Submitted:
26 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
Xpert MTB/RIF is rapid molecular diagnostic tool capable of simultaneously detecting Mycobacterium tuberculosis and rifampicin resistance. This study aimed to access the diagnostic precision of Xpert MTB/RIF assay to detect pulmonary and extra-pulmonary tuberculosis and to evaluate the performance for the detection of rifampicin resistance. Of 37695 samples, 7156(18.98%) were tuberculosis positive, 509(7.11%) were rifampicin-resistant. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for PTB were 99.87% (95%CI:99.75-99.94), 99.92%(95%CI:99.88-99.95), 99.71%(95%CI:99.54-99.82),99.97%(95%CI:99.93-99.98),21.38% (95%CI:20.92-21.86),and 99.91%(95%CI:99.87-99.94), respectively. For EPTB, the sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay accounted for 99.45% (95%CI:98.73-99.82),99.84%(95%CI:99.73-99.92),98.70%(95%CI:97.73-99.25),99.93% (95%CI:99.84-99.97),10.64%(95%CI:9.99-11.31),and 99.80%(95%CI:99.68-99.88), respectively. Despite its high sensitivity for detecting tuberculosis and rifampicin resistance, Xpert MTB/RIF had contradictory results for 20.5% of cases among patients with negative smear results and 54.9% of cases among patients with a high risk of Multidrug-resistant tuberculosis. Of 47 fluoroquinolone-resistant, 16.56% (26/157) of Multidrug-resistant tuberculosis isolates and 4.02% (20/498) isoniazid-resistant are fluoroquinolone-resistant, a characteristic distribution leading to about 17.2% of fluoroquinolone resistance events and relevant marker gyr-A mutations in MDR tuberculosis isolates. Further, our study indicated that increased fluoroquinolone resistance among Rifampicin-resistant and isoniazid-resistant tuberculosis endangers the success of newly endorsed MDR-TB regimens.
Keywords:
Mycobacterium tuberculosis
; Rifampicin
; drug resistant
; sensitivity
; specificity
1. Introduction
Tuberculosis (TB) is an infectious disease, one of the leading causes of global human death.TB was the foremost cause of death from a single contagious agent, ranking above HIV/AIDS until the coronavirus (COVID-19) pandemic emerged. The increase in TB ill from 10.1 million in 2020 to 10.6 million in 2021, reversing many years of slow decline of TB cases worldwide. Similarly, the estimated TB incidence rate (new cases per lakh population per year) increased by 3.6% between 2020 and 2021, following declines in TB incidence rate by about 2% per year for most of the past two decades[1]. The number of incident TB patients (new & relapse) notified has risen 19% from 16 28,161 in 2020 to 19 33,381 in 2021. The main reason for the increase in TB incidence between 2020 and 2021 is the impact of the COVID-19 pandemic on TB detection. Eight countries in the world accounted for more than two-thirds of global TB cases in 2021: India (28%), Indonesia (9.2%), China (7.4%), the Philippines (7.0%), Pakistan (5.8%), Nigeria (4.4%), Bangladesh (3.6%) and the Democratic Republic of the Congo (2.9%). Drug-resistant tuberculosis (DR-TB) is a severe public health problem worldwide, and the incidence rate of MDR/RR-TB cases has risen 3.1% from 437000 in 2020 to 450000 in 2021. Globally, three countries accounted for the largest share of incident cases of MDR/RR-TB in 2021: India (26% of global cases), the Russian Federation (8.5% of global cases), and Pakistan (7.9% of global cases) [2].
Innovative strategies such as services of rapid molecular diagnostics of TB to people everywhere and high-risk TB patient’s upfront (accessibility) and an integrated health-system approach for the delivery of service with other components, including counselling in the general healthcare system (availability) require explored and implemented for early diagnosis and decentralized delivery of drug-resistant TB services. Over a half million people have had Multidrug Resistance Tuberculosis (MDR-TB), and 156 071 were registered in MDR-TB treatment as per the World Health Organization [3] 2020 report. The Drug-resistance testing coverage ranges from 46% to 83% among new and formerly treated TB patients [4]. Prompt and ample tuberculosis diagnosis is essential for optimal tuberculosis control strategies, resulting in early treatment of tuberculosis and multidrug-resistant tuberculosis (MDR-TB) patients. Molecular tests for tuberculosis and multidrug-resistant tuberculosis (MDR-TB) have developed remarkably owing to the vital challenges faced by countries with high tuberculosis burden, the emergence of multidrug-resistant tuberculosis, and extremely drug-resistant tuberculosis (XDR-TB) worldwide.
WHO-endorsed Xpert MTB/RIF assay is a new test that revolutionizes tuberculosis (TB) control by contributing to the rapid diagnosis of Tuberculosis disease and drug resistance. Implementing rapid diagnostic tests like Xpert and expanding MDR-TB treatment centers at peripheral healthcare facilities were the interventions used to decrease gaps of low case detection and delayed treatment enrolment. The Xpert MTB/RIF testing is a rapid molecular diagnostic test performed with an automated cartilage-based Xpert machine (Cepheid, USA). The Xpert tool enables healthcare professionals to improve the speed and quality of TB diagnosis and helps diagnose TB in patients likely to be missed by traditional screening tests [5]. The fact that it allows diagnosis of TB simultaneously as pinpointing resistance to rifampicin treatment is vital in minimizing the transmission of drug-resistant TB in TB-endemic countries. The test function is based on a nucleic-acid amplification assay that detects M. tuberculosis and rifampicin resistance patterns from the sputum and other body fluids [6]. Therefore, this study aimed to appraise the wide range of molecular diagnostics for drug-resistant tuberculosis (DR-TB) endorsed by the World Health Organisation and assess Xpert's utility for the rapid molecular diagnosis of Tuberculosis in a high-burden setting, southern region in India.
2. Materials and Methods
2.1. Study Setting, Period, and Design
An institution-based retrospective study was conducted from January 2022 to December 2022 in the Intermediate Reference Laboratory, State TB Training Demonstration Centre, Government Hospital for Chest Diseases, Puducherry state, India. A total of 39,107 TB suspects were enrolled in this study from Puducherry (n= 9819) state and nine adjoining districts (Villupuram n-2912, Kallakuruchi n-3268, Cuddalore n-2442, Trichy n-7919, Perambalur n-2326, Thanjavur n-4019, Nagapattinam n-1048, Tanjavore n-2170, and Thiruvanamalai n-3184) of Tamil Nadu state. All TB patients and Rifampicin-resistant TB patients diagnosed by Xpert MTB/ were the study population for the First-Line and Second-Line Line probe assay (LPA) and culture and drug susceptibility testing (DST). Patients with incomplete data and undocumented methods of diagnosis were excluded from the study.
2.2. Sample processing for Light-emitting diode fluorescent microscopy
The concentrated samples were smeared on pre-labeled, clean, grease-free Microscopic slides and kept to air-dry completely for 15 - 30 minutes. Fixed the smear to the slide by passing it over the flame 3 to 5 times for 3 to 4 seconds each. Placed the slides on a staining rack with the smeared part uppermost, the slides not touching each other. Flooded the slides with freshly filtered auramine-phenol. Let stand for 20 minutes. Washed slides with running water, controlling the water flow to prevent washing away the smear. Decolorized the excess staining by covering it entirely with acid-alcohol for 2 minutes. Washed the slides with running water, as before, to wash away the acid alcohol. Counterstained the slides with 0.5% potassium permanganate for 30 seconds, Washed as before with water, and slope the slides to air dry. Stained smears were examined under LED-FM (Primo Star iLED, Carl Zeiss, Gottingen, Germany) with 400X magnification, and 40 fields were examined. LED-FM results were reported for the presence or absence of AFB using the International Union Against Tuberculosis and Lung Disease and World Health Organization scale, with a positive result corresponding to ≥ 1 AFB per 20x for screening and 40x for confirmation [7].
2.3. Expectorated Sputum Sample processing for Xpert MTB/RIF assay
Using a separate sterile plastic disposable pipette, added the Xpert sample reagent at a 2:1 (v/v) ratio to each specimen in a sputum container with a screw cap. The sputum cup was shaken vigorously 10-20 times using back-and-forth movements in a single shake and incubated the sample in the sputum cup for 15 minutes at room temperature. As described above, the sputum cup was shaken at least once during the incubation period. The sputum sample should be liquefied with no visible clumps of sputum after incubation. Using the sterile plastic transfer pipette provided in the Xpert/Rif kit, draw the liquefied sample into the transfer pipette until the meniscus of the pipette is above the minimum mark and transfer the homogenized, liquefied sample into the open port of the Xpert MTB/RIF cartridge. Finally, the cartridge was loaded into the Xpert instrument as per the manufacturer’s instructions [8].
2.4. Lymph nodes and other tissues sample processing for Xpert MTB/RIF assay
Lymph nodes and other tissue sample is cut into small pieces in a sterile mortar using a clean, sterile pair of forceps and dissection knives. Approximately 2ml of sterile phosphate buffer (PBS) was added to a mixer of dissected small pieces of tissue, and sterile PBS solution was ground with a mortar and pestle until a homogeneous suspension was obtained. Transfer Approximately 0.7 ml of homogenized tissue sample was transferred to a sterile conical, screw-capped tube using a transfer pipette. A double volume of Xpert MTB/RIF Sample Reagent (1.4 ml) was added to 0.7 ml of homogenized tissue using a transfer pipette and vigorously shaken using a vortex for at least 10 seconds. Incubate the suspension for 10 minutes at room temperature, and shake the specimen vigorously using a vortex for at least 10 seconds. Incubated the processed sample at room temperature for 5 minutes and transferred 2ml to the Xpert MTB/RIF cartridge using a fresh sterile transfer pipette. Finally, the cartridge was loaded into the Xpert instrument as per the manufacturer’s instructions [9].
