
Submitted:
06 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
Puberty identifies the transition from childhood to adulthood. It normally lasts from 3 to 5 years and begins from 9 years in males and 8 years in females, although with differences related to familiarity and geographical origin. Precocious puberty is the onset of signs of pubertal development before age 8 in girls and before age 9 in boys, it has an incidence of 1/5000–1/10.000 with an F:M ratio ranging from 3:1 to 20:1. Based on the mechanism that triggers puberty, precocious puberty can be classified as central, also known as gonadotropin-dependent precocious puberty or true precocious puberty, and peripheral, also known as gonadotropin-independent precocious puberty or precocious pseudopuberty. Thus, the main aim of this narrative report is to describe the standard clinical management and therapy of precocious puberty according to the experience and expertise of pediatricians and pediatric endocrinologists at Policlinico Umberto I, Sapienza University of Rome, Italy. In the suspicion of early sexual maturation, it is important to collect information regarding the age of onset, the speed of maturation of secondary sexual characteristics, exposure to exogenous sex steroids and the presence of neurological symptoms. The objective examination, in addition to the evaluation of secondary sexual characteristics, must also include the evaluation of auxological parameters. Initial laboratory investigations should include serum gonadotropin levels (LH and FSH) and serum levels of the sex steroids. Brain MRI should be performed as indicated by the 2009 Consensus Statement in all boys regardless of chronological age and in all girls with onset of pubertal signs before 6 years of age. The gold standard in the treatment of central precocious puberty is represented by GnRH analogs, whereas as far as peripheral forms are concerned, the triggering cause must be identified and treated. At the moment there are no reliable data establishing the criteria for discontinuation of GnRH analogs therapy. However, numerous pieces of evidence suggest that the therapy should be suspended at the physiological age at which puberty occurs.
Keywords:
Precocious puberty
; Pseudopuberty
; Children
; Pediatrician
; GnRh analogs.
1. Introduction
Puberty is the transitional period from childhood to adulthood characterized by major physical and psychological changes leading to the development of secondary sexual characteristics, the maturation of the gonads and the achievement of reproductive capacity [1]. Puberty is a complex process determined by environmental, genetic, geographical and metabolic factors [2]. The mechanism underlying pubertal activation remains unknown although the following have been identified as possible causes: adrenal activation, physical and psychological stress, an abundance of adipose tissue and the inflammation of the intestinal tract [3,4].
Puberty begins with the activation of hypothalamic-pituitary-gonadal axis (HPG), which already occurs during fetal life, but is usually silenced in the final period of pregnancy and then reactivated immediately after birth [5,6]. This post-natal transitory activation is defined as mini-puberty and lasts up to 6 months in boys and up to 2 years in girls, until the blockage of gonadotropin-releasing hormone (GnRH) secretion, which will resume during puberty [7,8].
The onset of puberty is determined by the secretion of GnRH at the hypothalamic level which in turn activates the production of two hormones by the pituitary gland, the gonadotropins luteinizing hormone (LH) and follicle stimulating hormone (FSH) [9]. LH and FSH act on the gonads promoting gametogenesis [10]. Pubertal development is considered physiological when it begins between the ages of 8 and 13 in females and between 9 and 14 years in males, although it is a variable process within each individual, lasting on average between 3 and 5 years [2,10].
Precocious puberty
Precocious puberty (PP) is the onset of secondary sexual characteristics before the age of 8 in girls and before the age of 9 in boys. Specifically, the first sign of pubertal activation is represented by thelarche in females and an increase in testicular volume in males greater than or equal to 4 ml [1,10]. It is a relatively rare condition affecting 1:5,000-1:10,000 children with an F:M ratio ranging from 3:1 to 20:1 [11,12]. There has been an increase in diagnoses of precocious puberty partly attributable to the SARS-CoV-2 pandemic, probably related to a sedentary lifestyle characterized by overweight, the use of electronic devices and stress related symptoms acting as endocrine disruptors [13,14,15,16,17].
PP can be classified as follows:
- –
- central or true precocious puberty (CPP), if it is determined by an early activation of the HPG axis with the production of gonadotropins
- –
- peripheral or precocious pseudopuberty (PPP), unrelated to the production of gonadotropins.
Central precocious puberty
CPP accounts for about 80% of all forms of PP and is caused by early activation of the HPG axis with increased GnRH secretion and gonadal activation [3,18]. Although rarer, CPP in males is more often related to underlying hypothalamic-pituitary organic lesions [7]. Although it is often idiopathic, numerous genetic mutations related to CPP have been identified, among these the loss of function mutation of the MKRN3 gene is one of the most involved [12]. The loss of function of the MKRN3 gene, located within the Prader-Willi syndrome region on chromosome 15q11.2, is responsible for a stimulatory action on GnRH secretion [19,20].
CPP can have a familial form in approximately one-quarter of the children [21]. The recognition of this inherited condition increased after the identification of autosomal dominant CPP with paternal transmission caused by mutations also in the DLK1 gene [21]. Indeed, it has been shown that the prevalence of familial CPP was estimated at 22%, with a similar frequency of maternal and paternal transmission[21]. Pedigree analyses of families with maternal transmission suggested an autosomal dominant inheritance. Clinical and hormonal features, as well as treatment response to GnRHa, were similar among patients with different forms of transmission of familial CPP [21]. MKRN3 loss-of-function mutations were the most prevalent cause of familial CPP, followed by DLK1 loss-of-function mutations, affecting, respectively, 22% and 4% of the studied families; both affected exclusively families with paternal transmission [21]. Rare variants of uncertain significance were identified in CPP families with maternal transmission [21].
