
Submitted:
05 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
Background: Peyronie’s disease (PD) represents a challenging urological disease, due to not optimal post-operative surgical outcomes. We aim to evaluate if vacuum erection devices (VED) treatment before pe-nile curvature surgery is able to improve the post-operative surgical outcomes. Methods: All enrolled patients were assigned to the following groups: a) treatment group, VED treatment (3 times per week) starting 3 months before surgery and (3 times per week) one months after surgery and b) control group, VED treatment (3 times per week) one months after surgery. Follow-up urologic visits were scheduled at 3 and 6 months after surgery and the two groups were compared. Results: Thirty-eight patients have been enrolled (median age 67 years, 57-74, IQR), 20 in the treatment group and 18 in the control group. At the follow-up visits, the two groups are different in terms of IIEF-5 (26 vs 24; p=0.02), ‘yes’ to SEP2 and 3 (85% vs 55%; p<0.001, 85% vs 50%; p<0.001, respectively) and PDQ (-16 vs -11; p=0.03). Complete correction of penile curvature was achieved in 36 patients (94.7%). In the treatment group, no hourglass deformity has been reported, while in the control group 1 patient reported a mild hourglass deformity. In the treatment group, we obtained a longer total penile length (median +1.5 cm). The overall satisfaction rate was 98% in the treatment group and 96% in the control group. Conclusions: The VED treatment before penile curvature surgery in patients affected by PD is able to improve the post-operative surgery.
Keywords:
Peyronie's Disease
; vacuum erection devices
; penile curvature
; surgery
; quality of life
1. Introduction
Peyronie’s disease (PD) represents a challenging andrological disease with an important impact on patients’ quality of life [1]. The social burden of the disease is high due to its prevalence among sexually active males, ranging between 0.4 and 20%, and its chronic evolution, with high frequency of recurrence and non-optimal efficacy of the current therapeutic strategies [2,3,4]. Moreover, its natural history is not fully understood [5]. The patients’ satisfaction and surgery outcomes are not always optimal and several medical and surgical treatment options have been purposed and introduced in everyday clinical practice [4]. In the chronic stable phase of the disease, surgery remains the recommended approach [6]. The most common surgical technique for the management of PD is the plaque incision and grafting with a reported success rate between 87.5% and 100% [4]. The use of vacuum erection devices (VED) is recommended due to its capability to obtain dilation of cavernous sinuses, decreased retrograde venous blood flow and increased arterial inflow [7]. International guidelines suggest to use VED as part of multimodal approach, highlighting that combination therapy is more effective when compared to monotherapy [8]. Here, we focus our attention on the role of VED as adjuvant therapy before surgery in patients with chronic stable phase of the disease. Even under the same pre-operative conditions, such as size and location of penile plaques, degree of curvature, complex deformities (hinge or hourglass), penile length and the presence or absence of erectile dysfunction, the surgical outcome and patient’s satisfaction is not fully associated to the surgical technique and surgeon’s skill. Several Authors highlighted the role of post-operative penile rehabilitation to improve surgical outcomes by using VED or penile traction devices [8,9,10]. Moreover, the use of VED have been recommended for the management of post-operative complications such as penile shorten, penile deformity or residual curvature [10]. On the basis of these considerations, we aim to evaluate if VED treatment before penile curvature surgery is able to improve the post-operative surgical outcomes.