2.5. Processing of Non-sterile Lymph nodes and other tissues for Xpert MTB/RIF assay
Lymph nodes and other tissue samples were cut into small pieces in a sterile mortar using a clean, sterile pair of forceps and a sterile, sharp dissection blade. Approximately 2ml of sterile phosphate buffer was added to ground dissected tissue/PBS-solution with a sterile mortar and pestle until a homogeneous suspension was obtained and transferred into a sterile and pre-labeled 50ml conical tube using a sterile transfer pipette. A sterile 4% NaOH was added equally and homogenized the suspension using a vortex mixer. Incubated for 15 minutes at room temperature and filled the tube within 2 cm of the top (e.g., to the 50-ml mark on the tube) with sterile PBS. Centrifuged the whole content at 3000g for 15 minutes and discarded the supernatant into a discard bin containing 5% phenol or other mycobacterial disinfectants. Added approximately 1-2 ml sterile PBS into deposited pellets using a sterile transfer pipette. About 0.7 ml of homogenized tissue sample was transferred to a sterile conical, screw-capped tube using a sterile transfer pipette, and added a double volume of Xpert MTB/RIF Sample Reagent (1.4 ml) to 0.7 ml of homogenized tissue using another sterile transfer pipette. Vigorously vortex for at least 10 seconds and Incubate for 10 minutes at room temperature, and again shake the homogenized specimen vigorously vortex for at least 10 seconds. Incubated the processed sample at room temperature for 5 minutes. Approximately 2ml of the processed sample was transferred to the Xpert MTB/RIF cartridge using a fresh transfer pipette and loaded the cartridge into the Xpert instrument as per the manufacturer’s instructions [9].
2.6. Sterile collection of Lymph nodes and other tissues for Xpert/MTB/RIF assay
The tissue sample was cut into small pieces in a sterile mortar using a clean, sterile pair of forceps and a dissection blade. Approximately 2ml of sterile phosphate buffer (PBS) was added to ground tissue/PBS solution with a mortar and pestle until a homogeneous suspension was obtained and adjusted to a final volume of approximately 2ml with sterile PBS. About 0.7 ml of homogeneous suspension was transferred to a sterile conical, screw-capped for the Xpert MTB/RIF using a transfer pipette and transferred a double volume of Xpert MTB/RIF Sample Reagent (1.4 ml) to 0.7 ml of homogenized tissue using a transfer pipette. Vigorously vortex for at least 10 seconds, incubate for 10 minutes at room temperature, and vortex for at least 10 seconds. Incubated the homogeneous suspension at room temperature for 5 minutes and transferred 2ml of the processed sample to the Xpert MTB/RIF cartridge using a fresh sterile transfer pipette. The cartridge containing homogeneous suspension was loaded into the Xpert instrument as per the manufacturer’s instructions [10].
2.7. Processing of CSF samples for Xpert MTB/RIF assay
If the CSF sample volume is less than 2 ml, add an equal volume of the Xpert MTB/RIF sample reagent to the CSF sample. Transferred about 2ml of the sample mixture directly to the Xpert MTB/RIF cartridge, and finally, the cartridge containing the CSF sample was loaded into the Xpert instrument as per the manufacturer’s instructions. If the sample volume exceeds 2 ml, transfer all sample content to a sterile conical centrifuge tube and centrifuge for 15 minutes at 4000 rpm. Carefully discard the supernatant into a discard bin containing 5% phenol or other mycobacterial disinfectants. A volume of 2ml of Xpert MTB/RIF sample reagent was added into the deposit using a fresh sterile transfer pipette, and transferred 2ml of the concentrated CSF sample to the Xpert MTB/RIF cartridge. The cartridge-filled CSF sample was loaded into the Xpert instrument as per the manufacturer’s instructions [10].
2.8. DNA Extraction using GenoLyse for MTBDRplus VER 2.0 assay
Approximately 1 ml of the liquid culture sample was transferred from each tube to a sterile 1.5 ml microcentrifuge tube with a screw cap using a disposable Pasteur pipette. The samples were centrifuged at 10,000 x g for 15 minutes in a centrifuge. After discarding the supernatant, the pellet was suspended in 100ul Lysis Buffer (A-LYS) and incubated at 95°C for 5 minutes. Approximately 100 µl of Neutralisation Buffer (A-NB) was added and vortexed the sample briefly for 5 seconds. The samples were centrifuged for 5 minutes at 10,000 x g and carefully transferred 40-80ul of supernatant to a separate clean, sterile microcentrifuge tube. The amplification mix (45 µl per PCR tube) was prepared in a room free from contaminating DNA. The amplification Mixer A and B (AM-A and AM-B) have all the reagents required for amplification. After thawing, mix AM-A and AM-B carefully. 5μl of DNA supernatant was added to corresponding PCR tubes except for contamination control, and 5 µl water was added to one aliquot for the contamination control. All the PCR tubes are placed in the PCR instruments, and run the programme as per the manufacturer’s instructions [11].
2.9. Hybridization for First-line drugs
Pre-warmed 20 µl of Denaturation Solution (DEN, blue) was dispensed in the corner of each of the wells used, and 20 µl of the amplified sample was added, pipetted up and down to mixed well and incubated at room temperature for 5 minutes, and carefully added to each well 1 ml of pre-warmed Hybridization Buffer (HYB, green). A strip was placed in each well of the GT Blot tray, and the strips must be covered entirely by the solution and ensure that the coated side faces upward. The tray was placed in the GT Blot instrument and incubated at 45°C for 30 minutes, and the shaking frequency of the GT Blot was to achieve a constant and thorough mixing of the solution.Aspitared the Hybridization Buffer using a sterile Pasteur pipette. 1 ml of Stringent Wash Solution (STR, red) was added to each strip, incubated at 45°C for 15 minutes in the GT Blot instrument, and completely removed the Stringent Wash Solution using a separate Pasteur pipette. Washed each strip once with 1 ml of Rinse Solution (RIN) for 1 minute in the GT Blot instrument. Added 1 ml of diluted Conjugate to each strip and incubated for 30 minutes in the GT Blot instrument. Removed solution using a sterile Pasteur pipette and washed each strip twice for 1 minute with 1 ml of Rinse Solution (RIN) and once for 1 minute with approximately 1 ml of distilled water. 1 ml of diluted substrate solution was added to each strip, incubated for 3-20 minutes, and protected from direct light without shaking. The reaction was stopped as soon as bands were visible by briefly rinsing twice with distilled water. The strips were removed from the tray using tweezers and pasted on an evaluation sheet provided in the kit [12].
2.10. DNA Extraction using GenoLyse for MTBDRsl VER 2.0 assay
Approximately 1 ml of culture suspension was transferred into a sterile 1.5 ml screw cap microcentrifuge tube using a disposable Pasteur pipette. The culture suspension was centrifuged at 10,000 x g for 15 minutes in a centrifuge. After discarding the supernatant, the pellet was suspended in 100ul Lysis Buffer (A-LYS) and incubated at 95°C for 5 minutes. Approximately 100 µl of Neutralisation Buffer (A-NB) was added and vortexed the sample briefly for 5 seconds. The liquid suspension was centrifuged at 10,000 x g for 5 minutes and carefully transferred 40-80ul of supernatant to a clean, sterile microcentrifuge tube. The amplification mix (45 µl per PCR tube) was prepared in a room free from contaminating DNA. The amplification Mixer A and B (AM-A and AM-B) have all the reagents required for amplification. After thawing, mix AM-A and AM-B carefully. 5μl of DNA supernatant was added to corresponding PCR tubes except for contamination control, and 5 µl water was added to one aliquot for the contamination control. All the PCR tubes are placed in the PCR instruments, and run the programme as per the manufacturer’s instructions [11].
2.11. Hybridization for second line drugs
Approximately 20μl of Denaturation Solution was Dispensed (DEN, blue) in the corner of each of the wells in the GT Blot tray, and 20μl of amplified PCR product was added into each well using a sterile pipette and incubated at room temperature for 5 minutes. Carefully add 1 ml of pre-warmed Hybridization Buffer (HYB, green) to each well and gently shake the tray until the solution is homogenous. Placed a pre-labeled strip into each well using sterile tweezers. Transferred the tray to the GT-Blot instrument and incubated for 30 minutes at 45°C. Completely aspirated Hybridization Buffer using a sterile Pasteur pipette. 1 ml of Stringent Wash Solution (STR, red) was added to each strip, incubated at 45°C for 15 minutes in the GT Blot instrument, and completely removed the Stringent Wash Solution using a separate Pasteur pipette. The strip was washed with 1 ml Rinse Solution (RIN) for 1 minute in the GT Blot instrument, and 1 ml diluted Conjugate was added to each strip and incubated for 30 minutes in the GT Blot instrument. Removed solution using a sterile Pasteur pipette and washed each strip twice for 1 minute with 1 ml of Rinse Solution (RIN) and once for 1 minute with approximately 1 ml of distilled water. 1 ml of diluted substrate solution was added to each strip, incubated for 3-20 minutes, and protected from direct light without shaking. The reaction was stopped as soon as bands were visible by briefly rinsing twice with distilled water. The strips were removed from the tray using tweezers and pasted on an evaluation sheet provided in the kit [13].
