Submitted:
29 September 2023
Posted:
29 September 2023
You are already at the latest version
Abstract
Extreme cytoreductive surgery (eCRS) may sometimes be required to achieve complete cytoreduction, which is one of the most important prognostic factors. This study investigated the impact of eCRS on survival and peri-postoperative outcomes. Malignant peritoneal mesothelioma (MPM) patients who underwent cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) were retrospectively examined. Patients who underwent CRS-HIPEC were divided into eCRS and less extensive CRS (leCRS) groups. Resection of ≥5 organs or ≥3 small bowel anastomoses was defined as eCRS. Survival and perioperative outcomes of both groups were compared.In the study including 31 patients, eCRS-HIPEC was used in 15 patients. Complete cytore-duction (CC score 0/1) was achieved in all 31 patients. Compared with LeCRS, mean length of stay, length of stay in the intensive care unit, mean peritoneal cancer index (PCI), and intraoperative blood loss were higher in the eCRS group. Additionally, the risk of developing complications was observed to be more frequent and the duration of surgery was longer. Rates of serious complications and morbidity were similar in patients undergoing eCRS compared with leCRS. In patients with high PCI and multiple organ involvement, complete cytoreduction can be achieved by performing eCRS and equivalent survival results can be achieved with low PCI..
Keywords:
cytoreductive surgery
; extreme cytoreductive surgery
; hyperthermic intraperitoneal chemotherapy
; malign peritoneal mesothelioma
; peritoneal cancer index.
1. Introduction
Malignant peritoneal mesothelioma (MPM) is a rare but lethal cancer with an incidence of 0.2-3 per 1,000,000 worldwide [1]. Mesothelioma originates from the mesothelial cells that form the pleura, pericardium, peritoneum, and tunica vaginalis [2]. MPM accounts for 7-30% of all mesotheliomas [3]. Most of malignant mesotheliomas originate in the pleura. Although pleural mesothelioma is more common in men, there is no difference in the incidence of MPM between men and women [4]. The most common risk factor is asbestosis [5,6]. There are 3 histologic subtypes of MPM: epithelioid, biphasic, and sarcomatoid [7].
MPM is initially asymptomatic in many patients. The disease is usually diagnosed at an advanced stage, and symptoms usually appear during this period. The most common symptoms are ascites (32%), abdominal pain (69%), asthenia (43%), weight loss (32%), anorexia (30%), and abdominal mass (30%) [8]. If the disease is left untreated, rapid progression occurs with an overall survival (OS) of 6-12 months [9,10,11,12]. In recent years, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) have become the main methods in the treatment of MPM [13,14,15]. Many multicenter studies have shown that the survival of patients with MPM can be improved with CRS-HIPEC [16,17,18,19,20]. The goal of CRS is complete cytoreduction. Complete cytoreduction means no residual lesion larger than 2.5 mm remains at the end of surgery. HIPEC aims to treat residual microscopic diseases. OS was observed between 34 and 92 months in MPM patients who received CRS-HIPEC as their first treatment option. Severe complications between 30% and 41% and postoperative mortality between 2.0% and 2.6% are observed in patients undergoing CRS-HIPEC [8,15,21,22,23,24,25].
Multivisceral resections are often required to achieve complete cytoreduction. The concept of extreme cytoreductive surgery (eCRS) is used in cases where ≥ 5 organs are removed or ≥ 3 bowel anastomoses are performed during surgery [26]. Studies on the effects of eCRS on survival and perioperative outcomes in patients with MPM are limited. Our aim in this study is to investigate the impact of eCRS on survival and peri-postoperative outcomes in patients who underwent CRS-HIPEC diagnosed with MPM.
2. Materials and Methods
2.1. Patient Selection and Data Collection
Patients who underwent CRS-HIPEC for MPM in the Department of Surgical Oncology at a University between 2004 and 2018 were retrospectively screened. Patients whose survival data could not be determined, who had an MPM subtype other than the epithelioid type, in whom complete cytoreduction could not be achieved, and who underwent emergency surgery were excluded from the study.
