
Submitted:
25 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Syphilis continues to be a significant global health concern, and understanding the latest advancements in immunology and pharmacological treatment is crucial for effective disease management. This review article provides an in-depth exploration of these advancements, aiming to contribute to the growing body of knowledge on syphilis research. The epidemiology of syphilis sets the stage for this review, highlighting the persistent burden of the disease worldwide. Current trends and challenges in disease control are discussed, shedding light on the need for comprehensive prevention strategies and improved surveillance systems. The immunological aspects of syphilis are the focus of this review. The intricate interplay between the host immune response and the evasive strategies employed by Treponema pallidum, the causative agent of syphilis, are explored. These include the mechanisms of immune evasion, the role of adaptive and innate immunity, and the development of immune-mediated tissue damage. The article also highlights advancements in diagnostic methods, with emphasis on the importance of accurate and timely detection. From traditional serological tests to the emergence of novel molecular and point-of-care assays, these developments have significantly improved the efficiency and accuracy of syphilis diagnosis. In terms of pharmacological treatment, the review covers the current recommendations and emerging strategies for managing syphilis infections. The challenges posed by antimicrobial resistance are addressed, emphasizing the importance of appropriate treatment regimens and close monitoring of therapeutic efficacy. Looking to the future, this review highlights the potential of vaccine development as a preventive measure against syphilis. Promising vaccine candidates and ongoing research efforts are discussed, offering hope for an effective means of disease prevention. In conclusion, this comprehensive review explores the advancements in syphilis research, from the understanding of immunological complexities to the development of innovative treatment strategies. By collectively advancing our knowledge, we can strive towards better disease management and minimize the impact of syphilis on global public health.

Keywords:
Disease management
; Epidemiology
; Immune response
; Global health
; Syphilis treatment.
1. Introduction
Syphilis, caused by the spirochete bacterium Treponema pallidum, remains a significant global health concern with substantial morbidity and mortality [1]. Despite considerable progress in understanding the disease over the years, challenges in effectively controlling and eradicating syphilis still persist. The emergence of antibiotic-resistant strains, complex immunological interactions, and the lack of an effective vaccine, underscores the need for innovative research to address this longstanding public health issue [2,3].
Immunology plays a pivotal role in syphilis research, as understanding the intricate interplay between the host immune response and T. pallidum infection is essential for identifying novel diagnostic methods, developing effective vaccines, and designing targeted immunotherapies [4]. Unravelling the mechanisms by which the bacterium evades the host's immune defenses and manipulates the inflammatory response is critical for devising strategies to curtail disease progression [5,6].
In parallel, pharmacological interventions are being explored to complement traditional antibiotic treatments and address challenges posed by antibiotic resistance. Novel drug targets are being identified through an in-depth understanding of the bacterium's pathogenesis, metabolism, and interactions with the host [7]. This quest for new pharmacological avenues aims to identify agents that can disrupt the bacterium's survival mechanisms, halt disease progression, and potentially eradicate latent infections [8].
In parallel, pharmacological interventions are being explored to complement traditional antibiotic treatments and address challenges posed by antibiotic resistance. Novel drug targets are being identified through an in-depth understanding of the bacterium's pathogenesis, metabolism, and interactions with the host. This quest for new pharmacological avenues aims to identify agents that can disrupt the bacterium's survival mechanisms, halt disease progression, and potentially eradicate latent infections [7,8,9].
This article serves as a comprehensive review, providing an in-depth exploration of the latest advancements in syphilis research, focusing on cutting-edge developments in immunology and pharmacology. Within these pages, we will delve into the ongoing efforts of scientists who relentlessly strive to address unanswered questions, refine existing approaches, and propel the field forward. Our review will place a particular emphasis on the profound implications of a comprehensive understanding of immunological responses and the emergence of novel pharmacological interventions. Ultimately, the goal is to explore potential strategies that can effectively curb the global burden of syphilis and pave the way for its control and eradication.
2. Epidemiology of Syphilis: Current Trends and Future Challenges
The incidence of syphilis refers to the number of new cases occurring within a specific population during a given period. The reporting and surveillance of new infections are essential for tracking the dynamic nature of the disease. Incidence rates can vary considerably across different regions, reflecting disparities in healthcare access, education, and risk behaviors [1,10].
In recent years, the WHO has reported an alarming rise in syphilis incidence in various parts of the world. Particularly concerning is the increase among key populations, including men who have sex with men (MSM), women of reproductive age, and pregnant women. This upsurge in cases demands targeted public health interventions to curb transmission and prevent adverse outcomes, such as congenital syphilis [1,11].
Prevalence represents the total number of individuals with syphilis within a given population at a specific time. Unlike incidence, prevalence encompasses both newly diagnosed and existing cases. High prevalence rates suggest a significant burden of the disease within a population and may indicate the need for enhanced screening and treatment efforts [12].
The prevalence of syphilis varies considerably based on geographical location, socio-economic conditions, and cultural practices. In some regions, pockets of high prevalence exist among vulnerable populations with limited access to healthcare services and sexual health education [13,14].
Identifying at-risk populations is essential for effective syphilis control and prevention strategies. As mentioned earlier, MSM, women of reproductive age, and pregnant women are among the key populations facing heightened risks. Additionally, individuals engaged in high-risk sexual behaviors, such as unprotected intercourse and having multiple sexual partners, are also at increased risk of contracting syphilis [1,11,15]. Moreover, individuals with substance use disorders, especially those using methamphetamine and other stimulants, are experiencing elevated syphilis rates due to their involvement in risky sexual networks [16,17].
Accurate epidemiological data on syphilis can be challenging to obtain due to several factors. Underreporting cases, especially in resource-limited settings, may lead to an underestimation of the true burden of the disease. Furthermore, asymptomatic or mild presentations of syphilis can go undetected, resulting in delayed diagnosis and continued transmission [1,18].
Despite these challenges, ongoing efforts by the WHO and other health organizations aim to strengthen syphilis surveillance systems and improve data collection, providing a more comprehensive understanding of the epidemiology and enabling evidence-based interventions [19,20].
The epidemiology of syphilis, characterized by varying incidence and prevalence rates, highlights the need for robust surveillance and targeted public health interventions. Analyzing data from authoritative sources, such as the WHO, provides valuable insights into the current trends, at-risk populations, and challenges faced in syphilis control. By implementing evidence-based strategies, promoting sexual health education, and ensuring accessible healthcare services, global health authorities can work towards reducing the incidence and prevalence of syphilis and its associated burden on public health [11,21].
3. Diagnosis of Syphilis: Advances and Challenges
The symptoms of syphilis are not commonplace or easy to perceive. This makes it necessary to diagnose this disease based on the patient's clinical and sexual history through physical examinations, laboratory tests and in some situations, radiological examinations [12].
The bacterium, Treponema pallidum, is a pathogen that is difficult to grow in culture, and there are many direct and indirect tests for the identification of contamination by this spirochete. Direct tests assess the specific spiral morphology of T. pallidum and are used in the diagnosis of early syphilis. However, not a reasonable amount of the bacteria is found in the smears of the cancer, since this lesion heals quickly and spontaneously [22].
