
Submitted:
23 August 2023
Posted:
24 August 2023
You are already at the latest version
Abstract
Background: The popularity of climbing via ferratas (VF) in the European Alps has increased a lot. We have analysed the pattern of injuries from accidents, which have occurred on VF, and First Aid (FA) knowledge from the persons on such alpine routes. The aim was to create specific FA courses for those who climb VF.
Material and Methods: Incidences and FA knowledge of the alpinists were investigated by a questionnaire. Data included details of the individual’s alpine experience, accidents or any kind of medical emergency they have ever experienced. FA knowledge was evaluated by 18 multiple choice questions with 5 answers each. The questionnaire was based on those of previous studies but was slightly adopted for VF. For this data from rescue operations on VF were used. Finally every participant was asked to judge his FA knowledge by a Likert scale (1 to 5).
Results: The collective consisted of 391 participants (28.4% women) with an average age of 41 years. A significant portion did no regular fitness training and in most cases the last FA training was years ago. Nobody had joined a specific FA course for climbers or mountaineers. The most common causes of emergencies were: weather conditions (19%), stumble (18.6%), falls (13.4%), and weariness and deficiency in concentration (13.4%). FA questions most often answered correctly were cardiac emergencies (49.6%), high altitude cerebral edema (HACE) (43.2%), snow blindness (40.9%), injuries of the head (37.1%) and hemorrhagic shock (35.3%). Those most often wrong were injuries of the back (1.0%), injuries of the thorax (2.8%), frostbite (9.0%), acute mountain sickness (AMS) (4.1%) and strategy of rescue (4.1%). VF climbers show significant less FA knowledge than mountaineers in the Western Alps and trekkers.
Conclusions: Data support the need of a specific FA training for VF climbers. Their FA knowledge does not fit with the demands in the mountains while some other knowledge they have is negligible on VFs (e.g. HACE). This is in accordance with earlier studies in “classic” alpine mountaineering and in trekking.
Keywords:
via ferrata
; first aid
; safety management
; first aid training
; climbing
; accidents
Introduction
The popularity of climbing via ferrata (“iron ways”, VF) in the region of the European Alps has increased a lot and so did emergencies and accidents en route [1,2]. Ströhle et al. reported an increase of accidents on VF by more than 60% from 2008 to 2018 [2]. VF are climbing routes where iron ropes, spikes and steps are fixed in the rock which otherwise would be impossible to be climbed by anyone except rock climbers who are fit enough for more or less extreme terrain. The first one was erected at Grossglockner in Austria in 1869, another one at the Marmolada (Italy) in 1903 [2]. In WWI they were established to facilitate the move of soldiers in the Dolomites and actually there are more than 1,000 VF in the European Alps [2]. They are used by a broad spectrum of alpinists, from beginners to experts, from childhood to 80+ years of age, from couch potatoes to athletes [2]. Recent studies showed that the activity is not a “high risk” one since more than half of the victims of emergencies are rescued uninjured and only 3.7% of the cases were fatal [2]. However, the uninjured persons cause significant costs for rescue and may unnessessarily pose rescuers at risk when the conditions (e.g. visibility, weather...) are bad. The uninjured cases were most often found on more difficult climbs (Table 1) where they were blocked because they had obviously overestimated their own capabilities. Most fatal cases were in easy sections (Grade A, 13.2%/B, 4.9%, Table 1) where the climbers obviously had underestimated the potential risk of falls [2].
- b
- Rother’s classification
The code is a combination of “KS” indicating that the difficulty descrive a VF (“Klettersteig”), then a number which indicates the technical difficulty and the a letter (A-E, S) which indicates the alpine environment
| KS1 | Route well traced out, comfortable protection, very easy to climb. Without the protection it could be compared to UIAA grade 1. |
| KS2 | Easy via ferrazta. Without the metal equipment it would be UIAA grade 1 to 2. |
| KS3 | Moderate difficult via ferrata. Some power of the arms necessary. Without the metal equipment it would be UIAA grade 2 to 3. |
| KS4 | Difficult via ferrata with steep rocky terrain, some of it vertical. Exposed route, experience in climbing and trained arms necessary.Without equipment such routes would be UIAA grade 3 to 4. |
| KS5 | Very difficult via ferratas. Vertical rock with few and small footsteps, very exposed. Climbing technique and powerful arms necessary. Without equipment such routes would be UIAA grade 5 to 6. You should know what you are doing here! |
| KS6 | Special grade. More easy rock climbing than via ferrata. No or very few protection, often combined terrain with firn or glaciers. Candidates must be able to climb UIAA grade 2 absolutely confident, also when soloing. |
| A | Easy hill walking up to 2,000m, some short climbs. Recommended for beginners. |
| B | Long hill walking at 2,000 to 2,700m with some short climbing. |
| C | Long hill walking at 2,300 to 2,700m, longer climbs. Adequate mountaineering experience necessary. |
| D | Long alpine tours, sometimes in the high Alps. Longer and more difficult climbing passages. For experienced mountaineers only. Stamina and navigation necessary. |
| E | High alpine tours at or above 3,000m. Sometimes ice axe, crampons and rope necessary. For very experienced mountaineers only. |
| S | Via ferrata for sport climbing. At low altitude, short access or near huts, but technically very challenging. |
- c
- Schall’s categories
| A (easy) |
Terrain | Flat-angle, some passages steep, often rocky terrain, exposed steps possible |
| Protection | Iron ropes, chains, iron clamps and sometimes some ladders; most parts may be climbed without using protection | |
| Prerequisites | Surefoodedness and no fear of heights recommended. Normal stamina (“buero training”) sufficient. | |
| Equipment | Via ferrata equipment recommended. Experienced climbers usually don’t need it here. | |
| B (easy to moderate, some passages energy-sapping) |
Terrain | Steeper rocky terrain, sometimes with small footsteps and with some exposed passages. |
| Protection | Iron ropes, chains, clams, longer ladders (probably vertical); climbing is possible without protection, but expert difficulties of grade 3 UIAA | |
| Prerequisites | As recommended for A, but better stamina necessary, also some power of the arms and legs necessary. | |
| Equipment | Via ferrata equipment recommended. Climb may be done as roped party. | |
| C (most parts difficult, strenuous and energy-sapping) |
Terrain | Steep or very steep terrain, mostly small footsteps, longer and common exposed passages. |
| Protection | Iron ropes, chains, clams, longer and some overhanging ladders; larger distances between fixpoints; in vertical passages sometinmes a steel rope only. Climbing without using the steel equipment possible, but it would be comparable to grade 4 UIAA | |
| Prerequisites | For well trained persons only | |
| Equipment | Via ferrata equipment as listed for B is strictly recommended. Less trained persons or children should be secured by a rope. | |
| D (very difficult, very strenuous and very energy-sapping) |
Terrain | Vertical, often overhanging terrain, often very exposed. |
| Protection | Iron ropes, chains, clams, longer and some overhanging ladders; often large distances between fixpoints; in vertical passages often a steel rope only. | |
| Prerequisites | As recommended for C, but well trained and experienced people only; sufficient power of the arms and hands for long vertical or overhanging passages, some free-climbing up to grade 2 UIAA without protection may occur | |
| Equipment | Via ferrata equipment obligatory; often also experienced mountaineers climb with rope belaying, not recommended for beginners and children. | |
| E (extreme difficult, very strenuous and very energy-sapping) |
Terrain | Vertical or overhanging, long very exposed passages, very small footsteps or fiction climbing. |
| Protection | As for D, but often combined with free climbing | |
| Prerequisites | Much power of hands (fingers), arms and legs necessary; good fitness, flexibility. There are longer passages where the arms have to provide most of the power. | |
| Equipment | Via ferrata equipment obligatory; often also very experienced mountaineers climb with rope belaying, not recommended for beginners and children. | |
| F (extreme difficult, in 2021 there were only 2 such climbs in the Alps) |
Terrain | Often overhanging and verry exposed, very small footsteps and fiction climbing |
| Protection | All devices are located in significant distances, often combination with feee climbing. | |
| Prerequisites | Advanced climbing technique absolute necessary, much power of the hands, fingers, arms, and legs. For well-trained and flexible climbers only. | |
| Equipment | Via ferrata equipment obligatory, toprope belaying recommended where possible. Strictly not recomended for people who are unable to climb grade E without any problem! |
First Aid (FA) in the mountains differs to the FA in urban regions because the conditions in the wilderness and the injury patterns or medical diagnoses differ significantly from those in the cities. The injury patterns also differ significantly between the several disciplines of alpine sports. Therefore, the data obtained in this study must be compared with the results of other disciplines (e.g. “classic” mountaineering, trekking...) to get an idea about the differences and to adopt any FA training specifically to address the respective target group adequately.
