
Submitted:
28 August 2023
Posted:
30 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Hypertension is one of the most common and significant cardiovascular risk factor. With the emergence of COVID-19, concerns have arisen about its potential to exacerbate cardiovascular morbidity and mortality. Several theories have emerged linking hypertension with COVID-19. However, the relationship between SARS-CoV-2 infection and long-term risk of hypertension remains insufficiently explored. Therefore, our study aimed to investigate the impact of COVID-19 infection on blood pressure and long-term risk of hypertension developing. A comprehensive search was conducted in the PubMed and SCOPUS databases up to 10th August 2023 for relevant papers. The analysis included 35 eligible articles. The majority of the latest studies pointed to increase BP after COVID-19 infection. However, several observations contradicted the influence of SARS-CoV-2 on the hypertension development or suggesting a transient effect. The possible role of the loss of angiotensin-converting enzyme 2, cytokine storm, increased sympathetic activity, and endothelial dysfunction were considered. On the other hand, BP changes following COVID-19 could be a consequence of lifestyle changes, which often accompanied COVID-19 infection. Our findings highlight the urgent need for comprehensive research on the COVID-19 and hypertension link. These insights are crucial for implementing effective prevention and management strategies for individuals with the history of COVID-19 infection.
Keywords:
COVID-19
; SARS-CoV-2
; hypertension
; blood pressure
; endothelial dysfunction
; long-covid
; post covid
1. Introduction
1.1. COVID-19 Cardiovascular Outcome
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in December 2019 in Wuhan, China. Its high infectivity quickly resulted in a global paralysis, triggering an avalanche of infections which was named Coronavirus disease 2019 (COVID-19). The World Health Organization (WHO) declared a pandemic in March 2020 and announced the end of pandemic in May 2023. The increasing number of cases caused concern among the public and overwhelmed healthcare systems. It is widely acknowledged as one of the worst disasters humans have experienced in recent decades. After over 3 years, effective diagnostic and treatment algorithms have been developed, as well as preventive measures for acute COVID-19. Thanks to vaccines, the mortality of the disease has decreased, as has the risk of its severe course.
However, patients with persistent symptoms continue to seek medical attention worldwide, despite the resolution of the acute phase of SARS-CoV-2 infection. Over 200 symptoms that impact multiple organ systems have been identified as a complication of COVID-19 [1]. Millions of people worldwide are estimated to be experiencing long COVID, with the number of cases increasing every day [2].
There are numerous definitions of long COVID. The National Institute for Health and Care Excellence (NICE) defines "long COVID" as follows: “Post-COVID-19 syndrome is characterized by signs and symptoms developed during or after an infection consistent with COVID-19, continue for more than 12 weeks, and are not explained by an alternative diagnosis. It usually presents with clusters of symptoms, often overlapping, which can fluctuate and change over time and can affect any system in the body. Post-COVID-19 syndrome may be considered before 12 weeks while the possibility of an alternative underlying disease is also being assessed [3]. According to the World Health Organization (WHO), post-COVID condition is defined as the presence of post-COVID symptoms that persist past 3 months, last for at least 2 months, and cannot be explained by an alternative diagnosis [4].
In addition to the clinical case definitions, the term "long COVID" is commonly used to describe signs and symptoms known to continue or develop after acute COVID-19. It includes both, ongoing symptomatic COVID-19 (from 4 to 12 weeks, and post-COVID-19 syndrome (12 weeks or more) [5].
Although COVID-19 was initially recognized as a respiratory disease, SARS-CoV-2 can damage multiple organ systems. Researchers have started to focus on complications following COVID-19. Every month, new studies emerge demonstrating clinical correlations with previous SARS-CoV-2 infection [6].
Above others, a negative impact of SARS-CoV-2 on cardiovascular function has been estimated. It causes an endothelial dysfunction, which can lead to various clinical complications, such as atherosclerosis, thrombotic disease, acute coronary syndrome, or possible changes in blood pressure (BP) [7]. The relationship between SARS-CoV-2 infection and long-term cardiovascular risk still remains under the investigation, as well as the frequency and nature of long-term cardiovascular consequences.
In this review, it was attempted to investigate the potential impact of COVID-19 infection on blood pressure and long-term risk of hypertension developing.
1.2. Renin-Angiotensin-Aldosterone System
Renin converts the tetradecapeptide angiotensinogen to angiotensin I (AT-I), which has weak biological activity. Angiotensin-converting enzyme (ACE), present in the endothelial cell membrane, converts AT-I to angiotensin II (AT-II). AT-II binds to its receptor angiotensin Ⅱ receptor type 1(RAt-1), causing a series of actions, including vasoconstriction, prothrombotic effects, and retention of water and sodium to maintain appropriate pressure and flow under conditions of hypovolemia and restore volume [8].
In the event of disruption to the circulatory system, angiotensin II is responsible for vasoconstriction and clotting at the site, followed by repair. However, excessive activity due to inappropriate stimulus or malfunction can lead to pathological processes such as hypertension or atherosclerosis.
Another action of angiotensin II is stimulation of aldosterone synthase, a substance with a strong influence on electrolyte balance and a very strong antiproliferative effect. The bradykinin system is antagonistic to the renin-angiotensin-aldosterone system (RAAS) and exerts effects opposite to those of AT-II.
There is also another variant of ACE known as angiotensin-aonverting enzyme type 2 (ACE-2), which converts Ang-II to angiotensin 1-7 (Ang 1-7), which acts on the MAS receptor. This peptide exhibits antifibrotic, antiproliferative, anti-inflammatory, vasodilatory, diuretic, and bradykinin-NO (nitric oxide) enhancing effects. It appears that the bradykinin-NO pathway is involved here [9,10]. Ang-(1–7) antagonizes the pressor effect of AT-I, thus causing, among other things, a decrease in blood pressure. It has been suggested the lack of ACE-2 accelerates heart dysfunction caused by pressure overload [11].
ACE2's ability to degrade Ang II and increase Ang (1–7) may counteract the negative effects of ACE receptor stimulation. ACE2 is also capable of degrading apelin-13, a peptide which likely causes vasoconstriction and regulates fluid homeostasis, as well as other peptides unrelated to renin-angiotensin system (RAS), such as kynetenin, dynorphin A, and neurotensin [12]. As a result, ACE-2 regulates blood pressure under physiological conditions, and a decrease in ACE-2 gene levels leads to increased blood pressure [13]. The simplified scheme of angiotensinogen metabolism and the end effects of these transformations are presented in Figure 1.
ACE2 and Ang II can regulate each other [14]. Ang II upregulates AT1R, increases a disintegrin and metalloprotease 17 (ADAM17) expression, leading to ACE-2 release and decreasing the protective effect of ACE-2 in hypertension, while Ang II can be converted to Ang-(1-7) by ACE-2 to inhibit its own negative effect [15,16]. Recently, it has been found ACE-2 overexpression also protects against neurogenic hypertension by regulating baroreceptor reflexes and autonomic function in the central nervous system (CNS) [17].
1.3. ACE-2 and COVID-19
There are studies suggested so far SARS-CoV-2 infection may lead to alterations in the ACE/ACE-2 and Ang-II/angiotensin-(1-7) balance, which can affect blood pressure and potentially lead to the development of hypertension. ACE-2 plays a crucial role in regulating the renin-angiotensin-aldosterone system, which controls blood pressure. SARS-CoV-2 infection may decrease ACE-2 expression, which could lead to increased Angiotensin II activity, which in turn can impact vascular and organ damage.
It is also worth noting, that the mechanisms by which SARS-CoV-2 affects the RAAS and blood pressure are still being investigated and it is not yet fully understood what the exact consequences of infection on the cardiovascular system are [18,19,20].
SARS-CoV-2 is thought to enter and cause infection in its host through the attachment of its structural protein known as the S-glycoprotein to angiotensin-converting enzyme 2 [21,22,23,24]. Domain of the spike glycoprotein binds to the tip of subdomain I of ACE-2, mediated fusion and promoted viral replication [25].
SARS-CoV-2 enters host cells using the spike glycoprotein receptor, following the fusion of the viral membrane and the host cell, viral RNA is released into the cytoplasm. Some transmembrane proteases, including ADAM17, transmembrane serine protease 2 (TMPRSS), and Tumor necrosis factor (TNF) converting enzyme, as well as proteins such as vimentin and clathrin, may participate in the entire process of establishing infection [26,27,28,29,30,31].
According to the research carried out by Wenhui et al [21]. SARS-CoV-2 transfects more efficiently on cells with ACE-2 than on those non-transfected with ACE. Their data also demonstrate a specific, high-affinity association between the S1 domain of the SARS-CoV-2 S protein and ACE-2 [32].
ACE-2 is expressed in nearly all human organs in varying degrees. ACE-2 or its transmembrane domain is internalized together with the virus and then shedded of soluble ACE-2 into the cellular supernatants which might be responsible for the significantly reduced ACE-2 expression in the context of SARS-CoV-2 infection [33].
