Submitted:
06 November 2023
Posted:
08 November 2023
You are already at the latest version
Abstract
Background: Citicoline, a medical food, lacks proven efficacy for ischemic stroke and has uncertainties around its harms. The continued prescription should be reevaluated given the more robust, high-quality Evidence against that medical food. This essay is based on a recent Cochrane review and uses only one all-cause mortality as the primary outcome. Therefore, the essay should be considered as something other than an updated Cochrane review but like a reflection based on Evidence-based Medicine and Philosophy of Science analysis.
Question Research: Why citicoline (a medical food) should not be prescribed to treat people with acute ischemic stroke: The certainty of the Evidence.?
Objective: Demonstrate from evidence-based medicine and philosophy of science perspective that citicoline should not be prescribed for acute ischemic stroke due to lack of efficacy and harm uncertainties.
Search publications: We searched in PubMed and Cochrane Library from 2020 until 30 October 2023. We, furthermore, used engineering machines Bing and Google Scholar to detect additional papers. Additionally, we also reviewed reference lists of the retrieved publications and review articles and searched the websites of the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA).
Selection criteria: We included systematic reviews, meta-analyses, randomized clinical trials, clinical guidelines focused on acute ischemic stroke and comparing citicoline versus placebo or no intervention. We excluded narrative reviews, observational studies and ongoing trials.
Data collection and analysis: We identified only new randomized clinical trials and assessed the risk of bias in seven domains. The other eight trials were already included in the mentioned Cochrane review. The systematic reviews with or without meta-analyses were assessed using McMaster University guidelines. We estimated risk ratios (RRs) for that outcome. We measured statistical heterogeneity using the I² statistic. We conducted our analyses using the fixed effect model. We did not use the GRADE approach due to what is shown in a Cochrane review published in 2020 by Martí-Carvajal et al. We used the RevMan 5.4 software from Cochrane Collaboration to conduct the forest plot. We used a Trial Sequential Analysis with Copenhagen Trial Unit Software. We estimated a Bayes factor from the relative risk and 95% confidence interval.
Results: We identified only one new RCT (N = 99) reported mortality data and three clinical guidelines. We conducted a new meta-analysis with nine trials (N = 4461) having a high risk of bias and showing little to no difference in mortality between citicoline and placebo (17.1% vs 18.4%; RR 0.94, 95% CI 0.82 to 1.06; I2 = 0%). The Bayes factor was 0.7, indicating weak Evidence for the null over the alternative hypothesis. Trial sequential analysis suggested sufficiency of Evidence for mortality. No guidelines recommend citicoline.
Conclusions: This essay reassessed citicoline for acute ischemic stroke after the 2020 Cochrane review. Adding a new RCT further supported the lack of mortality benefit with citicoline. The overall evidence quality could be better. Analyses using evidence-based medicine and philosophy of science approaches do not support prescribing citicoline due to a lack of efficacy substantiation and potential harms.
Keywords:
Citicoline
; Medical Food
; Acute Ischemic Stroke
; Evidence-based Medicine
; Philosophy of Science

1. Introduction
1.1. Acute Ischemic Stroke: A Brief Overview
To accurately define ischemic stroke, it is essential to consider both clinical symptoms and evidence of infarction, providing a comprehensive understanding of the ischemia experienced by a patient. In cases of brief focal arterial ischemia lasting less than 24 hours without signs of infarction (either through pathology or imaging), the condition should be categorized as a transient ischemic attack (TIA).1 Central nervous system infarction is defined as cell death in the brain, spinal cord, or retina due to ischemia, as evidenced by pathology, imaging, or other objective indicators of focal ischemic injury in a defined vascular distribution. Additionally, clinical evidence based on symptoms persisting for 24 hours or more, or until death, with other etiologies ruled out, is required.1
Acute ischemic stroke can be categorized into various types. The Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification system delineates ischemic stroke into five categories: 1) large-artery atherosclerosis, 2) cardioembolic events, 3) small vessel occlusion, 4) stroke of other determined etiology, and 5) stroke of undetermined etiology.2
Stroke remains a significant public health concern in the U.S., with an estimated 7 million Americans over 20 years of age having experienced a stroke. In 2016, there were nearly 800,000 new stroke incidents and 150,000 stroke-related deaths. The annual economic burden of stroke is substantial, costing the U.S. healthcare system approximately $45 billion. However, there has been a decline in incidence since 1999, attributed to better control of cardiovascular risk factors and advances in preventative treatments for arrhythmias. Despite this progress, more assertive prevention efforts, particularly focused on aging populations, are still imperative.3-4
The economic toll of stroke is indeed significant, with an estimated annual cost of $45.5 billion during the 2014-2015 period.4 This financial burden underscores the need for effective interventions and public health initiatives. In essence, while strides have been made in stroke management and prevention, the substantial impact of stroke in both human and economic terms highlights the urgency for continued research and effective public health strategies. The clinical guidelines provide a comprehensive roadmap for the care of acute arterial ischemic stroke in adults, covering the continuum of care from the prehospital setting to hospital management, and emphasizing the initiation of secondary preventive measures within the first two weeks of the event. The integration of stroke systems, encompassing both prehospital and hospital settings, is a fundamental aspect of these recommendations.5-7 In conclusion, the guidelines offer general advice based on the current evidence for physicians caring for adult patients with acute arterial ischemic stroke. However, it is important to acknowledge that existing data are often limited, highlighting the urgent need for ongoing research to further elucidate the treatment of this challenging condition. Saving lives and preventing debilitating outcomes will require not only the judicious application of current best practices but also an unwavering commitment to the pursuit of new knowledge.5-7
1.2. The Debate Surrounding Medical Foods and Supplements
In the vast spectrum of potential interventions, a particular class of treatment has stirred significant debate: medical foods and supplements. Citicoline, a medical food, has found itself at the center of this discourse (EFSA Panel 2013)1.8
Figure 1.
Citicoline. The structural formula of citicoline.
Initially heralded for its purported neuroprotective properties, the promise of citicoline was that it might aid the brain's recovery post-stroke. However, as is often the case in the realm of medical science, early enthusiasm was met with subsequent scrutiny. Preliminary studies hinting at benefits were later juxtaposed against more rigorous evaluations that cast doubt over citicoline's efficacy. This dichotomy has not just sparked academic debates but has instigated broader contemplations about the ethics and implications of prescribing treatments shrouded in uncertainty.
According to the U.S. Food and Drug Administration's explicit guidance9 and the European Union10, citicoline is a medical food or a supplement, not medication or drug.
The FDA defines medical foods as "a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation"16. Furthermore, it states that "Medical foods are not drugs and, therefore, are not subject to any regulatory requirements that specifically apply to drugs".16
The European Commission authorized citicoline as a novel food ingredient under food laws—neither categorized citicoline as a drug.10 Citicoline's specifications approved uses, and labeling aligned with a food framework in major regulatory jurisdictions. The totality of evidence indicates citicoline is considered a medical food or food ingredient, not a drug. Statements from the FDA and EU leave no room for interpretation and have definitively settled the issue: Citicoline is not a drug.
The World Health Organization's ATC/DDD system provides specifics about the classification and defined daily dose for citicoline.11 ATC stands for Anatomical Therapeutic Chemical Classification System, which categorizes medicinal products based on the organ or system they act on and their therapeutic, pharmacological and chemical properties. DDD stands for Defined Daily Dose. It is the assumed average daily maintenance dose for a medicine's main indication in adults. The ATC/DDD system maintained by WHO categorizes citicoline under the code N06BX06. This signifies:
- N06BX - Other psycho-stimulants and nootropics, a subgroup under the wider category of psycho-stimulants (N06B).
- N06BX06 - The specific code for citicoline as an individual nootropic agent.
The Defined Daily Dose for citicoline is 0.8 grams, taken orally. This is the assumed average daily maintenance dose when used therapeutically. So in the ATC/DDD system, citicoline is classified as a psycho-stimulant nootropic. This provides a specification for global comparison and analysis.11
1.3. Relevance and Role of the Triadic Conceptual Graph
This essay employs a triadic conceptual framework, visually represented in the initial graph to navigate this intricate tapestry of evidence, philosophical considerations, and clinical realities. This illustration is not merely an aesthetic inclusion but serves as a navigational compass, elucidating the intersections of Evidence-Based Medicine (EBM), the Philosophy of Science, and citicoline. By providing this snapshot at the outset, readers are equipped with a mental map, guiding them through the nuanced discussions that follow.
Figure 2.
Relationship between Evidence-based Medicine (EBM), Citicoline and Philosophy of Science. The Triadic Conceptual Graph: An Essence.
Figure 2.
Relationship between Evidence-based Medicine (EBM), Citicoline and Philosophy of Science. The Triadic Conceptual Graph: An Essence.