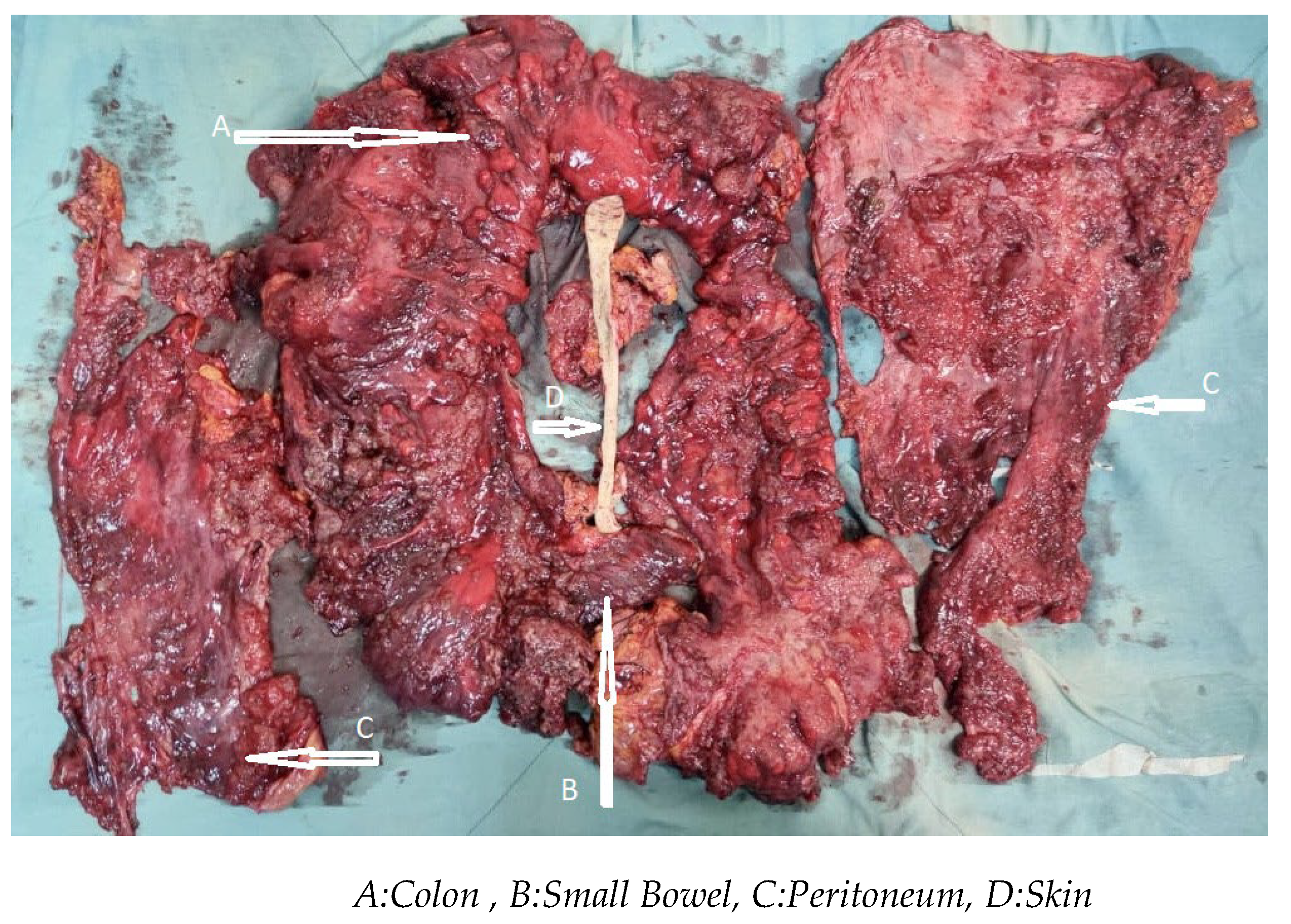
eCRS was defined as the resection of ≥ 5 major organs or the creation of ≥ 3 bowel anastomoses (Figure 1A). The major organs were the colon/rectum, small bowel, pancreas, gallbladder, spleen, stomach, diaphragm (full resection), uterus/ovary, urinary bladder/ureter/kidney, and liver (parenchymal resection of a segment). Peritoneum, omentum, superficial diaphragmatic resection, and capsular liver resection were excluded from the definition of major organ resection.
Less extensive CRS (leCRS) was defined as the resection of < 5 organs or < 3 small bowel anastomoses [26]. (Figure 1B).
Figure 1B.
Less Extensive Cytoreduction.
Patients were thus divided into two groups. Clinical and demographic characteristics of the patients, peritoneal cancer index (PCI), and completeness of cytoreduction (CC) score calculated during surgery, the number of organs removed, the number of anastomoses, histological subtype of tu-mors, complications, and degree of morbidity (Clavien-Dindo scale) [27], survival information, as-bestos exposure, prior abdominal surgery, American Society of Anesthesiologists (ASA) class, re-operation, readmission, Length of Hospital Stay (LOHS) day, Estimated Blood Loss (EBL), Body Mass Index (BMI), operative time, and length of stay days in the intensive care unit (ICU LOS) were retrospectively reviewed.
The PCI score was calculated according to the Sugarbaker classification [28]. The CC score was cal-culated as follows: CC -0: no visible tumor cells, CC -1 < 2.5 mm residual disease, CC -2 2.5mm-2.5 cm residual disease, CC -3 > 2.5 cm residual disease. CC - 0 and CC -1 were accepted as complete cytoreduction [29].
2.2. Results Surgery and Intraperitoneal Chemotherapy Procedure
Initially, complete cytoreduction was achieved. Then HIPEC was performed according to the closed method. Intraperitoneal chemotherapy with mitomycin-C (20 mg/m2), cisplatin (30 mg/m2), and paclitaxel (20mg/m2) was administered intraoperatively in 3000 ccs 0.9% saline heated to 41-43 C in all patients. The chemotherapy solution was drained through four drain catheters to maintain circulation through the heat pump. The HIPEC lasted 60 minutes. Gastrointestinal anastomoses were created before the HIPEC. Administration of EPIC began approximately after the postoperative 24 hours. Paclitaxel was administered in a solution via an infusion pump containing 1000 mL/h 3% NaCl. After approximately 23 hours, the drains were opened, and the fluid was drained from the abdominal cavity. This procedure was performed for 5 consecutive days.
2.3. Statistical Analysis
Data were analyzed using IBM SPSS V23. Conformity to normal distribution was assessed with the Shapiro-Wilk test. The Pearson chi-square test, Yates correction, and Fisher's exact test were used to compare categorical variables by the group. The independent samples t-test was used to compare normally distributed variables by groups, and the Mann-Whitney U test was used to compare varia-bles that did not conform to the normal distribution. Cox regression analysis was used to examine the factors affecting survival. The log-rank test was used to compare survival between groups. Analysis results were presented as frequency (percentage) for categorical variables and mean ± standard deviation and median (minimum-maximum) for quantitative variables. The significance level was taken as p < 0.05.
