
Submitted:
23 August 2023
Posted:
25 August 2023
You are already at the latest version
Abstract
We aimed to investigate the clinical results following poor-quality embryo transfer and the parameters to foresee the prognosis. In this study, 2123 cycles that had day 3 and day 5 single-fresh embryo with a poor-quality embryo transfers and a good-quality embryo transfers were compared. The cycles according to transfer day were evaluated by conducting a subgroup analysis. The correlation between all the obtained demographic characteristics, controlled ovarian stimulation parameters and cycle results were analysed. Clinical pregnancy was established in 53 patients that underwent transfer in the poor-quality embryo group (14.9%). Of these patients, 36 had live birth (live birth rate per clinical pregnancy 67.9%). In cleavage-stage embryos, live birth rates per clinical pregnancy were higher in poor-quality blastocyst transfer. When analysing the factors affecting live births in poor-quality embryo group, as the total gonadotropin dose increases, the probability of live birth decreases, as in the probability of hCG positivity. In conclusion; although the probability of pregnant is low, when clinical pregnancy is established, there is a high chance of having a live birth after poor-quality embryo transfers. This could be regarded as an acceptable option in cycles when only poor-quality embryos were available.
Keywords:
In vitro fertilization
; gonadotropin dose
; live birth rate
; poor embryo quality
1. Introduction
Embryo quality is a significant determinant of treatment success via assisted reproductive techniques (ART). The majority of the ART treatment protocols have shifted towards single embryo transfer (SET) and focus on the specification and transfer of good quality embryos oriented towards the achievement of live birth. Poor-quality embryos are generally not preferred for transfer or cryopreservation because their implantation potentials are lower than good-quality embryos. Despite insufficient evidence, it is believed that transfer of poor-quality embryos results in spontaneous abortion or pregnancy loss. On the other hand, a correlation was demonstrated between cleavage stage embryo morphological score and chromosomal anomalies. Although the possibility of euploidy is higher in embryos with good morphology during the blastocyst stage, the effect of aneuploidy on embryo quality is unclear [1]. Therefore, an embryo with excellent morphology may carry a genetic anomaly; contrarily, an embryo with poor morphology posing the potential to be euploid is not ruled out [2,3]. Although each of the studies carried out in recent years evaluated this differently, it was observed that pregnancies following poor-quality and good-quality embryo transfers produced similar obstetric and neonatal results and embryo quality was not correlated with increased adverse obstetric and neonatal risks [2,3,4,5,6,7,8].
When considering that poor-quality embryo transfer does not affect perinatal results, this may provide a valuable option to couples in the decision-making process. The aim of this study is to investigate the factors affecting clinical results following poor-quality embryo transfer and the presence of parameters to foresee the prognosis.
2. Materials and Methods
2.1. Study Design
Medical records of all patients undergoing treatment at the Etlik Zübeyde Hanım Training and Research Hospital between September 2007 and September 2021 were examined retrospectively, and fresh single embryo transfer cycles were included in the study. Approval was obtained from Etlik Zübeyde Hanım Training and Research Hospital Ethics Committee (21.04.2022/ 05).
Included in the study were only the cycles that had day 3 and day 5 single fresh embryo transfers; and patients that underwent two or more embryo transfers, frozen/thawed cycles, patients with cancelled cycles (insufficient response, no oocytes retrieved, absence of sperm, fertilization failure, poor embryo development) as well as day 2, day 4, and day 6 embryo transfers were excluded from the study. Demographic characteristics (age, body mass index (BMI), number of cycle , duration of infertility, anti-mullerian hormone (AMH) level, basal follicle stimulating hormone (FSH), estradiol (E2) level, antral follicle count (AFC), indication of treatment, male age, total progressive motile sperm count (TPMSC) and morphology) and controlled ovarian stimulation parameters (stimulation protocol, duration of stimulation, total gonadotropin dose, trigger protocol, E2 level- endometrial thickness- number of developed follicles on the trigger day, number of retrieved total and mature oocyte, and fertilization rates) of patients carrying inclusion criteria were evaluated.
2.2. Ovarian Stimulation, Intracytoplasmic Sperm Injection (ICSI), and Embryo Transfer Procedures
After the evaluation of ovarian reserve markers for each patient, GnRH antagonist, long agonist, or microdose flare-up protocols. Gonadotropin dosages were personalised according to the age of the patient, basal serum FSH level, AFC, BMI and adjusted based on ovarian response. Cycles were followed with serial transvaginal ultrasonographic evaluations and measurements of serum E2 levels. When a minimum of three follicles reached an average of 18mm diameter, human chorionic gonadotropin (hCG) was administered to induce final oocyte maturation. Oocyte pick-up (OPU) procedure was carried out by transvaginal ultrasound about 35.5-36 hours after hCG administration. Mature oocytes were inseminated by ICSI method. Embryo transfer was conducted with transabdominal ultrasonography. All the patients were provided with similar luteal phase support starting from the date of oocyte pick-up.
2.3. Assessment of Embryo Development
Fertilization of oocytes was evaluated 18-20 hours after ICSI upon observing the presence of pronuclei. Day 3 embryos (61-65 hours after ICSI) were rated using an embryo scoring system according to the cell count, size, symmetry, and fragmentation rate. A scoring system was formed for day 5 embryos at the blastocyst stage by considering the blastocyst expansion, inner cell mass, and trophectoderm structure. Scoring was carried out from the best (Grade 1) to the worst (Grade 5) according to this criteria [9]. Grade 1 and Grade 2 embryos were classified as good-quality embryos, and Grade 3 and Grade 4 embryos were deemed poor-quality embryos. Grade 5 embryos were not transferred.