2. Materials and Methods
Study design and patient’s population
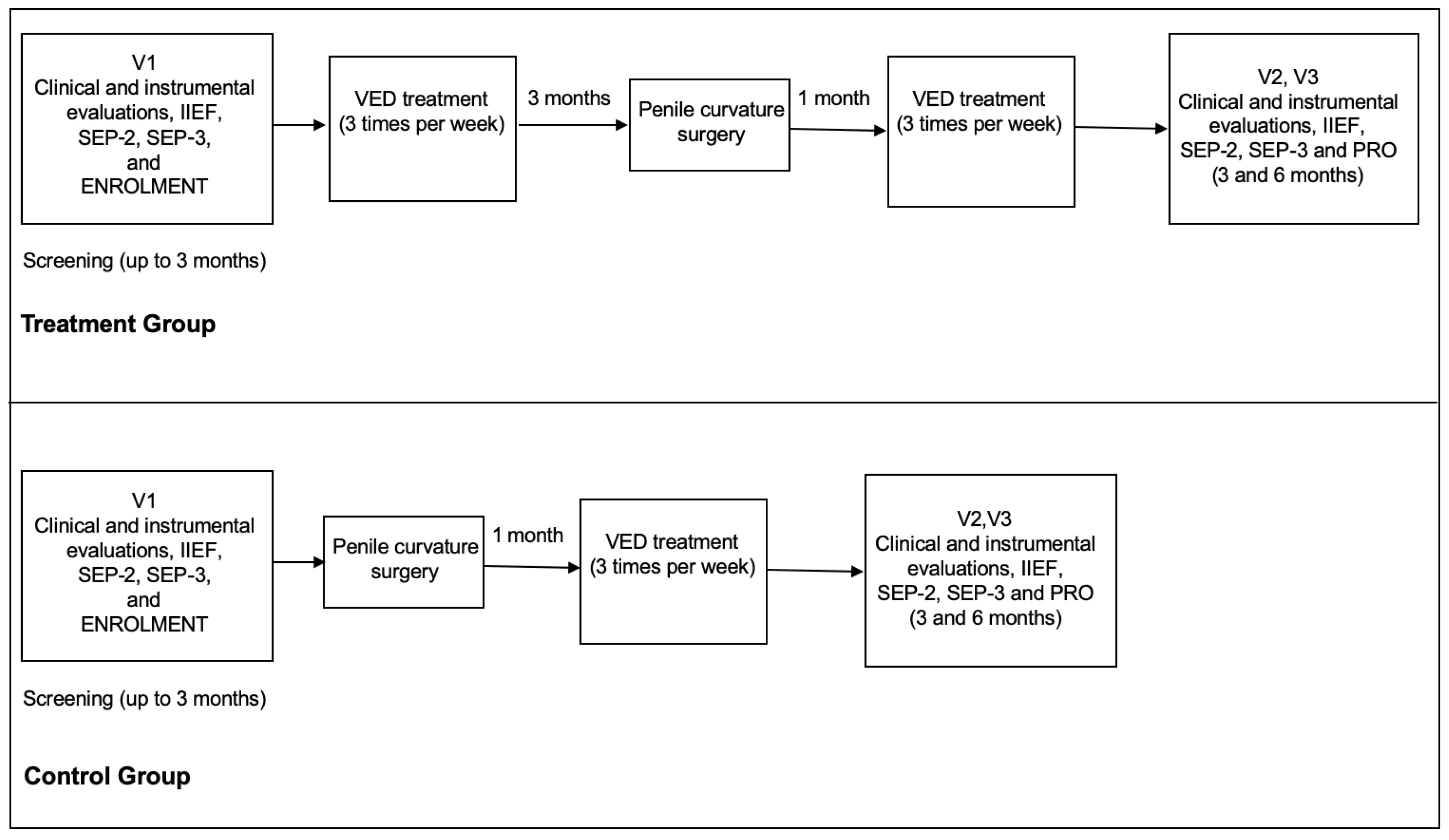
In this study we included all consecutive adult patients with Peyronie’s disease who were treated by plaque incision and bovine pericardium grafting between January 2020 and September 2022 in an Italian referral center. All patients underwent 3 months VED treatment (3 times per week) before penile curvature surgery and then VED treatment (3 times per week) starting one month after surgery. At 6 months after surgical procedure all patients were scheduled for follow-up visit with dedicated questionnaires. The results of this group of patients have been compared with a cohort of patients who were treated by plaque incision and bovine pericardium grafting between January 2017 and December 2019 at the same institution treated with VED treatment only after surgical treatment. The two groups were compared in terms of patients’ satisfaction and surgical outcome.
Figure 1.
The figure 1 shows the study schedule.
Inclusion and exclusion criteria
Patients were considered for this study if they match the following characteristics: to have a chronic stable phase of the disease, to be refractory to conservative management, to have a severe curvature (> 60°) or penile complex deformity (hourglass or hinge) without any evidence of erectile dysfunction (IIEF-15 more than 22). We excluded all patients with PD in active phase, erectile dysfunction, congenital penile curvature or significant medical conditions.