3. Results
Thirty-nine patients underwent CRS-HIPEC and were diagnosed with MPM. Five patients were excluded from the study because complete cytoreduction was not performed, and three patients were excluded because survival data were undetermined. Thirty-one patients were enrolled in the study. The eCRS group included 15 patients (48.4%). The mean age of the patients was 62.5 years, and 45.2% were women. Asbestos exposure was present in 74%, and 32% had prior abdominal surgery. The average BMI was 28.1 and considering the ASA classes, the rate of those in class 2 was 25.8%, the rate of those in class 3 was 54.8%, and the rate of those in class 4 was 19.4%. The rate of those with CC -0 was 41.9%, and the rate of those with CC -1 was 58.1%. The mean of PCI was calculated to be 20.6. The overall complication rate was 38.7%, and the incidence of Clavien-Dindo 3-4 complications was 22.6%. The reoperation rate was 16.1%, and the readmission rate was 22.6%. Median survival was calculated as 35 months, LOHS as 13.7 days, EBL as 335.3 mL, operative time as 6.8 hours, and ICU LOS as 2.5 days (Table 1).
The patterns of organ resection during cytoreduction are shown in Table 2. The most commonly resected organs were the colon (19.4%) and small bowel (18%), followed by the spleen (13.8%), gallbladder (11.1%), uterus/over/vagen, and stomach (8.3%). Liver (2.7%), pancreas, and rectum (5.5%) resections were rare. Diaphragmatic resections (6.9%) were performed more on the left side (4.1%) than on the right side (2.7%).
When comparing categorical variables by group, complications were statistically significantly more common in the eCRS group than in the leCRS group (60% vs. 18.8 p= 0.047). There was no significant difference between the two groups regarding gender, CC score, asbestos exposure, prior abdominal surgery, ASA class, reoperation, readmission, and Clavien-Dindo 3-4 complications (Table 3).
When comparing quantitative variables by group, the eCRS had statistically significant higher PCI (mean 25.2 v.s 16.3 p<0.001), LOHS (mean 15 v.s 11.5 days p<0.001), EBL (mean 398.6 v.s 275.9 ml p<0.001), BMI (mean 26 v.s 29 p<0.001), operative time (mean 7.6 v.s 6.1 hour, p<0.001) and ICU LOS (3 v.s 2 days, p<0.001) than in the leCRS group. No significant difference was found between the two groups regarding age and survival (Table 4).
The effect of the independent variables on survival was examined using Cox regression analysis. When the univariate mo-del was considered, it was found that the risk of death in men was lower than in women (HR =0.14; p=0.003). When the model was examined as a multivariate model, it was found that men's risk of death was lower than women's (HR<0.001; p=0.001). Other variables had no statistically significant effect on survival (Table 5).
There was no statistically significant difference between the mean OS by group (p=0.895). While the mean OS in the eCRS group was 37.5 months, the mean OS duration in the leCRS group was 42.8 months (Table 6, Figure 2A-B).
4. Discussion
Historically, treatment of MPM consisted of chemotherapy, palliative surgery, and radiotherapy. With this treatment modality, which was used before the 2000s, OS was only about 1 year [30]. 0. After MPM was recognized as a surgically treatable disease, the treatment modalities and prognosis changed significantly. Complete cytoreduction with total peritonectomy and visceral resections became the standard surgical procedure [31]. Subsequently, the contribution of intraperitoneal chemotherapy has been demonstrated 17. OS has been shown to have a prognosis ranging from 34-92 months in patients with MPM who have undergone CRS-HIPEC [8,15,21,22,23,24,25]. The aim of CRS is to achieve complete cytoreduction and this usually requires multivisceral resections. The resection of ≥ 5 major organs or the creation of ≥ 3 intestinal anastomoses are considered eCRS. The potential morbidity and mortality associated with complex organ resections during eCRS discourage many surgeons. On the other hand, there is limited evidence on the impact of eCRS on survival due to the small number of studies. In this study, we aimed to present to investigate the impact of eCRS on survival and peri-postoperative outcomes in patients who underwent CRS-HIPEC diagnosed with MPM.
In one of the first studies of eCRS, Berger et al. retrospectively studied 269 patients who underwent CRS-HIPEC with a diagnosis of peritoneal carcinomatosis originating from different primers [26]. Complete cytoreduction was achieved in 76% of patients. eCRS-HIPEC was performed in 50 patients diagnosed with colorectal carcinoma, adenocarcinoma of the appendix, gastric carcinoma, low-grade neoplasm of the appendix, ovarian carcinoma, adenocarcinoma of the small bowel, and cholangiocarcinoma (17, 20, 6, 3, 2, and 1 patient, respectively). As a result, longer operative time, longer LOHS days, longer ICU LOS days, higher EBL, and more frequent complication rates were observed in the eCRS group. Survival was lower in the eCRS group [26]. However, when evaluating the survival results of this study [26], it should be kept in mind that these were patients with different primary diagnoses and not patients with MPM. We did not find any study using eCRS in patients with MPM in the literature. On the other hand, although there is no eCRS, the study by Roife et al. on the concept of "multiorgan resection" in patients with MPM attracts attention. They included 174 patients who underwent CRS-HIPEC for MPM [10]. Multiorgan resection was categorized as 0, 1, or 2+ organs (94, 45, and 35 patients, respectively). They achieved complete cytoreduction in 117 patients. Similar to Berger et al., ICU LOS, LOHS, operative time, and EBL were higher in the group that underwent more aggressive surgery. However, these variables were not shown to affect survival. It is not surprising that ICU LOS days, total LOS, operative time, and EBL are higher after such complex operations. Our results are similar, and these variables have not affected survival. In addition, similar to Berger et al., the complication rate increases with the width of the surgery, but there was no difference in the complication frequency of Clavien Dindo 3-4 (Table 3-5). This may be considered a reason for the long hospital stay in patients undergoing eCRS, but it has no impact on survival. It is undisputable that an experienced team is required to perform surgery safely in patients requiring eCRS.
