
Submitted:
31 October 2023
Posted:
01 November 2023
You are already at the latest version
Abstract
Emotional eating (EE) can be understood as a manifestation of difficulties with emotion regulation (ER) among individuals with eating disorders. Existing interventions do not always successfully treat EE. We developed a novel ER intervention based upon virtual reality to improve EE among adults with an eating disorder diagnosis. The design pivoted to non-immersive virtual delivery to increase access, particularly given heightened demand during COVID-19 for EE treatment. The study aimed to investigate the feasibility, acceptability, and preliminary signals of effectiveness of this novel ER protocol that utilized evidence-based strategies such as mindfulness and imagery rescripting as well as innovative techniques such as virtual reality. Twenty-one adults with a history of an eating disorder diagnosis and self-reported EE were recruited from the Adult Eating Disorders Program within Stanford University to receive seven weekly one-hour virtual experiences (VE) focusing on ER. Participants chose between the novel VE-Emotion Regulation (VE-ER) intervention or continuing with their current treatment as usual. Before and after the seven sessions, participants completed an assessment by filling out online questionnaires. Overall, VE-ER treatment was feasible (100% completion), and participant and therapist acceptability of VE-ER treatment was fairly high. In terms of preliminary effectiveness, the results showed a significant reduction in the frequencies of disordered eating behaviors in both groups, but a greater improvement in EE in the VE-ER group. The VE-ER group also had a significant reduction in emotion dysregulation after the treatment.
Keywords:
emotional eating
; eating disorder
; binge-eating disorder
; bulimia nervosa
; virtual reality
; treatment
; somatic marker
1. Introduction
Emotion regulation (ER) is a complex process defined as the initiation, maintenance, and modification of the occurrence, intensity, and duration of feeling states [1]. Research over the last decade shows difficulty with ER is a core transdiagnostic construct across both the eating disorder spectrum and other disorders such as depression, anxiety, substance use, and borderline personality, thus partly explaining their high comorbidity with eating disorders [2]. Emotional eating (EE), or eating in response to negative emotions or stress, is one of the key manifestations of difficulties with ER within eating disorders [3]. EE is positively associated with both the presence and severity of binge eating [4], but despite its prevalence (20.5%) [5] and important transdiagnostic features, it has not received much research attention.
EE, in particular, was found to increase in the context of psychological distress during the COVID-19 lockdown and isolation [6], with EE predicted by higher depression and anxiety levels [7]. These findings support prior research [8,9,10], which show a relation between EE and stress, modulated by body mass index (BMI) [11,12,13]. Indeed, EE has been associated with emotion regulation difficulties [8,9] and a higher level of alexithymia (difficulty experiencing, identifying, and expressing emotions [14]. Some posit that higher alexithymia impairs one’s ability to identify emotional states and to distinguish them from internal signals of hunger and satiety, resulting in food consumption as a way to regulate emotions [14,15], with downstream effects on BMI [15,16,17]. Research supports a relation between EE with higher weight as well as challenges with weight [9,18,19]. Given the presence of weight stigma and weight-based discrimination in society [20], these weight changes may evoke significant distress, and result in a vicious cycle between negative mood and eating.
Given the links between emotion dysregulation and EE [21], existing interventions targeting EE have utilized mindfulness and emotion regulation skills training. Despite the fact that such interventions that teach mindfulness and/or other emotion regulation skills have shown promise in reducing symptoms, [22,23,24] innovative technologies and theoretical approaches offer the promise of improved outcomes and reduced attrition.
Virtual reality (VR) has been studied as a successful technique for enhancing psychological treatment [25]. Virtual interventions allow researchers and clinicians to recreate life-like experiences in a safe environment, and in particular, have been widely used in populations [26]. Further, VR enhanced treatments for eating disorders show superior efficacy, faster results, and better maintenance compared to non-VR delivery [27].
Previous authors indicated virtual experiences integrated with biofeedback, mindfulness, and imagery techniques offer a therapeutic approach that helps patients make new associations with negative memories, thereby altering emotional states [28]. This is typically done through cognitive techniques; for example, a patient might be encouraged to envision a future outcome turning out positively [29,30,31]. A meta-analysis that investigated imagery rescripting as a clinical intervention for aversive memories found it effective for reducing psychological symptoms [32]. An immersive intervention can modify the user’s ER by allowing for the modification of the emotional response across a reappraisal of emotional stimuli and therefore inspiring new actions. This re-evaluated experience is more easily encoded into memory. In this light, immersive intervention integrated with imagery rescripting may be able to modify emotional core beliefs [33].
Riva’s recent paradigm of embodied cognition [34,35] reconceptualized the nature of cognition by specifying that cognition occurs in a specific bodily environment. In other words, the mind must be considered and studied in relation to a physical body that interacts with the world. Hence, human cognition is not centralized, abstract and clearly distinct from the peripheral modules of input and output, but has deep roots in sensorimotor processing [35].
Recently, it has been suggested that our brain generates simulations that filter the incoming sensory input, guide action and cause perception and other psychological phenomena, including emotion [36,37,38].
Barret explains: “Our brain constructs meaning by correctly anticipating (predicting and adjusting to) incoming sensations. Sensations are categorized so that they are: (i) actionable in a situated way; and therefore (ii) meaningful, based on past experience. When past experiences of emotion (e.g., happiness) are used to categorize the predicted sensory array and guide action, then one experiences or perceives that emotion (happiness)” [37]. In this light, we must alter the body’s experience related to an emotion in order to regulate that emotion.
Relatedly, Damasio, in his somatic marker theory [39], posits that emotions are changes in both our body and brain states. Over time, emotions and their corresponding bodily changes, or "somatic markers", become associated with particular situations and their past outcomes. Once formed, the somatic markers are reactivated every time the person encounters similar situations to those that originally induced the emotion reaction. The reactivation of the somatic markers calls forth the historically associated body state. Somatic markers permit a comparatively fast pre-selection of the relevant alternatives which are then subjected to more detailed cognitive processing for final decision making. In this way, somatic markers increase the efficiency and accuracy of human decision making [40]. In other words, when we experience a situation similar to one in the past, our body reproduces the same emotional and behavioral responses it had learned in the previous situation. This automatic mechanism makes it difficult to modify the emotional reaction with a more adaptive one. Rescripting a somatic marker through immersive experiences has the exciting potential for patients to create a new emotional experience with their bodies, which could in turn influence their ER and eating behavior (e.g., EE).
To date, many VR treatments for eating disorders have focused on body image or exposure methods and have not exclusively focused on EE [25]. There has been a call made by experts in the field for a “new generation” of VR interventions, capable of utilizing VR’s potential more fully [25]. To our knowledge, there are no studies that have investigated the combination of VR, mindfulness techniques, and imagery rescripting to treat EE starting from a somatic view of emotional experience. Rescripting somatic markers through immersive experiences involving the body would represent a novel direction in the treatment of EE.
A recent promising case study [41] reported on a patient who decreased emotional eating and improved emotion regulation after receiving a novel ER-based VR intervention that used rescripting techniques based on Damasio’s somatic marker theory [39]. This led us to undertake the current, larger study to further investigate the acceptability, feasibility, and preliminary signals of effectiveness of this same innovative protocol using VR to improve current EE among adults with a history of an eating disorder diagnosis. Given links between emotion dysregulation and EE [21], the intervention utilized evidence-based strategies such as mindfulness and imagery rescripting. However, due to the COVID-19 pandemic (requiring lockdown) and efforts to increase access to care during this period, the virtual immersive scenarios could not be delivered using 3D head-set virtually as originally planned (as it would have required in-person sessions to access the head-set). Instead, the intervention was delivered remotely via 2-D video conferencing software. Previous studies [42,43,44,45,46] have found 2D virtual experiences (VE) effective in improving the overall psychological and emotional well-being of adults during the COVID-19 pandemic.
2. Materials and Methods
2.1. Participants
Twenty-one participants were recruited between 09/2020 and 09/2021 from the Adult Eating Disorders Program (AEDP) within Stanford University School of Medicine. All participants were informed about the purpose of the research and provided written informed consent. The study was approved by the Institutional Review Board (IRB) of Stanford University. Inclusion criteria included English speaking adults with a history of a DSM-5 eating disorder diagnosis (e.g., binge-eating disorder, bulimia nervosa, other specified feeding and eating disorder) from an AEDP clinician and current (i.e., within past month) subjective emotional eating (see Measures, below). Exclusions were current significant suicidal ideation, psychosis or bipolar I (unless stably remitted on maintenance therapy for at least 1 year), and/or any newly initiated (e.g., < 1 month) psychotropic medication or adjunctive psychotherapy.
2.2. Study Design
Patients were referred by clinic providers to the study. All patients met eligibility criteria, as confirmed by the research coordinator. Participants were given informed consent. They then choose between two treatment options: 1) to continue their current clinic treatment as usual (TAU), or 2) engage in the novel virtual experience for emotion regulation (VE-ER) intervention. Participants had the option to select whichever treatment option best suited their needs and comfort level.