The results obtained from patients designated as the study group that underwent poor-quality embryo transfer were compared with the results of patients that had a good-quality embryo transfer. Additionally, whether a difference was present between cycles that underwent day 3 and day 5 embryo transfer was evaluated by conducting a subgroup analysis. The correlation between all the obtained parameters and cycle results (whether gestation occurred, biochemical pregnancy, clinical pregnancy, miscarriage, or live birth) was analysed. Parameters that may effectively predict successful cycle outcome of day 3 and day 5 poor quality embryo transfers were also evaluated.
2.4. Pregnancy Outcomes
Plasma BhCG value above ≥10 IU/l measured on day 14 of embryo transfer was defined as a positive pregnancy result. Pregnancy loss before the gestational week 22 was called a miscarriage, and the birth of a live baby after the gestational week 22 was specified as live birth.
2.5. Statistical Method
Data were analysed using IBM SPSS V23 software. Conformity to normal distribution was analysed using the Kolmogorov-Smirnov test. According to groups, Pearson’s Chi-square test, Fisher’s Exact test, and Yates’ Correction were utilised for the categorical data comparison. Mann-Whitney U test was used to compare data that do not distribute normally based on two groups. Binary logistic regression analysis was conducted for the affecting factors, and the Backward: Wald method was used to include the independent variables in the multivariate model. Analysis results were presented as mean±standard deviation, median (minimum-maximum), and categorical data as frequency (percentage). The significance level was taken as p<0.050.
3. Results
2,123 IVF cycles that met inclusion and exclusion criteria were included in the study. Good-quality embryos were obtained in 1,768 of these cycles, and poor-quality were received in 355. Flow chart of the study group is shown in Figure 1.
Mean age of the female and male, basal FSH and E2 levels were higher, and total AFC was lower in the poor-quality embryo group than the good-quality embryo group (p<0.001). When treatment indications were evaluated, a statistically significant difference was found in those with advanced maternal age and unexplained infertility diagnosis. Age-related infertility in 3.2% of the good quality embryo group and 7.3% of the poor quality group (p<0.001), unexplained infertility in 31.2% of the good quality group and 25.4% of the poor quality group (p=0.028) was diagnosed.
The total gonadotropin dose used was statistically significantly higher in the cycles with poor embryo transfer group than good quality embryo transfer group (p<0.001). Also, in the group that underwent poor quality embryo transfer, the E2 level on the trigger day, numbers of oocyte retrieved, numbers of mature oocyte, the numbers of oocyte used for ICSI, oocyte quality index, and numbers of 2PN were found significantly lower (p<0.001). A significant difference was not observed in other parameters (p>0.050) (Table 1).
Clinical pregnancies rate was 38.3% of the good-quality group and 14.9% of the poor-quality pregnancy group, and the difference was statistically significant (p<0.001). Similarly, the difference regarding the live birth rates between the groups was found to be statistically significant (30.6% in the good-quality embryo group vs 10.1% in the poor-quality embryo group, p<0.001). Live birth per clinical pregnancy was significantly higher in the good-quality embryo group, and miscarriage per clinical pregnancy was lower (p<0.001). A significant difference was not observed in terms of biochemical pregnancy and miscarriage (p>0.050). Clinical pregnancy was established in 53 patients that underwent transfer in the poor-quality embryo group (14.9%). Of these patients, 36 had live birth (live birth rate per clinical pregnancy 67.9%) (Table 2).
When compared in terms of embryo transfer day it was found that the clinical pregnancy and live birth rates in the 5th day transfer were statistically significantly higher compared to the 3rd day transfer in the good embryo transfer group (46.1% vs 33% and 37.7% vs 26.1%, respectively) (Table 3). A statistically significant difference was not observed between day 3 and day 5 embryo transfer in the group that underwent poor-quality embryo transfer regarding clinical pregnancy and live birth rates (p>0.05). However, live birth per clinical pregnancy was higher in embryos transferred on day 3 compared to embryos transferred on day 5 (75% vs 57.1%, respectively) and that miscarriage per clinical pregnancy was lower (25% vs 42.8%, respectively) (p<0.001) (Table 3).
Factors affecting the hCG positivity in poor-quality embryo groups were examined using binary logistic regression analysis. When analysing the univariate model results, the chance of conception was lower parallel to the increase in total gonadotropin dosage adopted in controlled ovarian hyperstimulation (COH) (OR=0.997; p=0.049). Whereas, in the multivariate model result, the chance of conception increases by 1,416 as the 2PN number rises (p=0.045). Other factors did not have a statistically significant impact on conception (p>0.050). When analysing the factors affecting live births in poor-quality embryo group, as the total gonadotropin dose used in COH increases, the probability of live birth decreases, as in the result of pregnancy (OR=0.995; p=0.024). Other factors, however, were not established to have any statistically significant effect on live birth (p>0.050) (Table 4).
4. Discussion
This study showed that clinical pregnancy and live birth rates and miscarriage rates were higher in the poor-quality embryo transfer group than good-quality embryo transfer group. Half of the patients reached to term and gave birth in poor quality embryo transfer group when clinical pregnancy was achieved. Although clinical pregnancy and live birth rates were significantly higher following day 5 transfers in good-quality embryo transfers, we established that clinical pregnancy rates were similar in day 3 and day 5 transfers of poor-quality embryo transfers but that the chance of live birth was higher in cleavage period embryos compared with blastocyst transfer if clinical pregnancy was accomplished.
