
Submitted:
21 November 2023
Posted:
22 November 2023
You are already at the latest version
Abstract
Lower urinary tract symptoms (LUTS) and hematuria are common symptoms in men with benign prostatic hyperplasia (BPH) and prostate cancer (PCa) mainly affecting the elderly population. Prostatic arterial embolization (PAE) is a minimally invasive pro-cedure that has shown promising results in managing massive intractable prostatic he-maturia in patients with BPH and PCa. A few studies, however, have provided valuable insights into the durability and efficacy of PAE focusing on the long-term effectiveness, quality of life, and cancer-specific control of hemostasis and urinary symptoms. As a result of concomitant cardiovascular conditions, these patients often take anticoagulants or antithrombotics, which can worsen their hematuria and clinical status. Transurethral resection of the prostate (TURP) is considered a very high-risk procedure even without massive bleeding, and requires discontinuation of Vitamin K antagonists and antiplate-let therapies. Such patients usually have their surgery postponed, and PAE should be considered a safe alternative treatment. We aimed to report a narrative review from 1976 to June 2023 of the current state of PAE for massive and intractable hematuria highlighting recent developments in this technique, including prospective cohort stud-ies and focusing on long-term outcome, safety, and complication management in PCa patients with significant hemorrhagic symptoms. As an additional contribution, we propose a simple algorithm for treating intractable bleeding associated with prostate cancer in a 92-year-old man with LUTS.
Keywords:
prostate
; prostatic carcinoma
; benign prostatic hyperplasia
; haematuria
; angiography
; prostate artery embolization
; urinary bladder hemorrhage
1. Introduction
After lung cancer, prostate carcinoma (PCa) is a worldwide health problem being the second most frequent malignancy in men, with 1,276,106 newly diagnosed cases and causing 358,989 deaths (3.8% of all deaths caused by cancer in men) in 2018 [1]. Death rates for PCa have been decreasing and this is mainly due to earlier diagnosis because of screening and improved treatment, resulting in a real postponement of death for some men with metastatic disease and often in a consequent variation in the attribution of cause of death [2]. Metastatic prostate carcinoma presents significant morbidity and fast worsening of the quality of life. More than 30% of these patients will necessitate lower urinary tract surgery and in the late stages of the disease more than 25% will require indwelling bladder catheterization (IBC) insertion through the urethra or suprapubic, or palliative transurethral resection of the prostate (TURP) [3,4]. PCa and benign prostatic hyperplasia (BPH) represent two distinct yet interconnected urological conditions that significantly impact the male population. These disorders are notorious for their potential to induce acute lower urinary tract symptoms (LUTS) that can have profound implications for patients’ health and quality of life. Among these symptoms, urinary retention requiring IBC and urinary tract hemorrhage stand out as particularly alarming clinical manifestations, often necessitating immediate medical intervention and even emergency care.
While these conditions differ in their underlying pathology and clinical course, they share a common thread in the potential to precipitate acute LUTS that can be severe and life-threatening especially in the elderly population with multimorbidity.
TURP is considered the surgical gold standard for patients with severe symptomatic BPH. It is effective and durable, but it can cause several complications, including bleeding, dilutional hyponatremia, sexual dysfunction, and incontinence [5]. Moreover, TURP is a “high risk of bleeding” procedure that, in high-risk patients, involves discontinuation of anticoagulant/antiplatelet therapy while PAE is considered a safe treatment alternative for high-risk patients on anticoagulants. These features boosted the development of less invasive treatment options for BPH: holmium laser enucleation of the prostate, thulium laser–based enucleation, GreenLight laser therapy, and transurethral water vaporizing therapy. However, none of these treatment options has shown superior clinical benefit when compared with TURP [6].
In 1976 Mitchell reported selective hypogastric embolization in 4 patients experiencing severe prostatic hemorrhage, after undergoing biopsy or prostatectomy, with high success rates [7]. The first successful therapeutic PAE for bleeding in a PCa patient was reported in 1977 by Bischoff and Goertler [8] using Gelfoam; later, Nadalini [9] described 14 cases of hypogastric arteries embolized with isobutyl-2-cyanoacrylate for hemorrhage due to bladder and prostatic carcinomas. Prostatic artery embolization (PAE) was later used in high-surgical-risk patients with acute urinary retention who had IBC, and eventually emerged as a potential innovative technique for selected patients as a minimally invasive alternative treatment to TURP in patients with moderate to severe BPH determining urinary tract symptoms and/or bladder outlet obstruction. In all patients with LUTS, PAE proved to be a minimally invasive treatment option for BPH and was shown to be safe and effective in reducing prostatic volume and improving LUTS relating to BPH [10,11] with a low morbidity rate and lower incidence of sexual dysfunction due to retrograde ejaculation [12].
In 1990, Li [13] performed PAE in BPH in a group of 16 patients, with an age range of 44-72 years. Nine patients had bladder cancer, one had prostatic cancer, and six had BPH. A combination of Gelfoam (Pharmacia & Upjohn, Kalamazoo, MI) and coils were employed to embolize the internal iliac arteries and hemostasis was achieved in 15 patients without complications. Since then, transarterial PAE of symptomatic BPH has slowly gained popularity. This is because it is minimally invasive, does not require general anesthesia, and appears to be effective in stopping bleeding and relieving voiding difficulties. In 2000 DeMeritt [14] reported a case of PAE performed with polyvinyl alcohol particles for hematuria associated with BPH: the patient had symptomatic improvement, hematuria was immediately stopped, and prostate size was reduced by 52% of the initial size in the first five-month follow-up and 62% of the initial size at 12-month follow-up. In 2010, Carnevale [15] reported PAE using microspheres in two patients as a primary treatment for acute urinary retention due to BPH. For elderly men with symptomatic BPH, PAE can be an alternative treatment: it is performed by a femoral artery puncture and under conscious sedation instead of general anesthesia. PAE produces an immediate infarction of the central gland resulting in its overall volume decrease; delayed fibrosis produces a further size reduction. Moreover, in BPH the transitional zone, the noncancerous growth of the prostate surrounding the prostatic urethra, becomes ischemic. This process is also extended in the peripheral zone suggesting a potential clinical role as a palliative treatment for prostate carcinoma [16]. However, despite the available data, PAE has yet to be established as a standard-of-care treatment option for patients with LUTS and low urinary tract bleeding due to BPH/PCa.
In this study, we aimed to perform a systematic literature review on indications and outcomes of PAE in the treatment of refractory bleeding from the lower urinary tract especially focusing on the management of refractory bleeding from prostatic adenocarcinoma. In addition, we present a simple treatment algorithm based on a challenging case report of a patient with multimorbidity who presented with massive refractory bleeding from prostatic adenocarcinoma and developed massive refractory haematuria successfully treated with PAE.
2. PAE and the importance of careful evaluation of the prostate gland’s vascular supply.
When planning PAE, it is vital to carefully consider the anatomical connections of the prostate gland [17]. There are two prostatic arteries (left and right), also known as the inferior vesical arteries, and other arteries that supply structures and organs in the male pelvic region. As a result, unintended embolization may occur in non-target areas. The inferior vesical artery (IVA), which supplies blood to the bladder, is situated in the pelvic area. It branches off from the internal iliac artery, usually alongside the middle rectal artery within the anterior division. Its blood flow reaches the bladder fundus. The inferior vesical artery supplies blood to the prostate and seminal vesicles in males, like the vaginal artery in females. In addition, this artery can share a trunk with the superior gluteal and internal pudendal arteries, and it can also branch off from the internal pudendal artery. In most cases, there is only one additional branch, but this varies from individual to individual. The IVA also supplies the ductus deferens, a segment of the spermatic passageway. Regarding the prostatic arteries, their origins can significantly differ between the left and right sides of the body and among patients. Most commonly, they originate from the internal pudendal artery. The prostate has a dual arterial supply: the cranial or vesico-prostatic artery (sometimes called the anterior-lateral prostatic pedicle) and the caudal prostatic artery (known as the posterior-lateral prostatic pedicle). In cases with only one prostatic artery (occurring in 60% of cases), both prostatic pedicles may arise from the same artery. However, in patients with two independent prostatic arteries (occurring in 40% of cases), the pedicles originate separately. On the other hand, the posterior-lateral prostatic pedicle has an inferior or distal origin, providing blood to the peripheral and caudal glands. It may be closely associated with rectal or anal branches. Careful evaluation of the prostate’s vascular anatomy is crucial for the successful planning of PAE. It is significant to note that up to 60% of cases exhibit significant connections between the prostatic branches and surrounding arteries. These connections should be carefully considered when planning an embolization. Figure 1 shows a schematic illustration of the main anatomical variations in bladder and prostatic vascularization.
The prostatic artery (Pa) presents highly variable origins. De Assis AM and coll. has suggested five types of anatomic origins of Pas which have been classified as follows [17]:
Type I: PA originating from the anterior division of the IIA, in a common trunk with the SVA 28.7%,
Type II: PA originating from the anterior division of the IIA, inferior to the SVA 14.7%,
Type III: PA originating from the obturator artery 18.9%,
Type IV: PA originating from the IPA 31.1%,
Type V (others): less common origins 5.6%. This subgroup includes the “corona mortis” (crown of death), a connection between the obturator and the external iliac artery or vein. It is located behind the superior pubic ramus at a variable distance from the symphysis pubis (range 40-96 mm). The name “corona mortis” suggests that a significant hemorrhage may occur if accidentally cut and it is difficult to achieve subsequent hemostasis [18].
3. Materials and Methods
Research Methodology for Literature Review
This literature review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. The search was conducted across multiple databases, including PubMed, EMBASE, Web of Science, and Cochrane, from 1976 to June 2023. Our search employed MeSH terms, including “prostatic artery embolization” AND “hematuria”. Following the removal of duplicate entries, we meticulously screened the remaining articles based on their titles and abstracts. For inclusion in this review, we considered all peer-reviewed articles published in the English language that involved patients with hematuria stemming from PCa or BPH and who had undergone angioembolization to control bleeding (see Figure 2 PRISMA flowchart). As a subsequent step, we searched for publications containing prospective clinical trials of PAE for the management of massive intractable bleeding originating from PCa. All prospective clinical trials were extracted and classified according to qualitative synthesis in a dedicated table.
4. Results
As a result of our search, we were able to find 211 articles in EMBASE, 80 in PubMed, 167 in Web of Sciences; no article was found in the Cochrane database. A total of 73 papers were excluded as conference abstracts, letters, editorials, surveys, or concise reviews. After eliminating duplicate articles, we meticulously analysed 96 relevant publications (see Figure 2). From this pool, we identified and synthesized data from 30 comparative and prospective studies exclusively focused on prostatic artery embolization. In addition, we synthesized data from the remaining 66 non-prospective studies and case reports. All 30 prospective studies are comprehensively presented and summarized in Table 1 for detailed examination. Table 1 presents the first author, year of research, region, age, number of patients treated, angioembolization material, outcomes for patients, and some critical points highlighted by the Authors. A summary of the remaining 66 articles about PAE for bleeding and LUTS secondary to PCa was provided and reported on the following topics: Efficacy, Yield, Morbidity and Complications, Patient selection, Long-term outcomes, Comparison with other treatments.
