
Submitted:
16 November 2023
Posted:
21 November 2023
You are already at the latest version
Abstract
Globally, the adoption of Solid Organ Transplantation (SOT) as first-line therapy for end-stage organ failure has not come without its share of complications. Enterococcal endocarditis poses a substantial risk to renal transplant patients, and multiple factors must be considered due to the grave nature of this infection. Such factors include addressing multidrug-resistant organisms, antibiotic therapy-related toxicity, and preserving the transplanted organ. Additional considerations include salvaging an affected cardiac valve and avoiding the need for a valve replacement with the attendant complications. Ampicillin and gentamicin have historically been the standard of care as first-line treatment for many years until the aminoglycoside sparing regimen of ampicillin and ceftriaxone showed non-inferiority in clinical studies. We present a second case report with an aminoglycoside sparing regimen of ampicillin and daptomycin in a renal transplant patient who developed Enterococcus faecalis endocarditis. We conclude with a brief review of published research with this combination.
Keywords:
endocarditis
; enterococcal
; daptomycin
; transplant
; ampicillin
Introduction
At the turn of the 21st century, multiple paradigm shifts occurred in various disciplines of medicine. Due to improved surgical techniques and anti-rejection therapies, solid organ transplantation (SOT) became unanimously accepted as a therapeutic option for end-stage kidney, heart, and liver organ failure. As a result, overall survival in these patients improved substantially. [1]
There were more than 948,252 SOT procedures done between 2001 and 2023 in the United States.[1] Renal transplantation, in particular, is being performed worldwide and has become the standard of care in patients progressing to end-stage renal disease (ESRD) in preference to any form of dialysis. By the end of 2023, 558,675 patients will have had a functioning transplanted kidney in the US.[2]
SOT patients are permanently at risk for many potential complications, not only in the immediate post-transplant stage but extending throughout their lifetime. Infections are always a threat given the long-term immunosuppressed state that results from anti-rejection medications. Petro et al. confirmed this observation in a comprehensive contemporary review, which noted that renal transplant patients have a significantly higher risk of infective endocarditis (IE) than other SOT patients. An extensive search of the published data has shown that the leading organisms were gram-positive in 57.4% of the cases, and among them, Enterococci were the leading cause in 26.1% of the cases.[1]
Of all the Enterococcal species, Enterococcus faecalis is the leading causative organism in endocarditis, causing 90% of all cases in the general population and all organ transplant patients. This distribution is also replicated in the renal transplant population.[3]
Enterococcal endocarditis requires prompt identification and timely implementation of effective combination antibiotic therapy to eradicate the infection and avoid damage to a transplanted kidney. Additionally, rapid identification and antibiotic therapy may avoid potential complications of cardiac valve replacement and even death.
Twentieth-century antibiotic practices have brought forth the current era of multidrug resistance, bringing the urgent need to seek alternative therapeutic options. As a result, the most recent international guidelines have included new regimens for treating Enterococcal endocarditis.[4] These regimens are both first and second-line therapies that spare the use of aminoglycosides. The most utilized aminoglycoside sparing combination is ampicillin and ceftriaxone for Enterococcus faecalis. This combination has proven equivalent to ampicillin and gentamicin in treatment outcomes without the additional well-known and established renal and ototoxicity of the aminoglycosides.[5]
In 2012, the first reported success of the combination of ampicillin and daptomycin provided a new experience with aminoglycoside sparing agents.[6] Subsequently, in 2015, a cohort of five chronic kidney disease (CKD) patients supported this regimen's efficacy for treating Enterococcus faecalis endocarditis.[7] However, when first used, the combination was met with a challenge in a kidney transplant patient in 2018.[8] Later, a retrospective study of 35 patients treated with ampicillin and daptomycin was presented at the European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) 2020.[9] This was a landmark study that spanned three countries with all subspecies of Enterococcus, including E. faecium. This was the largest registry ever compiled in literature, with results spanning the last decade.
This accumulated clinical experience supports the utilization of another promising aminoglycoside sparing regimen. We present a second case of a kidney transplant patient with Enterococcus faecalis endocarditis treated successfully with this combination. This manuscript reports this second case and reviews our experience using this combination.
Materials and Methods
Data Search
This review followed the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). We conducted a comprehensive search for eligible studies in PubMed and Google Scholar from their inception using the following text words: "bacterial endocarditis," "Enterococcus," and "renal transplant."
The initial search was performed on July 7, 2023, and the final search was conducted on July 28, 2023. Consequently, all studies identified and published before July 28, 2023, were considered for inclusion.
Study selection
Included in the analysis were studies that met the following criteria:
- Published in English.
- Studies that reported data on patients' clinical characteristics, microbiology, treatment, and outcomes.
- Published in 2015 or later.
The following studies were excluded from the analysis.
- Those considered secondary research papers, such as reviews, or did not report results on primary research.
- Studies which were conducted on non-human subjects.
- Studies that were conducted on patients who had not undergone transplantation.
- Studies not written in English.
To ensure rigorous study selection, two investigators (CB and GL) independently reviewed the titles and abstracts of the resulting references. Subsequently, they retrieved and rescreened the full-text publications of potentially relevant articles. The final selection of studies was based on consensus. References of the included studies were also examined for additional relevant articles.
Study Outcomes
The main objectives of the study were the following:
- Document the epidemiological characteristics of kidney transplant recipients with infective endocarditis (IE).
- Examine the clinical characteristics of the patients involved in the study.
- Document the treatment methods used for Enterococcal IE.
- Assess the clinical cure outcomes in the patients under investigation.
Data Extraction and Definitions
Two investigators (CB and GL) extracted data from each eligible study. The extracted information encompassed study details such as type, year of publication, and country. It also included patient demographic data, such as age and gender, and relevant medical history (time after transplantation). The data also covered microbiological aspects, the treatment administered for IE, and whether the treatment outcome was cure or death.