Numerous studies in the literature have shown a strong correlation between low clinical pregnancy rates and live birth rates per transfer in morphologically poor-quality embryos [4,5,6,7]. In their study that compared transfer cycles of 488 patients, Kirilova et al. reported that implantation, clinical pregnancy, and live birth rates of poor-quality embryo transfer cycles were lower compared with cycles with good-quality embryo transfer and that the results did not demonstrate any difference based on whether they were day 3 or day 5 transfer [4]. Although Oron G et al. [5] reported that miscarriage and live birth rates were equivalent between poor- and high-quality embryo transfer groups, a study by Zhu J et al. [6] demonstrated that live birth rate per clinical pregnancy was considerably lower in the poor-quality embryo transfer group compared with good-quality embryo transfer group and that miscarriage rate per clinical pregnancy was higher. While the previous study [5] combined both cleavage and blastocyst embryos, the following study [6] evaluated only cleavage embryos and defended that the quality of embryos may affect pregnancy results following the clinical pregnancy during the cleavage stage. Similarly, Akamine et al. [7] combined both groups and found that, in the poor-quality embryo transfer group, the live birth rate per clinical pregnancy was significantly lower, and the miscarriage rate per clinical pregnancy was higher in the good-quality embryo transfer group (69.1% vs 49.1% and 26% vs 40.4%). Li M et al., on the other hand, found that approximately 70% (17/22) of infertile patients resulted in live birth following achieving clinical pregnancy (21.6%, 22/102) after low-grade blastocyst transfer, which is generally not preferred for embryo transfer [8].
This study also established a significant difference in good- quality and poor-quality embryo transfer groups in terms of clinical pregnancy and live birth (38.3% vs 14.9% and 30.6% vs 10.1%). However, of the poor-quality embryo transfer pregnancies reaching the clinical pregnancy stage, 67.9% resulting in live birth stands out as remarkable. When a comparison is conducted based on transfer day as well, it was observed that the clinical pregnancy and live birth rates via blastocyst transfer in good-quality embryo transfers were significantly higher and that a difference was not found based on transfer day between clinical pregnancy and live birth rates following poor-quality embryo transfers.
Numerous studies have shown that blastocyst transfer theoretically achieved a better synchronisation between the embryonic stage and endometrial receptivity, was more physiological, and accomplished undeniable success rates, specifically in the population with good prognoses [10,11,12,13]. It was explicitly proven in the cleavage stage that the embryo culture strategy was distinctively effective when numerous good-quality embryos were present [12,13]. However, although sufficient data is non-existent, embryo quality during the cleavage stage may not seem to affect clinical results following good-quality blastocyst transfer [10,12]. We established in the literature that the value of foresight was limited on blastocyst formation following day 3 embryo morphology and that only 51% of embryos pre-selected for transfer on day 3 and only 21% of poor-quality embryos achieved blastocysts on day 5 [14]. Another study claimed that grade 3 and 4 embryos had similar rates for progressing to blast but could not foresee blastocyst quality forming [15]. A recent review suggested the view that poor-quality blastocyst transfer should be focused on rather than a poor-quality day 3 embryo and that transfer can be carried out during the cleavage stage only when a single poor-quality embryo is present [16]. In our study, we did not establish a difference between clinical pregnancy and live birth rates based on transfer day following the poor-quality embryo transfer either. However, in cleavage-stage embryos, live birth rates per clinical pregnancy were higher in poor-quality blastocyst transfer (75% vs 57.1%). These results give rise to the thought that the success rate would be higher for the patient to have cleavage-stage transfer instead of waiting till day 5 for patients with poor-quality embryos on day 3 and that this would be a more appropriate approach.
In ART, obtaining as many transferable embryos as possible is critical to having an increased clinical pregnancy rate. And the grounds for attaining transferable embryos is to obtain many normal fertilized oocytes. In this study, when analysing the demographic and COH parameters of the group that received poor-quality embryos, what stands out is that they were of more advanced age compared with the other group, their basal FSH values were higher, AFC levels were lower, and also during COH, these patients had fewer oocytes while receiving more gonadotropin. All these factors demonstrate that the total gonadotropin dose used during COH significantly affected live birth as much as pregnancy outcome.
Numerous publications demonstrated that increased numbers of oocyte retrieved improves the live birth rate [17,18,19], and when the effect of obtained numbers of oocyte is analysed, COH may be accepted as a key success factor. A previous study in the literature showed that the higher the Ovarian Sensitivity Index (OSI; the ratio between gonadotropin dosage and numbers of oocyte retrieved), the higher the pregnancy rates. It also suggested that healthy ovaries that respond well to low-dose gonadotropins provide better oocyte quality and fertilization [20].
However, it was suggested that excessive ovarian stimulation has a detrimental effect on oocyte and embryo quality and that this causes embryos with higher aneuploidy rates. Its effects on oocyte and embryo quality were specifically well-characterised in animal models, and it was shown that the aggressive stimulation caused a weaker embryo development potential and that it may increase chromosomal anomaly rates and embryo development is negatively impacted in a dose-dependent manner [21,22,23,24,25,26,27,28]. Results of a dose-response study conducted on cattle showed that FSH doses exceeding maximum response caused a reduction in ovarian follicle count per OPU, E2 production, number of collected oocytes, and number of fertilised oocytes [22,23,24,25] resulted in the rise of degenerated embryo count [22], and that it increased aneuploidy compared with mild protocols in rats as well [26]. In addition, it was demonstrated that high dosage caused luteinisation in FSH granulosa cells and that it deteriorated blastocyst development independently of luteinisation [27,28]. As for humans, it was suggested that the euploid oocyte rate was directly proportional to the number of mature oocytes and inversely proportional to the number of gonadotropin unit used per mature oocyte obtained [29,30]. Studies conducted with preimplantation genetic screening (PGS) showed that high ovarian response to conventional ovarian stimulation did not raise embryo aneuploidy rates [31,32].