4.1. Efficacy of PAE
PAE has shown promising efficacy in controlling bleeding and improving LUTS in patients with PCa. Saro and coll. [47] confirm the effectiveness and safety of PAE in elderly patients aged ≥ 80 years old (mean 85.29, range 80-98). There were significant improvements in the International Prostate Symptom Score (IPSS) and quality of life (QoL) showing that PAE is a feasible low-risk treatment for prostatic hematuria also in elderly patients with or without urinary retention.
Several prospective studies were carried out to evaluate PAE for acute urinary retention and/or prostates larger than 80 mL, which are not typically eligible for TURP. In these studies the procedure proved to be safe and effective also in larger prostates, with reported clinical success in 72.4%–98% of patients [9,17,21,29,30].
4.2. Yield of PAE
The yield of PAE in terms of bleeding control generally appears favorable and varies among studies, from 67% [23], where patients had PCa and refractory hematuria, to 100% [41]. It is critical to recognize a success rate of 94.1% in patients aged > 80 years old [31]. Success rates may depend on the patient population, the severity of bleeding, and the expertise of the interventional radiologists performing the procedure.
4.3. Morbidity and complications
Anyway, PAE is generally considered a minimally invasive procedure with a low rate of major complications. Informed consent should include a further discussion of the rare but potentially serious complications of nontarget embolization to the penis, rectum, and bladder [49]. Minor complications include post-PAE syndrome, dysuria, hematuria, and hematospermia. In our review, 4 cases major complications of partial bladder necrosis 1 sepsis 2 cases of penile ulcers all requiring surgery have been reported [9,33,34,40]. Access site complications are described and include puncture size hematoma (PSH) and femoral artery dissection (FAD); 4 (1.85%) FAD cases and 4 (1.85%) PSH cases were reported by Ray [34], 1 (1.3%) FAD case by Insausti [48] and 6 PSH cases (11.8%) by Brown [39]. Postembolization syndrome (i.e gluteal pain, fever, nausea, emesis) has been reported as manageable with symptomatic treatment approach only, with complete resolution within few days. As compared with superselective embolization as distal as possible, embolization of the main trunk of the internal iliac artery or the whole anterior or posterior division of the iliac artery increased the risk of ischemic complications.
4.4. Patient selection for PAE
Proper patient selection is crucial to the success of PAE. Patients should be carefully evaluated to determine if they are suitable candidates for the procedure. PAE in non-emergency setting is typically considered for patients who have failed conservative management and are not candidates for more invasive treatments. Moreover, it is necessary to have a detailed understanding of the anatomy of the pelvic arteries to safely perform the procedure avoiding nontarget embolization [49]. In the emergency setting in patients with recurrent or intractable bleeding secondary to Pca hemorrhage PAE should be considered the preferred therapeutic indication also in those patients who will be candidates for a definitive surgical treatment; detection of active bleeding by CT scan or angiography is not an obligatory finding to proceed with PAE in patients with refractory cancer haemorrhage.
4.5. Long-term Outcomes
Long-term outcome data in PCa patients show that PAE successfully treats complications associated such as LUTS, urinary retention, and hematuria with a low risk of serious adverse events [49]. PAE as the primary oncological treatment for PCa is currently inadequate [42]: more large-scale randomized trials are needed for further assessment of PAE as a potential option for a combination treatment for prostate cancer.
4.6. Comparison to Other Treatments
PAE can be an alternative to other treatments, especially in BPH LUTS refractory to medical therapy. It is necessary to underline that α-blockers and 5α-reductase inhibitors are associated with adverse side-effects associated with a decrease in sexual function and QoL [50]. We found several studies [9,10,29,48] where a comparison PAE/medical therapy in BPH has been performed, especially in patients with LUTS refractory to pharmacological treatment, where QoL was significantly improved. Furthermore, PAE has been compared to other treatments such as surgical interventions, radiation therapy, or cystoprostatectomy in patients with massive intractable bleeding from PCa. Several studies have compared PAE and TURP in patients with LUTS showing promising results in patients treted with PAE, including rates of resolution of urinary tract symptoms, with significant reductions in the International Prostate Symptom Score (IPSS), improvement in peak urinary flow (Qmax), and overall lower complication rates [34,42,48]. More comparative prospective studies are essential to establish its role relative to other treatment options.
5. A suggested algorithm and a demonstrative patient profile
As an illustration of our proposed algorithm (Figure 9) we describe a clinical complex case report in a patient with LUFT who underwent PAE as a rescue procedure for intractable urinary bleeding from his prostate cancer. A 92-year-old man, affected by PCa and with a long-term indwelling bladder catheter (IBC), was admitted for a massive bladder hemorrhage. The patient, a former smoker, had blood hypertension treated with an ACE inhibitor; he presented with elevated PSA levels of 62 ng/mL, and his symptomatology was limited to nocturia causing 2–3 nocturnal lifts. A prostatic biopsy revealed a Gleason score of 7 (3 + 4) adenocarcinoma in 6 of 12 specimens. Laboratory blood test values were within the reference range; chest X-ray, bone scan, and thoracic and abdominal CT scan were negative. The chest CT scan showed initial pulmonary fibrosis as an incidental finding. Because of the advanced stage of the disease and pulmonary fibrosis, the primary treatment modality was hormonal therapy: so, he assumed Bicalutamide 50 mg/day and Triptorelin 11,75 mg, a synthetic agonist analog of gonadotropin-releasing hormone (GnRH). After 6 months Triptorelin was discontinued, and only Bicalutamide 150 mg/day was prescribed. In March 2019 he underwent Choline PET-CT demonstrating common iliac and aortic nodal chains with metastatic involvement and in June PSA was 20,78. In January 2020 PSA was 27 ng/mL and increased to 38 ng/mL in May and in August the value was 53 ng/mL; testosterone was < 0,1 ng/mL. At this point, a Choline PET scan showed several skeletal secondary localizations, dorsal and lumbar vertebral bodies, the pelvis, and the 11th right rib. In January 2022 the patient started to have hematuria that rapidly became a gross hemorrhage with clot formation and urinary obstruction. In addition to urinary obstruction and massive hemorrhage, the patient also suffered three syncopal episodes. He was immediately hospitalized, and a three-way IBC was positioned for continuous bladder irrigation to prevent blood clots. Hb dropped from 14.5 g/dL to 7.9 g/dL and a blood transfusion was done; despite continuous bladder irrigation, blood was still present in the urine. Chest and abdominal CT scans revealed large bleeding associated with PCa expansion into the bladder involving the neck and trigone (Figure 3). To stop the bleeding, a PAE was performed. The procedure is described in Figure 4, Figure 5, Figure 6 and Figure 7. Hematuria was resolved one week after the procedure, LUTS ameliorated, and quality of life improved significantly. The patient died at the age of 93 in the fourth post-procedure month of respiratory insufficiency due to pulmonary fibrosis.
5.1. Technical details of PAE
In an angio-suite, a 5 Fr valved sheath was inserted into the right common femoral artery. Under direct fluoroscopic guidance, selective catheterization of the internal iliac arteries was carried out with a 5 Fr pre-curved catheter Vertebral. PAE was performed using the standard “Proximal Embolization First, Then, Embolize Distal” (PErFecTED) technique [26].
Prostatic arteries showed bilateral origin type 2. After a super-selective catheterization of both prostatic arteries with a microcatheter 2.0 F (Progreat, Terumo), PAE was completed using PErFecTED technique by injecting a solution of microbeads (Embosphere 300-500 μm, Merit Medical) mixed with 9 ml of saline and 9 ml of contrast medium. The procedure was safe and effective resulting in the complete embolization of prostatic arteries. Finally, groin hemostasis was achieved with Angioseal 6 Fr. Hematuria was resolved one week after the procedure, LUTS ameliorated, and quality of life improved significantly.
Figure 9.
A simple algorithm to evaluate prostatic artery embolization in patients with LUTS and prostate cancer. TF = transfemoral, TR = transradial, LUTS = low urinary tract symptoms, BPH = benign prostate hyperplasia, PCa = prostate carcinoma, QoL = quality of life, TURP = transurethral resection of the prostate.
Figure 9.
A simple algorithm to evaluate prostatic artery embolization in patients with LUTS and prostate cancer. TF = transfemoral, TR = transradial, LUTS = low urinary tract symptoms, BPH = benign prostate hyperplasia, PCa = prostate carcinoma, QoL = quality of life, TURP = transurethral resection of the prostate.

6. Discussion
The management of patients with high-risk, early-stage PCa represents a major challenge for all disciplines involved in the treatment of this common malignant neoplasm.
Pisco and Coll. [40] made preliminary evidence of the technical feasibility and safety of prostatic artery chemoembolization (PACE) for treating PCa: in their prospective study, 20 PCa patients underwent PACE; the mean Gleason score range was 6 to 10, and their staging was T2N0M0. PACE was performed with a combination of Chelidonium majus extract, docetaxel, and 150–300-µm Embosphere particles. All patients were treated on an outpatient basis and discharged home the same day. Technical success of the procedure, defined as bilateral PAE, was achieved in 16 out of 20 patients. Adverse events were few and mostly minor. Multiparametric prostate MRI done at 12 months for the 10 patients with biochemical successes showed that of the seven patients with a Gleason score of 6, no changes were seen in the lesions, whereas the three patients with a Gleason score of > 7 had > 50% tumor size reduction. Peacock’s prospective study demonstrated that PAE is a clinically significant adjunctive therapy for alleviating LUTS and achieving significant volume reduction before RT, resulting in decreased radiation-related toxicity from prostate alone RT for PCa [44]. According to the Society of Interventional Radiology, PAE might lead to minor and major complications. Side effects of embolization i.e. pain, hematuria, hematospermia, urethral burning, rectal bleeding, urinary tract infection, balanitis, hematoma, diarrhea, dissection acute urinary retention, non-target embolization. Non-target embolization complications have been categorized as major complications depending on the necessity of the therapy, overnight admission, or prolonged hospitalization.
The present systematic review collected the available data attributable to prostate arterial embolization in patients with prostate cancer. We analysed and assessed comparative and non-comparative publications. Not all focused only on the patients with prostate cancer. Nevertheless, the heterogeneity of the population showed the wide range of indications and effectiveness of this method. The studies prove the procedure is safe, burdened with low risk of complications, and accomplishes technical and clinical success. In selecting the optimal treatment method in poor surgical patients, the minimally invasive method has to be considered. Thereby, prostate artery embolization for patients with PCa experiencing massive hematuria is a promising option with an important impact on the quality of life as pain reduction, improvement in urinary symptoms, and overall well-being and is now becoming a part of the standard-of-care treatment algorithm for patients with urinary hemorrhage and other sequelae secondary to prostate cancer.
In this article, we also tried to provide a systematic review of PAE delving into some intricate aspects and clinical challenges in those patients with prostatic cancer associated with important comorbidities.