3. Results
Overall, a total of 39,107 samples of Tuberculosis suspects were processed for upfront Xpert MTB/RIF testing between January 2022 and December 2022. Of 29,114(74.45%) pulmonary samples tested, 21.42 %( n=6,236) were positive for tuberculosis and 7.68 %( n=479) were rifampicin drug resistant (Figure 1). Among 8,581(21.95%) extra-pulmonary samples processed for tuberculosis diagnosis using upfront Xpert MTB/RIF assay, 10.72 %( n=920) and 3.26 % (n=30) were resistant to the rifampicin drug. Thirty-four thousand eight hundred fourteen samples (92.36%) were referred from public sector facilities, and only 7.64% (n=2881) were referred from the private sector (Figure 2). Among 37,695 Tuberculosis suspect samples tested, 18.98% (n = 7156) were positive for M.tuberculosis, and 7.11 % (n = 509) were resistant to rifampicin drug using the Xpert MTB/RIF test. A total of 1,412 (3.6%) Xpert MTB/RIF cartridges were wasted in this complete study. A total of 32,825 patients with presumptive TB were enrolled for the study, out of which 15.01 %( n = 4927) were positive for M.tuberculosis, and 4.22% (n = 208) were rifampicin drug resistant. Among 4870 Presumptive DR-TB (Pulmonary) patients, 45.77 %( n = 2229) were positive for M.tuberculosis, and 13.50% (n = 301) were rifampicin drug-resistant (Table 1).
Of 2,374 samples received from PL-HIV patients, 7.54% (n = 179) were positive for M.tuberculosis, and 5.59% (n = 10) were rifampicin-resistant. Among 2,257 paediatric samples processed for diagnosis of TB, 2.22% (n = 50) were positive for M.tuberculosis. 20.53% (n = 2,306) were positive for M.tuberculosis among all smear-negative presumptive TB cases, either from previously treated patients or new suspects, and MDR suspect (n=11, 233) samples processed for diagnosis of tuberculosis and 4.90% (n =113) were resistant for rifampicin drug using Xpert MTB/RIF test. A total of 1,820 samples were received from other vulnerable () for diagnosis of tuberculosis using Xpert MTB/RIF assay, out of which 14.45% (n = 263) were positive for M.tuberculosis and 3.80% (n =10) were rifampicin drug resistant. Out of 595 Contacts of TB & DR-TB patient samples tested, 16.97 %( n=101) were positive for M.tuberculosis, and 23.76 %( n=24) were rifampicin drug-resistant. Among 7,639 EPTB (extra-pulmonary tuberculosis) samples tested, 9.78 %( n =747) were M.tuberculosis, positive, and 3.48 %( n=26) were rifampicin resistant. Of 4,026 samples offered for the upfront molecular test, 14.88% (n=599) were M.tuberculosis positive, and about 1% were rifampicin-resistant (Table 1). Out of the total 3,846 presumptive adults (new) notified TB patients who have provided sputum samples for M.tuberculosis diagnosis,40.90%(n=1,573) were M.tuberculosis positive, and 17.04%(n=268) were rifampicin resistant. Of 462 notified pre-treated TB patient samples tested for M.tuberculosis diagnosis, 4048 % (n=187) were positive for M.tuberculosis, and 10.16 %( n=19) were rifampicin drug resistant. Among 562 non-responders (Drug sensitive tuberculosis-DSTB and isoniazid mono-resistant tuberculosis-HrTB) tested for M.tuberculosis diagnosis, 83.45% (n=469) were M.tuberculosis positive and 2.99% were rifampicin resistant. Xpert sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated using the concentrated smear microscopy (Fluorescence) method.
The sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for PTB were found to be 99.87 % (CI: 0.12-0.07), 99.92%(CI: 0.04-0.03), 99.71%(CI: 0.17-0.11), 99.97%(CI: 0.04-0.01), 21.38%(CI: 0.46-0.48) and 99.91%(0.04-0.03) respectively. For EPTB, the sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay counted for 99.45 % ( CI: 0.72- 0.37), 99.84% (CI: 0.11-0.08) 98.70% (CI: 0.97-0.55) 99.93% (CI: 0.09-0.04) 10.64% (CI: 0.65-0.67) and 99.80% (CI: 0.12-0.08), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Presumptive TB were found to be 99.82%(CI: 0.17-0.10), 99.91%(CI: 0.04-0.03), 99.51% (CI: 0.23-0.16), 99.97% (CI: 0.03-0.01), 14.96% (CI: 0.38-0.39) and 9.93% (CI: 0.04-0.02), respectively (Table 2). For Presumptive DRTB (Pulmonary), the sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay counted for 99.82% (CI: 0.28-0.13), 99.77% (CI: 0.26-0.15), 99.73% (CI: 0.33-0.15), 99.85% (CI: 0.25-0.09), 45.73% (CI: 1.41-2.41) and 99.92% (CI: 0.10-0.05), respectively.
Among 32,825 presumptive TB enrolled for this study, the sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for PL-HIV out of presumptive TB (n=2374) were 99.44% (CI: 2.53-0.55), 99.91% (CI: 0.24-0.08), 98.88% (CI: 3.20-0.84), 99.95% (CI: 0.27-0.04), 7.50% (CI: 1.03-1.13) and 99.87% (CI: 0.24-0.10), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for Paediatric out of presumptive TB (n=2257) were found to be 97.96% (CI: 8.81-1.99), 99.91% (CI: 0.24-0.08), 96.00% (CI: 10.28-2.27), 99.95% (CI: 0.26-0.04), 2.17% (CI: 0.56-0.69) and 99.87% (CI: 0.26-0.10), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Smear Negative, X-ray suggestive TB (n=11233) were found to be 100% (CI: 0.16-0.0), 99.99% (CI: 0.05-0.01), 99.96% (CI: 0.27-0.03) 100% (CI: 0.04-0.00), 20.52% (CI: 0.74-0.76) and 99.99 % (CI: 0.04-0.01), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for Other Vulnerable group TB (n=1820) were found to be 99.62% (CI: 1.73-0.37), 99.87% (CI: 0.33-0.11), 99.24% (CI: 2.21-0.57), 99.94% (CI: 0.39-0.05), 14.40% (CI: 1.59-1.69) and 99.84% (CI: 0.32-0.13), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Contacts of TB & DRTB patients (n=595) were found to be 100% (CI: 3.69-0.00), 99.40% (CI: 1.15-0.48), 97.03% (CI: 5.67-1.99), 100% (CI: 0.74-0.00), 16.47% (CI: 2.89-3.23) and 99.50% (CI: 0.97-0.40), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for extra-pulmonary TB (n=7639) were found to be 99.60% (CI: 0.78-0.32), 99.90% (CI: 0.11-0.06), 99.06% (CI: 1.00-0.39), 99.96% (CI: 0.09-0.03), 9.73% (CI: 0.66-0.68), and 99.87% (CI: 0.11-0.07), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Upfront Molecular test offered(n=4026) were found to be 99.83% (CI: 0.76-0.17), 99.97% (CI: 0.13-0.03), 99.83% (CI: 1.00-0.15), 99.97% (CI: 0.18-0.03), 14.88% (CI: 1.09-1.54) and 99.95% (CI: 0.13-0.04), respectively.
Among 4,870 the Presumptive DR-TB (Pulmonary) enrolled for this study, the sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Notified TB patients (New)- UDST (n=3846)were 99.94% (CI: 0.34-0.06), 99.87% (CI: 0.25-0.10), 99.81% (CI: 0.40-0.13), 99.96% (CI: 0.27-0.03), 40.85% (CI: 1.56-1.57) and, 99.90% (CI: 0.17-0.07), respectively. The sensitivity, specificity, PPV, NPV, Diseases prevalence and accuracy of Xpert MTB/RIF assay for Notified TB patients (Previously treated) -UDST (n=462)were found to be 99.47% (CI: 2.41-0.52), 99.64% (CI: 1.65-0.35), 99.47% (CI: 3.13-0.45), 99.64% (CI: 2.15-0.31), 40.48% (CI: 4.51-4.63)and 99.57% (CI: 1.12-0.38), respectively (Table 2). The sensitivity, specificity, PPV, NPV, Diseases prevalence, and accuracy of Xpert MTB/RIF assay for Non-responders (n=562) were found to be 99.57% (CI: 1.10-0.38), 97.85% (CI: 5.40-1.89), 99.57% (CI: 1.23-0.32), 97.85% (CI: 5.91-1.60), 83.45% (CI: 3.33-2.98) and, 99.29% (CI: 1.10-0.62), respectively.
The Xpert assay test provides semi-quantitative M. tuberculosis detection based on the probe’s Cycle Threshold (Ct)-the number of PCR cycles required for amplifying MTB DNA to detectable levels. Xpert assay cycle threshold values (CT) is a semi-quantitative measure of bacillary burden in the specimen. Out of 509 RR-TB detected results, 36(7.07%) are reported as “High” (Ct<16), 98(19.25%), 163(32.02%), 212(41.65%) are reported as “Medium” (Ct16-22),” Low” (Ct 22-28) and “Very Low” (Ct >28) respectively (Figure 3). Delta Ct (ΔCt) max was calculated as the difference between the earliest and latest Ct across the five molecular beacon (A-E) probes (Table 3). Out of 509 rifampicin-resistant, 243(47.74%) were reported as “dropout” (no hybridization), and 266(52.25%) cases were reported as “delayed” (ΔCt >4), as represented in Table 3. The most common probes for RIF resistance detection were E (n=68, 13.36%), D (n=57, 11.20%), and B (n=55, 10.81%). The probe with the most delayed binding Ct value was categorized as ΔCt 4.1-4.9(49, 20.16%) and ΔCt >5(194, 79.84%).
