
Submitted:
14 September 2023
Posted:
22 September 2023
You are already at the latest version
Abstract
Background: The current review was conducted to determine the effectiveness of atenolol on all-cause mortality rate among Asian patients with chronic progressive diseases, mainly diabetes mellitus, primary hypertension, and coronary artery disease.
Methods: We searched the COCHRANE, MEDLINE, TRIP, and EMBASE databases for published articles up to 31 March 2023. Studies that compared all-cause mortality rates among Asian patients who were on atenolol or other medications were included.
Results: The review included 79603 Asian patients from three cohort studies. Out of the studied patients, 36046 were atenolol users and 43557 were non-atenolol users. The review revealed that atenolol users recorded lower all-cause mortality rates compared to non-users with a significant difference (OR= 0.57, CI= 0.44-0.75, P<0.001). The pooled estimate of the all-cause mortality rate was also lower among atenolol users (7.02%) compared to metoprolol tartrate users (13.15%) with a significant difference (OR= 0.50, CI= 0.47-0.53, p < 0.0001). Although the included studies were categorized as having a low risk of bias for most of the studied domains, significant heterogeneity was recorded across these studies (I2 =88%, P=0.001).
Conclusion: This review found that atenolol when compared to a control or metoprolol tartrate, has a significant effect in reducing the all-cause mortality rate among Asian patients with chronic progressive disease.
Keywords:
Atenolol
; mortality
; Asians
; chronic progressive disease
; cardiovascular disease
Key points
- -
- The study included 79,603 Asian patients with chronic progressive diseases.
- -
- Patients using atenolol had lower all-cause mortality rates compared to non-users with a significant difference.
- -
- All-cause mortality rate was also lower among atenolol users compared to metoprolol tartrate users with a significant difference.
1. Introduction
Patients with cardiovascular diseases (CVDs) are encouraged to use drugs such as beta-blockers along with other medications to reduce all-cause and cardiovascular morbidity and mortality. Beta-blockers are not only recommended for this group of patients, but are also recommended as a first-line treatment for hypertensive patients with cardiovascular disease (i.e., heart failure and coronary artery disease) [1]. Furthermore, despite controversies, beta-blocker agents are recommended to reduce all-cause mortality in patients undergoing non-cardiac surgery and who have two or more of specific diseases, including coronary artery disease, diabetes mellitus, renal insufficiency, and cerebrovascular disease [2,3].
Several studies had evaluated beta-blocker agents and made comparisons between them regarding the effectiveness of reducing all-cause death of patients with chronic diseases. Assimon et al. showed that carvedilol, when compared to metoprolol, is associated with 1.08 fold higher rates of all-cause mortality among patients with end stage renal disease (ESRD) [4]. In another study conducted among patients with the same chronic disease (ESRD), Wu et al. revealed that bisoprolol was significantly associated with lower rates of all-cause mortality than carvedilol [5]. Among patients with ventricular tachyarrhythmia, Schupp et al. found that the all-cause mortality rate was not significantly lower in metoprolol users compared to carvedilol [6]. With no significant difference, all-cause mortality rate among patients with advanced stages of heart failure was higher among nebivolol users than bisoprolol [7]. In the study conducted by Shin et al., it was found that mortality rate was higher among atenolol users than bisorpolol, however, no significant difference was detected [8].
According to the American Heart Association (AHA) guidelines, atenolol is one of the beta-blocker agents that should be not be used for patients diagnosed with stable ischemic heart disease (SIHR) [9]. This recommendation is based on numerous studies that investigated the risk of cardiovascular event among Caucasian patients who used 25-100 mg of atenolol once daily [10].
Dosing potency and frequency of atenolol and pharmacokinetic interactions are some of the reasons behind the recommendations made against the use of atenolol. Some studies found that an atenolol dose ranging from 100 to 200 mg per day was more effective that 25 and 50 mg doses per day in patients with angina [11,12].
Furthermore, specific gene mutations, which could be dominant in some ethnic groups, can affect the responsiveness of atenolol. For instance, gene polymorphisms related to TBX2 and GNB3 genes significantly reduce the antihypertensive effect of atenolol [13,14]. Moreover, the rs3213619 and rs2144300 alleles related to ABCB1 and GALNT2 genes, have respectively been found to be significantly associated with lower levels of high-density lipoprotein cholesterol (HDL-C) [15]. The TBX2 mutation that is related to abnormal efficacy of atenolol is commonly found in over 69% of Finish, non-Finish European, Amish, and Ashkenazi Jewish ethnic groups. However, this mutation is less detected among African, African American, and Asians [16]. Similarly, the rs2144300 allele related to GALNT2 gene is carried by no more than 21% of Asians Africans, and African-Americans, while more than 60% of non-Finish Europeans are carriers of this mutated allele [17].
Rationale
This justifies the exclusion of Asians, Africans, African-Americans from the AHA recommendations against the use of atenolol, and may point to atenolol’s benefit in reducing all-cause mortality in these ethnic groups.
Objectives
The current study was conducted to determine the effectiveness of atenolol on reducing all-cause mortality rate among Asian patients with chronic progressive disease, mainly diabetes mellitus, primary hypertension, and coronary artery disease.
2. Materials and methods
Eligibility criteria and information sources
The review included cohort studies in the English language. The studies compared the effect of atenolol versus other beta-blockers and non-beta-blockers on the overall all-cause-mortality in Asian patients diagnosed with chronic progressive diseases. We excluded studies that that included non-Asian patients, non-Asian patients using Atenolol, Asian patients without chronic diseases, and Asian patients on other antihypertensive drugs. In addition, studies that met the inclusion criteria but did not mention the number of atenolol users were also excluded.