Majority of studies conducted on humans designed to evaluate the effect of gonadotropins on oocyte quality compared distinct gonadotropin doses. When mild and conventional stimulation were compared, a higher rate of good morphological quality embryos was observed in mild protocols [33,34]. Baker et al. analysed the correlation between total gonadotropin dosage and live birth in a quite vast patient series (more than 650,000) that received fresh cycle and observed that gonadotropin dosage as a factor independent of the number of collected oocytes demonstrated a negative correlation with the chance of live birth. They established a 20% decrease in live birth between cycles that received higher doses and those with lower doses [35]. Additionally, the effects of supraphysiological E2 levels or P secretion during high-dose gonadotropin stimulation on endometrium should not be overlooked [36,37]. In this study, too, that supports the results noted above, the rise in total gonadotropin dosage was demonstrated to be a parameter negatively impacting pregnancy and live birth rates.
5. Conclusions
Consequently, considering that the obstetric and neonatal outcomes of pregnancies occurring after poor-quality embryo transfers are like good-quality embryos, it could be regarded as an acceptable option in cycles when only poor-quality embryos were available. Patients should be clearly informed, although the probability of pregnant is low, when clinical pregnancy is established, there is a high chance of reaching term and having a live birth.
Author Contributions
Conceived and designed the study: NK, İK, İK. Analyzed the data: NK, İK. Wrote the manuscript: NK, İK. Final edit of paper: NK, İK, SD, YEU. All authors of this paper have read and approved the final version.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures were performed in accordance with the ethical standards of the Declaration of Helsinki and National Research Committee. Approval was obtained from Etlik Zübeyde Hanım Training and Research Hospital Ethics Committee ( protocol number: 21.04.2022/ 05 ).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Data can be made accessible upon demand.
Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
IVF: In Vitro Fertilization; ART: Assisted Reproductive Techniques; SET: Single Embryo Transfer; FSH: Follicle Stimulating Hormone; E2: Estradiol; AFC: Antral Follicle Count; ICSI: Intracytoplasmic Sperm Injection; 2PN: 2Pronuclear; hCG: Human Chorionic Gonadotropin; COH: Controlled Ovarian Hyperstimulation; OSI: Ovarian Sensitivity Index; OPU: Oocyte pick-up; PGS: Preimplantation Genetic Screening; BMI: Body Mass Index; AMH: Anti-Mullerian Hormone; TPMSC: Total Progressive Motile Sperm Count; GnRH: Gonadotropin-Releasing Hormone.
References
- Fragouli, E.; Alfarawati, S.; Spath, K.; Wells, D. Morphological and cytogenetic assessment of cleavage and blastocyst stage embryos. Mol Hum Reprod. 2014, 20, 117–26. [Google Scholar] [CrossRef] [PubMed]
- Hardarson, T.; Caisander, G.; Sjögren, A.; Hanson, C.; Hamberger, L.; Lundin, K. A morphological and chromosomal study of blastocysts developing from morphologically suboptimal human pre-embryos compared with control blastocysts. Hum Reprod. 2003, 18, 399–407. [Google Scholar] [CrossRef]
- Alfarawati, S.; Fragouli, E.; Colls, P.; Stevens, J.; Gutieérrez-Mateo, C.; Schoolcraft, W.B. , et al. The relationship between blastocyst morphology, chromosomal abnormality, and embryo gender. Fertil Steril. 2011, 95, 520–4. [Google Scholar] [CrossRef] [PubMed]
- Kirillova, A. , et al. Should we transfer poor quality embryos? Fertil Res Pract. 2020, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Oron, G.; Son, W.Y.; Buckett, W.; Tulandi, T.; Holzer, H. The association between embryo quality and perinatal outcome of singletons born after single embryo transfers: a pilot study. Hum Reprod. 2014, 29, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Lian, Y.; Li, M.; Chen, L.; Liu, P.; Qiao, J. Does IVF cleavage stage embryo quality affect pregnancy complications and neonatal outcomes in singleton gestations after double embryo transfers? J Assist Reprod Genet. 2014, 31, 1635–1641. [Google Scholar] [CrossRef]