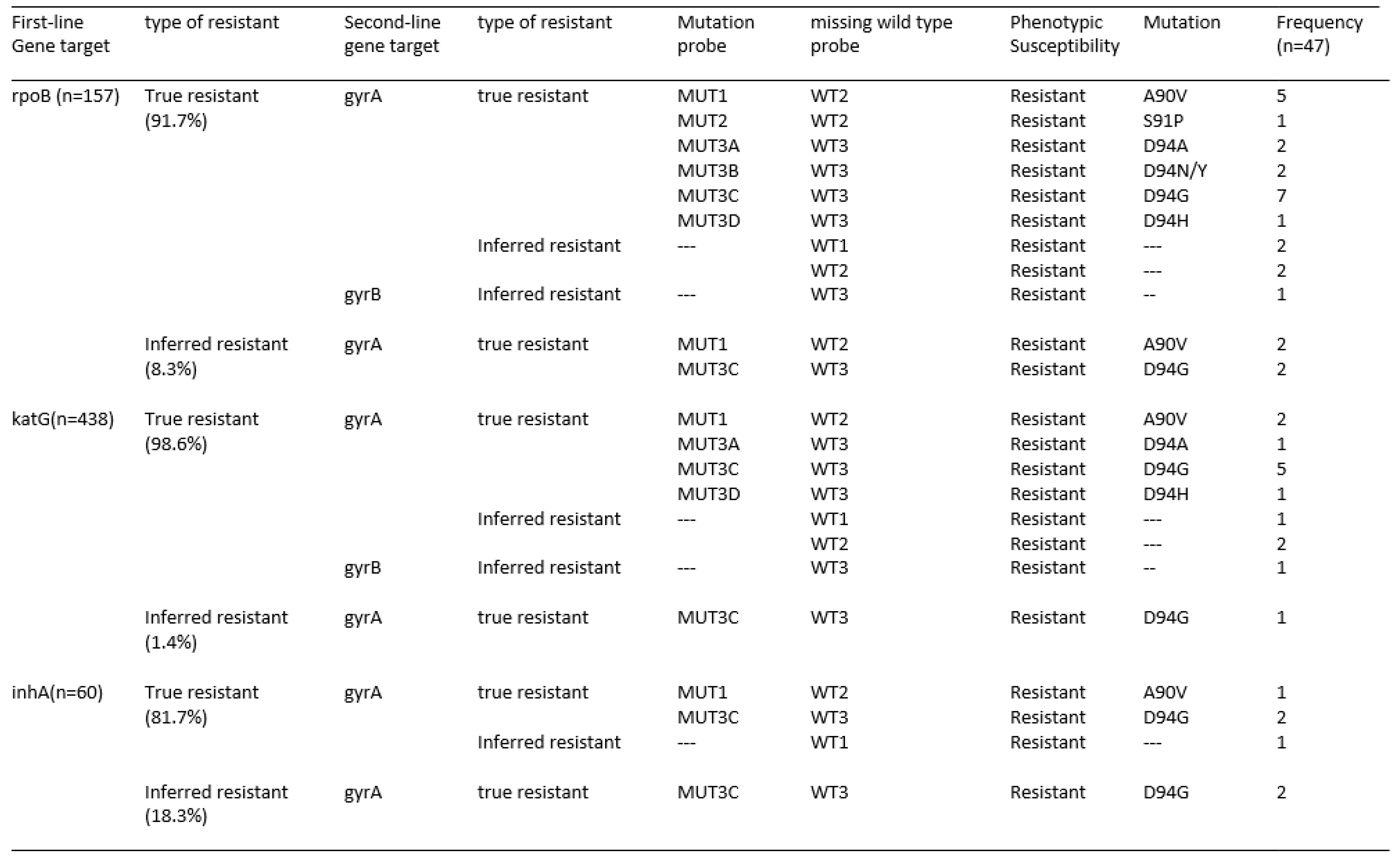
Among 7,156 (18.33%) M.tuberculosis positive cases, 7.11 % (n=509) were rifampicin-resistant, and 92.89 % (n=6647) were rifampicin-sensitive tuberculosis (Table 1). Of 157(30.84%) RR tested for MDBDRsl assay, 16.56 % (n=26) were pre-XDR, and 0.64 % (n=1) were XDR tuberculosis. 69.16 % (n=352) were not tested for MDBDRsl assay due to the non-availability of samples. Of 6,647(92.89%) RS-TB cases, 92.1% (n=6,122) were tested for the MDBDRplus assay, and 525(7.9%) were not tested for the MDBDRplus assay due to non-availability of samples. Among 6,122 RS TB were tested for MDBDRplus assay, 8.13% (n=498) were HR-TB and 91.87% (n=5624) were HS tuberculosis. Of 498(8.13%) HR tested for MDBDRsl assay, 4.02% (n=20) were pre-XDR tuberculosis (Figure 1). Of 47 fluoroquinolone-resistant, 16.56% (26/157) of Multidrug-resistant tuberculosis isolates and 4.02% (20/498) isoniazid-resistant are fluoroquinolone-resistant, a characteristic distribution leading to about 17.2% of fluoroquinolone resistance events and relevant marker gyr-A mutations in MDR tuberculosis isolates (Table 4).
4. Discussion
Tuberculosis is the most dreadful infectious disease in the world, with high morbidity and mortality among people. Thus, early detection is of utmost importance for reducing deaths and transmission. The lack of rapid and accurate diagnostic tests hampers global TB control. Xpert MTB/RIF assay (Cepheid Inc., Sunnyvale, CA, USA) is the semi-quantitative real-time polymerase chain reaction (PCR) to rapidly detect the M.tuberculosis complex and rifampicin resistance by amplifying a DNA fragment containing the 81bp hotspot region of the rpoB gene (codons 507–533) that is then hybridized to five molecular beacon probes.
Overall, this study's MTB and Rifampicin Resistant TB frequency was 18.33% and 7.11%, respectively. The incidence rate of M. tuberculosis (18.33%) in this study was higher than the previous study reported 6.5% [14] and 7.9% [15] in Ethiopia, 13.8% [16] in Nepal, and 12% [17] in India. The incidence rate of M. tuberculosis infection among total suspects (n=39107) tested for Xpert MTB/RIF was 18.33% (7156/39107), which is lower than the previous study reported 38.77% [18] in China, 22.65 % [19], 22.9%[20] in Nigeria and 23.82% [21] in India. The 3.26% positivity among the 8581 Extra-pulmonary samples tested for tuberculosis using Xpert MTB/RIF assay in this study is lower than the previous study (13%) conducted by Anwar et.al. [22].
Elbrolosy et al. [23] reported in their study that the sensitivity specificity of Xpert MTB/RIF assay for PTB was found to be 90.2 % and 86.9 %, respectively, while for EPTB, the sensitivity specificity of Xpert MTB/RIF assay counted for 81.6 % and 78.9 %, respectively. Mulengwa et al. [24]reported sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the Xpert MTB/RIF test was 91.6%, 95.3%,83%, and 97.80%, respectively. But in this study, the sensitivity, specificity, PPV, NPV, Disease prevalence, and accuracy of Xpert MTB/RIF assay for PTB were found to be 99.87 %,99.92%, 99.71%, 99.97%, 21.38%, and 99.91% respectively and for EPTB, the sensitivity, specificity, PPV, NPV, Disease prevalence, and accuracy of Xpert MTB/RIF assay counted for 99.45 %, 99.84%, 98.70%, 99.93%, 10.64%, and 99.80%, respectively compared to concentrated smear (Fluorescence Microscopy) method. Raina et al. [25]reported that the sensitivity, specificity, PPV, and NPV of Xpert MTB/RIF were 100%, 99.5%, 97.5%, and 100%, respectively, compared to the gold standard culture method.
Of 2,374 PLHIV samples enrolled for this study, the sensitivity, specificity, PPV, NPV, Disease prevalence, and accuracy of Xpert MTB/RIF assay for PLHIV out of presumptive TB were 99.44%, 99.91%, 98.88%, 99.95%, 7.50%, and 99.87%, respectively. In countries with low endemicity rates, the sensitivity and the specificity of Xpert MTB/RIF vary between 82, 95, and 98% for sensitivity and 96 and 99% for specificity. However, in countries with high endemicity, these rates vary between 80 and 88% for sensitivity and between 95 and 98% for specificity [26,27,28].In another study, Faria et al. [29] reported Xpert MTB/RIF assay’s sensitivity ranging from 68% to 100%. Specificity ranged from 91.7% to 100%, the positive predictive value from 79.2% to 96.1%, and the negative predictive value from 84.6% to 99.3%.
In their study, Cox et al. [30] reported 76% sensitivity and 98% specificity for 5,717 smear-negative samples processed for Xpert MTB/RIF. In our study, the sensitivity of Xpert MTB/RIF was also high 100% among smear-negative, and specificity was 99.99% with 99.99% accuracy. Rimal et al. [31] reported the sensitivity, specificity, positive predictive value, and negative predictive values of Xpert MTB/RIF assay for smear-negative sputum samples were 74.3%, 96.6%, 86.7%, and 92%, respectively. In this study, 11,223 sputum samples were collected and processed by microscopy followed by Xpert MTB/RIF assay. The sensitivity, specificity, PPV, NPV, Disease prevalence, and accuracy of Xpert MTB/RIF assay for Smear Negative, X-ray suggestive TB (n=11,233) were found to be 100%, 99.99%, 99.96%,100%, 20.52%, and 99.99 %, respectively.
