
Submitted:
13 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
Backround Cochlear implant is the first approved cranial nerve stimulator that works by directly stimulating the cochlear nerve. Various attempts have been made to evaluate the dimensions of the cochlea related to cochlear implantationThe preoperative computed tomographic examination is essential in assessing the anatomical aspect of the cochlea, but also in determining its dimensions, in order to choose an appropriate electrode, in order to obtain the best possible audiological performance.
Method
In the present paper, we aimed to carry out an observational study, regarding the role of cochlear measurements in the preoperative evaluation of patients proposed for cochlear implant. The purpose of the study was to measure the cochlea and to establish the existence of a correlation between the size of the cochlea and the age and gender of the patients.
Results
From the group of 35 examined patients, 54% (n= 19) were male and 46% (n=16) female. The average length of the cochlea in the age group 0-4 years is 7.82 mm in the left ear and 7.86 in the right ear, in the age group 4-7 years it is 7.82 mm and 7.94 mm respectively, for the age group 7-14 years the dimensions increase to 8.48 and 8.77 mm respectively, and after 14 years these dimensions reach 9.12, respectively 9.18 mm. Comparative measurements of the length of the cochlea by age groups show an increase in length with the patient's age, but this increase does not exceed 1.5 mm for both the right and left ears. The measurements of the width of the cochlea, by age group, start from 6.84 mm left ear and 6.81 mm right ear at 0-4 years, 6.94 mm and respective 6.97 mm at the group 4-7 years, 7.71 mm and respective 7.55 mm at 7-14 years , and reaching 8.19 mmm and 8.12 mm at the age of over 14 years.
Conclusions
From the study carried out it can be concluded that the evaluation of the dimensions of the cochlea is important for cochlear implantation, the size variables, although small, are still an element to be considered in correlation with the age of the patient and the implanted ear. This increase is statistically insignificant, but it still exists, even if from a theoretical point of view, it is considered that the dimensions of the cochlea remain constant.
Keywords:
cochlear implant
; computer tomography
; cochlea width
; cochlea length
1. Introduction
The cochlear implant is the first example of a neural prosthesis that can replace a sensory organ, overcoming the non-functional auditory periphery of people suffering from bilateral sensorineural hearing loss. Cochlear implant is the first approved cranial nerve stimulator that works by directly stimulating the cochlear nerve. The medical and societal impact of this revolutionary device cannot be understated1.The cochlear implant is a neural prosthesis that can replace a sensory organ, restarting an electrical stimulation of the cochlear nerve. With the help of this cochlear amplifier called a cochlear implant, low-amplitude waves are transformed into high-amplitude [1]. Cochlear implants have a long history complete with innovations that have resulted in a high performing device today. Totally implanted devices, improving neural health and survival through drug-directed therapy, intraneural electrode placement, electroacoustic stimulation and hybrid cochlear implants, and methods to improve the neural prosthetic interface are evolving areas of cochlear implant innovation.