According to some studies SARS-CoV-2, through interactions with ACE-2, increased level of disintegrin and metalloproteinase 17 expression, which in turn induced the release of ACE-2. Consequently, the function of ACE-2 was impaired, while at the same time there was an increase in the expression of ACE and Ang II. A higher level of Ang II increases the release of cytokines, including interleukins 6 (IL-6) and interleukins 7 (IL-7), which activate the mitogen-activated protein kinase (MAPK) pathway and thus increase the expression of ADAM17, creating a positive feedback loop. Several studies have shown that SARS-CoV-2 infection can decrease the expression of ACE-2, leading to an imbalance in ACE/ACE-2 and Ang-II/angiotensin-(1-7), which in turn can cause damage to many organs [8].
Downregulation of ACE-2 makes an ACE/ACE-2 disproportion and excessive production of angiotensin by the related ACE enzyme.
ACE-2 is expressed in many organs including cells lining the blood vessels (endothelial cells), pneumocytes, macrophages, perivascular pericytes, and cardiomyocytes.
SARS-CoV-2 virus using ACE-2 can causes myocardial, endothelial and microvascular dysfunction, plaque instability, and myocardial infarction [34].
1.4. Other Factors Contributing to the Hypertension Development
Many factors contribute to the development of hypertension, including obesity, insulin resistance, and sympathetic nervous system disorders [100]. The pathogenesis of hypertension also involves dysfunction of the endothelium, manifested by changes in endothelin and nitric oxide [37,38]. COVID-19 can cause the appearance or exacerbation of those risk factors, indirectly leading to the development of arterial hypertension.
It is widely known that patients recovered from COVID-19 infection may complain of chronic fatigue and worsened exercise tolerance, which can persist for several months, especially in those who required admission to the ICU(Intensive Care Unit) [39,40,41,42]. Additionally, the emergence of anxiety, depression, or exacerbation of pre-existing mood disorders, associated not only with COVID-19 itself but also with quarantine and isolation during the pandemic, collectively predisposes individuals to a sedentary lifestyle and consequently, weight gain, becoming overweight, and ultimately obesity [43]. This, in turn, is associated with a high risk of hypertension developing [44,45].
Another mechanism which may play a role in the pathogenesis of hypertension as an outcome of COVID-19 is autonomic nervous system dysfunction, which has been reported in several studies [46]. However, it is not well known yet whether COVID-19-related dysautonomia is related to the neurotropism of the virus to autonomic pathways, immunological mechanisms, or is the result of a cytokine storm [47,48,49].
Some of recent discoveries, indicated long COVID contribution to the sympathetic nervous system activation due to suppressing the parasympathetic system. The consequences of this particular dysregulations may include increased heart rate and elevated blood pressure [50,51].
Furthermore, other studies indicated that patients with COVID-19, especially those treated in intensive care units, exhibited tendencies toward hyperreninemia with hypernatremia, hyperchloremia, and volume overload [52]. All of above mechanism may lead to the blood pressure elevation in individuals with previously normal blood pressure range or worsen blood pressure value in those with previously well-controlled hypertension [53].
Endothelial dysfunction, understood as an imbalance between vasodilatory and vasoconstrictive factors, can increase vasoconstriction, cause arterial wall stiffening and weakened vasorelaxation [54,55]. All described pathomechanisms may contribute to hypertension development as well as were observed in COVID-19 infection what suggests their involvement in long-term symptoms after the infection [56,57,58].
Nothing impedes the notion that there is ample evidence suggesting the impact of the SARS-CoV-2 virus on the development of arterial hypertension, both directly through its influence on the renin-angiotensin-aldosterone system and indirectly by exacerbating classical risk factors for this disease. Figure 2 shows possible mechanisms through which SARS-CoV-2 can cause hypertension. However, the definitive pathogenic mechanism of these changes has not yet been established, and we are still awaiting studies which will shed light on this puzzle.
2. Materials and Methods
We systematically searched the PUBMED and SCOPUS databases, focusing on studies examined adults. The first search was conducted on April 16th 2023 incorporating relevant medical subject headings. A final database search was conducted on August 10, 2023.
Medical Subject Headings (MeSH) with all subheadings included and with 3 years limitations. After reading the articles, excluded studies were containing irrelevant final statements or inappropriate research methods, inappropriate reports, or disseminated incomplete reports. The counted articles were published in English.
We incorporated studies focused on outcomes occurring at least 14 days or longer after infection with SARS-CoV-2 for analysis. MeSH terms included: "COVID-19", "SARS-CoV-2", "post COVID", "long COVID", "after COVID", "vascular", "microvascular", "endothelial", "ACE2", "hypertension", "blood pressure", "consequences", and "complications", "effect" for our search. The terms were combined individually using the Boolean operator ‘AND’ or "OR" if it was needed.
Duplicates were removed. Afterwards, titles and abstracts of the remaining studies were screened by three reviewers (E.B., P.S. AZ-K and P.P) in order to identify relevant articles. Disagreements between reviewers were resolved by the opinion of the fourth reviewer (E.Z.) Finally, selected eligible articles were fully reviewed.
3. Results
The initial search using all MeSH terms resulted in finding 13,233 records. After analyzing the titles, 131 articles were selected for further analysis. These articles were evaluated based on reading the abstracts, resulting in the extraction of 73 studies. Five duplicates were eliminated. After evaluating the full texts, 28 articles were excluded as they were not in English, the study population was below 18 years of age, or they were not relevant to the impact on hypertension. Ultimately, 35 qualifying articles were included in this document. The flowchart illustrating the complete search strategy is presented in Figure 2.
Figure 2.
PRISMA flow diagram of systematic reviews process performed in this study.

Table 1 presents a summary of the studies included in the review, along with a brief description of the study population and observation period.
4. Discussion
Hypertension (HT) is a huge health problem worldwide. It is estimated that the number of adults affected by HT has doubled from 1990 to 2019, reaching now approximately 650 billion [98,99].
The primary point of hypertension treatment is a modification of risk factors such as lipid disorders, obesity, diabetes, and smoking. When identifying patients at risk of disease progression, efforts can be made to implement prevention, early detection, and complication avoidance [100].
During COVID-19 pandemic, the impact of SARS-CoV-2 infection on various aspects of human physiology has garnered significant attention. Among others, the virus's impact on blood pressure regulation has been pointed. The studies over COVID-19 patients revealed different, sometimes even contrary, effects on BP changes. The possible pathomechanisms include disturbances of RAAS, endothelial damage, systemic inflammatory response, autonomic nervous system dysfunction or lifestyle changing.
4.1. Research Supporting BP Increase as a Complication of Long COVID
One of the pilot studies, "COVID-19 blood pressure endothelium interaction study" (OBELIX), found that participants with no history of hypertension, who had COVID-19 infection more than 12 weeks befour, exhibited higher systolic blood pressure, than those who did not suffer from COVID-19 [36].
Solon A. et al. [90], Alfadda et al. [67], Gameil et al. [64] and Mahmoud et al. [69] found significantly higher systolic blood pressure in individuals who had experienced SARS-CoV-2 infection. Their hypothesis posits that COVID-19 induced alterations in sympathetic activity, endothelial function or inflammatory response leading to disruptions in blood pressure regulation.
Referring to findings of Lopez-Leon S et al. [102], the researchers speculated that these adjustment in mentioned above hypotesis were linked to post-COVID-19 symptoms. They also did not exclude the influence of the pandemic and its accompanying feelings of fear, anxiety, psychological disorders and reduced physical activity, which could potentially have worsened blood pressure control.
The above findings highlighted the clinical phenotypes of cardiovascular manifestations of post-acute sequelae of SARS-CoV-2 (PASC), but did not clarify the pathophysiology.
Furthermore, Ratchford et al. [72] discovered higher mean systolic and diastolic blood pressure in the group of young adults positive tested for SARS-CoV-2 3–4 week prior to study compared with a control group of healthy young adults through a short observation, which lasted 25 ± 5 days. It is interesting to add, other results provided evidence for impaired nitric oxide bioavailability and reduced vascular function caused by SARS-CoV-2. This hypothesis was formulated based on the results of the brachial artery flow-mediated dilation (FMD) and single passive limb movement (sPLM) tests, which are likely functional biological tests for endothelium-derived NO [95,96,97]. Lower responses in these tests were demonstrated among individuals tested positive for SARS-CoV-2 presence 3-4 weeks prior to the study [97].
Tanni SE et al. [66] observed young adults about 99 days after the diagnosis of COVID-19. The subjects’ systolic and diastolic blood pressure increased slightly but significantly compared to the baseline values. In contrast, there were no correlations between symptoms and inflammatory or cardiac biomarkers.
Another scientists performed assessment of BP using ambulatory blood pressure monitoring (ABPM). The analysis revealed elevated blood pressure values during wakefulness and sleep, as well as a smaller nocturnal drop in young patients with diagnosed long-COVID syndrome compared to an age-matched healthy subjects who had not suffered from it. This abnormalities can increases the risk of cardiovascular events in future [75].