A simple algorithm was developed from our experience that can be utilized in the emergency setting as a life-saving procedure in case of massive hematuria showing the essential strategy for timely and effective management of prostatic symptoms. Simple algorithms can be useful in emergency clinical practice with a possible positive impact on patient outcomes. PAE can be performed on an outpatient basis and usually does not require IBC unless the patient has urinary retention [51,52] and can be considered a good alternative to the standard TURP [53,54].
Concomitant ischemic heart disease and low left ventricle ejection fraction are not a contraindication to PAE and several case reports have been reported in these high-risk patients with important LUTS improvement [55,56,57]. In patients with severe pain and bleeding caused by advanced prostate cancer PAE appears as one of the most reliable and advantageous options [58].
PAE is a minimally invasive technique associated with a high success rate of hemostasis and a low incidence of recurrence [59]. In patients with patent carpal circulation, PAE can been successfully performed via transradial access [60,61].
In the context of prostate cancer and massive hematuria, a collaborative approach may contribute to better outcomes and care for these patients. For this reason, a multidisciplinary collaboration in the management of prostatic cancer patients with massive hematuria involving interventional radiologists, urologists, and oncologists.is of the utmost importance.
7. Conclusions
Finally, PAE in elderly patients with LUTS, urinary retention, and prostatic hematuria should be considered as an effective alternative to surgery when feasible. PAE appears to be a promising option for controlling bleeding and improving lower urinary tract symptoms (LUTS) in patients with prostatic adenocarcinoma who experience urinary tract massive or recurrent hemorrhage or severe LUTS. However, further research, including long-term follow-up studies and comparative trials, is needed to better define its exact role in the overall management of these patients.
Abbreviations
PCa prostate carcinoma, IBC indwelling bladder catheterization, BPH = benign prostatic hyperplasia, PAE = prostatic artery embolization, TURP = transurethral resection of the prostate, LUTS = acute lower urinary tract symptoms, PA= Prostatic artery, PAs = Prostatic arteries, IIA = internal iliac artery, ATIIA = anterior trunk internal iliac artery, PTIIA = posterior trunk internal iliac artery, SVA = superior vesical artery, OA = obturator artery, IPA = internal pudendal artery, FU = follow-up, TS = technical success, CF = clinical failure, CS = clinical success, COMP/PROSP = comparative/prospective study, OP = open prostatectomy, BIL = bilateral, UNI = unilateral, ATH = atherosclerosis, HEM = hematuria, UI = urinary infection, UR = urinary retention, AUR = acute urinary retention, M = months, UB = urethra burning, PV = prostate volume, PVR = post-void residual, IIEF = international index erectile function, IPSS =International Prostate Symptom Score, QoL = quality of life, ED = erectile dysfunction, EF = ejection fraction, FAD = femoral artery dissection, PES = post-embolization syndrome, HS = hospital stay, IBC = indwelling bladder catheter, RHOPA = refractory hematuria of prostatic origin, MRI = magnetic resonance imaging, PSH = puncture size hematoma, DYS = dysuria, HEMS = hemospermia, PACE = prostatic artery chemoembolization, HT = hormonal therapy, HTR = hormone therapy resistant, IHD = ischemic heart disease, SDYS = sexual dysfunction, BF = biochemical failure, BS = biochemical success, MOF = multiorgan failure, PK = peak flow, NK = no known, RI = respiratory insufficiency, RT = radiotherapy.
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Wong MC, Goggins WB, Wang HH, Fung FD, Leung C, Wong SY, Sung JJ. Global incidence and mortality for prostate cancer: analysis of temporal patterns and trends in 36 countries. Eur Urol. 2016, 70, 862–874. [Google Scholar] [CrossRef]
- Collins A, Sundararajan V, Millar J, Burchell J, Le B, Krishnasamy M, et al. The trajectory of patients who die from metastatic prostate cancer: a population-based study. BJU Int. 2018.
- Babaian K, Truong M, Cetnar J, Cross DS, Shi F, Ritter MA, Jarrard DF. Analysis of urological procedures in men who died from prostate cancer using a population-based approach. BJU Int. 2013, 111, E65–E70. [Google Scholar]
- Rink JS, Froelich MF, McWilliams JP, Gratzke C, Huber T, Gresser E, Schoenberg SO, Diehl SJ, Nörenberg D. Prostatic Artery Embolization for Treatment of Lower Urinary Tract Symptoms: A Markov Model-Based Cost-Effectiveness Analysis. J Am Coll Radiol 2022; S1546-1440(22)00275-7. [CrossRef]
- Westwood J, Geraghty R, Jones P, Rai BP, Somani BK. Rezum: a new transurethral water vapour therapy for benign prostatic hyperplasia. Ther Adv Urol 2018; 10:327-333.
- Mitchell ME, Waltman AC, Athanasoulis CA, Kerr WS Jr, Dretler SP. Control of massive prostatic bleeding with angiographic techniques. J Urol 1976, 115, 692–695. [Google Scholar] [CrossRef]
- Bischoff, W.; Goertler, U. Successful intra-arterial embolization of bleeding carcinoma of the prostate. Urologe A, 1977, 16, 99–102. [Google Scholar]
- Nadalini, V.F.; Positano, N.; Bruttino, G.P.; Medica, M.; Fasce, L. Therapeutic occlusion of the hypogastric arteries with isobutyl-2-cyanoacrylate in vesical and prostatic cancer. Radiol Med (Torino) 1981, 67, 61–66. [Google Scholar]
- Grosso, M.; Balderi, A.; Arnò, M.; Sortino, D.; Antonietti, A.; Pedrazzini, F.; Giovinazzo, G.; Vinay, C.; Maugeri, O.; Ambruosi, C.; Arena, G. Prostatic artery embolization in benign prostatic hyperplasia: preliminary results in 13 patients. Radiol Med 2015, 120, 361–368. [Google Scholar] [CrossRef]
- Pisco, J.M.; Rio Tinto, H.; Campos Pinheiro, L.; Bilhim, T.; Duarte, M.; Fernandes, L.; Pereira, J.; Oliveira, A.G. Embolisation of prostatic arteries as treatment of moderate to severe lower urinary symptoms (LUTS) secondary to benign hyperplasia: results of short- and mid-term follow-up. Eur Radiol 2013, 23, 2561–2572. [Google Scholar] [CrossRef]
- Wang, X.-Y.; Chai, Y.-M.; Huang, W.-H.; Zhang, Y. Prostate artery embolization on lower urinary tract symptoms related to benign prostatic hyperplasia: A systematic review and metaanalys. World J Clin Cases 2022, 10, 11812–11826. [Google Scholar] [CrossRef]
- Li, B.C. Li BC. Internal iliac artery embolization for the control of severe bladder and prostate haemorrhage. Chung Hua Wai Ko Tsa Chic 1990; 28: 220-1, 253. Chinese.
- DeMeritt, J.S.; Elmasri, F.F.; Esposito, M.P.; Rosenberg, G.S. Relief of benign prostatic hyperplasia-related bladder outlet obstruction after transarterial polyvinyl alcohol prostate embolization. J Vasc Interv Radiol 2000, 11, 767–70. [Google Scholar] [CrossRef]
- Carnevale FC, Antunes AA, da Motta Leal Filho JM, Oliveira Cerri LM, Baroni RH, Marcelino AS, et al. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients. Cardiovasc Interv Radiol 2010; 33(2):355-61. [CrossRef]
- Lin Y-T, Amouyal G, Correas J-M, Pereira H, Pellerin O, Giudice CD, et al. Can prostatic arterial embolisation (PAE) reduce the volume of the peripheral zone? MRI evaluation of zonal anatomy and infarction after PAE. Eur Radiol 2016; 26:3466–73. [CrossRef]
- de Assis AM, Moreira AM, de Paula Rodrigues VC, Yoshinaga EM, Antunes AA, Harward SH, Srougi M, Carnevale FC. Prostatic artery embolization for treatment of benign prostatic hyperplasia in patients with prostates > 90 g: a prospective single-center study. J Vasc Interv Radiol. 2015, 26, 87–93. [Google Scholar] [CrossRef]
- Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat 2007 May;20(4):433-9. [CrossRef]
- Bilhim T, Pisco J, Campos Pinheiro L, Rio Tinto H, Fernandes L, Pereira JA, Duarte M, Oliveira AG. Does polyvinyl alcohol particle size change the outcome of prostatic arterial embolization for benign prostatic hyperplasia? Results from a single-center randomized prospective study. J Vasc Interv Radiol 2013, 24, 1595–602. [Google Scholar] [CrossRef]
- Gao YA, Huang Y, Zhang R, Yang YD, Zhang Q, Hou M, Wang Y. Benign prostatic hyperplasia: prostatic arterial embolization versus transurethral resection of the prostate—a prospective, randomized, and controlled clinical trial. Radiology 2014, 270, 920. [Google Scholar] [CrossRef]
- Kurbatov D, Russo GI, Lepetukhin A, Dubsky S, Sitkin I, Morgia G, Rozhivanov R, Cimino S, Sansalone S. Prostatic artery embolization for prostate volume greater than 80 cm3: results from a single-center prospective study. Urology 2014, 84, 400–4. [Google Scholar] [CrossRef] [PubMed]
- Bagla S, Martin CP, van Breda A, Sheridan MJ, Sterling KM, Papadouris D, Rholl KS, Smirniotopoulos JB, van Breda A. Early results from a United States trial of prostatic artery embolization in the treatment of benign prostatic hyperplasia. J Vasc Interv Radiol 2014, 25, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Russo GI, Kurbatov D, Sansalone S, Lepetukhin A, Dubsky S, Sitkin I, Salamone C, Fiorino L, Rozhivanov R, Cimino S, Morgia G. Prostatic arterial embolization vs open prostatectomy: a 1-year matched-pair analysis of functional outcomes and morbidities. Urology 2015, 86, 343. [Google Scholar] [CrossRef] [PubMed]
- Li Q, Duan F, Wang MQ, Zhang GD, Yuan K. Prostatic Arterial Embolization with Small Sized Particles for the Treatment of Lower Urinary Tract Symptoms Due to Large Benign Prostatic Hyperplasia: Preliminary Results. Chin Med J (Engl) 2015, 128, 2072–7. [Google Scholar] [CrossRef] [PubMed]
- Carnevale FC, Iscaife A, Yoshinaga EM, Moreira AM, Antunes AA, Srougi M. Transurethral resection of the prostate (TURP) versus original and PErFecTED prostate artery embolization (PAE) due to benign prostatic hyperplasia (BPH): preliminary results of a single center, prospective, urodynamic-controlled analysis. Cardiovasc Intervent Radiol. 2016, 39, 44–52. [Google Scholar] [CrossRef]
- Carnevale, F.C., Moreira, A.M., Antunes, A.A. The “PErFecTED Technique”: Proximal Embolization First, Then Embolize Distal for Benign Prostatic Hyperplasia. Cardiovasc Intervent Radiol 2014; 37:1602–1605. [CrossRef]
- Wang M, Guo L, Duan F, Yuan K, Zhang G, Li K, Yan J, Wang Y, Kang H. Prostatic arterial embolization for the treatment of lower urinary tract symptoms caused by benign prostatic hyperplasia: a comparative study of medium- and large-volume prostates. BJU Int 2016, 117, 155–64. [Google Scholar] [CrossRef]
- Gabr AH, Gabr MF, Elmohamady BN, Ahmed AF. Prostatic artery embolization: a promising technique in the treatment of high-risk patients with benign prostatic hyperplasia. Urol Int 2016, 97, 320–324. [Google Scholar] [CrossRef]
- Pisco JM, Bilhim T, Pinheiro LC, Fernandes L, Pereira J, Costa NV, Duarte M, Oliveira AG. Medium- and long-term outcome of prostate artery embolization for patients with benign prostatic hyperplasia: Results in 630 patients. J Vasc Interv Radiol 2016; 27:1115-1122. [CrossRef]
- Isaacson AJ, Raynor MC, Yu H, Burke CT. Prostatic artery embolization using Embosphere microspheres for prostates measuring 80-150 cm3: early results from a US trial. J Vasc Interv Radiol 2016, 27, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Yu SC, Cho CC, Hung EH, Chiu PK, Yee CH, Ng CF. Prostate artery embolization for complete urinary outflow obstruction due to benign prostatic hypertrophy. Cardiovasc Intervent Radiol 2017, 40, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Chen JW, Shin JH, Tsao TF, Ko HG, Yoon HK, Han KC, Thamtorawat S, Hong B. Prostatic Arterial Embolization for Control of Hematuria in Patients with Advanced Prostate Cancer. J Vasc Interv Radiol 2017, 28, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Mordasini L, Hechelhammer L, Diener P-A, Diebold J, Mattei A, Engeler D, et al. Prostatic artery embolization in the treatment of localized prostate cancer: a Bicentric Prospective Proof-of-Concept Study of 12 patients. J Vasc Interv Radiol 2018; 29:589–97.