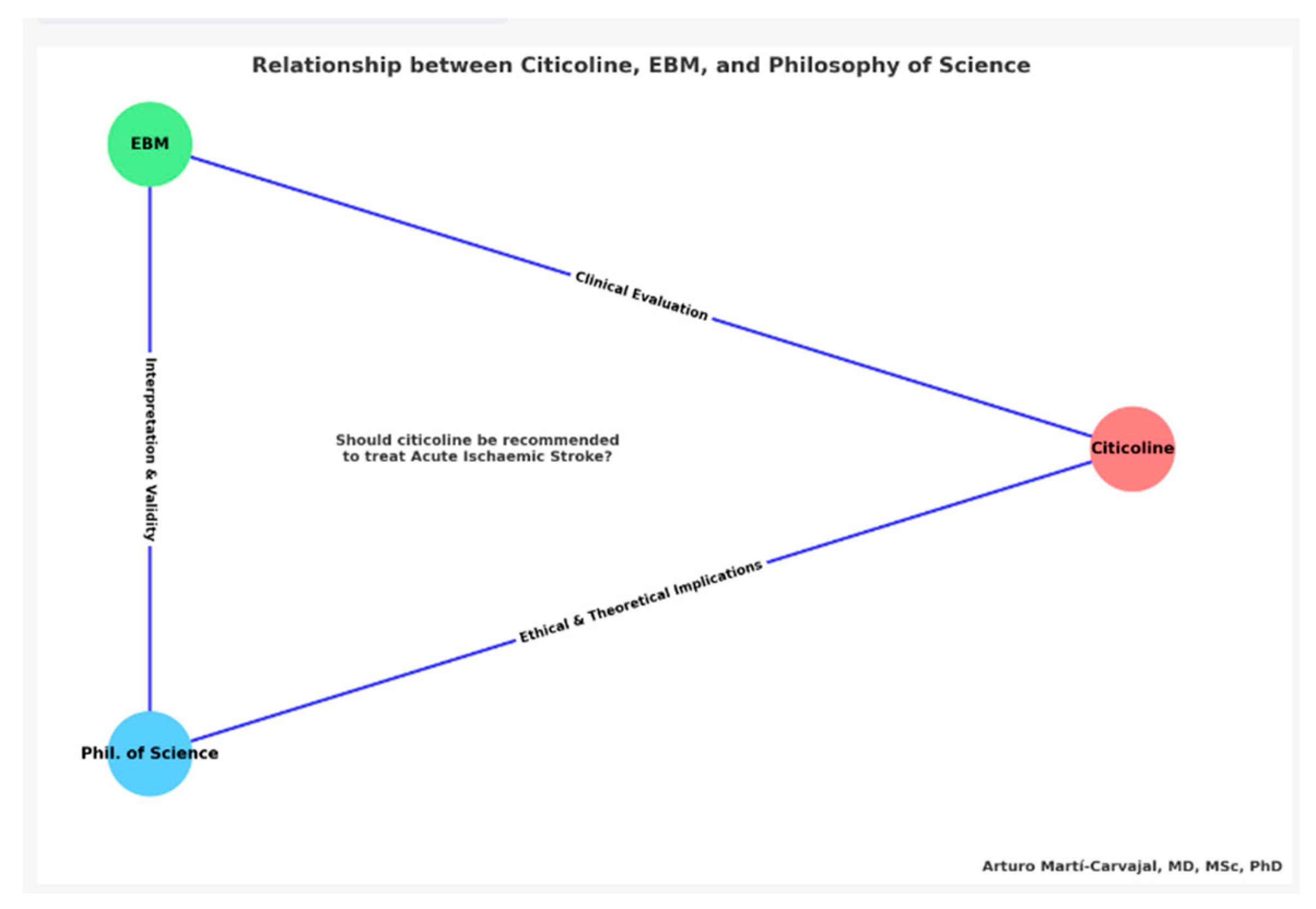
At the crux of this analytical piece, we navigate through a triadic conceptual graph, intricately woven to explore the intricate dynamics between Evidence-Based Medicine (EBM), the Philosophy of Science, and citicoline in acute ischemic stroke scenarios. This graph transcends mere aesthetic value, encapsulating the foundational beliefs of the essay and visually mapping out the complex interrelations among these pivotal domains.
1.3.1. The Bedrock and Cornerstone: Evidence-Based Medicine (EBM)
In our conceptual triad, the 'EBM' vertex stands resilient, serving both as the bedrock and cornerstone of our exploration. It epitomizes the stringent methodologies and guiding principles imperative for medical decisions rooted in systematically evaluated and critically reviewed evidence. This vertex draws strength from the pioneering works of Archibald 'Archie' L. Cochrane12 and David L. Sackett13-14, who fervently advocated for melding clinical acumen with the highest caliber of research evidence. Positioned at the triad’s foundation, EBM stands as the moral imperative for clinicians, beckoning them to harmonize their individual expertise with the paramount external evidence in their medical deliberations. EBM’s guiding light directs us toward systematic reviews, converging the apexes of clinical research to inform medical practice and elevate patient care to its zenith.
A key philosophical principle underpinning EBM is Ockham's razor15, which favors the simplest explanation supported by the evidence. This aligns with EBM's hierarchical prioritization of evidence quality, with randomized trials at the top. Ockham's razor reinforces EBM's wariness of anecdotal data or speculative pathophysiology as sole justification for treatments. Applying this to citicoline, the lack of robust efficacy and safety evidence in ischemic stroke points to discontinuing its prescription as the simplest conclusion, rather than hypothesizing unsubstantiated benefits and risks. As Simon and Rios16 stated, principles like Ockham's razor are crucial for evidence-based practice to avoid perpetuating unsupported interventions. Integrating such philosophy expands EBM's methodological rigor.
1.3.2. The Prism: Philosophy of Science
On the opposing end, the 'Philosophy of Science' vertex unravels the profound epistemological layers of scientific investigation. Illuminated by intellectual giants such as Karl Popper17 and the Vienna Circle18, this vertex scrutinizes the methodologies, ethical considerations, and foundational beliefs that sculpt our perception of scientific truth. The left vertex casts a philosophical gaze upon science, dissecting the methodologies, ethics, logic, and epistemology that constitute scientific knowledge. Figures like Sir Karl Popper, Michel Foucault and Sir Peter Medawar have intricately woven the fabric of understanding, dictating how scientific theories are birthed, validated, and embraced. Through the philosophy of science’s lens, we critically appraise the underlying biases, contexts, and assumptions permeating biomedical research.
1.3.3. The Exemplar: Citicoline
The 'Citicoline' vertex, positioned at the triad’s pinnacle, symbolizes the medical food attributed with neuroprotective potentials, serving as the essay’s focal case study.16 Citicoline, believed to offer neuroprotection post-acute ischemic stroke, stands as the concrete example scrutinized through the EBM and Philosophy of Science frameworks. In this crucible of medicine, citicoline manifests as a nexus where ethical considerations, scientific validation, and philosophical introspections converge.
1.3.4. The Unifying Query
Interlinking these domains is the pivotal question: Is citicoline a viable prescription for acute ischemic stroke patients? This inquiry, deeply entrenched in efficacy, safety, and ethical considerations, propels our exploration forward. The triadic synergy of EBM, philosophical inquiry, and the citicoline discourse amalgamates to scrutinize this central dilemma.
In essence, the triadic graph serves as a conceptual compass, guiding us through the pivotal realms of evidence-based medicine, scientific philosophy, and the nuanced clinical debate surrounding citicoline. Both visually and narratively, the graph sheds light on the synergistic integration of these elements, informing the pivotal question regarding citicoline’s role in clinical practice. At the triangle’s heart, the urgent research inquiry arises, tying together the vertices and encouraging a holistic evaluation of citicoline, transcending empirical evidence and delving into philosophical depths. This graph, therefore, encapsulates the essay’s odyssey, a quest through evidence, philosophical inquiry, and clinical realities, in pursuit of answers with far-reaching implications for patient care and societal well-being.
2. Research Question
Why citicoline (a medical food) should not be prescribed to treat people with acute ischemic stroke: The certainty of the evidence?
The journey of scientific discovery often mirrors the profound depths of linguistic etymology, weaving a rich tapestry of history, meaning and potential. The term "etiology" epitomizes this parallel. Derived from the Greek words "aitia" (cause) and "logos" word proposed by Heraclitus of Ephesus in 540 BCE (study, reason), etiology encapsulates the relentless quest to comprehend causation and the origins of phenomena.
In medicine, and specifically in investigating acute ischemic stroke, unraveling etiology acquires crucial significance. Like skilled linguists deciphering semantic evolution, physicians probe complex pathophysiology, seeking reasons and definitive evidence to guide therapeutic choices. At this crossroads, armed with robust research methodology and an unwavering spirit of inquiry, the scientific community strives to illuminate the obscured etiology of disease and construct the most apt interventions.
In this spirit, we explore a compound that holds promise against the ravages of acute ischemic stroke – citicoline. The scientific world anticipates robust etiological understanding that could elevate citicoline from possibility to proven prescription. Nevertheless, assertions require rigorous scrutiny; potential must transition to evidence-based efficacy before infiltrating clinical practice.