Hebte et al. [32] reported 89.1% (n=106) positivity and 4.2% (n=5) rifampicin-resistant TB out of 119 index TB cases enrolled for Xpert assay. The positivity rate among the 494 contacts of TB and drug-resistant tuberculosis patients registered for this study was 16.97%. Its sensitivity, specificity, positive predictive value, negative predictive value, Disease prevalence, and Xpert MTB/RIF assay accuracy were 100%, 99.40%, 97.03%, 100.00%, 16.47%, and 99.50, respectively. Our study reported lower positivity than that reported by Hebte et al. and higher than that reported by Gebretsadik et al.[33]. He said 8.98% (n=38) positivity and 5.3% (n=3) rifampicin-resistant TB out of 423 index TB cases enrolled for Xpert assay. In their recent study, Gurung et al. [34] reported 4.5 % (n=770) positivity out of 17114 index TB cases registered for Xpert assay. Kalra et al. [35] reported 6.6% positivity (n=6270) and 8.7% (n=545) rifampicin-resistant, of the total 94,415 presumptive pediatric TB cases diagnosed on Xpert MTB/RIF assay. However, the positivity rate among the 2257 pediatric cases enrolled for this study was 2.22%. Its sensitivity, specificity, positive predictive value, negative predictive value, Disease prevalence, and Xpert MTB/RIF assay accuracy were 97.96%, 99.91%, 96.00%, 99.95%, 2.17%, and 99.87%, respectively.
In a previous study, Ibrahim et al. [19] reported the incidence of M.tuberculosis and rifampicin resistance was 22.68% and 4.50%, respectively, out of 2451 samples tested on Xpert assay. Of total 990 presumptive tuberculosis tested [16], the estimated prevalence of M.tuberculosis in presumptive TB patients was 13.8% (95%CI: 11.88%–16.16%), and the estimated prevalence of rifampicin resistant in M.tuberculosis confirmed patients was 10.2% (4.97%–15.1%). Of 132 notified new TB cases enrolled in a previous study [36], the positivity on Xpert MTB/RIF assay was 78.79%. The sensitivity, specificity, PPV, and NPV of GXP in diagnosing and detecting rifampicin resistance in pulmonary TB were 95%, 93%, 98%, 84% and 96%, 100%, 100%, and 96% respectively. The positivity rate among the 3846 notified new TB cases enrolled for this study was 40.90%. Its sensitivity, specificity, positive predictive value, negative predictive value, Disease prevalence, and accuracy of Xpert MTB/RIF assay were 99.94%, 99.87%, 99.81%, 99.96%, 40.85%, and 99.90%, respectively. Our study reported a higher (40.90%) incidence of M.tuberculosis and rifampicin-resistant (17.04%) rate than the previous studies mentioned here.
In a recent study, Worku et al.[37] reported an 11.9% incidence of M.tuberculosis positivity rate and 2.5% rifampicin resistance out of 1828 smear-negative and re-treatment cases tested on Xpert MTB/RIF assay. Of 462 notified previously treated patients enrolled for this study, the TB positivity rate was 40.98%. Its sensitivity, specificity, positive predictive value, and negative predictive value, Disease prevalence, and accuracy of Xpert MTB/RIF assay were 99.47%, 99.64%, 99.47%, 99.64%, 40.48%, and 99.57%, respectively. Farra et al. [38,39] reported 79.1% (488/617) M.tuberculosis positivity rate and 42.2% rifampicin resistant in confirmed M.tuberculosis (206/488) in their study out of 617 samples (55.8% relapse; 31.6% failure and 10.2% defaulter) tested using Xpert MTB/RIF assay. Of 562 non-responders (DS TB and INH resistant TB) patients enrolled for this study, the tuberculosis positivity and rifampicin resistance detection rate was 83.45% and 2.99%, respectively and its sensitivity, specificity, positive predictive value, and negative predictive value, Diseases prevalence and accuracy of Xpert MTB/RIF assay was 99.57%, 97.85%, 99.57%, 97.85%, 83.45%, and 99.29%, respectively.
In this study, 16.56% (26/157) of Multidrug-resistant tuberculosis isolates and 4.02% (20/498) isoniazid-resistant are fluoroquinolone-resistant, a characteristic distribution leading to about 17.2% of fluoroquinolone resistance events and relevant marker gyr-A mutations in MDR tuberculosis isolates. Dreyer et al. [40] reported 69.2% (703/1016) fluoroquinolone resistance among 1016 Multidrug-resistant tuberculosis isolates tested for resistance. In India, 36% of the Multidrug-resistant tuberculosis isolates are browned to have additional resistance to fluoroquinolone [41,42], and about 3% of MDR-TB isolates are estimated to have extensively drug-resistant (XDR-TB). Sharma et al. [43] reported 3.2% (35/1099) fluoroquinolone resistance among first-line drug-sensitive tuberculosis cases. Furthermore, the increase of fluoroquinolone resistance among isoniazid-resistant tuberculosis suggests that the active adoption of antibiotic stewardship in the community is urgently required.
About 3.6% (n=1412) of samples were not processed due to challenges in getting resamples. Of 1412 samples, 65,301,138,908 were rifampicin indeterminate, invalid, no result, and errors, respectively. The acceptable rate of rifampicin indeterminate, invalid, no result, and error calculations need to be defined. This study reported that 69.16% (352/509) of rifampicin-resistant patient’s samples were not processed to know further the drug susceptibility pattern of fluoroquinolones and second-line tuberculosis drugs. The control of tuberculosis, once unchecked, is extremely difficult to contain and manage, requiring a multidisciplinary, coordinated set of activities. The cornerstones of classic tuberculosis control approaches include:
- Early diagnosis.
- Novel case-finding methods beyond healthcare facilities.
- Shorter and simpler successful treatment regimens for drug-sensitive and drug-resistant tuberculosis.
- A greater focus on prevention strategies.
- Steps to reduce mortality and transmission in adults and children.
The status quo for many rifampicin-resistant patients is a severe systemic illness characterized by significant lung damage and high mycobacterial burden. Early identification and screening of rifampicin resistance may facilitate better treatment outcomes and less transmission. Similarly, earlier diagnosis would reduce cumulative immunopathological and structural lung damage (morbidity) and potentially reduce mortality. The molecular characteristics of the disease burden and resistant pattern using Xpert MTB/RIF assay, together with Geographic Information System (GIS) mapping of the location where the specimen was received and tested, could be used as a crude epidemiological tool to identify hot spots of tuberculosis transmission and changes in patterns of circulating rifampicin resistance strains.
5. Conclusions
Our study unveiled a high positivity rate of M. tuberculosis in presumptive TB and presumptive drug-resistant tuberculosis patients. Our analysis also demonstrated a high Rifampicin-resistant (RR-TB) tuberculosis rate among M. tuberculosis confirmed patients. The performance of Xpert MTB/RIF detected in M.tuberculosis and rifampicin resistant is in agreement with other researchers who established the diagnosis in a significant proportion of cases. A high rate was observed in both previously treated and treatment-naive patients. In conclusion, Xpert can be a valuable diagnostic tool in patients of suspected Pulmonary Tuberculosis, either AFB smear-negative or positive, due to its rapidity and synchronized detection of Rifampicin resistance, especially advantageous in a patient with MDR and HIV-associated tuberculosis. This study confirms that the Xpert remains the rapid diagnostic tool for diagnosing TB and confirming sensitivity/resistance to RIF in pulmonary and extra-pulmonary samples. The high sensitivity and specificity of Xpert MTB/RIF allows ruling out the disease with a high degree of confidence. Molecular epidemiological studies to understand the genetic diversity of M. tuberculosis and link the index cases with the secondary infection among close contacts would be valuable. Our study indicated that increased fluoroquinolone resistance among Rifampicin-resistant and isoniazid-resistant tuberculosis endangers the success of newly endorsed MDR-TB regimens. Furthermore, the presence of fluoroquinolone resistance among isoniazid resistant tuberculosis suggests that the active adoption of antibiotic stewardship in the community is urgently required.
Author Contributions
Formal Analysis and supervision- Muthuraj Muthaiah, Govindarajan Soundappan and Asha Frederick. Investigation, writing and data curation-Venkateswari, Ramachandra, Aaina Muralidhar, Anbazhagi Muthukumar, Revathi Mani. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable
Conflicts of Interest
The authors declare no conflict of interest
References
- Global tuberculosis report 2022. Geneva: World Health Organization; 2022 (https://www.who.int/publications/i/item/9789240037021).
- Dean, A.S.; et al. 25 years of surveillance of drug-resistant tuberculosis: achievements, challenges, and way forward. Lancet Infect Dis .2022, 22(7), e191-E196. [CrossRef]
- Global tuberculosis report 2020. Geneva: World Health Organization; 2020 (https://www.who.int/publications/i/item/9789240037021).
- Nandlal, L.; Perumal, R.; Naidoo, K. Rapid Molecular Assays for the Diagnosis of Drug-Resistant Tuberculosis. Infect Drug Resist. 2022, 15, 4971-4984. [CrossRef]
- Tamirat, K.S.; Kebede, F.B.;Baraki, A.G.; Akalu, T.Y. The Role of GeneXpert MTB/RIF in Reducing Treatment Delay Among Multidrug Resistance Tuberculosis Patients: A Propensity Score Matched Analysis. Infect Drug Resist. 2022, 15,285-294. [CrossRef]
- Pongpeeradech,N.;Kasetchareo,Y.; Chuchottaworn,C.; Lawpoolsri,S.; Silachamroon, U.; Kaewkungwal, J. (2022) Evaluation of the use of GeneXpert MTB/RIF in a zone with high burden of tuberculosis in Thailand. PLoS ONE.2022, 17(7), e0271130. [CrossRef]
- International Union against Tuberculosis and Lung Disease. The Public Health Service National Tuberculosis Reference Laboratory and the National Laboratory Network. Paris: International Union Against Tuberculosis and Lung Disease; 1998.
