
Submitted:
13 November 2023
Posted:
14 November 2023
You are already at the latest version
Abstract
(1) Background: Environmental and public health research has given considerable attention to the impact of air quality on brain health, with systematic reviews widespread. No literature review has been done for cognitive frailty – a multidimensional syndrome combining physical frailty and cognitive impairment and their apparent co-dependence, linked to increased vulnerability and adverse health outcomes, including dementia. Instead, cognitive decline and frailty is implicitly explored through research on air quality and comorbid cognitive and physical decline in elderly populations. (2) Methods: A scoping review was conducted to explore the need for a systematic review. Combining Arksey and O’Malley [1] and PRISMA-ScR checklist [2], a scoping review of SCOPUS using ‘cogniti*’ + ‘resilience’ + ‘air quality’ or ‘cogniti*’ + ‘ageing’ + ‘air quality’ resulted in N=2503 articles, screened and reduced using inclusion and exclusion criteria, to N=16 articles. (3) Results: Air quality appears to be a critical risk factor for cognitive decline, even at air quality levels below WHO targets. Moderate long-term ambient air pollution appears linked to increased risk of cognitive frailty, suggesting earlier and more active interventions to protect older people. There are varied effects on cognition across the life course, with both emotional and functional impacts. Effects may be more detrimental to elderly people with existing conditions, including economic and health inequalities. Generalisation of results is limited due to the absence of a dose-response, variations in methods, controlling for comorbid effects, and variance across studies. (4) Conclusions: The findings support the need for more research and a more extensive summary of the literature.
Keywords:
Cognitive function
; ambient air quality
; air pollution and brain health
; older adults
; cognitive frailty
1. Introduction
There is growing evidence that exposure to high levels of air pollutants across the life course, particularly in old age, is detrimental to brain health and increases the risk of dementia syndrome and cognitive function [3]. In the elderly, this impact ranges from global cognition and neurodegenerative disorders to neuroinflammation and cognitive frailty [4,5,6].
Our scoping review focused on cognitive frailty – a new term for describing the simultaneous presence of physical frailty and cognitive impairment without dementia [7,8].
While the definitions and underlying mechanisms of cognitive frailty are still debated, older adults with both frailty and cognitive impairment are at higher risk of adverse health outcomes, including death, disability, hospitalisation and incident dementia, than those with either condition alone [9]. In some cases, the progression of cognitive frailty can be impeded or even reversed. Understanding modifiable risk factors could lead to interventions in lowering the risk of progression to dementia, neurodegenerative disorders, and other mental health consequences [10].
One such modifiable risk factor for cognitive frailty is air pollution. Ambient air pollution is the largest environmental risk to public health, contributing to ~4.2 million premature global deaths each year, [11] with significant direct and indirect economic costs. [12] Air pollution is measured through exposure to gases such as nitrogen oxides (NOx), sulphur dioxide (SO2), ozone (O3), and particulate matter. [13] Of particular concern for brain health, including cognitive frailty, is fine particulate matter (particulate matter with an aerodynamic diameter of ≤2.5 μm, PM 2.5). The World Health Organisation (WHO) Air Quality Guidelines (AQGs) were updated in 2021, reflecting evidence of adverse health impacts at low exposure levels (Table 1). [14]
Various proposed direct and indirect causal mechanisms have been reported on how air pollution impacts ill health, be it through the respiratory system, the cardiovascular system, central nervous system, gastrointestinal system, or epigenetic changes to DNA. [15,16,17] In terms of the brain, air pollution impacts health “via key biomarkers, inflammatory processes (neuro and vascular) and cardiopulmonary disease; and there is growing research showing that chronic exposure can deteriorate the protective barriers of the brain” [18] (p. 2). For example, ultrafine particles (with a diameter less than 0.1 µm, PM0.1) can potentially enter the brain via the olfactory bulb, resulting in neuroinflammation and cognitive impairment [19,20,21,22].
In terms of cognitive frailty, a recent nationwide prospective cohort study found a positive association between long-term PM2.5 exposure (defined as 10 μgm-3 increment of PM2.5) and a 5.0% increase in the incidence risk of frailty [5]. The estimated disease burden indicated that implementing clean air actions may reduce functional frailty and substantially offset the burden of population ageing worldwide. Evidence is also emerging that greater exposure to airborne pollutants, such as NOx, is associated with a higher probability of being in both the pre-frail and frail categories (odds ratio 1.003; 95% CI, 1.001–1.004) [23]. Similarly, the increase in the exposure to PM2.5–10 was associated with a higher probability of being pre-frail and frail (OR 1.014; 95% CI [1.001–1.036]), such as the increment in the exposure to PM2.5 that was associated with a higher probability of being frail (odd ratio 1.018; 95%, CI 1.001–1.037) [23]. PM2.5 exposure in older adults has also been linked to an increase in their depressive and anxiety symptoms [24].
While such studies have begun to identify key linkages, the research on the relationship between long-term exposure to particulate matter and cognitive frailty and functional disability in the elderly is limited, with no current summary of the literature. This gap in the literature is largely due to the fact that cognitive frailty is not presently treated as an explicit outcome; instead, it is implicitly explored through research on air quality and comorbid cognitive and physical decline in elderly populations. Hence the focus of our study. Combining [1] and PRISMA-ScR checklist [2], we piloted a scoping review to. (1) investigate the effects of poor air quality on cognitive frailty in older populations and (2) identify gaps in the evidence surrounding this. For our protocol, an examination of the SCOPUS database using ‘cogniti*’ + ‘resilience’ + ‘air quality’ or ‘cogniti*’ + ‘ageing’ + ‘air quality’ resulted in a total of N=16 articles for study. Following [2], the purpose of our scoping review was to determine if there is value in undertaking a more rigorous and systematic review of the literature and to identify which measures of air quality and cognitive frailty have been used in studies to date, with a view to, first, standardising reported measures for the future, and second, aiding in the planning and commissioning of future research [2] (p. 467).
2. Materials and Methods
2.1. Scoping review approach
This scoping review is part of a larger set of three separate scoping reviews that explore the impact of environmental factors on cognitive frailty. For our protocol, we followed [1]. Research questions were derived through their six stages using discussion and searches. Our rationale for using [1] – which [2] also use to construct the PRISMA-ScR checklist – is because it is useful for consultation and for policy makers, practitioners and service users whilst adopting transparent methods and global good practice standards for data analysis and presentation [25]. To organise and write up our study according to current practice, we used the PRISMA-ScR checklist [2].
2.2. Protocol
The literature database SCOPUS was searched to identify relevant observational and longitudinal studies. The terms ‘cogniti*’ + ‘resilience’+ ’air quality’ or ‘cogniti*’ + ‘ageing’ + ‘air quality’ were used; and, though aware of the limitations this brings, only results in English were included. Following the initial search, all duplicates were removed, and the titles were screened against inclusion and exclusion criteria. Book chapters, reviews and commentaries were excluded.
Titles/abstracts were screened by two of the lead authors of the study, and their eligibility for the study, based upon the rigorousness of their ambient air quality data, was screened by a lead author and the air quality expert on the team. Titles had to clearly indicate that the study explored the impact of air quality on cognitive aspects of frailty (excluding dementia or specifically mild cognitive impairment) and that the participants were an older age group, or a specific older age range. The abstracts of the remaining studies were then screened to identify those that specifically addressed cognition as a part of frailty in older persons because the aetiology of cognitive frailty may be different and is potentially reversible. This stage was important to exclude studies relating exclusively to physical frailty which were the majority.