Other genetic mutations have been associated with CPP, including gain-of-function mutations in the KISS1 gene, which encodes the kisspeptin proteins capable of stimulating the production of gonadotropins, and the KISS1R gene, formerly known as GPR54, which encodes its G protein-coupled receptor [22]. Among the most important factors in the development of precocious puberty we certainly find endocrine disruptors that significantly increase the risk of precocious puberty [3]. One of the most studied factors would be leptin which would seem to increase with the increase in visceral fat causing an early release of GnRH [15].
Another peptide involved would appear to be ghrelin, a peptide with orexigenic action produced in the stomach, which instead has an inhibitory action on the production of GnRH by decreasing the responsiveness of LH to its release factor [10] and simultaneously increasing pituitary growth hormone (GH) secretion, thus acting at the intersection of gonadotropic and somatotropic axes [23].
In recent years, an association has emerged between pubertal timing and exposure to environmental factors that would cause an early activation of the pubertal axis [24,25]. Some of these substances act as estrogen receptor agonists or androgen receptor antagonists [7,22,26,27]. These endocrine-disrupting chemicals have been suggested as affecting the age of pubertal onset and include: phthalates, pesticides, isoflavonoids, phytoestrogens, polybromobiphenyl and mycotoxins [11,28].
Peripherical precocious puberty
PPP is characterized by an increase in adrenal and gonadal sex steroids in the absence of activation of the HPG axis; the pubertal characteristics may be appropriate for the child's sex (isosexual) or inappropriate, with virilization of females and feminization of males (contrasexual) [29]. It can be congenital, with the most frequent forms represented by congenital adrenal hyperplasia and McCune-Albright syndrome, or acquired, mainly related to hormone-secreting endocrine tumors [2,11,30].
The main purpose of this work is to describe the standard clinical management and therapy of precocious puberty according to the experience and expertise of the pediatric endocrinology of Policlinico Umberto I, Sapienza University of Rome, Italy where approximately 50 children and adolescents are treated each year, equally distributed between sexes.
2. Diagnosis
Regardless of the cause, PP must be promptly recognized since it is associated with accelerated stature growth and skeletal maturation if untreated, inducing an early growth arrest with premature epiphyseal fusion due to excess sex steroids, which results in short adult height [2]. The key features suggesting PP are the progressive development of breasts in girls and testicular volume in boys over a short period of observation (3-6 months) associated with rapid height growth (height velocity 6-7 cm/year ) especially in girls aged between 6-8 years, when this condition occurs more frequently [5,31,32].
The family pediatrician plays a fundamental role in paying attention to pubertal development during normal health checks of the child, quickly referring a patient to a pediatric endocrinologist in case of pubertal activation signs, considering its increased prevalence in European countries [30,33].
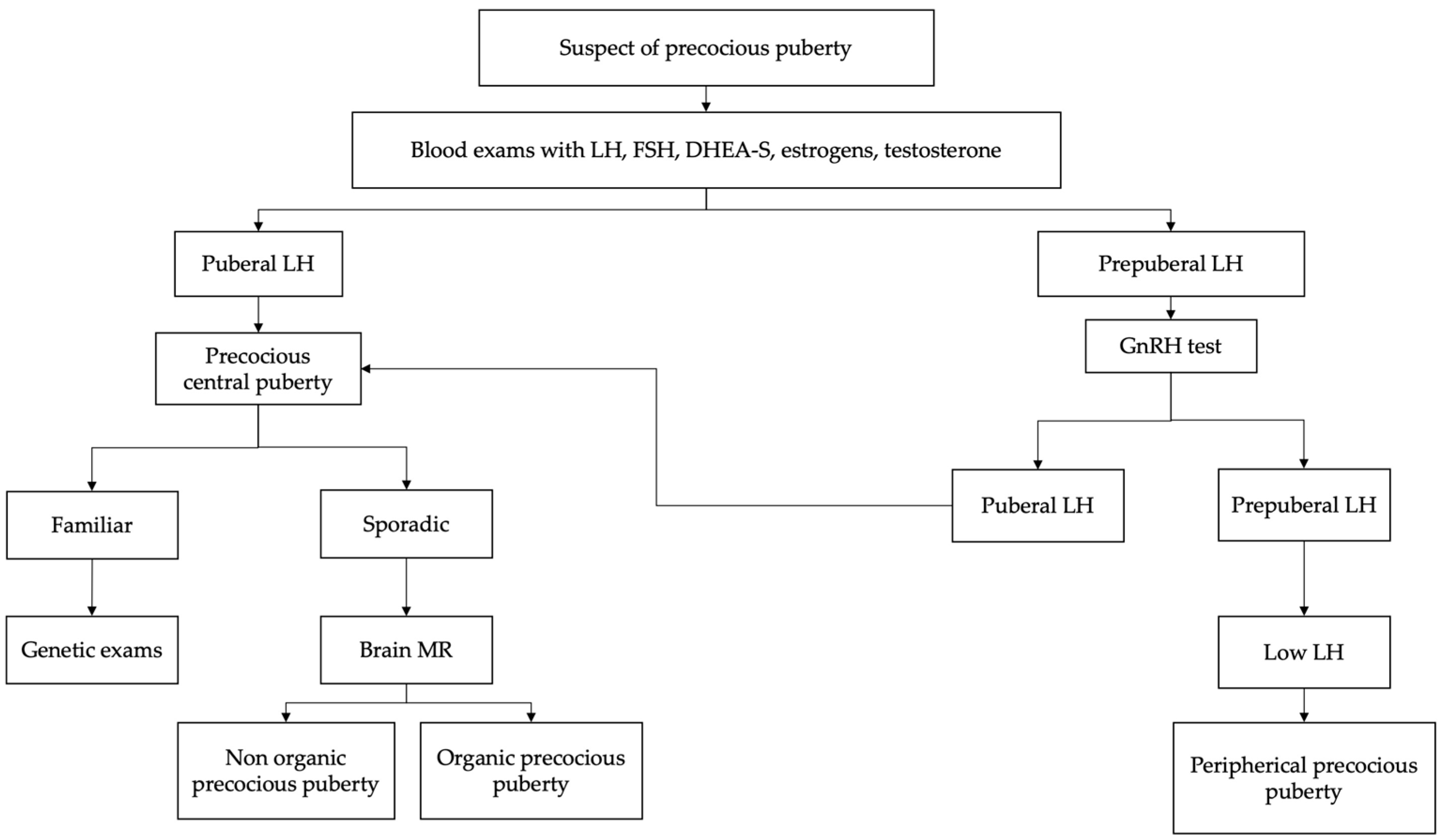
In the suspicion of early sexual maturation, in children presenting with signs of secondary sexual development before the age of 8 (females) or 9 (males), the evaluation should begin with an accurate medical and familial history as shown in Flowchart 1 [22,34]. It is important to collect information regarding age of onset, rate of maturation of secondary sexual characteristics, exposure to exogenous sex steroids and the presence of neurological symptoms [10,14].