- Kabir, S.; Parash, M.T.H.; Emran, N.A.; Hossain, A.B.M.T.; Shimmi, S.C. Diagnostic challenges and Gene-Xpert utility in detecting Mycobacterium tuberculosis among suspected cases of Pulmonary tuberculosis. PLoS ONE.2021, 16(5): e0251858. [CrossRef]
- Mukhida, S.; Vyawahare, C.R.; Mirza, S.B.; Gandham, N.R; Khan, S.; Kannuri, S.; Role of GeneXpert MTB/RIF assay for the diagnosis of cervical lymph node tuberculosis and rifampicin resistance. Tzu Chi Med J. 2022, 34(4),418-422. [CrossRef]
- Xpert MTB/RIF system for the diagnosis of pulmonary and extra-pulmonary TB and rifampicin resistance in adults and children. A pre-publication version of the policy guidance may be accessed at: http://www.stoptb.org/wg/gli/assets/documents/WHO Policy Statement on Xpert MTB-RIF 2013 pre-publication 22102013.pdf.
- Smita, S.S.; Venkatesh, K.; Usharani, B.; Anbazhagi, S.; Vidya Raj,C.K.; Chitra,A.; Muthuraj, M. Prevalence and factors associated with multidrug-resistant tuberculosis in South India.Sci Rep.2020, 10,17552. [CrossRef]
- C.K. Vidyaraj,C.K.; Chitra,A.; Smita,S.; Muthuraj,M.; Govindarajan,S.; Usharani,B.; Anbazhagi,A. Prevalence of rifampicin-resistant Mycobacterium tuberculosis among human-immunodeficiency-virus-seropositive patients and their treatment outcomes. J Epidemiol Glob Health.2017,7(4), 289 - 294. [CrossRef]
- Aaina, M.; Venkatesh, K.; Usharani, B.; Anbazhagi, M.; Rakesh, G.; Muthuraj, M. Risk Factors and Treatment Outcome Analysis Associated with Second-Line Drug-Resistant Tuberculosis. J Respir. 2022, 2, 1–12. [CrossRef]
- Sinshaw, W.; Kebede ,A.; Bitew, A.; Tesfaye, E.; Tadesse, M.; Mehamed, Z. Prevalence of tuberculosis, multidrug resistant tuberculosis and associated risk factors among smear negative presumptive pulmonary tuberculosis patients in Addis. BMC Infect Dis. BMC Infect Dis. 2019, 19, 1-15. [CrossRef]
- Wasihun, A.G.; Dejene, T.A.; Hailu, G.G. Frequency of MTB and rifampicin resistance MTB using Xpert-MTB/RIF assay among adult presumptive tuberculosis patients in Tigray, Northern Ethiopia: A cross sectional study. PLoS ONE.2020, 15(11), e0240361. [CrossRef]
- Shiv, K.S.; Pramod, R.B.; Anjana, S.; Deepak, D.; Deepa, G.; Renu, S.; Rifampicin-resistant Mycobacterium tuberculosis by GeneXpert MTB/RIF and Associated Factors among Presumptive Pulmonary Tuberculosis Patients in Nepal. Infect Drug Resist. 2020,13, 2011-2019. [CrossRef]
- William,A.; Yogita Rai,Y.; Ravinder Kaur,R. Evaluation of Rifampicin-resistant Tuberculosis in Pediatric Patients by GeneXpert MTB/RIF. J Microbiol Infect Dis. 2021, 11 (2), 81-87. [CrossRef]
- Zhua,W.; Wanga,Y.; Lic,T.; Chenc,W.; Wang,W. Gap to End-TB targets in eastern China: A joinpoint analysis from population-based notification data in Zhejiang Province, China, 2005–2018. Int J Infect Dis.2021, 104, 407-414. [CrossRef]
- Ibrahim, M.M.; Tom, M.I.; Umoru, M.A.; Jidda, B.U.; Mustafa A. I.; Adam, M.; Akbar, S.Trends in the incidence of Rifampicin resistant Mycobacterium tuberculosis infection in northeastern Nigeria. Sci Afr, 2022, 17, e01341. [CrossRef]
- Peter, O.; Ikuabe. I.D.E. Assay in patients with pulmonary tuberculosis in Yenagoa, Nigeria. Pan Afr Med J. 2018, 29, 1-4.
- Nemagouda, S.K. A three-year experience with genexpert MTB/RIF assay in tuberculosis control programme (RNTCP)- a clinical study. J Evolution Med Dent Sci. 2019,8(41),3080-3083. [CrossRef]
- Anwar, S.K.; Sajid Ali , Muhammad Tahir Khan , Sajjad Ahmed , Yasir Khattak, Abduljabbar , Muhammad Irfan , Wasim Sajjad 2018. Comparison of GeneXpert MTB/RIF assay and LED-FM microscopy for the diagnosis of extra pulmonary tuberculosis in Khyber Pakhtunkhwa, Pakistan. Braz J microbiol. 2018, 4(9), 909–913. [CrossRef]
- Elbrolosy, A.M.; Helbawy,R.H.E.; Mansour,O.M.; Latif,R.A. Diagnostic utility of GeneXpert MTB/RIF assay versus conventional methods for diagnosis of pulmonary and extrapulmonary tuberculosis. BMC Microbiol.2021, 21,144. [CrossRef]
- Mulengwa,D.L.; Maropeng Charles Monyama,M.C.; Lebelo,S.L. Evaluation of the GeneXpert MTB/RIF assay performance in sputum samples with various characteristics from presumed pulmonary tuberculosis patients in Shiselweni region, Eswatini. Infect Dis.2022, 54:3, 170-177. [CrossRef]
- Raina, C.; Sabita, B.; Alina,S.; Manoj, P.; Brajendra, S.; Yengkokpam, S.; Ranjit, S.; Zareena, F.; Rachana, M.; Ali, A.R.; Alfonso, J.; Rodriguez,M.; Kuldeep, D. Diagnostic performance of GeneXpert MTB/RIF assay compared to conventional Mycobacterium tuberculosis culture for diagnosis of pulmonary and extra pulmonary tuberculosis, Nepal. Narra J. 2021, 1(2): e33. [CrossRef]
- Li, S.; Liu, B.; Peng, M.; Chen, M.; Yin, W.; Tang, H. Diagnostic accuracy of Xpert MTB/RIF for tuberculosis detection in different regions with different endemic burden: a systematic review and meta-analysis. PLoS One. 2017,12. [CrossRef]
- Opota, O.; Zakham, F.; Mazza-Stalder, J.; Nicod, L.; Greub, G.; Jaton, K. Added Value of Xpert MTB/RIF Ultra for Diagnosis of Pulmonary Tuberculosis in a Low-Prevalence Setting. J Clin Microbiol. 2019, 57, e01717-18. [CrossRef]
- Tang, T.; Liu, F.; Lu, X.; Huang, Q. Evaluation of GeneXpert MTB/RIF for detecting mycobacterium tuberculosis in a hospital in China. J Int Med Res. 2017, 45,816-822. [CrossRef]
- Faria, M.G.B.F.; Andrade, R.L.P.; Camillo, A.J.G.; Leite, K.F.S.; Saita, N.M.; Bollela, V.R. Effectiveness of GeneXpert in the diagnosis of tuberculosis in people living with HIV/AIDS. Rev Saude Publica. 2021,55,89. [CrossRef]
- Cox, H.; Dickson,H.; Ndjeka, N.; Hoog, A.G.; Cobelens, A.F.; Stevens, W. Delays and loss to follow-up before treatment of drug-resistant tuberculosis following implementation of Xpert MTB/RIF in South Africa: A retrospective cohort study. PLoS Med. 2017, 14:2, e1002238. [CrossRef]
- Rimal, R.; Shrestha, D.; Pyakurel, S.; Poudel, R.; Shrestha ,P.; Rai, K R, et al. Diagnostic performance of GeneXpert MTB/RIF in detecting MTB in smear-negative presumptive TB patients. BMC Infect Dis. 2022, 22,321. [CrossRef]
- Habte, D.; Melese, M.; Hiruy, N.; Gashu, Z.; Jerene, D.; Moges, F.; Yifru, S.; Girma, B.; Kassie, Y.; Haile, Y.K.; Suarez, P.G.; Tessema, B. The additional yield of GeneXpert MTB/RIF test in the diagnosis of pulmonary tuberculosis among household contacts of smear positive TB cases. Int J Infect Dis. 2016, 49,179-184. [CrossRef]
- Gebretsadik, D.; Ahmed, N.; Kebede, E.; Mohammed, E.; Belete, M.A. Prevalence of Tuberculosis by Automated GeneXpert Rifampicin Assay and Associated Risk Factors among Presumptive Pulmonary Tuberculosis Patients at Ataye District Hospital, North East Ethiopia. Infect Drug Resist. 2020,13,1507-1516. [CrossRef]
- Gurung, S.C.; Dixit, K.; Paudel, R.; Sah, M.K.; Pandit, R.N.; Aryal, T.P.; Khatiwada, S.U.; Majhi, G.; Dhital, R.; Paudel, P.R.; et al. Comparing Additionality of Tuberculosis Cases Using GeneXpert or Smear-Based Active TB CaseFinding Strategies among Social Contacts of Index Cases in Nepal. Trop. Med. Infect. Dis. 2023, 8, 369. [CrossRef]
- Kalra, A.; Parija, D.; Raizada, N.; Sachdeva, K.S.; Rao, R.; Swaminathan, S. Upfront Xpert MTB/RIF for diagnosis of pediatric TB—Does it work? Experience from India. PLoS ONE.2020, 15(8), e0236057. [CrossRef]
- Sasikumar,C.; Utpat,K.; Desai,U.; oshi,J. The role of Genexpert in the diagnosis of Mycobacterium tuberculosis. Eur Respi J.2019, 54, PA3003. [CrossRef]
- Worku,M.; Agonafir,M.; Yassin,M.A.; Yassin,M.A.; Datiko,D.G.; Theobald,S.; Cuevas,L.E. Use of Xpert MTB/RIF for the Identification of TB and Drug Resistance among Smear-Negative and Re-Treatment Cases in Rural Areas of Ethiopia. Open Microbiol J. 2019, 13, 188-192. [CrossRef]
- Farra,A.; Manirakiza,A.; Yambiyo,B.M.; Zandanga,G.; Lokoti,B.; Arthaud,A.B.; Ngaya,G.; Hermana,G.; Ourandji,L.M.; Ignaleamoko,A.;Nzonzo,A.D.K.; Simelo,J.P.; Iragena,J.D. Surveillance of Rifampicin Resistance With GeneXpert MTB/RIF in the National Reference Laboratory for Tuberculosis at the Institut Pasteur in Bangui, 2015–2017.Open Forum Infect Dis.2023. [CrossRef]
- Zhou R et al (2022). Drug resistance characteristics of Mycobacterium tuberculosis isolates obtained between 2018 and 2020 in Sichuan, China. Epidemiol Infect.2022, 150, e27, 1–9. [CrossRef]
- Dreyer, V.; Mandal, A.; Dev,P.; Merker.M.; Barilar.I.; Utpatel,C.; Nilgiriwala,K.; Rodrigues,C.;Crook,D.W.et al.high fluoroquinolone resistance proportions among multidrug-resistant tuberculosis driven by dominant L2M.tuberculosis clones in the Mumbai Metropolitan region. Genome Med.2022, 14, 95. [CrossRef]
- WHO-Global tuberculosis Report 2020[internet].WHO.World Health Organization; [cited 2020 November 4].Available from:http://www.eho.int/ tb/ publications/ global_report/en/.