As a direct test, we have the dark field microscopy test, where an optical microscope is used to visualize the morphology of the treponema in a chancre scraping slide taken from a patient with primary syphilis. This test has a sensitivity of 71 to 100%, and is fast, simple and inexpensive, but to avoid subjectivity in the results, it must be performed by a well-trained technician [22,23,24]. Another direct test is the fluorescent antibody staining technique which detects pathogenic treponema using an antigen-antibody reaction, suitable for lesion smears, concentrated fluids and tissue brushes. The type of antibody used determines the specificity of this method since the monoclonal antibody H9-1 specific for T. pallidum does not react with other commensal spirochetes. The biggest restriction of this test is finding reliable companies that commercialize T. pallidum-specific antibodies [25,26,27].
Immunohistochemistry tests are sensitive and specific for the detection of syphilis, being an excellent complementary test if necessary. This technique exposes the T. pallidum epitope in tissue biopsies by heat induction, followed by incubation with anti-T. pallidum immunoglobulin G (IgG) antibodies. Then, biotinylated rabbit antibodies for IgG are added, and, finally, they are incubated with peroxidase-conjugated avidin-biotin complex, and then the reaction with T. pallidum is observed. As a limitation, in this test, there may be a cross-reaction between T. pallidum and other spirochetes, such as Borrelia burgdorferi and with intestinal spirochetes [28].
The most prevalent test for the diagnosis of syphilis nowadays is serology to detect antibodies to T. pallidum, using nontreponemal tests (NTT) and treponemal tests (TT) [12,29]. NTTs are the most performed in laboratory routines since they are effective, simple to perform, fast and low cost [30]. However, in some diseases or conditions, such as pregnancy, autoimmune diseases, infections, and others, there is a risk of false-positive results. NTTS tests include the rapid plasma reagin test, Toluidine Red Unheated Serum Test (TRUST), and the Venereal Disease Research Laboratory (VDRL) test, which quantify levels of immunoglobulin M or G anti-lipid antibodies produced in response to lipoidal material released by host cells or cardiolipin from T. pallidum [31].
Tuddenham and co-worker [32], described that the serum sensitivity of NTTs is 62 to 78% for cases of primary syphilis, 97 to 100% for secondary syphilis and 82 to 100% for early latent syphilis. For tertiary syphilis, the sensitivity ranges from 47% to 64%. As a non-treponemal test, RPR and VDRL are used as additional tests. RPR uses serum and plasma samples from various stages of syphilis patients. VDRL is also used in patients with neurosyphilis from samples collected from cerebrospinal fluid (CSF) [33].
Another line of serological tests is the treponemal tests (TTs), which have high sensitivity in secondary syphilis (approximately 100%), 95.2–100% sensitivity in early latent syphilis, and 86.8–98.5% sensitivity in syphilis late latent [34]. Other features of TTs include repairing NTT deficiencies in early syphilis, as TT can become positive at the onset of primary cancer. On the downside, none of the TTs can assess the effectiveness of treatment (as they do not distinguish the active stage from a previously treated infection) since treponemal antibodies persist throughout life in patients with syphilis [22].
TTs, which include the absorbed fluorescent treponemal antibody absorption (FTA-ABS), T. pallidum particle agglutination, T. pallidum particle agglutination assay (TPHA), enzyme immunoassay (EIA) and chemiluminescence immunoassay (CLIA), detect antibodies against T. pallidum proteins [22].
Using an indirect immunofluorescent stain, FTA-ABS mixes a solvent (extract of a non-pathogenic Reiter's treponema) to the contaminated serum and exposes the Nichols strain antigens. Anti-human IgG (Fc) FITC-Labeled antibody is added and combined with the patient's antibodies. In a positive result, the presence of antibodies to T. pallidum is visible by fluorescence microscopy [35]. Although it can yield variable results due to variations in equipment, reagents and misinterpretation, FTA-ABS has high sensitivity [22,30].
The TPPA and TPHA tests are indirect agglutination assays that range from 82% to 100% and have a specificity of 99%. Surface antigens from T. pallidum are coated on red blood cells or gelatine particles and react with serum. They are efficient assays that provide accurate results and meet high demands for screening patients with syphilis [12,22].
Using molecular techniques to detect infection by T. pallidum, the Nucleic Acid Amplification Technique (NAATs) has been widely used nowadays, and several molecular methods can be used, having as target genes the polA, tpp47, bmp genes, 16S rRNA gene, tmpC and tmpA. However, the main employees are polA, tpp47 and bmp (Centurion- [22,36,37,38,39].
To perform the NAATs, samples of lesions are used, including genital, anal or oral ulcers, superficial skin eruptions, tissue lesions and mucosal erosion, when possible, since these types of samples are more difficult to obtain, and can be using body fluid samples such as blood, urine and saliva. The stage of syphilis and the molecular method used will determine the sensitivity and specificity of NAATs, which vary depending on the method as well as the stage of syphilis. Routine molecular methods are conventional PCR, nested PCR (nPCR), real-time PCR (qPCR), reverse transcription PCR (RT-PCR), and Loop-Mediated Isothermal Amplification (LAMP) assay [22].
Another method that can be used to detect syphilis is mass spectrometry (MS), but it is rarely used in clinical laboratories because data analysis is time-consuming and the equipment is expensive. This test detects T. pallidum proteins using a technique where chemical compounds are ionized into molecules and the mass-to-charge ratio is measured (m/z) [40].
4. Pharmacological Interventions
Syphilis patients were once subjected to prolonged treatment with arsenic and toxic compounds. Treatment failure are often associated with periodic and sporadic outbreaks [41,42]. The discovery of T. pallidum susceptibility to penicillin in 1943 redefined the treatment of this disease from toxic compounds to antibiotics. A decrease in cases of syphilis was recorded with the widespread use of penicillin. According to Janier et al., 2020, the control of syphilis over the past 50 years has been excellent compared to the prepenicillin era. Penicillin is considered treponemicidal at the at the concentration that is substantially lower than the maximally effective in vitro concentration (0.36 mg/L). The number of bacterial generation times (30–33 h) demands 7–10 days antimicrobial treatment duration to maintain a treponemicidal. Possible persistence of treponemes and relapses after successful treatment could justify longer duration of treatment or administration of long-acting BPG 2.4 million units which provides a treponemicidal penicillin concentration in blood for up to 21 days. Oral amoxicillin in association with probenecid results in treponemicidal drug levels within the CSF. The intramuscular or intravenous extended-spectrum cephalosporin (ESC) ceftriaxone are among the newer anti-treponemal antibiotics. Intramuscular (IM) benzathine penicillin G (BPG) does not achieve a sufficient concentration in cerebrospinal fluid (CSF), unlike aqueous penicillin G intravenously being recommended treatment for neurosyphilis. Allergic reactions are among some important limitations to the use of penicillin. Data for alternative antibiotics are mostly less robust. Non-penicillin antibiotics including tetracyclines and macrolides have been evaluated with interesting results. Patients with early syphilis who are allergic to penicillin may be treated with oral doxycycline or ceftriaxone (IM or IV) (Figure 1) [12]. The emergence of macrolide-resistant T. pallidum was reported with the empirical use of azithromycin [41]. Several studies have described emergence of resistance and clinical failures of azithromycin [43,44,45].