An additional factor is that the time necessary for the rescue service to reach the patient is much longer than in urban regions. During this period the victims depend on the FA knowledge of their companions. Because of the rising popularity of VF and the high number of people with limited experience in climbing and mountaineering, the number of accidents increased significantly in the last years and an adequate FA education is necessary.
The goal of the current study was to get detailed information about accidents, medical emergencies, and FA knowledge of the climbers to create specific FA trainings for this target group. The individual’s knowledge was of interest because it wouldn’t make sense to train topics which people do right, whether with or without training.
Material and Methods
A total of 391 questionnaires were completed at the Fiderepass Hut (2070 m, Allgäu Alps, Germany) and the Tuckett Hut (2272 m, Brenta, Dolomite Alps, Italy). At the Fiederepass Hut the participants had completed the “Mindelheimer Klettersteig”, a VF of grade B according to Schall’s system (Table 1). At Tuckett hut they had completed “Bochette Alte” which is grade E according to Schall. The participants were asked to include all incidences they ever had on a VF in the questionnaire, not only those which might have happen at the respective climb of the day. All VF climbers at the huts aged 18+ were included. The age limit was given by the ethical commission (EK 096/09).
The participants were asked for demographic characteristics, overdue injuries and accidents while doing via ferrata. The injuries were classified according to UIAA recommendation [3,4]. The injuries’ location of this recommendation is similar to OSICS [5].
Then 18 questions about first aid in a wilderness region were asked (multiple choice with 5 answers each, resulting in a total of 90 statements per subject, see supplement 1). At the end the participants had to estimate their own first aid knowledge using a Likert scale. The results were related to those of the FA questionnaire. A deviation of +/-25% was rated as “good self-assessment” while more than +/-75% was rated as “poor self-assessment”. Data were analysed descriptively, differences between subgroups were proven by non-parametric tests (Χ2-test and Mann-Whitney-U-test). P<0.05 was defined as significant, P<0.1 was interpreted as tendency.
Results
The collective (N=391) included 111 (28.4%) women und 280 (71.6%) men. The average age was 41 years (18-79; median: 42 years). Details are given in Figure 1. The BMI of 367 participants (93.9%) could be calculated. The average was 23.4 kg/m² (17.6 - 32.0). 23.2% were overweight (BMI 25-30), 1.4% were obese (BMI>30), and 9.8% were underweight (BMI<20).
To get an idea about their physical fitness the probands were asked about the physical requirement of their profession and whether and how often they performed any kind of endurance training. The following answers concerning the profession were given: 35 persons (9%) rated the physical demands as “very hard”, 92 participants (23.5%) as “moderate”, 140 persons (35.8%) as “low” and 124 (31.7%) as “not at all”.
17 persons (4.4%) performed some kind of endurance sport every day, 8 persons (2.1%) six times per week, 22 (5.5%) five times per week, 40 (10%) four times per week, 102 persons (25.9%) three times per week, 72 (18.3%) two times per week, 77 persons once a week (19.5%), and 53 (13.4%) persons did no sports at all. The average experience in mountaineering was 19.5 years (0-52). In average the participants spent 23.2 days per year in the mountains (1-300), of which 3.8 days were on VF (1-50). 147 (37.6%) of the participants were rock or ice climbers. 26 (6.7%) of the probands climbed with and 365 (93.3%) without a mountain guide.
A total of 281 persons (71.9%) had completed a FA training while 110 (28.1%) answered that they never visited such a course. Often the last FA training was long ago: While a few participants had a training less than 3 years ago the longest time between the course and the actual study on VF was more than 50 years. 61/391 (16.2%) participants were paramedics, members of mountain rescue service, or nurses, 15 (4%) were doctors or medical students, and 315 persons (79.8%) had no medical education.
21 persons (5.4%) of the collective suffered from an overuse injury actually or earlier in their sports career. Two other persons had two overuse injuries leading to a total of 25 overuse injuries in the collective. The diagnoses most often reported were as follows: gonalgia, cramps, debility, bursitis, omalgia, overstain and strain. As underlying causes were given: dehydration, insufficient training status, route too long, altitude difference too large, and bad preparation. The following acute emergencies happened most often: sunburn (23.9%), contusion (17.7%), open wounds (13.1%), exhaustion (10.8%). Frostbite and metabolic diseases did not occur. For details see Figure 2. The main location of the injuries was the extremities and the head. The hand was affected most often at the upper extremity (9.7%). At the lower extremity the knee was most effected (20.4%). For details see Figure 3.
The following causes of emergencies were reported most often: weather conditions (19%), stumble (18.6%), falls (13.4%), and weariness and deficiency in concentration (“mental exhaustion”, 13.4%) (Figure 4).
Approximately the half of the probands carried a helmet, gloves and a first-aid kit with them while doing a VF (Figure 5). Only 10.5% of the persons took a bivouac sack with them. 50.5% carried pavement, 19.7% disinfectant, 17.7% a rescue blanked and 2.6% a SamSplint® along (Figure 6).
It is interesting who did the emergency care: 60.1% of the participants did it by themselves. In 21.4% a companion or another mountaineer was acting. 7.8% of the injured persons called the rescue service without any other FA and 10.7% did not have any care at all.
With 391 participants and 90 answers each a total of 35190 statements could be evaluated. 34/90 (37.8%) of the answers were correct in less than 25% of the participants, 20/90 (22.2%) in 25-50%, 25 (27.8%) in 51-75%, and 11 (12.2%) in more than 75%. The questionnaire with the correct answers indicated is available as supplement. For most questions the participants answered one or some of the five possible answers more or less correct. However, completely correct answered topics were limited: 5.6% had no correct answered questions, 14.6% just one, 25.1% two, 22% three, and 14.3% four, respectively. More than four correct answers were found in less than 10% (Figure 7). The best result was obtained by one participant with 9 and one other with 8 correct answers. Both did not have any medical training.
The following FA questions were answered most often correctly (Figure 8): cardiac emergencies (49.6%), high altitude cerebral edema (HACE) (43.2%), snow blindness (40.9%), injuries of the head (37.1%) and hemorrhagic shock (35.3%). The first-aid questions which were answered most often wrong were: injuries of the back (1.0%), injuries of the thorax (2.8%), frostbite (9.0%), acute mountain sickness (AMS) (4.1%) and strategy of rescue (4.1%).