To manage the findings and limit the range of variables involved in the association between air quality and cognition, the exclusion criteria were then amended to exclude all studies relating to indoor air quality or not considering PM2.5, as this aspect of air pollution has the most deleterious health effects and highest risk of negative cognitive impacts [3]. All of the included papers utilised some form of modelled air pollution mapping, validated by national, government-run field monitoring networks, such as the United States Environmental Protection Agency and Department for Food, Environment and Rural Affairs.
An excel spreadsheet was used for data extraction with headers that reflected key aspects of the findings in order to compare and contrast the ways that the studies were conducted, and data reported as population outcomes. Demographic information was identified (the age range of included participants, with gender and level of education attainment and social or financial status of the participants). The country of data collection, details on the methodology, sample size, and the methods of assessment of both air quality and the cognition were recorded. Study limitations and comments were also recorded by the author (CB) and the data extraction sheets were then shared with the wider transdisciplinary group of co-authors for the purpose of summarising and synthesising the data and prioritising the discussion.
Data analysis occurred following data extraction, with cognitive assessment and air quality measures compared within the selected papers. This was to identify how varied methods were used for the older adult cognitive frailty assessment and how the levels of pollutants were examined and reported. Data analysis included the assessment of air quality data utilised, and how this compared to WHO and national air quality guidelines and the inclusion of potential confounding variables used in analyses.
3. Results
3.1. Scoping Review
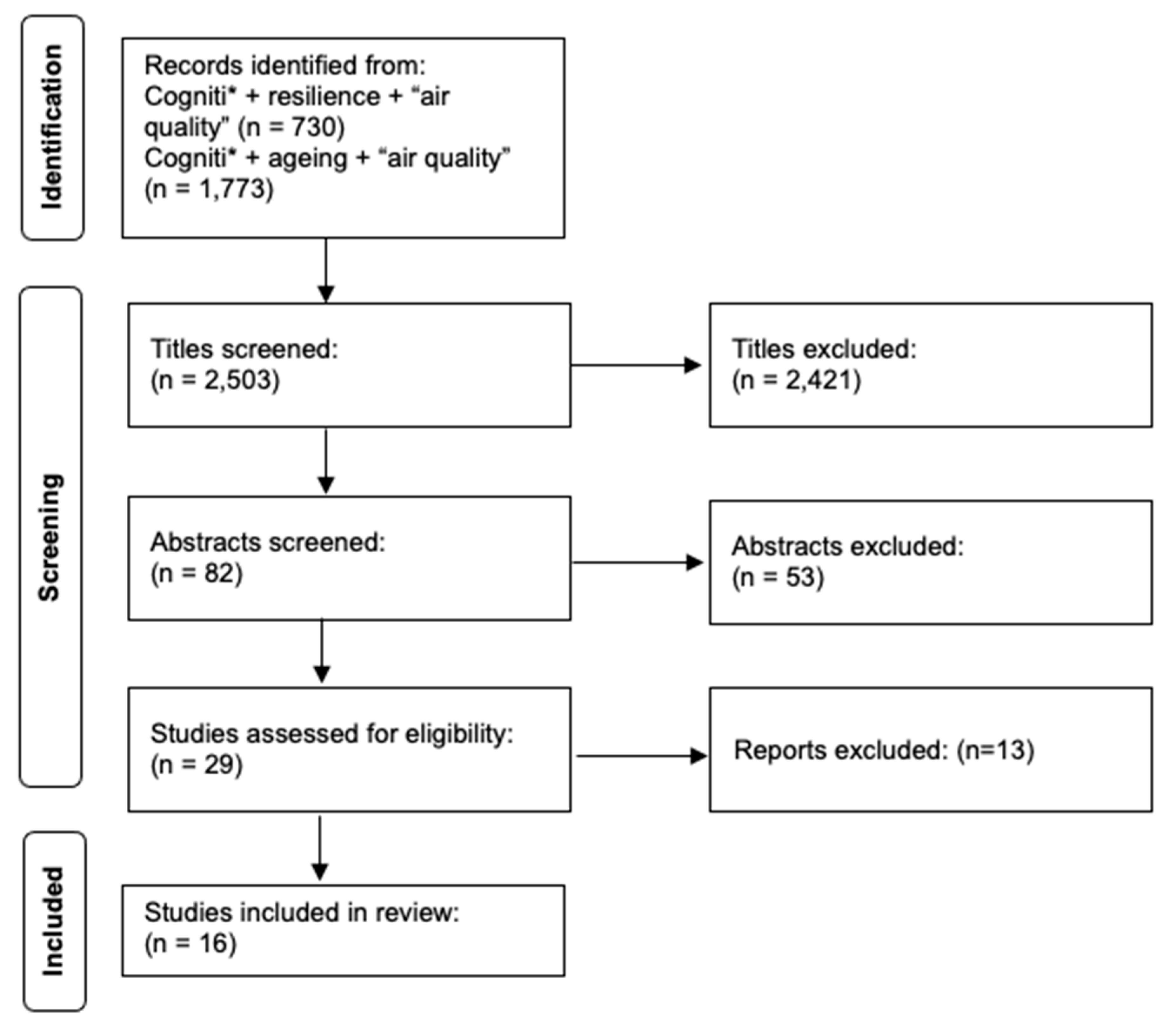
There were 16 papers selected for inclusion that represented international literature from both OECD countries (United States, Taiwan, China, and Scotland) and low to middle income countries (LMIC) including Mexico and Chile. Figure 1 below presents the process of article selection according to the PRISMA-ScR checklist [2]. It demonstrates the selection of articles according to refined inclusion and exclusion criteria.
Figure 2.
PRISMA-ScR checklist. Deselection following data extraction of a) indoor air quality (b) data that used atmospheric readings and c) where the data was not presented in such a way that the mean readings could be compared. All but one paper are quantitative studies and 11 are large cohort analysis of population data.
Figure 2.
PRISMA-ScR checklist. Deselection following data extraction of a) indoor air quality (b) data that used atmospheric readings and c) where the data was not presented in such a way that the mean readings could be compared. All but one paper are quantitative studies and 11 are large cohort analysis of population data.
All but four of the studies included gender balanced participant groups, with three of these females only. All but one study was quantitative, with the qualitative study used to study the effects of cardiorespiratory exercise on cognition in older women exposed to air pollution. The remaining studies included those with large cohorts reflecting a demographic of older people ages ranging from 50-98. The demographic factors associated with education level and household wealth were also extracted, based on the known shielding effect of higher levels of education and wealth associated with cognitive resilience. As presented in Table 2, the selected papers demonstrate inconsistencies in the reporting of wealth and education but were all included to identify the association between cognition in older adult populations in relation to poor air quality and the risks associated with declining cognition.
3.2. Variations in air quality assessment
As previously highlighted, the 16 papers selected for inclusion represented international literature from The Organization for Economic Cooperation and Development (OECD) referring to wealthier countries contrasting with low to middle income countries (LMIC) countries. PM2.5 data utilised in the studies was often modelled through a variety of methods, although the most commonly used was a version of kriging. Seven papers did not use fixed monitoring station data as a basis of their modelling but most of these did use satellite or other monitoring methods. Most but not all studies used static monitoring sources to validate model performance, and this showed strong correlations between models and monitoring stations. Averaging periods for PM2.5 exposure for the majority of studies was annual mean concentration, although some utilised 24 hour mean or longer exposure periods. Further details are presented in Table 3.