The WHO recommends the use of azithromycin for the treatment of syphilis only in settings where the prevalence of macrolide-resistant T. pallidum is known to be very low [42]. Alternatively, the development of protective vaccines is important. With the emergence of latent and resistant syphilis, repeated inoculation with γ-irradiated T. pallidum in rabbits has induced protective immunity [46,47]. Challenges with the discoveries of antibiotics, vaccines among others for syphilis treatment, are associated with the complexity of studying and researching T. pallidum, understanding of virulence and effective immunity against T. pallidum, inability to culture this bacterium, lack of experimentally T. pallidum infected rabbit, the need for many (number) of rabbits, long duration and high cost of studies. Treponemal susceptibility to linezolid, moxifloxacin, and clofazimine antibiotics, was reported in the culture of T. pallidum, rabbit infection and molecular analysis [48,49]. Haynes and co-workers [48] have demonstrated the utility of a novel approach to evaluate alternative antibiotics as potential candidates for efficacy testing in human clinical trials. The development of new antibiotics and the availability of vaccines are expected to increase therapeutic options and raise the hope for effective treatment of syphilis. The understanding of the immune system role, the severity of the syphilis-related disease, the indication of antimicrobials with correct spectrum of action, optimal dose, duration of treatment and efficacy among others are key to improved clinical outcomes [8,49].
5. Future Approaches in Syphilis Prevention and Control
Syphilis remains a global public health concern, necessitating continuous efforts to develop innovative strategies for prevention and control [12]. As the incidence of syphilis continues to rise in certain populations, there is an urgent need to explore new approaches to combat this sexually transmitted infection (STI). In this section, we will discuss potential future approaches in syphilis prevention and control, focusing on various aspects of research and intervention.
5.1. Development of Effective Vaccines
Researchers are continually exploring innovative vaccine formulations to enhance the immunogenicity and efficacy of syphilis vaccines. This includes investigating different adjuvants, delivery systems, and antigen combinations to elicit a robust and long-lasting immune response. Novel adjuvants and delivery platforms have shown promising results in preclinical studies, providing opportunities for more effective vaccine candidates in the future [46,50].
The development of a syphilis vaccine poses unique challenges due to the complex nature of the T. pallidum bacterium, which is the causative agent of syphilis [46,51]. Understanding the mechanisms of immune evasion employed by the bacterium is essential in guiding vaccine design. Researchers must address the antigenic variation of T. pallidum to ensure broad protection against different strains of the pathogen [52].
As the target population for a syphilis vaccine may differ from that of other STI vaccines, considerations must be given to factors such as age, gender, and risk behaviors. Determining the optimal age for vaccination, identifying high-risk groups, and tailoring the vaccine to address specific transmission patterns are critical aspects of designing an effective vaccination strategy [51,53].
Even after a successful vaccine candidate is identified, ensuring its widespread implementation and accessibility to vulnerable populations is critical. Overcoming logistical and financial barriers in vaccine distribution and uptake will be vital in achieving equitable protection against syphilis. The development of an effective syphilis vaccine is a complex yet vital endeavor to combat the rising burden of this sexually transmitted infection [51]. Advancements in vaccine formulation, understanding the challenges in vaccine design, considerations for target populations, ethical and safety aspects, collaboration, cross-protection potential, integration with existing control strategies, and vaccine implementation are all important factors that require attention in advancing syphilis vaccine research. A successful vaccine holds the promise of transforming syphilis prevention and control efforts, ultimately contributing to improved global sexual health outcomes [46,51,52].
5.2. Innovative Point-of-Care Diagnostics
Early and accurate diagnosis of syphilis is crucial for timely treatment and prevention of further transmission. Future approaches in syphilis diagnostics involve the development of innovative point-of-care tests that are rapid, sensitive, and easy to use. These advanced diagnostic tools could allow for on-the-spot testing in resource-limited settings, enabling early detection and immediate treatment initiation [54,55,56].
Early and accurate diagnosis of syphilis is crucial for timely treatment and prevention of further transmission. Future approaches in syphilis diagnostics involve the development of innovative point-of-care tests that are rapid, sensitive, and easy to use. These advanced diagnostic tools could allow for on-the-spot testing in resource-limited settings, enabling early detection and immediate treatment initiation [22,57,58].
Researchers are exploring various technologies to develop cutting-edge point-of-care tests for syphilis, including lateral flow assays, rapid immunochromatographic tests, loop-mediated isothermal amplification (LAMP), and nucleic acid amplification techniques. These technologies offer faster and more reliable results, making them suitable for use in diverse healthcare settings, including remote and resource-limited areas [59,60,61].
Moreover, the integration of multiple tests into a single platform, enabling simultaneous detection of different sexually transmitted infections, including syphilis, is being pursued. Multiplexed assays have the potential to enhance the efficiency of screening programs, reducing the burden on healthcare facilities and allowing for comprehensive testing in one simple procedure [62,63].
Additionally, future approaches in syphilis diagnostics are emphasizing user-friendliness and non-invasive sampling techniques. Saliva-based or urine-based point-of-care tests are being explored as alternatives to blood-based tests, making sample collection less invasive and more acceptable to individuals, particularly in high-risk populations. Integration of diagnostics with digital health solutions presents an exciting avenue for improving syphilis management [54,64]. Point-of-care tests equipped with connectivity features could allow for real-time data transmission to central databases, facilitating disease surveillance, monitoring treatment outcomes, and informing public health interventions [65].
5.3. Targeted Prevention Strategies
Targeted prevention strategies are vital components of syphilis control efforts, aiming to address the specific needs of high-risk populations and areas with elevated transmission rates. By focusing on key populations and tailoring interventions to their unique challenges, these strategies seek to optimize resource allocation and maximize the impact of preventive measures [20,66].
One of the primary targets of these prevention strategies is MSM and transgender individuals. These groups often face higher rates of syphilis transmission due to various factors, including social stigma, discrimination, and limited access to healthcare services. Tailored interventions for MSM and transgender individuals involve community engagement and peer-led initiatives to create safe spaces for discussions about sexual health and promote regular testing and treatment-seeking behavior [67].
In addition to MSM and transgender individuals, other high-risk populations, such as commercial sex workers, people who use drugs, and individuals with multiple sexual partners, also require focused prevention efforts. Partner notification and contact tracing are essential in these cases to identify undiagnosed cases and interrupt the transmission chain. Utilizing technology and community health workers can enhance the effectiveness of partner notification efforts and facilitate timely testing and treatment for those at risk [11,67].
Antenatal screening and prevention play a crucial role in preventing congenital syphilis, which occurs when syphilis is transmitted from an infected mother to her unborn child. Early detection and treatment during pregnancy are critical to protecting the health of both the mother and the baby. Integrating syphilis testing and treatment into existing antenatal care services ensures that pregnant women receive the necessary care and preventive measures [68].