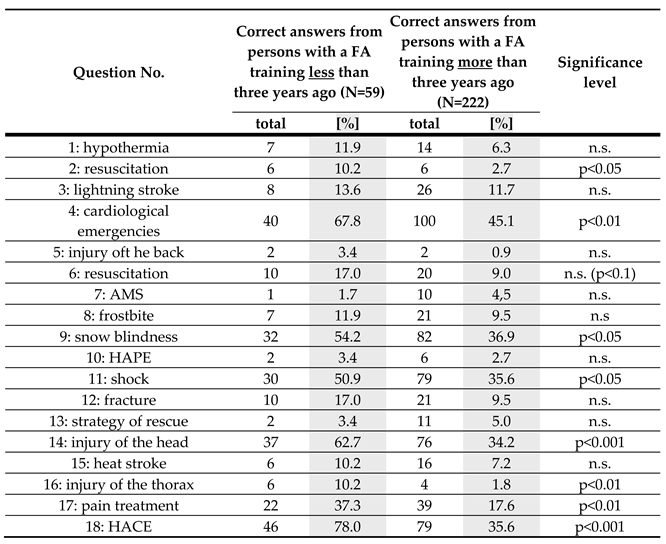
The distance since the last FA training showed variable results. While some topics were answered quite correct although the last training was more than three years ago (e.g. hypothermia, lightning stroke, AMS, HAPE, frostbite, fractures, heat stroke) others showed a marked decrease of knowledge during this period (e.g. resuscitation, cardiological emergencies, injuries of the head or thorax, haemorrhagic shock, pain treatment). Details according to the respective question of the questionnaire are given in Table 2.
The self-assessment “very good” of the FA knowledge is summarized in comparison to the answers in the FA questionnaire in Figure 9. Striking differences between the self-assessment and real performance is obvious for several topics.
By a re-evaluation of earlier studies the actual data were compared with those of other collectives of mountaineers, e.g. in the Western Alps [6] and trekkers in the Himalayas (Annapurna Region [7], Everest Region [8]). This re-evaluation showed that both collectives, the VF climbers and the mountaineers in the Western Alps, do not differ significantly in their low level of FA knowledge (P=0.998, Figure 10). There was also no difference of the total collectives between VF climbers and trekkers (P=0.999, data from [7]; P=0.829, data from [8]) or alpine mountaineers and trekkers (P=0,992, data from [6,7] and 0,836 with data from [6,8], respectively).
Discussion
To our best knowledge the study presented here is the first one which relates the data of injury patterns and medical incidences or emergencies on VF with the FA knowledge and emergency management of the climbers. The German Alpine Club (DAV), the alpine club with the largest number of members worldwide, has the most comprehensive database about the alpine accidents and emergencies ever established. They have published the incidence of any kind of alpine emergency (accidents / injuries and acute diseases) of 1:217,000 hours of VF climbing and fatal outcomes in 1:10,000,000 hours (in [2]). Recalculated with the common standard (cases per 1,000 hours of activity) this would correspond to 0,005 incidences per 1,000 hours of climbing and a fatality rate of 0,001/1,000 hours. All incidence data decrease significantly since years [9]. However, it must be noted that this database does not include those minor cases which were managed by the climbers themselves without the aid of any rescue infrastructure. Therefore the real number of incidences will be higher but, nevertheless, compared to other sports, even school sports, such injury rate is remarkable low [10]. However, taking the long rescue chain into account sufficient FA capabilities are a “must” for safe VF climbing.
In total 111 (28.4%) women and 280 (71.6%) men were included. This is similar to other studies about climbing, i.e. to Ströhle et al. who reported 64.8% male and 35.2% female climbers [2]. In a study of Paige et al., who compared the pattern of injuries of sport climbing and rock climbing, with a collective of 198 probands was the part of the women 20% and of the men 80% [11]. Wyatt et al. also researched the injuries while doing rock climbing. Here 79% were males and 21% females [12]. Bollen did a study about the pattern of injuries while doing rock climbing ang got a similar gender distribution (88% men, 12% women) [13]. Another study about the subject injuries while doing rock climbing showed 88% males and 12% females [14]. These five studies show that the distribution of the gender is relatively constant over the years (1999 until 2009) as well as over the different types of climbing (sport climbing, rock climbing, and VF) and the results correspond to the actual study. The biggest part of the women in these types of climbing is found in the group of persons who do VF. A portion of 20.2% of participants with any kind of professional medical training is also comparable to other studies about mountaineering emergencies, e.g. [6,15,16,17,18]. It is unlikely that this is biased because medical people are more interested in FA and emergencies since a positive response to participate was given by nearly 100% of those mountaineers who were asked to join the study. Summarized it can be concluded that the collective of the study presented here is representative for the discipline and well comparable to other studies.
The higher number of women on VF may be explained because most people think that doing a VF is not so difficult and not so dangerous and men perhaps prefer to do sport which brings them to their physical and mental limit. Table 1 gives an overview about common grading systems and the respective demands. Many people do a VF by the way when they are doing a hiking holiday. They think that they do not need a specific knowledge. This is supported by local tourism associations which promote via ferratas as fun or adventure event for (nearly) everybody. A short internet survey in July 2023 with the searching parameters “Brenta” (a well-known VF region in northern Italy) + “Klettersteig” (=VF) + “Tourismuswerbung” (= tourism advertising) resulted in 66 hits, all of them with comments like “...most beautiful...of the Alps...” or “explore the wonderful...region”. Not a single one added some information about the minimal requirements to do any of the suggested climbs. The tourism office of Lac Annecy / France advertises as follows: “The progression is done in complete safety, thus opening up steep and sometimes vertiginous terrain to a wide public.” (https://en.lac-annecy.com/activities/outdoor-sports/via-ferrata/ , 18.7.2023). The Departement Alpes de Haute Provence (France) has published “A fun alternative to climbing with all the thrills of altitude…” (https://www.tourism-alps-provence.com/via-ferrata/, 18.7.2023). The tourism office of Kotor (Montenegro) advertises the Škurda Canyon as follows: “Ferratas are suitable … for people with average physical fitness that are not engaged in active hiking and sports” (https://kotor.travel/via-ferrata/, 18.7.23). Similar phrasings may be found elsewhere, most of them without sufficient information (if any) about the respective requirements.
The average age was 41 years (18 - 70). Younger persons who do VF were seen during data acquisition but not registered because one including condition given by the ethical commission was a minimum of 18 years. With some younger people in the field the real collective should be a bit younger than given in our study. Küpper et al. identified an average age of 36.8 years in mountaineers who reached the Margherita hut (4559m, Monte Rosa, Switzerland) [6]. Here all, also those younger than 18 years, were included. In the study of Paige et al. the average age was 29 years (11 - 63). He compared the pattern of injuries while doing sport climbing and rock climbing [11]. The average age in the study of Wyatt et al., who investigated the injuries while doing rock climbing, was also 29 years [12]. In the study of Bollen, who focused on injuries of rock climbers, the average age was 27 years (15 - 46) [13]. Bowie et al. identified an average age of 27.5 years (14 - 64) from persons who do rock climbing [14]. The higher mean age in our study may be explained partially because of the including condition of a minimum of 18 years. It is also possible assumption that persons who do VF were older than persons who do (alpine) rock climbing because many people think that a VF is an easy and safe option to climb [19]. The most people do not have such a respect for VF than for rock climbing, so persons who did not get in touch with climbing, started also in a higher age with a VF. With regard to emergencies and FA a different spectrum of diagnoses and therefore different requirements for sufficient FA should be expected in an older collective.