Search strategy and selection process
We searched the Cochrane, Trip, EMBASE, and Google Scholar databases up to 31 March 2023. In addition, we reviewed the reference lists of the selected articles for further studies. We used the following terms in the search: Atenolol, OR Beta-blockers, AND Asians, OR Chinese, OR Korean, OR Taiwanese, OR Japanese, OR Vietnamese, OR Mongols, OR Thais, OR Cambodians, OR Indonesians, OR Malays, OR Bengalis, OR Nepalese, OR Pakistanis, OR Singaporeans, OR Burmese, OR Filipinos, OR Indians, AND Angina, OR Ischemic heart disease, OR Ischemia, OR Myocardial infarction, AND All-cause mortality.
Data Collection and Extraction
Two authors independently reviewed the abstracts of the screened articles. Eligible articles were acquired and their characteristics were extracted. Any disagreements between the authors were resolved by discussion.
Data items
The primary outcome measure was all-cause mortality rate among atenolol users and non-users. The secondary outcome measure was all-cause mortality rate among atenolol users versus metoprolol tartrate users.
Assessment of risk of bias
The risk of bias among the included studies was graded as high, low, or unclear, as recommended by The Newcastle Ottawa Scale for cohort studies [18]. The scale defines the following domains: 1) Selective reporting (reporting bias), 2) Adequate case definition (selection bias), 3) Consecutive representativeness of cases (selection bias), 4) Selection of community controls (selection bias), 5) Adequate control definition (selection bias), 6) Independent blind assessment of outcome (selection bias), 7) All subjects complete follow up period.
Effect measures and synthesis method
Review Manager version 5.3 was utilized for data analysis using a random effect model. The results were reported as Odds Ratios (OR) with 95% confidence intervals (CI).
Certainty assessment
The quality of outcome measures was classified into high, moderate, low, or very low according to the GRADE approach [19] and based on study limitations; namely, the risk of bias in each study, the directness of the evidence, consistency across studies, and precision of the pooled estimate.
Dealing with Heterogeneity
I2 test was used to test the heterogeneity across the included studies [20].
3. Results
Study selection
Out of 380 searched studies, 174 remained after removing duplicates. After excluding non-relevant manuscripts during the screening stage, 108 articles were evaluated for eligibility. Only three studies met our inclusion criteria. The details of the search are explained in PRISMA flow diagram (Figure 1).
Study characteristics
Results of individual studies
The review included 79,865 Asian patients, out of whom 36046 were atenolol users and 43,819 non-atenolol users. Patients were above 46 years of age. In the study conducted by Wongpraparut et al., all the patients had a history of cardiovascular diseases, while all patients included by Chen et al. and Wong et al. had diabetes and hypertension, respectively [21,22,23]. Furthermore, 68.5% (N=30,001) of the patients in the non-atenolol group used metoprolol tartrate [21,23], while, other non-atenolol users (31.5%) used carvedilol, metoprolol succinate, nebivolol, bisoprolol, and propranolol beta-blockers (N=262) [23] or non-beta-blocker agents (N=13,556) [22].
Risk of bias among the included studies including reporting bias
Overall, the included studies recorded a low risk of bias for most of the studied domains and no high risk of bias was recorded for any aspect. Reporting bias was recorded low risk of bias among the studied three articles. However, some unclear risk of bias regarding specific aspects were determined in the three included articles (selection of community controls, adequate definition of controls, and complete follow-up period aspects in the Wongpraparut et al. study; adequate definition of controls, blind assessment of outcome, and complete follow-up period aspects in the Wong et al. study; independent blind assessment of outcome aspect in Chen et al. study) (Figure 2).
Results of syntheses
Figure 3 shows a forest plot of the all-cause mortality rate among 36,046 atenolol users and 43,819 non-users from the three included studies. The pooled estimate of the all-cause mortality rate was lower among atenolol users (5.57%) compared to non-users (10.50%) with a significant difference (OR= 0.58, CI= 0.44-0.76, p < 0.0001). However, a considerable significant heterogeneity was recorded across the analysis (I2 =88%, p < 0.001).
For the secondary outcome, Figure 4 revealed a forest plot of the all-cause mortality rate among 22,490 atenolol users and 30,001 metoprolol tartrate users from two of the three included studies [21,23]. The pooled estimate of the all-cause mortality rate was also lower among atenolol users (7.02%) compared to metoprolol tartrate users (13.15%) with a significant difference (OR= 0.50, CI= 0.47-0.53, p < 0.0001) with insignificant heterogeneity (I2 =0%, p = 0.97).
Certainty of evidence
Overall, the surveyed studies were primarily observational with low risk of bias, which downgraded the quality of evidence for each outcome measure by one level. However, directness was not an issue, as all studies recorded the same outcome measures. Regarding the pooled estimate, the all-cause mortality rate among atenolol users compared to non-users, we judged the quality of evidence to be low. We downgraded the evidence by two levels due to the observational design of the included studies and the significant considerable heterogeneity (I2 = 88%). Whereas, insignificant heterogeneity was reported in the analysis of the all-causes mortality rate among atenolol users compared to metoprolol tartrate users. Thus, we judged the quality of evidence for this outcome to be moderate. We downgraded the evidence by one level only duo to the observational design of the included studies
4. Discussion
In recent years, few studies have focused on atenolol, whereas newer beta-blocker drugs are being well studied using advanced research methods and materials and conducted among various ethnic groups [24,25,26,27]. Thus, only three studies were included in the current review, which aimed to focus on the effectiveness of atenolol in reducing all-cause-mortality among Asians diagnosed with chronic progressive diseases, including diabetes mellitus, primary hypertension, and coronary artery disease. The outcomes showed that atenolol was more effective in reducing all-cause mortality compared to non-atenolol drugs, including metoprolol tartrate.