2.3. Treatment as Usual (TAU)
Participants that chose TAU continued to receive the evidence-based treatment that they were currently receiving in the Stanford Eating Disorders Clinic [e.g., group or individual cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), or interpersonal psychotherapy (IPT)]. Participants were asked to complete study assessments/surveys before and after seven weeks.
2.3. Non-Immersive Multisensory Virtual Experience for Emotional Regulation Intervention (VE-ER)
The intervention was developed as a collaboration between Stanford's Virtual Reality Lab Immersive Technology (VR-IT) Clinic, a VR/AR Tech Company, Become-hub, and the Department of General Psychology at the Catholic University of the Sacred Heart. Participants in the VE-ER group participated in a total of seven sessions. The first session included an initial assessment to allow for greater personalization of treatment. Sessions two and three were dedicated to the emotion regulation component, which aimed to increase the participant’s ability to recognize emotional states. Sessions four, five, six, and seven included an emotional rescripting component that aimed to increase the participant’s confidence in their ability to experience and skillfully manage challenging emotional states. Each session also included an experiential component based on the somatic marker theory (e.g., the anchoring hand gesture) that enables interaction between the narrative and bodily experience. Sessions were 50-60 minutes. Please see Table 1 for further description of the virtual scenarios and Table 2 for greater detail on the protocol.
Over the course of seven weeks, participants were guided through a series of scenarios, each connected to the development of skills for improved emotion regulation and eating. Before every session, the participants were sent the Zoom link. The first session assessed the participant’s symptoms of EE and disordered eating patterns in detail to personalize treatment, including obtaining the frequency of disordered behaviors (large binges, small binges, purges, EE) All subsequent sessions began with brief assessment of the frequency of disordered eating over the previous week (e.g., large binges, small binges, purges, EE), which was documented in the therapist’s session note. Starting with session 3, this was followed by a review of the homework from the previous session. The goal of the towER sessions was to help participants improve ER abilities and to increase their awareness of emotional states. The first experience was a therapist-guided mindfulness breath and bodily sensation exercise. This was followed by introduction to the virtual scenario in which the patient was guided to implement mindfulness-based strategies to explore landscapes while identifying internal states. Afterwards, the therapist asked the patient to recall the immersive experience and identify a moment they experienced pleasant emotions. This was referred to as a "safe place" that the therapist helped the patient to "anchor" by linking the positive emotions experienced during the virtual environment to an actual positive experience the patient had in the "real world." While doing so, the therapist encouraged them to generate vivid details about the real-life experience while making a hand gesture (closing their thumb between their four fingers) in order to anchor this positive feeling within the body.
Participants were taught strategies for accessing and using safe place visualization and somatic markers (i.e., the anchoring hand gesture) to regulate affect at appropriate times during the week. For daily homework, the participant practices re-experiencing the immersive moment by listening to an audio or video file of the session. See Supplementary Table for additional detail.
The emotional rescripting experiences represent a metaphorical journey towards healing (i.e., beginning in a fragile state, overcoming obstacles, and practicing skills). Each scenario has a specific meaning and associated obstacle (see Table 3). Emotional rescripting sessions begin with the same five-minute mindfulness exercise described above (“focus on attention” exercise), followed by the immersive experience. During each metaphorical experience, the participant makes use of real-life objects or sensorimotor reinforcements, with the aim of encouraging changes in the somatic markers and increasing the body’s involvement in the immersive experience. After the video was viewed, the patient was asked to identify their emotions and localize them in their body. If the emotions were predominantly positive, the therapist amplified the emotion by facilitating mindful awareness of the emotion and anchoring it to a real-life experience. If the emotions were predominantly negative, the therapist could help the participant reduce the negative experience by rescripting the negative memories associated with similar emotions, and/or through awareness, acceptance, and physicalizing exercises (e.g., treating unwanted content as an object that the participant could visualize as moving away into the horizon until it disappeared and/or was contained).
For daily homework, the participant listened to the session while holding a real-life object associated with the scene/emotion. Overall, the participant was rehearsing and reinforcing stability and self-confidence at each stage of the journey.
2.3. Measures
Data were collected remotely through the use of Qualtrics, a secure online survey tool. Descriptive data were collected during the first session. In both conditions (VE-ER and TAU), preliminary signals of effectiveness data were collected before the intervention (at baseline) and after seven sessions (the duration of the VE-ER condition).
2.3.1. Descriptive Variables
A demographic form inquiring about age, sex, race/ethnicity, socioeconomic status, and concurrent treatment was obtained at baseline.
2.3.2. Feasibility
Outcomes assessing feasibility included: (1) number of therapists who, after attending an information session about VR and eating disorders, chose to attend the two study training workshops; (2) number of providers who, after attending the training workshops, subsequently enrolled as study therapists; (3) number of eligible (clinician-referred) patients who chose to enroll in the study; (4) number of sessions attended and number of study completers. The choice of these definitions of feasibility were based on the research literature [47].
2.3.3. Acceptability
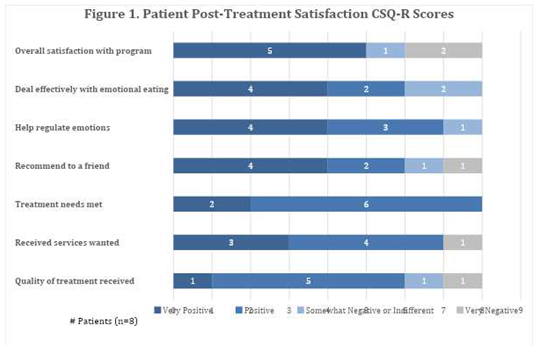
The Client Satisfaction Questionnaire-Revised (CSQ-R) [48] was used as the acceptability measure. This eight-item measure is used to assess satisfaction with a product or service and was modified to be suitable for therapists and participants in both the VE-ER and TAU conditions. Scores on the CSQ-R range from 8 to 32, with higher scores indicating greater satisfaction.
2.3.4. Exploratory Outcomes of Effectiveness
Before and after the intervention (at baseline and after seven sessions) participants from both conditions (VE-ER and TAU) were asked to complete the following measures.
- −
- Difficulties in Emotion Regulation (DERS) [49]. This self-report scale asks respondents to rate how they manage their emotions on a 5-point Likert scale ranging from never to always. Six subscales emerge from the questionnaires: (1) “The inability to accept emotional responses,” (2) “Impulse control difficulties,” (3) “Difficulty engaging in goal-directed behavior,” (4) “A lack of emotional awareness,” (5) “Lack of emotional clarity,” and (6) “Limited access to emotion regulation strategies.” Higher scores indicate greater problems with emotion regulation. In this study we considered only the Total Scores that range from 36 to 180. There are no standardized clinical cutoffs for this measure, however prior research suggests that the clinical range on the DERS total score varies from averages of approximately 80 to 127 [50].
- −
- The Dutch Eating Behavior Questionnaire (DEBQ) [51]. The DEBQ is a 33-item self-report questionnaire that assesses three distinct eating behaviors in adults: (1) emotional eating, (2) external eating, and (3) restrained eating. Items on the DEBQ range from 1 (never) to 5 (very often), with higher scores indicating greater endorsement of the eating behavior. Similar to the DERS, there are no standardized clinical cutoffs. Research community samples suggest a score > 3.25 as the 80% percentile.
- −
- Frequency of disordered eating. At the beginning of each session in both conditions, therapists assessed the participant’s frequency of disordered eating. This information was entered into a Therapist Note on Qualtrics. Preliminary signals of effectiveness were determined by changes in the frequency of disordered eating behaviors over the previous 7 days [e.g., number of EE episodes, evaluation of the trend of EE, number of objective binge episodes (OBEs), subjective binge episodes (SBEs), purging episodes]. EE episode frequency was assessed using a 5-point Likert scale: Never (1), Seldom (2), Sometimes (3), Often (4), Always (5). Binge episodes were distinguished as objective or subjective as defined by the Eating Disorder Examination Questionnaire (EDE-Q). OBEs and SBEs episodes were assessed asking for a specific number of episodes over prior week.
- −
- The Acceptance and Action Questionnaire (AAQ-II) [52]. This seven-item measure assesses for psychological inflexibility and experiential avoidance. Items range from 1 (never true) to 7 (always true). The scale is scored by summing the seven items. Higher total scores indicate less flexibility, while lower total scores mean more flexibility (total range: 7-49).
- −
- - Weight Efficacy Life-Style Questionnaire (WELSQ) [53]. The Weight Efficacy Lifestyle Questionnaire (WELSQ) is a commonly used measure of eating self-efficacy consisting of 20-items and five situational factors (negative emotions, availability, social pressure, physical discomfort, positive activities). Respondents rate their confidence to resist eating in certain situations on a 10-point Likert scale ranging from 0 (not confident) to 9 (very confident). The WELSQ yields five subscales’ scores ranging from 0-36. High WELSQ scores indicate a higher self-efficacy to resist eating.