The physical examination, in addition to the evaluation of secondary sexual characteristics, must also include the evaluation of auxological parameters, such as weight, height, body mass index and height velocity (cm/year) [12,34]. Growth spurt is an important feature of pubertal development. In fact, growth acceleration with growth centile change supports the diagnosis of pubertal activation and therefore of PP [5,26].
Evaluation of bone age should be performed, because children with PP frequently show advanced bone age, greater than 2 standard deviations beyond chronological age [35,36,37]. However, an advanced bone age does not rule out a benign pubertal variant, since up to 30% of children with benign premature adrenarche have bone ages ≥ 2 years in advance of their chronologic age [25,38,39].
The physical examination should include assessment of visual fields (given the possibility of a central nervous system (CNS) lesion) and examination for café-au-lait spots (suggestive of neurofibromatosis or McCune-Albright syndrome) [29,40].
Marshall and Tanner criteria are used to assess the stage of pubertal development as illustrated in the Table 1 [41]. Furthermore, it may be difficult to distinguish precocious puberty from benign variants of precocious pubertal development such as isolated premature thelarche premature, premature adrenarche premature and lipomastia [1].
In girls under two years of age, the finding of isolated thelarche is frequent and is rarely associated with a pathological condition. Isolated premature thelarche is a benign, self-limiting condition characterized by the appearance of breast tissue in the absence of other signs indicative of pubertal development [12]. Transient thelarche also appears to be a frequent and benign phenomenon, characterized by peculiar subsequent pubertal timing and pathway, apparently unrelated to HPG axis activation or adiposity [42].
Premature adrenarche is also a benign condition, characterized by the appearance of pubic hair, axillary hair and acne that occurs in girls under 8 years of age and in boys under 9 years of age, in the absence of other signs of pubertal development and is caused by adrenal androgen secretion in the absence of activation of the HPG axis [22]. Furthermore, in obese or overweight girls it is important to distinguish a condition of lipomastia, an accumulation of adipose tissue in the breast area, from the thelarche, which is identified with the presence of glandular breast tissue below the areola [43].
Initial laboratory investigations should include serum gonadotropin (LH and FSH) levels and serum levels of the sex steroids, estradiol in girls and testosterone in boys [44,45,46]. Baseline LH > 0.3 mIU/mL is considered diagnostic for central precocious puberty; however, values below this limit do not exclude the diagnosis and require further diagnostic investigations. Measurable estradiol values or testosterone values >30 ng/dL suggest, but do not confirm the diagnosis [47,48]. Therefore, children with clinical signs of early pubertal development and baseline LH values < 0.3 mIU/mL are candidates for GnRH stimulation testing to identify HPG axis activation. Peak LH values > 5 mIU/mL are considered indicative of pubertal activation. FSH values alone are not diagnostic, but the post-stimulus LH/FSH ratio is useful as an indicator of increased LH secretion using a cut-off between 0.6 and 1 [6,19]. However, the sensitivity and specificity of this index are lower than using the isolated post-stimulus LH surge.
In contrast, suppressed FSH values associated with elevated sex steroid levels suggest the diagnosis of PPP. In these cases it is essential to complete the diagnostic procedure with the dosage of tumor markers (alpha 1-fetoprotein, beta-HCG, CEA and CA125), in order to exclude a hypersecretion of sex steroids of a neoplastic or paraneoplastic nature, and the measurement of serum dehydroepiandrosterone sulphate (DHEA-S) and 17-hydroxyprogesterone levels is advisable, which may be increased in adrenal tumors or congenital adrenal hyperplasia due to 21-hydroxylase deficiency [11,49].