Furthermore, community-based organizations and healthcare providers play a significant role in delivering targeted prevention interventions. These organizations are often well-positioned to reach at-risk populations, provide health education, and facilitate access to testing and treatment services [69,70,71]. Culturally sensitive and non-stigmatizing approaches are essential in building trust and promoting engagement with these communities [72,73].
Comprehensive health education and awareness campaigns are essential components of targeted prevention strategies [70]. By raising awareness about syphilis transmission, prevention methods, and the importance of regular testing, these campaigns empower the public to take charge of their sexual health [74]. Promoting open discussions about sexual health and reducing the stigma surrounding syphilis and other sexually transmitted infections can foster a more supportive environment for prevention behaviors [69,74].
5.4. Integration of Syphilis Services into Primary Healthcare
The integration of syphilis services into primary healthcare is a crucial step in improving the accessibility and delivery of syphilis prevention, diagnosis, and treatment. By embedding syphilis services within existing primary healthcare systems, individuals can receive comprehensive and timely care, leading to better health outcomes and a reduction in syphilis transmission [75].
One of the primary benefits of integrating syphilis services into primary healthcare is the increased reach to diverse populations. Primary healthcare facilities serve as the first point of contact for individuals seeking medical care, regardless of their socio-economic status or healthcare needs. By integrating syphilis services into these facilities, individuals are more likely to access testing and treatment services, particularly in underserved and remote areas where specialized clinics may be scarce [76,77]
Furthermore, integration allows for a holistic approach to sexual health. Primary healthcare providers are well-positioned to address multiple health needs of their patients, including sexual health. By incorporating syphilis services into routine health check-ups and screenings, primary healthcare providers can offer comprehensive care and promote regular testing for STIs, including syphilis [77,78].
The integration of syphilis services also facilitates early detection and prompt treatment. Primary healthcare providers can identify syphilis cases during routine medical visits, enabling timely intervention and reducing the risk of complications. Additionally, integration promotes regular testing for syphilis among high-risk populations, such as pregnant women, men who have sex with men, and individuals with multiple sexual partners, improving the chances of early diagnosis and treatment [66,74,79].
Incorporating syphilis services into primary healthcare enhances continuity of care. Patients who test positive for syphilis can receive follow-up care, monitoring, and treatment from the same healthcare provider, ensuring that they receive appropriate and continuous support throughout their healthcare journey [30,75].
Moreover, integration fosters de-stigmatization and normalizes discussions around sexual health. By providing syphilis services within primary healthcare settings, the stigma often associated with seeking specialized STI care is reduced. This normalization of sexual health discussions can encourage individuals to be more open about their sexual behaviors, allowing healthcare providers to offer tailored prevention strategies and support [11,79].
Training and capacity-building for primary healthcare providers are essential components of successful integration. Equipping healthcare professionals with the knowledge and skills to provide comprehensive syphilis services ensures accurate diagnoses, appropriate treatment, and effective prevention counseling. Additionally, incorporating syphilis services into medical education curriculum can further promote awareness and expertise among future healthcare providers.
6. Future Directions
Advancing syphilis research and implementing innovative approaches are paramount in the global efforts to prevent and control syphilis. The comprehensive understanding of the immunological aspects of syphilis is opening new avenues for the development of effective vaccines, which could potentially revolutionize syphilis prevention strategies. These vaccines have the potential to provide long-lasting protection and significantly reduce the burden of syphilis worldwide.
Moreover, the development of innovative point-of-care diagnostics is transforming syphilis testing and diagnosis. Rapid and sensitive diagnostic tools that are easily accessible and deployable in resource-limited settings can lead to early detection and immediate treatment initiation, reducing transmission rates and preventing complications.
Targeted prevention strategies, tailored to specific at-risk populations, are crucial in curbing the spread of syphilis. By addressing individual risk factors and promoting behavioral changes, targeted interventions can effectively reduce syphilis incidence in vulnerable communities.
The integration of syphilis services into primary healthcare systems plays a vital role in expanding access to syphilis prevention and treatment services. By incorporating syphilis care into routine healthcare visits, we can destigmatize discussions around sexual health and reach diverse populations, ensuring that everyone has access to quality and timely care.
Looking ahead, a multi-faceted approach that combines immunological advancements, innovative diagnostics, targeted prevention strategies, and integration into primary healthcare settings can strengthen syphilis control efforts and contribute to achieving global health goals. Continued investment in research, capacity-building, and awareness campaigns will be key to sustaining progress in syphilis prevention and control.
In summary, addressing the challenges posed by syphilis requires a collaborative effort from governments, healthcare systems, researchers, and communities. By harnessing the potential of immunology, diagnostics, prevention strategies, and integration into primary healthcare, we can move towards a syphilis-free future, promoting better sexual health and well-being for all.