With ethical principles as our guideposts, we embark on an odyssey through clinical trials and systematic insights, seeking the elusive etiology that transforms therapeutic speculation into a confident recommendation. Like language detectives united by curiosity, we persevere until science speaks clearly.
This spirit of scientific rigor and objective analysis, guided by principles of beneficence and nonmaleficence (First, do not harm!) leads us to investigate the central research question systematically: Should citicoline be prescribed for individuals with acute ischemic stroke? The answer awaits at the journey's end.
3. Objective
Our primary aim in this essay is to conduct a rigorous analysis of citicoline's clinical effectiveness and examine the ethical dimensions surrounding its use for acute ischemic stroke. We approach this evaluation through the lenses of Evidence-Based Medicine and Philosophy of Science, incorporating insights from esteemed thinkers like Michel Foucault, Sir Karl Popper, and Sir Peter Medawar. While citicoline's intricate pharmacodynamics and pharmacokinetics warrant exploration, dissecting these mechanisms in detail extends beyond the scope of this current work. We focus on synthesizing the highest quality clinical evidence regarding citicoline's efficacy and safety for acute ischemic stroke and weighing the implications of prescribing this medical food through an ethical lens. By integrating principles of clinical epidemiology and scientific philosophy, we seek to reach judicious conclusions rooted in both empirical data and moral reasoning, elucidating not just what can be done but what should be done to benefit patients in keeping with ethical medical practice.
4. Methodology: Navigating the Sea of Evidence
In scientific inquiry, methodology is the beacon that guides our exploration, ensuring that the journey is rigorous, systematic, and unbiased. Our methodology in this essay is rooted in a multidimensional approach, striving to balance empirical evidence, critical analysis, and best practices in research evaluation.
4.1. Sources of Data and Document Evaluation
Our starting point was a meticulous selection and evaluation of data sources. The vast expanse of biomedical literature, teeming with studies, reviews, and reports, necessitates a discerning eye. We focused on randomized clinical trials (RCTs) that emerged post-2020, ensuring their alignment with the criteria established by the Cochrane review on citicoline19. For this essay, each document underwent a thorough vetting process, evaluating its relevance, credibility, and contribution to the overarching research question. We searched in PubMed using the clinical query approaches recommended by that database and Cochrane Central Register of Controlled Trials (CENTRAL). Furthermore, we searched in Google Scholar and the search engine Bing from Microsoft. The search was limited to 2020 to October 15, 2023. We also searched Clinical Guidelines from scientific organizations for retrieving potential recommendations about the citicoline’s use in people with acute ischemic stroke.
In our rigorous journey to uncover the intricacies of citicoline’s role in acute ischemic stroke, we have meticulously chosen our sources of evidence, adhering to the highest standards of scientific inquiry. A pivotal decision in our methodology was to exclude either narrative reviews or ongoing trials from our pool of resources. This decision was rooted in our commitment to uphold the principles of Evidence-Based Medicine (EBM) and ensure the robustness of our conclusions.
Narrative reviews, while informative and often insightful, do not adhere to the systematic and transparent methods characteristic of systematic reviews and randomized controlled trials. They are typically authored based on the personal expertise and interpretative skills of the authors, and they may not follow a predefined protocol for literature search and selection. This subjective nature can introduce bias, as the selection of studies and the interpretation of results may be influenced by the authors’ perspectives and preferences.
In contrast, systematic reviews and RCTs offer a more objective and reproducible approach to evidence synthesis. They follow strict protocols for literature search, study selection, and data extraction, minimizing the risk of bias and ensuring that the conclusions drawn are based on a comprehensive and balanced view of the available evidence. By focusing on these sources, we aim to provide a more reliable and unbiased assessment of citicoline’s efficacy in acute ischemic stroke.
Our commitment to EBM principles guided our decision to exclude narrative reviews, as we sought to base our conclusions on the highest quality of evidence available. This approach ensures that our findings are grounded in robust scientific data, providing a trustworthy and valid contribution to the ongoing discourse on citicoline and acute ischemic stroke. This focused justification clarifies the rationale behind excluding narrative reviews, emphasizing the commitment to EBM principles and the pursuit of unbiased and reliable evidence.
We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram in this manuscript to demonstrate the author's firm commitment to the highest reporting standards for systematic reviews.20 However, we have clearly stated that this manuscript is not an update of the Cochrane review mentioned earlier.
Figure 3.
Deciphering the Tapestry of Research: A Comprehensive PRISMA-Guided Systematic Review on Citicoline in Acute Ischemic Stroke.
Figure 3.
Deciphering the Tapestry of Research: A Comprehensive PRISMA-Guided Systematic Review on Citicoline in Acute Ischemic Stroke.
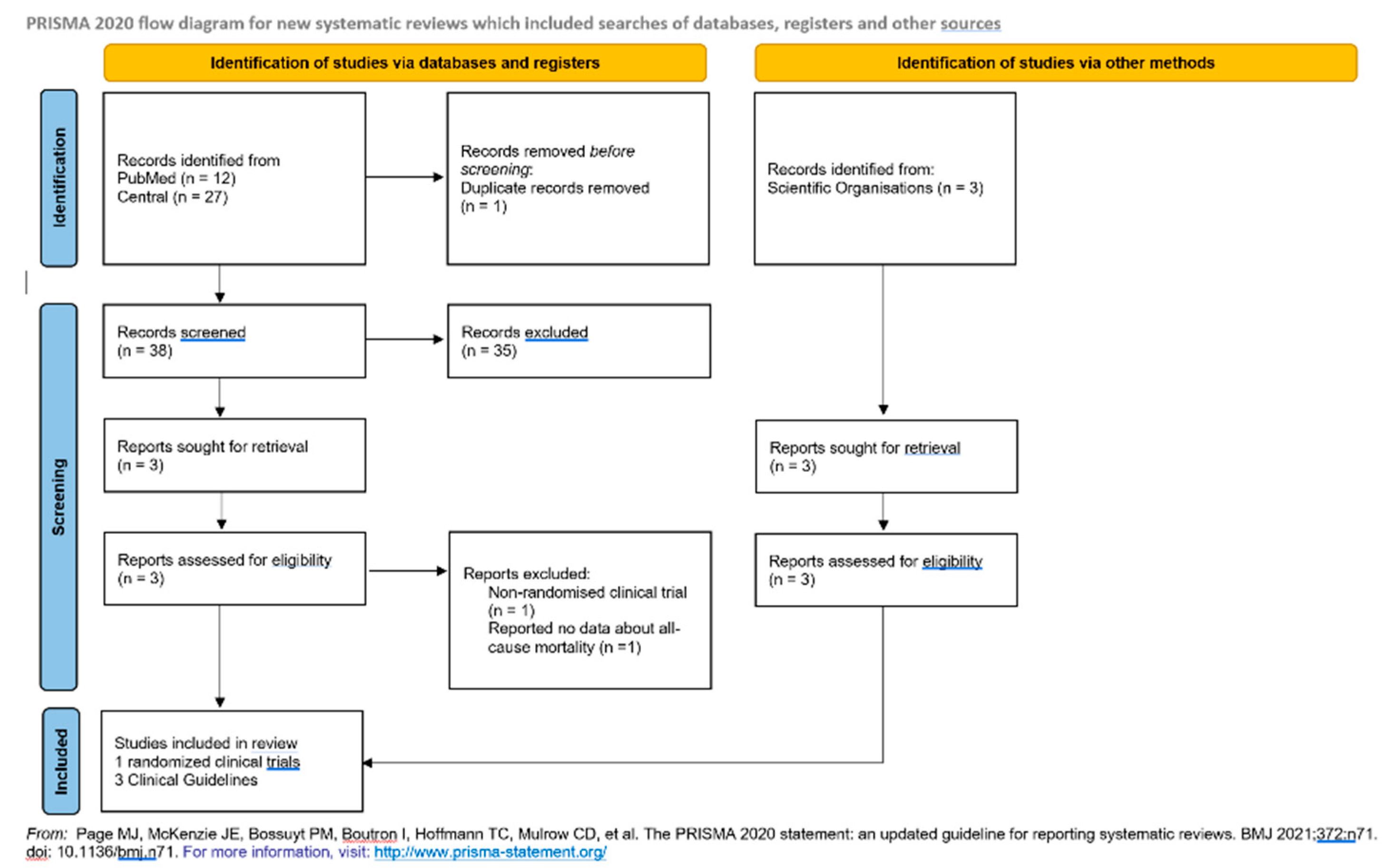
PRISMA is an evidence-based guideline that consists of a checklist and flow diagram to improve the reporting of systematic reviews and meta-analyses. By following PRISMA guidelines, the author provides complete transparency about their rigorous review methodology, thus increasing confidence in their findings. Specifically, the diagram details every step of the study selection process, from the comprehensive search across multiple sources through the careful application of eligibility criteria to the final decision of which studies to include in the synthesis. Readers can follow the path traced by the authors in their systematic pursuit of the best available evidence. The adherence to PRISMA, an established reporting guideline, sends an unambiguous signal: this is no rushed or sloppy work. Instead, it is a rigorous, meticulous, systematic review worthy of the highest consideration from the scientific community. The findings presented deserve to be taken seriously, given the painstaking process that produced them. In conclusion, the presence of a PRISMA flow diagram establishes the high methodological standards of this review and reaffirms the commitment to transparency and scientific excellence. Its inclusion warrants confidence and validation of the critical findings reported herein.