Ethics Statement
Written consent of the patient and IRB approval was obtained.
Case Report
The patient is a 45-year-old African American female who works as a correctional officer with a significant medical history of lupus-associated nephropathy requiring hemodialysis before receiving a second renal transplant in 2017. Additional comorbidities include hypertension, diabetes mellitus, and construction of arteriovenous shunt. The patient has had anaphylaxis with associated angioedema to levofloxacin. Current medications included tacrolimus 3 mg PO BID and prednisone 5 mg PO daily. The patient was in her usual state of health until she presented on October 16, 2022, to the emergency department (ED) with diarrhea that had onset two days before the initial consultation. The diarrhea was not described as bloody or associated with vomiting or abdominal pain. She denied recent travel, contact with sick individuals, or antibiotic use. A review of the systems was positive for fever, muscle aches, nasal congestion, and headache. Vital signs at the consultation showed a blood pressure (BP) of 140/75, a heart rate (HR) of 112, and an oral temperature of 100.9 F. The initial cardiac examination was routine; specifically, there were no murmurs. Examination of the lungs and abdomen was also unremarkable.
A complete workup, including blood cultures, was performed. The chest x-ray report mentioned cardiomegaly with mild bibasilar pulmonary opacities. An abdominal computed tomography (CT) scan revealed no acute intra-abdominopelvic abnormalities. Automated complete blood count (CBC) showed a white blood cell (WBC) count of 11,560 cells/mm3 (range: 4,800- 10,800), neutrophils 79.6% (range: 50- 75%), and lymphocytes 8.10% (range: 20- 40%). Hemoglobin level was 13.2 g/dl (range 11.5- 16.0), and platelet count was mildly decreased at 129,000 per cubic mm (range: 130,000 – 400,000). A complete metabolic panel (CMP) revealed increased creatinine levels at 2.81 mg/dl (range: 0.57- 1.11), and blood urea nitrogen (BUN) levels were 36 mg/dl (range: 7-20). Urinalysis showed increased urine WBC of 6-10 (range: 0-2) and the presence of red blood cells and proteinuria 2+. (Figure 1) Due to her stable condition, the patient was discharged with oral cephalexin 500 mg every 6 hours (PO) for seven days due to possible urinary tract infection and acute viral rhinitis with frontal sinusitis.
A day later, the patient was asked to return to the ED due to a positive blood culture for Enterococcus faecalis. The patient was admitted to the hospital and initially started on intravenous vancomycin 1.25 g IV push. Upon admission, a transthoracic echocardiogram was performed, which revealed aortic sclerosis and trace mitral regurgitation. Endocarditis could not be ruled out, which prompted initiating antibiotic coverage with ampicillin/sulbactam 3 g every 12 hours intravenously (IV). The physical examination was positive for a systolic murmur in the right parasternal border and a systolic murmur in the left fifth intercostal space. Axillary and inguinal lymph nodes were palpable, and trace edema was present.
The multidisciplinary team, guided by infectious disease specialists, established that the main goal was to treat the infection without causing any further damage to the renal function. A daptomycin 6 mg/kg IV regimen with ampicillin/sulbactam 3g IV was initiated. It is to be noted that this combination of ampicillin with sulbactam was given for two weeks due to lack of availability; however, for the remaining four weeks of treatment, only ampicillin was given, and it adjusted accordingly to the glomerular filtration rate (GFR). If the GFR were greater than 30, the patient would receive daptomycin every 24 hours and ampicillin every 12 hours. The duration of the treatment was determined to be six weeks. Heart valve replacement was not needed during the treatment.
Two days after consultation, the patient underwent a transesophageal echocardiogram, which confirmed the presence of a 0.7 x 0.6 cm vegetation attached to the posterior leaflet annulus of the mitral valve. (Figure 2) Eight days after the initiation of symptoms, the patient was transferred to a skilled nursing unit to continue intravenous treatment as established by infectious disease specialists.
During her hospitalization, the patient's blood work began to improve, showing a decrease in her WBC and an improvement in creatinine levels, which were reported to be 1.83 mg/dl. Six weeks later, the patient was discharged from the skilled nursing unit in stable and improved condition, thus having experienced a full recovery. At a six-month follow-up, blood cultures were negative. The patient is alive as of the writing of this manuscript and with baseline renal function a year after, at least, our last contact.
Discussion
Gram-positive bacteria comprise more than eighty percent of the pathogens responsible for native and prosthetic valve IE.[10] Traditionally, Enterococcus is the third most common microbiological agent when considered under the original classification of acute, subacute, and chronic IE. This format is intended to group the different types of IE based on clinical pathophysiological presentation and, therefore, predict the potentially infecting organism. A novel approach has proposed implementing a more practical and contemporary system based on the population studied, including categories of community-acquired, nosocomial, non-nosocomial healthcare-associated, IV drug users, prosthetic valves, pacemakers, and defibrillators.[11] When this classification is applied, Enterococcus becomes a common cause of IE in the hospital and nosocomial environments, second only to Staphylococcus.