Many studies have been performed on prognostic factors in patients with MPM. Poor prognostic factors include CC -score > 1, sarcomatoid or biphasic subtype, lymph node involvement, Ki67 > 9%, and PCI > 177. Yan et al., in a study that included 294 patients with MPM and achieved complete cytoreduction in 139 patients, found that high PCI, histopathologic subtype, and high CC score were associated with prognosis [32]. Kusamura et al. studied 117 patients with MPM in another study examining prognostic factors. Complete cytoreduction was achieved in 94 of the patients. As a result, they defined PCI > 17 and Ki-67 > 9% as poor prognostic factors [33]. All our patients were MPM of epithelioid type, and complete cytoreduction (CC 0-1) was achieved in all patients. In our study, the median PCI was calculated as 26 in the eCRS group and 17 in the leCRS group, and a statistically significant difference was found. However, there was no significant difference in patient survival. We believe this is related to the fact that complete cytoreduction was achieved in all patients included in the study. On the other hand, the median PCI was at the poor prognostic level defined by Kusamura et al., even in the leCRS group, suggesting that our patient group consists of advanced-stage patients [33].
One of the most influential factors for survival is the residual disease. Therefore, achieving complete cytoreduction is crucial. When complete cytoreduction cannot be achieved in MPM, outcomes are worse than in patients with complete cytoreduction because the benefit of systemic therapy to patients is limited. Even if multiorgan involvement is detected during CRS, eCRS can be applied in suitable patients. In this way, equal survival rates can be achieved in patients with high and low PCI.
Retrospective and single-center design, relatively small number of patients can be considered as limitations. On the other hand, the fact that all of the patients achieved complete cytoreduction, none of them had received chemotherapy before surgery, and that all of them were epithelioid type MPM show that our patient group is homogeneous. In addition, the lack of similar studies of MPM in the literature makes our results valuable.
5. Conclusions
In patients with MPM, in cases of high PCI and multiorgan involvement, eCRS is a suitable option if complete cytoreduction can be achieved. Complications and morbidity rates in patients undergoing eCRS are similar to leCRS. In case of high PCI and multiorgan involvement, the application of eCRS in selected MPM patients can provide equal survival to patients with low PCI.
Author Contributions
Conceptualization, M.M and U.K.; methodology, M.M.; K.K; software, M.M; K.K; T.E.S; M.E.B;K.K; validation, M.M, K.K. and M.E.B.; formal analysis, M.M; U.K.; K.K; investigation, M.M; K.K; T.E.S; M.E.B; K.K; resources, M.M; U.K; and K.K; data curation, M; K.K; T.E.S; M.E.B and K.K; writing—original draft preparation, M.M; K.K; T.E.S; M.E.B;K.K; writing—review and editing, M.M; U.K and K.K;.; visualization, M.M; U.K; T.E.S; M.E.B; supervision, M.M; K.K; project administration, M.M.; K.K; funding acquisition, M.M; K.K; T.E.S; M.E.B;K.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee Sivas Cumhuriyet University (protocol code 03/25 - 2022).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lurvink, R.J.; Villeneuve, L.; Govaerts, K.; de Hingh, I.; Moran, B.J.; Deraco, M.; Van der Speeten, K.; Glehen, O.; Kepenekian, V.; Kusamura, S. The Delphi and GRADE Methodology Used in the PSOGI 2018 Consensus Statement On Pseudomyxoma Peritonei And Peritoneal Mesothelioma. Eur. J. Surg. oncol. 2021, 47, 4–10. [Google Scholar] [CrossRef]
- Hiriart, E.; Deepe, R.; Wessels, A. Mesothelium and Malignant Mesothelioma. J. Dev. Biol. 2019, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Moolgavkar, S.H.; Meza, R.; Turim, J. Pleural and Peritoneal Mesotheliomas in SEER: Age Effects And Temporal Trends, 1973-2005. Cancer causes & control. 2009, 20, 935–944. [Google Scholar]