4.2. Application of Cochrane Collaboration Recommendations
The Cochrane Collaboration stands as a gold standard in the world of systematic reviews, renowned for its rigorous methodologies and dedication to evidence-based medicine. In our endeavor, we leaned heavily on the Cochrane Collaboration's recommendations20, especially in synthesizing and interpreting the data from various RCTs. Their guidelines offered a structured framework, enabling us to assess the quality of evidence, minimize biases, and derive meaningful conclusions about citicoline's efficacy in treating acute ischemic stroke. We conducted a new meta-analysis including a new RCT published in 2022.21. The meta-analysis was by subgroup due to the new RCT assessed citicoline administered immediately after recanalization therapy for acute ischemic stroke.21 No trial included Cochrane review19 had been used Agarwal’s approach. To assess the imprecision, we followed the recommendations from GRADE group.22 We limited this essay to the main primary outcome of the Cochrane review19: all-cause mortality. Full details about the other outcomes are available in Martí-Carvajal, et al.19
4.3. Critical Analysis of Biomedical Literature
A systematic review requires more than just a rigorous process - it demands critical analysis. We looked beyond the surface data, evaluating each trial and report as a product of its context, biases, and assumptions. In the construction of the evidence in this essay, our goal was not merely aggregating empirical findings, but gaining a complete picture of the evidence - both the tangible results and the wider scientific narratives that shape our comprehension. This comprehensive scrutiny and skepticism allow moving closer towards an accurate understanding of citicoline for stroke, though absolute truth likely remains elusive. A thoughtful systematic review illuminates both what we know and how we know it.
4.4. Trial Sequential Analysis
Our trial sequential analysis methodology aligns with the approach explained in detail by Martí-Carvajal, et al.19. In summary, adding the new RCT, we recalculated the required information size, or minimum sample size needed, accounting for heterogeneity and using a 20% relative risk reduction, 80% power, 5% alpha, and diversity adjustment.
Based on the required information size, I constructed trial sequential monitoring boundaries to assess whether the cumulative evidence definitively proves or disproves the hypothesized treatment effect before reaching the required sample size. Crossing the boundary indicates further trials are likely unnecessary, while not reaching the boundary signals additional trials are still needed. I applied trial sequential analysis software to evaluate if the cumulative meta-analysis crossed the futility boundary.
Per my typical approach, I only conducted trial sequential analysis for the primary outcome of all-cause mortality. This aligns with the methodology I have followed and described extensively in prior publications to optimize type I and II error control and objectively evaluate futility or conclusiveness of cumulative randomized evidence. I believe using trial sequential analysis provides a scientifically rigorous way to determine the need for additional trials. I conducted TSA using software from the Copenhagen Trial Unit.23
I reconducted the new TSA because we found one trial reporting all-cause mortality.21 It was an ongoing trial when the Cochrane review on citicoline was published in 2020.19
In sum, our methodology was a fusion of systematic processes, critical thinking, and philosophical inquiry, all converging to shed light on the central question of Citicoline's role in acute ischemic stroke management.
6. The Scaffold of Scientific Trust: Deciphering the Hierarchy of Evidence
In the grand tapestry of medical science, not all evidence is woven with the same thread. The strength, consistency, and reliability of scientific findings vary, necessitating a structured approach to discern the weight of different types of evidence. This is where the concept of the 'Hierarchy of Evidence' comes to the fore, acting as a beacon for clinicians and researchers navigating the vast seas of medical literature.25
6.1. The Essence of Evidence-Based Medicine (EBM)
Evidence-Based Medicine, at its core, is a commitment—a vow to ensure that clinical decisions are anchored in the most robust and relevant evidence available. But how does one determine what constitutes 'robust' evidence? EBM doesn't just champion the use of evidence; it emphasizes the quality of that evidence. The Hierarchy of Evidence25, in essence, is a tool that helps segregate studies based on their methodological rigor and susceptibility to bias. From case reports at the base to randomized controlled trials higher up, each rung of this ladder represents a different level of trustworthiness.
6.2. The Cochrane Review: A Gold Standard in Medical Research
Perched at the zenith of this hierarchical pyramid is the systematic review, and among them, the Cochrane systematic review is often considered the gold standard.20 Why? Because it embodies the very principles EBM holds dear: comprehensiveness, rigor, transparency, and a commitment to minimizing bias. Cochrane reviews synthesize the best available evidence on a given topic, subjecting individual studies to meticulous scrutiny and pooling data to provide a consolidated view. When it comes to understanding the role of citicoline in acute ischemic stroke, the Cochrane review serves as a lighthouse, illuminating the path with its rigorous analysis and evidence synthesis.
7. Diving into the Cochrane Systematic Review
The domain of medical inquiry is immensely broad, weaving a complex tapestry of studies, assertions, and counterarguments. Within this intricate expanse, systematic reviews stand as pivotal navigational beacons, with those orchestrated by the esteemed Cochrane Collaboration26 holding a particularly luminous position. These comprehensive analyses act as compasses, steering clinicians, researchers, and policymakers through the intricate maze toward conclusions grounded in robust evidence.
In this critical juncture of our exploration, we immerse ourselves in an in-depth examination of the Cochrane review that scrutinizes the role of citicoline in the management of acute ischemic stroke.19 This review, distinguished by its meticulous methodology and commitment to impartiality, serves as a cornerstone in our understanding, offering a well-rounded and discerning perspective on this pivotal medical inquiry.
We stand at the precipice, ready to unravel the layers, navigate the complexities, and derive clarity from the wealth of accumulated knowledge. It is through this lens of rigorous evaluation and keen insight that we endeavor to shed light on the intricate interplay of factors surrounding the use of citicoline, guiding our journey through the vast expanse of medical knowledge.
7.1. The Cochrane Gold Standard
The Cochrane Collaboration's stringent methodological criteria and commitment to minimizing bias ensure its systematic reviews represent the highest quality evidence.20
By meticulously combining individual studies and extracting meaningful truths, Cochrane reviews serve as a compass to guide understanding of healthcare interventions. In 2020, Martí-Carvajal et al. published a Cochrane review19 assessing the clinical benefits and harms of citicoline for treating acute ischemic stroke patients. This review was essential to evaluate citicoline amid conflicting prior evidence. While some studies suggested benefits, others showed no significant improvements versus placebo or controls. Furthermore, previous meta-analyses had limitations, including lack of Trial Sequential Analysis and suboptimal effect measures. With many industry-funded trials, independent assessment was needed. Despite inconclusive evidence, some countries still prescribed citicoline. By adhering to rigorous Cochrane methods, this review aimed to conclusively determine if citicoline provided meaningful clinical benefits and harms compared to other acute ischemic stroke treatments. The conclusion of the authors was (verbatim): This review assessed the clinical benefits and harms of citicoline compared with placebo or any other standard treatment for people with acute ischemic stroke. The findings of the review suggest there may be little to no difference between citicoline and its controls regarding all-cause mortality, disability or dependence in daily activities, functional recovery, neurological function and severe adverse events, based on low-certainty evidence. None of the included trials assessed quality of life and the safety profile of citicoline remains unknown. The available evidence is of low quality due to either limitations in the design or execution of the trials. For full details, readers can refer to Martí-Carvajal, et al 2020.19
7.2. Unraveling the Findings
At the intersection of hope and skepticism, where anecdotal experiences meet rigorous scientific scrutiny, the Cochrane review on citicoline offers a synthesized perspective. Drawing from a multitude of randomized controlled trials, it provides a panoramic view of citicoline's impact on acute ischemic stroke. The results, encapsulated visually in the forest plot, offer a clear picture of the effect sizes from individual studies and their combined influence.
Figure 4.
Forest plot depicting the effect of citicoline on all-cause mortality in people with acute ischemic stroke based on subgroup analysis.
Figure 4.
Forest plot depicting the effect of citicoline on all-cause mortality in people with acute ischemic stroke based on subgroup analysis.