Preoperative assessment and VED adjuvant treatment
All patients, included both groups, underwent preoperative evaluation with detailed medical history, physical examination, the International Index of Erectile Function Questionnaire (IIEF-5), Peyronie's Disease Questionnaire (PDQ), measurement of penile length during relaxation and erection, and penile Doppler ultrasound during prostaglandin-induced erection, in line with the recommendations of the international guidelines8. Penile Doppler ultrasound has been performed by intra-cavernous injection of 10 mcg alprostadil to assess the angle and direction of penile curvature. After the inclusion in the study, all patients, were counselled about the use of VED, according to the group. All patients underwent vacuum erection therapy by using the same device from MEDIS, Medical Service - Rozzano - Milan - Italy.
Surgical treatment and post-operative management
All surgical procedures have been performed by the same urologists (T.C., D.T.) by using the same surgical technique, in the both treatment periods. In brief, after penile degloving, the Buck’s fascia has been carefully divided and the dorsal neurovascular bundle mobilized. Erection has been intraoperatively obtained by injecting 0.9% NaCl into the corpus cavernosum. A double "Y" shape incision has been performed at the maximum curvature. The wound edges were expanded as much as possible, the distance between the edges of the defect measured by ruler. Bovine pericardium graft (Bovine pericardium tissue – Baxter – Italy) was placed on the resulting defect and was sutured with continuous running sutures with the MonoPlus® No. 4 (B. Braun - Germany). No oversizing of the graft was performed. Artificial erection has been induced in order to check the curvature correction and the presence of residual penile deformities. The Buck's fascia and the skin were, then, sutured and a compressive penile bandage has been performed after Foley catheter placement. The catheter and penile bandage were removed 24 hours after surgery and the patient immediately discharged. All patients underwent phosphodiesterase type-5 inhibitors therapy (tadalafil 5 mg 1 tablet per day) for 3 months starting immediately after surgery. Moreover, starting 30 days after surgery, all patients have been asked to continue VED therapy (3 times per week). All patients have been asked to avoid sexual intercourses for 6 weeks. Follow-up visits have been scheduled at 30 days, 3, and 6 months after surgery. The 30 days visit has been performed to test short-term surgical complications, to check the adherence to phosphodiesterase type-5 inhibitors therapy and to counsel the patients for the future therapy and follow-up visits. At 3- and 6-months follow-up visits, all patients underwent urological visit, penile length and evaluation of eventual residual curvature and penile deformity, by using self-made photography with erected penis. Moreover, all patients underwent IIEF-5 questionnaires and Patient Reported Outcomes (PROs).
Outcome Measurements
The primary outcome was to evaluate superiority of neo-adjuvant therapy with VED in patients candidates to penile curvature surgery when compared with penile curvature surgery alone, in terms erectile function domain score (International Index of Erectile Function, PDQ and SEP-2 and SEP-3) and patients satisfaction (PROs). Moreover, the penile length change has been considered a secondary outcome measure.
Questionnaires
Efficacy measures were the International Index of Erectile Function (IIEF) and the Sexual Encounter Profile (SEP) questionnaires [11,12,13], collected for each patient at the baseline and at the end of each treatment phase and at the follow-up evaluation. The Peyronie’s Disease questionnaire (PDQ) has been used, too [14].
Statistical and ethical considerations
Demographic and baseline characteristics have been presented as numbers and percentages. Numeric variables have been showed as mean standard deviation when normally distributed, and median and interquartile range in case of not normal distribution. The McNemar’s test was used to compare categorical variables. Friedman test has been used in case of not normally distributed variables. The change between the two groups in the EF domain score and EF questions 3 and 4 scores were analyzed using a covariance (analysis of covariance) model with treatment and study site as the main factors and the baseline EF domain score as the covariate. Responses to the SEP questions were analyzed using a one-way analysis of variance with treatment as a factor. Two-tailed p values less than 0.05 were considered statistically significant. All statistical analyses were performed using SPSS 22 for Apple-Macintosh (SPSS, Inc. Chicago, IL, USA). However, all anamnestic, clinical and laboratory data containing sensitive information about patients were de-identified to ensure the analysis of anonymous data only. The de-identification process was performed by non-medical staff by means of dedicated software15. The study was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki.