Enterococcus is the third leading agent worldwide, accounting for nearly ten percent of the cases.[12] Moreover, Enterococci are the top causative agents of endocarditis in Transcatheter Aortic Valve Implantation (TAVI) [13] and the second leading cause of prosthetic valve endocarditis in hemodialysis-dependent patients.[3,14] Enterococcus faecalis is the most common subspecies identified, responsible for 90% of the cases.[15] E. faecium accounts for far fewer cases but is associated with hospital-acquired infections and is known for its ability to develop more excellent antibiotic resistance. New data has shown the gap closing between E. faecium and E. faecalis bacteremia, with a comparable ratio of 1:1.8, respectively.[16]
The increasing antibiotic resistance shown by Enterococcus species has highlighted the importance of gaining newer insights about different treatment options, as discussed by Nappi et al. [17] This is critical because Enterococcal IE affects the chronically ill, including those with renal, cardiac, and pulmonary disease, as well as the elderly, immunosuppressed, and SOT population. The result of prolonged immunosuppression and the increased use of invasive procedures in these populations has dramatically impacted the incidence and spectrum of opportunistic infections. Therefore, it is easy to conclude that the most affected cohort is exposed in the hospital setting, which is the perfect environment for bloodstream infections.[18]
In a landmark study that broke decades of longstanding tradition of including aminoglycosides in any combination of therapy, Fernandez-Hidalgo et al. showed the non-inferiority of ampicillin and ceftriaxone compared to ampicillin plus gentamicin for treating E. faecalis IE.[5] The median length of treatment was six weeks in both groups. Clinical outcomes were not significantly different in either group, except for the development of renal failure, which was considerably less frequent in the ampicillin plus ceftriaxone group. With ampicillin plus ceftriaxone, the clinical cure rate was 71.4 %. The success rate after three months was 67.4%, with a relapse rate of 5% and a 1-year mortality of 23.3%. These results were based on a large cohort, together with a smaller study with overlapping results by Pericàs et al. that was published later, that led to both the AHA and ESC guidelines to include ampicillin plus ceftriaxone as a first-line treatment option for E. faecalis, and the preferred choice for high-level aminoglycoside resistant (HLAR) strains.[4,19,20] Another advancement and possibility is a two-week shortened gentamicin course within the beta-lactam plus gentamicin therapeutic combination supported by non-inferiority and more extensive safety data shown in a Danish study.[21] Although considered a breakthrough in science, these results and guidelines did not come without their share of criticism.
M. Beganovic et al. has an exceptional review of 30 years of literature regarding Enterococcal endocarditis. This review emphasizes that combination therapy remains the ideal approach to reduce the high rates of morbidity and mortality observed in the past. The authors stress that critical steps are needed to encourage more research regarding this infection. In one of their conclusions, they highlight that the double beta-lactam therapy, ampicillin, and ceftriaxone combination is a refreshing strategy that spares aminoglycosides, albeit they leave the door open in the future for potential aminoglycoside sparing regimens. We refer the reader to the manuscript for complete details.[22]
Koehler et al., in a letter to the editor, wrote that the double beta-lactam combination is still up for debate. He raises reasonable concern about potentially increasing the incidence of Clostridium difficile associated colitis and the emergence of gram-negative bacteria resistance.[23]
Daptomycin is a cyclic lipopeptide antibiotic with bactericidal activity against many gram-positive bacteria, including vancomycin-resistant Enterococci (VRE).[24] This antibiotic has an unusual mechanism of action, and when combined with ampicillin, results in unexpected synergy. The mechanism of this synergy has yet to be fully understood. However, this combination seems to enhance daptomycin's bactericidal activity, [10] and the broad safety profile makes it especially appealing for patients with impaired or compromised renal function.
Thus far, the data regarding the use of daptomycin with ampicillin in clinical practice for IE is mostly case reports. [8,29] (Table 1) However, in a rabbit model, the authors recently compared the efficacy of combination therapy of daptomycin and ampicillin versus daptomycin monotherapy. Comparison was made against developed Daptomycin Non-Susceptible (DNS) strains in an experimental Enterococcal endocarditis model.[25] The study used a collection of E. faecalis strains from patients infected with IE and created an experimental endocarditis model using infected rabbits. In daptomycin-sensitive strains, the combination of daptomycin and ampicillin was significantly more effective than daptomycin alone. Daptomycin and ampicillin combination therapy was also similarly as effective as ampicillin and ceftriaxone therapy. The authors recommended that daptomycin MIC with the E-test be performed on all initial IE blood isolates to rule out DNS strains. If DNS strains were observed, it was recommended that the combination of daptomycin and ampicillin should be avoided, and ampicillin and ceftriaxone should be utilized instead due to inherent resistance.
In 2012, Sakoulas et al. reported a case of left-sided endocarditis with an ampicillin and vancomycin-resistant E. faecium that failed daptomycin and linezolid combination therapy.[26] The bacteremia, however, subsided with the combination of daptomycin and ampicillin. The patient had no septicemia within 24 hours of initiating this therapy after days of persistent bacteremia.
Sierra Hoffman et al. have published several individual cases in case series. All subjects had some degree of renal disease with a spectrum from chronic kidney disease, end-stage renal disease on hemodialysis, or temporary hemodialysis while the infection occurred. A sixth case was a kidney transplant patient who had kept her renal function within normal range for 11 years. [6,8] In all these cases, the treatment was successful when used as a primary regimen or salvage therapy, in other words, applied after failing a prior regimen or when applied as first-line treatment from the start. In all of them, the renal function was preserved in the patient with pre-existing renal disease, or in the case of a transplanted patient, the infection was eradicated. No recurrence was noted even at a one-year follow-up. We have summarized the clinical features, renal status, and outcome in Table 2, including our case report.
The findings of Pericas et al. [3] and Herrera-Hidalgos et al. [27] contemporary reviews align with our data presented in Table 2. They demonstrate that Enterococcal endocarditis is the second most prevalent cause of infective endocarditis within the chronic hemodialysis population, trailing behind only Staphylococcus aureus with percentages of 15.4% and 47.8%, respectively. It's important to note that the researchers highlight the higher occurrence of relapses compared to previous studies and an increase in both in-hospital and six-month mortality rates among hemodialysis-treated patients, reaching levels of 30.4% and 39.8%, respectively. Furthermore, individuals diagnosed with Enterococcal endocarditis tend to be older and have a greater prevalence of comorbidities. Similar patterns were observed in our limited patient group in Table 2, where all seven were associated with hemodialysis, had established chronic kidney disease, were renal transplanted patients, or were iatrogenically immunosuppressed.