- Ray AF, Powell J, Speakman MJ, Longford NT, DasGupta R, Bryant T, Modi S, Dyer J, Harris M, Carolan-Rees G, Hacking N. Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity-matched comparison with transurethral resection of the prostate (the UK-ROPE study). BJU Int 2018; 122:270-282.
- Abt D, Hechelhammer L, Müllhaupt G, Markart S, Güsewell S, Kessler TM, Schmid HP, Engeler DS, Mordasini L. Comparison of prostatic artery embolisation (PAE) versus transurethral resection of the prostate (TURP) for benign prostatic hyperplasia: randomised, open label, non-inferiority trial. BMJ 2018 Jun 19; 361:k2338. [CrossRef]
- Maclean D, Harris M, Drake T, Maher B, Modi S, Dyer J, Somani B, Hacking N, Bryant T. Factors predicting a good symptomatic outcome after prostate artery embolisation (PAE). Cardiovasc Intervent Radiol 2018; 41:1152–1159.
- Salem R, Hairston J, Hohlastos E, Riaz A, Kallini J, Gabr A, Ali R, Jenkins K, Karp J, Desai K, Thornburg B, Casalino D, Miller F, Hofer M, Hamoui N, Mouli S. Prostate artery embolization for lower urinary tract symptoms secondary to benign prostatic hyperplasia: results from a prospective FDA-approved investigational device exemption study. Urology 2018; 120:205–210.
- Franiel T, Aschenbach R, Trupp S, Lehmann T, von Rundstedt FC, Grimm MO, Teichgräber U. Prostatic Artery Embolization with 250-μm Spherical Polyzene-Coated Hydrogel Microspheres for Lower Urinary Tract Symptoms with Follow-up MR Imaging. J Vasc Interv Radiol 2018 Aug;29(8):1127-1137. [CrossRef]
- Brown N, Walker D, McBean R, Pokorny M, Kua B, Gianduzzo T, Dunglison N, Esler R, Yaxley J. Prostate artery Embolisation Assessment of Safety and feasibilitY (P-EASY): a potential alternative to long-term medical therapy for benign prostate hyperplasia. BJU Int 2018 Nov;122 Suppl 5:27-34. [CrossRef]
- Pisco J, Bilhim T, Costa NV, Ribeiro MP, Fernandes L, Oliveira AG. Safety and Efficacy of Prostatic Artery Chemoembolization for Prostate Cancer-Initial Experience. J Vasc Interv Radiol 2018 Mar;29(3):298-305. [CrossRef]
- Thulasidasan N, Kok HK, Elhage O, Clovis S, Popert R, Sabharwal T. Prostate artery embolisation: an all-comers, single-operator experience in 159 patients with lower urinary tract symptoms, urinary retention, or haematuria with medium-term follow-up. Clin Radiol 2019 Jul; 74(7):569.e1-569.e8. [CrossRef]
- Malling B, Røder MA, Lindh M, Freveri S, Brasso K, Lönn L. Palliative prostate artery embolisation for prostate cancer: a case series. Cardiovasc Intervent Radiol 2019; 42:1405-1412.
- Rampoldi A, Barbosa F, Secco S, Migliorisi C, Galfano A, Prestini G, Harward SH, Di Trapani D, Brambillasca PM, Ruggero V, et al. Prostatic Artery Embolization as an Alternative to Indwelling Bladder Catheterization to Manage Benign Prostatic Hyperplasia in Poor Surgical Candidates. Cardiovasc Interv Radiol 2017; 40:530–536. [CrossRef]
- Peacock J, Sikaria D, Maun-Garcia L, Javedan K, Yamoah K, Parikh N. A Proof-of-Concept Study on the Use of Prostate Artery Embolization Before Definitive Radiation Therapy in Prostate Cancer. Adv Radiat Oncol 2020 Nov 21;6(3):100619. [CrossRef]
- Insausti I, Saez de Ocariz A, Galbete A, Capdevila F, Solchaga S, Giral P, et al. Randomized Comparison of Prostatic Artery Embolization versus Transurethral Resection of the Prostate for Treatment of Benign Prostatic Hyperplasia. J Vasc Interv Radiol 2020 Jun; 31(6):882-890. [CrossRef] [PubMed]
- Tapping CR, Little MW, Macdonald A, Mackinnon T, Kearns D, Macpherson R, Crew J, Boardman P. The STREAM Trial (Prostatic Artery Embolization for the Treatment of Benign Prostatic Hyperplasia) 24-Month Clinical and Radiological Outcomes. Cardiovasc Intervent Radiol 2021 Mar;44(3):436-442. [CrossRef]
- Saro H, Solyman MTh, Zaki M, Hasan NMA, Thulasidan N, Clovis S, Elhage O, Popert R, Sabharwal T. Prostate Artery Embolization in Patients above Eighty Years Old: Clinical Efficacy and Safety. Arab J Intervent Radiol 2022; 6:63–71.
- Insausti I, Galbete A, Lucas-Cava V, et al. “Prostatic artery embolization (PAE) using polyethylene glycol microspheres: safety and efficacy in 81 patients”. Cardiovasc Interv Radiol 2022; 45 (9):1339–1348.
- Picel AC, Hsieh TC, Shapiro RM, Vezeridis AM, Isaacson AJ. Prostatic Artery Embolization for Benign Prostatic Hyperplasia: Patient Evaluation, Anatomy, and Technique for Successful Treatment. RadioGraphics 2019; 39(5):1526–1548.
- Carbone DJ, Hodges S. Medical therapy for benign prostatic hyperplasia: sexual dysfunction and impact on quality of life. Int J Impot Res 2003; 15:299–306.
- Wang MQ, Guo LP, Zhang GD, Yuan K, Li K, Duan F, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms due to large (> 80 mL) benign prostatic hyperplasia: results of midterm follow-up from Chinese population. BMC Urology 2015; 15:33.
- Delgal A, Cercueil JP, Koutlidis N, Michel F, Kermarrec I, Mourey E, Cormier L, Krausé D, Loffroy R. Outcome of transcatheter arterial embolization for bladder and prostate hemorrhage. J Urol 2010, 183, 1947–1953. [Google Scholar] [CrossRef]
- Marszalek M, Ponholzer A, Rauchenwald M, Madersbacher S. Palliative transurethral resection of the prostate: functional outcome and impact on survival. BJU Int 2007; 99:56–9.
- Williams SG, Aw Yeang HX, Mitchell C, Caramia F, Byrne DJ, Fox SB, Haupt S, Schittenhelm RB, Neeson PJ, Haupt Y, Keam SP. Immune molecular profiling of a multiresistant primary prostate cancer with a neuroendocrine-like phenotype: a case report. BMC Urol 2020; 20(1):171. [CrossRef]
- Kably IM, Bhatia SS, Narayanan G. Prostatic Artery Embolization for Intractable Hematuria in Prostate Cancer. Intervent Oncol 360 2015, 3, E30–E35.
- Deng L, Li C, He Q, Huang C, Chen Q, Zhang S, Wang L, Gan Y, Long Z. Superselective Prostate Artery Embolization for Treatment of Severe Haematuria Secondary to Rapid Progression of Treatment-Induced Neuroendocrine Prostate Cancer: A Case Report. Onco Targets Ther 2022; 15:67-75. [CrossRef]
- Nerli RB, Adhikari P, Mulimani N, Bidi S, Rangrez S, Chandra S, Ghagane SC. Prostate Artery Embolisation as a Palliative Care in a Patient with Prostate Cancer: A Case Report. Oncology Case Reports 2020. [CrossRef]
- Parikh N, Keshishian E, Manley B, Grass GD, Torres-Roca J, Boulware D, Feuerlein S, Pow-Sang JM, Bagla S, Yamoah K, Bhatia S. Effectiveness and safety of prostatic artery embolization for the treatment of lower urinary tract symptoms from benign prostatic hyperplasia in men with concurrent localized prostate cancer. J Vasc Interv Radiol 2021, 32, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- Tapping CR, Crew J, Proteroe A, Boardman P. Prostatic artery embolization (PAE) for prostatic origin bleeding in the context of prostate malignancy. Acta Radiol Open 2019; 8(6):2058460119846061. [CrossRef]
- Bhatia S, Harward SH, Sinha VK, Narayanan G. Prostate Artery Embolization via Transradial or Transulnar versus Transfemoral Arterial Access: Technical Results. J Vasc Interv Radiol 2017 Jun;28(6):898-905. [CrossRef]
- Gil R, Shim DJ, Kim D, Lee DH, Kim JJ, Lee JW. Prostatic Artery Embolization for Lower Urinary Tract Symptoms via Transradial Versus Transfemoral Artery Access: Single-Center Technical Outcomes. Korean J Radiol 2022 May;23(5):548-554. [CrossRef]
Figure 1.
Prostate arteries (PAs) have common origins and anastomoses with feeding arteries of critical pelvic structures: understanding prostatic arterial supply is necessary to predict non-target embolization risk. IIA = internal iliac artery, ATIIA = anterior trunk internal iliac artery, PTIIA = posterior trunk internal iliac artery, SVA = superior vesical artery, OA = obturator artery, IPA = internal pudendal artery; in red are signed the type I–IV PA origin.