- Henley, S.J.; Larson, T.C.; Wu, M.; Antao, V.C.; Lewis, M.; Pinheiro, G.A.; et al. Mesothelioma incidence in 50 states and the District of Columbia, United States, 2003-2008. International journal of occupational and environmental health. 2013, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Price, B.; Ware, A. Time Trend of Mesothelioma Incidence in The United States and Projection of Future Cases: An Update Based On SEER Data for 1973 Through 2005. Crit. Rev. Toxicol. 2009, 39, 576–588. [Google Scholar] [CrossRef]
- Neumann, V.; Löseke, S.; Nowak, D.; Herth, F.J.; Tannapfel, A. Malignant Pleural Mesothelioma: Incidence, Etiology, Diagnosis, Treatment, And Occupational Health. Dtsch Arztebl Int. 2013, 110, 319–326. [Google Scholar] [PubMed]
- Kusamura, S.; Kepenekian, V.; Villeneuve, L.; Lurvink, R.J.; Govaerts, K.; De Hingh, I.H.J.T.; Moran, B.J.; Van der Speeten, K.; Deraco, M.; Glehen, O.; PSOGI. Peritoneal mesothelioma: PSOGI/EURACAN Clinical Practice Guidelines For Diagnosis, Treatment And Follow-Up. Eur J Surg Oncol. 2021, 47, 36–59. [Google Scholar] [CrossRef]
- Manzini, V.P.; Recchia, L.; Cafferata, M.; Porta, C.; Siena, S.; Giannetta, L.; Morelli, F.; Oniga, F.; Bearz, A.; Torri, V.; Cinquini, M. Malignant Peritoneal Mesothelioma: A Multicenter Study On 81 Cases. Ann Oncol. 2010, 21, 348–353. [Google Scholar] [CrossRef]
- Chua, T.C.; Yan, T.D.; Morris, D.L. Outcomes of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Mesothelioma: The Australian Experience. J. surg. Oncol. 2009, 99, 109–113. [Google Scholar] [CrossRef]
- Roife, D.; Powers, B.D.; Zaidi, M.Y.; Staley, C.A.; Cloyd, J.M.; Ahmed, A.; Grotz, T.; Leiting, J.; Fournier, K.; Lee, A.J.; Veerapong, J.; Baumgartner, J.M.; Clarke, C.; Patel, S.H.; Hendrix, R.J.; Lambert, L.; Abbott, D.E.; Pokrzywa, C.; Lee, B.; Blakely, A.; Greer, J.; Johnston, F.M.; Laskowitz, D.; Dessureault, S.; Dineen, S.P. CRS/HIPEC with Major Organ Resection in Peritoneal Mesothelioma Does not Impact Major Complications or Overall Survival: A Retrospective Cohort Study of the US HIPEC Collaborative. Ann.surg. oncol 2020, 27, 4996–5004. [Google Scholar] [CrossRef]
- Miura, J.T.; Johnston, F.M.; Gamblin, T.C.; Turaga, K.K. Current Trends In The Management Of Malignant Peritoneal Mesothelioma. Ann. Surg. Oncol. 2014, 21, 3947–3953. [Google Scholar] [CrossRef] [PubMed]
- eldman, A.L.; Libutti, S.K.; Pingpank, J.F.; Bartlett, D.L.; Beresnev, T.H.; Mavroukakis, S.M.; Steinberg, S.M.; Liewehr, D.J.; Kleiner, D.E.; Alexander, H.R. Analysis of Factors Associated With Outcome In Patients With Malignant Peritoneal Mesothelioma Undergoing Surgical Debulking And Intraperitoneal Chemotherapy. J Clin Oncol. 2003, 21, 4560–4567. [Google Scholar] [CrossRef]
- Turaga, K.K.; Deraco, M.; Alexander, H.R. Current Management Strategies for Peritoneal Mesothelioma. Int. J. Hyperthermia. 2017, 33, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H.; Turaga, K.K.; Alexander, H.R., Jr; Deraco, M.; Hesdorffer, M. Management of Malignant Peritoneal Mesothelioma Using Cytoreductive Surgery and Perioperative Chemotherapy. J. Oncol.Pract. 2016, 12, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.D.; Deraco, M.; Baratti, D.; Kusamura, S.; Elias, D.; Glehen, O.; Gilly, F.N.; Levine, E.A.; Shen, P.; Mohamed, F.; Moran, B.J.; Morris, D.L.; Chua, T.C.; Piso, P.; Sugarbaker, P.H. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience. J. Clin. Oncol. 2009, 27, 6237–6242. [Google Scholar] [CrossRef] [PubMed]
- Yano, H.; Moran, B.J.; Cecil, T.D.; Murphy, E.M. Cytoreductive Surgery and Intraperitoneal Chemotherapy For Peritoneal Mesothelioma. Eur. J. Surg. Oncol. 2009, 35, 980–985. [Google Scholar] [CrossRef]
- Sugarbaker, P.H.; Welch, L.S.; Mohamed, F.; Glehen, O. A Review of Peritoneal Mesothelioma at the Washington Cancer Institute. Surg Oncol Clin N Am. 2003, 12, 605–621. [Google Scholar] [CrossRef]
- Deraco, M.; Nonaka, D.; Baratti, D.; Casali, P.; Rosai, J.; Younan, R.; Salvatore, A.; Cabras, A.D.; Kusamura, S. Prognostic Analysis Of Clinicopathologic Factors In 49 Patients With Diffuse Malignant Peritoneal Mesothelioma Treated With Cytoreductive Surgery And Intraperitoneal Hyperthermic Perfusion. Ann. Surg. Oncol. 2006, 13, 229–237. [Google Scholar] [CrossRef]
