Submitted:
07 November 2023
Posted:
08 November 2023
You are already at the latest version
Abstract
Postmenopausal abnormal uterine bleeding is a common clinical problem addressed in gynecological practice and should prompt clinical investigation due to the significant prevalence of malignant and premalignant lesions of endometrium in this age group. Nevertheless, other causes should be considered since its diagnostic and therapeutic management may differ considerably. Here, we present a case of a colouterine fistula due to chronic diverticulitis presenting with postmenopausal abnormal uterine bleeding. This is extremely rare and is caused by the rupture of a diverticular abscess into the uterine wall, resulting in an inflammatory adhesion of the colon and uterus, with necrosis and subsequent fistula formation. The clinical presentation is variable and may include abdominal pain, gastrointestinal tract symptoms, vaginal discharge and abnormal uterine bleeding. The laboratory and imaging techniques may be not completely conclusive and definitive diagnosis can be made intraoperatively. There are different treatment options, being the en bloc resection and primary anastomosis the most used, allowing complete treatment. The prognosis for a colouterine fistula secondary to diverticulitis is excellent after surgery. This case highlights the importance of clinical suspicion of an unusual cause of uterine bleeding and an effective and multidisciplinary approach that allowed complete surgical treatment and patient recovery.
Keywords:
Abnormal uterine bleeding
; Menopause
; Colouterine fistula
; Diverticular fistula
; Colon diverticulosis
; Diverticulitis
1. Introduction
Postmenopausal abnormal uterine bleeding (AUB) is a common clinical problem and occurs in approximately 4 to 11 percent of postmenopausal women [1]. This symptom requires a prompt clinical and aetiological evaluation, mainly to exclude malignant or premalignant lesions of the endometrium. It should include a detailed medical history, physical examination and diagnostic imaging and laboratory tests that can help clarify clinical suspicions [2].
A colouterine fistula is extremely rare and can cause AUB due to chronic inflammation in the uterine wall adjacent to the colonic diverticulum. CT scan is routinely performed for suspected diagnosis but usually cannot alone provide a definitive diagnosis, which enhances the need for a proper clinical medical history, correlation with physical examination and radiological findings to select appropriate management. Resection is the treatment of choice for colouterine fistulas and, in most cases, en bloc sigmoid and uterus resection has now become the preferred technique, especially in cases where malignancy is suspected.
We describe a patient with a history of AUB due to a colouterine fistula after chronic diverticulitis.
2. Case Presentation
This is a case of a 71-years-old female, with a prior medical history of high blood pressure taking an oral hypertensive daily, without previous surgeries or other significant medical problems. She had two normal pregnancies and two eutocic deliveries; menopause was around 51 years-old and she did not take any hormonal replacement therapy.
The patient was referred to gastroenterology practice due to a routine faecal occult blood test that was positive and abnormal findings in the colonoscopy. She mentioned she had vaginal bleeding in scarce quantity few months prior, without other symptoms, namely changes in the gastrointestinal habits, abdominal pain, haematochezia, or weight loss. The colonoscopy revealed inflammatory changes in sigmoid colon mucosa wall around 20cm from anal verge, with a suspicion of a fistulous tract with drainage. The histopathological analysis of the biopsied areas showed chronic inflammatory unspecific colitis without malignant or premalignant changes and a hypothesis of colonic ulcer or fistula was made.
Due to abnormal vaginal bleeding, she was referred to gynaecology practice. She denied other gynaecological symptoms and mentioned the bleeding was painless, as a light spotting, and started few months prior. On examination, she had normal vital signs, without fever. She was obese (body mass index of 32kg/m2), examination of the abdomen was unremarkable, without masses or pain with palpation. On speculum examination, she had vaginal atrophy, the cervix had no changes, and no uterine or vaginal bleeding was noted. The vaginal discharge was normal. The uterus was felt to be of normal size for her age and adnexa were not palpable.
Transvaginal ultrasound showed the uterus in anteverted position with 3 small FIGO type 3-4 myomas with less than 1cm in diameter, regular outer contour, and an endometrium thickness of 3mm, with regular lining. Adnexa were normal and a small amount of fluid in the rectouterine pouch was noted. No tenderness or pain was noted during the probe examination. The diagnostic hysteroscopy showed atrophic endometrium without intracavitary lesions, both tubal orifices were seen, and the sampled endometrium ruled out endometrium malignant or premalignant changes.
The CT enterography requested by the gastroenterology showed a mass adjacent to uterine fundus and in continuity with sigmoid colon wall, with dimensions of 3.4 x 3.2 x 4.3cm, with calcifications and gas areas. Blood examinations and serum tumour markers (CA 125, CEA and CA 19.9) were normal.
The differential diagnosis of uterine malignancy of the myometrium (leiomyosarcoma), colonic ulcer or fistula was made.
