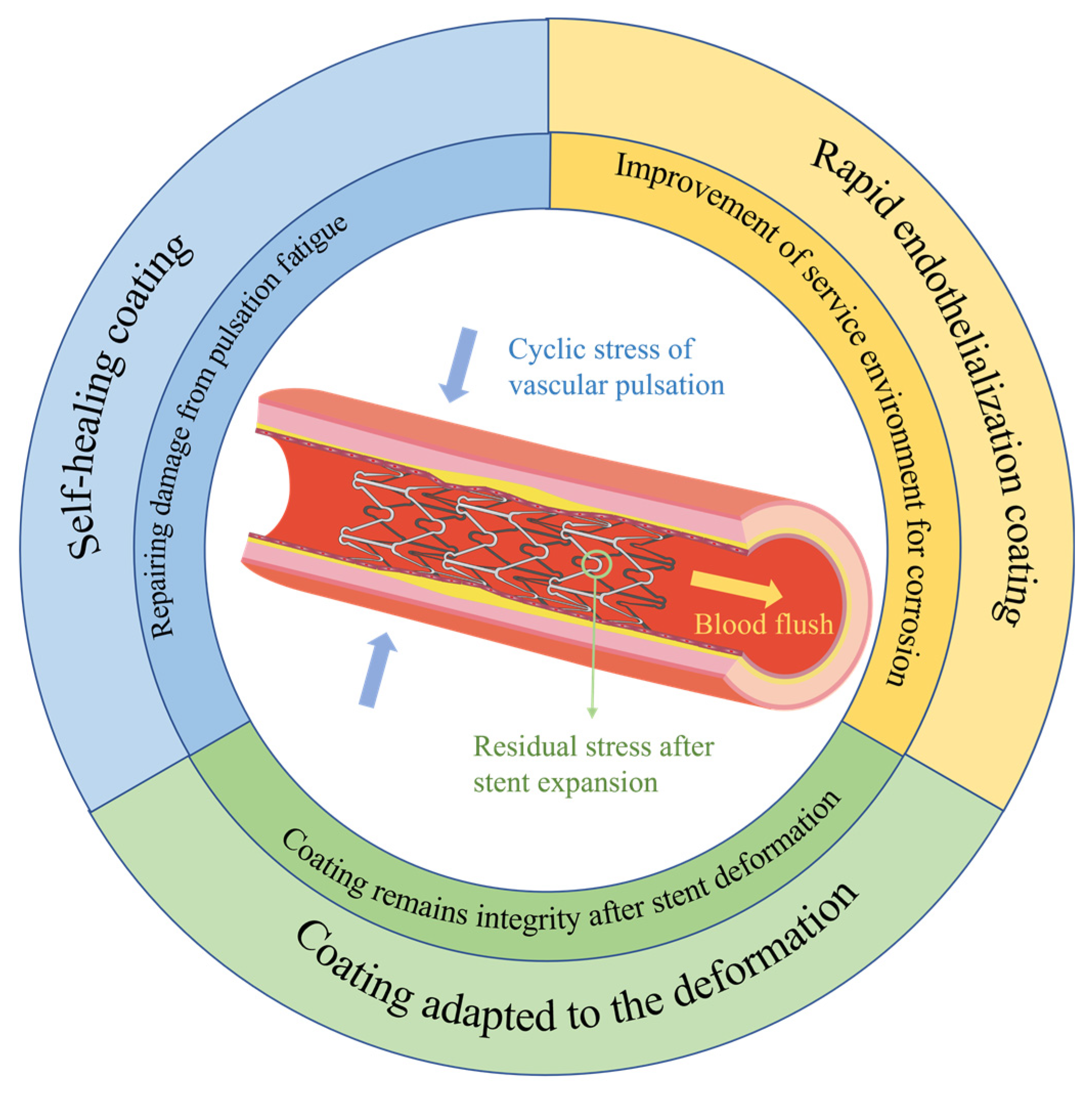
Figure 3.
Surface morphologies of stents with PDLLA-F and PBAT-F coatings after deformation and immersion in PBS[133].
Figure 3.
Surface morphologies of stents with PDLLA-F and PBAT-F coatings after deformation and immersion in PBS[133].
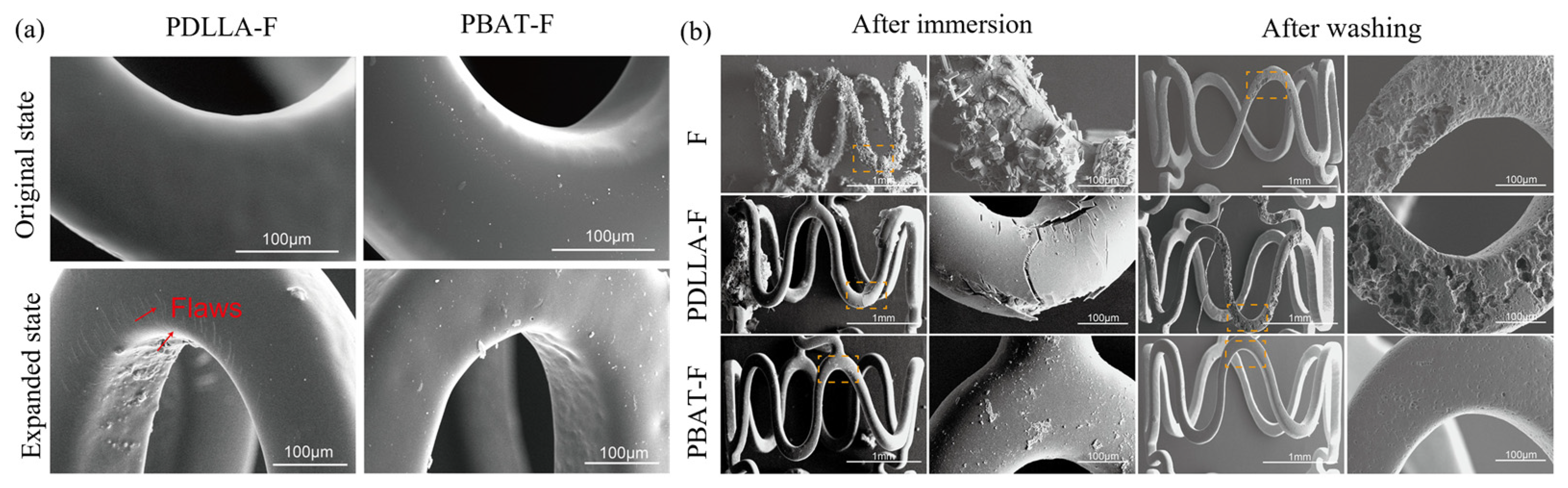
Figure 10.