3.3. Overall results
There is evidence that living in areas with the highest quintiles of cumulative PM2.5 was associated with risk of developing poor cognitive function [26] and that higher levels of exposure to ambient PM2.5 are associated with worse cognitive decline [27]. Long term exposures to PM2.5 and NOx, estimated from participants addresses, were directly associated with lower global cognitive performance [28]. The association between particulate air pollution with cognitive function, as well as cognitive decline over time, were also confirmed [29]. [30] shows that 11-year exposure to elevated PM2.5 levels was associated with poor global cognition over four-year follow-up; and, over time, the likelihood of impact from long term exposure was an increased incidence of 46% [31]. In addition, the Lothian Birth Cohort analysis [6], which reported higher air pollution modelled from 1935 (when participants would have been in utero), was associated with worse change in IQ from age 11-70 years, suggesting that a life course paradigm is essential for understanding cognitive decline in relation to air pollution.
Some studies differentiated the risks to different groups, for example, PM2.5 was unrelated to cognition among those with 13 or more years of education [32]. Similarly, exposure to PM2.5 was associated with other risk factors in older people, for example cognitive function appeared to be reduced in those who smoked [32]. For example, [33] identified higher risk of effect between PM2.5 and incidence of disability in men, smokers, and participants with cognitive impairment. [34] recognised non-Hispanic participants had less cognitive change when exposed to higher PM2.5 concentration; they also lacked the genetic factor (genotype E4 (APOE-ε4) allele) that accelerated the rate of decline. [35] also observed an association between air pollution with cognitive decline mediated via air pollution impacting the sleep cycle which resulted in brain structure changes. [31] observed a notable association of cumulative PM2.5 and worse cognitive function being more pronounced in participants whose diets scored lower on the plant-based diet index.
The presence of different covariates is important to note, given the number of studies that seek to adjust for community social characteristics and individual social, demographic, economic, and health characteristics. In some studies, area-level household income and house value modified the associations between ozone exposure and cognitive effects, with residents of lower income or house-value neighbourhoods having an increased response to ozone [36]. However, in [28] the emotional distress associated with (in particular) NOx was not confounded by socio-economic factors (age, geographical region, race/ethnicity, education, and income), lifestyle (smoking, alcohol, and physical activity), employment status or clinical characteristics [28].
The level of disability caused in more vulnerable populations from PM2.5 exposure means that the threshold for significant risk is important. Wang et al. (2020) identified that each 10 μgm-3 increase in PM2.5 was associated with a 5.1% increased risk of poor cognitive function. Subgroup analyses suggested stronger associations between PM2.5 and poor cognitive impairment in men than women [37]. [36] also notes a positive association between short to medium term (average one and four weeks) ambient exposure to gaseous pollutants (ozone and NOx) and elevated psychiatric symptom intensity. One study provided limited population-based evidence for the oldest subjects and detected a threshold of 33 μgm-3. Below this level there may be a lower risk of disability in activities of daily living [33]. The operative thresholds of functional disability enable the consideration of consequent needs arising from cognitive impairment.
Mean PM2.5 relative to WHO target air quality guidelines are shown in Figure 2 below. All but one of the sixteen studies [36] showed a detrimental impact of PM2.5 on cognitive function. Levels of PM2.5 that negatively influenced cognition varied from lowest detrimental concentration being 7.9 μgm-3, below the WHO Interim Target 4 (10 μg/m3), up to 50.3 μgm-3.
3.4. Variations in cognitive assessments
Some studies focussed on memory assessment as a means of measuring cognition, as in [32] who used 10 word immediate and delayed recall and serial 7s subtraction (attention and processing speed, working memory and counting backwards) to assess incident cognitive decline. Similar methods for immediate and delayed 10-noun free recall tests to measure memory, included a serial 7 subtraction test to measure working memory, a backwards counting test to measure processing speed, recall the date and name of the president and vice president to measure orientation and an object naming test to measure knowledge and language [38]. The focus on working memory being adversely affected by exposure to PM2.5 suggests that older people’s long-term memory and recollection of previous experiences may also be affected by other ageing phenomena or accelerated by the effect of pollution on the cardiovascular and other systems [32,38].
Functionally oriented tests perhaps provide a more reliable measure of change over time that can be attributed to personal characteristics such as intelligence and individual cognitive resilience. [30], for example, used the Montreal Cognitive Assessment-Taiwanese version (MoCA-T, [39]) to test domain-specific cognition e.g., memory, executive function, category/semantic fluency, and attention. They also used the Wechsler Memory Scale, 3rd edition to assess attention performance and verbal fluency tests. [29] used the Alice Heim 4-I test (see NSHD - Age 15 - The Alice Heim Group Ability Test (AH4) - CLOSER ) for global intelligence – comprised of a series of 65 verbal and mathematical reasons items of increasingly difficulty – to measure the impact of air quality on inductive reasoning and the ability to identify patterns and infer principles and rules. They also used a 20-word recall test short term verbal memory; and two measures of verbal fluency to measure cognitive function and decline over time in cognition. These studies, along with [6] also sought to identify protective factors, as in the case of educational level and diet, which may provide resilience to cognitive frailty. [6] also used Lothian Birth Cohort data collected from the Moray House Test in 1947 (for subjects born in 1936) and considered whether risk is accumulated through long-term exposure or whether there are sensitive or critical periods in the life course.
In contrast, [33] used Katz Index of Independence in Activities of Daily Living (alz.org) with the oldest elderly Chinese subjects in their study to assess functional changes in relation to PM2.5 and showed a decline in relation to exposure. The rationale for functional assessment to measure cognition is well established and aligns with the International Classification of Functioning, Disability and Health (ICF) (who.int), which is an assessment of health and health-related domains and the disability of an individual that occurs in a context. The ICF also includes a list of environmental factors that impact on the ability to perform tasks, and which are meaningful to individuals, such as the presence of support/carer/family in the environment.
Several studies e.g., [32,40] used specific dementia assessments to identify those with normal cognition, such as the Data_Description_Langa_Weir_Classifications2020.pdf (umich.edu). Commonly the Mini-Mental State Exam, CASI (C-2.0) is used to measure the impact of air quality in the elderly on orientation, memory registration, concentration, delayed recall memory, language and construction. CASI: attention, orientation, short-term memory, long-term memory, language abilities, mental manipulation, verbal fluency, abstract thinking, drawing (see Mini-mental state examination (MMSE) - Oxford Medical Education ). These functional tests were used in six of the 16 studies and are appropriate for the identification of working memory, also used by [41] and [28]. These latter studies aimed to identify the association between long-term ambient air pollution exposure, emotional distress and cognitive decline in older adulthood as a precursor to a psychiatric condition.
3.5. Limitations of the selected studies
The first limitation concerns assessing or controlling for covariate factors. The 16 studies selected for this scoping review all reported mean levels of particulates. Potential studies that did not report a mean were excluded. Doing so allowed us to compare pollution levels and their impact on cognitive frailty across studies. These other studies aside, when looking at the 16 studies in this scoping review, while the methods of analysis for cohort data were deemed reliable, they did not control for the presence of multiple covariate factors e.g., pre-existing conditions, the effect of long-term poverty, low paid work, and an assumed lack of resilience to other environmental factors, all of which negatively impact old age [42]. Future studies need to take these covariates into consideration.