Figure 1.
Prostate arteries (PAs) have common origins and anastomoses with feeding arteries of critical pelvic structures: understanding prostatic arterial supply is necessary to predict non-target embolization risk. IIA = internal iliac artery, ATIIA = anterior trunk internal iliac artery, PTIIA = posterior trunk internal iliac artery, SVA = superior vesical artery, OA = obturator artery, IPA = internal pudendal artery; in red are signed the type I–IV PA origin.
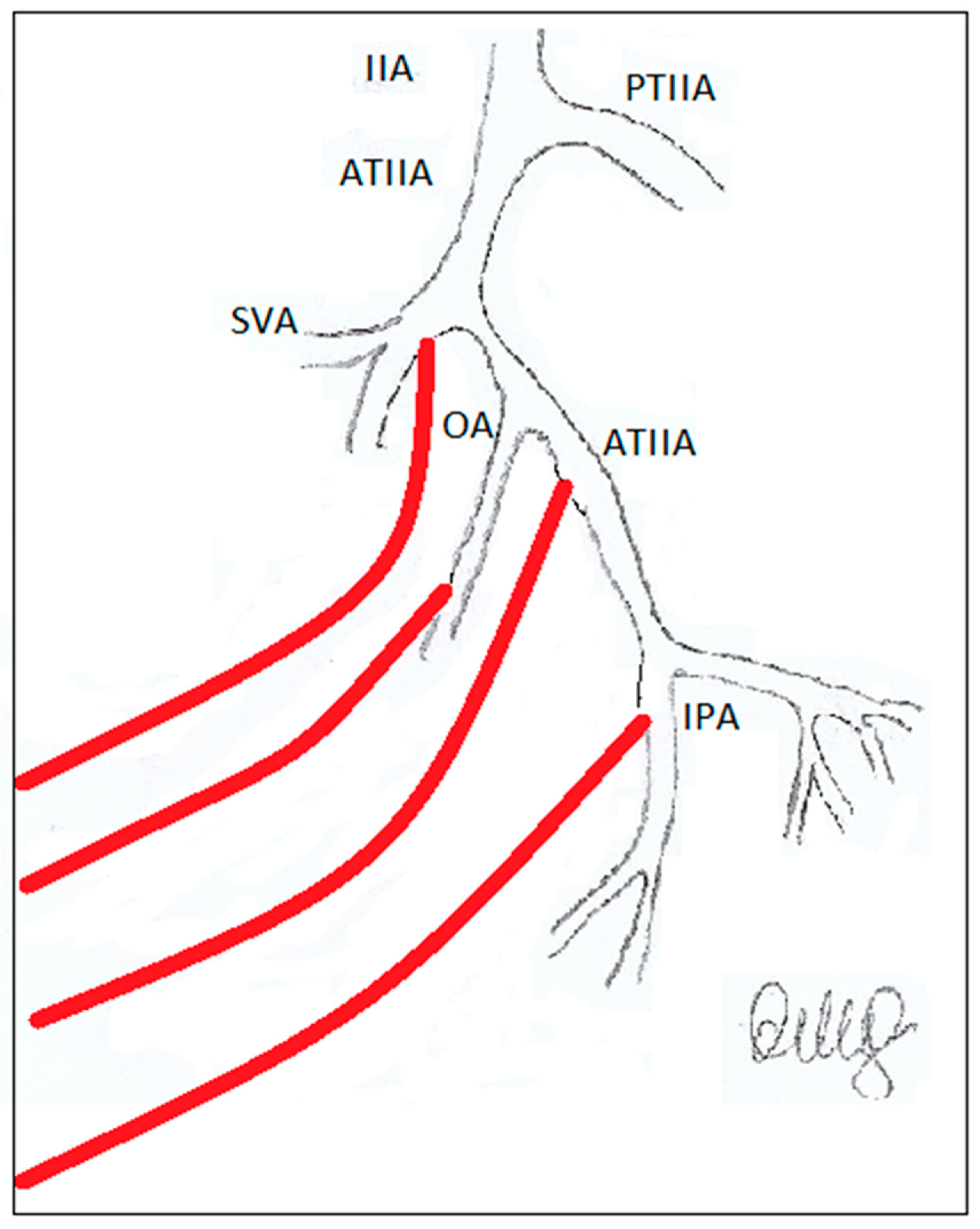
Figure 2.
PRISMA flow chart diagram.
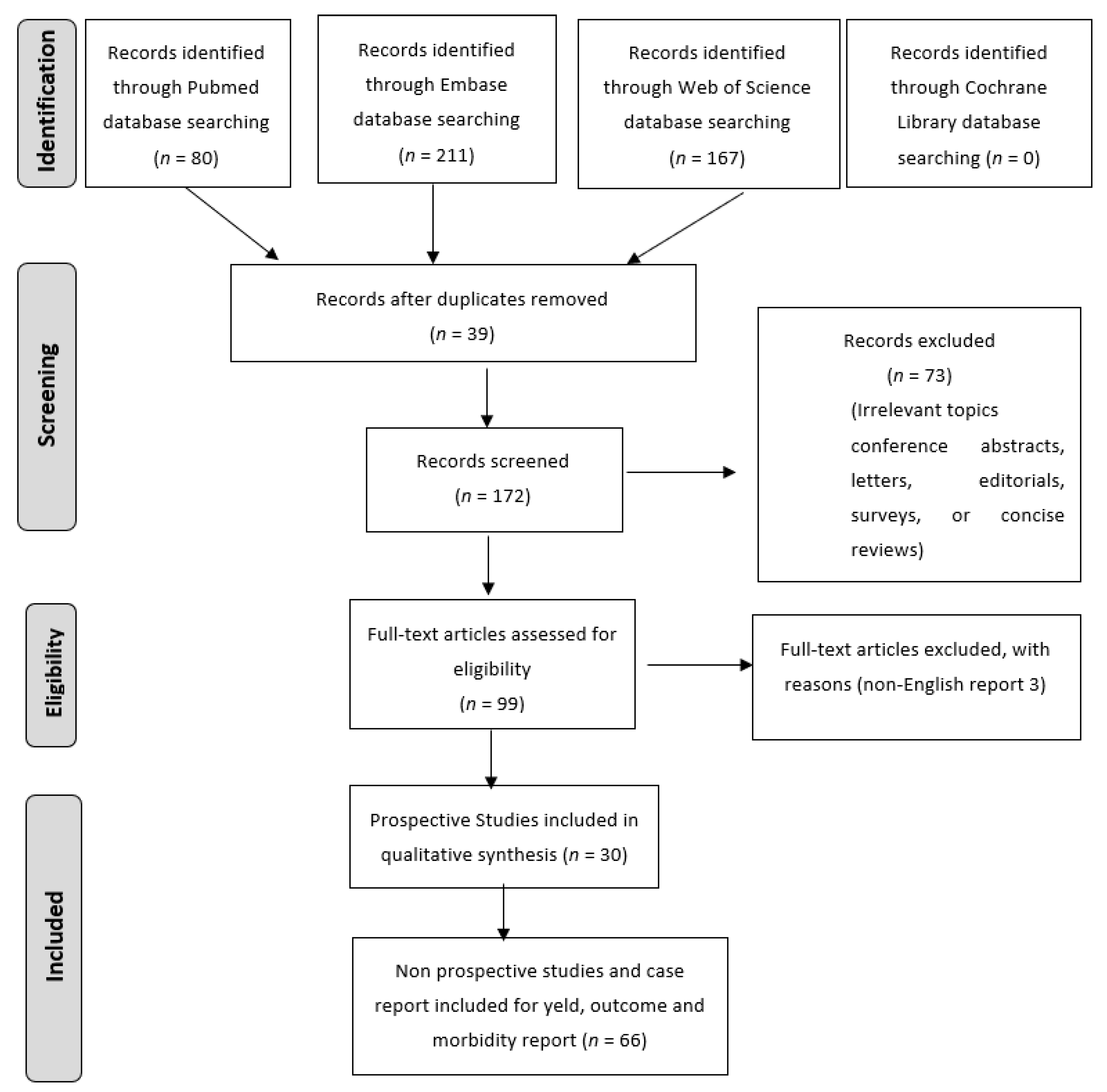
Figure 3.
AngioCT 3D, A frontal view, B right oblique anterior view; the empty right arrows indicate the bladder where inside the huge tumoral mass demonstrating hypervascular staining in red. The patient specific 3D models were displayed using ARTICOR® (Artiness srl, Milano, Italy) and obtained using a marching cube algorithm.
Figure 3.
AngioCT 3D, A frontal view, B right oblique anterior view; the empty right arrows indicate the bladder where inside the huge tumoral mass demonstrating hypervascular staining in red. The patient specific 3D models were displayed using ARTICOR® (Artiness srl, Milano, Italy) and obtained using a marching cube algorithm.
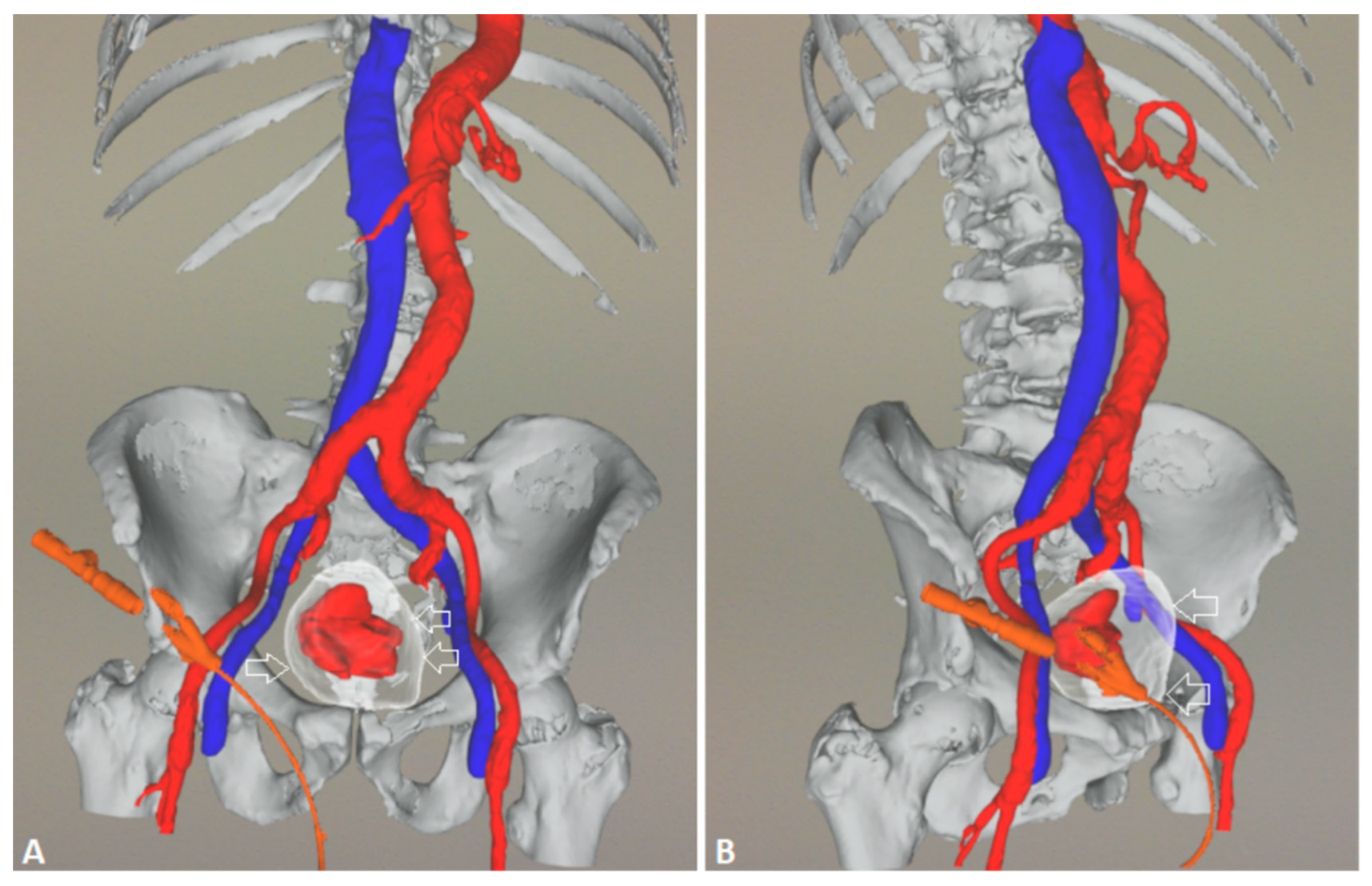
Figure 4.