In the diagnostic process of suspected precocious puberty it is always important to exclude an unknown and therefore untreated hypothyroidism condition, especially if there is a poor activation of the pituitary gonadotropins after a stimulus test [50]. Initial evaluation of the child with suspected precocious puberty should include assessment of bone age, because children with precocious puberty frequently have advanced bone age, greater than 2 SDs of chronological age [35,36,37].
Furthermore, pelvic ultrasound, a quick, non-invasive and low-cost examination, is a useful support for diagnosis by evaluating uterine development and ovarian volume and to investigate the presence of ovarian cysts or tumors [7,51]. During infancy the ovarian volume is stable, the fundus of the uterus and the cervix have a similar width and assume a tubular configuration, while in the pubertal phase the uterus increases in volume and the cervix assumes the typical pear shape of adulthood [11,52] .
The following ultrasound criteria aid in correctly identifying PP:
The presence of an endometrial stripe on pelvic ultrasound is also indicative of precocious puberty [56,57]. Overall, the ovarian volume represents the best indicator of PP, whereas uterine length is more capable of differentiating isolated premature thelarche from premature puberty [55]. The uterine fundal/cervical ratio ≥1 is generally inaccurate and no longer used [55].
Ultrasound examination also aids in the evaluation of boys with suspected PP, in which testicular enlargement represent the first sign of HPG axis activation. Specifically, testicular ultrasound represents the gold standard technique for the assessment of testicular volume [58], with a cut-off of 2.7 mL (calculated employing Lambert’s formula) corresponding to the traditional criteria of 4 mL defining Tanner stage II [59]. Furthermore, testicular ultrasound can predict testicular function [60] and is crucial for the evaluation of cryptorchidism and causes of scrotal enlargement, such as inguino-scrotal hernias, hydrocele, epididymo-orchitis, varicocele, testicular cancer and oncohematological disorders [58].
In patients in whom the diagnosis of PPC is reached, it is important to exclude the presence of organic pathology affecting the CNS [61]. Among the main risk factors suggesting the presence of organic brain lesions are male sex, early age of onset, rapid progression and the presence of neurological signs and symptoms. Brain MRI should also be considered in all children with rapidly progressive CPP [62]. However, numerous studies have shown that the detection of CNS tumors in girls aged between 6 and 8 years with PPC is a rare occurrence. Brain MRI in all boys regardless of chronological age and in all girls with onset of pubertal signs before 6 years of age. To date, it is still under discussion whether to perform this instrumental investigation in girls aged between 6 and 8 years, especially in those with normal sequence of pubertal development and no clinical evidence of CNS lesions, in particular in the presence of a family history of earlier pubertal onset [4].
Genetic analysis should be considered in the presence of a family history of CPP or in the event that clinical features attributable to syndromic forms are present. To date, the mutation in the MKRN3 gene represents the most frequent form of monogenic CPP with a prevalence of 33-47% in forms with familial recurrence and 0.4-5% in sporadic cases [1,35]. Furthermore, CPP is a key feature of several genetic syndromes such as Silver-Russell syndrome, Williams-Beuren syndrome, and Temple syndrome [12,19,63,64]
A pelvic ultrasound in females with PPP should be performed to help identify the presence of an ovarian cyst or tumor, while in males an ultrasound examination of the testes to rule out a Leydig cell tumor is essential In both females and males, peripheral precocity and progressive virilization and/or markedly elevated serum adrenal androgens may be due to an adrenal tumor, thus a computed tomography or MRI of the adrenal glands should be performed whenever other conditions such as congenital adrenal hyperplasia and exogenous androgen exposure have been excluded [65].
3. Treatment
Treatment of PP aims at preserving growth potential, synchronizing pubertal development with peers, and improving psychological distress [11,12]. The main clinical criterion for initiation of therapy is the finding of pubertal progression, in children under the age of 8 (females) or 9 (males), with growth acceleration confirmed in a 3-6 month follow-up period [66,67,68]. This observation period may not be necessary if the bone age is markedly advanced or if the girl or boy presents with Tanner stage III [41,43]. The treatment is also indicated if PP is responsible for psychological and psychosocial disorders that can compromise the quality of life of patients and cause emotional and behavioral disorders that can also be detected in later ages [1,69].
The gold standard in the treatment of CPP is represented by GnRH analogues (GnRHa) [70]. Their rationale for use is based on the recognition that, after an initial transient stimulation of gonadotropin secretion from the pituitary (termed ‘flare up’), high concentrations of GnRH eventually cause a complete, but reversible suppression of the HPG axis by down-regulating the GnRH receptor, consequently inhibiting the secretion of gonadotropins [10,12]. GnRHa are available in different formulations: although slow-release formulations administered monthly were previously the most frequently used, formulations administered every 3 or 6 months (leuprolide and triptorelin) have been introduced in recent years, as well as subcutaneous implants of histrelin capable of inducing suppression of the hypothalamic-pituitary-gonadal axis for a period of 12-24 months [1,66,71,72]. As regards to the therapeutic dosage required for the suppression of the HPG axis, there is no univocal opinion; in the USA higher dosages are used (7.5 mg/month) while in Europe the monthly dosage used is 3.75 mg every 28 days [72,73]. The Table 2 shows the different available formulations of GnRHa.