The second issue is measurement error for air pollution estimates, e.g., PM2.5 and NOx exposures [28]. Similarly, [6] highlight that results have large degrees of uncertainties, considering the various methodologies used to produce the different air pollution concentration estimates. Furthermore, all but one study [41] compared pollution concentrations to WHO air quality guidelines and interim targets and/or national guideline concentrations. This is an area that would be beneficial to be included in future studies to allow for greater comparison against WHO standards and help map out reduction pathways for local authorities to improve air quality and population exposure.
4. Discussion
4.1. Limitations of scoping review and gaps in the literature
This scoping review collated evidence on the impact that ambient air quality has on various measures of cognitive outcomes in older adult populations, known more recently as muti-dimensional cognitive frailty. The value of this review was that, presently, no such summary of the literature has been conducted. Our goal was to (1) investigate what the literature has to say on the effects of poor air quality on cognitive frailty in older populations and (2) to see if we could identify gaps in the evidence surrounding this. Following [2], we also sought, more widely, to determine if there is value in undertaking a more rigorous and systematic review of this literature and to identify which measures of air quality and cognitive frailty have been used in studies to date, with a view to, first, standardising reported measures for the future, and second, aiding in the planning and commissioning of future research.
As concerns our primary goal, we can conclude that, yes, there is a need for a more systematic review of the literature and that, there are a number of limitations and gaps in the literature that we identified which can inform future research. First, given that our study was a scoping review, we did not provide an assessment of quality for the 16 studies. There is also, presently, an insufficient number of studies to do so. Any future in-depth summary of the literature would benefit from such an assessment. Second, cognitive frailty is a new term, and only more recently used as a defined and explicit condition. While the studies we reviewed measure different aspects of cognitive frailty in the elderly, it is essential, going forward, that future research address this gap by making cognitive frailty an explicit topic of study. Third, as mentioned earlier, another gap in the literature concerns differences across studies in the degree to which they assessed or controlled for covariates making it difficult to determine the overall impact of air quality on frailty. Finally, as with most literature reviews, there is the limitation of making generalisations due to differences in how cognitive outcomes are measured across studies.
We also acknowledge that, given our focus on SCOPUS, certain studies may have been missed due to not being part of its database or key-worded differently. Also, given that the definition of cognitive frailty is somewhat contested or not known by researchers in the broader field of air quality and brain health, there is a chance authors of certain studies could have used other terms.
We also recognized that, in terms of another gap in the literature, there are few studies on this topic for low-to-middle-income countries. Another is the absence of rigorous socio-demographic data or in-depth reporting sufficient to engage in a summary review of the role socioeconomic deprivation or inequalities play in the impact air pollution has on the elderly across different countries. Similarly, the potential of higher education and wealth to ameliorate the risks of frailty and cognitive impairment were not accessible due to the failure to systematically report demographic details. This is important because the differentiated health effects from poor air quality are experienced at a range of scales, with demography, density and health geography all playing a part [43,44,45]. In most instances the oldest and most disadvantaged within a community experience the worst pollution levels, while also often lacking the ability to negate detrimental effects and pollution exposure [46,47]. In addition to air quality, the socio-ecological systems that people live and spend time in either for work or leisure are important factors when considering health effects [43,44,45]. The effects of air quality are also exacerbated by dementia and other health risks [48].
4.3. Standardizing measures of air quality and cognitive frailty
Following [2], we also concluded that our findings warrant a more rigorous and systematic review of the literature. In terms of standardisation of measures, we established that measures of PM2.5 are the most useful, particularly when reported as means and with the impact of covariates on cognitive frailty outcomes taken into consideration. In terms of measuring cognitive frailty, in addition to the need to make this outcome more explicitly measured and rigorous, we identified several cognitive measures used, including tests for immediate and delayed recall, episodic memory, and cognitive functionality, including the Montreal Cognitive Assessment-Taiwanese version (MoCA-T, [38]); the Wechsler Memory Scale, 3rd edition; and the Alice Heim Group Ability Test (AH4). Finally, to measure independence, the Katz Index of Independence in Activities of Daily Living was used. Functionality was particularly important because it provides a more reliable measure of cognitive change over time.
4.3. Thinking about policy and practice
The increasing number of older adults across the world represents a demographic megatrend that is transforming economies and societies [48]. While all countries are experiencing an ageing of their populations, their respective health trends manifest along different trajectories, mostly as a function of differences in environmental and socio-demographic factors, as in the case of air pollution [50,51]. The incidence of frailty in older people is increasing too and measures that reduce the risk of disease and promote the maintenance of function, confidence and engagement are important to support healthy ageing and ease the pressure on healthcare systems [52].
In this context, the scoping review aimed to identify the association between air pollution and cognitive frailty in older people but without dementia. The incidence of cognitive frailty (1-12% of the adult <65 population) is now being recognised as a cause of subsequent disability The identification of cognitive impairment as an intersectional feature of frailty provides an opportunity for secondary prevention: alleviating cognitive impairment in older adults improves their functional health [8]. In addition to programmes to ameliorate cognitive frailty from either a cognitive or physical approach, we must also address underlying mediatory factors such as air pollution that live outside of the control of the individual.
The intersection between climate change and population ageing has only begun to receive attention despite being considered a critical global issue [53]. Older populations are particularly vulnerable, often with pre-existing morbidities that are sensitive to the consequences of climate change, such as extreme heat and air pollution [54]. Green planning initiatives such as improving air quality may reduce the future population burden of poor cognitive function, especially in areas ambient air pollution is identified as a risk factor for older adults. But current policy initiatives are associated with reduction of ‘impact’ from pollution and not the reduction of air pollution per se. For example, the UK government has announced that councils in England have been granted almost £11 million in funding for projects that will improve air quality [55]. This annual ‘Air Quality Grant’ helps councils develop and implement measures to benefit schools, businesses and communities by reducing the impact of air pollution on people’s health. Older adults are not a homogenous group and councils will need to decide on the targeting of poorer communities (where air pollution is often the highest) or on more general interventions such as clean air zones [56]. In addition, a systematic review published in the Lancet has suggested low emission air zones can reduce air-pollution related health outcomes, and that ongoing evaluation of these interventions may help explore their role in reducing cognitive frailty in the hope that high risk and vulnerable groups benefit alongside the general population [57].
4.4. The differential impact of air quality, even when guidelines are met
Differential levels of air pollution and their effects on cognition and frailty can be seen in the selected literature. This includes studies demonstrating that even low levels of air pollution (<10 μgm-3) can have a harmful health effect, particularly over long periods. This effect is also often below the WHO Interim Target 3 concentration of 15 μgm-3, which was highlighted as being close to the mean PM2.5 concentration reported in long term exposure studies [57]. The WHO AQGs and Interim Targets have been designed to provide a framework for authorities to work towards and through, which coupled with our scoping review, highlights the need to increase the number of long-term exposure studies determining the life course impact of even low levels of pollution on cognition [58]. However, with the exception of one paper, none of the 16 articles reviewed here included reference to WHO or national guidelines for pollution concentrations [41].