The temporal bone has a very complex anatomical structure, in which the sensory organs of the cochlea and the vestibular system are contained in a small space, together with the sound conduction system of the middle ear. Therefore, detailed imaging is necessary in this anatomical area. There are many clinical objectives for which the highest possible spatial resolution is required. These include locating cerebrospinal fluid (CSF) fistulas, detecting malformations of the middle and inner ear, vestibulocochlear nerve and facial nerve, and locating abnormalities of arterial and venous structures while also confirming dehiscence of the semicircular canals. The cochlea, from an anatomical point of view, can vary in size, however, the cochlear structures remain approximately similar. However, there are certain changes in size, which can influence the insertion of the cochlear implant. Various attempts have been made to evaluate the dimensions of the cochlea related to cochlear implantation. Little attention was paid to the distinct narrowing of the scala tympani in the region of the ascending part of the cochlear duct, although from the literature, it is known that electrode insertion trauma frequently occurs here. Individual variations of the cochlear micromorphology may additionally contribute to the failure of preformed electrode arrays, but the challenge of guiding the electrode array around the first bend of the cochlear turn, that is, the pars ascenders, is obviously impaired by the interindividual constant narrowing in this area. Therefore, this finding may have implications on the development of electrode designs and insertion methods [2]. The diameter of the Scala Tympani decreases by approximately 300 microm during the ascending part of the basal turn [2,3]. Thus, in patients with a smaller cochlear base, the insertion of the cochlear electrode is influenced by the appearance of resistance points. The cochlear lumen shows a noncontinuous spiraling path leading to potential pressure points during cochlear implantation at the basilar membrane in the region of 180 to 225 (12-14 mm) and 725 degrees (22-26 mm) and at the floor of the Scala tympani around 0 to 90, 225 to 270, and 405 to 450 degrees3. Measuring the basal length of the cochlea before cochlear implantation plays an important role, as it can give valuable indications in anticipating difficulties in electrode insertion [4,5]. From a structural point of view, the cochlear electrode has a diameter of 0.5 mm at the apical level, and a diameter of 0.8 mm at the basal level. The full insertion of the cochlear electrode does not exceed the active length of 15 mm [6,7].