References
- Kojima, N.; Klausner, J.D. An Update on the Global Epidemiology of Syphilis. Curr. Epidemiol. Reports 2018, 5, 24–38. [Google Scholar] [CrossRef]
- Tiecco, G.; Degli Antoni, M.; Storti, S.; Marchese, V.; Focà, E.; Torti, C.; Castelli, F.; Quiros-Roldan, E. A 2021 Update on Syphilis: Taking Stock from Pathogenesis to Vaccines. Pathogens 2021, 10, 1364. [Google Scholar] [CrossRef]
- Li, S.; Li, W.; Jin, Y.; Wu, B.; Wu, Y. Advancements in the Development of Nucleic Acid Vaccines for Syphilis Prevention and Control. Hum. Vaccin. Immunother. 2023, 19. [Google Scholar] [CrossRef] [PubMed]
- Osias, E.; Hung, P.; Giacani, L.; Stafylis, C.; Konda, K.A.; Vargas, S.K.; Reyes-Díaz, E.M.; Comulada, W.S.; Haake, D.A.; Haynes, A.M.; et al. Investigation of Syphilis Immunology and Treponema Pallidum Subsp. Pallidum Biology to Improve Clinical Management and Design a Broadly Protective Vaccine: Study Protocol. BMC Infect. Dis. 2020, 20, 444. [Google Scholar] [CrossRef] [PubMed]
- Mues, N.; Chu, H.W. Out-Smarting the Host: Bacteria Maneuvering the Immune Response to Favor Their Survival. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.N. V; Sarkar, T.; Kratofil, R.M.; Kubes, P.; Thanabalasuriar, A. Unraveling the Host’s Immune Response to Infection: Seeing Is Believing. J. Leukoc. Biol. 2019, 106, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Miethke, M.; Pieroni, M.; Weber, T.; Brönstrup, M.; Hammann, P.; Halby, L.; Arimondo, P.B.; Glaser, P.; Aigle, B.; Bode, H.B.; et al. Towards the Sustainable Discovery and Development of New Antibiotics. Nat. Rev. Chem. 2021, 5, 726–749. [Google Scholar] [CrossRef]
- Murugaiyan, J.; Kumar, P.A.; Rao, G.S.; Iskandar, K.; Hawser, S.; Hays, J.P.; Mohsen, Y.; Adukkadukkam, S.; Awuah, W.A.; Jose, R.A.M.; et al. Progress in Alternative Strategies to Combat Antimicrobial Resistance: Focus on Antibiotics. Antibiotics 2022, 11, 200. [Google Scholar] [CrossRef]
- Huemer, M.; Mairpady Shambat, S.; Brugger, S.D.; Zinkernagel, A.S. Antibiotic Resistance and Persistence—Implications for Human Health and Treatment Perspectives. EMBO Rep. 2020, 21. [Google Scholar] [CrossRef]
- Tuite, A.R.; Testa, C.; Rönn, M.; Bellerose, M.; Gift, T.; Fridge, J.; Molotnikov, L.; Desmarais, C.; Berruti, A.; Menzies, N.; et al. Exploring How Epidemic Context Influences Syphilis Screening Impact: A Mathematical Modeling Study. Sex. Transm. Dis. 2020, 47, 798–810. [Google Scholar] [CrossRef]
- Schmidt, R.; Carson, P.J.; Jansen, R.J. Resurgence of Syphilis in the United States: An Assessment of Contributing Factors. Infect. Dis. Res. Treat. 2019, 12, 117863371988328. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Mabey, D.; Kamb, M.L.; Chen, X.-S.; Radolf, J.D.; Benzaken, A.S. Syphilis. Nat. Rev. Dis. Prim. 2017, 3, 17073. [Google Scholar] [CrossRef] [PubMed]
- de Souza, T.A.; Teixeira, K.K.; Santana, R.L.; Penha, C.B.; Medeiros, A. de A.; de Lima, K.C.; Barbosa, I.R. Intra-Urban Differentials of Congenital and Acquired Syphilis and Syphilis in Pregnant Women in an Urban Area in Northeastern Brazil. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Pereira Nogueira, W.; Figueiredo Nogueira, M.; de Almeida Nogueira, J.; Freire, M.E.M.; Gir, E.; Silva, A.C. de O. e Syphilis in Riverine Communities: Prevalence and Associated Factors. Rev. da Esc. Enferm. da USP 2022, 56. [Google Scholar] [CrossRef]
- Macêdo, V.C. de; Lira, P.I.C. de; Frias, P.G. de; Romaguera, L.M.D.; Caires, S. de F.F.; Ximenes, R.A. de A. Risk Factors for Syphilis in Women: Case-Control Study. Rev. Saude Publica 2017, 51, 78. [Google Scholar] [CrossRef]
- Amerson, E.H.; Castillo Valladares, H.B.; Leslie, K.S. Resurgence of Syphilis in the US—USPSTF Reaffirms Screening Guidelines. JAMA Dermatology 2022, 158, 1241. [Google Scholar] [CrossRef]
- Copen, C.E.; Brookmeyer, K.A.; Haderxhanaj, L.T.; Hogben, M.; Torrone, E.A. Sexual Risk Behaviors Among Persons Diagnosed With Primary and Secondary Syphilis Who Reported High-Risk Substance Use: Data From the National Notifiable Diseases Surveillance System, 2018. Sex. Transm. Dis. 2022, 49, 99–104. [Google Scholar] [CrossRef]
- Šmit, R.; Wojtalewicz, N.; Vierbaum, L.; Nourbakhsh, F.; Schellenberg, I.; Hunfeld, K.-P.; Lohr, B. Epidemiology, Management, Quality of Testing and Cost of Syphilis in Germany: A Retrospective Model Analysis. Front. Public Heal. 2022, 10. [Google Scholar] [CrossRef]
- Ramos Jr., A. N. Persistence of Syphilis as a Challenge for the Brazilian Public Health: The Solution Is to Strengthen SUS in Defense of Democracy and Life. Cad. Saude Publica 2022, 38. [Google Scholar] [CrossRef]
- Valentine, J.A.; Bolan, G.A. Syphilis Elimination: Lessons Learned Again. Sex. Transm. Dis. 2018, 45, S80–S85. [Google Scholar] [CrossRef]
- Kitayama, K.; Segura, E.R.; Lake, J.E.; Perez-Brumer, A.G.; Oldenburg, C.E.; Myers, B.A.; Pourjavaheri, P.; Okorie, C.N.; Cabello, R.L.; Clark, J.L. Syphilis in the Americas: A Protocol for a Systematic Review of Syphilis Prevalence and Incidence in Four High-Risk Groups, 1980–2016. Syst. Rev. 2017, 6, 195. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Xie, Y.; Xiao, Y. Laboratory Diagnostic Tools for Syphilis: Current Status and Future Prospects. Front. Cell. Infect. Microbiol. 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Wolgemuth, C.W. Flagellar Motility of the Pathogenic Spirochetes. Semin. Cell Dev. Biol. 2015, 46, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Forrestel, A.K.; Kovarik, C.L.; Katz, K.A. Sexually Acquired Syphilis. J. Am. Acad. Dermatol. 2020, 82, 17–28. [Google Scholar] [CrossRef]
- Hook, E.W.; Roddy, R.E.; Lukehart, S.A.; Hom, J.; Holmes, K.K.; Tam, M.R. Detection of Treponema Pallidum in Lesion Exudate with a Pathogen-Specific Monoclonal Antibody. J. Clin. Microbiol. 1985, 22, 241–244. [Google Scholar] [CrossRef]
- Ito, F.; Hunter, E.F.; George, R.W.; Pope, V.; Larsen, S.A. Specific Immunofluorescent Staining of Pathogenic Treponemes with a Monoclonal Antibody. J. Clin. Microbiol. 1992, 30, 831–838. [Google Scholar] [CrossRef]
- Morshed, M.G. Current Trend on Syphilis Diagnosis: Issues and Challenges. In; 2014; pp. 51–64.