4.5. Thinking about co-benefits
The impacts of air pollution and climate change are often understood as global and considered to occur over a timescale of decades. Viewing these impacts from a co-benefits lens allows them to be considered from a local, short-term perspective which is often more politically relevant. These co-benefits, which have both health and economic advantages, include not only mitigating against or even reversing cognitive frailty, but also, across the life course, reducing premature mortality, sickness days, healthcare expenditures, and poor indoor air quality [59]. Many older adults spend a considerable amount of their time indoors – a topic not addressed by this scoping review, but of importance to any wider summary of the literature. For example, a longitudinal study found that both indoor and ambient air pollution had adverse effects on the mental health of the elderly, particularly with regards to depressive symptoms [60]. It is well established that depression is associated with cognitive impairment and so addressing air pollution may be one way in which reversible elements of cognitive frailty can have other positive brain health effects.
5. Conclusion
Environmental and public health research has given considerable attention to the impact of air quality on brain health, with systematic reviews widespread. No summary of the literature has been done for cognitive frailty – a multidimensional syndrome combining frailty and cognitive impairment, linked to increased vulnerability and adverse health outcomes, including dementia. This gap in the literature is largely due to the fact that cognitive frailty is not presently treated as an explicit outcome; instead, it is implicitly explored through research on air quality and its impact on comorbid cognitive and physical decline in elderly populations.
Hence the focus of our scoping review. Combining [1] and PRISMA-ScR checklist [2], a scoping review of SCOPUS using ‘cogniti*’ + ‘resilience’ + ‘air quality’ or ‘cogniti*’ + ‘ageing’ + ‘air quality’ resulted in N=2503 articles, screened and reduced using inclusion and exclusion criteria, for a total of N=16 articles.
We identified several insights across the literature, albeit tentatively, given the small number of studies. For example, we found evidence of an association between higher PM2.5 levels and worse cognitive function and rate of decline in cognitive function over the life course, although certain population factors influenced the size of the effect. We also found that air quality appears to be a critical risk factor even at air quality levels below World Health Organization targets. There are also varied effects on cognition across the life course, with both emotional and functional impacts. Effects may be more detrimental to elderly people with existing conditions, including economic and health inequalities. Finally, in terms of standardizing measures, we identified PM2.5 averages being central, as well as several cognitive measures, with cognitive function being particularly reliable, given the potential reversibility of cognitive frailty.
In terms of the value of these insights for policy and practice, interventions aimed at improving air quality and minimising the impact of exposure to air pollution for those with this particular cognitive impairment could actively address the disability associated with increased frailty and significant additional healthcare utilisation. The benefits of cleaner air are particularly great for older, and more vulnerable elderly groups; but systemic improvements to air quality will benefit society as whole and further prevent the lifespan effects of air pollution on neonates, children, and vulnerable adults. The suggested health risk at even low levels of air pollution on cognition needs to be subject of a major policy initiative for those with recognised vulnerability due to age or pre-existing morbidity. The estimated disease burden indicates that implementing clean air actions may prevent frailty and substantially offset the burden of population ageing worldwide.
Author Contributions
JH – air quality appraisal and review, manuscript writing and review, final draft production, CB – data curation, manuscript writing and review, BC - manuscript writing and review, AE - manuscript writing and review, RY - manuscript writing and review, HT - manuscript writing and review, RB - manuscript writing and review, OEJ - manuscript writing and review, SFD – conceptualisation, manuscript writing and review, supervision.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors would like to acknowledge the international transdisciplinary network funded by BBSRC/MRC RCUK, namely, Harnessing knowledge of lifespan biological, health, environmental and psychosocial mechanisms of cognitive frailty for integrated interventions as part of the UK ageing network (UKAN Network - UKAN (ukanet.org.uk)).
Declaration of competing interest
The authors declare no competing interests.
References
- Arksey, Hilary, and Lisa O'Malley. "Scoping studies: towards a methodological framework". International journal of social research methodology 2005, 8, 19–32. [CrossRef]
- Tricco, Andrea C., Erin Lillie, Wasifa Zarin, et al. "PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation". Annals of internal medicine 2018, 169, 467–473. [CrossRef] [PubMed]
- Delgado-Saborit, Juana Maria, Valentina Guercio, et al. "A critical review of the epidemiological evidence of effects of air pollution on dementia, cognitive function and cognitive decline in adult population". Science of the Total Environment 2021, 757, 143734. [CrossRef] [PubMed]
- Chandra, M., Rai, C.B., Kumari, N., et al. Air pollution and cognitive impairment across the life course in humans: a systematic review with specific focus on income level of study area. Int. J. Environ. Res. Publ. Health 2022, 19, 1405. [CrossRef] [PubMed]
- Lv, Yuebin, Ze Yang, Lihong Ye, et al. "Long-term fine particular exposure and incidence of frailty in older adults: findings from the Chinese Longitudinal Healthy Longevity Survey". Age and Ageing 2023, 52, afad009. [CrossRef] [PubMed]
- Russ, Tom C., Mark PC Cherrie, Chris Dibben, et al. "Life course air pollution exposure and cognitive decline: modelled historical air pollution data and the Lothian birth cohort 1936". Journal of Alzheimer's Disease 2021, 79, 1063–1074. [CrossRef] [PubMed]
- Clegg, Andrew, John Young, Steve Iliffe, et al. "Frailty in elderly people". The lancet 2013, 381, 752–762. [CrossRef]
- Kelaiditi, Eirini, M. Cesari, Marco Canevelli, et al. "Cognitive frailty: rational and definition from an (IANA/IAGG) international consensus group". The journal of nutrition, health & aging 2013, 17, 726–734. [CrossRef]
- Sugimoto, Taiki, Hidenori Arai, Takashi Sakurai. "An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions". Geriatrics & Gerontology International 2022, 22, 99–109. [CrossRef]
- Ramnath, Udhir, L. Rauch, Estelle Victoria Lambert, et al. "The relationship between functional status, physical fitness and cognitive performance in physically active older adults: A pilot study". PloS one 2018, 13, e0194918. [CrossRef]
- WHO. Ambient (outdoor) air pollution. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health, 2022a, accessed 21/6/2023.
- Mannucci, Pier Mannuccio, Sergio Harari, Massimo Franchini. "Novel evidence for a greater burden of ambient air pollution on cardiovascular disease". haematologica 2019, 104, 2349. [CrossRef] [PubMed]
- Sun, Zhuanlan, Demi Zhu. "Exposure to outdoor air pollution and its human health outcomes: A scoping review". PloS one 2019, 14, e0216550.
- WHO. WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulphur dioxide and carbon monoxide, 2021 https://apps.who.int/iris/handle/10665/345329.
- Calderon-Garciduenas, Lilian, Robert R. Maronpot, Ricardo Torres-Jardon, et al. "DNA damage in nasal and brain tissues of canines exposed to air pollutants is associated with evidence of chronic brain inflammation and neurodegeneration". Toxicologic pathology 2003, 31, 524–538. [CrossRef] [PubMed]
- Shou, Yikai, Yilu Huang, Xiaozheng Zhu, et al. "A review of the possible associations between ambient PM2. 5 exposures and the development of Alzheimer's disease". Ecotoxicology and Environmental Safety 2019, 174, 344–352. [CrossRef] [PubMed]
- COMEAP. Air pollution: cognitive decline and dementia. A report by the Committee on the Medical Effects of Air Pollutants (COMEAP), 2022. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1090376/COMEAP-dementia-report-2022.pdf.