- Lee, H.W.; Yim, J.J. Fluoroquinolone resistance in multidrug-resistant tuberculosis patients. Korean J Intern Med. 2019,34,286-287. [CrossRef]
- Rohini Sharma,R.; Singha,B.K.; Kumar,K.; Ramachandran,R.; Jorwa,P. Presence of Fluoroquinolone mono-resistance among drug-sensitive Mycobacterium tuberculosis isolates: An alarming trend and implications. Clinl Epidemiol Glob Health.2019, 7, 363-366. [CrossRef]
Figure 1.
The procedures followed for screening and diagnosis tuberculosis and drug resistant tuberculosis cases.
Figure 1.
The procedures followed for screening and diagnosis tuberculosis and drug resistant tuberculosis cases.
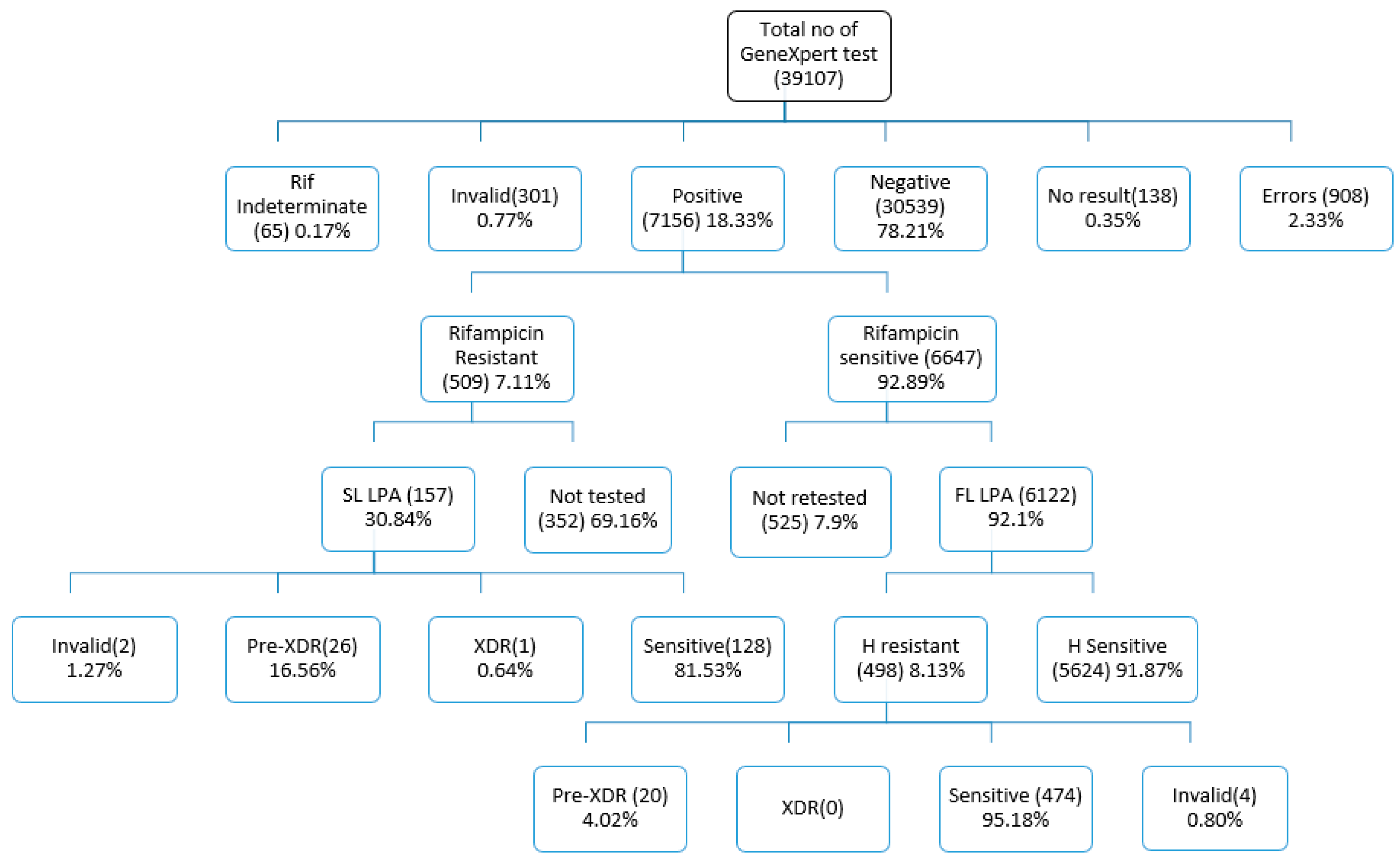
Figure 2.
Cumulative number of public and private facilities linked and cumulative number of referrals from ten cities in India, 2022.
Figure 2.
Cumulative number of public and private facilities linked and cumulative number of referrals from ten cities in India, 2022.
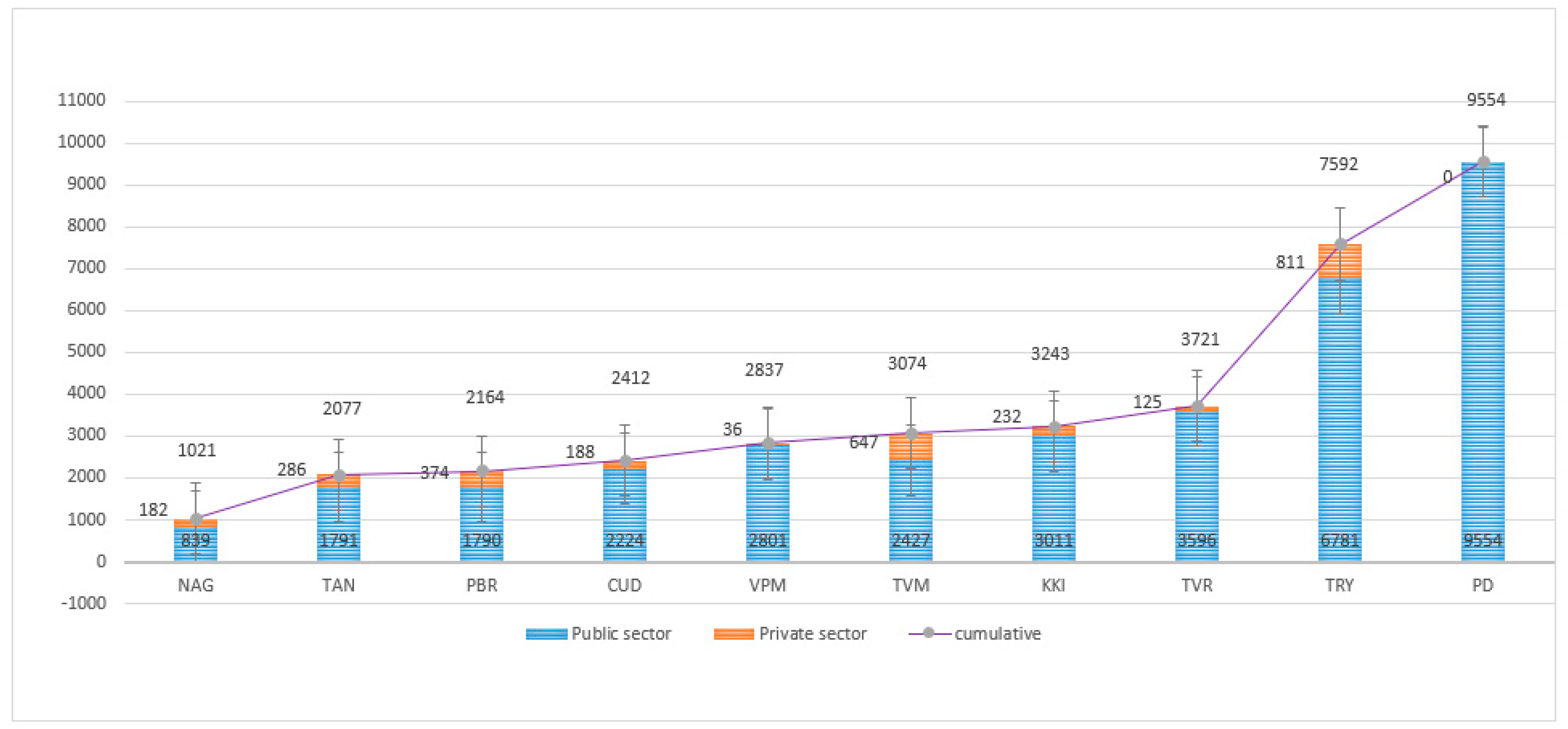

Table 1.