2.4. Data Analysis
Descriptive statistics (e.g., mean, standard deviation) were used given the small sample size of the study. Exploratory analyses using the Mann-Whitney were performed to analyze differences between groups pre- and post-intervention data. The Wilcoxon test was used to evaluate the change within the two groups. Unfortunately, in the virtual group, only 5 out of 10 received the post treatment questionnaires. This was due to personnel error associated with staffing changes during COVID-19. In addition, there were no differences in the VE-ER group on baseline measures between the five participants who received post-treatment questionnaires versus the five who did not, including no differences in binge eating severity, measures of emotion regulation and EE. Given the substantial missing data in the VE-ER group, the decision was made to analyze paired t-test within-group differences on the exploratory measures and not to compare the two conditions using independent t-tests to assess for between-group differences. As regards participant’s frequency of disordered eating obtained from the therapist note and completed by all participants, a repeated measures ANOVA was carried out for pre-post treatment evaluation between conditions. We adopted a significant p-value as <0.05. The Statistical Package for Social Sciences (SPSS, version 27) was used for all analyses.
3. Results
3.1. Descriptive Analysis
Participants were, on average, 41.7 (SD=15.7) years of age, female (90.5%), Caucasian (81%), at least college educated (100%), had a history of BED and had previous experience of psychotherapy (100%). Nearly half of them were engaged in other treatment for a psychiatric disorder (42.9%), the majority (90%) for medication management.
3.2. Feasibility
3.2.1. Therapists
Eleven therapists attended an initial information session about VR and eating disorders. Of these 11, six enrolled as study therapists. All therapists were eating disorder specialists at the doctoral level (PhD, PsyD, MD). All were female.
3.2.2. Patients
Twenty-three patients were referred by clinic providers to the study. Eleven patients expressed interest in the VE-ER treatment and twelve expressed interests in the TAU condition. Of the 11 eligible participants that expressed interest for the VE-ER condition, 10 chose to enroll, and of the 12 eligible participants for TAU condition, 11 chose to enroll. There was a 100% completion rate in both conditions. The average number of sessions attended was 7 out of 7 for both groups. The majority (90%) of the ten participants in the VE-ER condition who received all surveys completed surveys; however, as per above, not all participants in this condition received all of the post-treatment assessments.
3.3. Acceptability
3.3.1. VE-ER Intervention
The mean client satisfaction questionnaire-revised (CSQ-R-Patients) score was 24.75 (SD=6.7, n=8) out of a possible 32, indicating a fairly good treatment satisfaction (Figure 1). The majority of the participants, 75% (6/8), rated the quality of the treatment as “excellent” or “good”. Generally, two participants (25%) had neutral to negative feedback about the treatment. Six of the participants (75%) reported they would participate in the intervention again if they sought services for emotional regulation. Five of the participants (62.5%) reported they would participate in the intervention again if they sought services for emotional eating.
Participants were also asked about their satisfaction with the 2-D virtual scenarios and technology. All but one participant (87.5%, 7/8) reported that the journeys clearly conveyed the various emotional themes; one (12.5%) found them only “a little” clear. When asked to rate their satisfaction with the narrator's voice, participants responded as follows: 12.5% (1/8) “very satisfied”, 12.5% (1/8) “mostly satisfied”, 50% (4/8) “indifferent or mildly satisfied”, or 12.5% (1/8) “quite dissatisfied.” Participants rated the sound effects as helping “a great deal” (25%; 2/8), “somewhat” (37.5%, 3/8), or “didn’t really help” (37.5%, 3/8). Most of the participants found the virtual scenarios “realistic” (50%, 4/8) or “a little realistic” (25%, 2/8); two found them “not at all” realistic (25%). Open ended responses from these two participants suggest they did not find them realistic because of connectivity issues (“choppy movement” during the video) or the stimuli not being relatable to real world stimuli. One participant wrote, “It felt like I was watching a cartoon and the exposures were not advanced enough cinematically without a VR setting. This really needs to be in a VR setting --- I understand covid upended the in-person study, but the team needs to explore an at home VR experience...” All but one participant (87.5%) reported being at least a little successful at using the audio recordings outside of treatment sessions.
In an open-ended response format, all participants were asked about the most helpful aspects of the intervention. Fifty percent of participants (4/8) stated that talking with the therapist was helpful; many felt a strong therapeutic alliance was critical in addition to meaningful reflection, processing, and insights following immersive scenes. Some responses additionally added that “the physical participation of holding a compass, or carrying a backpack” and “accessibility to videos as needed” were helpful. Participants were asked about the least helpful aspects of the intervention. Thirty-eight percent of participants (3/8) responded that audio or video quality was the least helpful; participants found the video “choppy” or “botched” intermittently during screenshare. One participant commented, “The program (or maybe the therapist?) did not do a good job relating the videos and topics on emotion regulation to binge eating.”
Participants were asked how they would improve the intervention. Twenty-five percent of participants (2/8) reported that they would improve the quality of the VR-ER videos; for example, one participant stated, “I had hoped the immersive experiences would have felt more realistic.” Other responses included using 3D VR (37.5%, 3/8), personalizing videos for each participant (25%, 2/8), being more open to the intervention (12.5%, 1/8), and having videos be more easily accessible for between-session review (i.e., not emailed but accessible on an app) (12.5%, 1/8).
3.3.2. TAU Treatment
The mean CSQ-R score was 24.50 (SD= 1.58) out of possible 32, indicating good treatment satisfaction. The majority of the participants, 80% (8/10), rated the quality of the treatment as “excellent”, 20% (2/10) rated the quality of the treatment as “good”. Overall, 90% (9/10) of patients were satisfied with the TAU treatment, 10% (1/10) of patients were indifferent or mildly dissatisfied.
3.3.3. Therapists’ Satisfaction with Virtual Intervention
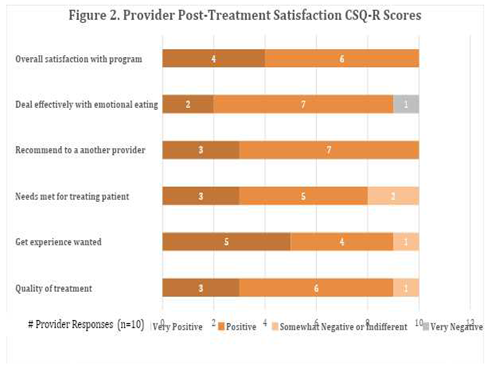
Therapist’s mean CSQ-R score was 22.71 (SD= 1.89, n=10) out of possible 32, indicating overall fairly good satisfaction in delivering the intervention (Figure 2). Ninety percent of therapists (9/10) rated the quality of the intervention as either “excellent” (3/10) or “good” (6/10) with one therapist (10%) rating it as “fair.” This same therapist rated the intervention as making “no difference" in the participants' EE. Most therapists 90% (9/10) thought they would use the intervention again in the treatment of eating disorders.
Therapists were also asked specifically about the manual and homework. Seventy percent (7/10) of therapists found the manual “clear” whereas 30% (3/10) found it “a little” clear. Most therapists (60%, 6/10) felt “comfortable” or “very comfortable” administering the intervention, whereas 40% felt “a little” uncomfortable (4/10). All therapists (100%) felt “successful” or “very successful” at using the videos for the immersive intervention.
Therapists were asked about the most helpful aspects of the intervention and responded in an open-ended format. Eighty percent of therapists (8/10) reported that the metaphorical journeys were helpful and that the post-processing and discussion that occurred after video review was particularly impactful. Therapists described using cognitive strategies including cognitive restructuring, reframing, and developing coping phrases to build motivation, confidence, and resiliency; to target cognitive rigidity; and to rescript unhelpful narratives. One therapist stated, “the metaphors in the re-scripting videos were… effective in helping to change rigidity related to expectations she had for herself, and empowering her with the sense that she has internal resources she can access at any time to overcome challenges.” Another therapist commented, “The metaphorical journeys… seemed to help reinvigorate her to commit to treatment, as motivation was somewhat low when initially referred to therapy. The visual aspect of therapy also seemed to help keep her engaged as she reported difficulty with engagement in the DBT group and her existing [individual] therapy. The videos also helped patients manage urges to sit w/ cravings.” Some therapists commented that the videos helped evoke different emotional states enabling either exposure to negative emotions or promotion of relaxation states. Sixty percent of therapists (6/10) reported that using the hand gesture or a physicalizing exercise was helpful.
Therapists were also asked about the least helpful aspects of the intervention with an open-ended response format. Thirty percent of therapists (3/10) reported issues with video quality or technical problems (e.g., audio delays, issues with screen share). For example, the “patient found it difficult to feel truly ‘immersed’ in the intended emotional experience.” Thirty percent of therapists (3/10) found the hand gesture unhelpful. Therapists were asked what changes they recommend for the VE-ER environments. Fifty percent of therapists (5/10) recommended creating a more realistic immersive experience, including utilizing 3-D VR or making refinements to specific immersive environments. Forty percent of therapists (4/10) reported that they would improve the quality of the narrating voice. One therapist responded with, “not necessarily a change but a point to consider - one of the journeys (The Hero and the Dragon) was triggering for this pt who has a trauma history. The journey became both a trauma exposure and an exposure related to emotional eating… As these journeys are visual (and ideally immersive), [it] may be worth adding a disclaimer or disclosing the scenery of the videos ahead of time in order to enhance safety for the pt.”