Schematic illustration of PDA/ Cu2+ eluting coating on magnesium alloy stents for controlling degradation of Mg matrix and modulating local release of Mg2+ and Cu2+, which contributed to the superior bio-efficacy with prolonged stent durability, and enhanced anti-inflammation and anti-restenosis functions through synergistic effect on fostering HUVECs while inhibiting HUASMCs[143].
Figure 10.
Schematic illustration of PDA/ Cu2+ eluting coating on magnesium alloy stents for controlling degradation of Mg matrix and modulating local release of Mg2+ and Cu2+, which contributed to the superior bio-efficacy with prolonged stent durability, and enhanced anti-inflammation and anti-restenosis functions through synergistic effect on fostering HUVECs while inhibiting HUASMCs[143].
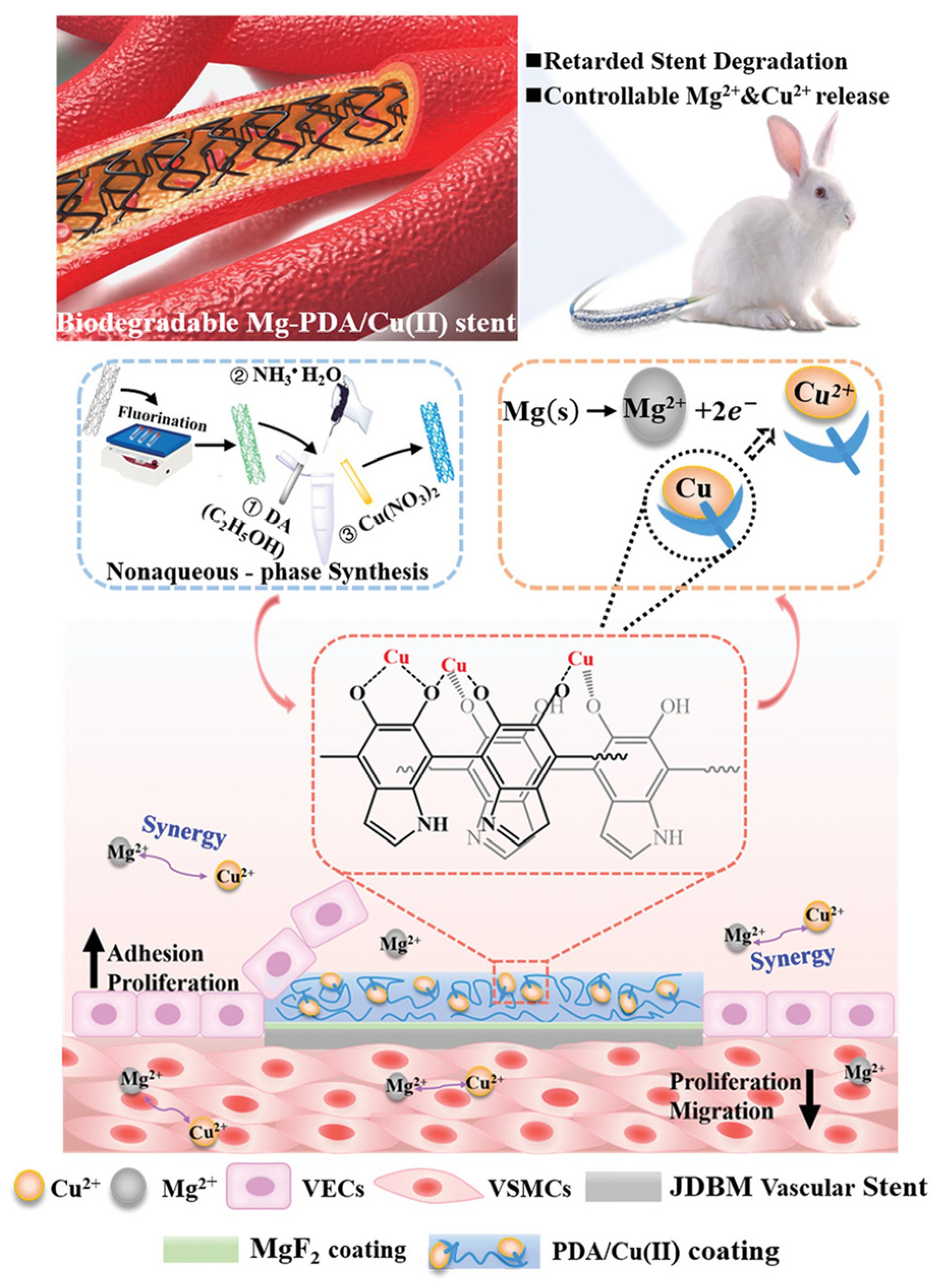
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