Pelvic angiography to evaluate the iliac vessels: a 5F sheath is placed in the right common femoral artery under local anesthesia.
Figure 4.
Pelvic angiography to evaluate the iliac vessels: a 5F sheath is placed in the right common femoral artery under local anesthesia.

Figure 5.
A 5F pigtail catheter is advanced into the abdominal aorta to the level of the iliac bifurcation and then the left prostatic artery is selected; DSA (digital subtraction angiography) image following super selective microcatheterization of the left prostatic artery which appears hypertrophied and is seen arising from the anterior division of the internal iliac artery via a common vesicoprostatic trunk; note extravasation of contrast medium from branches of the left prostatic artery before treatment.
Figure 5.
A 5F pigtail catheter is advanced into the abdominal aorta to the level of the iliac bifurcation and then the left prostatic artery is selected; DSA (digital subtraction angiography) image following super selective microcatheterization of the left prostatic artery which appears hypertrophied and is seen arising from the anterior division of the internal iliac artery via a common vesicoprostatic trunk; note extravasation of contrast medium from branches of the left prostatic artery before treatment.
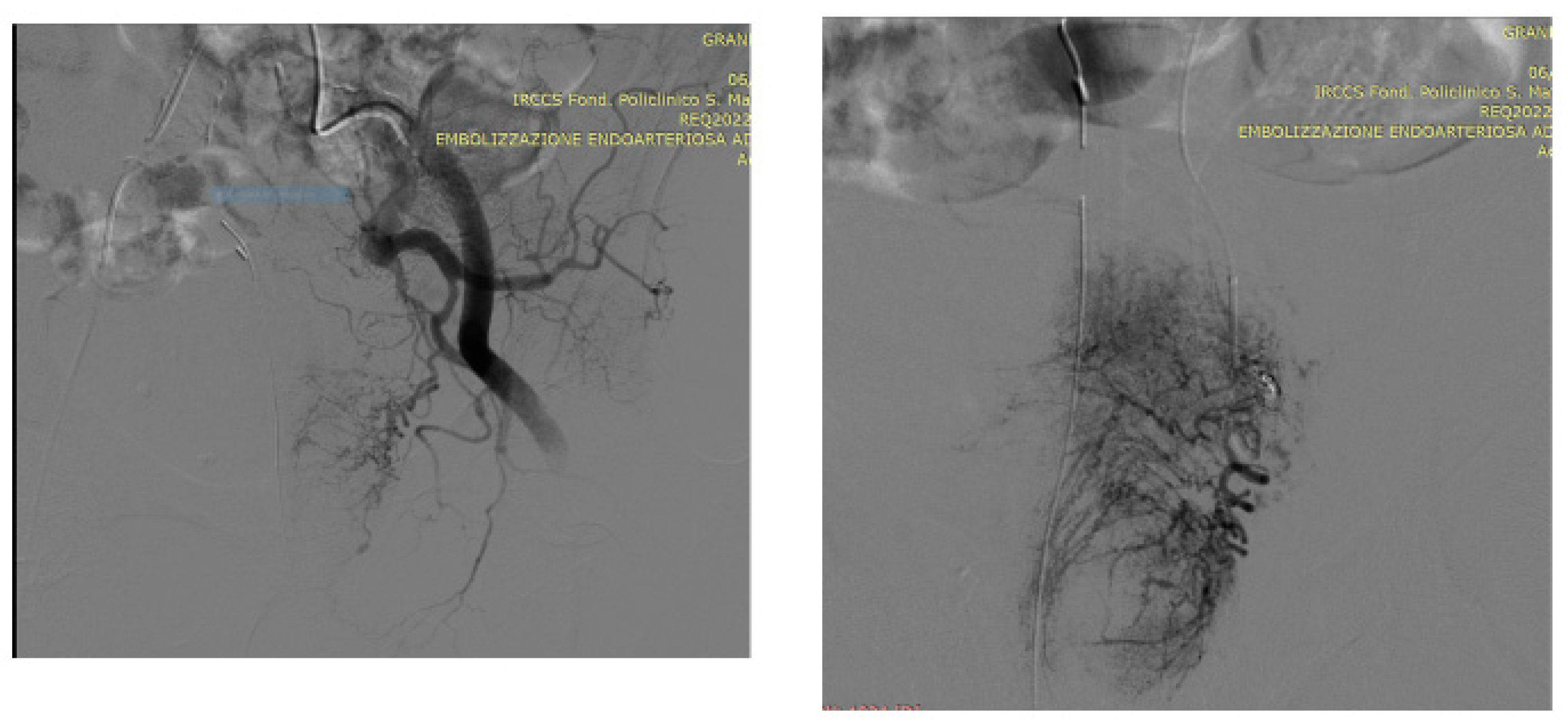
Figure 6.
Left prostatic artery embolization (PAE) performed using the standard proximal embolization first, followed by the distal (PErFecTED) technique [26]; PAE was obtained by injecting a solution of microbeads (Embosphere 300-500 μm, Merit Medical) mixed with 9ml of saline and 9 ml of contrast medium.
Figure 6.
Left prostatic artery embolization (PAE) performed using the standard proximal embolization first, followed by the distal (PErFecTED) technique [26]; PAE was obtained by injecting a solution of microbeads (Embosphere 300-500 μm, Merit Medical) mixed with 9ml of saline and 9 ml of contrast medium.
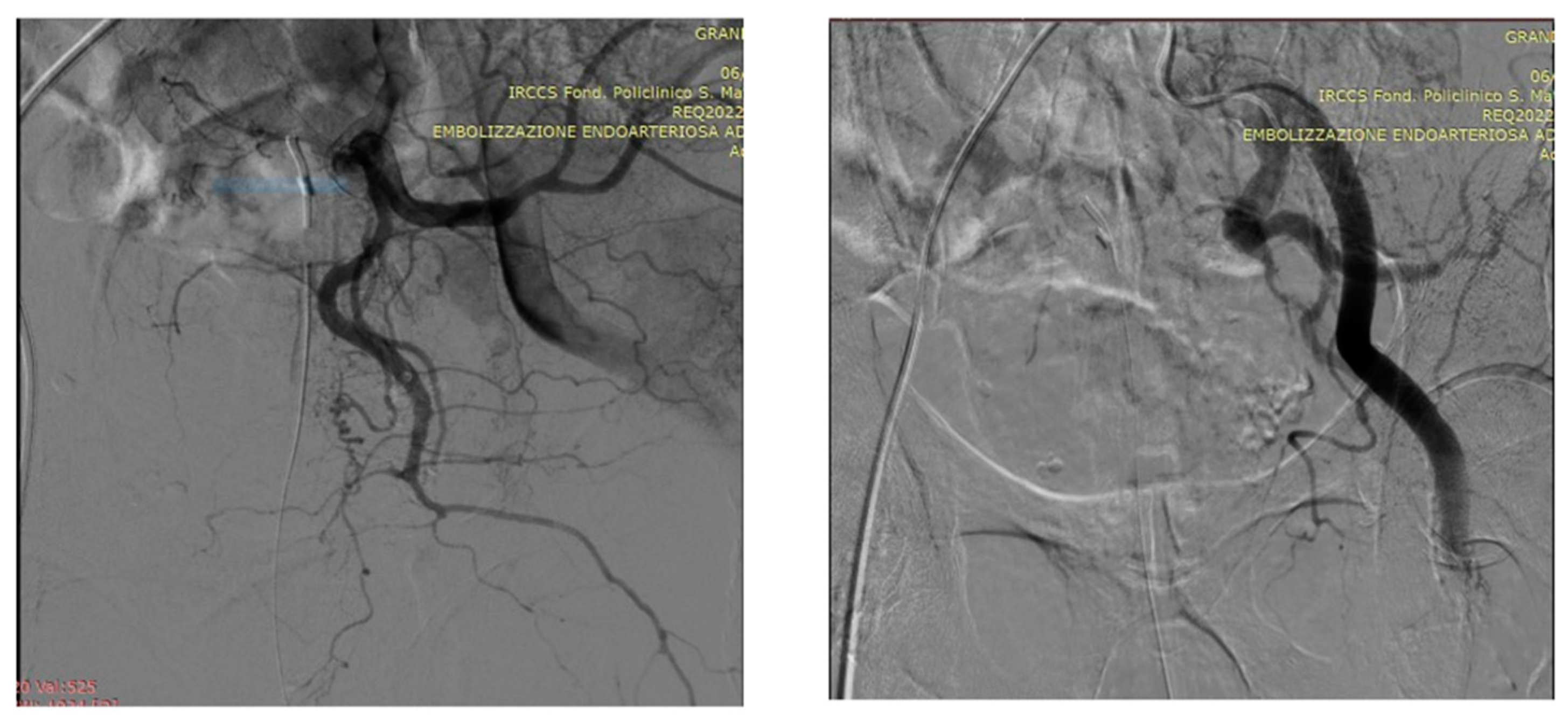
Figure 7.
DSA (digital subtraction angiography) image following super selective microcatheterization of the right prostatic artery appearing extremely hypertrophied.
Figure 7.
DSA (digital subtraction angiography) image following super selective microcatheterization of the right prostatic artery appearing extremely hypertrophied.