3. Results
Twenty patients have been enrolled from January 2020 to September 2022 (treatment group) (median age 67 years, 57-74, Interquartile range (IQR)) and compared with 18 patients enrolled from January 2017 and December 2019 (control group) (median age 66 years, 54-75, IQR).
3.1. Clinical characteristics of the study participants at the enrolment
Dorsal curvature was the most frequent site of curvature (65%). The median curvature at preoperative evaluation was 65° (ranging from 60 to 80°). All patients had stable-phase PD, at least for the preceding 12 months. Each patient received a previous medical/conservative treatment without any clinical success. No patient received VED treatment alone or in association with other therapies before the enrolment. The IIEF-15 median score was 23, ranging from 22 to 24. The median erect penile length at preoperative evaluation was 114 mm (110-140, IQR).

Table 1.
Clinical and anamnestic characteristics of all patients at the enrolment.
| Treatment | Control | p | |
| No. of patients | 20 | 18 | |
| Age (years) | 1 | ||
| Median (IQR†) | 67 (57-74) | 66 (54-75) | |
| Marital status | 0.99 | ||
| Married | 18 (90) | 17 (94.4) | |
| Single | 2 (10) | 1 (5.6) | |
| Duration of disease - time from onset (months) | 0.89 | ||
| Median (IQR†) | 13 (12-22) | 14 (13-21) | |
| Penile curvature | 0.94 | ||
| Angle, degrees (IQR†) | 66 (60-80) | 64 (60-80) | |
| Direction, no. | |||
| dorsal | 13 (65) | 12 (66.6) | |
| lateral | 4 (20) | 5 (27.7) | |
| ventral | 3 (15) | 1 (5.7) | |
| Penile deformity | 0.77 | ||
| Hourglass | 3 (15) | 2 (11.1) | |
| Penile length (cm) | 0.83 | ||
| Median (IQR†) | 113 (110-140) | 115 (110-140) | |
| Plaque size (mm) | 0.94 | ||
| Median (IQR†) | 21 (15-31) | 22 (16-35) | |
| IIEF-15* | 0.82 | ||
| Median (IQR†) | 24 (22-24) | 22 (22-24) | |
| PDQ° | 0.75 | ||
| Median (IQR†) | 28 (19-35) | 28 (18-34) | |
| PDQ-Penile Pain | 13 (1-23) | 13 (1-23) | |
| PDQ-Symptom Bother | 10 (5-16) | 9 (4-16) | |
| PDQ-Psychological and Physical Symptoms | 3 (0-20) | 4 (0-20) | |
| SEP-2§ | 0.65 | ||
| Yes | 11 (55) | 9 (50) | |
| SEP-3§ | 0.84 | ||
| Yes | 10 (50) | 9 (50) | |
The table 1 shows all clinical and anamnestic characteristics of all patients at the enrolment. IQR†= interquartile range; IIEF-15*= International Index of Erectile Function; PDQ°= Peyronie’s Disease questionnaire; SEP§= Sexual Encounter Profile. Data in parentheses are percentage unless otherwise specified.
3.2. Intra-operative and peri-operative findings
No clinically significant differences have been reported between the VED treatment starting and the surgical time in the both groups. The median operative time was 105 minutes (84-132, IQR). Intraoperative complications were very low, in only one case a lesion of neurovascular bundle occurred. The lesion has been repaired with VICRYL® No. 4 (ETHICON SPA Pomezia - Rome).
Table 2.
Intra-operative and peri-operative findings.
| Treatment | Control | p | |
| Operative time (min) | 0.98 | ||
| Median (IQR†) | 105 (84-132) | 103 (84-128) | |
| Complete curvature correction | 0.57 | ||
| No. | 19 (95) | 17 (94.4) | |
| Penile length (cm) | 0.41 | ||
| Median (IQR†) | 116 (112-140) | 114 (110-140) | |
| Complications | 0.95 | ||
| Haematoma | 3 (15) | 3 (16.6) | |
| Oedema | 9 (45) | 8 (40) | |
The table 2 shows all intra-operative and peri-operative findings. IQR†= interquartile range. Data in parentheses are percentage unless otherwise specified.