3.4. Exploratory Outcomes of Effectiveness
An independent sample t-test was performed to evaluate differences between the two groups at baseline (VE-ER vs TAU group). The results showed no significant differences between the two conditions in all baseline characteristics, except on the WELSQ_NE subscale. Specifically, the VR-ER group showed a lower self-efficacy to resist eating triggered by negative emotions compared to the TAU group (Table 4).
A repeated measures ANOVA was performed to evaluate differences between group frequencies of disordered eating from the therapist note. Results (Table 5) showed a reduction in the frequency of objective binge eating, subjective binge eating, and EE (#OBES, #SBES and #EE) in both groups. Furthermore, results showed an interaction effect of the two conditions and time on EE episodes, specifically there was greater improvement in the VE-ER group. Results showed no other significant differences between the two groups over time.
Finally, a within group analysis was performed to evaluate differences between pre and post treatment on measures in both groups. Results (Table 6) showed a significant reduction in emotion dysregulation (DERS_TOT) post-treatment in the VE-ER group (p value= 0.42; Z value= -2.032) and no other significant changes in the other measures. The TAU group did not show any significant differences from pre- to post-treatment.
4. Discussion
The current study is the first to: (1) elaborate a virtual experiential intervention focused on using emotion regulation strategies for emotional eating and binge eating disorders; (2) integrate somatic manipulation and mindfulness exercises with virtual scenarios in the treatment of eating disorders; and (3) pilot test a virtual experience for emotional eating in a real-world outpatient eating disorders clinic. In a small non-randomized study, we tested the feasibility, acceptability, and preliminary signals of effectiveness of the intervention for improving emotional regulation over eating among adults who had prior eating disorder treatment with a TAU evidence-based eating disorder intervention comparison control. The COVID-19 pandemic prevented the delivery of the virtual immersive scenarios using 3D head-set in person. Instead, the scenarios were delivered remotely via 2-D video conferencing software. Previous studies [36,37,38,39,40] showed the effectiveness of the 2D experience of virtual scenarios in improving participant’s overall psychological and emotional well-being during the COVID-19 pandemic.
Overall, participant retention in treatment was high, with 100% (10/10) of the VE-ER group and 100% of the TAU group completing the interventions. Other psychotherapy trials for binge-eating disorder report drop rates of 4 to 34% [54,55,56,57]. Furthermore, therapist interest in this technology-assisted intervention was reasonably high with 54.55% (6/11) of invited therapists joining the study. In general, these data suggest the adoption of VR-ER appears feasible within a real-world clinic.
In regards to acceptability, participant and therapist CSQ-R scores for VE-ER treatment were in the moderate range at 24.75 and 22.71, respectively, out of a possible total score of 32. In regards to participant satisfaction, the majority suggested that the treatment helped them better regulate emotions and emotional eating, with at least half reporting they would participate in VE-ER again. In regards to the therapist's satisfaction, the majority of them would recommend the VE-ER to another provider treating emotion dysregulation and considered the intervention “excellent” and “good”.
In addition to the therapeutic alliance and cognitive processing or rescripting that occurred during sessions, some patients considered the physical participation of holding objects to be among the most helpful aspects of the VE-ER intervention. From the therapists’ view, one of the most important aspects was the opportunity to discuss and elaborate the metaphorical meaning of the scenarios. These data add to the extensive scientific and clinical literature [58] supporting the importance of therapeutic alliance for work in the clinical setting. These data also reinforce the power of virtual experiences as a metaphorical and narrative tool to be integrated within psychotherapy [34]. These findings further suggest that the addition of bodily involvement is a potential element of therapeutic change.
However, regarding the technology and the virtual scenarios, patient and therapist feedback included the suggestion to convert the technology to 3D VR as well as to improve the narrator’s voice and sound effects. Two participants found the virtual scenarios not at all realistic because of the stimuli not being relatable to real world stimuli. As noted, the intervention initially had been intended to be delivered through a 3-D virtual reality headset and it is assumed that these concerns about realism would have been fewer if a greater sense of presence had been established, as has been found with the multi-sensory stimulation of 3-D virtual reality [59]. Finally, future studies should consider personalizing videos for each participant, a possibility that is actually feasible in VR, for example, by omitting the narrator’s voice while maintaining ambient sounds, or replacing it with that of the therapist. Other options for personalization include having a selection of accents, genders, intensities, duration, pitch, and timbre. The 3-D VR version would also improve accessibility to videos for between-session review by providing unlimited access to all videos on demand.
Despite these recommended enhancements, our study found signals of VE-ER intervention effectiveness. Notwithstanding the pilot nature of this study, the VE-ER intervention did appear to result in a significantly greater rate of EE reduction compared to TAU by end of treatment. In other words, while both groups reduced EE, there was a greater improvement in the VE-ER group. In addition, there was a significant reduction in emotion dysregulation (DERS-TOT scores) only in the VE-ER intervention, with post-intervention DERS-TOT scores close to the non-clinical average range [50]. Consistent with these results, in the VE-ER group only, there was a trend for decreased EE based on the DEBQ_E subscale score and an increasing trend in the ability to resist eating while experiencing negative emotions (on the WELSQ_NE subscale score) from baseline to end of treatment. These findings suggest the clinical utility of combining somatic, multisensory and cognitive manipulations for helping patients with EE to manage their emotions. They are intriguing given the lack of significant changes in emotion regulation from pre- to post-treatment in the TAU group that received a gold-standard treatment.
Our preliminary findings about effectiveness support our expectations regarding the utility of combining somatic marker and virtual scenarios based upon narrative, metaphorical experiences in treating emotional eating.
Specifically, the initial virtual scenarios focus on helping patients identify, experience and accept different emotional states. These scenarios were chosen given evidence that patients with binge eating disorders often have difficulties managing emotions (such as difficulties identifying and classifying the emotional states and/or difficulty in refraining from impulsive behaviors rather than behaving in ways related to their values and long-term goals) [60]. As noted, the somatic marker theory [39] emphasizes that our emotions have a strong somatic component contributing to decision making. As such, maladaptive emotional coping strategies may be the result of past negative experiences that then become habitual and automatic ways of responding.
Our virtual scenarios offered a multisensory experience that seemed to help patients improve interoceptive awareness, to be connected to and focused on their internal body emotional sensations in a nonjudgmental way. Somatic objects promoted sensory stimulation at a tactile level, while virtual scenarios enabled visual and auditory stimulation such that a multisensory experience was ensured.
The nonjudgmental focus on emotional states could have enabled them to become more accepting of negative emotions, rather than feeling compelled to change them by eating or in other ways that might be harmful. Several previous studies showed the efficacy of VR in treating and or/preventing anxiety and pain in patients with eating disorders [61] and in mental health [62].
Other virtual scenarios focused on emotional rescripting may have offered patients a fresh perspective on events that happened in the past, thereby eliciting new feelings, identifying unmet needs, and breaking negative automatic responses (including by thought processes and behaviors) associated with emotions and eating.
Second, the engagement of the body could have enabled to foster the processes mentioned above, spurred by the use of somatic objects and the multi-sensoriality of virtual scenarios that allowed patients to be stimulated at a cognitive, tactile, auditory and visual levels.
Finally, the use of mindfulness technique combined with the use of metaphors and virtual scenarios may have shown the transformative potential of VR [42,63,64] in reinforcing emotional resources and abilities.
There were numerous non-significant changes on the DEBQ subscales (e.g., external eating and restriction) as well as the WELSQ (measuring eating self-efficacy), and AAQ-II (measuring psychological flexibility) scales. Participant scores on the AAQ-II in both groups remained in a clinical range post-treatment [65]. It is interesting however to note, regarding the DEBQ subscales that we started the treatment with a clinical sample with significant findings above 80% from a community norm and were able to drop below that and both the measures. As for the other measures, we hypothesize that our short-term intervention focused on targeting emotion regulation, may be less focused on affecting change in other constructs, such as overall psychological flexibility, or that such effects would be observable over time (e.g., 6-month post-intervention). It is also possible we lacked adequate power to detect significant differences due to our small sample size.
The study has several limitations. First, our primary goal was to investigate feasibility and acceptability. As such, the sample size was small (to conserve resources) and data were primarily descriptive with between and within group analyses exploratory. All exploratory findings need to be interpreted with caution. Furthermore, the study lacked diversity in relation to gender, ethnicity, and socio-economic status. However, these demographics are fairly reflective of the academic eating disorders clinic’s actual patient population, indicating the need to increase access to care to other populations. Second, results showed some missing data (mostly in post-treatment assessment) due to personnel error associated with staffing changes during COVID-19. Relatedly, we could not use the 3-D version and instead used the 2-D version that could be screen shared via telehealth. This is also a strength of the study- in that even with this limitation the study found acceptability and preliminary effects.
Future studies should include a larger, randomized sample, and follow-up to evaluate the long-term effect. Additionally, converting content to a 3D version of the intervention with a VR headset for testing is likely to strengthen user experience and outcome. Collecting physiological measurements, such as skin conductance or heart rate variability, would provide useful objective data to determine the impact of various treatment components.