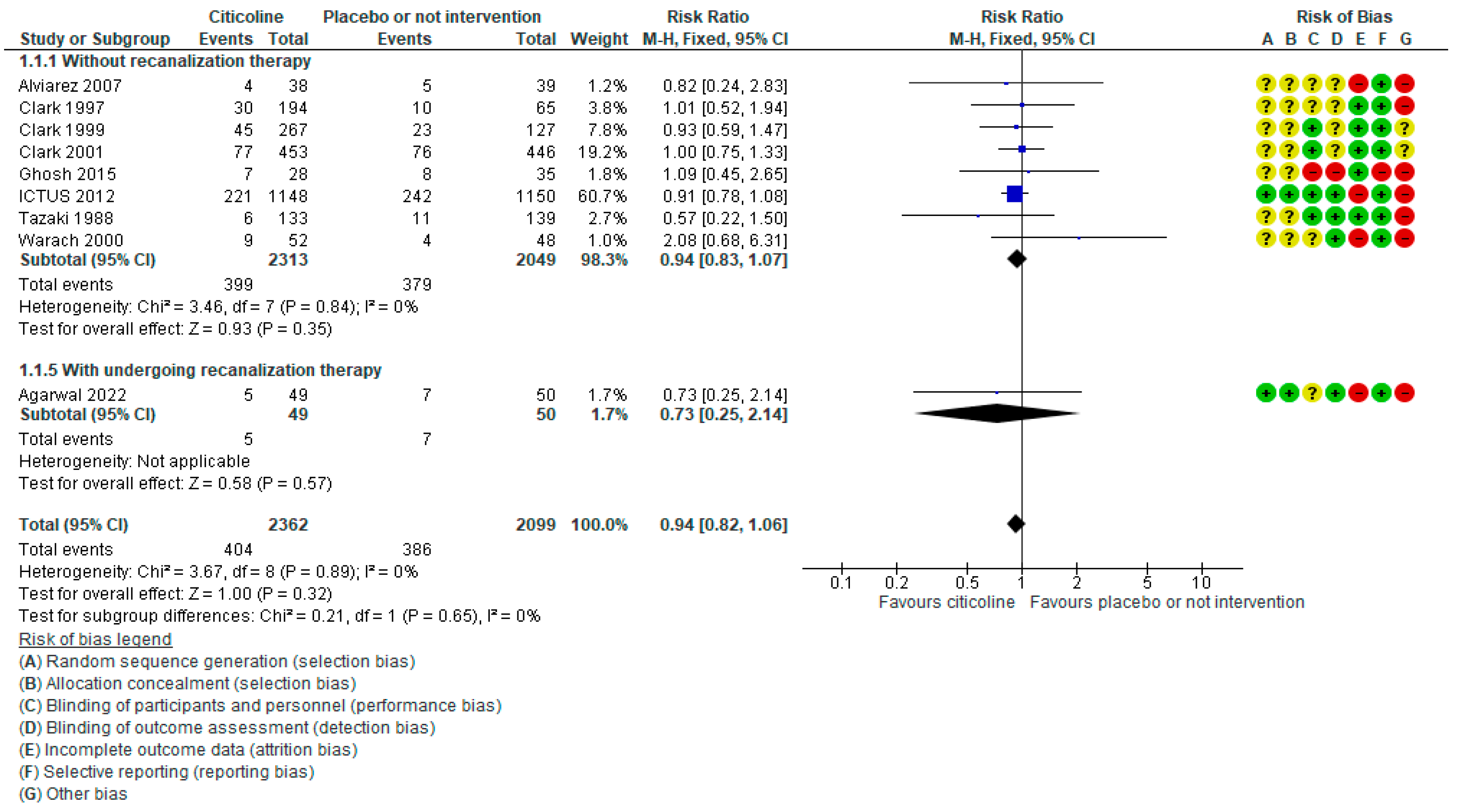
The forest plot displays the results of nine individual studies categorized into two subgroups. The horizontal lines represent 95% confidence intervals for each study's effect estimate. The squares denote the risk ratio point estimates, with the size of the square proportional to the study's weight in the meta-analysis. The vertical line indicates the null effect of relative risk = 1. The diamonds represent the pooled effect estimates from a meta-analysis using a fixed-effect model.
The first subgroup includes eight trials without recanalization therapy. The pooled risk ratio is 0.94 (95% CI 0.83 to 1.07), with low heterogeneity (I2 = 0%). The total sample size was 4362 patients, representing 13.65% of the optimal information size (4362/31900) required to detect a significant treatment effect conclusively. The 95% CI includes the possibility of no mortality benefit.
The second subgroup comprises one trial involving patients undergoing recanalization therapy.21 This trial showed a risk ratio 0.73 (95% CI 0.25 to 2.14). The sample size of 99 patients is 4.78% of the optimal information size (99/2070). The wide 95 % CI includes the possibility of no treatment effect.
The forest plot encompasses nine trials with 4461 participants. The overall meta-analysis risk ratio is 0.94 (95% CI 0.86 to 1.06, I2: 0%), suggesting no significant mortality reduction with citicoline compared to placebo/no intervention. The total sample represents 14% of the optimal information size required, indicating imprecision. Furthermore, the 95% CI includes the possibility of no benefit. The test for subgroup differences was P = 0.65 and I2: 0%. Bayes factor was 0.93, using the RR and its 95% CI of the meta-analysis. It indicates that the data is inconclusive - the evidence does not favor either the null hypothesis or the alternative hypothesis. The Bayes factor of 0.93 shows that the data do not provide enough evidence to conclude either way about the effect. More data would be needed to strengthen the evidence in favor of the null or alternative hypothesis.
The Bayesian analysis may be limited by potentially inappropriate prior and assumptions. With limited data, results can be sensitive to outliers. The analysis relied solely on the meta-analytic data without considering the broader theoretical and empirical landscape. While the Bayes factor is tentatively aligned with the lack of efficacy, over-interpreting statistical analyses without grounding in the literature can lead to spurious conclusions.
Based on the current evidence from this meta-analysis, there is no convincing mortality benefit for citicoline compared to placebo/no intervention in patients with acute ischemic stroke. The totality of data needs to be revised to demonstrate any treatment effect due to suboptimal sample size and imprecision. Additionally, the included trials have a high risk of bias, severely limiting the reliability of the results. There is no significant statistical heterogeneity.
In brief, the evidence firmly indicates citicoline provides no mortality advantage over placebo or standard care in acute ischemic stroke people. The meta-analysis results are decisively null regarding mortality reduction. The judgment of certainty is very low due to the imprecision and high risk of bias. Currently, the evidence convincingly fails to support using citicoline, a medical food, specifically to reduce mortality in this population.
Figure 5.
Mapping of Scientific Evidence on Citicoline in the Treatment of Acute Ischemic Stroke.
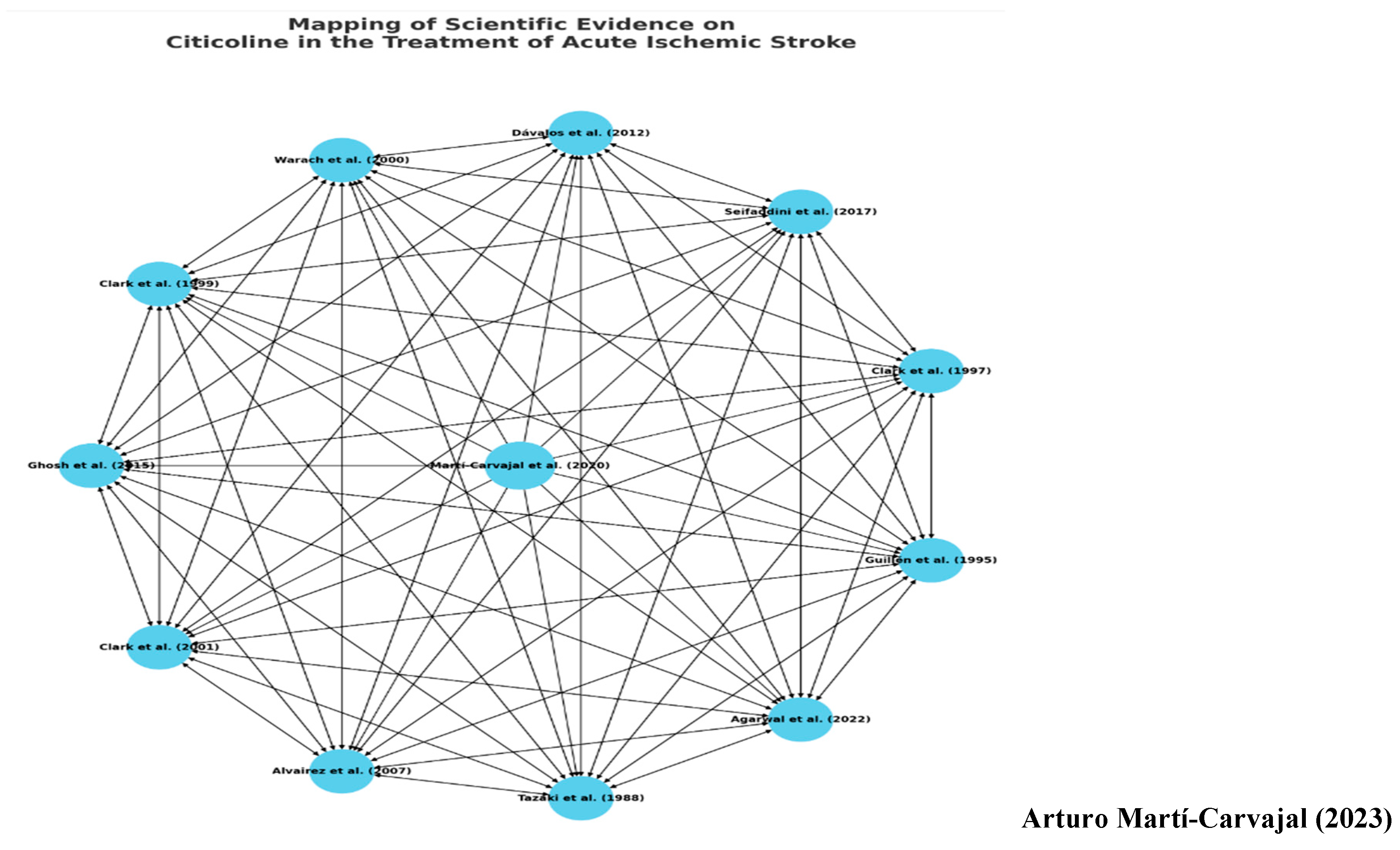
The graph unfolds as a meticulously constructed network of randomized clinical trials, each delving into the intricacies of citicoline’s role in treating acute ischemic stroke. In this visual representation, individual studies are denoted as nodes, while the edges draw lines of potential relationships and scholarly dialogues between them.