- Akamine, K.; Mekaru, K.; Gibo, K.; Nagata, C.; Oishi, S.; Miyagi, M.; Heshiki, C.; Kinjo, T.; Masamoto, H.; Aoki, Y. Comparative study of obstetric and neonatal outcomes of live births between poor- and good-quality embryo transfers. Reprod Med Biol. 2018, 17, 188–194. [Google Scholar] [CrossRef]
- Li, M.; Yin, M.; Wu, L.; Yan, Z.; Lyu, Q.; Yan, Z.; Li, B. Pregnancy and neonatal outcomes of morphologically grade CC blastocysts: are they of clinical value? Arch Gynecol Obstet. 2020, 302, 1511–1521. [Google Scholar] [CrossRef]
- Baczkowski, T.; Kurzawa, R.; Głabowski, W. Methods of embryo scoring in in vitro fertilization. Reprod Biol. 2004, 4, 5–22. [Google Scholar]
- Rehman, K.S.; Bukulmez, O.; Langley, M.; Carr, B.R.; Nackley, A.C.; Doody, K.M.; Doody, K.J. Late stages of embryo progression are a much better predictor of clinical pregnancy than early cleavage in intracytoplasmic sperm injection and in vitro fertilization cycles with blastocyst-stage transfer. Fertil. Steril. 2007, 87, 1041–1052. [Google Scholar] [CrossRef]
- Van den Abbeel, E.; Balaban, B.; Ziebe, S.; Lundin, K.; Cuesta, M.J.; Klein, B.M.; Helmgaard, L.; Arce, J.C. Association between blastocyst morphology and outcome of single-blastocyst transfer. Reprod. Biomed. Online 2013, 27, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Glujovsky, D.; Blake, D.; Farquhar, C.; Bardach, A. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Syst. Rev. 2012, 7, CD002118. [Google Scholar]
- Guerif, F.; Lemseffer, M.; Blanchard, M.; Royere, D. Top quality embryos at day 2: a prerequisite for single blastocyst transfer? An observational cohort study in women under 36. J. Assist. Reprod. Genet. 2009, 26, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Rjinders, P.M.; Jansen, C.A.M. The predictive value of day 3 embryo morphology regarding blastocyst formation, pregnancy and implantation rate after day 5 transfer following in vitro fertilization or intracytoplasmic sperm injection. Hum Reprod 1998, 13, 2869–73. [Google Scholar] [CrossRef] [PubMed]
- Balaban, B.; Urman, B.; Alatas, C.; Mercan, R.; Aksoy, S.; Isiklar, A. Blastocyst-stage transfer of poor-quality cleavage-stage embryos results in higher implantation rates. Fertil Steril. 2001, 75, 514–8. [Google Scholar] [CrossRef] [PubMed]
- Kemper, J.M.; Liu, Y.; Afnan, M.; Hammond, E.R.; Morbeck, D.E.; Mol, B.W.J. Should we look for a low-grade threshold for blastocyst transfer? A scoping review. Reprod Biomed Online. 2021, 42, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Sunkara, S.K.; Rittenberg, V.; Raine-Fenning, N.; et al. Association between the number of eggs and live birth in IVF treatment: an analysis of 400 135 treatment cycles. Hum Reprod. 2011, 26, 1768–1774. [Google Scholar] [CrossRef]
- Drakopoulos, P.; Blockeel, C.; Stoop, D.; et al. Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos? Hum Reprod. 2016, 31, 370–376. [Google Scholar] [CrossRef]
- Drakopoulos, P.; Errázuriz, J.; Santos-Ribeiro, S.; Tournaye, H.; Vaiarelli, A.; Pluchino, N.; Blockeel, C.; Polyzos, N.P. Cumulative live birth rates in in-vitro fertilization. Minerva Ginecol. 2019, 71, 207–210. [Google Scholar] [CrossRef]
- Huber, M.; Hadziosmanovic, N.; Berglund, L.; Holte, J. Using the ovarian sensitivity index to define poor, normal, and high response after controlled ovarian hyperstimulation in the long gonadotropin-releasing hormoneagonist protocol: suggestions for a new principle to solve an old problem. Fertil Steril 2013, 100, 1270–6. [Google Scholar] [CrossRef]
- Lee, S.T.; Kim, T.M.; Cho, M.Y.; Moon, S.Y.; Han, J.Y.; Lim, J.M. Development of a hamster superovulation program and adverse effects of gonadotropins on microfilament formation during oocyte development. Fertil Steril 2005, 83 (Suppl. 1), 1264–74. [Google Scholar] [CrossRef]