We believe this pilot study provides a valuable contribution to the scant literature investigating the efficacy and acceptability of translating somatic markers theory described in research literature into real-world clinic settings. The findings from this small study provide preliminary evidence that this virtual intervention for emotional eating among patients is generally acceptable and shows a promising signal of effectiveness within a U.S. clinic setting. This pilot study will serve as a basis for larger, controlled studies evaluating effectiveness.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Summary of VR Intervention’s sessions.
Author Contributions
Conceptualization, C.M., D.L.S., G.R., C.R..; methodology, C.M., D.L.S., C.R., software, L.B., G.R., validation, G.R.; formal analysis, C.M.; investigation, D.L.S. C.R., C.M.; resources, Stanford University, Meta, BECOME Research and Psychology Hub; data curation, C.M..; writing—original draft preparation, C.M., C.K.S., writing—review and editing, D.L.S., C.R., S.L.Y.; visualization, C.M., C.K.S., S.L.Y., D.L.S., C.R. G.R.., supervision, D.L.S., C.R., G.R.; project administration, C.M.; funding acquisition, C.R., D.L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Eating Disorders Association (NEDA) Feeding Hope Fund for Clinical Research, SPO = 133020. Runfola, and Safer, received financial support from this grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board of Stanford University School of Medicine (IRB protocol # = 56591, date of approval = 8/18/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors. The data are not publicly available due to the small sample size and confidentiality concerns.
Acknowledgments
We thank BECOME Research for the contributions to this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McRae, K.; Gross, J.J. Emotion regulation. Emotion 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Vintró-Alcaraz, C.; Munguía, L.; Granero, R.; Gaspar-Pérez, A.; Solé-Morata, N.; Sánchez, I.; Sánchez-González, J.; Menchón, J.M.; Jiménez-Murcia, S.; Fernández-Aranda, F. Emotion regulation as a transdiagnostic factor in eating disorders and gambling disorder: Treatment outcome implications. J Behav Addict 2022, 11, 140–146. [Google Scholar] [CrossRef]
- Reichenberger, J.; Schnepper, R.; Arend, A.-K.; Blechert, J. Emotional eating in healthy individuals and patients with an eating disorder: Evidence from psychometric, experimental and naturalistic studies. Proc Nutr Soc 2020, 79, 290–299. [Google Scholar] [CrossRef]
- Ricca, V.; Castellini, G.; Lo Sauro, C.; Ravaldi, C.; Lapi, F.; Mannucci, E.; Rotella, C.M.; Faravelli, C. Correlations between binge eating and emotional eating in a sample of overweight subjects. Appetite 2009, 53, 418–421. [Google Scholar] [CrossRef]
- Barak, R.; Shuval, K.; Li, Q.; Oetjen, R.; Drope, J.; Yaroch, A.L.; Fennis, B.M.; Harding, M. Emotional eating in adults: The role of sociodemographics, lifestyle behaviors, and self-regulation—Findings from a U.S. national study. Int J Environ Res Public Health 2021, 18, 1744. [Google Scholar] [CrossRef]
- Bemanian, M.; Mæland, S.; Blomhoff, R.; Rabben, Å.K.; Arnesen, E.K.; Skogen, J.C.; Fadnes, L.T. Emotional eating in relation to worries and psychological distress amid the covid-19 pandemic: A population-based survey on adults in Norway. International Journal of Environmental Research and Public Health 2021, 18, 130. [Google Scholar] [CrossRef]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef]
- Braden, A.; Musher-Eizenman, D.; Watford, T.; Emley, E. Eating when depressed, anxious, bored, or happy: Are emotional eating types associated with unique psychological and physical health correlates? Appetite 2018, 125, 410–417. [Google Scholar] [CrossRef]
- Lazarevich, I.; Irigoyen Camacho, M.E.; Velázquez-Alva, M.D.C.; Zepeda Zepeda, M. Relationship among obesity, depression, and emotional eating in young adults. Appetite 2016, 107, 639–644. [Google Scholar] [CrossRef]
- Schneider, K.L.; Appelhans, B.M.; Whited, M.C.; Oleski, J.; Pagoto, S.L. Trait anxiety, but not trait anger, predisposes obese individuals to emotional eating. Appetite 2010, 55, 701–706. [Google Scholar] [CrossRef]
- Nguyen-Rodriguez, S.T.; Chou, C.-P.; Unger, J.B.; Spruijt-Metz, D. BMI as a moderator of perceived stress and emotional eating in adolescents. Eat Behav 2008, 9, 238–246. [Google Scholar] [CrossRef]
- Tchanturia, K.; Davies, H.; Harrison, A.; Fox, J.R.E.; Treasure, J.; Schmidt, U. Altered social hedonic processing in eating disorders. International Journal of Eating Disorders 2012, 45, 962–969. [Google Scholar] [CrossRef]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef]
- Pink, A.E.; Lee, M.; Price, M.; Williams, C. A Serial mediation model of the relationship between alexithymia and BMI: The role of negative affect, negative urgency and emotional eating. Appetite 2019, 133, 270–278. [Google Scholar] [CrossRef]
- Tan, C.C.; Chow, C.M. Stress and Emotional Eating: The mediating role of eating dysregulation. Personality and Individual Differences 2014, 66, 1–4. [Google Scholar] [CrossRef]
- Casagrande, M.; Mingarelli, A.; Guarino, A.; Favieri, F.; Boncompagni, I.; Germanò, R.; Germanò, G.; Forte, G. Alexithymia: A facet of uncontrolled hypertension. International Journal of Psychophysiology 2019, 146, 180–189. [Google Scholar] [CrossRef]
- Taylor, G.J.; Parker, J.D.; Bagby, R.M.; Bourke, M.P. Relationships between Alexithymia and psychological characteristics associated with eating disorders. J Psychosom Res 1996, 41, 561–568. [Google Scholar] [CrossRef]
- Blair, A.J.; Lewis, V.J.; Booth, D.A. Does emotional eating interfere with success in attempts at weight control? Appetite 1990, 15, 151–157. [Google Scholar] [CrossRef]
- Frayn, M.; Knäuper, B. Emotional eating and weight in adults: A review. Current Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Porter, A.M. Weight stigma and eating behavior: A review of the literature. Appetite 2016, 102, 3–14. [Google Scholar] [CrossRef]
- Michopoulos, V.; Powers, A.; Moore, C.; Villarreal, S.; Ressler, K.J.; Bradley, B. The mediating role of emotion dysregulation and depression on the relationship between childhood trauma exposure and emotional eating. Appetite 2015, 91, 129–136. [Google Scholar] [CrossRef]
- Katterman, S.N.; Kleinman, B.M.; Hood, M.M.; Nackers, L.M.; Corsica, J.A. Mindfulness meditation as an intervention for binge eating, emotional eating, and weight loss: A systematic review. Eat Behav 2014, 15, 197–204. [Google Scholar] [CrossRef]
- Beaulac, J.; Sandre, D.; Mercer, D. Impact on mindfulness, emotion regulation, and emotional overeating of a DBT skills training group: A Pilot Study. Eat Weight Disord 2019, 24, 373–377. [Google Scholar] [CrossRef]
- Lattimore, P. Mindfulness-based emotional eating awareness training: Taking the emotional out of eating. Eat Weight Disord 2020, 25, 649–657. [Google Scholar] [CrossRef]
- Geraets, C.N.W.; van der Stouwe, E.C.D.; Pot-Kolder, R.; Veling, W. Advances in immersive virtual reality interventions for mental disorders: A new reality? Curr Opin Psychol 2021, 41, 40–45. [Google Scholar] [CrossRef]
- Colombo, D.; Díaz-García, A.; Fernandez-Álvarez, J.; Botella, C. Virtual reality for the enhancement of emotion regulation. Clinical Psychology & Psychotherapy 2021, 28, 519–537. [Google Scholar] [CrossRef]
- Brown, T.; Vogel, E.N.; Adler, S.; Bohon, C.; Bullock, K.; Nameth, K.; Riva, G.; Safer, D.L.; Runfola, C.D. Bringing virtual reality from clinical trials to clinical practice for the treatment of eating disorders: An example using virtual reality cue exposure therapy. Journal of Medical Internet Research 2020, 22, e16386. [Google Scholar] [CrossRef]
- Mancini, A.; Mancini, F. Rescripting memory, redefining the self: A meta-emotional perspective on the hypothesized mechanism(s) of imagery rescripting. Front Psychol 2018, 9, 581. [Google Scholar] [CrossRef]
- Arntz, A. Imagery rescripting as a therapeutic technique: Review of clinical trials, basic studies, and research agenda. Journal of Experimental Psychopathology 2012, 3, 189–208. [Google Scholar] [CrossRef]
- Riva, G.; Malighetti, C.; Serino, S. Virtual reality in the treatment of eating disorders. Clinical Psychology & Psychotherapy 2021, 28, 477–488. [Google Scholar] [CrossRef]
- Ghaderi, A.; Welch, E.; Zha, C.; Holmes, E.A. Imagery rescripting for reducing body image dissatisfaction: A randomized controlled trial. Cogn Ther Res 2022, 46, 721–734. [Google Scholar] [CrossRef]
- Morina, N.; Lancee, J.; Arntz, A. Imagery rescripting as a clinical intervention for aversive memories: A meta-analysis. J Behav Ther Exp Psychiatry 2017, 55, 6–15. [Google Scholar] [CrossRef]
- Riva, G. The key to unlocking the virtual body: Virtual reality in the treatment of obesity and eating disorders. J Diabetes Sci Technol 2011, 5, 283–292. [Google Scholar] [CrossRef]
- Riva, G. Virtual reality in clinical psychology. Comprehensive Clinical Psychology 2022, 91–105. [Google Scholar] [CrossRef]