In scientific inquiry, each study is a beacon of knowledge, yet it does not stand in isolation. Much like the famous poet John Donne (1572–1631) once eloquently expressed, ‘No man is an island,’ this network of trials epitomizes the interconnected nature of scientific pursuit. The graph emphasizes that each piece of research, each node in this network, contributes to a collective understanding, building bridges of knowledge and insight across the expanse of medical literature. In essence, this visual narrative serves not just as a map of existing research but also as a reminder that in pursuing scientific truth, each study is a vital part of the greater whole, interconnected, and indispensable.
It remembers the critical thinking from Sir Peter Medawar, as mentioned. Specifically, Medawar's emphasis on focusing scientific inquiry on "soluble" questions which can advance understanding, rather than getting stuck on insoluble problems, is tremendously valuable advice.
As Medawar elegantly states: "There are questions which science cannot answer, and it is no good beating one's head against these questions. What matters is to learn to discriminate between soluble questions with real and accessible answers, and questions that are beyond solution for the time being." This highlights the wisdom of channeling curiosity toward questions matched to current capabilities, while appreciating present limitations. Progress lies in pursuit of the soluble. Medawar also astutely notes that even incorrect answers can unveil fragments of truth and "expose the substratum on which truth rests." Science expands its edifice brick by brick through this spirit of imaginative, yet grounded, inquiry. These philosophical principles remain highly pertinent, both broadly to research methodology and specifically to exploring controversial areas like the citicoline debate. Focusing on judiciously framed, tractable questions allows the gradual accretion of knowledge.
Martí-Carvajal, et al.19, standing as the root of this intricate network, occupies a central position, symbolizing its comprehensive nature and its pivotal role in analyzing multiple studies on the topic. As a Cochrane review, it holds a high standard of evidence, serving as a linchpin in the network and a reliable guide for clinical decision-making.
The other nodes, representing various randomized clinical trials, showcase the diverse investigations conducted over the years, each contributing unique insights into the effects of citicoline across different settings and populations. These studies are not isolated islands of knowledge; they are interconnected parts of a larger conversation, contributing to and influenced by the collective understanding synthesized in the Cochrane review.
The edges, or connections, represent the relationships between the studies, highlighting how each is interconnected, complementing, contrasting, and contributing to the broader research landscape on citicoline in acute ischemic stroke.
The node sizes visually represent the relative importance or weight of the studies, with the Cochrane review standing out due to its comprehensive and systematic nature, serving as a testament to the power of collective inquiry and the crucial role of systematic reviews in navigating the complex seas of medical research.
7.3. Beyond Numbers - Implications for Practice
While the data and statistics form the backbone of the review, their actual value lies in their clinical implications. How does the evidence from the Cochrane review translate to bedside decisions? What does it mean for a patient with acute ischemic stroke awaiting treatment decisions? These are the pressing questions this section seeks to answer, marrying numbers with narratives and research with real-world ramifications. It is the essence of this essay: First, do not harm! This paragraph brings to Sir Karl Popper’s thoughts27. Evidence-based medicine, though accused of dogmatism, strongly aligns with Karl Popper's falsification principles. At its core, robustly testing medical claims against empirical scrutiny. This spirit of critical inquiry, of tentatively gleaning truth through refutation, permeates EBM’s essence. Yet clinical practice demands more than an abstract search for statistical certainty. It requires a profoundly humanistic approach centered on understanding patients' values and goals. Formulating the initial question reveals this truth. It necessitates appraising internal expertise and anticipating real-world applicability. But crucially, it involves an intimate exploration of patients’ preferences to establish mutually agreeable objectives. Here, we grapple with ethically complex decisions affecting others’ wellbeing. Mastering empathy, counseling, and narrative medicine becomes vital to properly frame the clinical question. We must see our patients not as data points or outcomes, but as people hoping to be heard, understood, and empowered. Evidence-based medicine, robustly practiced, is this weaving together of science and compassion. The meticulous examination of research evidence requires pairing with the humanistic art of opening dialogue. In this full embodiment of EBM, we stay grounded in the Popperian principles of critical thinking while elevating care to an act of moral agency and human connection.27
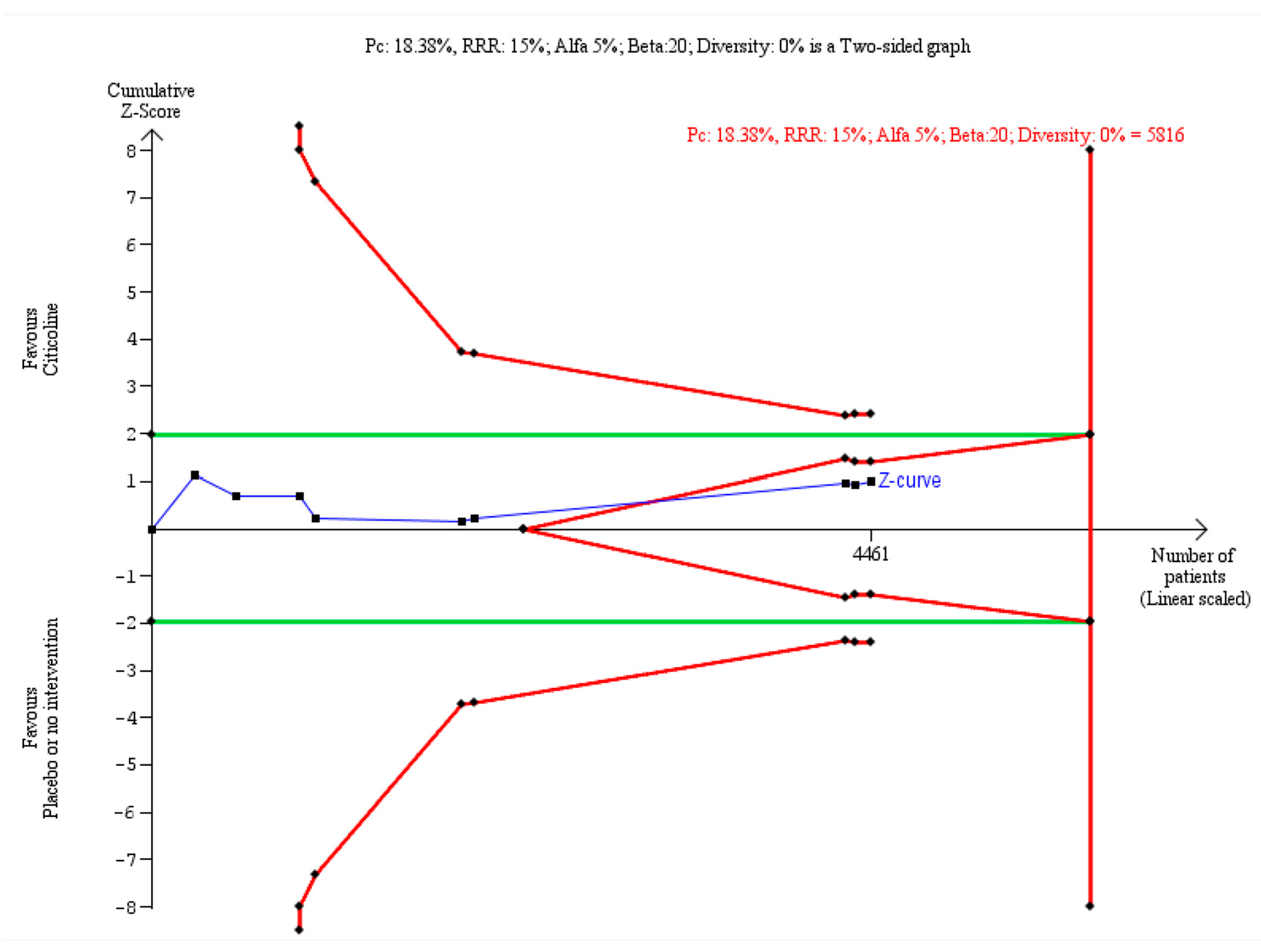
7.4. Trial Sequential Analysis (TSA) - The Final Seal
Supplementing the systematic review's findings, the TSA offers another layer of evidence.28 By visually depicting the trajectory of cumulative data, it can demonstrate whether more trials on citicoline are warranted or if the evidence has reached a point of futility. In the case of citicoline, the TSA provides compelling insights into the medical food's future research needs.