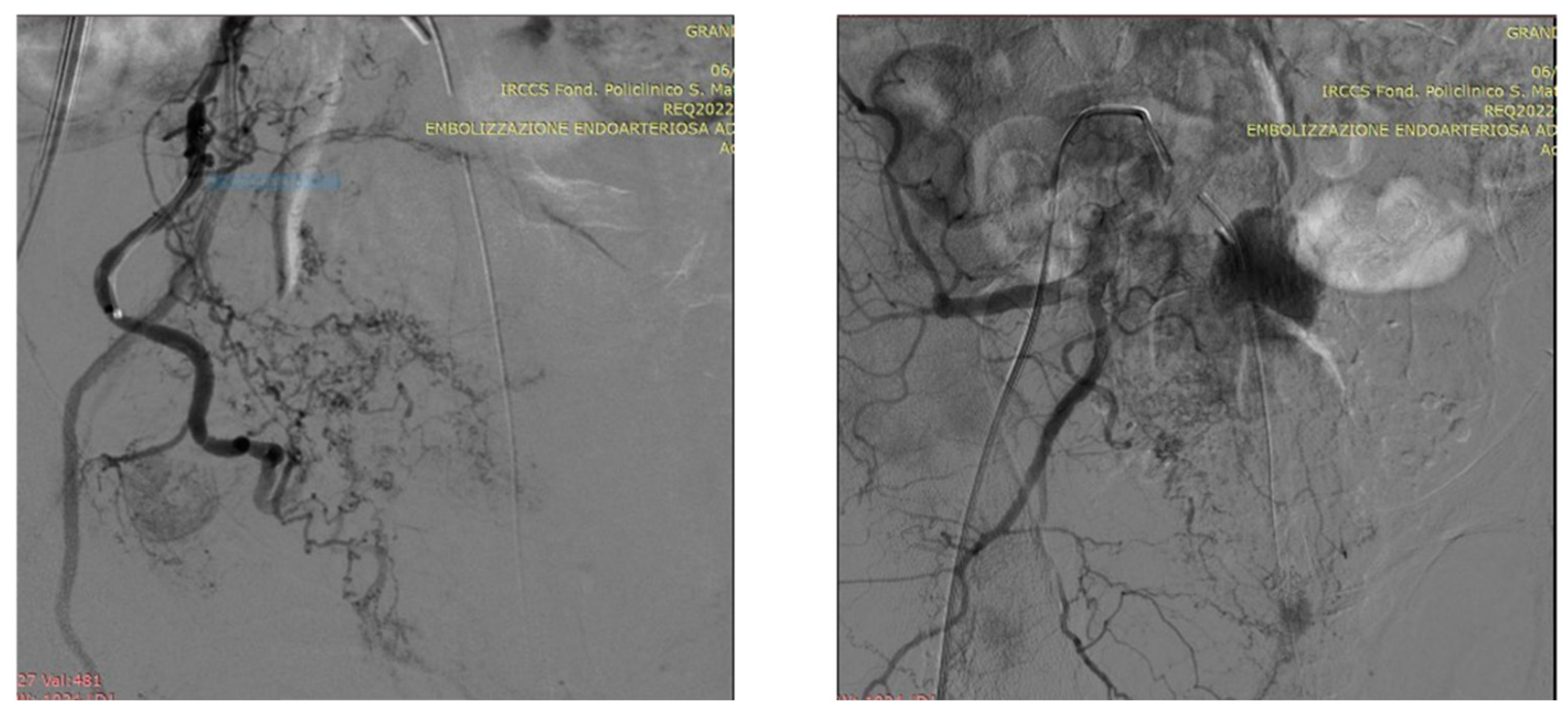
Figure 8.
Right PAE result.
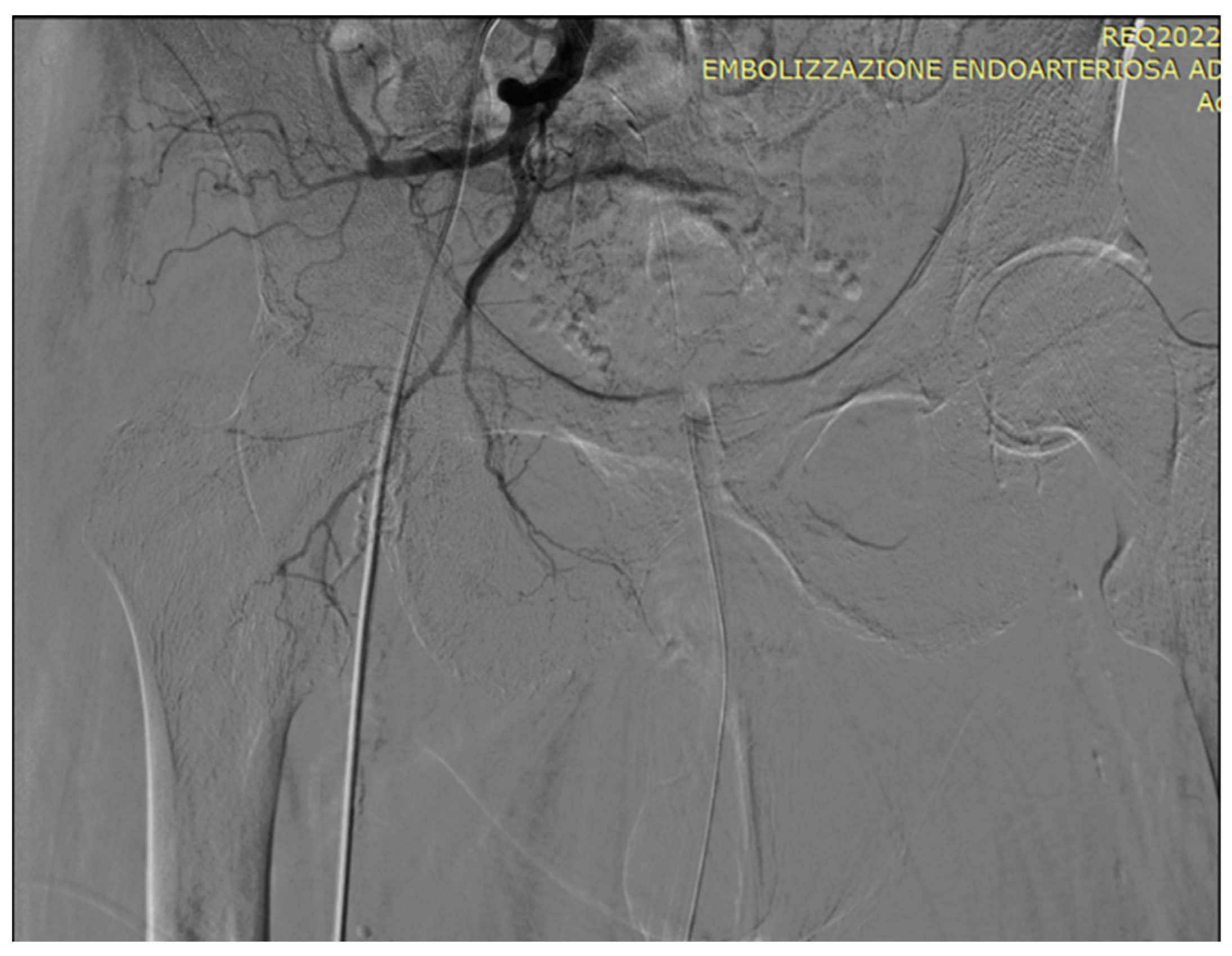

Table 1.
comparative, prospective studies in prostatic artery embolization (PAE) reporting: the name of the first Author, the year of the study, the region where the study was performed, the age and number of patients treated, the material used for angioembolization, outcomes of patients, and relevant points highlighted by the Authors. Legenda: IPSS =International Prostate Symptom Score, FU = follow-up, TS = technical success, CF = clinical failure, CS = clinical success, COMP/PROSP = comparative/prospective study, OP = open prostatectomy, BIL = bilateral, UNI = unilateral, ATH = atherosclerosis, HEM = hematuria, UI = urinary infection, UR = urinary retention, AUR = acute urinary retention, M = months, UB = urethra burning, PV = prostate volume, PVR = post-void residual, IIEF = international index erectile function, QoL = quality of life, ED = erectile dysfunction, EF = ejection fraction, FAD = femoral artery dissection, PES = post-embolization syndrome, HS = hospital stay, IBC = indwelling bladder catheter, RHOPA = refractory hematuria of prostatic origin, MRI = magnetic resonance imaging, PSH = puncture size hematoma, DYS = dysuria, HEMS = hemospermia, PACE = prostatic artery chemoembolization, HT = hormonal therapy, HTR = hormone therapy resistant, IHD = ischemic heart disease, SDYS = sexual dysfunction, BF = biochemical failure, BS = biochemical success, MOF = multiorgan failure, PK = peak flow, NK = no known, RI = respiratory insufficiency, RT = radiotherapy.
Table 1.
comparative, prospective studies in prostatic artery embolization (PAE) reporting: the name of the first Author, the year of the study, the region where the study was performed, the age and number of patients treated, the material used for angioembolization, outcomes of patients, and relevant points highlighted by the Authors. Legenda: IPSS =International Prostate Symptom Score, FU = follow-up, TS = technical success, CF = clinical failure, CS = clinical success, COMP/PROSP = comparative/prospective study, OP = open prostatectomy, BIL = bilateral, UNI = unilateral, ATH = atherosclerosis, HEM = hematuria, UI = urinary infection, UR = urinary retention, AUR = acute urinary retention, M = months, UB = urethra burning, PV = prostate volume, PVR = post-void residual, IIEF = international index erectile function, QoL = quality of life, ED = erectile dysfunction, EF = ejection fraction, FAD = femoral artery dissection, PES = post-embolization syndrome, HS = hospital stay, IBC = indwelling bladder catheter, RHOPA = refractory hematuria of prostatic origin, MRI = magnetic resonance imaging, PSH = puncture size hematoma, DYS = dysuria, HEMS = hemospermia, PACE = prostatic artery chemoembolization, HT = hormonal therapy, HTR = hormone therapy resistant, IHD = ischemic heart disease, SDYS = sexual dysfunction, BF = biochemical failure, BS = biochemical success, MOF = multiorgan failure, PK = peak flow, NK = no known, RI = respiratory insufficiency, RT = radiotherapy.