The treatment approach was discussed in a multidisciplinary team with Gynaecology, Gastroenterology and General Surgery. The patient underwent exploratory laparotomy via a midline incision which identified the sigmoid wall adherent to uterine fundus with an approximately 3cm extension, the uterus was normal in size and consistency with small myomas identified, the adnexa were atrophic, there were no adhesions or other abnormal findings. The procedure continued with en bloc colonic resection and primary anastomosis, total hysterectomy and bilateral adnexectomy. Intraoperative frozen section examination revealed fibrous and inflammatory tissue without malignant aspects and, therefore, the procedure was finalized (Figure 1 and Figure 2).
3.1. Figures, Tables and Schemes
All figures and tables should be cited in the main text as Figure 1, Table 1, etc.
Figure 1.
Intraoperative findings showing the sigmoid colon adherent to the serosal surface of the uterine fundus with a fistulous communication between the two viscera.
Figure 1.
Intraoperative findings showing the sigmoid colon adherent to the serosal surface of the uterine fundus with a fistulous communication between the two viscera.
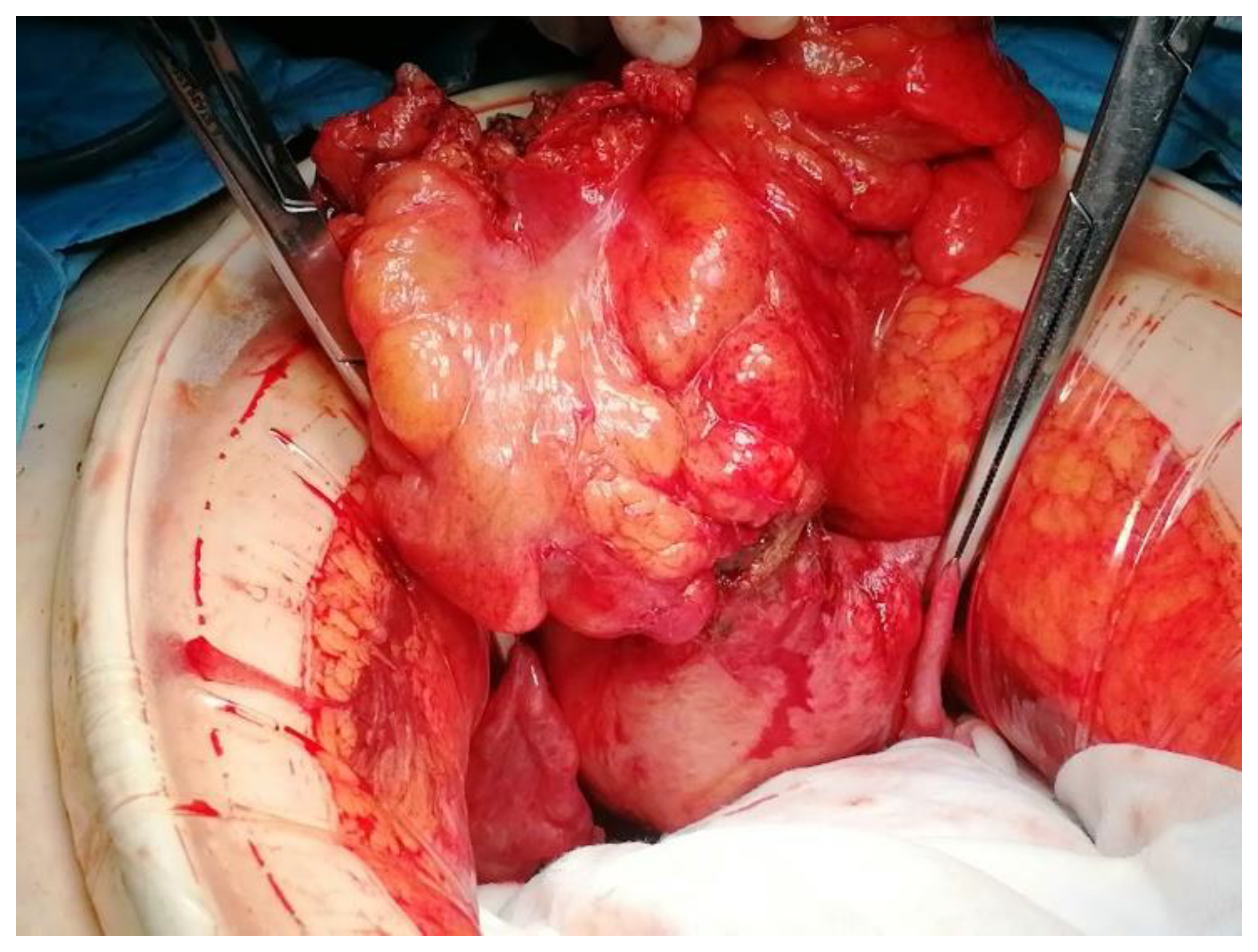
Figure 2.
A close look of the sigmoid colon adherent to the serosal surface of the uterine fundus with a fistulous communication between the two viscera.
Figure 2.
A close look of the sigmoid colon adherent to the serosal surface of the uterine fundus with a fistulous communication between the two viscera.

Post-operative recovery was uneventful, and the patient was discharged after the 6th post-operative day without complications. One year after the surgery, the patient is well.