- Graham, R.P.; Naini, B. V.; Shah, S.S.; Arnold, C.A.; Kannangai, R.; Torbenson, M.S.; Lam-Himlin, D.M. Treponema Pallidum Immunohistochemistry Is Positive in Human Intestinal Spirochetosis. Diagn. Pathol. 2018, 13, 7. [Google Scholar] [CrossRef]
- Radolf, J.D.; Deka, R.K.; Anand, A.; Šmajs, D.; Norgard, M. V.; Yang, X.F. Treponema Pallidum, the Syphilis Spirochete: Making a Living as a Stealth Pathogen. Nat. Rev. Microbiol. 2016, 14, 744–759. [Google Scholar] [CrossRef]
- Morshed, M.G.; Singh, A.E. Recent Trends in the Serologic Diagnosis of Syphilis. Clin. Vaccine Immunol. 2015, 22, 137–147. [Google Scholar] [CrossRef]
- Gao, K.; Shen, X.; Lin, Y.; Zhu, X.-Z.; Lin, L.-R.; Tong, M.-L.; Xiao, Y.; Zhang, H.-L.; Liang, X.-M.; Niu, J.-J.; et al. Origin of Nontreponemal Antibodies During Treponema Pallidum Infection: Evidence From a Rabbit Model. J. Infect. Dis. 2018, 218, 835–843. [Google Scholar] [CrossRef]
- Tuddenham, S.; Katz, S.S.; Ghanem, K.G. Syphilis Laboratory Guidelines: Performance Characteristics of Nontreponemal Antibody Tests. Clin. Infect. Dis. 2020, 71, S21–S42. [Google Scholar] [CrossRef] [PubMed]
- Marra, C.M.; Tantalo, L.C.; Maxwell, C.L.; Ho, E.L.; Sahi, S.K.; Jones, T. The Rapid Plasma Reagin Test Cannot Replace the Venereal Disease Research Laboratory Test for Neurosyphilis Diagnosis. Sex. Transm. Dis. 2012, 39, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Park, I.U.; Fakile, Y.F.; Chow, J.M.; Gustafson, K.J.; Jost, H.; Schapiro, J.M.; Novak-Weekley, S.; Tran, A.; Nomura, J.H.; Chen, V.; et al. Performance of Treponemal Tests for the Diagnosis of Syphilis. Clin. Infect. Dis. 2019, 68, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.A.; Steiner, B.M.; Rudolph, A.H. Laboratory Diagnosis and Interpretation of Tests for Syphilis. Clin. Microbiol. Rev. 1995, 8, 1–21. [Google Scholar] [CrossRef]
- Centurion-Lara, A.; Castro, C.; Shaffer, J.M.; Van Voorhis, W.C.; Marra, C.M.; Lukehart, S.A. Detection of Treponema Pallidum by a Sensitive Reverse Transcriptase PCR. J. Clin. Microbiol. 1997, 35, 1348–1352. [Google Scholar] [CrossRef]
- Gayet-Ageron, A.; Sednaoui, P.; Lautenschlager, S.; Ferry, T.; Toutous-Trellu, L.; Cavassini, M.; Yassir, F.; Martinez de Tejada, B.; Emonet, S.; Combescure, C.; et al. Use of Treponema Pallidum PCR in Testing of Ulcers for Diagnosis of Primary Syphilis1. Emerg. Infect. Dis. 2015, 21, 127–129. [Google Scholar] [CrossRef]
- Xiao, Y.; Xie, Y.; Xu, M.; Liu, S.; Jiang, C.; Zhao, F.; Zeng, T.; Liu, Z.; Yu, J.; Wu, Y. Development and Evaluation of a Loop-Mediated Isothermal Amplification Assay for the Detection of Treponema Pallidum DNA in the Peripheral Blood of Secondary Syphilis Patients. Am. J. Trop. Med. Hyg. 2017, 97, 1673–1678. [Google Scholar] [CrossRef]
- Morshed, M.G.; Lee, M.-K.; Jorgensen, D.; Isaac-Renton, J.L. Molecular Methods Used in Clinical Laboratory: Prospects and Pitfalls. FEMS Immunol. Med. Microbiol. 2007, 49, 184–191. [Google Scholar] [CrossRef]
- Singhal, N.; Kumar, M.; Kanaujia, P.K.; Virdi, J.S. MALDI-TOF Mass Spectrometry: An Emerging Technology for Microbial Identification and Diagnosis. Front. Microbiol. 2015, 6. [Google Scholar] [CrossRef]
- Stamm, L. V. Syphilis: Re-Emergence of an Old Foe. Microb. Cell 2016, 3, 363–370. [Google Scholar] [CrossRef]
- Douglas, J.M. Penicillin Treatment of Syphilis. JAMA 2009, 301, 769. [Google Scholar] [CrossRef] [PubMed]
- Katz, K.A.; Klausner, J.D. Azithromycin Resistance in Treponema Pallidum. Curr. Opin. Infect. Dis. 2008, 21, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.-S.; Yin, Y.-P.; Wei, W.-H.; Wang, H.-C.; Peng, R.-R.; Zheng, H.-P.; Zhang, J.-P.; Zhu, B.-Y.; Liu, Q.-Z.; Huang, S.-J. High Prevalence of Azithromycin Resistance to Treponema Pallidum in Geographically Different Areas in China. Clin. Microbiol. Infect. 2013, 19, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Orbe-Orihuela, Y.C.; Sánchez-Alemán, M.Á.; Hernández-Pliego, A.; Medina-García, C.V.; Vergara-Ortega, D.N. Syphilis as Re-Emerging Disease, Antibiotic Resistance, and Vulnerable Population: Global Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1546. [Google Scholar] [CrossRef]
- Cameron, C.E.; Lukehart, S.A. Current Status of Syphilis Vaccine Development: Need, Challenges, Prospects. Vaccine 2014, 32, 1602–1609. [Google Scholar] [CrossRef]
- Miller, J.N. Immunity in Experimental Syphilis. J. Immunol. 1973, 110, 1206–1215. [Google Scholar] [CrossRef]
- Haynes, A.M.; Giacani, L.; Mayans, M.V.; Ubals, M.; Nieto, C.; Pérez-Mañá, C.; Quintó, L.; Romeis, E.; Mitjà, O. Efficacy of Linezolid on Treponema Pallidum, the Syphilis Agent: A Preclinical Study. EBioMedicine 2021, 65, 103281. [Google Scholar] [CrossRef]
- Stamm, L. V. Hope for New Antibiotics for Syphilis Treatment. EBioMedicine 2021, 66, 103320. [Google Scholar] [CrossRef]
- Vickram, A.S.; Dhama, K.; Thanigaivel, S.; Chakraborty, S.; Anbarasu, K.; Dey, N.; Karunakaran, R. Strategies for Successful Designing of Immunocontraceptive Vaccines and Recent Updates in Vaccine Development against Sexually Transmitted Infections - A Review. Saudi J. Biol. Sci. 2022, 29, 2033–2046. [Google Scholar] [CrossRef]