These results contradicted with Carlberg et al. who found that atenolol was not inferior to no treatment in reducing all-cause mortality [28]. Besides, Carlberg et al. did not analyze studies that compared atenolol with other beta-blockers regrading all-cause mortality [28]. Accordingly, atenolol should still be recognized as one of the suitable beta-blocker drugs in treatment options. Furthermore, the 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization did not differentiate between beta-blocker agents when treating certain medical conditions, yet, it may recommend using some particular beta-blockers for patients carrying specific genetic variants [29]. In the same line, won et al. showed that all-cause mortality was reduced among Asians with acute myocardial infarction using any beta-blocker drug compared to non-users [30].
Hung et al. compared patients using atenolol or nebivolol, a recent beta-blocker agent, regarding the progression of coronary artery disease. Their study revealed no significant differences in the endothelial function, oxidative stress biomarkers, and coronary plaque volumetric between nebivolol and atenolol users. Moreover, hung et al. showed that some particular factors among patients (e.g., wall shear stress of arteries) can significantly affect plaque progression and coronary artery disease prognosis regardless of the type of beta-blocker drug used [31]. The studies concluded that specific beta-blockers were more effective in reducing all-cause-mortality than other beta-blocker agents, however this interpretation could be limited due to the lack of ideal group matching.
During the last three decades, several studies and reviews warned that atenolol not increase survival rate compared to placebo and may associate with higher all-cause mortality rate compared to other drugs agents such as amlodipine, losartan, and metoprolol [28,32,33,34,35]. Yet, the vast majority of those studies and reviews were concerned on patients belonged to non-Asian ethnic groups [28,32,33,34,35].
As known, ethnicity and culture-related lifestyle, which cannot be overlooked, are some factors may affect the prognosis of numerous chronic diseases [36,37]. Besides, pharmacogenomics is described as a substantial tool during the treatment phases of numerous chronic progressive diseases, which could help in adjusting drugs’ doses or finding suitable alternative treatment options [38,39]. There are various gene polymorphisms associated with treatment failure. For instance, calcium channel blockers (CCB), such as amlodipine, might be more effective in reducing blood pressure among Asians than Europeans and Africans [40,41]. This better efficacy is due to the high prevalence of rs588076 allele related to PICALM gene among Eastern Asians (32.4%) and South Asians (26.7%), while found in 19.7% and 13.2% of the Europeans and Africans, respectively [41].
In the same line, atenolol would provide better blood pressure control in Eastern Asians than Europeans, Africans, and Latinos when we concern, for example, about the frequencies of three gene polymorphisms (ALDH1A2 rs261316 [42,43], EDN1 rs5370 [44,45], and ZMAT4 rs1367094 [46,47]) among the abovementioned ethnic groups.
According, and based on the current study results, we suggest revising the recommendation regarding the use of atenolol for patients with SIHR as it should be specific for some ethnic groups [9]. Besides, we encourage the researchers to conduct clinical trials on all-cause mortality using data belong to an adequate number of patients originating from various ethnic groups.
In summary, this review found that atenolol, when compared to a control or metoprolol tartrate, has a significant effect in reducing the all-cause mortality rate among Asian patients with chronic progressive diseases. Further systematic reviews and meta-analysis with low heterogeneity and high quality of evidence are recommended to support our results and to investigate the effectiveness of atenolol in different ethnic groups.
Potential bias encountered during the review process
It is unlikely that bias introduced in this systematic review, as we systematically searched the major database for eligible articles. In addition, two authors conducted the screening and data extraction independently.
Registration and protocol
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline and registered through International Prospective Register of Systematic Reviews (PROSPERO) under the registration number: CRD42023413623.
Author Contributions
AK and NR contributed in conceptualization and extracted the study characteristics and judged the risk of bias among included studies. AK, EA and AH contributed in writing—original draft preparation. MNF, HQ, NM, AF, and MK contributed in writing—review and editing. AK, NR, HQ, NM, MAF, AF, and MK contributed in resources. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any funding from any agency.
Ethical approval and consent to participate
Not applicable.
Data availability
The data that support the findings of this study were derived from the following resources available in scientific journals:
- -
- Wong MC, Tam WW, Lao XQ, Wang HH, Kwan MW, Cheung CS, Tong EL, Cheung NT, Yan BP, Yu CM, Griffiths SM. The effectiveness of metoprolol versus atenolol on prevention of all-cause and cardiovascular mortality in a large Chinese population: a cohort study. International journal of cardiology. 2014 Aug 20;175, 425-32. https://doi.org/10.1016/j.ijcard.2014.06.009
- -
- Chen RJ, Chu H, Tsai LW. Impact of Beta-Blocker Initiation Timing on Mortality Risk in Patients With Diabetes Mellitus Undergoing Noncardiac Surgery: A Nationwide Population-Based Cohort Study. Journal of the American Heart Association. 2017 Jan 10;6, e004392. https://doi.org/10.1161/JAHA.116.004392
- -
- Wongpraparut N, Siwamogsatham S, Thongsri T, Ngamjanyaporn P, Phrommintikul A, Jirajarus K, Tangcharoen T, Bhumimuang K, Kaewsuwanna P, Krittayaphong R, Pongakasira R. Impact of guideline-recommended versus non-guideline-recommended β-blocker and Doppler echocardiographic parameters on 1-year mortality in Thai ischemic cardiomyopathy patients: A prospective multicenter registry. BMC Cardiovascular Disorders. 2020 Dec;20:1-9. https://doi.org/10.1186/s12872-019-01311-4
Acknowledgment
The researchers would like to thank Dr. Yousef Almutairi (Saudi Ministry of Health, Riyadh, Saudi Arabia) for his assistance in reviewing the manuscript.