The final pathology result showed a 11cm sigmoid colon with irregular serous layer and adherent to uterine fundus. The microscopic examination showed a colonic diverticulum without its epithelial lining and abundant granulation tissue and fibrinous exudate extending into uterine wall with signs of haemorrhage and chronic inflammation, which was diagnostic of a colouterine fistula of diverticular aetiology with no evidence of malignancy. The endometrium was thin and atrophic, without malignant or atypical aspects. The uterine wall comprised three small myomas and the ovaries and tubes had no abnormalities.
A diagnosis of diverticulitis and fistulisation into the uterine cavity was made.
4. Discussion
A colouterine fistula is extremely rare and few cases are reported in the literature worldwide. This may be due to the thick muscular structure of the uterus that can usually provide a protective barrier against an inflammatory or malignant disease. The aetiology of fistula involving the reproductive tract includes rupture of an abscess into the adjacent viscera, malignant disease involving the gynaecologic or other pelvic organs, inflammatory bowel disease, surgery complications and radiotherapy complication [3,4,5,6,7,8].
Inflammatory adhesion of the colon and uterus can occur during an episode of diverticulitis, which results in necrosis and subsequent fistula formation due to destruction of two serosae of two epithelialized surfaces in proximity, commonly resulting in linkage of the fundus of the uterus and the sigmoid colon [3], as we observed in this case.
The clinical presentation is variable and, in our case, presentation without abdominal pain, gastrointestinal tract changes, fever or other significant lower gastrointestinal symptoms is highly unusual. AUB was the main clinical sign that ignited the inflammatory or cancerous disease involving sigmoid colon and uterus [3,5].
Diagnosis by imaging or endoscopy were not completely conclusive. The CT findings were suggestive of diverticulitis and colouterine fistula since it showed air bubbles adjacent to the uterine cavity and colon wall joined to the uterus. Nevertheless, definitive diagnosis was limited because CT findings cannot accurately distinguish inflammatory from neoplastic disease and may not be conclusive distinguishing a fistula tract from complicated diverticulitis.
The prognosis for a colouterine fistula secondary to diverticulitis is excellent after surgery [3,5]. The choice of en bloc resection and primary anastomosis was appropriate in our case, considering patient conditions, intraoperative findings, viability of colonic tissue and team expertise, and allowing complete treatment and resolution. In fact, malignant aetiology was not excluded preoperatively, the colon could not be completely separated from the uterine fundus due to chronic inflammation and the uterus and adnexa were easily removed, so there was no need to preserve the uterus and adnexa and close the fistulous opening, avoiding potential future complications such as infections and future needs of uterine drainage.
5. Conclusions
Abnormal uterine bleeding is a common symptom and an important medical problem. In postmenopausal women, should prompt further investigation mainly to rule out endometrial malignancies that are prevalent in this age group. Nevertheless, other less common causes should be suspected and, therefore, the diagnostic and therapeutic approach should be adapted.
This case was remarkable for its unusual presentation with postmenopausal abnormal uterine bleeding, absent gastrointestinal tract symptoms and abnormal findings in routine colonoscopy. It was successfully managed due to a multidisciplinary team of gynaecology and general surgery.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
This article received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Local Health Unit of Alto Minho
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
No new data was created.
Acknowledgments
The authors have no acknowledgments.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Astrup K, Olivarius Nde F: Frequency of spontaneously occurring postmenopausal bleeding in the general population. Acta Obstet Gynecol Scand. 2004, 83:203-7. [CrossRef]
- Khafaga A, Goldstein SR: Abnormal Uterine Bleeding. Obstet Gynecol Clin North Am. 2019, 46:595-605. [CrossRef]
- Gabriel Rodrigues, Krishna Kalyan, Reddy Janumpalli, Shyamala Guruvare, Suresh Arjun, Afroz Khan, Balaji Jayasankar: Sigmoido-uterine fistula: An uncommon communication! 2019. [CrossRef]
- Aggarwal R, Indiran V, Maduraimuthu P: Different etiologies of an unusual disease: Colouterine fistula - Report of two cases. Indian J Radiol Imaging. 2018, 28:37-40. [CrossRef]
- Sentilhes L, Foulatier O, Verspyck E, Roman H, Scotté M, Marpeau L: Colouterine fistula complicating diverticulitis: a case report and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2003, 10:107-10. [CrossRef]
- Perez AR, Chiong-Perez ME, Arcilla CE Jr, Merin JI: Colouterine fistula: A case report of a rare complication of diverticular disease managed during the pandemic. Int J Surg Case Rep. 2021, 79:150-155. [CrossRef]
- Maamer A, Zaafouri H, Noomene R, Haoues N, Bouhafa A, Oueslati A, Cherif A: Colouterine fistula complicating diverticulitis. LA TUNISIE MEDICALE - 2013; Vol 91.
- Guevara-Morales GR, Maldonado-Barrón R. Fístula colo-uterina: Una complicación rara en diverticulitis aguda. Revista de Gastroenterología de México. 2019, 84:104-105. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