- Wilson, J.M.; Jones, A.L.; Moore, K.; Looney, C.R.; Bondioli, K.R. Superovulation of cattle with a recombinant-DNA bovine follicle stimulating hormone. Anim Reprod Sci 1993, 33, 71–82. [Google Scholar] [CrossRef]
- Mapletoft, R.J.; Steward, K.B.; Adams, G.P. Recent advances in the superovulation in cattle. Reprod Nutr Dev 2003, 42, 601–11. [Google Scholar] [CrossRef]
- Barati, F.; Niasari-Naslaji, A.; Bolourchi, M.; Sarhaddi, F.; Razavi, K.; Naghzali, E.; et al. Superovulatory response of Sistani cattle to three different doses of FSH during winter and summer. Theriogenology 2006, 66, 1149–55. [Google Scholar] [CrossRef]
- Souza, A.H.; Sartori, R.; Guenther, J.N.; Caraviello, D.; Monson, R.; Wiltbank, M. Effect of semen source and dose of FSH on superovulatory response and embryo production in Holstein heifers. Anim Reprod 2007, 4, 70–6. [Google Scholar]
- Roberts, R.; Iatropoulou, A.; Ciantar, D.; Stark, J.; Becker, D.L.; Franks, S.; et al. Follicle- stimulating hormone affects metaphase I chromosome alignment and increases aneuploidy in mouse oocytes matured in vitro. Biol Reprod 2005, 72, 107–18. [Google Scholar] [CrossRef] [PubMed]
- Scheetz, D.; Folger, J.K.; Smith, G.W.; Ireland, J.J. Granulosa cells are refractory to FSH action in individuals with a low antral follicle count. Reprod Fertil Dev 2012, 24, 327–36. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.D. Models of luteinization. Biol Reprod 2000, 63, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Haaf, T.; Hahn, A.; Lambrecht, A.; Grossmann, B.; Schwaab, E.; Khanaga, O.; et al. A high oocyte yield for intracytoplasmic sperm injection treatment is associated with an increased chromosome error rate. Fertil Steril 2009, 91, 733–8. [Google Scholar] [CrossRef]
- Gianaroli, L.; Magli, M.C.; Cavallini, G.; Crippa, A.; Capoti, A.; Resta, S.; et al. Predicting aneuploidy in human oocytes: key factors which affect the meiotic process. Hum Reprod 2010, 25, 2374–86. [Google Scholar] [CrossRef]
- Ata, B.; Kaplan, B.; Danzer, H.; Glassner, M.; Opsahl, M.; Tan, S.L. , et al. Array CGH analysis shows that aneuploidy is not related to the number of embryos generated. Reprod Biomed Online 2012, 24, 614–20. [Google Scholar] [CrossRef]
- Labarta, E.; Bosch, E.; Mercader, A.; Alam_a, P.; Mateu, E.; Pellicer, A. Relationship between ovarian response and number of euploid embryos in oocyte donor cycles. Fertil Steril 2012, 98, S282. [Google Scholar] [CrossRef]
- Hohmann, F.P.; Macklon, N.S.; Fauser, B.C. A randomized comparison of two ovarian stimulation protocols with gonadotropin-releasing hormone (GnRH) antagonist cotreatment for in vitro fertilization commencing recombinant follicle-stimulating hormone on cycle day 2 or 5 with the standard long GnRH agonist protocol. J Clin Endocrinol Metab 2003, 88, 166–73. [Google Scholar] [PubMed]
- Baart, E.B.; Martini, E.; Eijkemans, M.J.; Van Opstal, D.; Beckers, N.G.; Verhoeff, A.; et al. Milder ovarian stimulation for in-vitro fertilization reduces aneuploidy in the human preimplantation embryo: a randomized controlled trial. Hum Reprod 2007, 22, 980–8. [Google Scholar] [CrossRef] [PubMed]
- Baker, V.L.; Brown, M.B.; Luke, B.; Smith, G.W.; Ireland, J.J. Gonadotropin dose is negatively correlated with live birth rate: analysis of more than 650,000 assisted reproductive technology cycles. Fertil Steril. 2015, 104, 1145–52. [Google Scholar] [CrossRef]
- Horcajadas, J.A.; Minguez, P.; Dopazo, J.; Esteban, F.J.; Dominguez, F.; Giudice, L.C.; et al. Controlled ovarian stimulation induces a functional genomic delay of the endometrium with potential clinical implications. J Clin Endocrinol Metab 2008, 93, 4500–10. [Google Scholar] [CrossRef]
- Andersen, C.Y.; Ezcurra, D. Human steroidogenesis: implications for controlled ovarian stimulation with exogenous gonadotropins. Reprod Biol Endocrinol 2014, 12, 128. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study group.
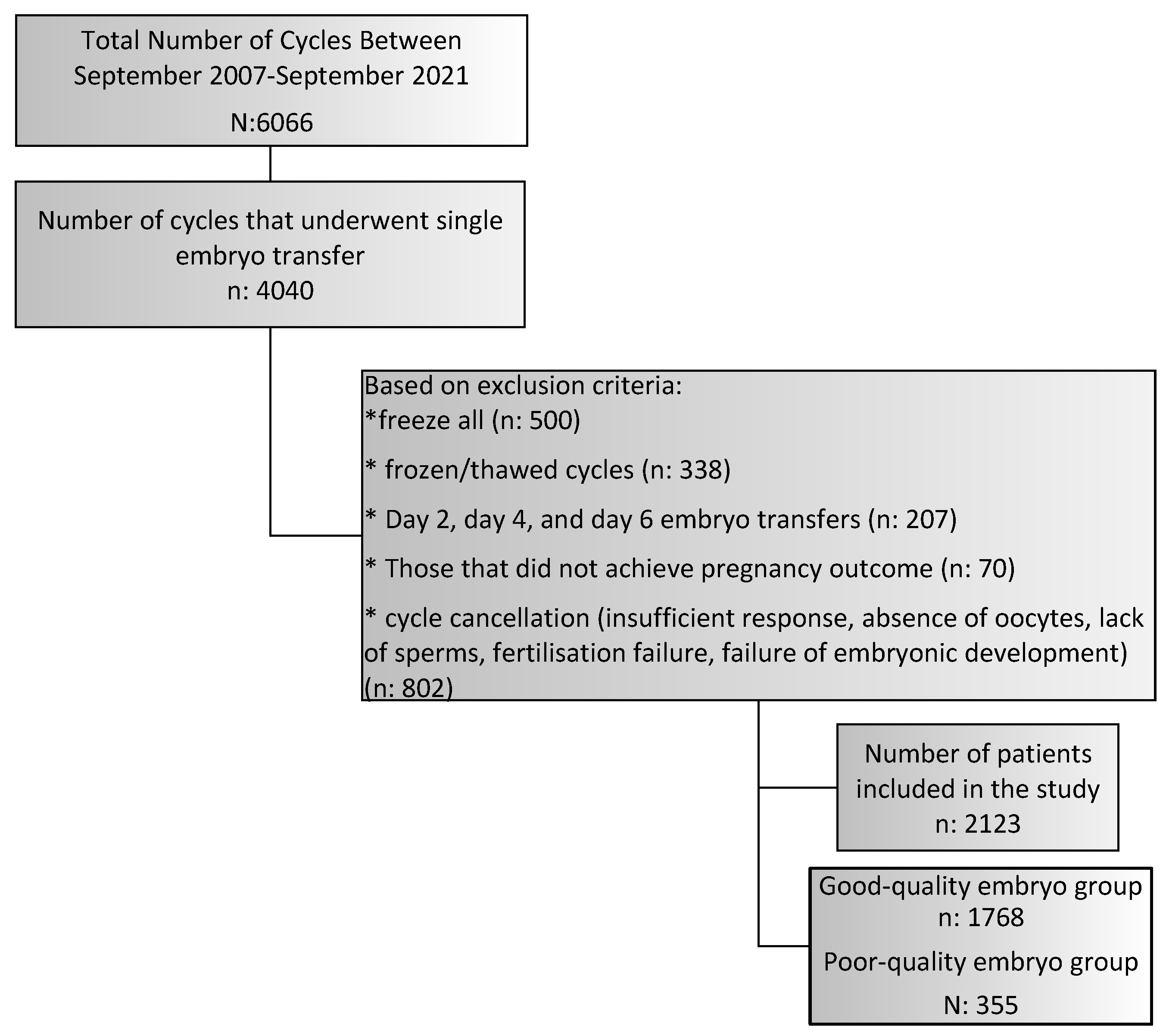

Table 1.