- Hesdorffer, M.E.; Chabot, J.A.; Keohan, M.L.; Fountain, K.; Talbot, S.; Gabay, M.; Valentin, C.; Lee, S.M.; Taub, R.N. Combined Resection, Intraperitoneal Chemotherapy, And Whole Abdominal Radiation For The Treatment Of Malignant Peritoneal Mesothelioma. Am J Clin Oncol.. 2008, 31, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Blackham, A.U.; Shen, P.; Stewart, J.H.; Russell, G.B.; Levine, E.A. Cytoreductive Surgery With Intraperitoneal Hyperthermic Chemotherapy For Malignant Peritoneal Mesothelioma: Mitomycin Versus Cisplatin. Ann. Surg. Oncol. 2010, 17, 2720–2727. [Google Scholar] [CrossRef]
- Helm, J.H.; Miura, J.T.; Glenn, J.A.; Marcus, R.K.; Larrieux, G.; Jayakrishnan, T.T.; Donahue, A.E.; Gamblin, T.C.; Turaga, K.K.; Johnston, F.M. Cytoreductive Surgery And Hyperthermic Intraperitoneal Chemotherapy For Malignant Peritoneal Mesothelioma: A Systematic Review And Meta-Analysis. Ann. Surg. Oncol. 2015, 22, 1686–1693. [Google Scholar] [CrossRef] [PubMed]
- Jänne, P.A.; Wozniak, A.J.; Belani, C.P.; Keohan, M.L.; Ross, H.J.; Polikoff, J.A. Open-Label Study Of Pemetrexed Alone Or In Combination With Cisplatin For The Treatment Of Patients With Peritoneal Mesothelioma: Outcomes Of An Expanded Access Program. Clin. llung. cancer. 2005, 7, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Carteni, G.; Manegold, C.; Garcia, G.M.; Siena, S.; Zielinski, C.C.; Amadori, D.; Liu, Y.; Blatter, J.; Visseren-Grul, C.; Stahel, R. Malignant Peritoneal Mesothelioma-Results From The International Expanded Access Program Using Pemetrexed Alone Or In Combination With A Platinum Agent. Lung Cancer. 2009, 64, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Deraco, M.; Baratti, D.; Hutanu, I.; Bertuli, R.; Kusamura, S. The Role Of Perioperative Systemic Chemotherapy In Diffuse Malignant Peritoneal Mesothelioma Patients Treated With Cytoreductive Surgery And Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2013, 20, 1093–1100. [Google Scholar] [CrossRef]
- Alexander, H.R., Jr; Bartlett, D.L.; Pingpank, J.F.; Libutti, S.K.; Royal, R.; Hughes, M.S.; Holtzman, M.; Hanna, N.; Turner, K.; Beresneva, T.; Zhu, Y. Treatment factors associated with long-term survival after cytoreductive surgery and regional chemotherapy for patients with malignant peritoneal mesothelioma. Surgery. 2013, 153, 779–786. [Google Scholar] [CrossRef]
- Berger, Y.; Aycart, S.; Mandeli, J.P.; Heskel, M.; Sarpel, U.; Labow, D.M. Extreme Cytoreductive Surgery And Hyperthermic Intraperitoneal Chemotherapy: Outcomes From A Single Tertiary Center. Surg Oncol. 2015, 24, 264–269. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; Graf, R.; Vonlanthen, R.; Padbury, R.; Cameron, J.L.; Makuuchi, M. The Clavien-Dindo Classification Of Surgical Complications: Five-Year Experience. Ann Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical Research Methodologies In Diagnosis And Staging Of Patients With Peritoneal Carcinomatosis. Cancer Res Treat. 1996, 82, 359–374. [Google Scholar]
- Sugarbaker, P.H. Management Of Peritoneal-Surface Malignancy: The Surgeon's Role. Langenbecks Arch Surg. 1999, 384, 576–587. [Google Scholar] [CrossRef]
- Sugarbaker, P.H.; Yan, T.D.; Stuart, O.A.; Yoo, D. Comprehensive Management Of Diffuse Malignant Peritoneal Mesothelioma. Eur. J. Surg. Oncol. 2006, 32, 686–691. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritonectomy Procedures. Ann.Surg. 1995, 221, 29–42. [Google Scholar] [CrossRef]
- Yan, T.D.; Deraco, M.; Elias, D.; Glehen, O.; Levine, E.A.; Moran, B.J.; Morris, D.L.; Chua, T.C.; Piso, P.; Sugarbaker, P.H. A Novel Tumor-Node-Metastasis (TNM) Staging System Of Diffuse Malignant Peritoneal Mesothelioma Using Outcome Analysis Of A Multi-Institutional Database. Cancer. 2011, 117, 1855–1863. [Google Scholar] [CrossRef]
- Kusamura, S.; Torres Mesa, PA.; Cabras, A.; Baratti, D.; Deraco, M. The Role of Ki-67 and Pre-cytoreduction Parameters in Selecting Diffuse Malignant Peritoneal Mesothelioma (DMPM) Patients for Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). Ann. Surg. Oncol. 2016, 23, 1468–1473. [Google Scholar] [CrossRef]
Figure 1A.
Extreme Cytoreductıon.
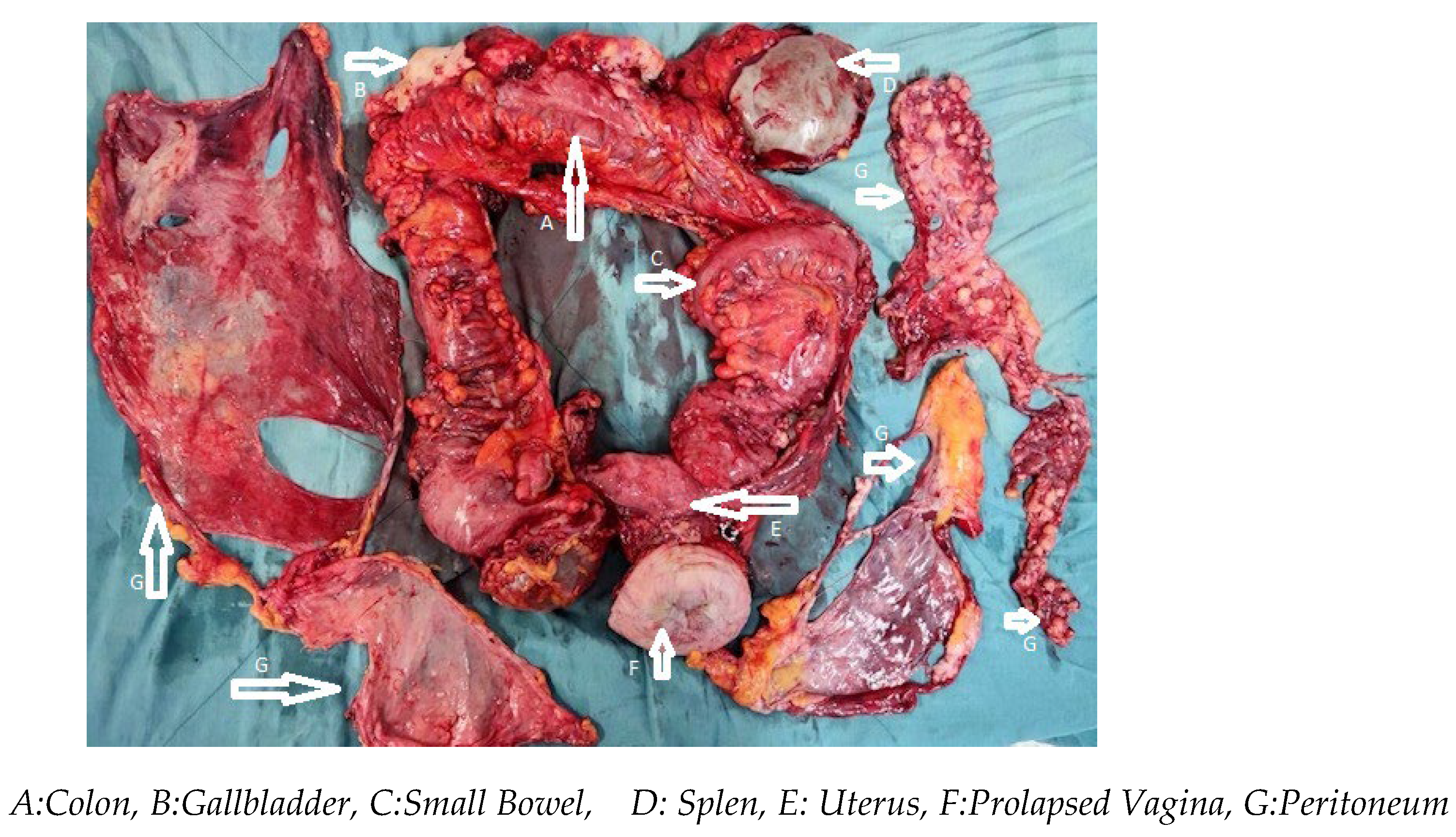

Table 1.