In general, the complete insertion of the electrode is indicated, in order to ensure effective cochlear stimulation and achieve the best hearing performance. However, due to multiple anatomical variations, electrode insertion is difficult to achieve..The preoperative computed tomographic examination is essential in assessing the anatomical aspect of the cochlea, but also in determining its dimensions, in order to choose an appropriate electrode, in order to obtain the best possible audiological performance. Added to these is the possibility of anticipating some intraoperative complications that could occur [8]. Preoperatively, CT can be helpful in making decisions about the most optimal surgical approach and can help minimize complications during surgery. With the help of computer tomography, bone structures can be properly evaluated, establishing their contours, their dimensions and shape. The choice of appropriate settings, as well as the use of contrast in the evaluation of the appearance of the cochlea, allow an adequate evaluation of its shape and dimensions. The possibility of multiplane reconstructions, with the help of a high-resolution computer tomography, measurements of the length, width and basal diameter of the cochlea can be made, the measurement plane being between the round and oval window, in a plane that includes the cochlear canal [9,10], the vestibule and parts of the semicircular canals (Figure 1).
Figure 1.
A- Length and B-width cochlea measurments.
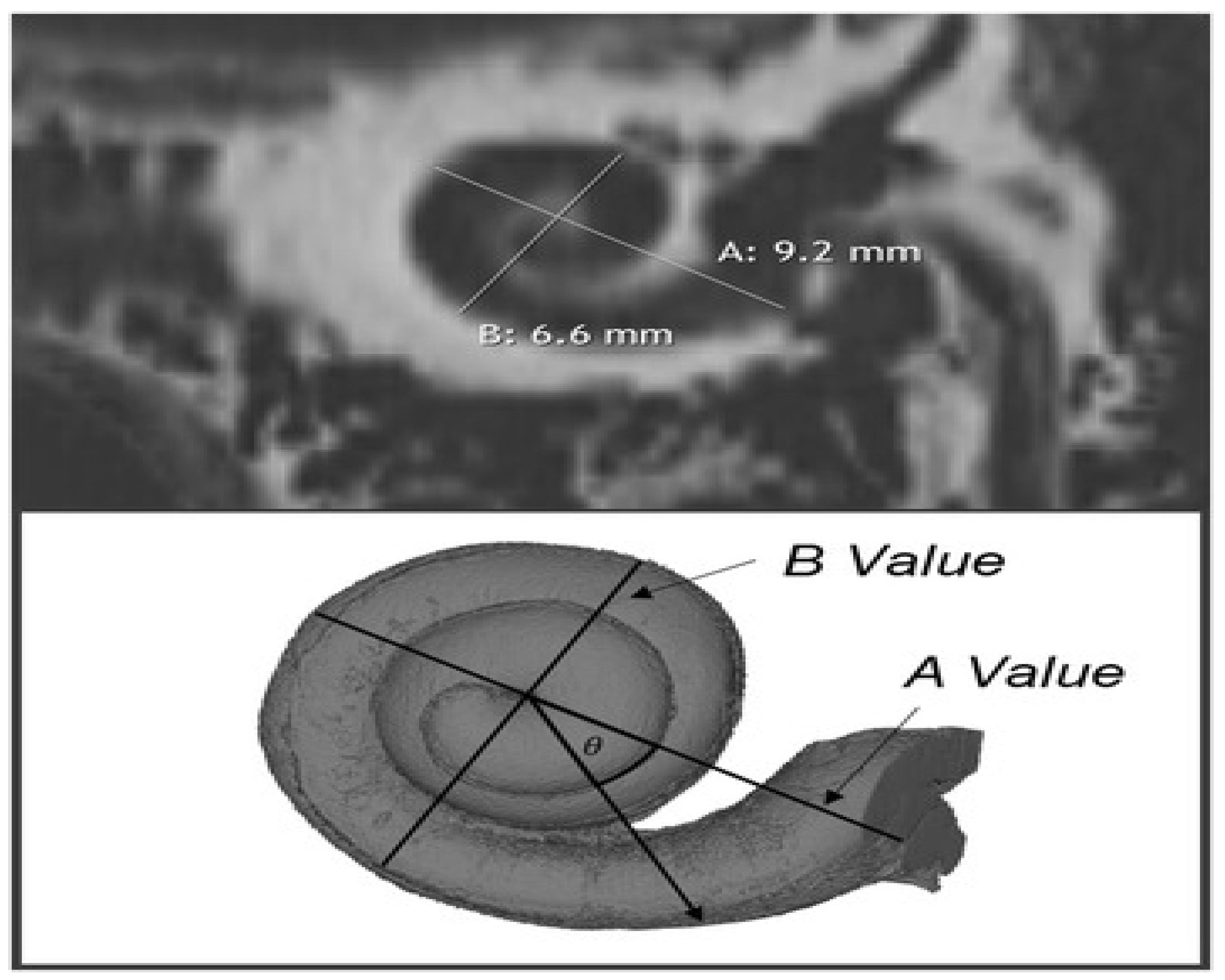
Knowledge of the cochlear implant array's precise position is important because of the correlation between electrode position and speech understanding. Several groups have provided recent image processing evidence to determine scalar translocation, angular insertion depth, and cochlear duct length (CDL); all of which are being used for patient-specific programming. Cone beam computed tomography (CBCT) is increasingly used in otology due to its superior resolution and low radiation dose. [11]. Measurement of the angular depth of insertion (aDOI) of cochlear implant electrode arrays has numerous clinical and research applications. Plain-film radiographs are easily obtained intraoperatively and have been described as a means to calculate aDOI. CT imaging with 3D reformatting can be used for cochlea measurement, but is less conveniently obtained and requires higher radiation doses, a particular concern in pediatrics. The extent to which plain-film and 3D CT image-based measurements are representative of the true position of the electrode within the cochlea is unknown [12]. In the present paper, we aimed to carry out an observational study, regarding the role of cochlear measurements in the preoperative evaluation of patients proposed for cochlear implant. The purpose of the study was to measure the cochlea and to establish the existence of a correlation between the size of the cochlea and the age and gender of the patients, as well as to show the existence of some of its variations. This study was carried out by using preoperative CT images in implanted patients and evaluating the length and width of the cochlea. The data were correlated with those from the specialized literature, as well as with the demographic data of the patients.