To determine whether additional trials are needed to evaluate the effect of citicoline on all-cause mortality conclusively, we conducted a trial sequential analysis incorporating the cumulative data from the trials included in the meta-analysis forest plot (Figure 4).
Figure 6 displays the trial sequential analysis results for all-cause mortality, including all trials in the prior meta-analysis.
The trial sequential analysis reveals the diversity-adjusted required information size to conclusively detect or reject a 15% relative risk reduction in all-cause mortality was calculated to be approximately 5816 patients, based on the proportion of events in the control group and specified α and β levels. The cumulative Z-curve crossed the futility boundary after just seven trials, indicating firm evidence that further trials are unlikely to alter the conclusion of no significant mortality difference between citicoline and control.
The totality of current data provides decisive evidence that citicoline does not confer a mortality benefit compared to placebo or no intervention in this population. Achieving the required information size of 5816 patients is unnecessary, as futility has already been demonstrated. No single trial individually reached statistical significance for mortality. There is absolutely no indication additional randomized controlled trials on this outcome are warranted, as the cumulative results appear resolute that citicoline does not significantly reduce all-cause mortality risk compared to placebo or no comparison. The trial sequential analysis provides compelling evidence that further investigation of this particular outcome is futile.
7.5. Concluding Thoughts
Armed with the rigorous analysis of the Cochrane review and the visual clarity of the forest plot and TSA, this section provides readers with a comprehensive understanding of citicoline's role in acute ischemic stroke. It underscores the importance of evidence-based practice, urging clinicians to base their decisions on the best available evidence, even when it challenges long-held beliefs or popular narratives. There is a need to address that citicoline is not a medication but a medical food or supplement.
8. Probing the Citicoline Controversy: A Discourse Analysis through Popper, Medawar and Foucault.
This section directs us back to Figure #1: the graph illustrating the intricate relationship between the Philosophy of Science, Evidence-Based Medicine, and Citicoline. Let us delve deeper into this interconnectedness.
The intersection of Evidence-Based Medicine (EBM), Philosophy of Science, and the specific topic of Citicoline in the scope of acute ischemic stroke, as visualized in the graph, is a critical juncture. The narrative we have constructed around Popper's Medawar’s and Foucault's philosophies concerning EBM and the citicoline debate serves as a central pillar of the essay. This confluence of ideas at the vertex reinforces the core question and themes of this essay, emphasizing the intertwined nature of scientific inquiry, philosophical understanding, and medical practice. The graph visually symbolizes this connection, and the narrative explanation delves deeper into its essence and significance.
8.1. Bridging the Divide: A Comparative Evaluation of Current Evidence on Citicoline for Acute Ischemic Stroke
Despite differences in scope and methods compared to this essay, the systematic review by Sagaro et al. aligned with our essay, concluding that citicoline does not significantly improve outcomes for patients with acute ischemic or hemorrhagic stroke.20
Given the lack of proven benefit, philosophers like Immanuel Kant might logically question the rationale for continuing to promote citicoline for stroke treatment. Ischemic stroke has high mortality and disability, so proposed therapies require rigorous support (Gonzales 2022)30. While preclinical citicoline studies seem promising, benefits have not translated in phase 3 trials19. More research is required to elucidate mechanisms in humans and determine if citicoline provides tangible improvements in stroke patients.
According to the TSA, no more RCTs are needed for citicoline in people with acute ischemic stroke (Data are not shown in this essay). In summary, this assessment raises valid questions about the justification for citicoline use in stroke care, given inconclusive clinical trial findings to date.
8.2. Philosophy of Science and Evidence-Based Medicine
8.1.1. Bridging Two Domains
The discipline of medicine, while rooted in the empirical, is also profoundly entangled with philosophy. The practice of medicine is not merely the application of biological knowledge but also engages with more profound questions about the nature of evidence, the structure of scientific inquiry, and the ethics of clinical practice. This intersection of the philosophy of science and evidence-based medicine offers a rich tapestry of ideas that can inform and refine the practice of medicine.
8.1.2. Popperian Falsification and the Citicoline Debate
Sir Karl Popper, one of the most influential philosophers of science, posited that scientific theories can never be proven, only disproven. This principle of falsification becomes particularly pertinent in the debate around citicoline. If the evidence from randomized controlled trials and systematic reviews, such as the Cochrane review, consistently fails to support the efficacy of citicoline in acute ischemic stroke, then the Popperian approach would argue against its use. The essence of Popper's philosophy urges us to be sceptics, to challenge prevailing notions, and to let evidence guide our beliefs and practices.14
8.1.3. Foucauldian Analysis - Beyond the Surface
In the Archaeology of the Knowledge, Foucault stated that These problems can be summarized in one word: the review of the document's value. There is no ambiguity: it is patently obvious that since the discipline of history exists, documents have been used, questioned, and questioned about them; not only what they wanted has been asked of them, but whether they told the truth well, and with what entitlement they could claim it; whether they were sincere or falsifiers, well informed or ignorant, authentic or altered. But each of these questions and all this great critical concern pointed to the same end: to reconstruct, from what these documents say - at times in half-words - the past from which they emanate and which has now faded far behind them; the document continued to be treated as the language of a voice now reduced to silence: its fragile trace, but fortunately decipherable.31 Foucault's insight distills historical analysis and interrogates documents to reconstruct the past. Nevertheless, the documents' truth is uncertain. Questioning their claims unveils their subjectivity. Nevertheless, amidst partiality, traces of the past emerge.
Foucault's insight on scrutinizing documents applies aptly to the citicoline debate. Like historians, we must critically analyze these scientific documents, aware that their truth is uncertain. Questioning the literature's claims unveils its subjectivity. Randomized trials, reviews, guidelines - all contain biases. Nevertheless, amidst their partiality, traces of truth regarding citicoline's efficacy emerge. We must dig beneath the surface to challenge the literature's assumptions to reconstruct an objective understanding. Foucault reminds us that documents reveal as much by what they conceal as what they share. Their silences speak volumes. With a sharply critical eye, we can divine fragments of reality from even the most biased accounts. However, only by remembering that to find truth in documents, we must first question their truth32. Popper's principle of falsification also offers a critical perspective here. It encourages rigorously testing citicoline's efficacy claims against empirical evidence to see if they hold up to scrutiny. The combination of Foucault's document analysis and Popper's falsification provides a sharp lens to assess the citicoline evidence base.
Medawar's thoughts remain. Specifically, Medawar's emphasis on focusing scientific inquiry on "soluble" questions, which can advance understanding rather than getting stuck on insoluble problems, is tremendously valuable advice. As Medawar elegantly states: "There are questions which science cannot answer, and it is no good beating one's head against these questions. What matters is to learn to discriminate between soluble questions with real and accessible answers and questions that are beyond solution for the time being." It highlights the wisdom of channeling curiosity toward questions matched to current capabilities while appreciating present limitations. Progress lies in the pursuit of the soluble. Medawar also astutely notes that even incorrect answers can unveil fragments of truth and "expose the substratum on which truth rests." Science expands its edifice brick by brick through this spirit of imaginative yet grounded inquiry. These philosophical principles remain highly pertinent, broadly to research methodology and specifically to exploring controversial areas like the citicoline debate. Focusing on judiciously framed, tractable questions allows the gradual accretion of knowledge.
The systematic review process requires meticulously examining the literature, probing each study's methodology, assessing the risk of bias, and synthesizing the totality of evidence. It aligns closely with Foucault's emphasis on interrogating documents to reconstruct reality from their selective perspectives and inherent subjectivity. Unlike individual studies, which offer a narrow window, systematic reviews provide a panoramic view - meticulously surveying the landscape to discern the contours of truth. The protocols guard against bias by casting a wide net and pre-specifying rigorous inclusion criteria. This systematic digging beneath the literature's surface allows faint signals to emerge from the noise. In this way, a scrupulous systematic review operationalizes Foucault's approach to document analysis. It crystallizes his ideals of questioning claims, unpacking assumptions, and piecing together truth from imperfect accounts. When rigorously conducted, the review methodology filters out bias to reveal the tentative insights documents can offer when probed critically. In short, the systematic review, emphasizing comprehensive searching, objective appraisal, and synthesis, epitomizes the spirit of interrogating truth in documents that Foucault advocates. It constructs meaning from complexity. Of note, the randomized controlled trial with the largest sample size, which was industry-sponsored, found that citicoline was ineffective for treating moderate to severe acute ischemic stroke.33
8.1.4. Concluding Thoughts
In the journey of this essay, we have explored a multidimensional landscape to address one fundamental question: Should citicoline not be prescribed for individuals with acute ischemic stroke?