- Castellani, Brian, Suzanne Bartington, Jonathan Wistow, et al. "Mitigating the impact of air pollution on dementia and brain health: Setting the policy agenda". Environmental Research 2022, 114362. [CrossRef]
- Oberdörster, Günther, Zachary Sharp, Viorel Atudorei, et al. "Translocation of inhaled ultrafine particles to the brain". Inhalation toxicology 2004, 16, 437–445. [CrossRef] [PubMed]
- Heusinkveld, Harm J., Tina Wahle, Arezoo Campbell, et al. "Neurodegenerative and neurological disorders by small inhaled particles". Neurotoxicology 2016, 56, 94–106. [CrossRef] [PubMed]
- Tian, Lin, Yidan Shang, Rui Chen, Ru Bai, et al. "Correlation of regional deposition dosage for inhaled nanoparticles in human and rat olfactory". Particle and fibre toxicology 2019, 16, 1–17. [CrossRef]
- Tian, Qu, Murat Bilgel, Abhay R. Moghekar, et al. "Olfaction, cognitive impairment, and PET biomarkers in community-dwelling older adults". Journal of Alzheimer's Disease 2022, 86, 1275–1285. [CrossRef] [PubMed]
- Veronese, Nicola, Laura Maniscalco, Domenica Matranga, et al. "Association Between Pollution and Frailty in Older People: A Cross-Sectional Analysis of the UK Biobank". Journal of the American Medical Directors Association 2023, 24, 475–481. [CrossRef]
- Pun, Vivian C., Justin Manjourides, Helen Suh. "Association of ambient air pollution with depressive and anxiety symptoms in older adults: results from the NSHAP study". Environmental health perspectives 2017, 125, 342–348. [CrossRef]
- Lockwood, Craig, Kelli Borgess Dos Santos, Robin Pap. "Practical guidance for knowledge synthesis: Scoping review methods". Asian nursing research 2019, 13, 287–294. [CrossRef]
- Yao, Yao, Xiaozhen Lv, Chengxuan Qiu, et al. "The effect of China's Clean Air Act on cognitive function in older adults: a population-based, quasi-experimental study". The Lancet Healthy Longevity 2022, 3, e98–e108. [CrossRef]
- Weuve, Jennifer, Robin C. Puett, Joel Schwartz, et al. "Exposure to particulate air pollution and cognitive decline in older women". Archives of internal medicine 2012, 172, 219–227. [CrossRef]
- Petkus, Andrew J., Xinhui Wang, Daniel P. Beavers, et al. "Outdoor air pollution exposure and inter-relation of global cognitive performance and emotional distress in older women". Environmental Pollution 2021, 271, 116282. [CrossRef]
- Tonne, Cathryn, Alexis Elbaz, Sean Beevers, et al. "Traffic-related air pollution in relation to cognitive function in older adults". Epidemiology (Cambridge, Mass.) 2014, 25, 674. [CrossRef]
- Chen, Jen-Hau, Tsung-Yu Kuo, Hwa-Lung Yu, et al. "Long-term exposure to air pollutants and cognitive function in Taiwanese community-dwelling older adults: a four-year cohort study". Journal of Alzheimer's Disease 2020, 78, 1585–1600. [CrossRef]
- Zhu, Anna, Hui Chen, Jie Shen, et al. "Interaction between plant-based dietary pattern and air pollution on cognitive function: A prospective cohort analysis of Chinese older adults". The Lancet Regional Health–Western Pacific 2022, 20.
- Ailshire, Jennifer, Katrina M. Walsemann. "Education differences in the adverse impact of PM 2.5 on incident cognitive impairment among US older adults". Journal of Alzheimer's Disease 2021, 79, 615–625. [CrossRef] [PubMed]
- Lv, Yuebin, Jinhui Zhou, Virginia Byers Kraus, et al. "Long-term exposure to PM2. 5 and incidence of disability in activities of daily living among oldest old". Environmental Pollution 2020, 259, 113910. [CrossRef] [PubMed]
- Kulick, Erin R., Mitchell SV Elkind, Amelia K. Boehme, et al. "Long-term exposure to ambient air pollution, APOE-ε4 status, and cognitive decline in a cohort of older adults in northern Manhattan". Environment international 2020, 136, 105440. [CrossRef] [PubMed]
- Lo, Chen-Chen, Wen-Te Liu, Yueh-Hsun Lu, et al. "Air pollution associated with cognitive decline by the mediating effects of sleep cycle disruption and changes in brain structure in adults". Environmental Science and Pollution Research 2022, 29, 52355–52366. [CrossRef] [PubMed]
- Qiu, Xinye, Mahdieh Danesh-Yazdi, Marc Weisskopf, et al. "Associations between air pollution and psychiatric symptoms in the Normative Aging Study". Environmental Research Letters 2022, 17, 034004. [CrossRef] [PubMed]
- Wang, Jiaonan, Tiantian Li, Yuebin Lv, et al. "Fine particulate matter and poor cognitive function among Chinese older adults: evidence from a community-based, 12-year prospective cohort study". Environmental health perspectives 2020, 128, 067013. [CrossRef] [PubMed]
- Ailshire, Jennifer A., Eileen M. Crimmins. "Fine particulate matter air pollution and cognitive function among older US adults". American journal of epidemiology 2014, 180, 359–366. [CrossRef] [PubMed]
- Tsai CF, Lee WJ, Wang SJ, et al. “Psychometrics of the Montreal Cognitive Assessment (MoCA) and its subscales: validation of the Taiwanese version of the MoCA and an item response theory analysis”. Int Psychogeriatr. 2012, 24, 651–658. [CrossRef] [PubMed]
- Salinas-Rodríguez, Aarón, Julián Alfredo Fernández-Niño, et al. "Exposure to ambient PM2. 5 concentrations and cognitive function among older Mexican adults". Environment international 2018, 117, 1–9. [CrossRef] [PubMed]
- Molina-Sotomayor, Edgardo, Marcelo González Orb, Francisco Pradas de la Fuente, et al. "Effects of cardiorespiratory exercise on cognition in older women exposed to air pollution". International journal of environmental research and public health 2019, 16, 245. [CrossRef] [PubMed]
- Marmot, Michael. "Health equity in England: the Marmot review 10 years on". Bmj 2020, 368.
- Al-Kindi, Sadeer G., Robert D. Brook, Shyam Biswal, et al. "Environmental determinants of cardiovascular disease: lessons learned from air pollution". Nature Reviews Cardiology 2020, 17, 656–672. [CrossRef]
- Hoffmann, Barbara. "Air pollution in cities: Urban and transport planning determinants and health in cities". Integrating human health into urban and transport planning: A framework 2019, 425–441.
- Koman, Patricia D., Kelly A. Hogan, et al. "Examining joint effects of air pollution exposure and social determinants of health in defining “at-risk” populations under the Clean Air Act: susceptibility of pregnant women to hypertensive disorders of pregnancy". World medical & health policy 2018, 10, 7–54.
- Fairburn, Jonathan, Steffen Andreas Schüle, Stefanie Dreger, et al. "Social inequalities in exposure to ambient air pollution: a systematic review in the WHO European region". Int j of environ research and public health 2019, 16, 3127. [CrossRef] [PubMed]
- Ferguson, Lauren, Jonathon Taylor, Ke Zhou, et al. "Systemic inequalities in indoor air pollution exposure in London, UK". Buildings & cities 2021, 2, 425.