Conflicts of interest disclosure
The authors declare no conflict of interest.
Clinical trials registration number
Not applicable.
PROSPERO registration number
CRD42023413623.
Permission to reproduce material from other sources
Not applicable.
List of abbreviation
| AHA | American Heart Association |
| ACC | American College of Cardiology |
| SCAI | Society for Cardiovascular Angiography & Interventions |
| OR | Odds Ratio |
| CVDs | Cardiovascular Diseases |
| SIHR | Stable Ischemic Heart Disease |
| HDL-C | High Density Lipoprotein-Cholesterol |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| ESRD | End-Stage Renal Disease |
| GRADE | Grading of Recommendations Assessment, Development, and Evaluation |
References
- Chrysant, S.G.; Chrysant, G.S. Antihypertensive and cardioprotective effects of three generations of beta-adrenergic blockers: an historical perspective. Hospital Practice. 2022, 50, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Vivas, D.; Raposeiras, S. Comments on the ESC 2022 guidelines on cardiovascular assessment and management of patients undergoing noncardiac surgery. Revista Espanola de Cardiologia (English ed.). 2022 Nov 12:S1885-5857.
- Nan, Y.; Jia, F.; Du, X.; Mei, Z. Beta-blocker exposure for short-term outcomes following non-cardiac surgery: a meta-analysis of observational studies. International Journal of Surgery. 2020, 76, 153–162. [Google Scholar] [CrossRef]
- Assimon, M.M.; Brookhart, M.A.; Fine, J.P.; Heiss, G.; Layton, J.B.; Flythe, J.E. A comparative study of carvedilol versus metoprolol initiation and 1-year mortality among individuals receiving maintenance hemodialysis. American Journal of Kidney Diseases. 2018, 72, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Lin, Y.T.; Liu, J.S.; Tsai, Y.C.; Kuo, M.C.; Chiu, Y.W.; Hwang, S.J.; Carrero, J.J. Comparative effectiveness of bisoprolol and carvedilol among patients receiving maintenance hemodialysis. Clinical Kidney Journal. 2021, 14, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Schupp, T.; Behnes, M.; Abumayyaleh, M.; Weidner, K.; Rusnak, J.; Mashayekhi, K.; Bertsch, T.; Akin, I. Carvedilol versus Metoprolol in Patients with Ventricular Tachyarrhythmias. Journal of Cardiovascular Development and Disease. 2022, 9, 274. [Google Scholar] [CrossRef]
- AlHabeeb, W.; Mrabeti, S.; Abdelsalam, A.A. Therapeutic properties of highly selective β-blockers with or without additional vasodilator properties: focus on bisoprolol and nebivolol in patients with cardiovascular disease. Cardiovascular Drugs and Therapy. 2022, 36, 959–971. [Google Scholar] [CrossRef]
- Shin, D.H.; Kim, J.S.; Kim, B.K.; Park, S.; Lee, S.H.; Ko, Y.G.; Choi, D.; Ahn, H.A.; Joung, S.H.; Park, Y.M.; Hong, M.K. Atenolol versus Bisoprolol after Acute Myocardial Infarction.
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; MacLaughlin, E.J. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2018, 71, e127–e248. [Google Scholar]
- Aronow, W.S.; Fleg, J.L.; Pepine, C.J.; Artinian, N.T.; Bakris, G.; Brown, A.S.; Ferdinand, K.C.; Forciea, M.A.; Frishman, W.H.; Jaigobin, C.; Kostis, J.B. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension.
- Jackson, G.J.; Schwartz, J.A.; Kates, R.E.; Winchester, M.A.; Harrison, D.C. Atenolol: once-daily cardioselective beta blockade for angina pectoris. Circulation. 1980, 61, 555–560. [Google Scholar] [CrossRef]
- Schwartz, J.B.; Jackson, G.; Kates, R.E.; Harrison, D.C. Long-term benefit of cardioselective beta blockade with once-daily atenolol therapy in angina pectoris. American Heart Journal. 1981, 101, 380–385. [Google Scholar] [CrossRef]
- Iniesta, R.; Campbell, D.; Venturini, C.; Faconti, L.; Singh, S.; Irvin, M.R.; Cooper-DeHoff, R.M.; Johnson, J.A.; Turner, S.T.; Arnett, D.K.; Weale, M.E. Gene variants at loci related to blood pressure account for variation in response to antihypertensive drugs between black and white individuals: genomic precision medicine may dispense with ethnicity. Hypertension. 2019, 74, 614–622. [Google Scholar] [CrossRef]
- Filigheddu, F.; Argiolas, G.; Degortes, S.; Zaninello, R.; Frau, F.; Pitzoi, S.; Bulla, E.; Bulla, P.; Troffa, C.; Glorioso, N. Haplotypes of the adrenergic system predict the blood pressure response to β-blockers in women with essential hypertension. Pharmacogenomics. 2010, 11, 319–325. [Google Scholar] [CrossRef] [PubMed]
- McDonough, C.W.; Gillis, N.K.; Alsultan, A.; Chang, S.W.; Kawaguchi-Suzuki, M.; Lang, J.E.; Shahin, M.H.; Buford, T.W.; El Rouby, N.M.; Sá, A.C.; Langaee, T.Y. Atenolol induced HDL-C change in the pharmacogenomic evaluation of antihypertensive responses (PEAR) study. PloS one. 2013, 8, e76984. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). rs8068318 variant (TBX2 gene). Available at https://www.pharmgkb.org/variant/PA166199006. Accessed date 21 March 2023.
- Pharmacogenomics Knowledge Base (PharmGKB). rs2144300 variant (GALNT2 gene). Available at https://www.pharmgkb.org/variant/PA166153674. Accessed date 21 March 2023.