Akpek et al. [73] have also shown an increase of blood pressure that meets the criteria for hypertension diagnosis in 18 from 153 observed patients with diagnosed COVID-19. Only 5% of the study population were hospitalized during infection.
These approaches were also seen by Vyas et al. [87]. The study revealed that 32.3% of individuals experienced new-onset arterial hypertension one year after their recovery from COVID-19. A significant association was identified between severe inflammation, high computed tomography (CT) score severity, treatment with steroids during the hospital stay and the emergence of new-onset hypertension during the observation period. According to the authors those data suggested the potential impact of SARS-CoV-2 on inflammatory and renin-angiotensin-aldosterone systems, ACE-2 involvement, and baroreceptor dysfunction thus the occurrence of hypertension is worth considering.
These outcomes corresponded with the analysis of Xiong et al. [59] from Wuhan conducted on seven patients recently diagnosed with COVID-19. They developed high blood pressure within three months after discharge from the hospital and required antihypertensive medications despite having no history of hypertension prior to the COVID-19 illness.
Overall the above-mentioned observations are in accordance with findings reported by Mei et al. [60], where after a median follow-up of 144 days, six individuals developed hypertension as a consequence of the infections. In another study conducted on a group of 796 patients, with a follow-up observation of 6 months, new onset hypertension was diagnosed only in 0,4% participants. The main limitation of this study was that most of the symptoms were recorded as patient’s subjective descriptions and wasn’t focus of BP, but general about sequelae SARS-CoV-2 [61].
The interesting study was made by Delalic et al. [76]. They observed hypertension as a COVID-19 outcome affected approximately 16% of 200 patients. The authors concluded that about 1 of 6 individuals infected with COVID-19 are at risk for developing arterial hypertension or worsening pre-existing disease. Unfortunately, no laboratory markers were found to predict arterial hypertension following COVID-19 in this study. Additionally, the risk of worsening blood pressure control was demonstrated by a group of researchers from San Raffaele University Hospital in Milan [77]. In their study, forty patients (21,6%) had uncontrolled BP requiring changes in treatment after observation lasting from 20 to 29 days. According to authors, potential pathomechanisms may include endothelial dysfunction, the proinflammatory state, as well as the dysfunctional innate immune response common to both metabolic and viral disorders
In another study also made by Nandadewa D. et al. [91], it was demonstrated that women with post-acute sequelae of SARS-CoV-2 (PASC) exhibited elevated resting BP and central artery stiffness in comparison to the control group. These findings point towards an increased susceptibility of arterial hypertension development in women with PASC, irrespective of the severity of symptoms. Notably, the majority of PASC patients did not have hypertension prior to their COVID-19 illness, but post-COVID-19, there were instances of new hypertension diagnoses and elevated BP readings. These observations underscore the potential long-term cardiovascular implications of PASC.
Abumayyaleh M et al. [88] study was planned slightly from another perspective. Although the study concerned individuals with diabetes, results were also available for the control group of people without it. Data were collected from hospitalized patients with confirmed COVID-19 after an average observation period of 2.6 ± 4.6 months. It was demonstrated that the incidence of newly diagnosed arterial hypertension was slightly lower among patients with diabetes and amounted to 0,5% compared to 1,6% those without diabetes.
Subsequent studies referenced demonstrated the emergence of new-onset hypertension in individuals who recovered from COVID-19 infection. This condition was diagnosed within the timeframe of 4 to 12 months following their hospital post-infection discharge. The identification of new-onset hypertension was established by reviewing the clinical records of the enrolled patients.
Mizrahi B's [84] nationwide study proposed that patients with mild COVID-19 faced a hypertension burden of 1.27 and that those effects resolved within a year from the time of diagnosis. Another group of investigators reported an even higher rate, at 1.81 (with a 95% confidence interval ranging from 1.10 to 2.96). On the other hand, the study conveyed that the heightened risk of these complications persisted only for up to six months after the infection [68]. While the hazard ratio for hypertension in individuals with breakthrough SARS-CoV-2 infection, compared to the contemporary control group established by Al-Aly Z et al. [83], was estimated at 1.62. In a nationwide cohort study conducted by Tisler A. et al. [78], which spanned a 12-month period, hospitalized adults with confirmed COVID-19 were tracked alongside matched disease-free control groups from the general population. The risk of developing arterial hypertension was calculated to be 2.85.
Whereas Cohen K et al. [82] estimated excess risk and risk ratios of persistent and novel clinical consequences resulting from SARS-CoV-2 among adults aged >65 years during the post-acute phase of infection. In relation to arterial hypertension, the calculated coefficient stood at 4.43 (with a range of 2.27 to 6.37).
Another an international examination of electronic patient records from 277 hospitals was performed by Zhang HG et al. [81] Based on their analysis, an elevated risk of arterial hypertension was noted among patients post-COVID-19 infection. Interestingly, this risk was more pronounced among ambulatory patients compared to those who were hospitalized during the infection.
Based on the national databases of the United States Department of Veterans Affairs, among COVID-19 patients who survived at least 30 days after diagnosis and were not hospitalized, also excessive burden of arterial hypertension was observed (15.18 (11.53–18.62)). Interestingly, a comparison was made between coronavirus infection and influenza, revealing a higher burden of post-infection diseases as a consequence of SARS-CoV-2 infection. [92]
In the next cited studies, the risk factor for developing hypertension after COVID-19 was also made. Özcan et al [63], based on the observation of 406 patients after 3 and 6 months following hospitalization due to coronavirus disease, established the risk of arterial hypertension at 1.229 (0.748 – 2.019). They thought, similarly to other previous described, this may be related to ACE-2, which acts as the receptor for SARS-CoV-2.
Additionaly, Ogungbe O et al. [80], through a survey-based investigation, collected data indicating that 20% of surveyed patients were newly diagnosed with hypertension.
In the United States, a large study was conducted during COVID-19 as part of the Livongo Hypertension Program, which involved digital blood pressure measurements. After analyzing the results of 72,706 participants, it was found the monthly adjusted mean Systolic blood pressure (SBP) and diastolic blood pressure (DBP) and mean arterial pressure (MAP) were higher than before the pandemic outbreak. There was also an increase in the percentage of participants with monthly average BP classified as uncontrolled or severely uncontrolled hypertension [93]. A similar study is conducted by Excellence Centres of the European Society of Hypertension [94]. The aim of their report is to check the impact of a COVID-19 pandemic on blood pressure control by analysing results of ABPM in the pandemic period com-pared with the pre-pandemic one.
However, based on the collected data, it is not possible to determine the causes of such as effect. Some participants may have had COVID-19 infection during the study, but the increase in blood pressure could also be a result of lifestyle changes, isolation, or anxiety. Furthermore, it is worth recalling the concerns regarding antihypertensive medications that arose shortly after the outbreak of the pandemic. There were reports suggesting that the use of RAS inhibitors might increase the risk and/or severity of SARS-CoV-2 infection. This led to the discontinuation of treatment with these drugs in a significant number of patients. However, these data were not reflected in the studies. There are reports available indicating that the pandemic had a negative impact on patients with arterial hypertension adhering to medical recommendations [95].
In addition to the mentioned studies, it's worth citing one more papers. González-Hermosillo et al. [89] conducted a study in which they investigated hospitalized patients with COVID-19-associated pneumonia who developed Post-acute sequelae of SARS-CoV-2 and had no hypertension at discharge. Approximately 10.8 ± 1.9 months post-discharge, a head-up tilt test revealed an abnormal increase in blood pressure during orthostatic provocation in one-third of the examined individuals. The researchers suggest that orthostatic blood pressure elevation might herald overt hypertension in later life.
4.2. Studies Suggesting a Transient Increase in BP Following an Acute COVID-19 Infection
A similar pattern of results was obtained by the group of researchers from Italy [62]. Blood pressure was elevated in 25,8% participants approximately 30 days after discharge from the hospital. However, what was observed so far during the follow-up visit, only 14% still exhibited this abnormality. The abnormal value of CRP, elevated ferritin level and D-dimer level also decreased during observation. It is important to highlight the fact that this condition was more common in hospitalized patients, treated with steroids and oxygen therapy.
Reduction in blood pressure values over time was also detected in other analyses. Fernández-Ortega MÁ et al. [85] observed 71 individuals who had survived COVID-19-related pneumonia and had been hospitalized. Data for the registry were collected via telephone interviews after 5 months from hospital discharge, and then again after 12 months from that date. At the 5-month mark, hypertension was present in every third patient (29.7%) who did not have hypertension prior to COVID-19, decreasing annually to 12.5%.
In the longitudinal investigation carried out by Steinmetz A. [79] as well as the mentioned group before, blood pressure demonstrated a gradual reduction over time with observations extending for a minimum of 6 weeks post-acute infection. However, the blood pressure was not relevantly elevated during the whole observation period.