Approximately two-thirds of the probands did not have any physical exercise in their profession. Therefore, they have to do endurance training in their leisure time to get a certain degree of fitness. In addition to the physical challenge of a VF it should be noted that in some regions the altitude, altitude difference, and the physical and mental load because of exposure in vertical or even overhanging terrain should be not neglected. This combined physical and mental load causes a more rapid exhaustion. In addition to physical exhaustion, which impairs climbing a difficult passage, mental stress causes a higher expenditure of energy, uneconomic movements and by this to an earlier exhaustion – not to mention “mental exhaustion” when people who could move on do not do so just because the mental batteries are low. It is a vicious circle.
We asked for endurance sport per week to get an idea of their fitness and their coenesthesia because this is important for doing a VF safe and successfully [20]. If the persons who do VF do not have a good physical condition, coenesthesia and surefootedness, the risk of an accident, and blocking by exhaustion increases a lot. It should be noted that the information about the endurance sport per week and the physical requirement of the participant’s profession was self-assessed which may cause a bias. A study of Prokop et al. researched the self-assessment of probands relating to their fitness [21]. 80% of the participants overestimated and 8% underestimated their fitness level. However, with 67% of the probands without physical workload at work and 34% who did endurance training only once per week or not at all the fitness of the participants must be rated as low and probably not adequate for the VF planned.
It is interesting that the probands were 23.3 days per year (1 - 300) in the mountains but only 3.7 days (1 - 50) of these days on a VF. This illustrates that most people do VF occasionally when they are in the mountains for any other reason. It is possible that the preparation for the VF suffers because the main purpose of the time in the mountains is to do something else, e.g. a hiking tour.
Only 37.6% of the probands were climbers which means that 62.4% probably were not experienced in using safety equipment. This is in accordance to Faulhaber et al. who reported that about 10% of VF climbers used inadequate safety equipment (or no such equipment at all) and females used significantly less helmets than men [22]. It is also probable that most participants were not used to move in exposed situations at higher altitudes or steep, vertical, or even overhanging terrain. Because of this they were unable to estimate the technical, physical and mental challenge correctly. Then the demands of the route will easily exceed the ability of the climber and often result in injuries or blockages. This chain of causation is discussed in detail in [23] and also since decades in the accident statistics from the DAV (German Alpine Club) [9,24]. In the more recent DAV statistics of the accidents in 2012/2013 it is mentioned that the accidents on VF have quadrupled since 2000 and that blockages were the most important problem (46%) and much more common than in other activities in the mountains [25]. Although the total incidence of accidents has decreased the problem of blockage is still the same (53% [26] or 56% [9], respectively).
Only 6.7% of the probands climbed with a mountain guide [25]. This is very few, especially with regard to the fact that most persons were not experienced climbers. The tendency from 2006/07 and 2012/13 has continued as more recent data (2020/21) of the German Alpine Club show. Blockages because of exhaustion and overestimation of the climber’s capabilities are the most common reason for emergencies at VF in the report 2020/21 again with 54% of all rescue operations at VF [9,27]. In some regions this might be even more: In the Allgäu (Southern Germany) which includes the “Mindelheimer Klettersteig” (one of our investigation sites) this might be up to 90% of all emergency calls from VF (U. Schwarz, preliminary evaluation of the data of “Christoph 17”, helicopter base in Kempten, personal communication, 2023). 9% “physical problems” may be added to the 54% because this should be inadequate fitness in most cases. With this one may conclude that 63% of all incidences could be avoided with proper preparation and tour planning. Of course, this would avoid any necessity for FA or rescue operations, too. Compared to these 63% all the other factors causing emergencies on VF are of minor importance: rock fall 3%, fall 24%, others 9% [27].
28.1% of the mountaineers reported that they didn’t ever participate in a FA course. This may be biased because most of them had a driving licence ad it is mandatory to have a FA training to get it. Probably this was very long ago and therefore they did not remind to have had a FA training. The knowledge of such courses decreases already after some months [28] which is also shown by the actual study (Table 2). Interestingly there are some topics which the participants obviously forget much earlier or more than others. Such themes should be more stressed in refresher trainings. The decrease of knowledge has been discussed in several papers and any recommendation for a regular refreshment of the knowledge is based on these studies (e.g. [29,30,31,32,33]). However, any training should be adapted to the specific demands of wilderness and especially VF. Specific mountaineering courses were joined by 27.6% of the probands. This shows that only a quarter of the people is interested to improve their skills. However, specific FA skills of the comrades are vital for the victim since professional rescue teams need at least half an hour at perfect weather conditions and in a region with perfect infrastructure to reach the site by helicopter [6]. Although just 20 probands investigated the group of mountaineers with a target group-oriented training in alpine FA and companion rescue outplayed all other groups with a total of 1423 participants to such an extent that such a specific training should be a “must” for any person going to the mountains.
The most frequent emergencies in the actual study were sunburn (23.9%), contusion (17.8%), open wounds (13.1%) and exhaustion (10.8%). In a study from Schwarz the most frequent emergencies while doing ice-climbing were open wounds (55.2%), haematoma (21.9%) and frostbite (9.4%) [34]. In a study from Küpper et al. were 49.5% of all emergencies from mountaineers trauma, 23.2% medical emergencies (internal medicine), 13.1% typical alpine emergencies (for example hypothermia, heat stroke, sunstroke, exhaustion), 7.9% altitude sickness and 3.3% other emergencies [6]. While the most frequent emergency while doing a sport in the mountains is traumatic injury the most important emergency on VF was exhaustion. This corresponds to information from the mountain rescue services: 46% [25] respectively 71% [23] or 63% [27] of the emergencies on VF were blockage or exhaustion. This shows that different disciplines of sport in the mountains have different kinds of injuries or medical problems, so that these different disciplines need different FA knowledge for a sufficient first treatment of an injured person. Any FA training for VF aspirants should take into account the specific spectrum of diagnoses described above and prevention by careful estimation of the own capabilities and the demands of the tour.
The exhaustion of persons who climbed VF was a frequent reason for emergencies which shows that the self-assessment of exercise capacity in relation to the tour planned was not adequate. It is interesting that hypothermia and lightning stroke were quite common on FA, but the FA questions on these topics were not well answered. Thomson and Howard researched over two years the lightning strokes in the USA and they figured out that the most lightning strokes occurred while doing outdoor leisure activities [35]. Cherington published similar results before [36]. Although the numbers of cases given by different studies differ it is generally accepted that the risk of a strike by lightning is significant higher in climbers than in a normal population. In our study the number of incidences cannot be compared directly with a normal population (e.g. Austia with about 5 cases / year [37,38]) because the probands were asked to report any incidence they had ever experienced. Decreasing weather conditions, stumble, fall and exhaustion or deficiency in concentration are significant risk factors for emergencies in the mountains. In the actual study the possibility of a rapid changing weather in the mountains was significantly underestimated because 3.1% of the probands got or experienced a lightning stroke which is significantly more than the normal (urban) population. In a study from Cherington persons who were in the mountains suffered also significantly more often from a lightning stroke [36]. In specific FA trainings there should be a chapter about meteorology included to prevent this kind of injury. Although epidemiological data are scarce it should be noted that only the minority of lightning strokes is primarily fatal and that even victims who do not breathe anymore have a good chance when resuscitation starts immediately [39,40,41,42,43]. The first treatment of lightning strokes is included in the curriculum of normal first-aid courses but it is an even more important topic for persons on VF. The correct behaviour in a case of a thunderstorm is also necessary to be taught.