- Cameron, C.E. Syphilis Vaccine Development: Requirements, Challenges, and Opportunities. Sex. Transm. Dis. 2018, 45, S17–S19. [Google Scholar] [CrossRef]
- Kojima, N.; Konda, K.A.; Klausner, J.D. Notes on Syphilis Vaccine Development. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Giacani, L. Strategies for Syphilis Vaccine Development. J. Bras. Doenças Sex. Transm. 2022, 34. [Google Scholar] [CrossRef]
- Pham, M.D.; Ong, J.J.; Anderson, D.A.; Drummer, H.E.; Stoové, M. Point-of-Care Diagnostics for Diagnosis of Active Syphilis Infection: Needs, Challenges and the Way Forward. Int. J. Environ. Res. Public Health 2022, 19, 8172. [Google Scholar] [CrossRef] [PubMed]
- Mabey, D.C.; Sollis, K.A.; Kelly, H.A.; Benzaken, A.S.; Bitarakwate, E.; Changalucha, J.; Chen, X.-S.; Yin, Y.-P.; Garcia, P.J.; Strasser, S.; et al. Point-of-Care Tests to Strengthen Health Systems and Save Newborn Lives: The Case of Syphilis. PLoS Med. 2012, 9, e1001233. [Google Scholar] [CrossRef] [PubMed]
- Causer, L.M.; Kaldor, J.M.; Conway, D.P.; Leslie, D.E.; Denham, I.; Karapanagiotidis, T.; Ryan, C.; Wand, H.; Anderson, D.A.; Robertson, P.W.; et al. An Evaluation of a Novel Dual Treponemal/Nontreponemal Point-of-Care Test for Syphilis as a Tool to Distinguish Active From Past Treated Infection. Clin. Infect. Dis. 2015, 61, 184–191. [Google Scholar] [CrossRef]
- Caya, C.; Maheu-Giroux, M.; Xia, Y.; Serhir, B.; Morin, V.; Libman, M.; Corsini, R.; Goldfarb, D.M.; Wong, T.; Singh, A.E.; et al. Stopping Syphilis Transmission in Arctic Communities through Rapid Diagnostic Testing: The STAR Study Protocol. PLoS One 2022, 17, e0273713. [Google Scholar] [CrossRef]
- Toskin, I.; Blondeel, K.; Peeling, R.W.; Deal, C.; Kiarie, J. Advancing Point of Care Diagnostics for the Control and Prevention of STIs: The Way Forward. Sex. Transm. Infect. 2017, 93, S81–S88. [Google Scholar] [CrossRef]
- Basing, L.A.W.; Simpson, S.V.; Adu-Sarkodie, Y.; Linnes, J.C. A Loop-Mediated Isothermal Amplification Assay for the Detection of Treponema Pallidum Subsp. Pertenue. Am. J. Trop. Med. Hyg. 2020, 103, 253–259. [Google Scholar] [CrossRef]
- Tharakan, S.; Faqah, O.; Asghar, W.; Ilyas, A. Microfluidic Devices for HIV Diagnosis and Monitoring at Point-of-Care (POC) Settings. Biosensors 2022, 12, 949. [Google Scholar] [CrossRef]
- Christodouleas, D.C.; Kaur, B.; Chorti, P. From Point-of-Care Testing to EHealth Diagnostic Devices (EDiagnostics). ACS Cent. Sci. 2018, 4, 1600–1616. [Google Scholar] [CrossRef]
- Naeem, F.; Karellis, A.; Nair, S.; Routy, J.-P.; Yansouni, C.P.; Kim, J.; Pai, N. Multiplexed Technologies for Sexually Transmitted Infections: Global Evidence on Patient-Centered and Clinical Health Outcomes. BMJ Glob. Heal. 2021, 6, e005670. [Google Scholar] [CrossRef] [PubMed]
- Karellis, A.; Naeem, F.; Nair, S.; Mallya, S.D.; Routy, J.-P.; Gahagan, J.; Yansouni, C.P.; Kim, J.; Pai, N.P. Multiplexed Rapid Technologies for Sexually Transmitted Infections: A Systematic Review. The Lancet Microbe 2022, 3, e303–e315. [Google Scholar] [CrossRef] [PubMed]
- Osbak, K.K.; Van Raemdonck, G.A.; Dom, M.; Cameron, C.E.; Meehan, C.J.; Deforce, D.; Ostade, X. Van; Kenyon, C.R.; Dhaenens, M. Candidate Treponema Pallidum Biomarkers Uncovered in Urine from Individuals with Syphilis Using Mass Spectrometry. Future Microbiol. 2018, 13, 1497–1510. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, M.; Wang, Z.; Li, S.; Deng, Y.; He, N. Point-of-Care Diagnostics for Infectious Diseases: From Methods to Devices. Nano Today 2021, 37, 101092. [Google Scholar] [CrossRef] [PubMed]
- Peterman, T.A.; Cha, S. Context-Appropriate Interventions to Prevent Syphilis: A Narrative Review. Sex. Transm. Dis. 2018, 45, S65–S71. [Google Scholar] [CrossRef]
- Copen, C.E.; Rushmore, J.; De Voux, A.; Kirkcaldy, R.D.; Fakile, Y.F.; Tilchin, C.; Duchen, J.; Jennings, J.M.; Spahnie, M.; Norris Turner, A.; et al. Factors Associated With Syphilis Transmission and Acquisition Among Men Who Have Sex With Men: Protocol for a Multisite Egocentric Network Study. JMIR Res. Protoc. 2022, 11, e40095. [Google Scholar] [CrossRef]
- Welch, J. Antenatal Screening for Syphilis. BMJ 1998, 317, 1605–1606. [Google Scholar] [CrossRef]
- Paiva, J.C. de L.; Dias-Trindade, S.; Gonzalez, M.O.A.; Barros, D.M. da S.; Cardoso, P.H.; Bezerra, P.H.C.; Lima, T.G.F. de M.S.; Lacerda, J. de S.; Muneiro, L.C.; Cunha-Oliveira, A.; et al. Analysis of the Impact of Communication Campaigns under the Project “Syphilis No”: A National Tool for Inducing and Promoting Health. Int. J. Environ. Res. Public Health 2022, 19, e15884. [Google Scholar] [CrossRef]
- Varshney, K.; Ikanovic, A.; Ghosh, P.; Shet, P.; Di Sipio, M.; Khatri, C.; Mahmood, M.Q. A Global Scoping Review of the Factors Associated with HIV and Syphilis Co-Infection: Findings from 40 Countries. Venereology 2022, 1, 98–113. [Google Scholar] [CrossRef]