- Callaghan, A., G. McCombe, A. Harrold, C. et al. "The impact of green spaces on mental health in urban settings: a scoping review". Journal of mental health 2021, 30, 179–193. [CrossRef] [PubMed]
- Hajkowicz, Stefan, Hannah Cook, Anna Littleboy. "Our future world: Global megatrends that will change the way we live.” Canberra: CSIRO, 2012.
- Wang, Haidong, Mohsen Naghavi, Christine Allen, et al. "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". The lancet 2016, 388, 1459–1544.
- Chew, Nicholas WS, Cheng Han Ng, Darren Jun Hao Tan, et al. "The global burden of metabolic disease: Data from 2000 to 2019". Cell Metabolism 2023, 35, 414–428. [CrossRef] [PubMed]
- Rechel, Bernd, Yvonne Doyle, Emily Grundy, et al. "How can health systems respond to population ageing?". Technical Report. World Health Organization Regional Office for Europe, Copenhagen. 2009.
- Haq, Gary, Gloria Gutman. "Climate gerontology: Meeting the challenge of growing old in a changing climate". Zeitschrift für Gerontologie und Geriatrie 2014, 47, 462–467. [CrossRef] [PubMed]
- Meade, Robert D., Ashley P. Akerman, Sean R. Notley, et al. "Physiological factors characterizing heat-vulnerable older adults: a narrative review". Environment international 2020, 144, 105909. [CrossRef] [PubMed]
- GOV £10.7 million in funding for local authorities to improve air quality - GOV.UK (www.gov.uk). 2023a. accessed 21/07/2023.
- GOV https://www.gov.uk/guidance/driving-in-a-clean-air-zone. 2023b. accessed 24/07/2023.
- Chamberlain, Rosemary C., Daniela Fecht, Bethan Davies, et al. "Health effects of low emission and congestion charging zones: a systematic review". The Lancet Public Health 2023, 8, e559–e574. [CrossRef]
- GOV New legally binding environment targets set out. https://www.gov.uk/government/news/new-legally-binding-environment-targets-set-out, 2022, accessed 1/2/2023. 2022.
- Vandyck, Toon, Kimon Keramidas, Alban Kitous, et al. "Air quality co-benefits for human health and agriculture counterbalance costs to meet Paris Agreement pledges". Nature communications 2018, 9, 4939. [CrossRef] [PubMed]
- Ao C-K., Dong Y. and Kuo P-F. Industrialization, indoor and ambient air quality, and elderly mental health. China Economic Review 2021, 69, 101676. [CrossRef]
Figure 2.
Mean PM2.5 concentrations reported in the 16 studies mapped against WHO AQGs. Green bars indicate a detrimental relationship between PM2.5 and cognition variables. Amber bars indicate no relationship was found.
Figure 2.
Mean PM2.5 concentrations reported in the 16 studies mapped against WHO AQGs. Green bars indicate a detrimental relationship between PM2.5 and cognition variables. Amber bars indicate no relationship was found.
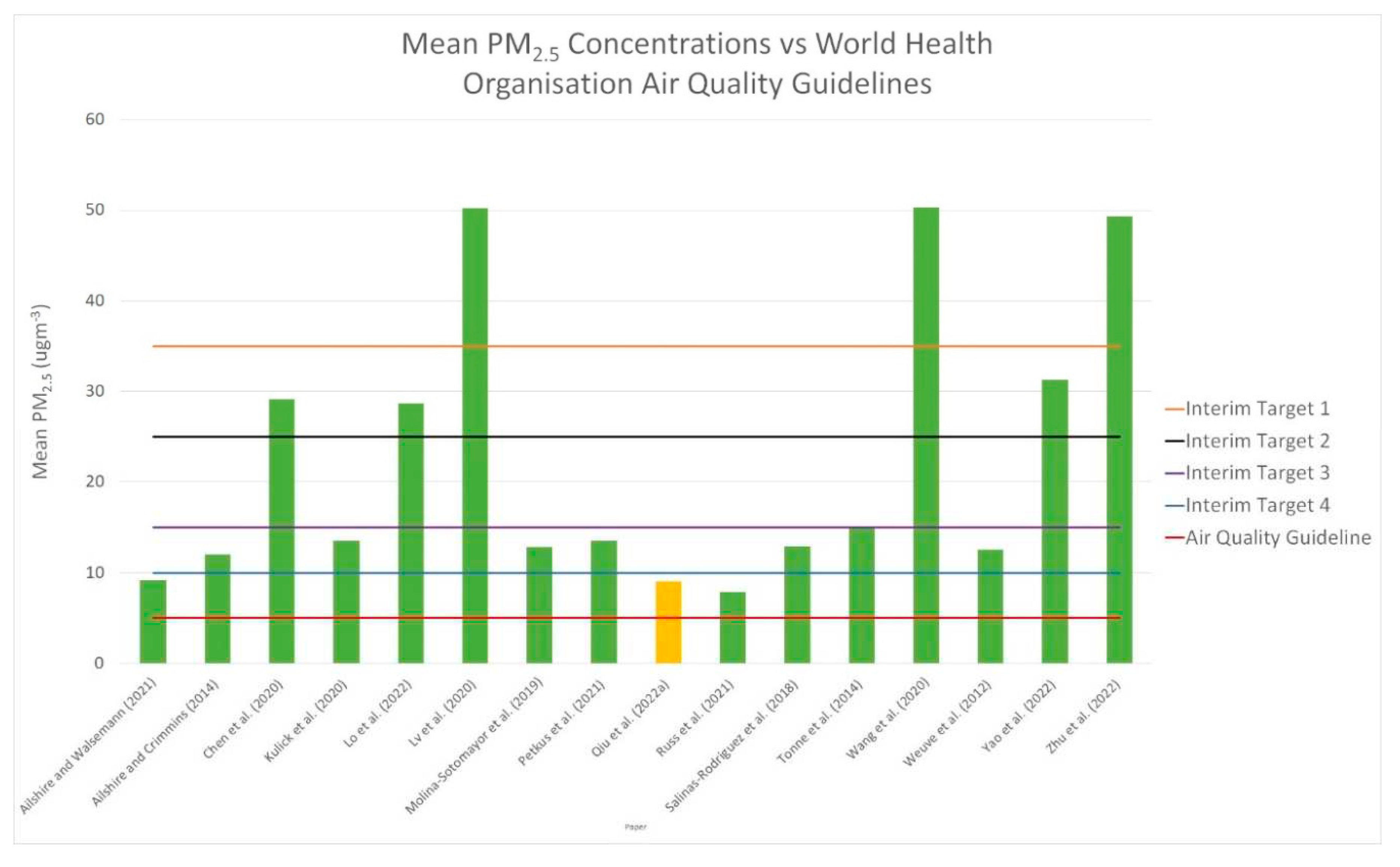

Table 1.
Changes in the World Health Organisations Air Quality Guidelines.
| Pollutant | Averaging Time | WHO 2005 Guideline | WHO 2021 Update | ||||
|---|---|---|---|---|---|---|---|
| Interim Targets | Guideline | ||||||
| 1 | 2 | 3 | 4 | ||||
| Fine Particles, PM2.5 | Daily (24 hour) mean (μgm-3) | 10 | 35 | 25 | 15 | 10 | 5 |
Table 2.