On the other hand, Stute et al. [70] performed study assesing the impact of SARS-CoV-2 on sympathetic neural activity and hemodynamics over 6 months following SARS-CoV-2 infection. Sympathetic neural parameters was estimated using the microneurographic technique, muscle sympathetic nerve activity (MSNA) and transduction was calculated using an open-source program by O'Brien et al. [101]. Unfortunately, the study was limited to a small group of ten patients. SBP and DBP were measured three times over 6 months first after 43 ± 16 days of infection, then after 103 ± 14 days, and finally after 168 ± 16 days. It was established that SBP and DBP decreased throughout recovery from mild SARS-CoV-2 infection. Authors hypothesized that the increase resting MSNA, caused hypertension, was elicited by elevated inflammatory cytokines during SARS-CoV-2 infection. However, the improvements in BP over 6 months of recovery from mild SARS-CoV-2 infection are unlikely due to changes in sympathetic activity.
4.3. Studies in Which No Changes in BP Values Were Observed after COVID-19
Contrary to the above findings, the results of studies conducted by researchers from the Netherlands did not mention any differences in blood pressure. The authors studied a group of nonhospitalized patients with COVID-19, at a median of 6 months post infection [65]. A similar conclusion was obtained by the team led by Nandadewa [74]. In their results, ambulatory daytime, nighttime, and 24-h SBP, DBP, and mean BP were not different between the control and COVID-19 group. It cannot be ruled out the transient effects of COVID-19 may include elevated BP and central arterial stiffness but closer to the diagnosis. The study presented some limitations such as small study population of 28 young adults who had COVID-19 and 10 controls, which may affect the accuracy of the results. Interestingly, an earlier work by the same author was cited, which demonstrated increased arterial blood pressure in women with PASC.
Jennifer K et al. [86], based on an analysis of both hospital and community control data documentation for up to 14 months, also did not find differences in the occurrence of hypertension in the control group and after recovering from COVID-19.
5. Conclusions
Despite the subsiding acute phase of SARS-CoV-2 infection, it is estimated the patients may experience persistent symptoms associated with the past infection. Findings from this review suggested, the blood pressure of individuals who have undergone COVID-19 was higher than prior to the infection and may even meet the criteria for diagnosis of arterial hypertension. Only two of the discussed research studies contraindicated this hypothesis. The most common cause of blood pressure changes due to SARS-CoV-2 infection proposed by various authors is interaction with ACE-2 receptor, endothelial dysfunction, and generalized inflammatory response. But the mechanism behind these alterations has not been definitively established yet.
Undoubtedly, this is an area for further research that will help explain the risk of developing arterial hypertensions in individuals who have undergone COVID-19 infection. A major cause of limitation of describing evaluations was a small participants number and too short period of time. Further studies still are needed to explore the topic more thoroughly and determine whether increased blood pressure can be linked to COVID-19 infection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Davis, H.E.; McCorkell, L.; Vogel, J.M. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Living with Covid19. 2020. Available online: https://evidence.nihr.ac.uk/themedreview/living-with-covid19/ (accessed on April 2023).
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir. Med. 2021, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Post COVID-19 Condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on April 2023).
- Munblit, D.; O'Hara, M.E.; Akrami, A.; Perego, E.; Olliaro, P.; Needham, D.M. Long COVID: Aiming for a consensus. Lancet Respir. Med. 2022, 10, 632–634. [Google Scholar] [CrossRef] [PubMed]
- Parhizgar, P.; Yazdankhah, N.; Rzepka, A.M.; Chung, K.Y.C.; Ali, I.; Lai Fat Fur, R.; Russell, V.; Cheung, A.M. Beyond Acute COVID-19: A Review of Long-term Cardiovascular Outcomes. Can. J. Cardiol. 2023, 39, 726–740. [Google Scholar] [CrossRef]
- Otifi, H.M.; Adiga, B.K. Endothelial Dysfunction in Covid-19 Infection. Am. J. Med. Sci. 2022, 363, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Alcocer-Díaz-Barreiro, L.; Cossio-Aranda, J.; Verdejo-Paris, J.; Odin-de-Los-Ríos, M.; Galván-Oseguera, H.; Álvarez-López, H.; Alcocer-Gamba, M.A. COVID-19 and the renin, angiotensin, aldosterone system. A complex relationship. Arch. Cardiol. Mex. 2020, 90, 19–25. [Google Scholar] [PubMed]
- Ferrario, C.M.; Chappell, M.C.; Tallant, E.A.; Brosnihan, K.B.; Diz, D.I. Counterregulatory actions of angiotensin-(1-7). Hypertension 1997, 30, 535–541. [Google Scholar] [CrossRef]
- Roks, A.J.; van Geel, P.P.; Pinto, Y.M.; Buikema, H.; Henning, R.H.; de Zeeuw, D.; van Gilst, W.H. Angiotensin-(1-7) is a modulator of the human renin-angiotensin system. Hypertension 1999, 34, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Ohishi, M.; Katsuya, T.; Ito, N.; Ikushima, M.; Kaibe, M.; Tatara, Y.; Shiota, A.; Sugano, S.; Takeda, S.; Rakugi, H.; Ogihara, T. Deletion of angiotensin-converting enzyme 2 accelerates pressure overload-induced cardiac dysfunction by increasing local angiotensin II. Hypertension 2006, 47, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Vickers C, Hales P, Kaushik V, Dick L, Gavin J, Tang J, Godbout K, Parsons T, Baronas E, Hsieh F, Acton S, Patane M, Nichols A, Tummino P. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J Biol Chem. 2000, 277, 14838–14843. [Google Scholar]
- Gurley, S.B.; Allred, A.; Le, T.H.; Griffiths, R.; Mao, L.; Philip, N.; Haystead, T.A.; Donoghue, M.; Breitbart, R.E.; Acton, S.L.; Rockman, H.A.; Coffman, T.M. Altered blood pressure responses and normal cardiac phenotype in ACE2-null mice. J. Clin. Invest. 2006, 116, 2218–2225. [Google Scholar] [CrossRef]
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/MAS Axis of the Renin-Angiotensin System: Focus on Angiotensin-(1-7). Physiol Rev. 2018, 98, 505–553. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, V.; Gjymishka, A.; Jarajapu, Y.P.; Qi, Y.; Afzal, A.; Rigatto, K.; Ferreira, A.J.; Fraga-Silva, R.A.; Kearns, P.; Douglas, J.Y.; et al. Diminazene attenuates pulmonary hypertension and improves angiogenic progenitor cell functions in experimental models. Am. J. Respir. Crit. Care Med. 2013, 187, 648–657. [Google Scholar] [CrossRef]
- Ferreira, A.J.; Shenoy, V.; Yamazato, Y.; Sriramula, S.; Francis, J.; Yuan, L.; Castellano, R.K.; Ostrov, D.A.; Oh, S.P.; Katovich, M.J.; Raizada, M.K. Evidence for angiotensin-converting enzyme 2 as a therapeutic target for the prevention of pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2009, 179, 1048–1054. [Google Scholar] [CrossRef]
- Feng, Y.; Xia, H.; Santos, R.A.; et al. Angiotensin-converting enzyme 2: A new target for neurogenic hypertension. Exp. Physiol. 2010, 95, 601–606. [Google Scholar] [CrossRef]
- Grimes, J.M.; Grimes, K.V. p38 MAPK inhibition: A promising therapeutic approach for COVID-19. J. Mol. Cell Cardiol. 2020, 144, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Tomasoni, D.; Italia, L.; Adamo, M.; et al. COVID-19 and heart failure: From infection to inflammation and angiotensin II stimulation. Searching for evidence from a new disease. Eur. J. Heart Fail. 2020, 22, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Oudit, G.Y.; Pfeffer, M.A. Plasma angiotensin-converting enzyme 2: Novel biomarker in heart failure with implications for COVID-19. Eur. Heart J. 2020, 41, 1818–1820. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.; Vasilieva, N.; Sui, J.; Wong, S.; Berne, M.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Wrapp, D.; Wang, N.; Corbett, K.; Goldsmith, J.; Hsieh, C.; Abiona, O.; et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Gui, M.; Wang, X.; Xiang, Y. Cryo-EM structure of the SARS coronavirus spike glycoprotein in complex with its host cell receptor ACE2. PLoS Pathog. 2018, 14, 1007236. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, W.; Farzan, M.; Harrison, S. Structure of SARS coronavirus spike receptor-binding domain complexed with receptor. Science 2005, 309, 1864–1868. [Google Scholar] [CrossRef]