The most often injured parts of the body were the upper and lower extremities and the head. This distribution was also found in a study of Johnson et al. [44]. In a study which investigated the injuries of persons who were rescued by helicopter over six years, the most affected part of the body was the lower extremities but here a significant number of patients were doing others than VF [45]. This was similar in the study from Schussman et al. [46]: most injuries were located at the lower extremities, second the head and third the upper extremities. Some injuries could be avoided or their severity could be reduced if the persons had the correct equipment (e.g. a helmet) and can handle it. It should be noted that even medically relatively harmless injuries may have dangerous consequences in the mountains if the person cannot move anymore and night and cold or bad weather is coming.
Another interesting fact is that many injuries occurred because of stumble, falls and exhaustion, tiredness or deficiency of concentration. If the persons cannot estimate their physical condition and their mental capacity correctly this often leads to accidents, injuries and blockage. A chapter in specific FA courses should focus on correct self-assessment.
Only a half of the probands wore a helmet (52.7%) and gloves (53.2%) while climbing a VF. In the actual study the hand was the second often and the head the fourth often injured part of the body. Obviously proper protection of these parts of the body is essential. Only 50.9% of the probands carried a FA kit along. Half of the persons could not treat an injury. Especially if we consider that many VF take several hours to go the part of the probands who took adequate supplies with them (67.5%) was inadequate.
66.2% of the persons had additional clothes, 27.9% a rescue blanket and 10.5% a bivouac sac. With regard that most emergencies on VF were blockages [24] such things may become vital, even on “easy” VF. This should be pointed out in FA trainings.
The fact, that open wounds were third of the most frequent injuries, is interesting because only 50.4% of the participants carried pavement, 42.5% bandaging material, 38.9% sterile compresses and 19.7% disinfectant with them. There is a discrepancy between the equipment and the material needed if something should happen. A consolidated knowledge of FA is important because 60.2% of persons who had an accident treated themselves and 21.4% were treated by a companion. Persons with a medical education took more often sunglasses (p<0.1), sun protection (p<0.05), bivouac sack (p<0.05), SamSplint® (p<0.1) and disinfectant (p<0.1) with them. Obviously, persons with a medical training are more sensitised to medical equipment they may need in the field.
The most frequent correct answered themes of the FA questions were cardiac emergencies (49.6%), high altitude cerebral edema (HACE, 43.2%), snow blindness (40.9%), injuries of the head (37.1%) and haemorrhagic shock (35.3%). In our society heart emergencies are very present, so many people have a rudimentary knowledge about this topic. However, in a study from Küpper et al. only 7.4% of the 2731 emergencies in the Valais (Switzerland) and Tyrol (Austria) were cardiac emergencies [47]. It can be concluded that FA knowledge about this topic is of less importance on VF. The knowledge about HACE is another topic which shows that the need in realty is not mirrored in the knowledge of the climbers: There is no VF so far which is located at an altitude where HACE is a risk for the mountaineers. Therefore climbers carry knowledge along which they will never need on VF. This is a good example that the topics FA trainings should differ to address the respective target group adequately.
The most frequently wrong answered themes of the FA questions were injuries of the back, injuries of the thorax, frostbite, acute mountain sickness and strategy of rescue. This was the same in earlier studies [6,8,16,18]. These themes are rare or absent in urban settings and therefore they are not included in normal first aid courses. However, injuries of the back and the thorax are quite frequent on VF. Both injuries may be life-threatening. The time until organized rescue will arrive must be managed by the companions as first responders with adequate FA. In a study from Küpper [47] the time of a rescue team to reach a place of an emergency showed a mean of 27.9 min in the region of Zermatt where the helicopter is based in the centre of the region. In Austria the helicopters are based in the Valley Inn and for any rescue operation they have to follow the long north-to-south oriented valleys for about another 30 min.
The persons who did a first aid-course in the last two years answered 9/18 FA questions correctly which was significantly different to those whose course was longer ago. This proves that a regular refreshment is necessary. This result is in accordance to several other studies [28,48,49,50,51,52,53].
The answers concerning strategy of rescue were insufficient. In the wilderness a strategic management of an emergency is vital due to the long rescue chain which needs hours, sometimes even more [47]. This illustrates that a specific training for emergencies at a remote place is necessary. This is in accordance to Donelan and Macias et al. who pointed out that also medical personnel needs a specific education for emergencies in the wilderness [54,55]. Küpper et al. published similar results 2003 in a study about the first aid-knowledge of mountaineers [6].
It is interesting that the persons who had the self-assessment “very good” for a respective theme, only 30% of these probands answered the corresponding FA question correctly, especially concerning the topics fractures, frostbite and heat stroke. Due to minor relevance this might be less important for resuscitation where most patients will not survive because of the long rescue chain from a VF, but the striking difference in hypothermia, fractures, strategy of rescue is remarkable. This shows that a self-assessment is not a valid indicator whether a refresher course is necessary. Küpper et. al and other groups had the same result in “classic” mountaineers and trekkers [6,7,15,16,56].
The conclusion of the actual study is that specific FA courses are essential to reduce the consequences of emergencies in the field. Furthermore, a regular refreshment should be recommended. The latter should be joined every three years. This is a compromise between several factors, especially the decrease of knowledge over time and the acceptance by a significant group of alpinists. Only few data are available when a refresher course for mountaineers should be recommended [6]. Like our study several authors have shown a significant decrease in skills in resuscitation over 1 year [28,48,50]. Surprisingly this was only a little less in paramedics [48]. Beside other factors the acceptance of courses is influenced by their duration. The “Wilderness First Responder (WFR)” has guides and instructors as primary target group [57] and it seems unrealistic to perform such an extensive training to a general public of alpinists. To train as many mountaineers as possible the basic training should not exceed 3 days or 6 evenings and the refresher should be limited to 1 day or 2 evenings [6]. Trainings are always time restricted and therefore a balance between stressing the principles and the practice of FA must be found. As Rettig and also Taubenhaus discuss in detail teaching principles should be favoured because understanding will produce more confidence than training emphasizing techniques but not understanding [58,59]. During training students needs to realize the problem, must be given a solution and be explained the solution [60,61,62].
Conclusion
FA capabilities of the general public going to the mountains is generally low. Although just 20 probands investigated the group of mountaineers with a target group oriented training in alpine FA and companion rescue outplayed all other groups with a total of 1423 participants to such an extent that such a specific training should be a “must” for any person going to the mountains. The most important topics for such a training for VF climbers are given in the paper.
References
- Randelzhofer, P., Bergunfallstatistik 2008-2009 [Statistics of mountain accidents 2008-2009]. 2010, Munich: Deutscher Alpenverein [German Alpine Club].
- Nakano, T., et al., Hypobaric hypoxia is not a direct dyspnogenic factor in healthy individuals at rest. Respir Physiol Neurobiol, 2015. 218: p. 28-31. [CrossRef]
- Schoffl, V., et al. Consensus Statement of the UIAA Medical Commission Vol.17: The UIAA Medical Commission Injury Classification for Mountaineering and Climbing Sports. 2010; Available from: www.theuiaa.org/medical_advice.html.
- Schoffl, V., et al., The UIAA Medical Commission injury classification for mountaineering and climbing sports. Wilderness Environ Med, 2011. 22(1): p. 46-51. [CrossRef]
- Orchard, J., Orchard Sports Injury Classification System (OSICS). Sport Health, 1995. 11(1): p. 39-41.