Laboratory findings of GeneXpert results among presumptive TB and presumptive DR TB.
| Stratification of patients | Total | MTB not detected (MTB-) | MTB detected (MTB+) | RIF resistance not detected | RIF resistance detected | % of MTB Positive | % of RIF Resistant |
|
| Presumptive TB | PLHIV out of presumptive TB | 2374 | 2195 | 179 | 155 | 10 | 7.54 | 5.59 |
| Paediatric out of presumptive TB | 2257 | 2207 | 50 | 49 | 0 | 2.22 | 0.00 | |
| Smear Negative, X-ray suggestive of TB | 11233 | 8927 | 2306 | 2088 | 113 | 20.53 | 4.90 | |
| Other Vulnerable group | 1820 | 1557 | 263 | 197 | 10 | 14.45 | 3.80 | |
| Contacts of TB & DRTB patients | 595 | 494 | 101 | 77 | 24 | 16.97 | 23.76 | |
| EP TB | 7639 | 6892 | 747 | 669 | 26 | 9.78 | 3.48 | |
| Upfront Molecular test offered | 4026 | 3427 | 599 | 191 | 6 | 14.88 | 1.00 | |
| Presumptive DRTB (Pulmonary) | Notified TB patients (New)- UDST | 3846 | 2273 | 1573 | 1210 | 268 | 40.90 | 17.04 |
| Notified TB patients (Pre-treated) -UDST | 462 | 275 | 187 | 165 | 19 | 40.48 | 10.16 | |
| Non-responders (DS TB & Hr TB) | 562 | 93 | 469 | 282 | 14 | 83.45 | 2.99 | |
| Private sector | Pulmonary TB | 1939 | 1430 | 509 | 472 | 15 | 26.25 | 2.95 |
| EPTB | 942 | 769 | 173 | 134 | 4 | 18.37 | 2.31 | |
| 37695 | 30539 | 7156 | 5689 | 509 | 18.98 | 7.11 | ||
Table 2.
Sensitivity, specificity, PPV and NPV, Disease prevalence and Accuracy TB screening tool among presumptive TB and presumptive DR TB.
Table 2.
Sensitivity, specificity, PPV and NPV, Disease prevalence and Accuracy TB screening tool among presumptive TB and presumptive DR TB.
| Number | % | Sensitivity (%) with 95% CI | Specificity (%) with 95% CI | PPV (%) with 95% CI |
NPV (%) with 95% CI |
Prevalence (%) with 95% CI | Accuracy (%) with 95% CI | Kappa with 95% CI | |
| PTB | 29114 | 74.45 | 99.87 (0.12-0.07) |
99.92 (0.04-0.03) |
99.71 (0.17-0.11) |
99.97 (0.04-0.01) |
21.38 (0.46-0.48) |
99.91 (0.04-0.03) |
0.99735 (0.99633-0.99837) |
| EPTB | 8581 | 21.94 | 99.45 (0.72- 0.37) |
99.84 (0.11-0.08) |
98.70 (0.97-0.55) |
99.93 (0.09-0.04) |
10.64 (0.65-0.67) |
99.80 (0.12-0.08) |
0.98962(0.98469-0.99455) |
| Presumptive TB | 32825 | 87.08 | 99.82 (0.17-0.10) |
99.91 (0.04-0.03) |
99.51 (0.23-0.16) |
99.97 (0.03-0.01) |
14.96 (0.38-0.39) |
99.93 (0.04-0.02) |
0.99605(0.99471-0.99740) |
| Presumptive DRTB (Pulmonary) | 4870 | 12.92 | 99.82 (0.28-0.13) |
99.77 (0.26-0.15) |
99.73 (0.33-0.15) |
99.85 (0.25-0.09) |
45.73 (1.41-2.41) |
99.92 (0.10-0.05) |
0.99586(0.99330-0.99842) |
| Presumptive TB: | |||||||||
| PLHIV out of presumptive TB | 2374 | 6.07 | 99.44 (2.53-0.55) |
99.91 (0.24-0.08) |
98.88 (3.20-0.84) |
99.95 (0.27-0.04) |
7.50 (1.03-1.13) |
99.87 (0.24-0.10) |
0.99091(0.98064-1.00000) |
| Paediatric out of presumptive TB | 2257 | 5.77 | 97.96 (8.81-1.99.) |
99.91 (0.24-0.08) |
96.00 (10.28-2.27) |
99.95 (0.26-0.04) |
2.17 (0.56-0.69) |
99.87 (0.26-0.10) |
0.96902(0.93400-1.00000) |
| Smear Negative, X-ray suggestive of TB | 11233 | 28.72 | 100.00 (0.16-0.0) |
99.99 (0.05-0.01) |
99.96 (0.27-0.03) |
100.00 (0.04-0.00) |
20.52 (0.74-0.76) |
99.99 (0.04-0.01) |
0.99973(0.99919-1.00000) |
| Other Vulnerable group | 1820 | 4.65 | 99.62 (1.73-0.37) |
99.87 (0.33-0.11) |
99.24 (2.21-0.57) |
99.94 (0.39-0.05) |
14.40 (1.59-1.69) |
99.84 (0.32-0.13) |
0.99332(0.98577-1.00000) |
| Contacts of TB & DRTB patients | 595 | 1.52 | 100.00 (3.69-0.00) |
99.40 (1.15-0.48) |
97.03 (5.67-1.99) |
100.00 (0.74-0.00) |
16.47 (2.89-3.23) |
99.50 (0.97-0.40) |
0.98190(0.96147-1.00000) |
| EP TB | 7639 | 19.53 | 99.60 (0.78-0.32) |
99.90 (0.11-0.06) |
99.06 (1.00-0.39) |
99.96 (0.09-0.03) |
9.73 (0.66-0.68) |
99.87 (0.11-0.07) |
0.99256(0.98796-0.99717) |
| Upfront Molecular test offered | 4026 | 10.29 | 99.83 (0.76-0.17) |
99.97 (0.13-0.03) |
99.83 (1.00-0.15) |
99.97 (0.18-0.03) |
14.88 (1.09-1.54) |
99.95 (0.13-0.04) |
0.99804(0.99532-1.00000) |
| Presumptive DRTB (Pulmonary): | |||||||||
| Notified TB patients (New)- UDST | 3846 | 9.83 | 99.94 (0.34-0.06) |
99.87 (0.25-0.10) |
99.81 (0.40-0.13) |
99.96 (0.27-0.03) |
40.85 (1.56-1.57) |
99.90 (0.17-0.07) |
0.99785(0.99574-0.99996) |
| Notified (Previously treated) -UDST | 462 | 1.18 | 99.47 (2.41-0.52) |
99.64 (1.65-0.35) |
99.47 (3.13-0.45) |
99.64 (2.15-0.31) |
40.48 (4.51-4.63) |
99.57 (1.12-0.38) |
0.99102(0.97859-1.00000) |
| Non-responders (DS TB & H Resistant TB) |
562 | 1.44 | 99.57 (1.10-0.38) |
97.85 (5.40-1.89) |
99.57 (1.23-0.32) |
97.85 (5.91-1.60) |
83.45 (3.33-2.98) |
99.29 (1.10-0.62) |
0.97423(0.94907-0.99939) |
| Private sector: | |||||||||
| Pulmonary TB | 1939 | 4.96 | 100.00 (0.78-0.00) |
99.93 (0.32-0.07) |
99.80 (0.18-0.17) |
100.00 (0.26-0.00) |
26.20 (1.95-2.02) |
99.95 (0.24-0.05) |
0.99867(0.99606-1.00000) |
| EPTB | 942 | 2.41 | 98.82 (3.01-1.04) |
99.35 (0.85-0.44) |
97.11 (3.77-1.66) |
99.74 (0.76-0.19) |
18.05 (1.41-2.60) |
99.26 (0.79-0.44) |
0.97505(0.95664-0.99346) |
Table 3.
Distribution of rifampicin-resistance patients in relation to different regions of rpoB gene detected through Probes A, B, C, D and E.
Table 3.
Distribution of rifampicin-resistance patients in relation to different regions of rpoB gene detected through Probes A, B, C, D and E.
| Xpert results | R resistant detected | Resistant Probes | |||||
| Probe A | Probe B | Probe C | Probe D | Probe E | Δ CT value >4 | ||
| Very low | 212(41.65%) | 09 | 27 | 19 | 22 | 29 | 106 |
| Low | 163(32.02%) | 13 | 15 | 17 | 21 | 28 | 69 |
| Medium | 98(19.25%) | 13 | 12 | 09 | 12 | 10 | 42 |
| High | 36(7.07%) | 2 | 1 | 4 | 2 | 1 | 26 |
| Total | 509 | 37(7.27%) | 55(10.81%) | 49(9.63%) | 57(11.20%) | 68(13.36%) | 243(47.74%) |
Table 4.
The frequency and mutations confer resistance to fluoroquinolone drug.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