Frequency distributions and descriptive statistics of variables (n:31).
| Variables | n | % |
|---|---|---|
| Surgical Procedure | ||
| Extreme CRS | 15 | 48.4 |
| Less Extensive CRS | 16 | 51.6 |
| Gender | ||
| Female | 14 | 45.2 |
| Male | 17 | 54.8 |
| Complications | ||
| No | 19 | 61.3 |
| Yes | 12 | 38.7 |
| CC Score | ||
| 0 | 13 | 41.9 |
| 1 | 18 | 58.1 |
| Asbest Exposure | ||
| No | 8 | 25.8 |
| Yes | 23 | 74.2 |
| Prior Abdominal Surgery | ||
| No | 21 | 67.7 |
| Yes | 10 | 32.3 |
| ASA Class | ||
| 2 | 8 | 25.8 |
| 3 | 17 | 54.8 |
| 4 | 6 | 19.4 |
| Reoperation | ||
| No | 26 | 83.9 |
| Yes | 5 | 16.1 |
| Readmission | ||
| No | 24 | 77.4 |
| Yes | 7 | 22.6 |
| Clavien Dindo 3-4 Complications | ||
| No | 24 | 77.4 |
| Yes | 7 | 22.6 |
| Mean± S.D | Median (min - max) | |
| Age | 62.55 ± 7.24 | 64 (45 - 78) |
| PCI | 20.68 ± 5.49 | 21 (12 - 30) |
| LOHS (days) | 13.74 ± 3.74 | 14 (7 - 21) |
| Survival (months) | 35.03 ± 12.23 | 40 (5 - 60) |
| EBL (ml) | 335.32 ± 102.43 | 300 (200 - 550) |
| BMI | 28.1 ± 2.72 | 27 (25 - 33) |
| Operative Time (hours) | 6.84 ± 1.24 | 7 (4.5 - 10) |
| ICU LOS (days) | 2.52 ± 1.03 | 3 (1 - 4) |
CRS:Cytoreductive Surgery, ASA : American Society of Anesthesiologists, PCI: Peritoneal Cancer Index, LOHS: Length of Hospital Stay, EBL: Estimated Blood Loss, BMI: Body Mass Index, ICU: Intensive Care Unit, LOS: Length of Stay.
Table 2.
Frequency of organ resection in patients with malignant peritoneal mesothelioma extreme CRS.
Table 2.
Frequency of organ resection in patients with malignant peritoneal mesothelioma extreme CRS.
| Organ resected | Number of patients (%) |
|---|---|
| Colon | 14(19.4) |
| Small bowel | 13 (18.0) |
| Spleen | 10 (13.8) |
| Gallbladder | 8 (11.1) |
| Uterus/vagen/over | 6 (8.3) |
| Stomach | 6(8.3) |
| Diaphragm | 5 (6.9) |
| Left | 3(4.1) |
| Right | 2(2.7) |
| Rectum | 4(5.5) |
| Pancreas | 4(5.5) |
| Liver | 2(2.7) |
Table 3.
Comparison of categorical variables by groups.