- Ni, W.; Yang, X.; Yang, D. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care 2020, 24, 422. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Look, D.; Tan, P.; Shi, L.; Hickey, M.; Gakhar, L.; et al. Ectodomain shedding of angiotensin converting enzyme 2 in human airway epithelia. Am. J. Physiol. Lung Cell Mol. Physiol. 2009, 297, 84–96. [Google Scholar] [CrossRef]
- Heurich, A.; Hofmann-Winkler, H.; Gierer, S.; Liepold, T.; Jahn, O.; Pöhlmann, S. TMPRSS2 and ADAM17 cleave ACE2 differentially and only proteolysis by TMPRSS2 augments entry driven by the severe acute respiratory syndrome coronavirus spike protein. J. Virol. 2014, 88, 1293–1307. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Li, F. Structure, function, and evolution of coronavirus spike proteins. Annu. Rev. Virol. 2016, 3, 237–261. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Chien, S.; Chen, I.; Lai, C.; Tsay, Y.; Chang, S.; Chang, M. Surface vimentin is critical for the cell entry of SARS-CoV. J. Biomed. Sci. 2016, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Tanaka, N.; Tanaka, Y.; Inoue, S.; Morita, K.; Zhuang, M.; et al. Clathrin-dependent entry of severe acute respiratory syndrome coronavirus into target cells expressing ACE2 with the cytoplasmic tail deleted. J. Virol. 2007, 81, 8722–8729. [Google Scholar] [CrossRef] [PubMed]
- Holmes, K.V.; et al. Coronavirus receptor specificity. Adv. Exp. Med. Biol. 1993, 342, 261–266. [Google Scholar] [PubMed]
- Glowacka, I.; Bertram, S.; Herzog, P.; Pfefferle, S.; Steffen, I.; Muench, M.O.; Simmons, G.; Hofmann, H.; Kuri, T.; Weber, F.; Eichler, J.; Drosten, C.; Pöhlmann, S. Differential downregulation of ACE2 by the spike proteins of severe acute respiratory syndrome coronavirus and human coronavirus NL63. J Virol. 2010, 84, 1198–1205. [Google Scholar] [CrossRef]
- Nappi, F.; Avtaar Singh, S.S. Endothelial Dysfunction in SARS-CoV-2 Infection. Biomedicines 2022, 10, 654. [Google Scholar] [CrossRef]
- Gathiram, P.; Mackraj, I.; Moodley, J. The Renin-Angiotensin System, Hypertension, and SARS-CoV-2 Infection: A Review. Curr. Hypertens. Rep. 2021, 23, 17. [Google Scholar] [CrossRef]
- Lip, S.; Mccallum, L.; Delles, C.; McClure, J.D.; Guzik, T.; Berry, C.; Touyz, R.; Padmanabhan, S. Rationale and Design for the LOnger-term effects of SARS-CoV-2 INfection on blood Vessels And blood pRessure (LOCHINVAR): An observational phenotyping study. Open Heart. 2022, 002057. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Stampfer, M.J.; Curhan, G.C. Diet and lifestyle risk factors associated with incident hypertension in women. JAMA 2009, 302, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Sonne-Holm, S.; Sørensen, T.I.; Jensen, G.; Schnohr, P. Independent effects of weight change and attained body weight on prevalence of arterial hypertension in obese and non-obese men. BMJ 1989, 299, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Raman, B.; Cassar, M.P.; Tunnicliffe, E.M.; Filippini, N.; Griffanti, L.; Alfaro-Almagro, F.; Okell, T.; Sheerin, F.; Xie, C.; Mahmod, M.; et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine 2021, 31, 100683. [Google Scholar] [CrossRef] [PubMed]
- Shouman, K.; Vanichkachorn, G.; Cheshire, W.P. Autonomic dysfunction following COVID-19 infection: An early experience. Clin Auton Res 2021, 31, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.L.; Leong, H.N.; Hsu, L.Y.; Tan, T.T.; Kurup, A.; Fook-Chong, S.; Tan, B.H. Autonomic dysfunction in recovered severe acute respiratory syndrome patients. Can. J. Neurol. Sci. 2005, 264. [Google Scholar] [CrossRef]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.J.; Feigen, C.M.; Vazquez, J.P.; Kobets, A.J.; Altschul, D.J. Neurological Sequelae of COVID-19. J. Integr. Neurosci. 2022, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yao, S.; Sun, G.; Yu, S.; Sun, Z.; Zheng, L.; Xu, C.; Li, J.; Sun, Y. Total and abdominal obesity among rural Chinese women and the association with hypertension. Nutrition 2012, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Itoh, H. Hypertension as a Metabolic Disorder and the Novel Role of the Gut. Curr. Hypertens. Rep. 2019, 21, 63. [Google Scholar] [CrossRef]
- Becker, R.C. Autonomic dysfunction in SARS-COV-2 infection acute and long-term implications COVID-19 editor's page series. J. Thromb. Thombolysis. 2021, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Goodman, B.P.; Khoury, J.A.; Blair, J.E.; Grill, M.F. COVID-19 Dysautonomia. Front. Neurol. 2021, 12, 624968. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborreli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; et al. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Jolkkoken, J.; Zhao, C. Neurotropism of SARS-CoV-2 and its neuropathological alterations: Similarities with other coronaviruses. Neurosci. Biobehav. Rev. 2020, 11, 184–193. [Google Scholar] [CrossRef]
- Marques, K.C.; Silva, C.C.; Trindade, S.d.S.; Santos, M.C.d.S.; Rocha, R.S.B.; Vasconcelos, P.F.d.C.; Quaresma, J.A.S.; Falcão, L.F.M. Reduction of Cardiac Autonomic Modulation and Increased Sympathetic Activity by Heart Rate Variability in Patients With Long COVID. Front. Cardiovasc. Med. 2022, 9, 862001. [Google Scholar] [CrossRef]
- Balcom, E.F.; Nath, A.; Power, C. Acute and chronic neurological disorders in COVID-19: Potential mechanisms of disease. Brain 2021, 144, 3576–3588. [Google Scholar] [CrossRef] [PubMed]
- Hultström, M.; von Seth, M.; Frithiof, R. Hyperreninemia and low total body water may contribute to acute kidney injury in COVID-19 patients in intensive care. J. Hypertens. 2020, 1613–1614. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.; Tadic, M.; Larsen, T.H.; Grassi, G.; Mancia, G. Coronavirus disease 2019 and cardiovascular complications: Focused clinical review. J. Hypertens. 2021, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Konukoglu, D.; Uzun, H. Endothelial dysfunction and hypertension. Adv. Exp. Med. Biol. 2017, 956, 511–540. [Google Scholar] [PubMed]
- Rogier van der Velde, A.; Meijers, W.C.; de Boer, R.A. “Chapter 3.7.1 - Cardiovascular biomarkers: Translational aspects of hypertension, atherosclerosis, and heart failure in drug development,” in Principles of Translational Science in Medicine, 2nd Edn. ed. M. Wehling (Boston, MA: Academic Press), 2015, pp 167–183.
- Muhamad, S.-A.; Ugusman, A.; Kumar, J.; Skiba, D.; Hamid, A.A.; Aminuddin, A. COVID-19 and Hypertension: The What, the Why, and the How. Front. Physiol. 2021, 12, 665064. [Google Scholar] [CrossRef]
- Ambrosino, P.; Parrella, P.; Formisano, R.; Perrotta, G.; D'Anna, S.E.; Mosella, M.; Papa, A.; Maniscalco, M. Cardiopulmonary Exercise Performance and Endothelial Function in Convalescent COVID-19 Patients. J. Clin. Med. 2022, 11, 1452. [Google Scholar] [CrossRef]
- Charfeddine, S.; Ibn Hadj Amor, H.; Jdidi, J.; Torjmen, S.; Kraiem, S.; Hammami, R.; Bahloul, A.; Kallel, N.; Moussa, N.; Touil, I.; et al. Long COVID 19 Syndrome: Is It Related to Microcirculation and Endothelial Dysfunction? Insights From TUN-EndCOV Study. Front. Cardiovasc. Med. 2021, 8, 745758. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2021, 89–95. [Google Scholar] [CrossRef]
- Mei, Q.; Wang, F.; Yang, Y.; Hu, G.; Guo, S.; Zhang, Q.; Bryant, A.; Zhang, L.; Kurts, C.; Wei, L.; Yuan, X.; Li, J. Health Issues and Immunological Assessment Related to Wuhan's COVID-19 Survivors: A Multicenter Follow-Up Study. Front Med (Lausanne). 2021, 8, 617689. [Google Scholar] [CrossRef]
- Shang, Y.F.; Liu, T.; Yu, J.N.; Xu, X.R.; Zahid, K.R.; Wei, Y.C.; Wang, X.H.; Zhou, F.L. Half-year follow-up of patients recovering from severe COVID-19: Analysis of symptoms and their risk factors. J. Intern. Med. 2021, 290, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Boglione, L.; Meli, G.; Poletti, F.; Rostagno, R.; Moglia, R.; Cantone, M.; Esposito, M.; Scianguetta, C.; Domenicale, B.; Di Pasquale, F.; et al. Risk factors and incidence of long-COVID syndrome in hospitalized patients: Does remdesivir have a protective effect? QJM Int. J. Med. 2021, 14, 865–871. [Google Scholar] [CrossRef] [PubMed]
- 63. Özcan S, İnce O, Güner A, Katkat F, Dönmez E, Tuğrul S, Şahin İ, Okuyan E, Kayıkçıoğlu M. Long-Term Clinical Consequences of Patients Hospitalized for COVID-19 Infection. Anatol. J. Cardiol. 2022, 305–315.