Outstanding features and associations of Enterococcus species have been validated and documented in contemporary literature in the 21st century. A compilation of these findings is discussed in Table 3.
Drawbacks of daptomycin therapy include the potential side effects of rhabdomyolysis and eosinophilic pneumonitis, which could be lethal if not recognized early. Another area for improvement in the first decade of daptomycin use was the need for global access due to cost and branded formulation, which potentially favored developed countries. However, in 2023, daptomycin is now generic and universally accessible.
We need to evaluate four fundamental variables when we review the chronological universal table of Enterococcus faecalis infective endocarditis in renal transplant patients. These include curing the underlying infectious disease process, preserving the cardiac valve, preserving the kidney itself, and overall survival. When these four variables are analyzed in the 12 cases of E. faecalis in renal transplant patients that have been reported, only 9 (75%) out of those 12 meet that goal. However, it raises the question of which of the available antibiotic combinations has achieved these goals more than once. To the best of our knowledge, after reviewing data until August 2023, only the combination of daptomycin and ampicillin has achieved this feat. This unique reproducibility should send a powerful message.
Conclusions
Enterococcal endocarditis is becoming more frequent, especially with the rise in elderly patients, those with comorbidities, and healthcare-associated infections. As the population of kidney transplant patients grows, Enterococcal IE is expected to become a significant complication. Although our data is mainly observational, fate has presented us with several of the most challenging patients in the renal community. We have utilized the data available to accept the challenge successfully. It is time to consider future randomized control trials comparing available aminoglycoside sparing alternatives, which include ampicillin and daptomycin.
References
- Ioannou, P., Alexakis, K., & Kofteridis, D. P. (2021). Endocarditis in kidney transplant recipients: a systematic review. Journal of Chemotherapy, 33(5), 269–275. [CrossRef]
- Lentine, K. L., Smith, J. M., Miller, J. M., Bradbrook, K., Larkin, L., Weiss, S., Handarova, D. K., Temple, K., Israni, A. K., & Snyder, J. J. (2023). OPTN/SRTR 2021 Annual Data Report: Kidney. American Journal of Transplantation, 23(2, Supplement 1), S21–S120. [CrossRef]
- Pericàs JM, Llopis J, Muñoz P, et al. A Contemporary Picture of Enterococcal Endocarditis. J Am Coll Cardiol. 2020 Feb 11;75(5):482-494.
- Baddour, L. M., Wilson, W. R., Bayer, A. S., Fowler, V. G., Tleyjeh, I. M., Rybak, M. J., Barsic, B., Lockhart, P. B., Gewitz, M. H., Levison, M. E., Bolger, A. F., Steckelberg, J. M., Baltimore, R. S., Fink, A. M., O'Gara, P., Taubert, K. A., & null, null. (2015). Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications. Circulation, 132(15), 1435–1486. [CrossRef]
- Fernández-Hidalgo, N., Almirante, B., Gavaldà, J., Gurgui, M., Peña, C., de Alarcón, A., Ruiz, J., Vilacosta, I., Montejo, M., Vallejo, N., López-Medrano, F., Plata, A., López, J., Hidalgo-Tenorio, C., Gálvez, J., Sáez, C., Lomas, J. M., Falcone, M., de la Torre, J., … Pahissa, A. (2013). Ampicillin Plus Ceftriaxone Is as Effective as Ampicillin Plus Gentamicin for Treating Enterococcus faecalis Infective Endocarditis. Clinical Infectious Diseases, 56(9), 1261–1268. [CrossRef]
- Sierra-Hoffman, M., Iznaola, O., Goodwin, M., & Mohr, J. (2012). Combination Therapy with Ampicillin and Daptomycin for Treatment of Enterococcus faecalis Endocarditis. Antimicrobial Agents and Chemotherapy, 56(11), 6064. [CrossRef]
- Sierra-Hoffman, M., Iznaola, O., Lamp, K. C., Mohr, J. F., & Winn, R. E. (2015). Daptomycin and Ampicillin Combination for Treatment of Enterococcus faecalis Endocarditis. Infectious Diseases in Clinical Practice, 23(4). https://journals.lww.com/infectdis/fulltext/2015/07000/daptomycin_and_ampicillin_combination_for.8.aspx.
- Castro-Lainez, M. T., Sierra-Hoffman, M., Valladares, V., Tillman, T., Iznaloa-Esquivel, O. A., Howell, A., Fader, R., Winn, R., & Jinadatha, C. (2018). A rationale for combination ampicillin and daptomycin in renal transplant patients with Enterococcal infective endocarditis. IDCases, 14, e00460. [CrossRef]
- Sierra-Hoffman, M.; Deliz, R.J.; Sekhon, A.K.; Gollapalli, A.; Saddler, K.; Stevens, M.; Castro-Lainez, M.; Pericas, J.M. 2020. "A multi-national study for the treatment of Enterococcal endocarditis with Ampicillin-Daptomycin combination therapy." 30th European Congress of Clinical Microbiology and Infectious Diseases Abstract book 2020, abstract 4165, page 1993.