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses.
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Bmj. 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Tam, W.W.; Lao, X.Q.; Wang, H.H.; Kwan, M.W.; Cheung, C.S.; Tong, E.L.; Cheung, N.T.; Yan, B.P.; Yu, C.M.; Griffiths, S.M. The effectiveness of metoprolol versus atenolol on prevention of all-cause and cardiovascular mortality in a large Chinese population: a cohort study. International journal of cardiology. 2014, 175, 425–432. [Google Scholar] [CrossRef]
- Chen, R.J.; Chu, H.; Tsai, L.W. Impact of Beta-Blocker Initiation Timing on Mortality Risk in Patients With Diabetes Mellitus Undergoing Noncardiac Surgery: A Nationwide Population-Based Cohort Study. Journal of the American Heart Association. 2017, 6, e004392. [Google Scholar] [CrossRef]
- Wongpraparut, N.; Siwamogsatham, S.; Thongsri, T.; Ngamjanyaporn, P.; Phrommintikul, A.; Jirajarus, K.; Tangcharoen, T.; Bhumimuang, K.; Kaewsuwanna, P.; Krittayaphong, R.; Pongakasira, R. Impact of guideline-recommended versus non-guideline-recommended β-blocker and Doppler echocardiographic parameters on 1-year mortality in Thai ischemic cardiomyopathy patients: A prospective multicenter registry. BMC Cardiovascular Disorders. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Sharma, K.; Desai, H.; Sharm, N.; Laddha, M.; Hansora, K.; Vazirani, P. To Evaluate the'Real World'Clinical Performance of Bisoprolol in Post-Myocardial Infarction with Left Ventricular Dysfunction: Tenacity Study. The Journal of the Association of Physicians of India. 2022, 70, 11–12. [Google Scholar]
- Chan, S.W.; Chu, T.T.; Ho, C.S.; Kong, A.P.; Tomlinson, B.; Zeng, W. Influence of CYP2D6 and CYP3A5 Polymorphisms on the Pharmacokinetics and Pharmacodynamics of Bisoprolol in Hypertensive Chinese Patients. Frontiers in Medicine. 2021, 8, 683498. [Google Scholar] [CrossRef]
- Marques, L.; Costa, B.; Vale, N. New Data for Nebivolol after In Silico PK Study: Focus on Young Patients and Dosage Regimen. Pharmaceutics. 2022, 14, 1911. [Google Scholar] [CrossRef]
- Sabidó, M.; Thilo, H.; Guido, G. Long-term effectiveness of bisoprolol in patients with angina: a real-world evidence study. Pharmacological Research. 2019, 139, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, B.; Samuelsson, O.; Lindholm, L.H. Atenolol in hypertension: is it a wise choice? The lancet. 2004, 364, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.; Tamis-Holland, J.; Bangalore, S.; Bates, E.; Beckie, T.; Bischoff, J.; Bittl, J.; Cohen, M.; DiMaio, J.; Don, C.; Fremes, S.; Gaudino, M.; Goldberger, Z.; Grant, M.; Jaswal, J.; Kurlansky, P.; Mehran, R.; Metkus, T., Jr.; Nnacheta, L.; Rao, S.; et al. . 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef] [PubMed]
- Won, H.; Suh, Y.; Kim, G.S.; Ko, Y.G.; Hong, M.K. Clinical impact of beta blockers in patients with myocardial infarction from the Korean National Health Insurance Database. Korean Circulation Journal. 2020, 50, 499–508. [Google Scholar] [CrossRef]
- Hung, O.Y.; Molony, D.; Corban, M.T.; Rasoul-Arzrumly, E.; Maynard, C.; Eshtehardi, P.; Dhawan, S.; Timmins, L.H.; Piccinelli, M.; Ahn, S.G.; Gogas, B.D. Comprehensive Assessment of Coronary Plaque Progression With Advanced Intravascular Imaging, Physiological Measures, and Wall Shear Stress: A Pilot Double-Blinded Randomized Controlled Clinical Trial of Nebivolol Versus Atenolol in Nonobstructive Coronary Artery Disease. Journal of the American Heart Association. 2016, 5, e002764. [Google Scholar]
- The Dutch TIA Trial Study Group. Trial of secondary prevention with atenolol after transient ischemic attack or nondisabling ischemic stroke. Stroke 1993, 24, 543–548. [Google Scholar] [CrossRef]
- MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: principal results. BMJ 1992, 304, 405–412. [Google Scholar] [CrossRef]
- Dahlöf, B.; Devereux, R.B.; Kjeldsen, S.E.; et al. Cardiovascular morbidity and mortality in the losartan intervention for endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002, 359, 995–1003. [Google Scholar] [CrossRef]
- Zanchetti, A.; Bond, M.G.; Henning, M.; et al. Calcium antagonist lacidipine slows down progression of asymptomatic carotid atherosclerosis. Principal results of the European lacidipine study on atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002, 106, 2422–2427. [Google Scholar] [CrossRef]
- Ye, D.Q.; Mao, Y.M.; Wu, J.; Fang, X.Y.; Li, B.Z. Cultural Epidemiology in China. Progress in China. Epidemiology 2023, 1, 401–418. [Google Scholar]
- Jin, Y.; Bratzke, L.; Baumann, L.C. Helping persons with multiple chronic conditions overcome barriers to self-management. The Nurse Practitioner. 2021, 46, 20–28. [Google Scholar] [CrossRef] [PubMed]
- García-González, X.; Cubo, E.; Simón-Vicente, L.; Mariscal, N.; Alcaraz, R.; Aguado, L.; Rivadeneyra-Posadas, J.; Sanz-Solas, A.; Saiz-Rodríguez, M. Pharmacogenetics in the Treatment of Huntington’s Disease: Review and Future Perspectives. Journal of Personalized Medicine. 2023, 13, 385. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R. Pharmacogenetic considerations when prescribing cholinesterase inhibitors for the treatment of Alzheimer’s disease. Expert Opinion on Drug Metabolism & Toxicology. 2020, 16, 673–701. [Google Scholar]
- Kamide, K.; Asayama, K.; Katsuya, T.; Ohkubo, T.; Hirose, T.; Inoue, R.; Metoki, H.; Kikuya, M.; Obara, T.; Hanada, H.; Thijs, L. Genome-wide response to antihypertensive medication using home blood pressure measurements: a pilot study nested within the HOMED-BP study. Pharmacogenomics. 2013, 14, 1709–1721. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). rs588076 variant (PICALM gene). Available at https://www.pharmgkb.org/variant/PA166154284. Accessed date 21 March 2023.