- Kupper, T., et al., First aid knowledge of alpine mountaineers. Resuscitation, 2003. 58(2): p. 159-169. [CrossRef]
- Scharfenberg, C., et al., The need for specific first aid and emergency knowledge whilst trekking in remote areas – results of the ADEMED (Aachen DEntal and MEDical) Expedition to the Annapurna region, Nepal. Health Promotion & Physical Activity (HPPA), 2021. 14(1): p. 17-24. [CrossRef]
- Gschwandtl, C., [Trekker and expedition climber as comrade rescuers in the Solo Khumbu-Mt.Everest Region, Nepal - development of a target group specific training concept for First Aid and risk management in remote high mountain regions - results of the ADEMED Expedition 2011], in Dept. of Occupational and Social Medicine. 2019, RWTH Aachen University: Aachen.
- Randelzhofer, P. Bergunfallstatistik 2020/2021. 2022.
- Schoffl, V., et al., Evaluation of injury and fatality risk in rock and ice climbing. Med Sport, 2010. 40(8): p. 657-679. [CrossRef]
- Paige, T.E., D.C. Fiore, and J.D. Houston, Injury in traditional and sport rock climbing. Wilderness Environ Med, 1998. 9(1): p. 2-7. [CrossRef]
- Wyatt, J.P., G.W. McNaughton, and P.T. Grant, A prospective study of rock climbing injuries. Br J Sports Med, 1996. 30(2): p. 148-50. 10.1136/bjsm.30.2.148.
- Bollen, S.R., Soft tissue injury in extreme rock climbers. Br J Sports Med, 1988. 22(4): p. 145-7. 10.1136/bjsm.22.4.145.
- Bowie, W.S., T.K. Hunt, and H.A. Allen, Jr., Rock-climbing injuries in Yosemite National Park. West J Med, 1988. 149(2): p. 172-7.
- Lechner, K., [Risk Management of Trekkers], in Inst. for Occupational and Social Medicine. 2013, Doctoral Thesis at the Medical Faculty, RWTH Aachen Technical University: Aachen.
- Scharfenberg, C., [First Aid Knowledge of Trekkers], in Doctoral Thesis, Inst. for Occupational and Social Medicine. 2013, RWTH Aachen Technical University: Aachen.
- Clarke, C.R., Cerebral infarction at extreme altitude (abstract), in Hypoxia, Exercise and Altitude, J.R. Sutton, C.S. Houston, and N.L. Jones, Editors. 1983, Liss: New York. p. 453-454.
- Lollgen, H., et al. Physical activity, exercise prescription for health and home-based rehabilitation. Sustainability, 2020. 12, 1-12. [CrossRef]
- Hellberg, F. and C. Semmel, Unfallgefahr auf Klettersteigen. Panorama, 2007. 59(5): p. 82-84.
- Hüsler, E.E., Klettersteiggehen. Lehrbuch und Ratgeber für alle Formen des Klettersteiggehens. 2006, Munich: Bruckmann Verlag GmbH.
- Prokop, N.W., et al., People who perceive themselves as active cannot identify the intensity recommended by the international physical activity guidelines. Open Access J Sports Med, 2014. 5: p. 235-241. [CrossRef]
- Faulhaber, M., et al., [Equipment, Risk Awareness and Safety-Relevant Behaviour of Via Ferrata Climbers]. Sportverletz Sportschaden, 2015. 29(3): p. 151-6. [CrossRef]
- Mosimann, U., Sécurité et accidents en via ferrata. Les Alpes, 2007(8): p. 18-21.
- Randelzhofer, P.M., Deutscher Alpenverein e.V., Bergunfallstatistik 2006-2007 [Statistics of mountain accidents 2006-2007]. 2008, Munich: Deutscher Alpenverein [German Alpine Club].
- Randelzhofer, P., Bergunfallstatistik 2012-2013 [Statistics of mountain accidents 2012-2013]. 2014, München: Deutscher Alpenverein [German Alpine Club].
- Hüper, L., L. Fritz, and J. Janotte, Herausgefordert, nicht überfordert - Tourenplanung für den Klettersteig. DAV panorama, 2022. 74(3): p. 64-68.
- Ulmer, H.V., Concept of an extracellular regulation of muscular metabolic rate during heavy exercise in humans by psychophysiological feedback. Experientia, 1996. 52(5): p. 416-20. [CrossRef]
- Spitzer, G., [Effectiveness surveillance of first aid education of lay persons]. Hefte Unfallheilkd, 1978. 132: p. 92-94.
- Goniewicz, M., [The ability of drivers to give first aid - testing by questionnaire]. Wiad Lek, 1998. 51(3-4): p. 208-215.
- Everson, G., et al., Ineffectiveness of a mass mailing campaign to improve poison center awareness in a rural population. Vet Hum Toxicol, 1993. 35(2): p. 165-167.
- Lejeune, P.O. and H.H. Delooz, Why did persons invited to train in cardiopulmonary resuscitation not do so? Eur Heart J, 1987. 8(3): p. 224-8. [CrossRef]
- Pearn, J., et al., Who accepts first aid training? Aust Fam Physician, 1980. 9(9): p. 602-605.
- Kupper, T., et al., Qualified rescue by ski patrols - safety for the skier. Int J Sports Med, 2002. 23(7): p. 524-9. [CrossRef]
- Schwarz, U., Das Risiko von Verletzungen und Überlastungsschäden beim Eisklettern, in Institut für Arbeits- & Sozialmedizin. 2009, Rheinisch-Westfälische Technische Hochschule (RWTH): Aachen.
- Thomson, E.M. and T.M. Howard, Lightning injuries in sports and recreation. Curr Sports Med Rep, 2013. 12(2): p. 120-4. [CrossRef]
- Cherington, M., Lightning injuries in sports: situations to avoid. Sports Med, 2001. 31(4): p. 301-8. [CrossRef]
- Ulmer, H.V., U. Janz, and H. Löllgen, Aspects of the validity of BORG's scale. Is it measuring stress or strain?, in Physical work and efford, G. Borg, Editor. 1976, Pergamon Press: Oxford, New York. p. 181-196.
- Fimml, W., Alpenverein Südtirol, Deutscher Alpenverein, Oesterreichischer Alpenverein, Schweizer Alpen-Club SAC. 3: 20-26., Risiko Blitzunfall. Bergundsteigen, 2003(3): p. 20-26.
- Fontanarosa, P.B., Electrical shock and lightning strike. Ann Emerg Med, 1993. 22(2 Pt 2): p. 378-87. [CrossRef]
- Zafren, K., et al., Lightning injuries: prevention and on-site treatment in mountains and remote areas. Official guidelines of the International Commission for Mountain Emergency Medicine and the Medical Commission of the International Mountaineering and Climbing Federation (ICAR and UIAA MEDCOM). Resuscitation, 2005. 65(3): p. 369-72. [CrossRef]
- Muehlberger, T., P.M. Vogt, and A.M. Munster, The long-term consequences of lightning injuries. Burns, 2001. 27(8): p. 829-33. [CrossRef]
- Mulder, M.B., et al., Remarkable rates of lightning strike mortality in Malawi. PLoS One, 2012. 7(1): p. e29281. [CrossRef]
- Strohle, M., et al., Lightning accidents in the Austrian alps - a 10-year retrospective nationwide analysis. Scand J Trauma Resusc Emerg Med, 2018. 26(1): p. 74. [CrossRef]
- Johnson, R.M., et al., Injuries sustained at Yellowstone National Park requiring emergency medical system activation. Wilderness Environ Med, 2007. 18(3): p. 186-9. [CrossRef]
- Kaufmann, M., B. Moser, and W. Lederer, Changes in injury patterns and severity in a helicopter air-rescue system over a 6-year period. Wilderness Environ Med, 2006. 17(1): p. 8-14. [CrossRef]
- Schussman, L.C., et al., The epidemiology of mountaineering and rock climbing accidents. J Wild Med, 1990. 1(3): p. 235-248. [CrossRef]
- Kupper, T., [Workload and professional requirements for alpine rescue], in Professoral Thesis, Dept. of Aerospace Medicine. 2006, RWTH Aachen Technical University: Aachen.