- Hoen B, & Duval X. (2013). Infective Endocarditis. New England Journal of Medicine, 369(8), 784–785. [CrossRef]
- Murdoch, D. R., Corey, G. R., Hoen, B., Miró, J. M., Fowler Jr, V. G., Bayer, A. S., Karchmer, A. W., Olaison, L., Pappas, P. A., Moreillon, P., Chambers, S. T., Chu, V. H., Falcó, V., Holland, D. J., Jones, P., Klein, J. L., Raymond, N. J., Read, K. M., Tripodi, M. F., … Investigators, I. C. on E. C. S. (ICE-P. (2009). Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century: The International Collaboration on Endocarditis–Prospective Cohort Study. Archives of Internal Medicine, 169(5), 463–473. [CrossRef]
- Chirouze, C., Athan, E., Alla, F., Chu, V. H., Ralph Corey, G., Selton-Suty, C., Erpelding, M.-L., Miro, J. M., Olaison, L., & Hoen, B. (2013). Enterococcal endocarditis in the beginning of the 21st century: analysis from the International Collaboration on Endocarditis-Prospective Cohort Study. Clinical Microbiology and Infection, 19(12), 1140–1147. [CrossRef]
- Regueiro, A., Linke, A., Latib, A., Ihlemann, N., Urena, M., Walther, T., Husser, O., Herrmann, H. C., Nombela-Franco, L., Cheema, A. N., le Breton, H., Stortecky, S., Kapadia, S., Bartorelli, A. L., Sinning, J. M., Amat-Santos, I., Munoz-Garcia, A., Lerakis, S., Gutiérrez-Ibanes, E., … Rodés-Cabau, J. (2016). Association Between Transcatheter Aortic Valve Replacement and Subsequent Infective Endocarditis and In-Hospital Death. JAMA, 316(10), 1083–1092. [CrossRef]
- Pericàs, J. M., Llopis, J., Jiménez-Exposito, M. J., Kourany, W. M., Almirante, B., Carosi, G., Durante-Mangoni, E., Fortes, C. Q., Giannitsioti, E., Lerakis, S., Montagna-Mella, R., Ambrosioni, J., Tan, R. S., Mestres, C. A., Wray, D., Pachirat, O., Moreno, A., Chu, V. H., de Lazzari, E., … Cabell, C. H. (2021). Infective Endocarditis in Patients on Chronic Hemodialysis. Journal of the American College of Cardiology, 77(13), 1629–1640. [CrossRef]
- Pericás, J. M., Zboromyrska, Y., Cervera, C., Castañeda, X., Almela, M., Garcia-de-la-Maria, C., Mestres, C., Falces, C., Quintana, E., Ninot, S., Llopis, J., Marco, F., Moreno, A., & Miró, J. M. (2015). Enterococcal endocarditis revisited. Future Microbiology, 10(7), 1215–1240. [CrossRef]
- Arias, C. A., Mendes, R. E., Stilwell, M. G., Jones, R. N., & Murray, B. E. (2012). Unmet Needs and Prospects for Oritavancin in the Management of Vancomycin-Resistant Enterococcal Infections. Clinical Infectious Diseases, 54(suppl_3), S233–S238. [CrossRef]
- Nappi, F.; Avtaar Singh, S.S.; Jitendra, V.; Fiore, A. Bridging Molecular and Clinical Sciences to Achieve the Best Treatment of Enterococcus faecalis Endocarditis. Preprints 2023, 2023080217. [CrossRef]
- Nardi Agmon, I., Goldberg, E., Cohen, E., & Krause, I. (2017). Infective endocarditis in the setting of renal transplantation: Case report and review of the literature. Transplant Infectious Disease, 19(6), e12786. [CrossRef]
- Pericas, J. M., Cervera, C., del Rio, A., Moreno, A., Garcia de la Maria, C., Almela, M., Falces, C., Ninot, S., Castañeda, X., Armero, Y., Soy, D., Gatell, J. M., Marco, F., Mestres, C. A., Miro, J. M., & The Hospital Clinic Endocarditis Study Group. (2014). Changes in the treatment of Enterococcus faecalis infective endocarditis in Spain in the last 15 years: from ampicillin plus gentamicin to ampicillin plus ceftriaxone. Clinical Microbiology and Infection, 20(12), O1075–O1083. [CrossRef]
- Habib, G., Lancellotti, P., Antunes, M. J., Bongiorni, M. G., Casalta, J.-P., del Zotti, F., Dulgheru, R., el Khoury, G., Erba, P. A., Iung, B., Miro, J. M., Mulder, B. J., Plonska-Gosciniak, E., Price, S., Roos-Hesselink, J., Snygg-Martin, U., Thuny, F., Tornos Mas, P., Vilacosta, I., … Group, E. S. C. S. D. (2015). 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European Heart Journal, 36(44), 3075–3128. [CrossRef]
- Dahl, A., Rasmussen, R. v, Bundgaard, H., Hassager, C., Bruun, L. E., Lauridsen, T. K., Moser, C., Sogaard, P., Arpi, M., & Bruun, N. E. (2013). Enterococcus faecalis Infective Endocarditis. Circulation, 127(17), 1810–1817. [CrossRef]
- Beganovic, M., Luther, M. K., Rice, L. B., Arias, C. A., Rybak, M. J., & LaPlante, K. L. (2018). A Review of Combination Antimicrobial Therapy for Enterococcus faecalis Bloodstream Infections and Infective Endocarditis. Clinical Infectious Diseases, 67(2), 303–309. [CrossRef]
- Koehler, P., Jung, N., Cornely, O. A., Rybniker, J., & Fätkenheuer, G. (2019). Combination Antimicrobial Therapy for Enterococcus faecalis Infective Endocarditis. Clinical Infectious Diseases, 69(5), 900. [CrossRef]
- Schleifer KH, Kilpper-Balz R. Transfer of Streptococcus faecalis and Streptococcus faecium to the Genus Enterococcus norn. rev. as Enterococcus faecalis comb. nov. and Enterococcus faecium comb. nov. :4.