- Nguyen, S.H.; Dang, A.K.; Vu, G.T.; Nguyen, C.T.; Le, T.H.T.; Truong, N.T.; Hoang, C.L.; Tran, T.T.; Tran, T.H.; Pham, H.Q.; et al. Lack of Knowledge about Sexually Transmitted Diseases (STDs): Implications for STDs Prevention and Care among Dermatology Patients in an Urban City in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 1080. [Google Scholar] [CrossRef]
- Valentine, J.A.; Delgado, L.F.; Haderxhanaj, L.T.; Hogben, M. Improving Sexual Health in U.S. Rural Communities: Reducing the Impact of Stigma. AIDS Behav. 2022, 26, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Grieb, S.M.; Jackman, K.-M.; Jennings, J.M. Recommendations From Black Sexual Minority Men: Building Trust to Improve Engagement and Impact of HIV/STI Research. Health Promot. Pract. 2021, 22, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Peterman, T.A.; Furness, B.W. Public Health Interventions to Control Syphilis. Sex. Health 2015, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Saes, M. de O.; Duro, S.M.S.; Gonçalves, C. de S.; Tomasi, E.; Facchini, L.A. Assessment of the Appropriate Management of Syphilis Patients in Primary Health Care in Different Regions of Brazil from 2012 to 2018. Cad. Saude Publica 2022, 38. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.M. dos; Rosendo, T.M.S. de S.; Lopes, A.K.B.; Roncalli, A.G.; Lima, K.C. de Weaknesses in Primary Health Care Favor the Growth of Acquired Syphilis. PLoS Negl. Trop. Dis. 2021, 15, e0009085. [Google Scholar] [CrossRef]
- van Weel, C.; Kidd, M.R. Why Strengthening Primary Health Care Is Essential to Achieving Universal Health Coverage. Can. Med. Assoc. J. 2018, 190, E463–E466. [Google Scholar] [CrossRef]
- McCormack, H.; Guy, R.; Bourne, C.; Newman, C.E. Integrating Testing for Sexually Transmissible Infections into Routine Primary Care for Aboriginal Young People: A Strengths-based Qualitative Analysis. Aust. N. Z. J. Public Health 2022, 46, 370–376. [Google Scholar] [CrossRef]
- Guedes, A.L. de L.; Guimarães, D.C. da S.; Sarkis, D.J.; Gabriel, T.T.; Delgado, C.S.; Campos, A.A.L.; Nogueira, M.C.; Ribeiro, L.C. Factors Associated with Women Diagnosed with Syphilis Who Received Prenatal Care in a Primary Healthcare Unit. einstein (São Paulo) 2023, 31. [Google Scholar] [CrossRef]
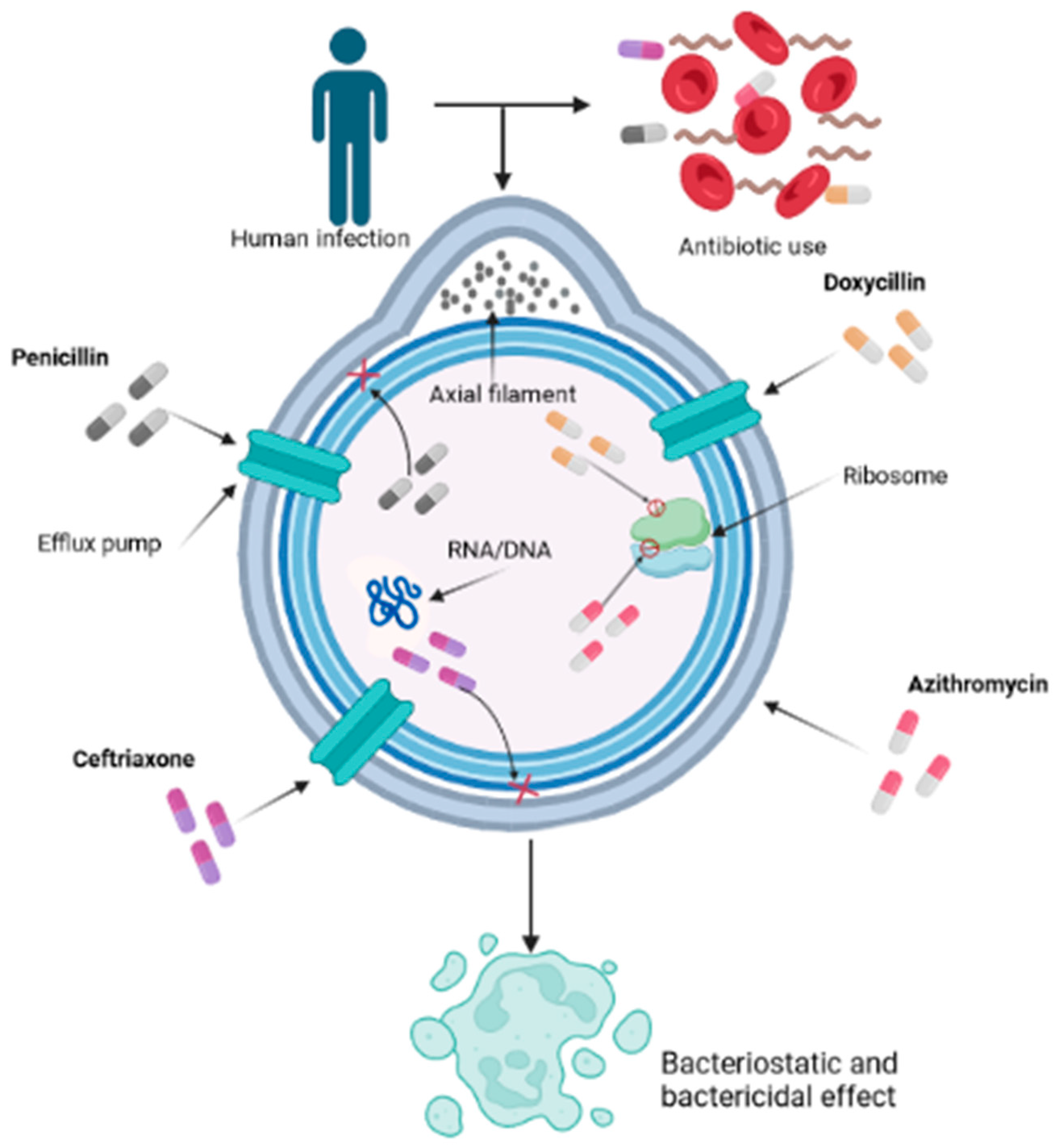
Figure 1.
Mechanism of action of various antibiotics on Treponema pallidum used for syphilis treatment. The intricate mechanism by which various antibiotics, notably penicillin, doxycycline, ceftriaxone, and azithromycin, play pivotal roles in combating the infection caused by T. pallidum, is a nuanced interplay at the forefront of scientific understanding. Penicillin, functioning as a β-lactam compound, disrupts the transpeptidase-mediated synthesis via cross-linking of peptidoglycan, thereby undermining the structural integrity of the cell wall and culminating in bacterial lysis. Doxycycline, classified as a tetracycline derivative, exerts its influence by suppressing protein translation through binding to the 30S subunit of the bacterial ribosome, thereby obstructing the intricate assembly of the translation complex. Ceftriaxone, a member of the cephalosporin class, further augments the multifaceted approach by targeting the bacterial cell wall, thwarting transpeptidase activity, and thereby weakening the structural robustness. In parallel, azithromycin, a representative of the macrolide family, exerts its effect by inhibiting bacterial protein synthesis through impeding the translocation process of the 50S ribosomal subunit, further contributing to the orchestrated disruption of essential bacterial processes.
Figure 1.
Mechanism of action of various antibiotics on Treponema pallidum used for syphilis treatment. The intricate mechanism by which various antibiotics, notably penicillin, doxycycline, ceftriaxone, and azithromycin, play pivotal roles in combating the infection caused by T. pallidum, is a nuanced interplay at the forefront of scientific understanding. Penicillin, functioning as a β-lactam compound, disrupts the transpeptidase-mediated synthesis via cross-linking of peptidoglycan, thereby undermining the structural integrity of the cell wall and culminating in bacterial lysis. Doxycycline, classified as a tetracycline derivative, exerts its influence by suppressing protein translation through binding to the 30S subunit of the bacterial ribosome, thereby obstructing the intricate assembly of the translation complex. Ceftriaxone, a member of the cephalosporin class, further augments the multifaceted approach by targeting the bacterial cell wall, thwarting transpeptidase activity, and thereby weakening the structural robustness. In parallel, azithromycin, a representative of the macrolide family, exerts its effect by inhibiting bacterial protein synthesis through impeding the translocation process of the 50S ribosomal subunit, further contributing to the orchestrated disruption of essential bacterial processes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