Currently, there are no firm data establishing criteria for discontinuation of GnRHa therapy [7,75,76]. However, numerous evidences suggest that the therapy should be suspended at the mean physiological age in which puberty occurs (between 10.5-11.5 years in females and between 12-13 years in males), or when a bone age of around 12 years in girls and 13 years in boys is reached, or in cases of marked reduction of growth velocity during therapy [11,75]. Thus, the decision to discontinue therapy is individualized and is based on many specific patient characteristics, including absolute and predicted height, chronological age, psychosocial factors, pubertal stage, and family preferences [3,77].
Major factors affecting height prognosis include timely initiation of treatment, age at onset of puberty, bone age at diagnosis, height at diagnosis, and target height [33,43]. Girls who start treatment before the age of 6 have better outcomes than patients who start treatment between 6 and 8 years, while starting therapy after 8 years of age does not appear to be associated with an increase in height in adulthood [1,11,71]. GnRHa therapy is generally well tolerated in childhood, although the most frequently reported adverse events are injection site reactions, headache and hot flushes, which in most cases occur early and resolve by subsequent administrations [11,78,79,80]. More rare is the occurrence of vaginal discharge, or the development of a sterile abscess at the injection site or at the subcutaneous implant site which may lead to loss of efficacy of the therapy [3,76]. Weight gain has been documented during therapy in some patients; however, the data available to date indicate that long-term GnRHa treatment does not affect body compo-sition and the onset of obesity or the increased incidence of polycystic ovary syndrome (PCOS) in adulthood [81,82].
4. Discussion and Conclusions
Puberty is a complex process of transition from childhood to adulthood and its mechanisms are still not well understood. PP is more common in females and more frequently it concerns idiopathic forms of CPP, but the recent characterization of genes involved in pubertal development underlines the important role of these factors in determining pubertal timing. It is important to identify the child with pathological pubertal development in order to undertake an accurate diagnostic and therapeutic procedure. The main goals of the treatment of precocious puberty are the preservation of growth potential, the synchronization of pubertal development with peers and the improvement of psychological distress. PPP is an extremely heterogeneous condition and can represent a manifestation of numerous pathologies, therefore an accurate etiological diagnosis is essential for correct management.
Author Contributions
Conceptualization, G.M., M.F. and L.T.; methodology, G.M., R.P., F.T., M.M., G.F., I.P., A.G., and F.C.; writing—original draft preparation, G.M.; writing—review and editing, G.M., R.P., M.F. and L.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
CNS: central nervous system; CPP: central precocious puberty; FSH: follicle stimulating hormone; GnRH: gonadotropin releasing hormone; GnRHa: gonadotropin releasing hormone analogues; GPR54: G-protein Coupled Receptor 54 ; HPG: hypothalamic-pituitary-gonadal axis; LH: luteinizing hormone; KISS1: kisspeptin 1; MKRN3: makorin Ring Finger Protein 3 ; MRI: magnetic resonance imaging; PP: precocious puberty; PPP: precocious pseudopuberty.
References
- Eugster EA. Treatment of central precocious puberty. J Endocr Soc 2019;3. [CrossRef]
- Miranda-Lora AL, Torres-Tamayo M, Zurita-Cruz JN, Aguilar-Herrera BE, Calzada-León R, Rivera-Hernández AJ, et al. Diagnosis of precocious puberty: Clinical guideline for the diagnosis and treatment of precocious puberty. Bol Med Hosp Infant Mex 2020;77. [CrossRef]
- Aguirre RS, Eugster EA. Central precocious puberty: From genetics to treatment. Best Pract Res Clin Endocrinol Metab 2018;32. [CrossRef]
- Loomba-Albrecht LA, Styne DM. The physiology of puberty and its disorders. Pediatr Ann 2012;41. [CrossRef]
- Wood CL, Lane LC, Cheetham T. Puberty: Normal physiology (brief overview). Best Pract Res Clin Endocrinol Metab 2019;33. [CrossRef]
- Koskenniemi JJ, Virtanen HE, Toppari J. Testicular growth and development in puberty. Curr Opin Endocrinol Diabetes Obes 2017;24. [CrossRef]
- Latronico AC, Brito VN, Carel JC. Causes, diagnosis, and treatment of central precocious puberty. Lancet Diabetes Endocrinol 2016;4. [CrossRef]
- Klein DA, Emerick JE, Sylvester JE, Vogt KS. Disorders of Puberty: An Approach to Diagnosis and Management. Am Fam Physician 2017;96.