Selected articles related to cognition, older adults and air pollution.
| Authors | Title | Published | Country | OECD /LMIC | Maximum Cohort number |
Gender Male/Female (in %) | Reported level of education | Wealth |
|---|---|---|---|---|---|---|---|---|
| Ailshire and Walseman | Education differences in the adverse impact of PM2.5 on incident cognitive impairment among U.S. older adults | 2021 | United States | OECD | 5,636 | 46/54 | 59%, 12 years of education | Majority high paid workers |
| Ailshire and Crimmins | Fine particulate matter air pollution and cognitive function among older US adults | 2014 | United States | OECD | 13,996 | 44/56 | Mean 14 years of education | No data |
| Chen et al. | Long-Term exposure to air pollutants and cognitive function in Taiwanese community-dwelling older adults: A four-year cohort study | 2021 | Taiwan | OECD | 605 (305 at follow up) | 46/54 | Mean 14 years of education | No data |
| Kulick et al. | Long-term exposure to ambient air pollution, APOE-ε4 status, and cognitive decline in a cohort of older adults in northern Manhattan | 2020 | United States | OECD | 4,821 | 32/68 | Mean 9 years of education | No data |
| Lo et al. | Air pollution associated with cognitive decline by the mediating effects of sleep cycle disruption and changes in brain structure in adults | 2022 | Taiwan | OECD | 4,866 | 69/31 | Mean 10 years of education | No data |
| Lv, et al. | Long-term exposure to PM2.5 and incidence of disability in activities of daily living among oldest old | 2020 | China | OECD | 15,453 | 44/56 | 67% illiterate 33% literate |
No data |
| Molina-Sotomayor et al. | Effects of cardiorespiratory exercise on cognition in older women exposed to air pollution | 2019 | Chile | LMIC | 181 | All women | No data | No data |
| Petkus et al. | Outdoor air pollution exposure and inter-relation of global cognitive performance and emotional distress in older women | 2021 | United States | OECD | 6,118 | All women | 71% higher educated | Assumed wealthier |
| Qiu et al. | Associations between air pollution and psychiatric symptoms in the Normative Aging Study | 2022 | United States | OECD | 570 | All men (veterans) | 13% higher educated | No data |
| Russ et al. | Life course air pollution exposure and cognitive decline: Modelled historical air pollution data and the lothian birth cohort 1936 | 2021 | Scotland UK | OECD | 572 | 53/47 | 28% higher educated | No data |
| Salinas-Rodríguez et al. | Exposure to ambient PM2.5 concentrations and cognitive function among older Mexican adults | 2018 - 2021 | Mexico | LMIC | 7,986 | 46/54 | No data | No data |
| Tonne et al. | Traffic-related air pollution in relation to cognitive function in older adults | 2014 | UK | OECD | 3,414 | 65/35 | 39% higher educated | 41% high paid |
| Wang et al. | Fine particulate matter and poor cognitive function among Chinese older adults: Evidence from a community-based, 12-year prospective cohort study | 2020 | China | 13,324 | 48/52 | 59% illiterate | No data | |
| Weuve et al. | Exposure to particulate air pollution and cognitive decline in older women | 2012 | United States | OECD |
19,409 | All women | 100% graduate nurses |
No data |
| Yao et al. | The effect of China's Clean Air Act on cognitive function in older adults: a population-based, quasi-experimental study | 2022 | China | OECD | 2,812 | 50/50 | No data | No data |
| Zhu et al. | Interaction between plant-based dietary pattern and air pollution on cognitive function: a prospective cohort analysis of older adults | 2022 | China | OECD | 6,525 | 49/51 | 48% formal education | 35% ‘financially independent’ |
Table 3.
Details of monitoring and modelling methods utilised as well as validation and pollution averaging periods.
Table 3.
Details of monitoring and modelling methods utilised as well as validation and pollution averaging periods.
| Authors | Publication | Country | Monitoring Method | Modelling Method | Validation Method | Averaging Period(s) |
|---|---|---|---|---|---|---|
| Ailshire and Walseman | 2021 | United States | United States Environmental Protection Agency (USEPA) monitoring stations | Gridded 12km model | None stated – utilising USEAP model | Annual average concentration |
| Ailshire and Crimmins | 2014 | United States | USEPA monitoring stations | Inverse distance weighting of monitoring stations to participant census tract | None stated | 24 hour mean |
| Chen et al. | 2021 | Taiwan | Taiwan Environmental Protection Administration monitoring stations | Bayesian maximum entropy | None stated | Annual mean concentration |
| Kulick et al. | 2020 | United States | USEPA monitoring stations | Universal kriging | None stated | Annual Average |
| Lo et al. | 2022 | Taiwan | Taiwan Environmental Protection Administration monitoring stations | Hybrid kriging-land-use regression | None stated | Daily concentrations aggregate to annual average |
| Lv, et al. | 2020 | China | Satellite, simulation and monitoring stations utilised to estimate resident exposure. | Not specified | Out-of-sample cross-validation with monitors | Annual concentration over 4 time points (2002, 2005, 2008, 2011) |
| Molina-Sotomayor et al. | 2019 | Chile | Not specified | Not specified | Not specified | Annual average (2012, 2013, 2014) |
| Petkus et al. | 2021 | United States | USEPA monitoring stations | Regionalised universal kriging | None stated | Annual mean concentration |
| Qiu et al. | 2022 | United States | USEPA monitoring stations, satellite-derived measurements | Machine-learning algorithms using geographically weighted regression | Cross-validated to monitored values | Averages of 1 week, 4 weeks, 8 weeks and one year prior to the visit |
| Russ et al. | 2021 | Scotland UK | N/A | EMEP4UK atmospheric chemistry transport model | Validated against UK monitoring stations | Annual mean PM2.5 concentration (1935, 1950, 1970, 1980, 1990, 2001) |
| Salinas-Rodríguez, et al. | 20182021 | Mexico | N/A | Aerosol optical depth information retrieved from remote sensing data. Combination of observations from the Moderate Resolution Imaging Spectroradiometer and Multiangle Imaging Spectroradiometer instruments on the Terra satellite (NASA satellites), and simulations with the Goddard Earth Observing System (GEOS) chemical transport model. | None stated | Annual average |
| Tonne et al. | 2014 | UK | N/A | KCLurban and CMAQ-Urban models | Validated against monitoring stations | 1-, 3- and 5-year average |
| Wang et al. | 2020 | China | N/A | Utilised aerosol optical depth data with a land-use regression model. | Global ground-based stations and geographical weighted regression method. | Averaged for study period as well as 3 years prior to recruitment |
| Weuve et al. | 2012 | United States | USEPA monitoring data | Geographic information system-based spatiotemporal smoothing | Not stated | 1 month and 7-14 year exposures |
| Yao et al. | 2022 | China | N/A | Atmospheric chemical transport model. | Not stated | Annual average concentration |
| Zhu et al. | 2022 | China | Remote sensing, Multiangle Imaging SpectroRadiometer and Sea-viewing Wide Field-of-view Sensor satellite instrument, vertical profiles derived from the GEOS-Chem chemical transport model | Utilised monitoring data previously described | Ground-based observations using geographically weighted regression | Annual mean from 1998-2014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