1. Materials and method
This retrospective observational study was performed on a group of 35 patients with bilateral sensorineural hearing loss hospitalized in the Targu Mures, Otorhinolaryngologic Department, in the period 2016-2017, where the demographic data regarding the age, sex, and patients were analyzed, and later the data related to the size of the cochlea were added, through the analysis of computed tomography images. The criteria for inclusion in the study were taken according to the age of the patients: 0-4 years, 4-7 years, 7-14 years and over 14 years. The data were analyzed only for patients with profound or severe sensorineural hearing loss, candidates for cochlear implants, being excluded from the study patients with moderate or mild unilateral or bilateral hearing loss, or with other types of hearing loss. The collected data were entered and processed in Microsoft Excel tables and the statistical processing was done with the GraphPad InStat3 program, using descriptive statistics. For the comparison of two or more variables we used the Fischer and student t tests. To consider a value as statistically significant, we considered a p<0.05.
1. Results
From the group of 35 examined patients, 54% (n= 19) were male and 46% (n=16) female, which demonstrates in our study the predominance of male patients, without this being a general rule of cochlear implantation, or a selective criterion for cochlear measurements. By measuring the width of the cochlea, at its base, without taking into account the sex and age of the patients, the presence of an average value of 7.42 mm ± 2 mm was found without a difference between the 2 cochleae. The length measurements show the existence of an average value of 8.41±6 mm, without a significant difference between the 2 cochlea, however it was found that the width of the cochlea in the right ear is smaller in all examined patients than the left ear, while which its length is greater, although the difference is insignificant. Referring to the correlation with the age of the patients, the results were as follows: 8.61 mm for females and 8.41 mm for males, the difference not being significant, taking into account the fact that the measurements have a subjective character. The average length of the cochlea in the age group 0-4 years is 7.82 mm in the left ear and 7.86 in the right ear, in the age group 4-7 years it is 7.82 mm and 7.94 mm respectively, for the age group 7-14 years the dimensions increase to 8.48 and 8.77 mm respectively, and after 14 years these dimensions reach 9.12, respectively 9.18 mm. Comparative measurements of the length of the cochlea by age groups show an increase in length with the patient's age, but this increase does not exceed 1.5 mm for both the right and left ears. The measurements of the width of the cochlea, by age group, start from 6.84 mm left ear and 6.81 mm right ear at 0-4 years, 6.94 mm and respective 6.97 mm at the group 4-7 years, 7.71 mm and respective 7.55 mm at 7-14 years, and reaching 8.19 mmm and 8.12 mm at the age of over 14 years. In the age group between 0 and 4 years, the optimal age for the cochlear implant, the difference in length between the 2 ears is 0.04 mm, and the width of the left cochlea is 0.03 mm larger than the right cochlea. In the age group 4-7 years the difference in length between the 2 cochlea shows the right cochlea larger than the left cochlea, in contrast the width measurements demonstrate right cochlea width 0.03 mm larger than the left cochlea width, inverse to the cochlea width measured in the 0-4 year group. The evaluation of the cochlear dimensions in the age group 7-14 years shows first of all a difference of 0.29 mm difference between the right and left cochlea in length, the right cochlea being larger than the left cochlea - the same as in the age groups 0-4 years, respectively 4-7 years. The width of the left cochlea is smaller than the right cochlea by 0.15 mm. It is also noticeable here that the left cochlea is smaller than the right, just like in the age group 4-7 years. In the over 14 age group, a difference of 0.06 mm is noted between the lengths of the right and left cochlea, while width measurements show an increase in the size of the left cochlea over the right by 0.07 mm. Comparative measurements of the length of the cochlea by age groups show an increase in length with the patient's age, but this increase does not exceed 1.5 mm for both the right and left ear. The evaluation of the width of the cochlea shows a gradual increase in it in all age groups for both the right and left cochlea. As with general measurements, the size difference between the right and left cochlea is maintained. The evaluation of the width of the cochlea shows a gradual increase in it in all age groups for both the right and left cochlea. Correlations between cochlear lengths, cochlear widths and age groups demonstrate the lack of a specific correlation, the coefficient being greater than 0.001.