- Brito VN, Canton APM, Seraphim CE, Abreu AP, Macedo DB, Mendonca BB, et al. The Congenital and Acquired Mechanisms Implicated in the Etiology of Central Precocious Puberty. Endocr Rev 2023;44. [CrossRef]
- Brito VN, Spinola-Castro AM, Kochi C, Kopacek C, Da Silva PCA, Guerra-Júnior G. Central precocious puberty: Revisiting the diagnosis and therapeutic management. Arch Endocrinol Metab 2016;60. [CrossRef]
- Sultan C, Gaspari L, Maimoun L, Kalfa N, Paris F. Disorders of puberty. Best Pract Res Clin Obstet Gynaecol 2018;48. [CrossRef]
- Manotas MC, González DM, Céspedes C, Forero C, Moreno APR. Genetic and Epigenetic Control of Puberty. Sex Dev 2022;16. [CrossRef]
- Petrella C, Nenna R, Petrarca L, Tarani F, Paparella R, Mancino E, et al. Serum NGF and BDNF in Long-COVID-19 Adolescents: A Pilot Study. Diagnostics 2022;12:1162. [CrossRef]
- Prosperi S, Chiarelli F. Early and precocious puberty during the COVID-19 pandemic. Front Endocrinol (Lausanne) 2023;13. [CrossRef]
- Chioma L, Bizzarri C, Verzani M, Fava D, Salerno M, Capalbo D, et al. Sedentary lifestyle and precocious puberty in girls during the COVID-19 pandemic: an Italian experience. Endocr Connect 2022;11. [CrossRef]
- Kim EY, Lee MI. Psychosocial aspects in girls with idiopathic precocious puberty. Psychiatry Investig 2012;9. [CrossRef]
- Tremblay L, Frigon JY. Precocious puberty in adolescent girls: A biomarker of later psychosocial adjustment problems. Child Psychiatry Hum Dev 2005;36. [CrossRef]
- Oliveira Neto CP de, Azulay RS de S, Almeida AGFP de, Tavares M da GR, Vaz LHG, Leal IRL, et al. Differences in Puberty of Girls before and during the COVID-19 Pandemic. Int J Environ Res Public Health 2022;19. [CrossRef]
- Shim YS, Lee HS, Hwang JS. Genetic factors in precocious puberty. Clin Exp Pediatr 2022;65. [CrossRef]
- Tauber M, Hoybye C. Endocrine disorders in Prader-Willi syndrome: a model to understand and treat hypothalamic dysfunction. Lancet Diabetes Endocrinol 2021;9. [CrossRef]
- Tinano FR, Canton APM, Montenegro LR, de Castro Leal A, Faria AG, Seraphim CE, et al. Clinical and Genetic Characterization of Familial Central Precocious Puberty. J Clin Endocrinol Metab 2023;108:1758–67. [CrossRef]
- Tajima T. Genetic causes of central precocious puberty. Clin Pediatr Endocrinol 2022;31. [CrossRef]
- Tenuta M, Carlomagno F, Cangiano B, Kanakis G, Pozza C, Sbardella E, et al. Somatotropic-Testicular Axis: A crosstalk between GH/IGF-I and gonadal hormones during development, transition, and adult age. Andrology 2021;9:168–84. [CrossRef]
- Xu YQ, Li GM, Li Y. Advanced bone age as an indicator facilitates the diagnosis of precocious puberty. J Pediatr (Rio J) 2018;94. [CrossRef]
- Cavallo F, Mohn A, Chiarelli F, Giannini C. Evaluation of Bone Age in Children: A Mini-Review. Front Pediatr 2021;9. [CrossRef]
- Chaudhry S, Tadokoro-Cuccaro R, Hannema SE, Acerini CL, Hughes IA. Frequency of gonadal tumours in complete androgen insensitivity syndrome (CAIS): A retrospective case-series analysis. J Pediatr Urol 2017;13:498.e1-498.e6. [CrossRef]
- Ahmed ML, Ong KK, Dunger DB. Childhood obesity and the timing of puberty. Trends Endocrinol Metab 2009;20. [CrossRef]
- Silventoinen K, Jelenkovic A, Palviainen T, Dunkel L, Kaprio J. The Association Between Puberty Timing and Body Mass Index in a Longitudinal Setting: The Contribution of Genetic Factors. Behav Genet 2022;52. [CrossRef]
- Haddad NG, Eugster EA. Peripheral precocious puberty including congenital adrenal hyperplasia: causes, consequences, management and outcomes. Best Pract Res Clin Endocrinol Metab 2019;33. [CrossRef]
- Tarani L, Rasio D, Tarani F, Parlapiano G, Valentini D, Dylag KA, et al. Pediatrics for Disability: A Comprehensive Approach to Children with Syndromic Psychomotor Delay. Curr Pediatr Rev 2021;18:110–20. [CrossRef]
- Jrgensen A, Rajpert-De Meyts E. Regulation of meiotic entry and gonadal sex differentiation in the human: Normal and disrupted signaling. Biomol Concepts 2014;5. [CrossRef]
- Perluigi M, Di Domenico F, Buttterfield DA. Unraveling the complexity of neurodegeneration in brains of subjects with Down syndrome: Insights from proteomics. Proteomics - Clin Appl 2014;8:73–85. [CrossRef]
- Profeta G, Micangeli G, Tarani F, Paparella R, Ferraguti G, Spaziani M, et al. Sexual Developmental Disorders in Pediatrics. Clin Ter 2022;173:475–88. [CrossRef]
- Yu T, Yu Y, Li X, Xue P, Yu X, Chen Y, et al. Effects of childhood obesity and related genetic factors on precocious puberty: protocol for a multi-center prospective cohort study. BMC Pediatr 2022;22. [CrossRef]
- Lewis K, Lee PA. Endocrinology of male puberty. Curr Opin Endocrinol Diabetes Obes 2009;16. [CrossRef]