Complete curvature correction (residual curvature < 10°) has been achieved in 36 patients (94.7%). The median penile length obtained at the end of the surgical procedure was 116 mm (112-140, IQR).
3.3. Follow-up results
All patients regularly used the VED. A statistically significant improvement of IIEF-5 (26 vs 24; p=0.02), ‘yes’ to SEP2 and 3 (85% vs 55%; p<0.001, 85% vs 50%; p<0.001, respectively) has been reported between the two groups. Moreover, the PDQ overall score significantly improved between the two groups (-16 vs -11; p=0.03). Thirty-five patients maintained a complete correction of penile curvature (zero degrees) at 6 months (92.1%). In the treatment group, no hourglass deformity has been reported. On the other hand, in the control group 1 patient reported a mild hourglass deformity, at 6 months of follow-up. Finally, in the treatment group, we obtained a longer total penile length (median +1.5 cm) in comparison with the control group. The overall satisfaction rate was 98% in the treatment group and 96% in the control group, on the basis of the Patient Reported Outcomes. Twenty-five patients (65.7%) had normal penile sensitivity while 13 (34.3%) reported mild hypesthesia. Fifteen patients (39.4%) continued to use on-demand tadalafil 20 mg for 6 months from surgery.
Table 3.
Clinical and questionnaires results at 12 months follow-up visit.
| Treatment | Control | p | |
| VED° use (regular) | 1 | ||
| No. | 20 (100) | 18 (100) | |
| Patient Reported Outcomes | 0.02 | ||
| Overall satisfaction | 19 (95) | 14 (77.7) | |
| Penile sensitivity | 0.03 | ||
| Normal | 14 (70) | 11 (61.1) | |
| IIEF-15* pre- |
0.02 |
||
| Median (IQR) | 24 (22-24) | 22 (22-24) | |
| IIEF-15* post- | |||
| Median (IQR) | 26 (22-24) | 24 (22-24) | |
| p = 0.03 | |||
| SEP-2§ pre- |
<0.001 |
||
| Yes | 11 (55) | 9 (50) | |
| SEP-2§ post- | |||
| Yes | 17 (85) | 12 (66.6) | |
| p < 0.001 | |||
| SEP-3§ pre- |
<0.001 |
||
| Yes | 11 (55) | 9 (50) | |
| SEP-3§ post- | |||
| Yes | 17 (85) | 13 (72.2) | |
| p < 0.001 | |||
| PDQ° overall - pre- |
0.03 |
||
| Median (IQR) | 28 (19-35) | 28 (18-34) | |
| PDQ° overall - post- | |||
| Median (IQR) | 12 (8-20) | 17 (16-28) | |
| p < 0.001 | |||
The table 3 shows all clinical and questionnaires results at 6 months follow-up visit. VED°= vacuum erection devices; IIEF-15*= International Index of Erectile Function; SEP§= Sexual Encounter Profile; PDQ°= Peyronie’s Disease questionnaire. Data in parentheses are percentage unless otherwise specified.
4. Discussion
The use of xenografts for the surgical management of PD has recently become popular and commonly used [16] even if this approach is associated with some possible risks such as penile shortening, de novo erectile dysfunction, glans hypoaesthesia or anaesthesia and residual or recurrent curvature [10,17]. In this sense, the use of vacuum devices could be useful for reduce the risk of complications and improve the patients’ outcome and satisfaction.
Main findings
Here, we demonstrated that the VED treatment before penile curvature surgery in patients affected by PD is able to improve the post-operative surgery, in terms of patients’ satisfaction and surgical outcome. To the best of our knowledge, this is the first study evaluating the role of VED treatment as adjuvant therapy to improve surgical outcome in PD patients.