- Gameil, M.A.; Marzouk, R.E.; Elsebaie, A.H.; et al. Long-term clinical and biochemical residue after COVID-19 recovery. Egypt. Liver Journal 2021, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- van der Sluijs, K.M.; Bakker, E.A.; Schuijt, T.J.; Joseph, J.; Kavousi, M.; Geersing, G.J.; Rutten, F.H.; Hartman, Y.A.W.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Long-term cardiovascular health status and physical functioning of nonhospitalized patients with COVID-19 compared with non-COVID-19 controls. Am. J. Physiol. Heart Circ. Physiol. 2023, 324, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Tanni, S.E.; Tonon, C.R.; Gatto, M.; Mota, G.A.F.; Okoshi, M.P. Post-COVID-19 syndrome: Cardiovascular manifestations. Int. J. Cardiol. 2022, 369, 80–81. [Google Scholar] [CrossRef]
- Alfadda, A.A.; Rafiullah, M.; Alkhowaiter, M.; Alotaibi, N.; Alzahrani, M.; Binkhamis, K.; Siddiqui, K.; Youssef, A.; Altalhi, H.; Almaghlouth, I.; et al. Clinical and biochemical characteristics of people experiencing post-coronavirus disease 2019-related symptoms: A prospective follow-up investigation. Front. Med. 2022, 9, 1067082. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, S.E.; Guo, Y.; Heath, K.; Dasmariñas, M.C.; Jubilo, K.G.; Samranvedhya, J.; Lipsitch, M.; Cohen, K. Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ. 2021, 373, 1098. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, Z.; East, L.; Gleva, M.; Woodard, P.K.; Lavine, K.; Verma, A.K. Cardiovascular symptom phenotypes of post-acute sequelae of SARS-CoV-2. Int. J. Cardiol. 2022, 22, S0167–5273. [Google Scholar] [CrossRef] [PubMed]
- Stute, N.L.; Szeghy, R.E.; Stickford, J.L.; Province, V.P.; Augenreich, M.A.; Ratchford, S.M.; Stickford, A.S.L. Longitudinal observations of sympathetic neural activity and hemodynamics during 6 months recovery from SARS-CoV-2 infection. Physiol. Rep. 2022, 10, e15423. [Google Scholar] [CrossRef]
- Szeghy, R.E.; Province, V.M.; Stute, N.L.; Augenreich, M.A.; Koontz, L.K.; Stickford, J.L.; Stickford, A.S.L.; Ratchford, S.M. Carotid stiffness, intima-media thickness and aortic augmentation index among adults with SARS-CoV-2. Exp Physiol. 2022, 107, 694–707. [Google Scholar] [CrossRef]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S.L. Vascular alterations among young adults with SARS-CoV-2. Am J Physiol Heart Circ Physiol. 2021, 320, 404–410. [Google Scholar] [CrossRef]
- Akpek, M. Does COVID-19 Cause Hypertension? Angiology 2022, 73, 682–687. [Google Scholar] [CrossRef]
- Nandadeva, D.; Skow, R.J.; Grotle, A.K.; Stephens, B.Y.; Young, B.E.; Fadel, P.J. Impact of COVID-19 on ambulatory blood pressure in young adults: A cross-sectional analysis investigating time since diagnosis. J Appl Physiol (1985). 2022, 133, 183–190. [Google Scholar] [CrossRef]
- Tetyana, M.; Ternushchak Marianna, I.; Tovt-Korshynska Antonina, V. Varvarynets AMBULATORY BLOOD PRESSURE VARIABILITY IN YOUNG ADULTS WITH LONG-COVID SYNDROME, Wiadomości Lekarskie, VOLUME LXXV, ISSUE 10, OCTOBER 2022, 75, 2481–2485.
- Delalić, Đ.; Jug, J.; Prkačin, I. ARTERIAL HYPERTENSION FOLLOWING COVID-19: A RETROSPECTIVE STUDY OF PATIENTS IN A CENTRAL EUROPEAN TERTIARY CARE CENTER. Acta Clin. Croat. 2022, 61, 23–27. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, R.; Conte, C.; Lanzani, C.; Benedetti, F.; Roveri, L.; Mazza, M.G.; Brioni, E.; Giacalone, G.; Canti, V.; Sofia, V.; et al. Residual clinical damage after COVID-19: A retrospective and prospective observational cohort study. PLoS ONE 2020, 15, e0239570. [Google Scholar] [CrossRef] [PubMed]
- Tisler, A.; Stirrup, O.; Pisarev, H.; Kalda, R.; Meister, T.; Suija, K.; Kolde, R.; Piirsoo, M.; Uusküla, A. Post-acute sequelae of COVID-19 among hospitalized patients in Estonia: Nationwide matched cohort study. PLoS ONE 2022, 17. [Google Scholar] [CrossRef]
- Steinmetz, A.; Gross, S.; Lehnert, K.; Lücker, P.; Friedrich, N.; Nauck, M.; Bahlmann, S.; Fielitz, J.; Dörr, M. Longitudinal Clinical Features of Post-COVID-19 Patients—Symptoms, Fatigue and Physical Function at 3- and 6-Month Follow-Up. J. Clin. Med. 2023, 12, 3966. [Google Scholar] [CrossRef] [PubMed]
- Ogungbe, O.; Gilotra, N.A.; Davidson, P.M.; et al. ardiac postacute sequelae symptoms of SARS-CoV-2 in community-dwelling adults: Cross-sectional study. Open Heart 2022, 9, e002084. [Google Scholar] [CrossRef]
- Zhang, H.G.; Dagliati, A.; Shakeri Hossein Abad, Z.; Xiong, X.; Bonzel, C.L.; Xia, Z.; Tan, B.W.Q.; Avillach, P.; Brat, G.A.; Hong, C.; et al. Consortium for Clinical Characterization of COVID-19 by EHR (4CE); Cai T, South AM, Kohane IS, Weber GM. International electronic health record-derived post-acute sequelae profiles of COVID-19 patients. NPJ Digit. Med. 2022, 5, 81. [Google Scholar] [CrossRef] [PubMed]
- Cohen, K.; Ren, S.; Heath, K.; Dasmariñas, M.C.; Jubilo, K.G.; Guo, Y.; Lipsitch, M.; Daugherty, S.E. Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ 2022, 376. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Mizrahi, B.; Sudry, T.; Flaks-Manov, N.; Yehezkelli, Y.; Kalkstein, N.; Akiva, P.; Ekka-Zohar, A.; Ben David, S.S.; Lerner, U.; Bivas-Benita, M.; Greenfeld, S. Long covid outcomes at one year after mild SARS-CoV-2 infection: Nationwide cohort study. BMJ. 2023, 380. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ortega, M.Á.; Ponce-Rosas, E.R.; Muñiz-Salinas, D.A.; Rodríguez-Mendoza, O.; Nájera Chávez, P.; Sánchez-Pozos, V.; Dávila-Mendoza, R.; Barrell, A.E. Cognitive dysfunction, diabetes mellitus 2 and arterial hypertension: Sequelae up to one year of COVID-19. Travel Med Infect Dis. 2023, 52, 102553. [Google Scholar] [CrossRef]
- Jennifer, K.; Shirley, S.B.D.; Avi, P.; Daniella, R.C.; Naama, S.S.; Anat, E.Z.; Miri, M.R. Post-acute sequelae of COVID-19 infection. Prev. Med. Rep. 2023, 31, 102097. [Google Scholar] [CrossRef] [PubMed]
- Vyas, P.; Joshi, D.; Sharma, V.; Parmar, M.; Vadodariya, J.; Patel, K.; Modi, G. Incidence and predictors of development of new onset hypertension post COVID-19 disease. Indian. Heart J. 2023, 0019-4832, 00103–00107. [Google Scholar] [CrossRef] [PubMed]
- Abumayyaleh, M.; Núñez Gil, I.J.; Viana-LLamas, M.C.; Raposeiras Roubin, S.; Romero, R.; Alfonso-Rodríguez, E.; Uribarri, A.; Feltes, G.; Becerra-Muñoz, V.M.; Santoro, F.; et al. HOPE COVID-19 investigators. Post-COVID-19 syndrome and diabetes mellitus: A propensity-matched analysis of the International HOPE-II COVID-19 Registry. Front Endocrinol (Lausanne). 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- González-Hermosillo, G.J.A.; Galarza, E.J.; Fermín, O.V.; González, J.M.N.; Tostado, L.M.F.Á.; Lozano, M.A.E.; Rabasa, C.R.; Martínez Alvarado, M.D.R. Exaggerated blood pressure elevation in response to orthostatic challenge, a post-acute sequelae of SARS-CoV-2 infection (PASC) after hospitalization. Auton. Neurosci. 2023, 247. [Google Scholar] [CrossRef]
- Saloň, A.; Neshev, R.; Teraž, K.; Šimunič, B.; Peskar, M.; Marušič, U.; Pišot, S.; Šlosar, L.; Gasparini, M.; Pišot, R.; et al. A pilot study: Exploring the influence of COVID-19 on cardiovascular physiology and retinal microcirculation. Microvasc. Res. 2023, 150, 104588. [Google Scholar] [CrossRef] [PubMed]
- Nandadeva, D.; Skow, R.J.; Stephens, B.Y.; Grotle, A.-K.; Georgoudiou, S.; Barshikar, S.; Seo, Y.; Paul, J. Fadel American Journal of Physiology-Heart and Circulatory Physiology 2023, 6, 713–720. 6.