Patient characteristics and clinical parameters of the cycles according to the quality.
| Good Quality n: 1,768 |
Poor Quality n: 355 |
P value | ||
| Female age (years) | 29.4±4.5 | 31.0±5.3 | <0.001* | |
| Body mass index (kg/m2) | 26.2±5.0 | 26.1±5.1 | 0.703* | |
| Number of cycles | 1.5±0.8 | 1.7±1.0 | <0.001* | |
| Basal D3 FSH (IU/L) | 8.2±21.2 | 8.8±6.1 | <0.001* | |
| Basal D3 E2 (pg/mL) | 48.1±32.4 | 50.6±34.6 | 0.021* | |
| AMH (ng/mL) | 3.0±3.5 | 2.7±3.0 | 0.376* | |
| Duration of infertility (months) | 62.1±43.4 | 63.5±46.9 | 0.906* | |
| Numbers of total antral follicle | 14.0±8.4 | 12.4±8.2 | <0.001* | |
| Male age (years) | 32.7±4.9 | 34.5±7.3 | <0.001* | |
| Total progressive motile sperm count (n) | 22,133.4±41,165.3 | 24,006.2±48,095.5 | 0.336* | |
| Sperm morphology: normal rate (%) | 8.2±4.3 | 6.7±7.5 | 0.806* | |
| Indication of treatment (%) | ||||
| Male factor | 733 (41.5) | 140 (39.4) | 0.480** | |
| Tubal factor | 127 (7.2) | 19 (5.4) | 0.259*** | |
| Diminished ovarian reserve | 243 (29.3) | 71 (35.9) | 0.072** | |
| Advanced female age | 56 (3.2) | 26 (7.3) | <0.001*** | |
| Hormonoovulatory dysfunction | 313 (17.7) | 57 (16.1) | 0.455** | |
| Unexplained infertility | 552 (31.2) | 90 (25.4) | 0.028** | |
| Severe pelvic adhesion | 11 (0.6) | 2 (0.6) | 1,000† | |
| Endometriosis | 102 (5.8) | 23 (6.5) | 0.604** | |
| Gnrh protocol (%) | ||||
| Microdose flare-up | 99 (5.6) | 16 (4.5) | 0.462** | |
| Antagonist | 984 (55.7) | 209 (58.9) | ||
| Long luteal | 685 (38.7) | 130 (36.6) | ||
| Duration of ovarian stimulation (n) | 9.9±1.7 | 10.0±1.8 | 0.441* | |
| Total gonadotropin dose (IU) | 2,187.1±897.0 | 2,414.8±1,038.2 | <0.001* | |
| Trigger (%) | ||||
| Hcg | 1,585 (89.6) | 322 (90.7) | 0.549** | |
| Agonist | 183 (10.4) | 33 (9.3) | ||
| Trigger Day | E2 level (pg/mL) | 2,433.7±1,629.4 | 2,197.3±1,470.2 | 0.027* |
| >=17mm follicle (n) | 3.3±2.6 | 3.3±2.6 | 0.671* | |
| 15-17mm follicle (n) | 3.8±3.1 | 3.3±2.7 | 0.001* | |
| 10-14mm follicle (n) | 6.0±4.8 | 4.9±4.2 | <0.001* | |
| Endometrial thickness (mm) | 10.1±2.0 | 9.8±2.1 | 0.072* | |
| Number of oocytes retrieved | 11.9±7.3 | 10.3±6.7 | <0.001* | |
| Number of mature oocytes | 8.9±5.6 | 7.6±5.3 | <0.001* | |
| Number of oocytes used for ICSI | 9.4±5.7 | 8.2±5.5 | <0.001* | |
| Oocyte quality index | 5.1±0.8 | 5.0±0.8 | 0.001* | |
| Numbers of 2PN | 4.8±3.6 | 3.6±2.7 | <0.001* | |
| Blastocyst transfer (n) | 0.33±0.48 | 0.33±0.49 | 0.980* | |
| Embryo transfer Day (%) | ||||
| Day 3 embryo transfers | 1,055 (59.7) | 221 (62.3) | 0.365** | |
| Day 5 embryo transfers | 713 (40.3) | 134 (37.7) | ||
*Mann-Whitney U test **Chi-square test, ***Yates’ Correction, †Fisher’s Exact test.
Table 2.
Clinical outcomes of poor and good/fair quality embryos.
| Good Quality n: 1,768 |
Poor Quality n: 355 |
P value | |
| No pregnancy | 992 (56.1) | 283 (79.7) | <0.001 |
| Biochemical pregnancy | 99 (5.6) | 19 (5.4) | NS |
| Clinical pregnancy | 677 (38.3) | 53 (14.9) | <0.001 |
| Miscarriage | 136 (7.7) | 17 (4.8) | NS |
| Live birth | 541 (30.6) | 36 (10.1) | <0.001 |
| Live Birth per Clinical Pregnancy | 541/677 (79.9) | 36/53 (67.9) | <0.001 |
| Miscarriage per Clinical Pregnancy | 136/677 (20) | 17/53 (32) | <0.001 |
*Chi-square test, NS: not statistically significant.