- Pericàs, J. M., García-de-la-Mària, C., Brunet, M., Armero, Y., García-González, J., Casals, G., Almela, M., Quintana, E., Falces, C., Ninot, S., Fuster, D., Llopis, J., Marco, F., Moreno, A., Miró, J. M., & Group, on behalf of the H. C. E. S. (2017). Early in vitro development of daptomycin non-susceptibility in high-level aminoglycoside-resistant Enterococcus faecalis predicts the efficacy of the combination of high-dose daptomycin plus ampicillin in an in vivo model of experimental endocarditis. Journal of Antimicrobial Chemotherapy, 72(6), 1714–1722. [CrossRef]
- Sakoulas G, Bayer AS, Pogliano J, Tsuji BT, Yang S-J, Mishra NN, et al. Ampicillin Enhances Daptomycin- and Cationic Host Defense Peptide-Mediated Killing of Ampicillin- and Vancomycin-Resistant Enterococcus faecium. Antimicrob Agents Chemother. 2012 Feb;56(2):838–44. [CrossRef]
- Herrera-Hidalgo L, Fernández-Rubio B, Luque-Márquez R, López-Cortés LE, Gil-Navarro MV, de Alarcón A. Treatment of Enterococcus faecalis Infective Endocarditis: A Continuing Challenge. Antibiotics (Basel). 2023 Apr 4;12(4):704. PMID: 37107066; PMCID: PMC10135260. [CrossRef]
- Carlos Armiñanzas, Concepción Fariñas-Alvarez, Jesús Zarauza, Patricia Muñoz, Víctor González Ramallo, Manuel Martínez Sellés, José Mª. Miró Meda, Juan Manuel Pericás, et al. Role of age and comorbidities in mortality of patients with infective endocarditis, European Journal of Internal Medicine, Volume 64, 2019, Pages 63-71, ISSN 0953-6205. [CrossRef]
- Juan M. Pericàs, Juan Corredoira, Asunción Moreno, M. José García-País, Carlos Falces, Ramón Rabuñal, Carlos A. Mestres, M. Pilar Alonso, Francesc Marco, Eduard Quintana, Manel Almela, Juan C. Paré, Jaume Llopis, Antoni Castells, José M. Miró. Relationship Between Enterococcus faecalis Infective Endocarditis and Colorectal Neoplasm: Preliminary Results From a Cohort of 154 Patients. Revista Española de Cardiología, Volume 70, Issue 6, 2017, Pages 451-458,ISSN 0300-8932. [CrossRef]
Figure 1.
Patients Lab Values During Hospitalization.
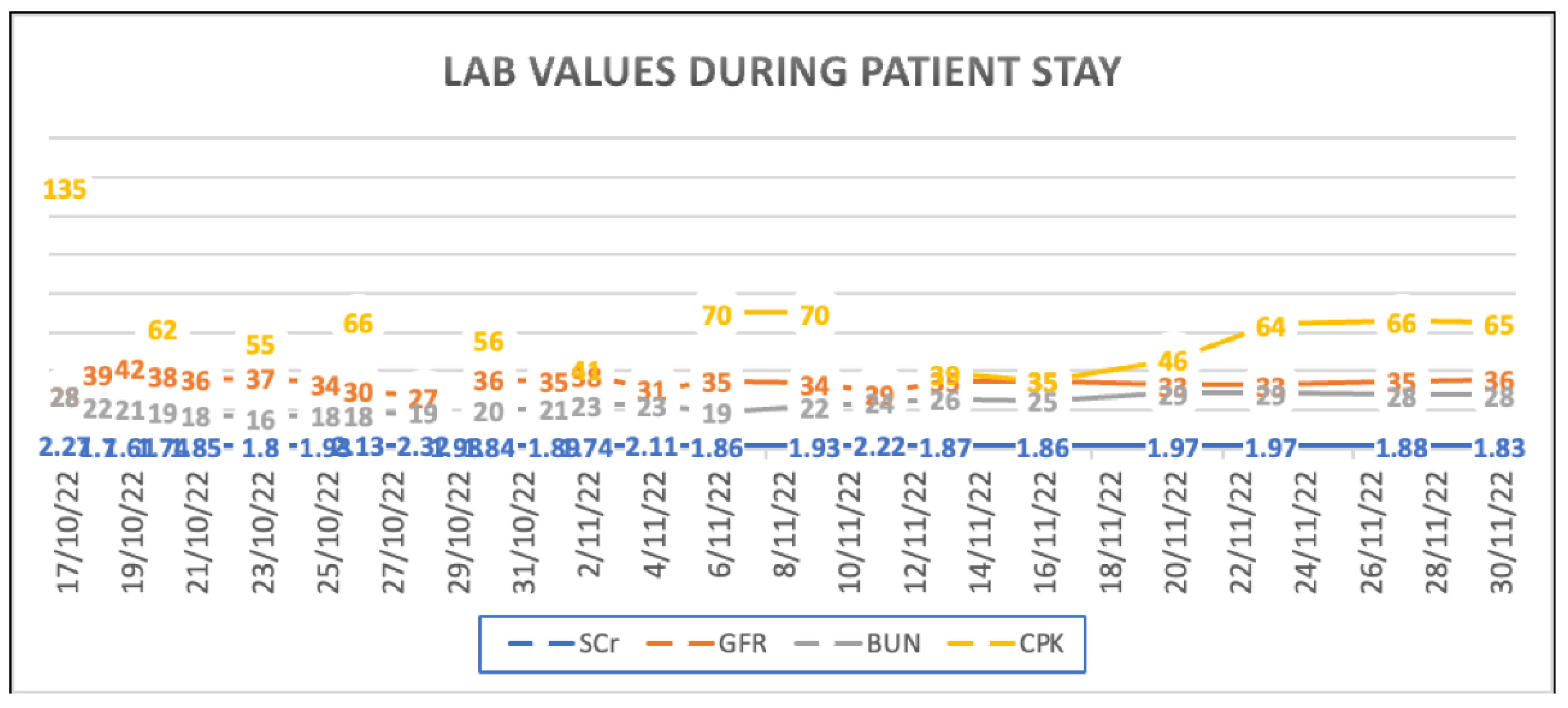
Figure 2.