- Magvanjav, O.; Gong, Y.; McDonough, C.W.; Chapman, A.B.; Turner, S.T.; Gums, J.G.; Bailey, K.R.; Boerwinkle, E.; Beitelshees, A.L.; Tanaka, T.; Kubo, M. Genetic Variants Associated With Uncontrolled Blood Pressure on Thiazide Diuretic/β-Blocker Combination Therapy in the PEAR (Pharmacogenomic Evaluation of Antihypertensive Responses) and INVEST (International Verapamil-SR Trandolapril Study) Trials. Journal of the American Heart Association. 2017, 6, e006522. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). rs261316 variant (ALDH1A2 gene). Available at https://www.pharmgkb.org/variant/PA166179574. Accessed date 21 March 2023.
- Hallberg, P.; Karlsson, J.; Lind, L.; Michaëlsson, K.; Kurland, L.; Kahan, T.; Malmqvist, K.; Öhman, K.P.; Nyström, F.; Liljedahl, U.; Syvänen, A.C. Gender-specific association between preproendothelin-1 genotype and reduction of systolic blood pressure during antihypertensive treatment---results from the Swedish irbesartan left ventricular hypertrophy investigation versus atenolol (SILVHIA). Clinical cardiology. 2004, 27, 287–290. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). rs5370 variant (EDN1 gene). Available at https://www.pharmgkb.org/variant/PA166156901. Accessed date 21 March 2023.
- Gong, Y.; Wang, Z.; Beitelshees, A.L.; McDonough, C.W.; Langaee, T.Y.; Hall, K.; Schmidt, S.O.; Curry, R.W., Jr; Gums, J.G.; Bailey, K.R.; Boerwinkle, E. Pharmacogenomic genome-wide meta-analysis of blood pressure response to β-blockers in hypertensive African Americans. Hypertension. 2016, 67, 556–563. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). rs1367094 variant (ZMAT4 gene). Available at https://www.pharmgkb.org/variant/PA166157555. Accessed date 21 March 2023.
Figure 1.
PRISMA flow diagram of studies in systematic review.
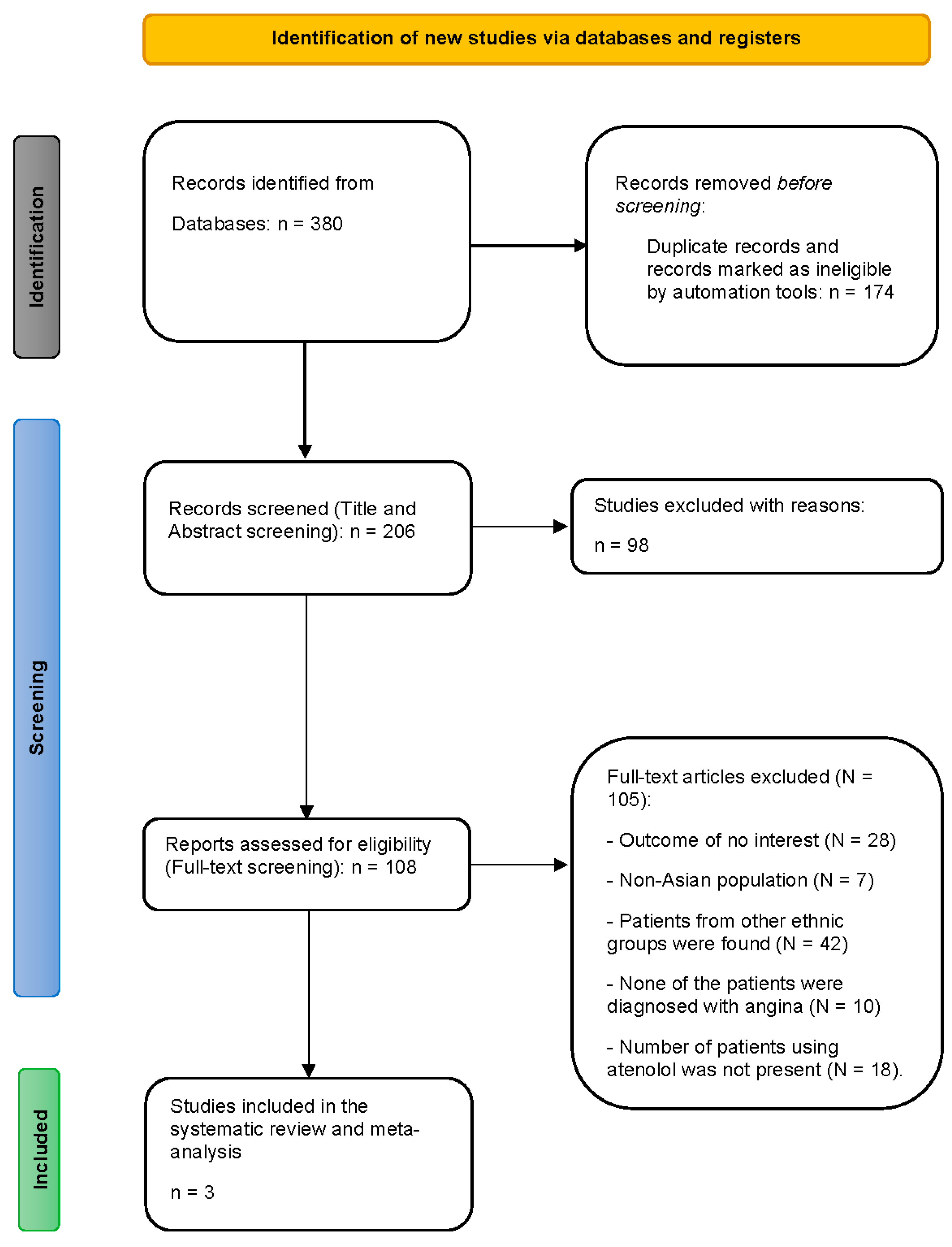
Figure 2.