| Group | Total | Statistic tests | p | ||
|---|---|---|---|---|---|
| eCRS | leCRS | ||||
| Gender | |||||
| Female | 6 (40) | 8 (50) | 14 (45.2) | 0.039 | 0.843** |
| Male | 9 (60) | 8 (50) | 17 (54.8) | ||
| Complications | |||||
| No | 6 (40) | 13 (81.2) | 19 (61.3) | 3.95 | 0.047** |
| Yes | 9 (60) | 3 (18.8) | 12 (38.7) | ||
| CC Score | |||||
| 0 | 7 (46.7) | 6 (37.5) | 13 (41.9) | 0.023 | 0.879** |
| 1 | 8 (53.3) | 10 (62.5) | 18 (58.1) | ||
| Asbest.exposure | |||||
| No | 3 (20) | 5 (31.3) | 8 (25.8) | --- | 0.685*** |
| Yes | 12 (80) | 11 (68.8) | 23 (74.2) | ||
| Prior Abdominal Surgery | |||||
| No | 8 (53.3) | 13 (8.,3) | 21 (67.7) | --- | 0.135*** |
| Yes | 7 (46.7) | 3 (18.8) | 10 (32.3) | ||
| ASA class | |||||
| Sınıf 2 | 2 (13.3) | 6 (37.5) | 8 (25.8) | 4.698 | 0.095* |
| Sınıf 3 | 8 (53.3) | 9 (56.3) | 17 (54.8) | ||
| Sınıf 4 | 5 (33.3) | 1 (6.3) | 6 (19.4) | ||
| Reoperation | |||||
| No | 13 (0.87) | 13 (0.81) | 26 (0.84) | --- | 1.000*** |
| Yes | 2 (0.13) | 3 (0.19) | 5 (0.16) | ||
| Readmission | |||||
| No | 12 (80) | 12 (75) | 24 (77.4) | --- | 1.000*** |
| Yes | 3 (20) | 4 (25) | 7 (22.6) | ||
| Clavien Dindo 3-4 Complications | |||||
| No | 12 (80) | 12 (75) | 24 (77.4) | --- | 1.000*** |
| Yes | 3 (20) | 4 (25) | 7 (22.6) | ||
* The Pearson Chi-Square Test; ** Yates Correction;*** Fisher's Exact Test; Frequency (Percentage) CC: Completeness of Cytoreduction, ASA : American Society of Anesthesiologists.
Table 4.
Comparison of quantitative variables by groups.
| Grup | St.Test | p | ||||||
|---|---|---|---|---|---|---|---|---|
| e CRS +HIPEC+EPIC | le Procedure | Total | ||||||
| Mean ± SD | Mean (min - max) | Mean ± SD | Mean (min - max) | Mean ± SD | Mean (min - max) | |||
| Age | 60.27 ± 9.18 | 60 (45 - 78) | 64.69 ± 4.01 | 65 (58 - 71) | 62.55 ± 7.24 | 64 (45 - 78) | -1.717 | 0.102* |
| PCI | 25.27 ± 3.03 | 26 (21 - 30) | 16.38 ± 3.28 | 17 (12 - 24) | 20.68 ± 5.49 | 21 (12 - 30) | 7.814 | <0.001* |
| LOHS (days) | 16.13 ± 2.8 | 15 (13 - 21) | 11.5 ± 3.1 | 11.5 (7 - 18) | 13.74 ± 3.74 | 14 (7 - 21) | 27 | <0.001** |
| Survival (months) | 34.47 ± 11.7 | 40 (5 - 49) | 35.56 ± 13.06 | 39.5 (5 - 60) | 35.03 ± 12.23 | 40 (5 - 60) | -0.245 | 0.808* |
| EBL (ml) | 398.67 ± 100.84 | 400 (250 - 550) | 275.94 ± 60.97 | 272.5 (200 - 400) | 335.32 ± 102.43 | 300 (200 - 550) | 4.068 | <0.001* |
| BMI | 26.47 ± 1.81 | 26 (25 - 32) | 29.63 ± 2.58 | 29 (25 - 33) | 28.1 ± 2.72 | 27 (25 - 33) | 35 | <0.001** |
| Operative Time (hours) | 7.6 ± 1.03 | 7.45 (6,15 - 10) | 6.13 ± 0.99 | 6 (4.5 - 8) | 6.84 ± 1.24 | 7 (4.5 - 10) | 4.042 | <0.001* |
| ICU LOS ( days) | 3.2 ± 0.68 | 3 (2 - 4) | 1.88 ± 0.89 | 2 (1 - 4) | 2.52 ± 1.03 | 3 (1 - 4) | 31.5 | <0.001** |
* The Independent Samples T-Test; ** Mann-Whitney U Test; Mean ± Standard Deviation; Median (Minimum-Maximum). PCI : Peritoneal Cancer Index, LOHS: Length of Hospital Stay, EBL: Estimated Blood Loss, BMI: Body Mass Index, ICU: Intensive Care Unit, LOS: Length of Stay.
Table 5.
Investigation of the influence of independent variables on survival with cox regression analysis.
Table 5.
Investigation of the influence of independent variables on survival with cox regression analysis.
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (%95 CI) | p | HR (%95 CI) | p | |
| Age | 0.932 (0.856 – 1.015) | 0.105 | ||
| PCI | 1.034 (0.942 – 1.136) | 0.483 | 0.767 (0.558 – 1.056) | 0.104 |
| LOHS (days) | 1.033 (0.906 – 1.176) | 0.630 | 1.516 (0.993 – 2.313) | 0.054 |
| EBL (ml) | 0.999 (0.995 – 1.004) | 0.786 | ||
| BMI | 0.921 (0.76 – 1.116) | 0.401 | ||
| Operative Time (hours) | 1.061 (0.702 – 1.603) | 0.778 | 0.616 (0.176 – 2.151) | 0.447 |
| ICU LOS (days) | 1.039 (0.655 – 1.646) | 0.872 | ||
CC: Completeness of Cytoreduction, ASA : American Society of Anesthesiologists, ASA : American Society of Anesthesiologists, PCI : Peritoneal Cancer Index, LOHS: Length Of Hospital Stay, EBL: Estimated Blood Loss, BMI: Body Mass Index, ICU: Intensive Care Unit, LOS: Length of Stay.
Table 6.
Comparison of survival times by groups.
| Means (%95 CI) | p | |
|---|---|---|
| eCRS | 37.5 (30.6 – 44.4) | 0.895 |
| le CRS | 42.8 (33.7 – 51.8) | |
| Overall | 43.0 (36.5 – 49.6) |
Log Rank Test , CRS: Cytoreductive Surgery
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