- Stratman, D., H. Nolte, and S. Sämann, [An investigation of the effectiveness of the training of ambulance personnel]. MMW Munch Med Wochenschr, 1974. 116(50): p. 2199-2204.
- Safar, P., et al., Education research on life-supporting first aid (LSFA) and CPR self-training systems (STS). Crit Care Med, 1981. 9(5): p. 403-404.
- Roth, H.J., A. Gaham, and R. Juchems, [Evaluating the knowledge of lay helpers following a single completed course in cardiopulmonary resuscitation]. Med Klin, 1988. 83(11): p. 367-369.
- Jayaraman, S., et al., First things first: effectiveness and scalability of a basic prehospital trauma care program for lay first-responders in Kampala, Uganda. PLoS One, 2009. 4(9): p. e6955. [CrossRef]
- Yeakel, A.E., A study of the effectiveness of programmed instruction in respiratory resuscitation. Anesth Analg, 1969. 48(4): p. 628-32.
- Pavesi, G., et al., [Assessment of the efficiency of the first aid course among construction companies in the Province of Bergamo]. G Ital Med Lav Ergon, 2006. 28(1 Suppl): p. 114-6.
- Donelan, S., Mountaineering and mountain rescue--an introduction. Wilderness Environ Med, 2004. 15(1): p. 42-3. [CrossRef]
- Macias, D.J., K. Rogers, and J. Alcock, Development of a wilderness and travel medicine rotation in an academic setting. Wilderness Environ Med, 2004. 15(2): p. 136-145. [CrossRef]
- Lechner, K., et al., Risk Management and First Aid Knowledge of Trekkers in Nepal. Health Prmot Phys Act (HPPA), 2020. 13(4): p. 21-24.
- Lindsey, L., et al., Wilderness First Responder: Recommended Minimum Course Topics. Wilderness Environm Med, 1999. 10: p. 13-19. [CrossRef]
- Rettig, A., [Mountain climbing accidents-measures and problems in first aid]. Osterr Schwesternztg, 1973. 26(8): p. 174-177.
- Taubenhaus, L.J., What to do until the ambulance comes. Phase I of community emergency care program. N Y State J Med, 1972. 72(4): p. 500-502.
- Donelan, S., Teaching wilderness emergency care. Wilderness Environm Med, 1999a. 10: p. 40-43.
- Donelan, S., Teaching emergency care skills. Wilderness Environm Med, 1999b. 10: p. 125-127.
- Donelan, S., Secrets of a successful lecture. Wilderness Environ Med, 1999c. 10(3): p. 185-8.
- Kupper, T., et al., Workload during cardiopulmonary resuscitation. Int Arch Occup Environ Health, 2015. 88(2): p. 175-84. [CrossRef]
- Narahara, H., et al., Effects of cardiopulmonary resuscitation at high altitudes on the physical condition of untrained and unacclimatized rescuers. Wilderness Environ Med, 2012. 23(2): p. 161-4. [CrossRef]
Figure 1.
Age distribution of the collective.
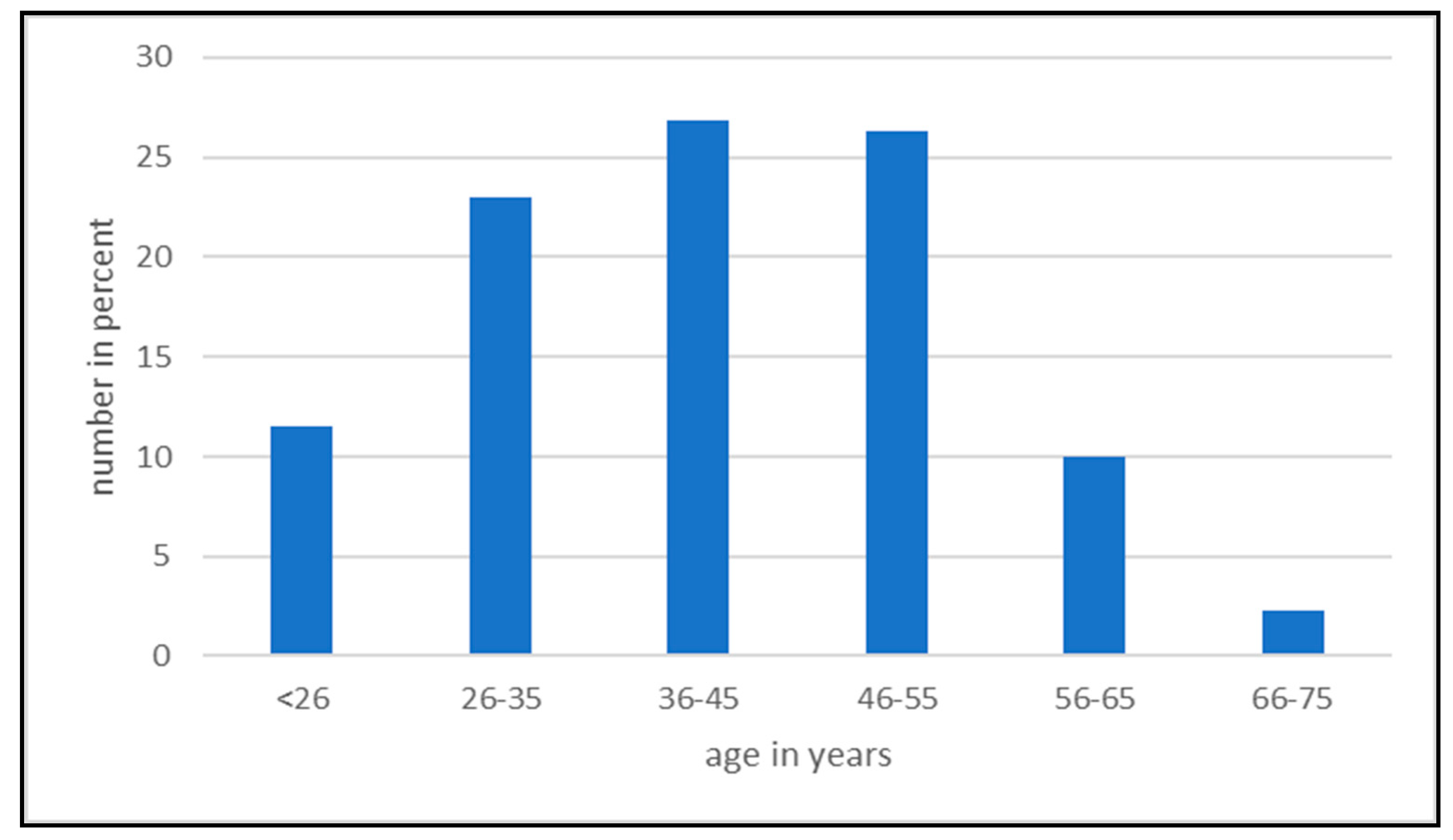
Figure 2.
Types of emergencies which occurred in the collective.