Risk of bias summary according to authors’ judgment.
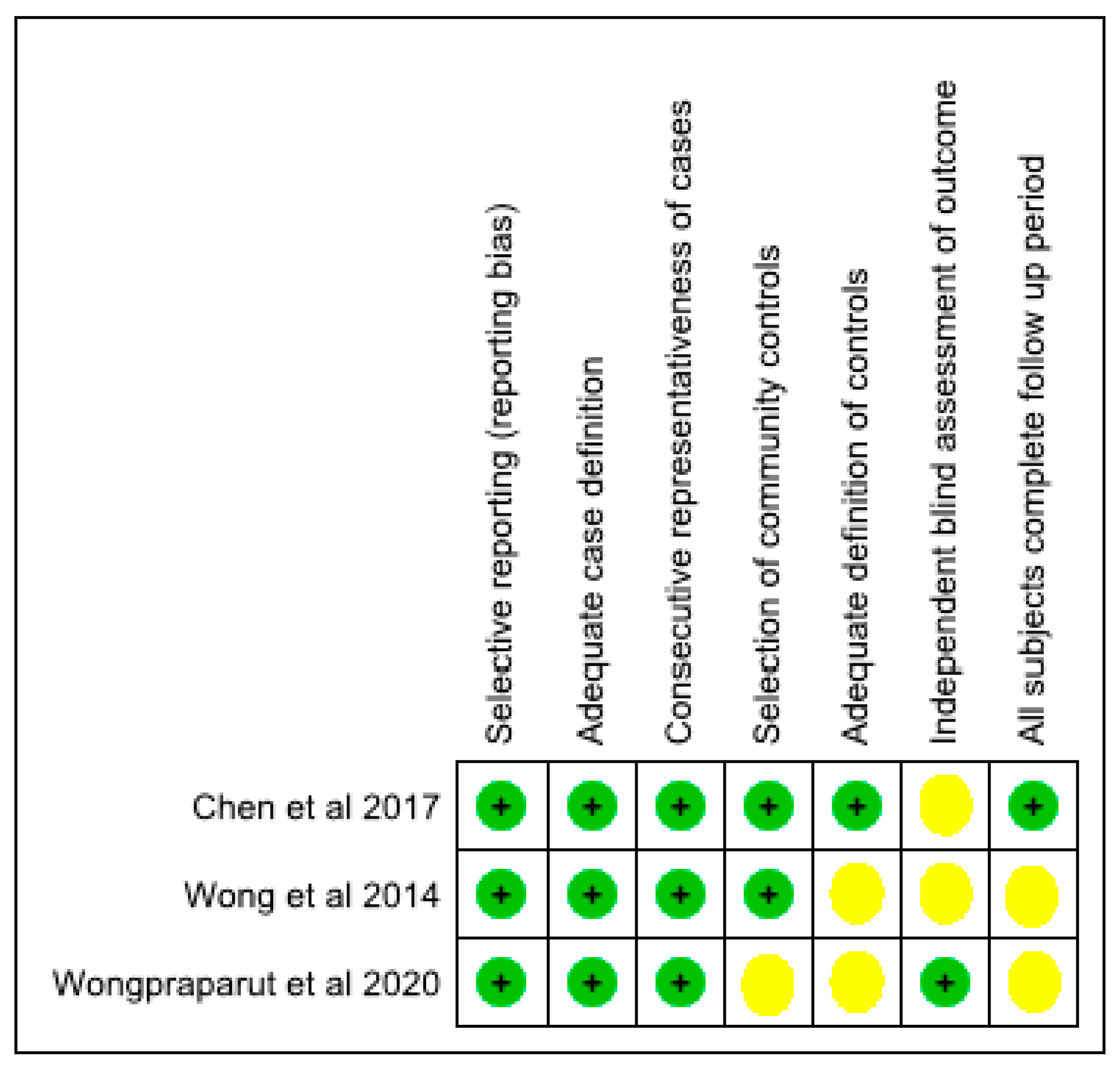
Figure 3.
Forest plot of the all-cause mortality rate among atenolol versus non-atenolol users.