Vegetation on a 2D ECHO. Trans-esophageal echo at the mid esophageal level in a 2-chamber view (61 degrees) demonstrates a 0.7 x 0.6 cm vegetation (arrow) on the atrial aspect of the anterior mitral leaflet.
Figure 2.
Vegetation on a 2D ECHO. Trans-esophageal echo at the mid esophageal level in a 2-chamber view (61 degrees) demonstrates a 0.7 x 0.6 cm vegetation (arrow) on the atrial aspect of the anterior mitral leaflet.
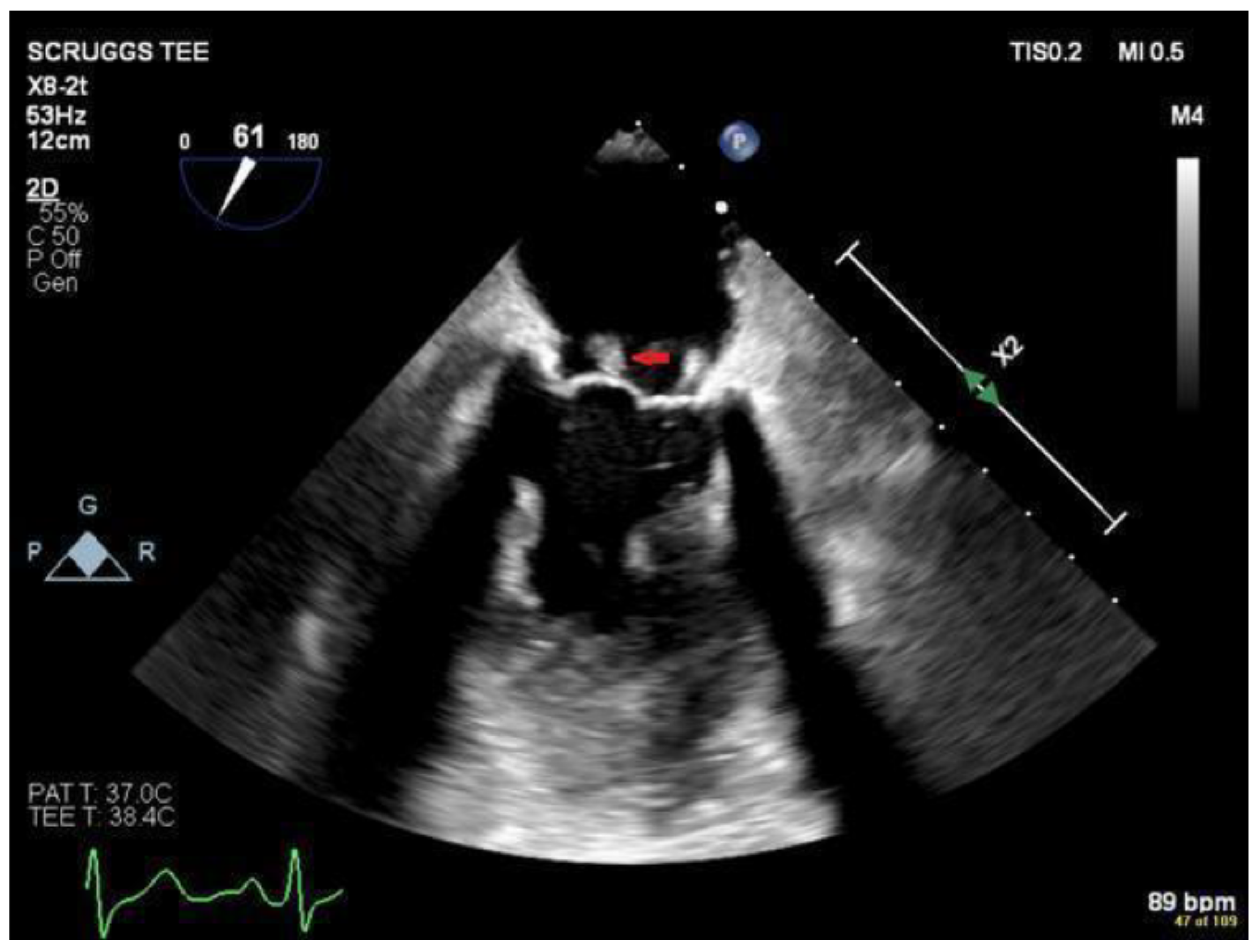

Table 1.