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.P.; Clare, R.M.; Chiswell, K.; Navar, A.M.; Shah, B.R.; Peterson, E.D. Trends of blood pressure control in the U.S. during the COVID-19 pandemic. Am. Heart J. 2022, 247, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Wojciechowska, W.; Rajzer, M.; Weber, T.; Prejbisz, A.; Dobrowolski, P.; Ostrowska, A.; et al. Ambulatory blood pressure monitoring in treated patients with hypertension in the COVID-19 pandemic - the study of European society of hypertension (ESH ABPM COVID-19 study). Blood Press. 2023, 322161998. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Spiegelhalter, D.J.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Joannides, R.; Haefeli, W.E.; Linder, L.; Richard, V.; Bakkali, E.H.; Thuillez, C.; Luscher, T.F. Nitric oxide is responsible for flow-dependent dilatation of human peripheral conduit arteries in vivo. Circulation 1995, 91, 1314–1319. [Google Scholar] [CrossRef]
- Harris, R.A.; Nishiyama, S.K.; Wray, D.W.; Richardson, R.S. Ultrasound assessment of flow-mediated dilation. Hypertension 2010, 55, 1075–1085. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.S.; Coronado, F.; Casper, M.; Loustalot, F.; Wright, J.S. County-Level Trends in Hypertension-Related Cardiovascular Disease Mortality-United States, 2000 to 2019. J Am Heart Assoc. 2022, 11, e024785. [Google Scholar] [CrossRef]
- Polsce, W.P.T.N. Rules for the management of hypertension. Arterial Hypertension 2008, 12, 317–342. [Google Scholar]
- O'Brien, M.W.; Petterson, J.L.; Kimmerly, D.S. An open-source program to analyze spontaneous sympathetic neurohemodynamic transduction. J. Neurophysiol. 2021, 125, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
Figure 1.
Angiotensinogen metabolism under the influence of ACE and ACE-2 together with the effects of end products.
Figure 1.
Angiotensinogen metabolism under the influence of ACE and ACE-2 together with the effects of end products.
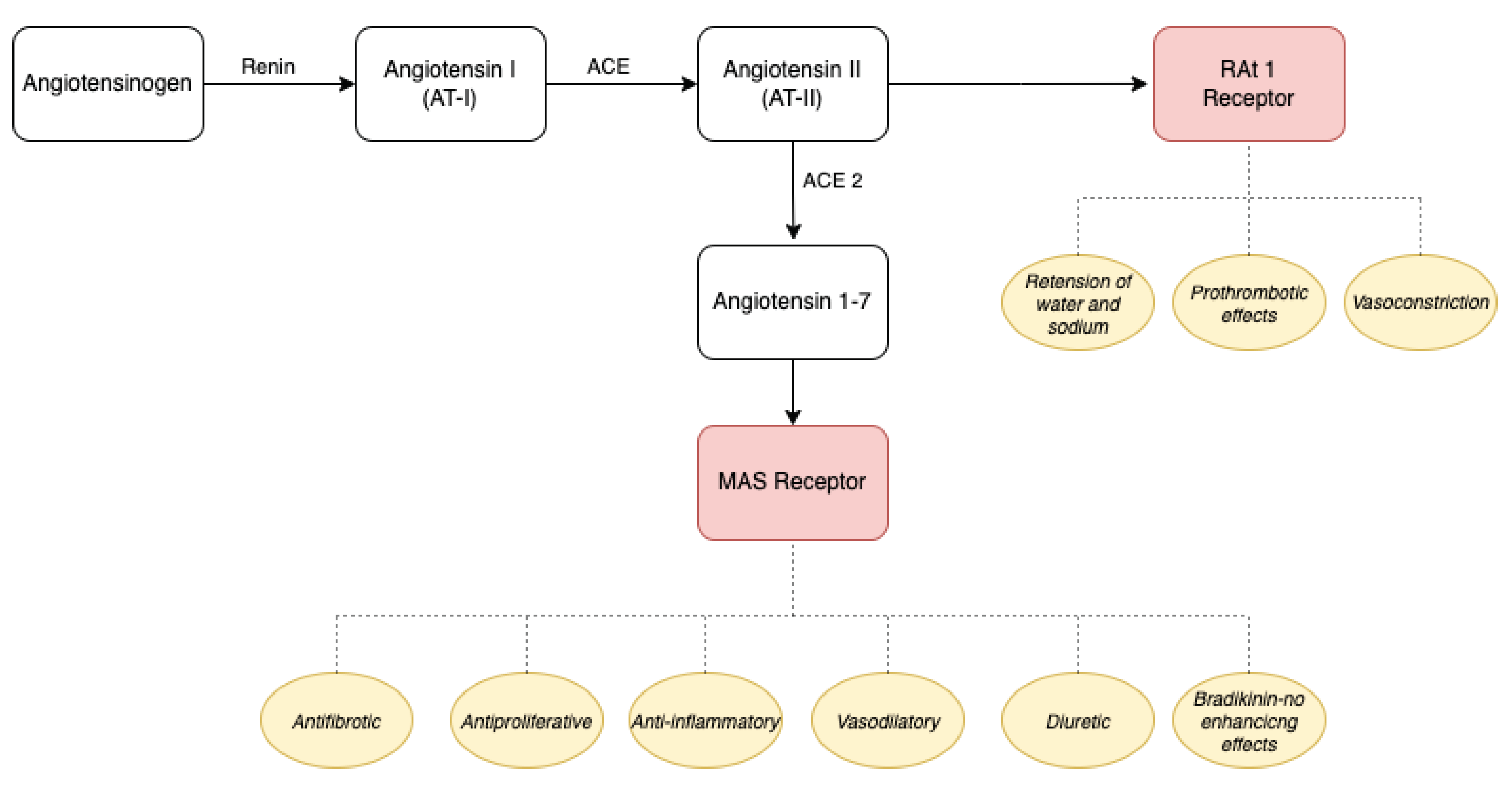
Figure 2.
Possible impact of SARS-CoV-2 infection on the hypertension developing.


Table 1.
Characteristic of all studies included in review.