- Wilson, M. Six views of embodied cognition. Psychon Bull Rev 2002, 9, 625–636. [Google Scholar] [CrossRef]
- Riva, G. The neuroscience of body memory: From the self through the space to the others. Cortex 2018, 104, 241–260. [Google Scholar] [CrossRef]
- Barrett, L.F. The theory of constructed emotion: An active inference account of interoception and categorization. Social Cognitive and Affective Neuroscience 2017, 12, 1–23. [Google Scholar] [CrossRef]
- Barrett-Cheetham, E.; Williams, L.A.; Bednall, T.C. A differentiated approach to the link between positive emotion, motivation, and eudaimonic well-being. The Journal of Positive Psychology 2016, 11, 595–608. [Google Scholar] [CrossRef]
- Damasio, A. Self Comes to Mind: Constructing the Conscious Brain; Self comes to mind: Constructing the conscious brain; Pantheon/Random House: New York, NY, US, 2010; pp. xi, 367. ISBN 978-0-307-37875-0. [Google Scholar]
- Damasio, A.; Carvalho, G.B. The nature of feelings: Evolutionary and neurobiological origins. Nat Rev Neurosci 2013, 14, 143–152. [Google Scholar] [CrossRef]
- Malighetti, C.; Schnitzer, C.; Potter, G.; Nameth, K.; Brown, T.; Vogel, E.; Riva, G.; Runfola, C.D.; Safer, D.L. Rescripting emotional eating with virtual reality: A Case Study. Annual Review of Cybertherapy and Telemedicine 2021. [Google Scholar]
- Malighetti, C.; Bernardelli, L.; Pancini, E.; Riva, G.; Villani, D. Promoting Emotional and Psychological Well-being during COVID-19 Pandemic: A self-help virtual reality intervention for university students. Cyberpsychology, Behavior, and Social Networking 2023, 26, 309–317. [Google Scholar] [CrossRef]
- Riva, G.; Malighetti, C.; Chirico, A.; Di Lernia, D.; Mantovani, F.; Dakanalis, A. Virtual reality. In Rehabilitation interventions in the patient with obesity; Capodaglio, P., Ed.; Springer International Publishing: Cham, 2020; pp. 189–204. ISBN 978-3-030-32274-8. [Google Scholar]
- Riva, G.; Bernardelli, L.; Castelnuovo, G.; Di Lernia, D.; Tuena, C.; Clementi, A.; Pedroli, E.; Malighetti, C.; Sforza, F.; Wiederhold, B.K.; et al. A virtual reality-based self-help intervention for dealing with the psychological distress associated with the COVID-19 lockdown: An Effectiveness Study with a Two-Week Follow-Up. International Journal of Environmental Research and Public Health 2021, 18, 8188. [Google Scholar] [CrossRef]
- Meyer, D.; Van Rheenen, T.E.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Sumner, P.J.; Rossell, S.L. Surviving the COVID-19 pandemic: An examination of adaptive coping strategies. Heliyon 2022, 8, e09508. [Google Scholar] [CrossRef]
- Farahimanesh, S.; Serino, S.; Tuena, C.; Di Lernia, D.; Wiederhold, B.K.; Bernardelli, L.; Riva, G.; Moradi, A. Effectiveness of a virtual-reality-based self-help intervention for lowering the psychological burden during the COVID-19 pandemic: Results from a randomized controlled trial in Iran. Journal of Clinical Medicine 2023, 12, 2006. [Google Scholar] [CrossRef]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The role and interpretation of pilot studies in clinical research. J Psychiatr Res 2011, 45, 626–629. [Google Scholar] [CrossRef]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of client/patient satisfaction: Development of a general scale. Eval Program Plann 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Harrison, A.; Sullivan, S.; Tchanturia, K.; Treasure, J. Emotional functioning in eating disorders: Attentional bias, emotion recognition and emotion regulation. Psychol Med 2010, 40, 1887–1897. [Google Scholar] [CrossRef]
- Van Strien, T.; Frijters, J.E.; Bergers, G.P.; Defares, P.B. The Dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. International Journal of Eating Disorders 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Tyndall, I.; Waldeck, D.; Pancani, L.; Whelan, R.; Roche, B.; Dawson, D.L. The acceptance and action questionnaire-II (AAQ-II) as a measure of experiential avoidance: Concerns over discriminant validity. Journal of Contextual Behavioral Science 2019, 12, 278–284. [Google Scholar] [CrossRef]
- Navidian A reliability and validity of the weight efficacy lifestyle questionnaire in overweight and obese individuals. International Journal of Behavioral Sciences 2009, 3, 217–222.
- Brownley, K.A.; Berkman, N.D.; Peat, C.M.; Lohr, K.N.; Cullen, K.E.; Bann, C.M.; Bulik, C.M. Binge-eating disorder in adults: A systematic review and meta-analysis. Ann Intern Med 2016, 165, 409–420. [Google Scholar] [CrossRef]
- De Zwaan, M.; Herpertz, S.; Zipfel, S.; Svaldi, J.; Friederich, H.-C.; Schmidt, F.; Mayr, A.; Lam, T.; Schade-Brittinger, C.; Hilbert, A. Effect of internet-based guided self-help vs individual face-to-face treatment on full or subsyndromal binge eating disorder in overweight or obese patients: The INTERBED Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 987–995. [Google Scholar] [CrossRef]
- Runfola, C.D.; Kirby, J.S.; Baucom, D.H.; Fischer, M.S.; Baucom, B.R.W.; Matherne, C.E.; Pentel, K.Z.; Bulik, C.M. A pilot open trial of UNITE-BED: A couple-based intervention for binge-eating disorder. Int J Eat Disord 2018, 51, 1107–1112. [Google Scholar] [CrossRef]
- Safer, D.L.; Robinson, A.H.; Jo, B. Outcome from a randomized controlled trial of group therapy for binge eating disorder: Comparing dialectical behavior therapy adapted for binge eating to an active comparison group therapy. Behav Ther 2010, 41, 106–120. [Google Scholar] [CrossRef]
- Zaitsoff, S.; Pullmer, R.; Cyr, M.; Aime, H. The role of the therapeutic alliance in eating disorder treatment outcomes: A systematic review. Eat Disord 2015, 23, 99–114. [Google Scholar] [CrossRef]
- Riva, G.; Malighetti, C.; Serino, S. Virtual reality in the treatment of eating disorders. Clinical Psychology & Psychotherapy 2021, 28, 477–488. [Google Scholar] [CrossRef]
- Dingemans, A.; Danner, U.; Parks, M. Emotion regulation in binge eating disorder: A review. Nutrients 2017, 9, 1274. [Google Scholar] [CrossRef] [PubMed]
- Surmay, C.; Vo, M.; Derenne, J.; Sherman, D. Virtual reality mindfulness therapy for anxiety and pain management in adolescent and young adult patients with eating disorders. Journal of Adolescent Health 2020, 66, S62–S63. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, D.; Xu, N.; Yang, J. The effectiveness of immersive virtual reality (VR) based mindfulness training on improvement mental-health in adults: A narrative systematic review. Explore (NY) 2023, 19, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K.; Mantovani, F. Neuroscience of virtual reality: From virtual exposure to embodied medicine. Cyberpsychol Behav Soc Netw 2019, 22, 82–96. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, E.; Quesnel, D.; Riecke, B. Understanding AWE: can a virtual journey, inspired by the overview effect, lead to an increased sense of interconnectedness? Frontiers in Digital Humanities 2019, 6. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the acceptance and action questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behav Ther 2011, 42, 676–688. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Virtual scenarios in the VE-ER for Sessions 2-7.
| Virtual Scenarios* | Description |
|---|---|
 |
The Secret Garden (duration 13:10 minutes) is characterized by a tranquil nature scene intended to help the viewer immediately perceive a sense of calm. Throughout the video the narrative voice guides participants on a walk around a garden on a sunny day. |
 |
The Waterfall in the Prairie (duration 14:13 minutes) scenario takes participants on a walk in a prairie that leads them to a waterfall. As in the first video, this scenario aims to help the participant experience calm and greater awareness of their sensations. |
 |
The Desert and the Oasis (duration 11:32 minutes) shows a stark and desolate environment. Here participants faced a sandstorm and a scorpion, a symbol of menace, which is overcome by participants in order to return to a more peaceful path. Themes such as loneliness, abandonment, silence, and survival may surface. |
 |
The Boat and the Sea (duration 11:12 minutes) involves a journey in a boat, during which a strong storm takes place, perhaps symbolizing a moment of difficulty or anxiety experienced in real life. Participants managed to overcome the storm, and re-experience clear skies and a serene view of the shore. |
 |
The Mountain and the Backpack (duration 13:32 minutes), is a walk along a path in the mountains, during which a heavy stone in a backpack is transformed into a lighter stone, enabling the journey to continue more easily. The scenario involves themes such as challenges, discovery, goals to achieve, resilience, and spirituality. |
 |
In the final video, The Hero and the Dragon (duration 14:05 minutes), participants encounter a frightening dragon that becomes smaller and smaller throughout the video. Participants then manage to reach a door that leads to a treasure chest from which a light emanates, symbolizing the achievement of goals and increasing awareness of their own resources in the face of difficulties. *Images courtesy of Become-hub. |
Table 2.