Table 3.
Clinical outcomes of the poor and good/fair quality embryo transfers in patients on day 3 or day 5 embryo transfers.
Table 3.
Clinical outcomes of the poor and good/fair quality embryo transfers in patients on day 3 or day 5 embryo transfers.
| Day 3 Transfers (n: 1,376) |
Day 5 Transfers (n: 847) |
P value | ||
| Good quality | No pregnancy | 655 (62.1) | 337 (47.3) | <0.001* |
| Biochemical pregnancy | 52 (4.9) | 47 (6.6) | NS* | |
| Clinical pregnancy | 348 (33) | 329 (46.1) | <0.001* | |
| Miscarriage | 73 (6.9) | 63 (8.8) | NS* | |
| Live birth | 275 (26.1) | 266 (37.3) | <0.001* | |
| Live Birth per Clinical Pregnancy | 275/348 (79) | 266/329 (80.8) | NS* | |
| Miscarriage per Clinical Pregnancy | 73/348 (20.9) | 63/329 (19.1) | NS* | |
| Poor quality | No pregnancy | 180 (81.4) | 103 (76.9) | NS** |
| Biochemical pregnancy | 9 (4.1) | 10 (7.5) | NS** | |
| Clinical pregnancy | 32 (14.5) | 21 (15.7) | NS** | |
| Miscarriage | 8 (3.6) | 9 (6.7) | NS** | |
| Live birth | 24 (10.9) | 12 (9) | NS** | |
| Live Birth per Clinical Pregnancy | 24/32 (75) | 12/21 (57.1) | <0.001** | |
| Miscarriage per Clinical Pregnancy | 8/32 (25) | 9/21 (42.8) | <0.001** | |
*Chi-square test, **Yates’ Correction, NS: not statistically significant.
Table 4.
Analysis of factors affecting the hCG positivity and live birth in poor-quality embryos.
| hCG POSITIVITY | LIVE BIRTH | ||||
| OR (95% CI) | P value | OR (95% CI) | P value | ||
| Indication of treatment (%) | |||||
| Male factor | 0.972 | 0.915 | 1.109 | 0.773 | |
| Tubal factor | 0.447 | 0.289 | 0.478 | 0.479 | |
| Diminished ovarian reserve | 0.871 | 0.690 | 0.96 | 0.920 | |
| Age-related infertility | 0.308 | 0.116 | 3.243 | 0.116 | |
| Hormonoovulatory dysfunction | 0.945 | 0.874 | 0.951 | 0.916 | |
| Unexplained infertility | 0.977 | 0.939 | 0.826 | 0.649 | |
| Severe pelvic adhesion | 3.972 | 0.332 | 0.252 | 0.332 | |
| Endometriosis | 1.099 | 0.857 | 0.835 | 0.813 | |
| Female age (years) | 0.976 | 0.339 | 0.945 | 0.111 | |
| Body Mass Index (kg/m2) | 1.024 | 0.363 | 1.048 | 0.158 | |
| Numbers of cycles | 0.906 | 0.484 | 0.932 | 0.704 | |
| Basal D3 FSH (IU/L) | 0.963 | 0.274 | 0.934 | 0.211 | |
| Basal D3 E2 (pg/mL) | 0.995 | 0.368 | 0.998 | 0.715 | |
| AMH (ng/mL) | 1.001 | 0.988 | 1.073 | 0.321 | |
| Duration of infertility (months) | 1 | 0.904 | 0.997 | 0.497 | |
| Numbers of total antral follicle | 1.015 | 0.352 | 1.022 | 0.280 | |
| Male age (years) | 0.986 | 0.486 | 0.97 | 0.279 | |
| Total progressive motile sperm count | 1 | 0.928 | 1 | 0.663 | |
| Sperm morphology: normal rate | 1.01 | 0.655 | 1.039 | 0.133 | |
| Protocol (Reference: long luteal) | |||||
| Microdose flare-up | 1.112 | 0.655 | 1.835 | 0.440 | |
| GnRH antagonist | 0.955 | 0.646 | 1.012 | 0.966 | |
| Duration of ovarian stimulation | 0.936 | 0.383 | 0.903 | 0.330 | |
| Total gonadotropin dose (IU) | 0.997 | 0.049 | 0.995 | 0.024 | |
| Trigger | 1.064 | 0.889 | 1.676 | 0.321 | |
| Trigger day | E2 level (pg/mL) | 1 | 0.376 | 1 | 0.423 |
| >=17 mm follicle | 1.062 | 0.223 | 0.987 | 0.853 | |
| 15-17mm follicle | 1.012 | 0.809 | 0.936 | 0.351 | |
| 10-14mm follicle | 1.043 | 0.150 | 1.043 | 0.269 | |
| Endometrial thickness (mm) | 1.103 | 0.155 | 1.072 | 0.453 | |
| Numbers of oocyte retrieved | 1.032 | 0.090 | 1.035 | 0.152 | |
| Numbers of mature oocyte | 1.037 | 0.120 | 1.035 | 0.256 | |
| Number of oocytes used for ICSI | 1.036 | 0.122 | 1.032 | 0.295 | |
| Oocyte quality index | 0.905 | 0.537 | 0.995 | 0.980 | |
| Numbers of 2PN | 1.416 | 0.045 | 1.097 | 0.111 | |
| Blastocyst transfer | 1.006 | 0.983 | 0.628 | 0.268 | |
| Transfer Day | 1.149 | 0.299 | 0.899 | 0.565 | |
*Backward: Wald method was used to include the independent variables in the multivariate model.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