- Korkmaz O, Sari G, Mecidov I, Ozen S, Goksen D, Darcan S. The Gonadotropin-Releasing Hormone Analogue Therapy May Not Impact Final Height in Precocious Puberty of Girls With Onset of Puberty Aged 6 - 8 Years. J Clin Med Res 2019;11. [CrossRef]
- Macedo DB, Cukier P, Mendonca BB, Latronico AC, Brito VN. [Advances in the etiology, diagnosis and treatment of central precocious puberty]. Arq Bras Endocrinol Metabol 2014;58. [CrossRef]
- Liimatta J, Utriainen P, Voutilainen R, Jääskeläinen J. Girls with a history of premature adrenarche have advanced growth and pubertal development at the age of 12 years. Front Endocrinol (Lausanne) 2017;8. [CrossRef]
- Novello L, Speiser PW. Premature adrenarche. Pediatr Ann 2018;47. [CrossRef]
- Wirth T. Fibrous dysplasia. Orthopade 2020;49:929–40. [CrossRef]
- Tanner Scale. Definitions, 2020. [CrossRef]
- Soto J, Pereira A, Busch AS, Almstrup K, Corvalan C, Iñiguez G, et al. Reproductive hormones during pubertal transition in girls with transient Thelarche. Clin Endocrinol (Oxf) 2020;93:296–304. [CrossRef]
- Balzer BWR, Garden FL, Amatoury M, Luscombe GM, Paxton K, Hawke CI, et al. Self-rated Tanner stage and subjective measures of puberty are associated with longitudinal gonadal hormone changes. J Pediatr Endocrinol Metab 2019;32. [CrossRef]
- Johannsen TH, Main KM, Ljubicic ML, Jensen TK, Andersen HR, Andersen MS, et al. Sex differences in reproductive hormones during mini-puberty in infants with normal and disordered sex development. J Clin Endocrinol Metab 2018;103. [CrossRef]
- Chaudhary S, Walia R, Bhansali A, Dayal D, Sachdeva N, Singh T, et al. FSH-stimulated Inhibin B (FSH-iB): A Novel Marker for the Accurate Prediction of Pubertal Outcome in Delayed Puberty. J Clin Endocrinol Metab 2021;106. [CrossRef]
- Soriano-Guillén L, Argente J. Central precocious puberty: Epidemiology, etiology, diagnosis and treatment. An Pediatr 2011;74. [CrossRef]
- Tomlinson C. Testosterone measurements in early infancy. Arch Dis Child - Fetal Neonatal Ed 2004;89:F558–9. [CrossRef]
- Alotaibi MF. Physiology of puberty in boys and girls and pathological disorders affecting its onset. J Adolesc 2019;71. [CrossRef]
- Muerköster AP, Frederiksen H, Juul A, Andersson AM, Jensen RC, Glintborg D, et al. Maternal phthalate exposure associated with decreased testosterone/LH ratio in male offspring during mini-puberty. Odense Child Cohort. Environ Int 2020;144. [CrossRef]
- DiVall SA, Radovick S. Endocrinology of female puberty. Curr Opin Endocrinol Diabetes Obes 2009;16. [CrossRef]
- Willemsen RH, Elleri D, Williams RM, Ong KK, Dunger DB. Pros and cons of GnRHa treatment for early puberty in girls. Nat Rev Endocrinol 2014;10. [CrossRef]
- Cheuiche AV, da Silveira LG, de Paula LCP, Lucena IRS, Silveiro SP. Diagnosis and management of precocious sexual maturation: an updated review. Eur J Pediatr 2021;180. [CrossRef]
- Razzaghy-Azar M, Ghasemi F, Hallaji F, Ghasemi A, Ghasemi M. Sonographic measurement of uterus and ovaries in premenarcheal healthy girls between 6 and 13 years old: Correlation with age and pubertal status. J Clin Ultrasound 2011;39:64–73. [CrossRef]
- Haber HP, Wollmann HA, Ranke MB. Pelvic ultrasonography: Early differentiation between isolated premature thelarche and central precocious puberty. Eur J Pediatr 1995;154:182–6. [CrossRef]
- Badouraki M, Christoforidis A, Economou I, Dimitriadis AS, Katzos G. Evaluation of pelvic ultrasonography in the diagnosis and differentiation of various forms of sexual precocity in girls. Ultrasound Obstet Gynecol 2008;32:819–27. [CrossRef]
- Yu J, Shin HY, Lee SH, Kim YS, Kim JH. Usefulness of pelvic ultrasonography for the diagnosis of central precocious puberty in girls. Korean J Pediatr 2015;58:294–300. [CrossRef]
- Messina MP, Piccioni MG, Petrella C, Vitali M, Greco A, Ralli M, et al. Advanced Midwifery Practice: Intrapartum Ultrasonography To Assess Fetal Head Station and Comparison With Vaginal Digital Examination. Minerva Obstet Gynecol 2021;73:253–60. [CrossRef]
- Spaziani M, Lecis C, Tarantino C, Sbardella E, Pozza C, Gianfrilli D. The role of scrotal ultrasonography from infancy to puberty. Andrology 2021;9:1306–21. [CrossRef]
- Oehme NHB, Roelants M, Bruserud IS, Eide GE, Bjerknes R, Rosendahl K, et al. Ultrasound-based measurements of testicular volume in 6- to 16-year-old boys — intra- and interobserver agreement and comparison with Prader orchidometry. Pediatr Radiol 2018;48:1771–8. [CrossRef]
- Pozza C, Kanakis G, Carlomagno F, Lemma A, Pofi R, Tenuta M, et al. Testicular ultrasound score: A new proposal for a scoring system to predict testicular function. Andrology 2020;8:1051–63. [CrossRef]
- Chadha NK, Forte V. Pediatric head and neck malignancies. Curr Opin Otolaryngol Head Neck Surg 2009;17:471–6. [CrossRef]