| Study, (year) | City/country | Sample size | Disease severity | Mean/Median follow-up periods | Mean/median age (years)/male (%) | Result |
|---|---|---|---|---|---|---|
| Xiong et al. (2020) [59] | Wuhan, China | 538 | General, severe and critical | Median (IQR): 97.0 (95.0–102.0) days |
Median (IQR): 52.0 (41.0–62.0 Male 46% | Newly diagnosed hypertension- 7 persons (1,3%) |
| Mei et al. (2021) [60] |
Wuhan, China | 3677 | Mild, severe and critical |
Median (IQR): 144 (135–157) days |
Median (IQR): 59.0 (47–68) Male 46% |
6 individuals developed hypertension |
| Shang et al., (2021) [61] | Wuhan, China | 796 | Severe, critical | 6 months |
Median (IQR): 62.0 (51.0–69.0) Male 51% |
3(0,4%) cases of newly diagnosed hypertension |
| Boglione et al., (2021) [62] | Italy | 449 | Hospitalized |
Median (IQR): 178.5 (165.5 – 211.5) days |
Median (IQR): 65.0 (56.0–75.5) Male 78% |
116 individuals reported hypertension on their first visit (25.8%), and it persisted in 61 (14%) individuals after 180 days from hospital discharge. |
| Sevgi Özcan et al. (2022) [63] | Turkey | 406 | Hospitalized | 3 and 6 months |
Age (years) WHO 3: 46.8 ± 13.3 WHO 4: 52.8 ± 13.1 WHO 5,6: 54.8 ± 11.8 Male n (%) WHO 3: 35 (42) WHO 4: 163 (56) WHO 5,6: 19 (60) |
Hypertension on 4 patients. Level risk risk: 1.229 0,784-2,019 |
| Mohammed Ali Gameil et al. (2021) [64] |
Egypt | 240 | From mild to moderate |
3-4 months: 58(48,3) 4-5 months: 37(30,8) 5-6 months: 15(12,5) > 6 months: 10(8.3) |
Mean age at 38.29 male 55.6% | Systolic blood pressure was significantly elevated (P=0.001) Control cases 120,63±8,49 vs research group 126,70±10,31 |
| Koen M vas der. Sluijs et al. (2022) [65] | Netherlands | 202 | mild | After 175 days [126-235] | Mean age at 59 and male 58% | There was no difference in blood pressure or pulse stiffness |
| Suzana E. Tanni et al. (2022) [66] |
Brazil | 100 | No data | After 99 days | Mean age at 46,3. Mostly female |
Systolic and diastolic blood pressure, heart rate and body weight were slightly but significantly increased compared to baseline. |
| Assim A. Alfadda et al. (2022) [67] | Saudi Arabia | 98 | Hospitalized | After 7,02 ± 1,6 months. | Mean age at 48.87 (±17.11) Male 51% (50) |
Higher mean blood pressure was found in the follow up 131.26 ± 15.3 |
| Sarah E. Daugherty et al. (2021) [68] | USA | 266586 | 8.2% hospitalized 1.1% admitted to the intensive care unit | median 87 days (45-124 days) |
Mean age (SD) 42.4 Małe 50,2 % |
Hypertensions ( risk ratio 1.81 (95% confidence interval from 1.10 to 2.96) |
| Zainab Mahmoud et al. (2022) [69] | USA, Washington | 100 | 23% of hospitalized patients and 5% OIT. | Median time 99 days. | Mean age at 46.3 Male 19% | There was a significant increase in median systolic (128 vs. 121.5 mmHg, p = 0.029) and median diastolic (83.5 vs. 76 mmHg, p < 0.001) blood pressure A total of 52 patients had an increase in systolic or diastolic blood pressure of 10 mmHg or more from baseline |
| Nina L. Stute et al. (2022) [70] | USA | 10 | Mild | Mean 41 ± 17, 108 ± 21 and 173 ± 16 days |
20,5 ± 1,2 years Małe 70% |
Resting and reactive BP, but not HR. Decrease during recovery. |
| Rachel E. Szeghy et al (2021) [71] | USA | 30 | Mild | Mean 3-4 weeks. |
Mean age 20 ± 1 years Małe 36,7 % |
Mean systolic and diastolic pressures were greater in the SARS-CoV-2 group compared with the control group. |
| Stephen M. Ratchford et al (2020) [72] | USA, North Carolina | 31 | Mild | 24 ± 6 days | Mean age 20,2 ± 1,1 Małe 29% |
Average systolic pressure: Control: 111,8 ± 13,4 vs SARS-CoV-2: 121,3 ± 12,3 |
| Mahmut Akpek et al. (2021) [73] | Turkey | 153 | 5% hospitalized Mild |
Mean 31.6 ± 5.0 days. |
Mean age 46.5 ± 12.7. Małe 34% |
New onset hypertension was observed in 18 patients at the end of 31.6 ± 5.0 days on average (P <.001). |
| Damsara Nandadewa et al. (2022) [74] | USA, Texas | 38 | Mild | Mean 11 ± 6 weeks |
Control: 23 ±3 yr COVID: 24,5 ±4yr Male 100% |
Taken together, these data suggest that the adverse effects of COVID-19 on BP in young adults are minimal and likely transient. |
| Ternushchak, Tetiana M. Et al (2022) [75] | Ukraine | 115 | mild,moderate | Mean 1.68 ± 1.2 months | Mean age 23.07 ± 1,54. | Patients with long-COVID syndrome have higher mean ABPM diurnal BP values especially at night, significant BP BP variability. |
| Djidji Delalic et al. (2022) [76] | Croatia, Zagreb | 199 | No data | Median 1 months | Mean age 57.3yr Male 46% |
32 (16,08%) of 199 patients studied had either newly verified (15) or worsened existing (17) hypertension. |
| Rebeka DeLorenzo et al. (2020) [77] | Italy, Milan | 185 | Mild, moderate, serve | Median time from hospital discharge 23 days | Mean age 57 male 66,5% |
40 (21,6%) patients had uncontrolled BP requiring therapeutic change. |
| Tisler A et al. (2022) [78] | Estonia | 3949 | 0 - 66,8 % Mild - 28,9 % Moderate - 3.8% Severe - 0,5 % |
Mean 294.9 | Mean age 65.4 Male 45,7% |
Risk of developing HT 2.85 |
| Steinmetz, A. (2023) [79] | Germany | 158 | mild | Median time from covid-19 infection 203 days |
Mean age 48.1 Male 21.4 % |
blood pressure (RR) was normal and decreased over time |
| Oluwabunmi Ogungbe et al.[80] | No data | 442 | mild, only 12% was hospitalized | Median time 12.4 (10.0–15.2) months. | Mean age 45.4 Male 29% |
20% of patients had newly diagnosed hypertension |
| Zhang HG et al (2022)[81] | Germany, France, Italy, Singapore, USA |
414,602 | hospitalized SARS-CoV-2 infection and not | Observation last 1 year | Mean age: no data Male 74% |
Increased risk of arterial hypertension after COVID-19 infection, and it was more significant among ambulatory patients |
| Cohen K et al (2022) [82] | USA | 2 895 943 |
In most cases- hospitalized | Median days78 (30-175) | Mean age 75,7: Male 42% |
HT was determined at a level of 4.43 (2.27 to 6.37) |
| Al-Aly Z et al (2022) [83] | USA | 5.017.43(cases:33 940) | mild, moderate, serve | Follow up-length: 6 months | Mean age: 64,9 Male:89,9% |
The hazard ratio for hypertension was estimated at 1.62. |
| Mizrahi B et al. (2023) [84] |
Israel | 1 913 234 (cases:320 857) | mild | Two time periods after infection Early (30-180 days) Late (180-360 days) |
Median age: 25 years old Male 49,4 % |
Patients with mild COVID-19 were at risk for a hypertension burden of 1.27, and that these effects were resolved within a year from diagnosis. |
| Fernández-Ortega MÁ et al. (2023) [85] |
Mexico | 71 | hospitalized | Two telephone interviews: First after 5 months of discharge, and second at 12 months. |
Age >18 years old Male 65,7% |
Arterial hypertension was one of the observed sequelae. |
| Jennifer K et al. (2022) [86] |
Israel | over 90,000 COVID-19 cases and matched comparison controls | no data | Follow up-length: 14 months | The patients were divided by age into those below and above 40 years old. | Didn’t find differences in the occurrence of hypertension in the control group and after recovering from COVID-19. |
| Pooja Vyas A et al. (2023) [87] |
India | 248 | Hospitalized | Follow up-length: 1 year | Age: 51,16 ± 12,71 Male: 68,1% |
32.3% of individuals experienced new-onset HT |
| Abumayyaleh M et al. (2023) [88] |
International | 8,719 | severe | Follow-up time (months (PCS)) diabeties 2.6 ± 4.6 nondiabeties 2.8 ± 4.9 |
Age: 72.6 +- 12.7 Male: 63.5 |
The incidence of newly diagnosed hypertension slightly lower in DM patients as compared to non-DM patients (0.5% vs. 1.6%; p = 0.18) |
| González-Hermosillo G JA et al. (2023) [89] | Mexico | 45 | hospitalized | 10.8 ±1.9 months from discharge | Age 49.7 ±9.6 Male 50% |
8 (34 %) had abnormal blood pressure response to orthostasis |
| Adam Saloň et al. (2023) [90] | Austria | 35 | hospitalized | Measurements were taken either on day 0 or on day 10 and the second measurement occurred 2 months after hospitalization. | Age 60 ± 10 Male 85% |
Significant changes in systolic blood pressure were observed, ranging from 142 mmHg (SD: 15) to 150 mmHg (SD: 19, p = 0.041). |
| Damsara Nandadeva et al. (2023) [91] | USA, Texas | 23 | no data | Median 15 months (3–30) |
Age group after COVID and control 48 ± 9 vs. 50 ± 13 yr; male 0% |
BPs were elevated in patients with PASC compared with controls |
| Ziyad Al-Aly et al (2021) [92] | USA | 5 808 018 | mild- non hospitalized | Median 126 (81–203) | Mean age 59.09 (15.92) Male 87.96% |
There was an excess burden of hypertension (15.18 (11.53–18.62)) |
| Nishant P. Shah et al (2022) [93] |
USA | 72 706 | no hospitalized | Pandemic months in 2020:April-June vs pre-pandemic January-March 2019 and 2020 |
Pre-COVID-19 vs during COVID-19 mean age 53.0 ± 10.7 years vs 53.3 ± 10.8 male 54% vs 49,4% |
Relative to the pre-pandemic period, during COVID-19 the proportion of participants with a mean monthly BP classified as uncontrolled or severely uncontrolled hypertension |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