| Age | Width Left Ear | Width right Ear | |||
| Age | Pearson Correlation | 1 | .597** | .610** | |
| Sig. (2-tailed) | .000 | .000 | |||
| N | 35 | 35 | 35 | ||
| Width left Ear | Pearson Correlation | .597** | 1 | .963** | |
| Sig. (2-tailed) | .000 | .000 | |||
| N | 35 | 35 | 35 | ||
| Width right Ear | Pearson Correlation | .610** | .963** | 1 | |
| Sig. (2-tailed) | .000 | .000 | |||
| N | 35 | 35 | 35 | ||
| Age | Left Ear length | Right Ear Length | |||
| Spearman's rho | Age | Correlation Coefficient | 1.000 | .652** | .668** |
| Sig. (2-tailed) | . | .000 | .000 | ||
| N | 35 | 35 | 35 | ||
| Left Ear length | Correlation Coefficient | .652** | 1.000 | .944** | |
| Sig. (2-tailed) | .000 | . | .000 | ||
| N | 35 | 35 | 35 | ||
| Right Ear length | Correlation Coefficient | .668** | .944** | 1.000 | |
| Sig. (2-tailed) | .000 | .000 | . | ||
| N | 35 | 35 | 35 | ||
1. Discussion
Although in the study carried out by us no significant differences in the growth of the cochlea by age groups were found, neither in the left nor in the right ear, however, knowing the dimensions of the cochlea are essential in the preoperative evaluation of patients for cochlear implant. From the studied group of 35 patients, the demographic assessment consists of the predominance of the male sex, without this being a general rule for cochlear implantation, or a selection criterion for patients. The evaluation of cochlear dimensions by age groups, although statistically insignificant, is nevertheless important from a surgical point of view. The evaluation of age groups shows a prevalence of age 0-4 years 14 patients, followed by 4-7 years 5 patients, 7-14 years 3 patients and over 14 years 13 patients. The predominance of patients 0-4 is also an essential criterion for selecting patients for cochlear implant. The evaluation of the length of the cochlea, performed right-left comparison, shows that there are differences between the 2 cochlea, in all age groups as follows: in the age group between 0 and 4 years, optimal age for performing the cochlear implant, the difference in length between the 2 ears is 0.04 mm, and in width the left cochlea is 0.03 mm larger than the right cochlea. As with general measurements, the size difference between the right and left cochlea is maintained; in the age group 4-7 years the difference in length between the 2 cochlea shows the right cochlea larger than the left cochlea, in contrast the width measurements demonstrate right cochlea width 0.03 mm greater than left cochlea width, inverse of cochlea width measured in the 0-4 years group; the assessment of cochlear dimensions in the age group 7-14 years shows primarily a difference of 0.29 mm difference between the right and left cochlea in length, the right cochlea being larger than the left cochlea - the same as in the age groups 0-4 years, respectively 4-7 years. The width of the left cochlea is smaller than the right cochlea by 0.15 mm. It is also noticeable here that the left cochlea is smaller than the right, just like in the age group 4-7 years; in the over 14 age group, there is a difference of 0.06cm between the lengths of the right and left cochlea, while the width measurements show an increase in the size of the left cochlea compared to the right by 0.07mm.
The optimal implantation age between 0-4 years is characterized in terms of cochlear dimensions, by smaller values in both width and length, but since this difference compared to older ages is not significant, the choice of the type of electrode it is not correlated with the patient's age. There is also a difference between the right and left ear both in length and width, which may raise the question of whether there is an indication for implants to take this difference into account. The specialized literature shows that cochlear anatomical variations, related to its dimensions, can influence the insertion of the electrode.