Results in the context of current knowledge
The authors of the ESSM Position Statement on Surgical Treatment of Peyronie's Disease highlighted that the aim of surgery is to improve penile deformities whilst minimizing any adverse outcomes [10]. In order to reduce the risk of complications and improve the outcome of surgery, penile traction therapy and VED techniques have been proposed [18]. VED therapy is able to improve dilation of cavernous sinuses, retrograde venous blood flow, increased arterial inflow resulting in decreasing of hypoxia-inducible factor-1a, transforming growth factor (TGF)-b1, collagenase, and apoptosis and increases in endothelial nitric oxide synthase and a-smooth muscle actin [18,19]. Only one study with limited number of enrolled patients has been published on the adjunctive use of a VED after incision and grafting surgery for PD [20]. In this study, the patients were encouraged to use a VED 30 minutes daily for 6 months, starting 1 months after surgery [20]. The authors demonstrated that patients treated with VED gained 2 inches in penile length compared with 1 inch in the man not using VED therapy. In this study, the authors evaluated the role of VED therapy after surgery as adjuvant procedure. In our experience, the use of VED beginning 3 months before the surgery is able to improve surgical outcome, probably by inducing the dilation of cavernous sinuses and increased arterial inflow. Another aspect to discuss is the role of VED in the management of penile curvature regardless of surgery. In our experience, no clinically significant differences have been reported between the VED treatment starting and the surgical time in the both groups, demonstrating that the patients’ satisfaction is related to the use of VED treatment before penile curvature surgery.
Strengths and limitations of this study
There are some limitations associated with this study. The nature of the study, retrospective and non-randomized clinical trial should be considered as a limitation. Strengths of this study are the fact that the study has been conducted in high volume andrological center and the use of a standardized surgical approach to the PD.
5. Conclusions
In conclusion, the VED treatment before penile curvature surgery in patients affected by PD is able to improve the post-operative results in terms of patients’ satisfaction and surgical outcome. Further studies with randomized and controlled feature are required in order to confirm our results. Moreover, future studies investigating the histologic and molecular changes in tunica albuginea and corpora cavernosa after VED could give informative data on the role of VED as adjuvant therapy of surgery in PD patients.
Author Contributions
Conceptualization, T.C. and M.C.; methodology, D.T.; formal analysis, P.V.; investigation, T.C.; data curation, M.P., C.C.; writing—original draft preparation, T.C.; writing—review and editing, P.G.; supervision, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study is a retrospective study involving patients who had undergone standard management of IPP. No ethical committee approval has been required by Italian bylaw. However, all anamnestic, clinical and laboratory data containing sensitive information about patients were de-identified to ensure the analysis of anonymous data only. The de-identification process was performed by non-medical staff by means of dedicated software. The study was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki.
Informed Consent Statement
Not applicable. All patients signed a standard informed consent before surgical procedure. No other informed consent has been required for this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moisés da Silva, G.V.; Dávila, F.J.; Rosito, T.E.; Martins, F.E. Global Perspective on the Management of Peyronie's Disease. Front Reprod Health 2022, 4:863844. [CrossRef]
- Kadioglu, A.; Dincer, M.; Salabas, E.; Culha, M.G.; Akdere, H.; Cilesiz, N.C. A Population-Based Study of Peyronie's Disease in Turkey: Prevalence and Related Comorbidities. Sex Med 2020, 8:679–85. [CrossRef]
- Stuntz, M.; Perlaky, A.; des Vignes, F.; Kyriakides, T.; Glass, D. The Prevalence of Peyronie’s Disease in the United States: A Population-Based Study. PLoS ONE 2016, 11(2):e0150157. [CrossRef]
- Ainayev, Y.; Zhanbyrbekuly, U.; Gaipov, A.; Suleiman, M.; Kadyrzhanuly, K.; Kissamedenov, N.; Zhaparov, U.; Akhmetov, D.; Khairli, G. Surgical Reconstruction of Penile Curvature due to Peyronie's Disease by Plaque Incision and Buccal Mucosa Graft. J Sex Med 2021, 18(7):1308-1316. [CrossRef]
- Milenkovic, U.; Ilg, M.M.; Cellek, S.; Albersen, M. Pathophysiology and Future Therapeutic Perspectives for Resolving Fibrosis in Peyronie’s Disease. Sex Med Rev 2019, 7(4):679–689. [CrossRef]
- Chung, E.; Gillman, M.; Tuckey, J.; La Bianca, S.; Love, C. A clinical pathway for the management of Peyronie’s disease: Integrating clinical guidelines from the International Society of Sexual Medicine, American Urological Association and European Urological Association. BJU Int 2020, 126(Suppl 1):12–17. [CrossRef]
- Broderick, G.A.; McGahan, J.P.; Stone, A.R.; White, R.D. The hemodynamics of vacuum constriction erections: Assessment by color Doppler ultrasound. J Urol 1992, 147(1):57-61. [CrossRef]
- European Association of Urology guidelines on Sexual and Reproductive Health. https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Sexual-and-Reproductive-Health-2022_2022-03-29-084141_megw.pdf. Access on 3th March 2023.