Emotion Regulation and Rescripting’s sessions .
| Emotion Regulation Sessions | The Role of the Experimenter |
| Introduction to the first two immersive experiences (5 minutes) | Remind patient of the purpose of the emotion regulation intervention and how the intervention will be administered. “We will now turn to the emotion regulation intervention. As a reminder, the purpose of this intervention is to help you to increase your awareness and ability to recognize your emotional states. I will begin with helping you focus on the present moment and your body. Then you will be immersed in a waterfall landscape and a voice will guide you in the exploration of this scene. The voice will encourage you to pay attention to physical sensations, your breath and to the environment. After the immersive experience we will talk about your feeling and thoughts about what you experienced. Let me know if you have any questions or need a break.” |
| Focus on Attention (5 minutes) |
“If you aren’t already, please sit in a comfortable position, letting your back adopt a straight but not rigid posture. A dignified and comfortable posture, with the soles of your feet parallel to the ground and your legs uncrossed. Place your hands comfortably on your thighs or on your lap. And if you feel comfortable, you can gently close your eyes or keep your eyes open, with a soft, unfocused gaze. When you are ready, bring your awareness to the level of your physical sensations, directing your attention to the sensations, pressure and friction in your body at the points where your body is in contact with the chair or whatever is supporting you. Spend a few moments exploring these sensations, in your feet, in your legs, and your hands, back, etc [pause]. And now direct your attention and focus it on the flow of physical sensations in your abdomen, while the air enters and exits the body [pause]. Try to connect yourself with the flow of the physical sensations in the abdomen for the entire duration of each inhalation and exhalation [pause]. There is no need to try to control your breathing, just let it go [pause]. As you continue to focus awareness on the bodily sensations of the area that enters and exits, sooner or later your mind may move away from the breath, perhaps wandering aimlessly, or be taken over by a thought, a project, a fantasy [pause]. This wandering and being distracted is a normal thing, not a mistake or a failure [pause]. When you notice that your attention is no longer on the breath, pause for a moment to see where the mind has gone, congratulating yourself for being aware of your experience in the moment [pause]. Then, voluntarily turn your attention away from what distracted you and gently bring it back to the sensation of breathing, by focusing completely on breathing in and out. [pause]. Remind yourself from time to time that your only goal is to be aware of your experience moment by moment, the best you can; and that breathing is available to you at all times, when you need an anchor to bring you back to the present moment [pause]. And now, when you're ready, slowly emerge from this experience, redirecting your attention to space and time.” [note: If possible, continue straight from this experience to the immersive environment to avoid moving the focus away from their focus on their bodily experience. If the person appears uncomfortable or voices any concerns, the therapist can feel free to ask about the experience. For example, you can ask: “What was it like to breathe in and out, focus on the breath, have your mind wander, etc?) |
| VR Scenarios (12 minutes) | Session 1: The Secret Garden Introduce Scene: “We will now start the secret garden immersive experience. In the secret garden experience, we will guide you through a protected place (a large but closed natural garden) where you will find access to a new, internal, world of well-being and awareness (through the portal of the cherry trees). Session 2: The Waterfall and the Prairie Introduce Scene: “In addition to the main goal of promoting relaxation, this experience, specifically, will help you lighten your thoughts and emotions providing a safety and protection feeling (an open but safe natural place protected by streams and fences).” |
| Identification of the safe place (5 minutes) |
After the immersive experience, ask the patient to think through the immersive experience and identify the moment of greatest well-being and serenity. For example: “Go back with your mind to the immersive journey and try to remember the moment when you felt the greatest sense of well-being or serenity. Describe the place and the feeling” If they did not experience a sense of well-being or serenity, therapist can ask what “positive” or “neutral” emotions they felt at any point. Let them describe where they felt them in the scene. |
| Anchoring the New Somatic Marker (10 minutes) |
Create an anchor by linking the positive emotion experienced in the virtual environment to a real experience the patient had in the “real world.” Let them close their thumb between their 4 fingers while they are retrieving the real-life experience. “Now, close your eyes, and --focusing on the emotion that you felt in the VR-- try to recall in your mind an experience that you had in your real life in which you felt this emotion. As you recall this event, close your thumb between the 4 fingers of your hand. Feel the contact of your thumb on your skin and recall as many details as possible. If you feel comfortable, could you share this event with me?” Let them describe the real-life experience in great detail to you. [The greater the detail, the more vivid the recollection and the subsequent re-experience.] “Every time that you need to feel this emotion you can make this gesture with your hands. This will bring you back to this present moment and to this positive sensation”. |
| Homework | Patients at the end of the experience will receive a mp3 or video copy of this immersive experience in order to practice it every day at home before breakfast or in a particular emotional moment of the day. “I will email you the mp3 and video of this VR experience. Try to listen or watch it before breakfast. This might help you to be more focused as well as more aware of yourself and of what you truly need. If you feel anxious or the urge to eat, try to listen this audio, and make the gesture with your hands that you’ve already learned. We are trying to help you to be more aware of what is happening in your body and to teach you some skills to face the obstacles that you may meet in your real life.” |
| Emotional Rescripting Sessions | The Role of Experimenter |
| Check in & review homework (5 minutes) |
“How did the homework go last week with listening (or watching) the… scenarios?” If completed, process experiences (thoughts and feelings) to facilitate new learning. Use CBT/DBT strategies. If not completed, assess barriers to completion and problem solve around overcoming barriers. |
| Assessment: Therapist Note | Assessment of any changes to emotional eating? (Obtain frequency of behaviors—OBEs, SBEs, and purges, as well as assess presence of emotional eating using the following scale: never, seldom, sometimes, often, always) Any changes to emotional eating compared to last session? (same, worse, better) |
| Brief Introduction to Rescripting Immersive Experiences |
The somatic marker theory posits that emotions are changes in both our body and brain states. Over time, emotions and their corresponding bodily changes, which are called "somatic markers", become associated with particular situations and their past outcomes. These changes are autonomic and reflect prior experience of that event, usually a negative consequence. Once formed, the somatic markers are reactivated every time the person encounters similar situations to those that originally induced the emotion reaction. The reactivation of the somatic markers reclaims the associated body state. For example, if you were judged in high school for what you ate-- causing understandable negative somatic experiences of anxiety, shame, rapid heartbeat, sweating, etc., then every time you ate in front of those peers, your body may have “memorized” the connection between the negative internal states and eating with others. As such, you might find the same feelings of discomfort present later in life even when those reactions wouldn’t make sense, for example, when eating with friends who make you feel safe and have never judged or criticized your eating before. An improvement in managing emotions then must depend on a change in the somatic memory of the body. If we experience a negative situation similar to one that we met in the past, our body reproduces the same answers learned in the past (due to body memory). This makes change impossible. It is necessary to rescript this automatic mechanism (somatic marker) to modify the emotional experience. We know that an individual’s awareness and understanding of emotions may constitute a necessary step to successfully regulate the emotions. |
| Focus on attention exercise (5 minutes). | The same script of previous sessions |
| VR Scenarios: The Desert and the Oasis Experience; The Mountain and the Backpack; The Boat and the Sea; The Hero and the Dragon |