| Author year | Country | Type study | N.° | Age, mean | Particles μm |
Results | Compl./notes |
|---|---|---|---|---|---|---|---|
| Pisco [11] 2013 | Portugal | PROSP in BPH LUTS refractory to medical therapy | 89 | 74.1 | 180-300 | TS 97% 86/89. FU 12 M. At 1 M IPSS, QoL, PVR, IIEF improved, all p<0.01. |
1 bladder wall necrosis that needed surgery |
| Bilhmt [19] 2013 | Portugal | PROSP in BPH to verify particle size effects 100 μm (A) vs 200 μm (B) | 80 | 63.9 | 100-200 | FU 6 M. No significant differences were found in pain scores. A had a greater ↓ in PV (8.75 cm3 p<0.13), PSA level (2.09 ng/mL p <0.001); B had greater ↓ in IPSS (3.64 points p<0.052) and QoL (0.57 points p<0.07). | No significant differences were found in adverse events between 2 groups. |
| Gao [20] 2014 | China | COMP/PROSP in BPH LUTS PAE/TURP | PAE57 TURP57 | 67.7 66.4 | 355-500 | TS TURP 100% PAE 94.7%, CF 3.9%/9.4%. FU 24 M. IPSS, QoL, Qmax, PVR, PV, PSA had significant improvements in both groups. | TURP had greater improvements in IPSS, QoL, Qmax, and PVR at 1 and 3 M, and greater ↓ in PSA and PV when compared with the PAE group (P <0.05). |
| Kurbatov [21] 2014 | Italy Russia | PROSP in BPH | 88 | 66.4 | NK | FU 12 M | IPSS QoL Qmax PVR PV p<0.05 |
| Bagla [22] 2014 | U.S.A. | PROSP in BPH | 20 | 66.6 | PROSP in BPH LUTS | TS 90%, 10% due to ATH, Significant ↓ IPSS QoL | No minor/major compl. |
| Russo [23] 2015 | Italy Russia | COMP/PROSP PAE/OP | 80 | 67 | 300-500 | FU 12 M OP had lower IPSS p<0.05, PVR lower p<0.05, higher PF p<0.01; PAE showed higher Hb, shorter HS and IBC time. | PAE could be a feasible minimally invasive technique but failed to demonstrate superiority to OP because of the increased risk of persistent symptoms and low PF after 1 year. |
| de Assis17 2015 | Brazil | PROSP in BPH LUTS in PV > 90 g | 35 | 64.8 | NK | FU 3 M: mean PV ↓ from 135.1 g to 91.9 g p<0.0001, IPSS and QoL improved p<0.001. | A significant negative correlation was observed between PSA at 24 h after PAE and IPSS 3 months after PAE (P = .0057): excessively elevated PSA within 24 h is associated with lower IPSS. |
| Li [24] 2015 | China | 24 | 74.5 | 50-100 | TS 92% Bil 86%, UNI 14% due to ATH IPSS QoL PVR p<0.002 PV p<0.001 |
No major complications. AUR 32% HEM 14% UB 36% |
|
| Carnevale [25] 2016 | Brazil | COMP/PROSP in BPH TURP/PAE/Perf | PAE15 Perf15 TURP15 |
63.5 60.4 66.4 |
NK | IPSS, QoL, PV and Qmax significantly improved. TURP and Perf both had significantly lower IPSS than PAE but not significantly different from one another. TURP had significantly higher Qmax and smaller PV but required spinal anesthesia and ↑ HS. | Perf = Perfected Proximal Embolization First, Then Embolize Distal [26] |
| Wang [27] 2016 | China | COMP/PROSP 2 groups for mean PV: A 129 / B 64 ml |
115 | 71.5 | 100 | TS A 93.8% B 96.8%. FU 12 M. Better outcome in larger PV | IPSS QoL Qmax PVRV IIEF PSA PV significantly improved in both groups. |
| Gabr [28] 2016 | Saudi Arabia | PROSP in BPH LUTS UR and IBC | 22 | 72.5 | 300-500 | TS 100% | FU 9 M: IPSS Qmax PV PSA p<0.001 No major compl. |
| Pisco [29] 2016 | Portugal | PROSP in BPH LUTS refractory to therapy | 630 | 65.1 | NK | TS 98.1% BIL 92.6% UNI 7.4% Clinical success rates at 1-3 y and 3-6.5 y were 81.9% and 76.3% | IPSS QoL Qmax PV PSA IIEF PVR p<0.001 |
| Isaacson [30] 2016 | U.S.A. | PROSP BPH LUTS | 12 | 69 | NK | TS 100%. FU 3 M: mean improvements in IPSS and QoL were 18.3 points (5–27) and 3.6 points (1–6), respectively. | 7 cases transfemoral access, 5 cases transradial access. No major compl., no ischemic injuries. |
| Yu [31] 2017 | China | COMP/PROSP in BPH PAE in AUR and IBC weaning vs relieving LUTS without AUR | 27 | 66 | 100-300 | PAE BIL 100% IBC removed in 14/16 87.5% | Outcome comparable to cases without AUR No periprocedural compl. |
| Chen [32] 2017 | Korea Taiwan | PROSP in PCa stage 4 Refractory HEM | 9 | 71.9 | NK | FU 3 M: 2 recurrent HEM, 4 died no PAE related, 3 no HEM | No complications |
| Mordasini [33] 2018 |
Switerland | Prosp to provide PAE tumoricidal effect in PCa patients | 12 | 45-75 | 100 | Complete necrosis in 2, partial in 5, viable cancer cells in all 12 | Partial bladder wall necrosis in 2 requiring surgery |
| Ray [34] 2018 | UK | COMP/PROSP in BPH PAE/TURP | PAE216 TURP89 | 66 |
NK | PAE is clinically effective, producing a median 10-point IPSS improvement from baseline at 12 M while TURP has a median 15-point improvement. TURP HS is significantly longer than PAE. | PAE compl.: sepsis 1, blood transfusion 1, FAD 4, PSH 4, penil ulcers 2. PAE provides significant improvement in IPSS and QoL, although some of these improvements are greater in the TURP arm. |
| Abt [35] 2018 | Switzerland | COMP/PROSP BPH PAE 48 / TURP 51 | 99 | PAE 65.7 TURP 66.1 | 250-400 | FU 3 M: PAE and TURP show similar results | PAE BIL 75% UNI 25% PAE HS 2.2 / TURP HS 4.2 p <0.001 |
| Maclean [36] 2018 | UK | PROSP in BPH to study clinical outcome PAE and PV | 86 | 64.9 | NK | UNI/BIL TS% 100/96.5 |
No major compl. Initial PV and %PV reduction at 3 M predict good clinical outcomes at 12 M. |
| Salem [37] 2018 | U.S.A. | PROSP in BPH LUTS | 45 | 67 | NK | FU at 1-3-6-12 M IPSS QoL Qmax p<0.001 PVR at 6 M p 0.02, at 12 M p 0.025; PV ↓ p 0.001 | Minor compl.: dysuria 13, HEM 6, HEMS 2, urinary frequency 3 and UR 2. |
| Franiel [38] 2018 | Germany | PROSP in BPH to study MRI predictors of clinical success | 30 | 66 | 250 | TS 90% 27/30 BIL in 24 (89%). Significant MRI predictors of clinical success were not identified. | FU 1-3-6 M: IPSS < 18 with ↓ > 25%, QoL score < 4 with ↓ ≥ 1, Qmax ≥ 15 mL/s and ↑ ≥ 3.0 mL/s) rates: 59% (16/27), 63% (17/27), 74% (20/27). |
| Brown [39] 2018 | Australia | PROSP in BPH LUTS (40), HEM (1), IBC (10) | 51 | 67.8 | 250 | BIL 92.2% UNI 7.8% FU 3 M: IPSS, QoL, Qmax, PV p<0.001; PVR p<0.018. 7 cases 70% had IBC removal. |
PSH 11.8%, DYS 84.3%, perineal pain 25.5%, HEMS 11.8%, fever 9.8%, 1 medial uni gluteal irritation, 1 transient rectal hemorrhagic spot. |
| Pisco [40] 2018 | Portugal | PROSP PACE in PCa staging T2N0M0, 15 refused surgery, 5 wanted to stop HT | 20 | 67.5 | 150-300 | TS 80%, 16/20. BF 18.7%, 3/16 (PSA ↓ to < 2 ng/mL followed by PSA ↑ to > 2 ng/mL within 1 month after success). BS at 12-18 M was 62.5%, 10/16. | FU 12-18 M: 1 small bladder wall necrosis removed by surgery, 2 UR, 2 SDYS, all recovered. PACE allowed a biochemical response and is a promising treatment. |
| Thulasidasan [41] 2019 | UK | PROSP to study PAE BPH LUTS or RHOPA | 159 | 70 | 100-200 | TS 98% IBC removal in 13/24 in retention. PAE controlled HEM in 12/12 RHOPA cases. | The highest baseline IPSS and reduction in PV on the 1st MRI present the most benefit from PEA. |
| Mailling [42] 2019 | Denmark | Prosp in advanced PCa LUTS 9, UR 6 cases | 11 | 75,8 | 300-500 | TS 93.3%, 1 case unsuccessful due to ATH, bilateral 10/15; IPSS reduced 12.2 points | 4 cases did not have Fu: 2 died, 1 lost, 1 not done for Ather. |
| Rampoldi [43] 2019 | Italy | PROSP in BPH, IBC in all cases | 43 | 77,9 | 300-500 | BIL 76.7%, UNI 18%, 4.7% no done for ATH. IBC removal in 80.5% | TPV reduced p<0.001 UI 3/7.5%, UR 6/14.6% |
| Peacock [44] 2020 | U.S.A. | PROSP PEA before RT in PCa LUTS | 9 | 71 | 300-500 | FU 18 M in 5 that had RT at the same center. Mean IPSS after PEA 13.8 p<0.02, mean PV ↓ was 23.1%. No BF. | PAE is a clinically significant adjunctive therapy for alleviating LUTS and achieving significant volume reduction before RT, resulting in decreased radiation-related toxicity from prostate alone RT for PCa. |
| Insausti [45] 2020 | Spain | COMP/PROSP in BPH PAE/TURP | PAE 23 TURP 22 | ? | 300-500 | FU 12 M: PAE had IPSS ↓ p<0.08 and better QoL p<0.002; PV ↓ was better in TURP p<0.001. | PAE group had fewer compl. 15/47 (TURP) p<0.001. |
| Tapping [46] 2021 | UK | PROSP in BPH symptoms refractory to medical therapy | 50 | 67 | 200-500 | TS 96% 48/50. FU 24 M. IPSS at 24 M ↓ p<0.001, PV ↓ at 3 and 12 M but not significantly different at 24 M. | Initial PV was not a good predictor of CS. |
| Saro [47] 2022 | UK | PROSP in BPH and PCa LUTS and HEM | 54 | 85.29 | 180-300 | TS 92.6%. 30 surgery was contraindicated, no possible for ATH 4. IPSS and QoL significantly improved at 12 and 24 M. PAE was successful in 19 out of 20 with IBC for UR. | 17 patients, 4 PCa, had HEM: PAE resulted in CS in 16 with immediate bleeding stoppage. PV ↓ significantly within 6 M. IBC removal successful in 16 out of 17. No intra-or postprocedural compl. were encountered. |
| Insausti [48] 2022 | Spain | PROSP in BPH LUTS refractory to therapy | 81 | 73.87 | 400±75 | TS 100% BIL 85.2% UNI 14.8%: 3 cases impossibility PA cannulation, 4 PA perfused rectum or penis, 5 ATH. CS 78.5% | FU 12 M: IPSS Q=L Qmax p<0.01, PVR <0.05 Compl. 11 cases: 3 UI 3 UR, 3 PES, 1 ED, 1 FAD. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