- Rybak, J.; Papagiannopoulos, D.; Levine, L. A retrospective comparative study of traction therapy vs. no traction following tunica albuginea plication or partial excision and grafting for Peyronie's disease: Measured lengths and patient perceptions. J Sex Med 2012, 9(9):2396-403. [CrossRef]
- Osmonov, D.; Ragheb, A.; Ward, S.; Blecher, G.,; Falcone, M.; Soave, A.; Dahlem, R.; van Renterghem, K.; Christopher, N.; Hatzichristodoulou, G.; Preto, M.; Garaffa, G.; Albersen, M.; Bettocchi, C.; Corona, G.; Reisman, Y. ESSM Position Statement on Surgical Treatment of Peyronie's Disease. Sex Med 2022, 10(1):100459. [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49(6):822-30. [CrossRef]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54:346–351. [CrossRef]
- Shaw, J.W.; Reardon, G.; Sandor, D.W.; Rosen, R.C.; Ferguson, D.M. Validation of stopwatch measurements of erection duration against responses to the sexual encounter profile and international index of erectile Function in patients treated with a phosphodiesterase type 5 inhibitor. J Sex Med 2010, 7(3):1147-59. [CrossRef]
- Hellstrom, W.J.G.; Feldman, R.; Rosen, R.C.; Smith, T.; Kaufman, G.; Tursi, J. Bother and distress associated with peyronie’s disease: Validation of the Peyronie’s disease questionnaire. J Urol 2013, 190:627-634. [CrossRef]
- Neamatullah, I.; Douglass, M.M.; Lehman, L.W.; Reisner, A.; Villarroel, M.; Long, W.J.; Szolovits, P.; Moody, G.B.; Mark, R.G.; Clifford, G.D. Automated de-identification of free-text medical records. BMC Med Inform Decis Mak 2008, 8:32. [CrossRef]
- Fernández-Pascual, E,; Manfredi, C.; Torremadé, J.; Ibarra, F.P.; Geli, J.S.; Romero-Otero, J.; García-Baquero, R.; Poblador, A.F.; Barbará, M.R.; Campos-Juanatey, F.; Rojo, A.E.; Iribarren, I.M.; Rodríguez, J.C.; Martínez-Salamanca, J.I. Multicenter Prospective Study of Grafting With Collagen Fleece TachoSil in Patients With Peyronie's Disease. J Sex Med 2020, 17(11):2279-2286. [CrossRef]
- Garaffa, G.; Trost, L.W.; Serefoglu, E.C.; Ralph, D.; Hellstrom, W.J. Understanding the course of Peyronie's disease. Int J Clin Pract 2013, 67(8):781-8. [CrossRef]
- Avant, R.A.; Ziegelmann, M.; Nehra, A.; Alom, M.; Kohler, T.; Trost, L. Penile Traction Therapy and Vacuum Erection Devices in Peyronie's Disease. Sex Med Rev 2019, 7(2):338-348. [CrossRef]
- Yuan, J.; Lin, H.; Li, P.; Zhang, R.; Luo, A.; Berardinelli, F.; Dai, Y.; Wang, R. Molecular mechanisms of vacuum therapy in penile rehabilitation: A novel animal study. Eur Urol 2010, 58(5):773-80. [CrossRef]
- Lue, T.F.; El-Sakka, A.I. Lengthening shortened penis caused by Peyronie's disease using circular venous grafting and daily stretching with a vacuum erection device. J Urol 1999, 161(4):1141-4. PMID: 10081856. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