Drawing from the robust framework of Evidence-Based Medicine, we have delved into the most rigorous research available, particularly the findings of the Cochrane systematic review focused on citicoline for acute ischemic stroke. This pinnacle of evidence has provided a clear message: the efficacy of citicoline in this context remains uncertain at best.
However, our analysis ventured beyond just the empirical data into the philosophical principles of scientific inquiry. Insights from Karl Popper reinforced the importance of the falsifiability of claims. When assessed through this lens, the case of citicoline faces obstacles.
As Peter Medawar wisely cautioned, research must focus on questions matched to current capabilities. Progress lies in the "soluble" while acknowledging present limitations. Although portions of citicoline's efficacy may one day be uncovered, current evidence raises barriers. Bridging philosophy and evidence provides a multidimensional perspective on the risks of unproven treatments. The lure of new interventions can obscure the need for robust proof. As Michel Foucault illuminated, exertion of power underlies medical "truths."
In conclusion, the amalgamated scientific and philosophical insights provide compelling grounds to question the justification of citicoline for acute ischemic stroke. While hope persists, judicious skepticism prevails given the current evidence favoring alternatives firmly proven effective.
Colophon
In closing, I am compelled to ask: Where is the definitive scientific evidence to support prescribing citicoline for acute ischemic stroke? The corpus of research contains abundant, consistent proofs that do not support using citicoline as a medical food for this indication. The lack of compelling proof of benefits, paired with philosophical principles of truth-seeking, gives me pause. Only when convincing positive evidence emerges will the science point away from prescribing citicoline for acute ischemic stroke, directing me towards proven options. While hope persists, I must align with the evidence. In the spirit of ethical, accountable inquiry, I remain open yet adequately skeptical.
Coda
Truth is ever to be found in simplicity, and not in the multiplicity and confusion of things. Isaac Newton
The important thing is not to stop questioning. Curiosity has its own reason for existence. Albert Einstein
Funding
The author did not receive any financial remuneration for the creation of this essay.
Conflicts of Interest
The lead author of this essay would like to disclose that there are no conflicts of interest associated with the composition of this manuscript.
Invitation
This essay was crafted in response to a gracious invitation.
| 1 | EFSA denotes The European Food Safety Authority. |
References
- Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJB, Culebras A; American Heart Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Peripheral Vascular Disease; Council on Nutrition; Physical Activity and Metabolism. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44(7):2013 Jul;44(7):2064-89. [CrossRef]
- Adams Jr HP, Bendixen BH, L J KappelleL J, Biller J, Love BB, Gordon Dl, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993 Jan;24(1):35-41;24(1):35-41. [CrossRef]
- Feske, SK. Ischemic stroke. Am. J. Med. 2021, 134, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carlson AP, et al. Heart disease and stroke statistics-2020 Update: a report from the American Heart Association. Circulation 2020;141(9):e139-e596. [CrossRef]
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K; American Heart Association Stroke Council. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019; 50:12: e46-e99. [CrossRef]
- National Institute of Health and Care Excellence. Stroke and transient ischaemic attack in over 16s: diagnosis and initial management. Available online: http://www.nice.org.uk/guidance/NG128 (accessed on 27 September 2023).
- Qiu S, Xu Y. Guidelines for acute ischemic stroke treatment. Neuroscience Bulletin. 2020;36(10):1229-32. [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2013. Scientific Opinion on the safety of “citicoline” as a Novel Food ingredient. EFSA Journal 2013; 11 (10):3421, 22 pp. [CrossRef]
- Food and Drug Administration. Frequently asked questions about medical foods; third edition guidance for industry. Silver Spring, MD: Food and Drug Administration; 2023 Mar.
- European Commission. Commission implementing decision of 1 July 2014 authorising the placing on the market of citicoline as a novel food ingredient under regulation (EC) No 258/97 of the European Parliament and of the Council (notified under document C(2014) 4252) (2014/423/EU). Off. J. Eur. Union 2014, L196, 24–26. [Google Scholar]
- WHO Collaborating Centre for Drug Statistics Methodology. Available online: https://www.whocc.no/atc_ddd_index/?code=N06BX06 (accessed on 30 October 2023).
- Cochrane, A.L. Effectiveness and efficiency: random reflections on health services. First edition. London: Nuffield Provincial Hospitals Trust, 1972.
- Sackett DL, Rosenberg WM. The need for evidence-based medicine. J R Soc Med. 1995; 88:620–4. [CrossRef]
- Sackett DL, Rosenberg WM, Gray JA, et al. Evidence based medicine: what it is and what it isn't. BMJ. 1996; 312:71–2. [CrossRef]
- Spade PV, Panaccio C. "William of Ockham", The Stanford Encyclopedia of Philosophy (Spring 2019 Edition), Zalta EN. (ed.). Available online: http://plato.stanford.edu/archives/spr2019/entries/ockham (accessed on 15 October 2023).
- Simon GL, Rios JC. Ockham's razor revisited. Archives of Internal Medicine 1984;144(71371-2). [CrossRef]
- Popper, K.R. The logic of scientific discovery. London and New York: Routledge Classics, 2002. [Other: ISBN 0-415-27844-9]. [Other.
- Uebel, T. "Vienna Circle", The Stanford Encyclopedia of Philosophy (Fall 2022 Edition), Zalta EN, Nodelman U. (eds.). Available online: http://plato.stanford.edu/archives/fall2022/entries/vienna-circle/> (accessed on 30 October 2023).
- Martí-Carvajal_AJ, Valli_C, Martí-Amarista_CE, Solà_I, Martí-Fàbregas_J, Bonfill Cosp_X. Citicoline for treating people with acute ischemic stroke. Cochrane Database of Systematic Reviews 2020, Issue 8. Art. No.: CD013066. [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions. 2nd Edition. Chichester (UK): John Wiley & Sons, 2019.
- Agarwal A, Vishnu VY, Sharma J, Bhatia R, Garg A, Dwivedi S, et al. Citicoline in acute ischemic stroke: A randomized controlled trial. PLoS ONE 2022;17(5):e0269224. [CrossRef]
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. Journal of Clinical Epidemiology 2011;64(12):1283-93. [PubMed: 21839614] Copenhagen Trial Unit. TSA - Trial Sequential Analysis. Available online: http://ctu.dk/tsa/ (accessed on 25 May 2017).
- Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C. User manual for Trial Sequential Analysis (TSA). Available online: http://ctu.dk/tsa/files/tsa_manual.pdf 2011 (accessed on 6 October 202023).
- Medawar, P. Pluto's Republic: Incorporating the art of the soluble and induction and intuition in scientific thought. Oxford: Oxford University Press, 1984. [Other: ISBN 9780192830395].
- Blunt, C. Hierarchies of evidence in Evidence -Based Medicine. The London School of Economics and Political Science. A thesis submitted to the Department of Philosophy, Logic & Scientific Method of the London School of Economics for the degree of Doctor of Philosophy, London, September 2015. Available online: http://etheses.lse.ac.uk/id/eprint/3284.
- Cassels, A. The Cochrane Collaboration Medicine's Best-Kept Secret. Gabriola, BC, Canada: Agio Publishing House, 2015. [Other: ISBN 97819277545303].
- Sestine, P. Epistemology and ethics of evidence-based medicine: putting goal-setting in the right place. Journal of Evaluation of Clinical Practice 2010;16(2):301-5. [CrossRef]
- Wetterslev J, Jakobsen JC, Gluud C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Medical Research Methodology 2017;17(1):39. [CrossRef]
- Sagaro GG, Amenta F. Choline-containing phospholipids in stroke treatment: A systematic review and meta-analysis. Journal of Clinical Medicine 2023;12(8):2875. [CrossRef]
- Gonzales NR, Grotta JC. Pharmacologic modification of acute cerebral ischemia. In: Grotta JC, Albers GW, Broderick JP, Day AL, Kasner SE, Lo EH, Sacco RL, Wong LKS, editor(s). Stroke. Pathophysiology, Diagnosis, and Management. Seventh edition. Philadelphia, PA: Elsevier, 2022:831-51.e6. [Other: ISBN: 978-0-323-69424-7].
- Foucault, M. La arqueología del saber. 1ra reimpresión. 1ra edición. Buenos Aires, Argentina: Siglo XXI Editores, S.A de C.V, 2004. [Other: ISBN 987-1105-07-X].
- Foucault, M. ¿Qué es la crítica? 1era edición. Buenos Aires, Argentina: Siglo XXI Editores Argentina, 2018. [Other: ISBN 978-987-629-869-8].
- Dávalos A, Alvarez-Sabín J, Castillo J, Díez-Tejedor E, Ferro J, Martínez-Vila E, International Citicoline Trial on acute Stroke (ICTUS) trial investigators. Citicoline in the treatment of acute ischaemic stroke: an international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet 2012;380(9839):349-57. [CrossRef]
Figure 6.
Trial Sequential Analysis for citicoline versus placebo or no intervention on all-cause mortality.
Figure 6.
Trial Sequential Analysis for citicoline versus placebo or no intervention on all-cause mortality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