Introduce Scene: “You will be immersed in a metaphorical journey through ….., holding a …. like object in your hand” [if in person session, can add: “that I will give you at the right time.”]. The immersive experience will take 10 minutes. After, we will talk about what you felt and thought during this journey”. During the experience, therapists should observe patients’ behavior silently. This observation of the patient’s body language can offer useful information. If the patient appears very distressed, for example and the therapists feel the need to intervene, the therapist could stop the video and take a moment to discuss with him/her what they are experiencing and possibly insert a coping skill, reframe, reminder about how repeated exposure can help regulate emotions, etc.) As noted, please ask the patient to have a real object similating a … available to grab while they’re watching the video. When the narrative voice mentions the …, please remind the patient to grab the real walking stick in order to involve the body for the somatic marker modification. If patient doesn’t have access to a walking stick, therapist can suggest some alternatives as per above. |
| Emotion Evaluation (10 minutes) |
Purpose: The concretization of what patients felt during the immersive experience will lead them to be able to face and manage their emotions. Once the immersive experience is over, ask the patients to identify and localize in the body what they felt. For example: “Return with your mind to the immersive experience. How did it feel? Did you feel a negative or a positive emotion? If they felt both positive and negative emotions, start always with NEGATIVE. Then, after the desensitization, start with positive reinforcement. IF NEGATIVE: Once the emotion is identified, in case of negative experience it will be reduced or tolerated through the use of awareness and acceptance, physicalizing exercises (treating unwanted content as an object), defusion/desensitization exercises (making it move away to the horizon until it disappears; make it smaller and smaller until it disappears; make it decompose into many small pixels until it disappears), and/or containment Potential questions to ask: Close your eyes and return with your mind to the immersive experience: Q1. (Awareness): Focus on the different parts of your body, WHERE did you feel this emotion? Q2. (Physicalizing) Can you give a shape to this emotion? As a natural element, or a Geometric object. Q3. What color is emotion? Q4. Is the object moving or still? Q5.(Systematic desensitization) “Close your eyes and try to focus on the object. It is (color and the name of the object) and it starts to move counterclockwise. As it starts to move, it moves further and further away to the horizon, until it disappears, like a dot.” Or talk about small pixels that crumble and moves further and further away as a cloud that branches out and there is no more. If the patient does not manage to make the negative emotion disappear... You can have him/her imagine a drawer or a box where to put the emotion left (containment) or assist them in simply sitting with the emotion (to improve tolerance) IF POSITIVE: Once the emotion is identified, in case of positive experience it will be amplified. Close your eyes and return with your mind to the immersive experience: Q1. Focus on the different parts of your body, WHERE did you feel this emotion? Q2. Can you give a shape to this emotion? As a natural element, or a Geometric object. Q3. What color is the emotion? Q4. Is the object moving or still? “Now that you have noticed where you felt this emotion in your body and that you have seen its shape, and its color, try to imagine to breath inside this emotion. Every breath you take, the emotion expands throughout the body.” At this point: Anchor by linking the positive emotion experienced in the immersive environment to a real experience lived in the real world. For example: “Close your eyes and try to recall in your mind an experience that you lived in the real world in which you felt this positive emotion. “Close your thumb between your 4 fingers. Feel the contact with the thumb and try to recall an episode when you felt this same way. Try to retrieve as many details as possible.” This positive experience will be memorized in your body and will be available to you every time you need it by making the gesture and using the mp3. |
| Homework: | At the end of each session, patients will be asked to repeat the rescripting experience every day before bedtime, using a mp3 audio version of the experience and the real objects associated. The audio version of the intervention will lead the patient to relive the immersive experience by recreating in mind the emotional and somatic screenplay. |
Table 3.
Summary of VE-ER sessions with the respective theme and somatic object.
| Summary of sessions | Theme |
|---|---|
| The Secret Garden | Build emotional awareness and strengthen mindfulness skills |
| The Waterfall and the Prairie | Build emotional awareness and strengthen mindfulness skills |
| The Desert and the Oasis | Continuing/proceeding despite adversity (sandstorm, scorpion). Somatic marker: a walking stick. |
| The Boat and the Sea | Using a/an (inner) compass to guide you, stay on course (i.e., values-directed action), see the bigger picture instead of overfocus on details, etc. Somatic marker: something that feels like a compass, such as the lid of a bottle or jar. |
| The Mountain and the Backpack | What is keeping the patient weighed down/stuck as they journey through life trying to achieve their goals? Somatic marker: a backpack that can be loaded (to be heavy) and then lightened. |
| The Hero and the Dragon | Patient is the hero of their own quest. Somatic marker: a key |
Table 4.
Differences between VE-ER and TAU group at baseline.
| Measures | VE-ER Group N=10 |
TAU Group N=11 |
t | Sign |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| DERS_TOT | 109.80±22.90 | 108.64±22.47 | .117 | .908 |
| DEBQ-R | 3.09±.79 | 2.78±.50 | 1.064 | .301 |
| DEBQ-E | 4.12±.49 | 3.55±1 | 1.634 | .119 |
| DEBQ-EXT | 3.35±.88 | 2.99±.60 | 1.093 | .288 |
| AAQ_II | 33.40±6.50 | 30.82±5.98 | .948 | .355 |
| WELSQ_NE | 9.90±6.80 | 15.73±6.21 | -2.051 | .054* |
| WELSQ_AV | 16.40±8.50 | 19.18±8.32 | -.757 | .458 |
| WELSQ_SP | 16.70±8.23 | 21.36±6.21 | .351 | .157 |
| WELSQ_PD | 17.20±9.36 | 20.18±6.94 | -.834 | .414 |
| WELSQ_PA | 22±5.59 | 24.45±4.84 | -1.092 | .288 |
| #OBES | 1.50±1.50 | .73±1.47 | .748 | .984 |
| #SBES | 1.70±1.98 | 3.43±2.57 | -1.962 | .951 |
| #PURGES | .60±1.35 | .64±2.11 | -.047 | .750 |
| #EE | 3.40±1.07 | 2.92±.90 | 1.26 | .222 |
*The mean difference is significant at the 0.05 level. DEBQ-R: restrained eating; DEBQ-E emotional eating; DEBQ-EXT external eating; DERS TOT: Difficulties in emotion regulation total score; AAQ_II The Acceptance and Action questionnaire; WELSQ_NE The negative emotions -Weight Efficacy Life-Style Questionnaire; WELSQ_AV The availability subscale; WELSQ_SP The social pressure subscale; WELSQ_PD The physical discomfort; WELSQ_PA the positive activities subscale. #OBEs: number of objectively large binge episodes in the previous week; #SBEs: number of subjectively large binge episodes in the previous week; #PURGEs: numbers of vomiting episodes in the previous week. #EE: emotional eating episodes frequency, Never (1), Seldom (2), Sometimes (3), Often (4) Always (5).
Table 5.
Between group differences (VE-ER vs TAU) for episodes of binges, subjective binges, purges, and emotional eating.
Table 5.
Between group differences (VE-ER vs TAU) for episodes of binges, subjective binges, purges, and emotional eating.
| VE-ER Group (n=10) |
TAU Group (n=11) |
Anova | ||||||
|---|---|---|---|---|---|---|---|---|
| Measures | Pre | Post | Pre | Post | Time | Group*time | ||
| Mean ±SD | Mean ±SD | Mean ±SD | Mean ±SD | F | Sig. | F | Sig. | |
| #EE | 3.40±1.07 | 1.90±.73 | 2.92±.90 | 2±.60 | 13.07 | .002* | 4.95 | .038* |
| #SBES | 1.70±1.98 | .80±1.13 | 3.43±2.57 | 1.42±1.24 | 9.29 | .007* | 2.69 | .117 |
| #Purge | .60±1.35 | 0±.00 | .64±2.11 | .45±1.50 | 3.03 | .098 | .869 | .363 |
| #OBES | 1.50±1.50 | .80±1.13 | .73±1.47 | .55±.88 | 7.61 | .012* | .005 | .947 |
Table 6.
Within group analysis for VE-ER and TAU conditions.
| VE-ER Group | TAU Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Pre N=10 |
Post N=5 |
Pre N=11 |
Post N=11 |
|||||
| Measures | Mean ± SD | Mean ± SD | z | Sign | Mean ± SD | Mean ± SD | z | Sign |
| DERS_TOT | 109.80±22.90 | 86±26.46 | -2.032 | .042* | 108.64±22.47 | 102.09±20.62 | -1.07 | .284 |
| DEBQ-R | 3.09±.79 | 2.66±.95 | -.674 | .500 | 2.78±.50 | 2.76±.72 | .089 | .929 |
| DEBQ-E | 4.12±.49 | 3.20±.67 | -1.753 | .060 | 3.55±1 | 3.38±.92 | -.561 | .575 |
| DEBQ-EXT | 3.35±.88 | 3.10±.99 | -1.604 | .109 | 2.99±.60 | 2.97±.49 | -.102 | .919 |
| AAQ_II | 33.40±6.50 | 30.20±10.68 | -1.095 | .273 | 30.82±5.98 | 29.91±7.36 | -.66 | .504 |
| WELSQ_NE | 9.90±6.80 | 18.80±5.63 | -1.753 | .070 | 15.73±6.21 | 15±5.86 | -.67 | .501 |
| WELSQ_AV | 16.40±8.50 | 20.80±9.49 | -944 | .354 | 19.18±8.32 | 16.82±8.08 | -.66 | -505 |
| WELSQ_SP | 16.70±8.23 | 23.40±7.05 | -1.214 | .225 | 21.36±6.21 | 19±11.27 | -81 | .413 |
| WELSQ_PD | 17.20±9.36 | 23.40±8.26 | .000 | 1 | 20.18±6.94 | 20.18±5.28 | -.35 | .720 |
| WELSQ_PA | 22.99±5.59 | 23.40±7.12 | -.406 | .684 | 24.45±4.69 | 22.36±6.57 | -.75 | .449 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