1. Conclusion
Assessment of cochlear dimensions is essential in preparing patients for cochlear implant. Variables in cochlear dimensions must be taken into account, as there may be anatomical variations of the cochlea, which may influence its size, which influences the way of insertion. Changes in the width of the cochlea are also related to its malformations, influencing the way of insertion, when cochleostomy is performed as a way of inserting the electrode. Variations in the dimensions of the cochlea, both in length and width, are related to age and sex, and there is an increase in them with advancing age. This increase is statistically insignificant, but it still exists, even if from a theoretical point of view it is considered that the dimensions of the cochlea remain constant. The dimensions change a little, not necessarily related to malformations of the cochlea. The study carried out evaluated the normally conforming cochlea. Knowing the length of the cochlea is important in how to insert the electrode, the explanation is as follows: the values of the length of the cochlea fluctuate according to age and sex, as well as between the right and left cochlea, not significantly, but enough to know it before the implant. The practical applicability consists in the functional necessity of inserting all the electrodes of the implant in order to obtain the expected audiological performances. Audiological performance is related to intraoperative measurements of cochlear implant functionality. These are directly related to the degree of insertion of the electrode into the cochlea, which must be complete, i.e. equivalent to its length of 1.5 mm. The fact that the growth of the cochlea does not occur over time over 1.5 mm, the standard size of the length of the electrode, means that at any age if there is a normally compliant cochlea, the electrode can be completely inserted into the cochlea, obtaining the expected audiological performances through electrical stimulation .
Author Contributions
CMN.: Methodology: Writing—Original Draft; EMD: Data curation, Visualization, Investigation, Writing—Original Draft; AGV.: Data curation, Investigation, Writing—Original Draft; AN: Methodology, Supervision, Project administration, Writing—Reviewing and Editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the legal guardian(s) of subjects.
Informed Consent Statement
Not applicable.
Data Availability Statement
Participant-level data are available from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Naples, J.G.; Ruckenstein, M.J. Cochlear Implant. Otolaryngol Clin North Am. 2020, 53, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Biedron, S.; Prescher, A.; Ilgner, J.; Westhofen, M. The internal dimensions of the cochlear scalae with special reference to cochlear electrode insertion trauma. Otol Neurotol. 2010, 31, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Verbist, B.M.; Ferrarini, L.; Briaire, J.J.; Zarowski, A.; Admiraal-Behloul, F.; Olofsen, H.; Reiber, J.H.; Frijns, J.H. Anatomic considerations of cochlear morphology and its implications for insertion trauma in cochlear implant surgery. Otol Neurotol. 2009, 30, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Ramamoorthy, S.; Deo, N.V.; Grosh, K. A mechano-electro-acoustical model for the cochlea: response to acoustic stimuli. J Acoust Soc Am 2007, 121, 2758. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.R.; Taber, L.A. Comparison of WKB calculations and experimental results for three-dimensional cochlear models. J Acoust Soc Am 1979, 65, 1007–1018. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, B.M.; Patuzzi, R.; Yates, G.K. Basilar membrane measurements and the travelling wave. Hear Res 1986, 22, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Shera, C.A.; Guinan, J.J., Jr. Revised estimates of human cochlear tuning from otoacousic and behavioural measurements. Proc Natl Acad Sci 2002, 99, 3318–3323. [Google Scholar] [CrossRef] [PubMed]
- Shera, C.A.; Guinan, J.J., Jr.; Oxenham, A.J. Otoacoustic estimation of cochlear tuning. JARO 2010, 11, 343–365. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.V. Smart biological systems as models for enghineered structures. Mater Sci Eng C 1996, 4, 19–26. [Google Scholar] [CrossRef]
- Allen, J.B. Cochlear micromechanics—a physical model of transduction. J Acoust Soc Am 1980, 68, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Nateghifard, K.; Low, D.; Awofala, L.; Srikanthan, D.; Kuthubutheen, J.; Daly, M.; Chan, H.; Irish, J.; Chen, J.; Lin, V.; et al. Cone beam CT for perioperative imaging in hearing preservation Cochlear implantation–a human cadaveric study. J Otolaryngol Head Neck Surg. 2019, 48, 65. [Google Scholar] [CrossRef] [PubMed]
- Gallant, S.; Friedmann, D.R.; Hagiwara, M.; Roland, J.T., Jr.; Svirsky, M.A.; Jethanamest, D. Comparison of Skull Radiograph and Computed Tomography Measurements of Cochlear Implant Insertion Angle. Otol Neurotol 2019, 40, e298–e303. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