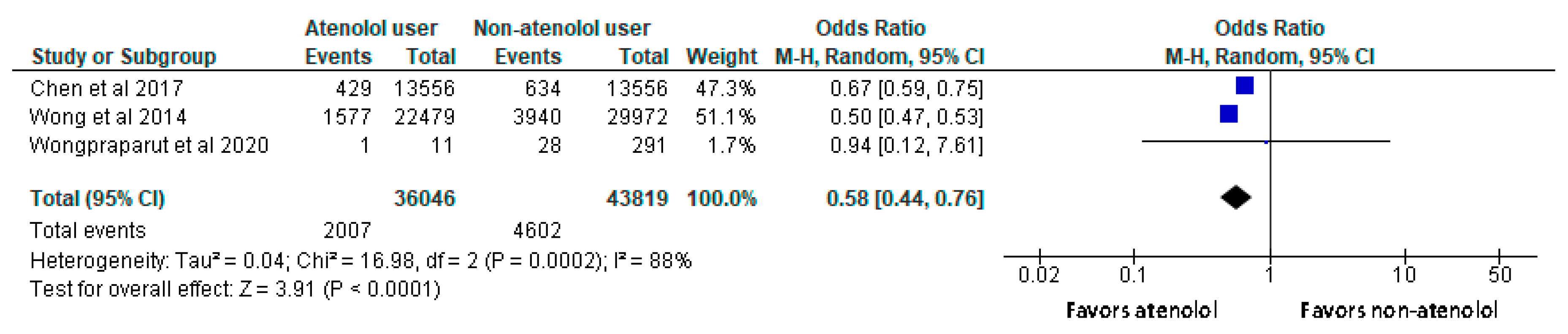
Figure 4.
Forest plot of the all-cause mortality rate among atenolol versus metoprolol tartrate users.
Figure 4.
Forest plot of the all-cause mortality rate among atenolol versus metoprolol tartrate users.
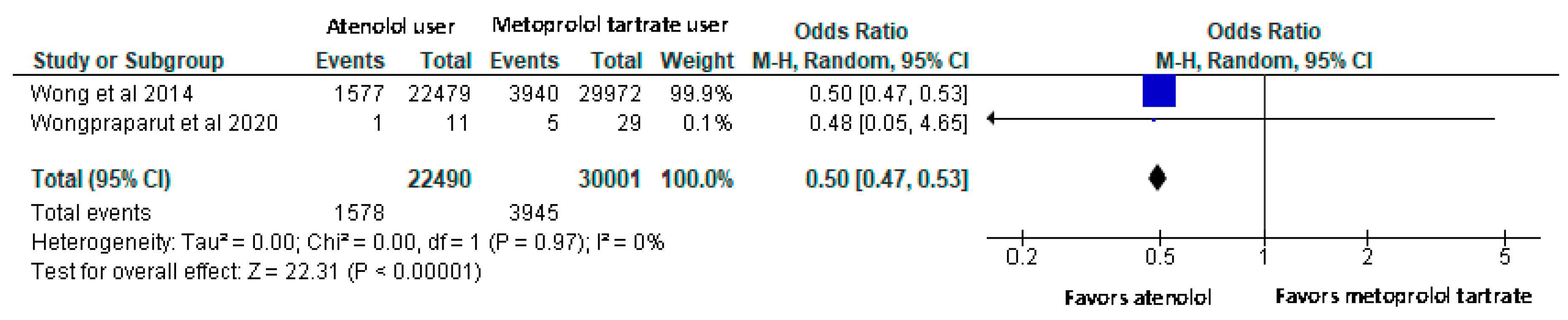

Table 1.
Characteristics of included studies.
| Author | Title | Study design | Setting/ duration | Aim | Participants | Outcome |
|---|---|---|---|---|---|---|
| Wong et al. (2014) | The effectiveness of metoprolol versus atenolol on prevention of all-cause and cardiovascular mortality in a large Chinese population: A cohort study | Retrospective cohort study | The study conducted in Hong Kong between 2001 and 2010. | Compared the incidence of all-cause mortality and cardiovascular mortality between patients newly prescribed atenolol vs. metoprolol tartrate users | Hypertensive patients using atenolol (N=22,479) or metoprolol tartrate (N=29,972). | 7.0% and 13.1% died of any causes among atenolol and metoprolol users, respectively (p <0.005). The incidence of cardiovascular mortality among atenolol users was lower than metoprolol users (1.4% vs. 3.7%, p < 0.001). |
| Chen et al. (2017) | Impact of Beta-Blocker Initiation Timing on Mortality Risk in Patients With Diabetes Mellitus Undergoing Non-cardiac Surgery: A Nationwide Population-Based Cohort Study | Retrospective cohort study | The study conducted using the Taiwan’s National Health Insurance Research Database between 2000 and 2011. | To explore the role of perioperative initiation of beta-blockers, including atenolol, in patients with diabetes mellitus undergoing non-cardiac surgery. | Diabetic patients undergoing non-cardiac surgery using atenolol (N=13,556) or non-atenolol matched controls (N=13,556). matched controls. | Beta-blocker users were associated with lower risks of in-hospital (odds ratio 0.75, 95% CI 0.68–0.82) and 30-day (odds ratio 0.75, 95% CI 0.70–0.81) mortality. |
| Wongpraparut et al. (2020) | Impact of guideline-recommended versus non-guideline-recommended β-blocker and Doppler echocardiographic parameters on 1-year mortality in Thai ischemic cardiomyopathy patients: A prospective multicenter registry | Prospective cohort study | The study conducted in 9 medical centers located across Thailand from December 2014 to November 2015. | To determine and to identify factors that significantly predicts 1-year mortality of Thai patients with ischemic cardiomyopathy | Patients with coronary artery disease using atenolol (N=11), metoprolol tartrate (N=29), or non-atenolol beta-blocker agent (N= 291). | The use of non-guideline-recommended beta-blockers (atenolol, metoprolol tartrate, and propranolol) rather than guideline recommended beta-blockers (Carvedilol, metoprolol succinate, nebivolol, and bisoprolol) were associated with increased with 1-year mortality. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