- Lloyd C, McHugh K. The role of radiology in head and neck tumours in children. Cancer Imaging 2010;10:49–61. [CrossRef]
- Micangeli G, Menghi M, Profeta G, Tarani F, Mariani A, Petrella C, et al. The Impact of Oxidative Stress on Pediatrics Syndromes. Antioxidants 2022;11:1983. [CrossRef]
- Bulcao Macedo D, Nahime Brito V, Latronico AC laudi. New causes of central precocious puberty: the role of genetic factors. Neuroendocrinology 2014;100. [CrossRef]
- Dorn LD. Psychological and social problems in children with premature adrenarche and precocious puberty. Curr Clin Neurol 2010. [CrossRef]
- Klein KO, Lee PA. Gonadotropin-Releasing Hormone (GnRHa) Therapy for Central Precocious Puberty (CPP): Review of Nuances in Assessment of Height, Hormonal Suppression, Psychosocial Issues, and Weight Gain, with Patient Examples. Pediatr Endocrinol Rev 2018;15. [CrossRef]
- Censani M, Feuer A, Orton S, Askin G, Vogiatzi M. Changes in body mass index in children on gonadotropin-releasing hormone agonist therapy with precocious puberty, early puberty or short stature. J Pediatr Endocrinol Metab 2019. [CrossRef]
- Song W, Zhao F, Liang S, Li G, Xue J. Is a combination of a GnRH agonist and recombinant growth hormone an effective treatment to increase the final adult height of girls with precocious or early puberty? Int J Endocrinol 2018;2018. [CrossRef]
- Cantas-Orsdemir S, Eugster EA. Update on central precocious puberty: from etiologies to outcomes. Expert Rev Endocrinol Metab 2019;14. [CrossRef]
- Partsch CJ, Sippell WG. Treatment of central precocious puberty. Best Pract Res Clin Endocrinol Metab 2002;16. [CrossRef]
- Głąb E, Wikiera B, Bieniasz J, Barg E. The influence of GnRH analog therapy on growth in central precocious puberty. Adv Clin Exp Med 2016;25. [CrossRef]
- Gła̧b E, Barg E, Wikiera B, Grabowski M, Noczyńska A. Influence of GnRH analog therapy on body mass in central precocious puberty. Pediatr Endocrinol Diabetes Metab 2009;15.
- Muratoğlu Şahin N, Dikmen AU, Çetinkaya S, Aycan Z. Subnormal growth velocity and related factors during GnRH analog therapy for idiopathic central precocious puberty. JCRPE J Clin Res Pediatr Endocrinol 2018;10. [CrossRef]
- Waal HAD-V De, Cohen-Kettenis PT, Delemarre-Van De Waal HA, Cohen-Kettenis PT. Clinical management of gender identity disorder in adolescents: A protocol on psychological and paediatric endocrinology aspects. Eur. J. Endocrinol. Suppl., vol. 155, 2006. [CrossRef]
- Mouat F, Hofman PL, Jefferies C, Gunn AJ, Cutfield WS. Initial growth deceleration during GnRH analogue therapy for precocious puberty. Clin Endocrinol (Oxf) 2009;70. [CrossRef]
- Pienkowski C, Tauber M. Gonadotropin-releasing hormone agonist treatment in sexual precocity. Endocr Dev 2016;29. [CrossRef]
- Fiore M, Tarani L, Radicioni A, Spaziani M, Ferraguti G, Putotto C, et al. Serum prokineticin-2 in prepubertal and adult Klinefelter individuals. Can J Physiol Pharmacol 2021;100:151–7. [CrossRef]
- Ferraguti G, Fanfarillo F, Tarani L, Blaconà G, Tarani F, Barbato C, et al. NGF and the Male Reproductive System: Potential Clinical Applications in Infertility. Int J Mol Sci 2022;23:13127. [CrossRef]
- Ferraguti G, Terracina S, Micangeli G, Lucarelli M, Tarani L, Ceccanti M, et al. NGF and BDNF in pediatrics syndromes. Neurosci Biobehav Rev 2023;145:105015. [CrossRef]
- Roberts SA, Kaiser UB. Genetics in endocrinology genetic etiologies of central precocious puberty and the role of imprinted genes. Eur J Endocrinol 2020;183. [CrossRef]
- Paparella R, Menghi M, Micangeli G, Leonardi L, Profeta G, Tarani F, et al. Autoimmune Polyendocrine Syndromes in the Pediatric Age. Children 2023;10. [CrossRef]
- Petrella C, Spaziani M, D’Orazi V, Tarani L, Terracina S, Tarani F, et al. Prokineticin 2/PROK2 and Male Infertility. Biomedicines 2022;10. [CrossRef]

| Tanner Stage | Breast (female) | Pubic hair (female, male) | Genitalia (male) |
|---|---|---|---|
| I | Preadolescent | None | Preadolescent |
| II | Breast bud palpable under the areola | Sparse, long, straight | Enlargement of scrotum/testes |
| III | Breast tissue palpable outside areola; no areolar development | Darker, curling, increased amount | Penis grows in length; testes continue to enlarge |
| IV | Areola elevated above the contour of the breast, forming a “double scoop” appearance | Coarse, curly, adult type | Penis grows in length/breadth; scrotum darkens, testes continue to enlarge |
| V | Areolar mound recedes into single breast contour with areolar hyperpigmentation, papillae development, and nipple protrusion | Adult, extend to thighs | Adult shape/size |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