Solid Organ Transplant Patients with Infective Endocarditis due to E. Faecalis.
| Case | Age (Sex) |
Underlying Disease /transplant organ | Time between transplant and IE development | Affected Valve(s) / type of endocarditis | Organism | Initial Therapy | Directed therapy | Outcome | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 28 (F) | kidney | 6 mo | Mitral and Aortic/native | E. faecalis | Vancomycin | Vancomycin; MVR; AVR | 1 yr follow-up: Alive and Well | (28) |
| 2 | 22 (M) | kidney | 5 mo | Mitral, Aortic/native | NM | Ampicillin 2G IV | Vancomycin and Amikacin added; AVR | 3 mo follow-up: Alive and Well | (28) |
| 3 | 60 (F) | Rheumatic valve disease, kidney |
2 mo | Mitral / native | NM | Ampicillin; Gentamicin | Ampicillin; Gentamicin | Alive and well | (29) |
| 4 | 50 (M) | heart | 2 yr | Aortic/native | E. faecalis | Vancomycin 1g every 12 hr; plus, gentamicin 80mg every 8 hrs | Ampicillin; plus, gentamicin 40 mg every 6 hr; AVR | Alive and well | (31) |
| 5 | 68 (F) | Diabetes Mellitus type 2; Burkitt Lymphoma (in remission); kidney |
11 yr | Aortic | E. faecalis | Ampicillin 2G IV q/4hr; Daptomycin 6mg/kg q/d for 6 weeks | Ampicillin 2G IV q/4hr; Daptomycin 6mg/kg q/d for 6 weeks | 6 mo follow-up: Alive and Well | (32) |
| 6 | 59 (M) | No comorbidities liver |
7 mo | Aortic and mitral valve/native | E. faecalis (HLR to Gentamicin) | Vancomycin | vancomycin | Alive | (29) |
| 7 | 67(M) | Heart | 18.5 mo | Tricuspid valve / NM | E. faecalis | NM | NM | Death (1 day after diagnosis) | (34) |
| 8 | 32 (F) | Cystic fibrosis, Heart-Lung |
11 mo | Aortic valve / native | NM | Benzylpenicillin and streptomycin | AVR High dose benzylpenicillin (9.6 gr) |
Alive and well | (35) |
| 9 | 60 (M) | kidney | 2 weeks | No described | E. faecalis | Sulfonamide (10 days). | Linezolid and piperacillin/tazobactam for 7 days. | Death | 2020 |
| 10 | 48 (M) | kidney | 1 week | No described |
E. faecalis | imipenem/cilastatin and linezolid. | imipenem/ cilastatin and linezolid | Death | 2020 |
| 11 | 77 (M) | Kidney right eye Endogenous endophthalmitis |
NM | mitral valve/ native | E. faecalis | Intravenous amoxicillin. | Intravenous amoxicillin (6-week total duration), oral ciprofloxacin and intravitreal vancomycin and ceftriaxone. | Good recovery from his endocarditis, loss of vision in the affected eye. | 2016 |
| 12 | 45 (F) | Kidney | 6 Yr | mitral valve/ native | E. faecalis | Daptomycin 450 mg IV daily for 42 days Ampicillin sodic/ sulbactam sodic 3 gm IV BID for 42 days |
Daptomycin 450 mg IV daily for 42 days Ampicillin sodic/ sulbactam sodic 3 mg IV BID for 42 days |
Good recovery from her endocarditis, alive and well. | 2022 |
NM: not mentioned.
Table 2.
Sierra Hoffman et al. Case series of enterococcal endocarditis treated with ampicillin and daptomycin combination.
Table 2.
Sierra Hoffman et al. Case series of enterococcal endocarditis treated with ampicillin and daptomycin combination.
| Case | Age | Infected Valve | Kidney Function status | Prior Therapy | Final Therapy | Outcome |
|---|---|---|---|---|---|---|
| 1 | 79 | Mitral and Aortic | ESRD | Ampicillin 2g every 24h x 3 week | Daptomycin 6mg/kg q/48h and Ampicillin 2g q/d x 6weeks | Success with 6-months follow-up |
| 2 | 83 | Aortic | CKD | Levofloxacin 500mg x 15 days | Daptomycin 6mg/kg q/48h and Ampicillin 2g q/12h x 6weeks | Success with 1-year follow-up |
| 3 | 59 | Mitral | Acute kidney injury requiring temporary HD for 3 months | None | Daptomycin 6mg/kg q/d and Ampicillin 2g q/6h x 6weeks | Success, died at 6months from pneumonia |
| 4 | 89 | Mitral | CKD | Levofloxacin 500mg x 10 days | Daptomycin 6mg/kg q/48h and Ampicillin 1g q/6h x 6weeks | Success with 11-months follow-up |
| 5 | 62 | Mitral annulus | ESRD | Vancomycin and gentamicin, dose and duration unknown | Daptomycin 6mg/kg q/48h and Ampicillin 2g q/12h x 8weeks | Success with 3-months follow-up |
| 6 | 68 | Aortic | Renal Transplant | Ampicillin 2g IV q/4h; Daptomycin 6mg/kg q/d for 6 weeks | Same as initial | Success with 1-year follow-up |
| 7 | 45 | Mitral | Renal Transplant | None | Daptomycin 6 mg/kg q/d and Ampicillin/sulbactam 3g q/12h x 6weeks | Success with 1-year follow-up |
Table 3.
21st century, new associations and features of Enterococcus.
| 1. Number 1 cause of IE in kidney transplanted patients.[1] |
| 2. Number 1 cause of IE in TAVI patients.[27] |
| 3. Number 2 cause of IE in hemodialysis patients.[14] |
| 4. Number 1 cause of most common cause of hospital acquired IE.[3] |
| 5. Enterococcal IE is significantly more frequent among patients aged 65 years or more.[28] |
| 6. Association between EFIE and colorectal neoplasm. [29] |
| 7. Third most common cause of Infective Endocarditis in high-income countries.[3] |
| 8. More frequently HCA disease occurring predominantly among elderly patients with a large burden of comorbidities and seldom a clear identifiable source.[3] |
| 9. The aortic valve is more frequently involved in enterococcal IE cases.[3] |
| 10. E. faecalis produced significantly more prosthetic valve IE cases than other enterococcal species while the latter produced significantly more native valve IE, which has not been noted before.[3] |
IE= Infective Endocarditis. TAVI= Transcatheter Aortic Valve Implantation. EFIE= Enterococcus faecalis infective endocarditis. HCA= Health care–associated.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