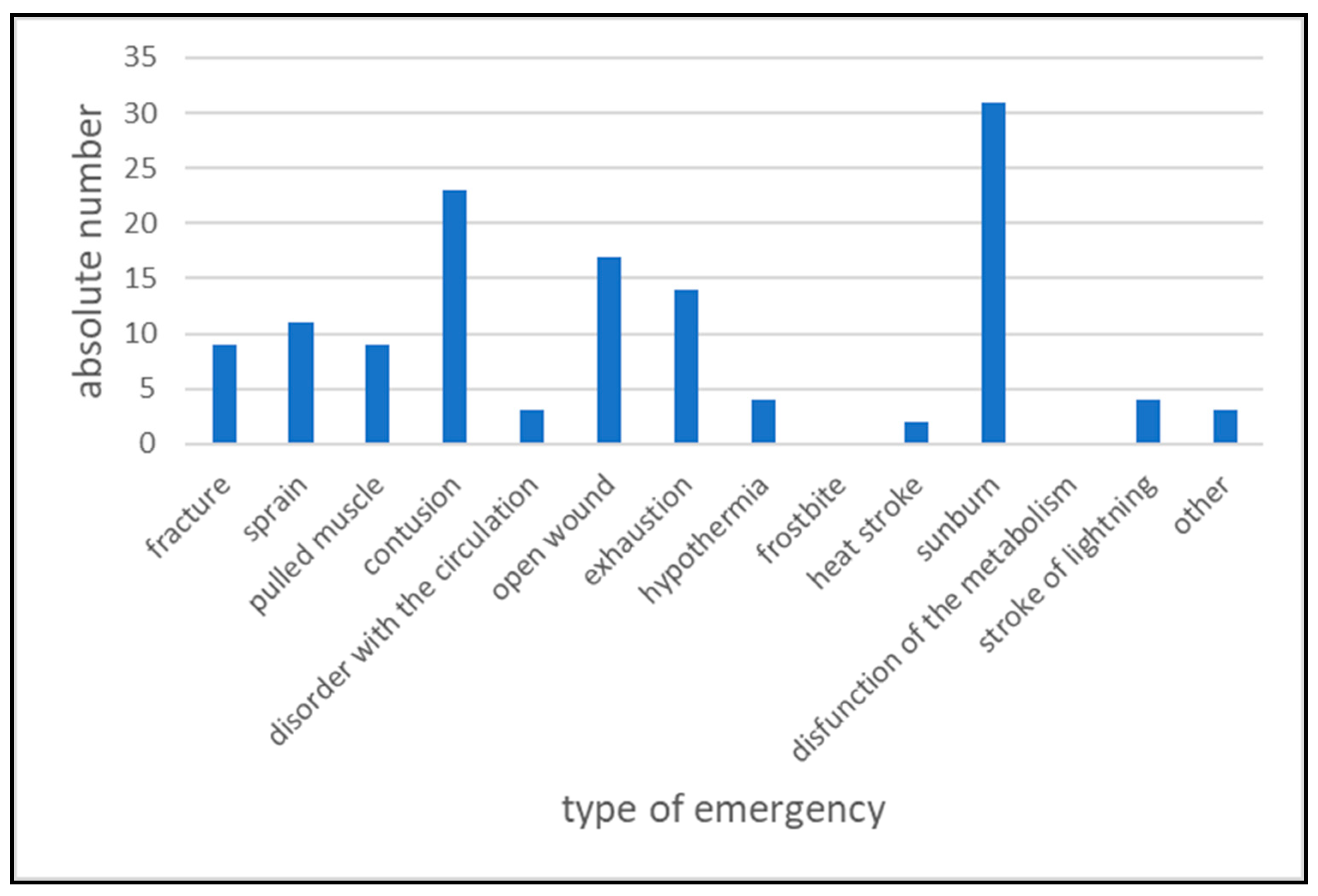
Figure 3.
Location of the injuries reported.
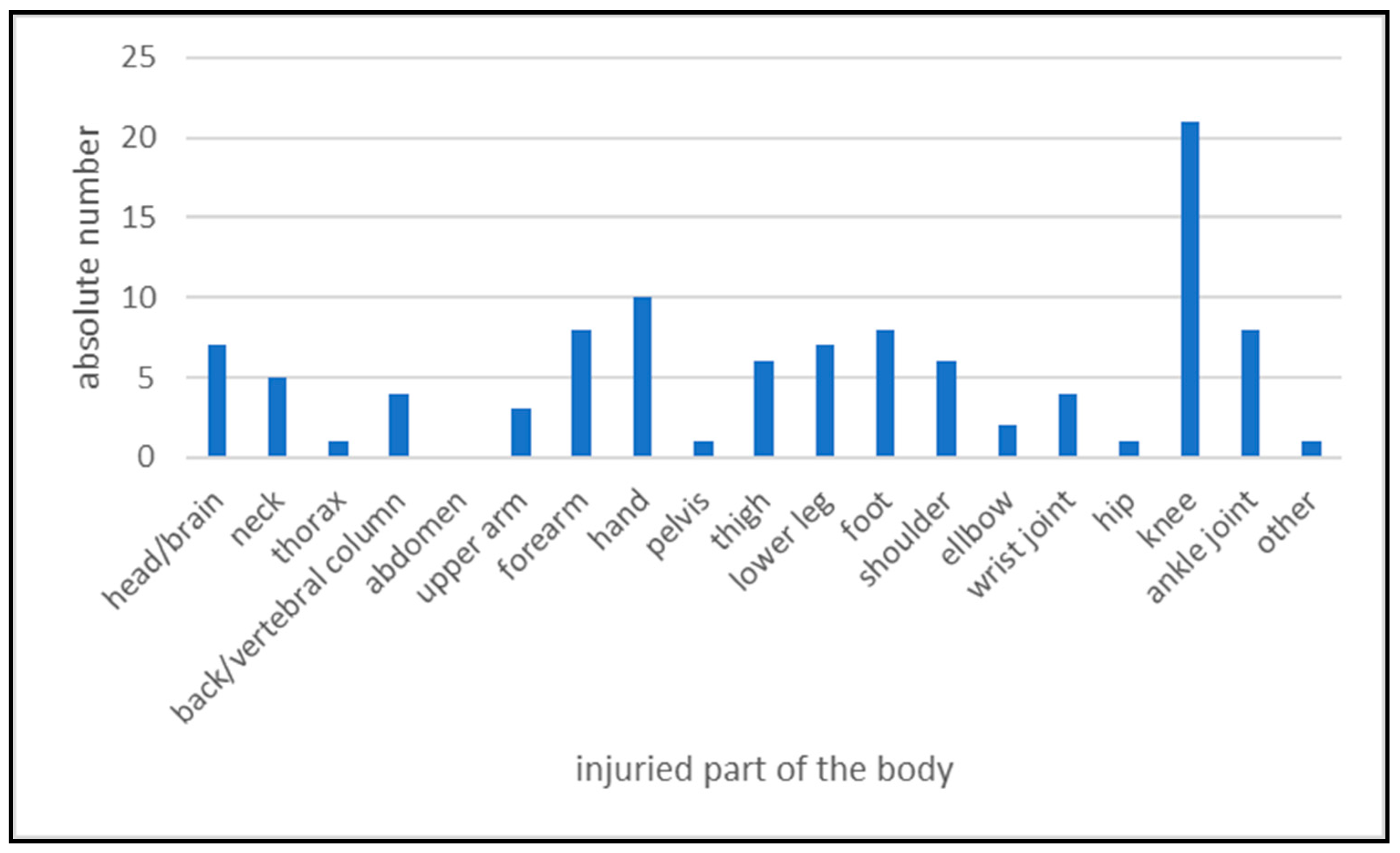
Figure 4.
Causes of emergencies on via ferratas.
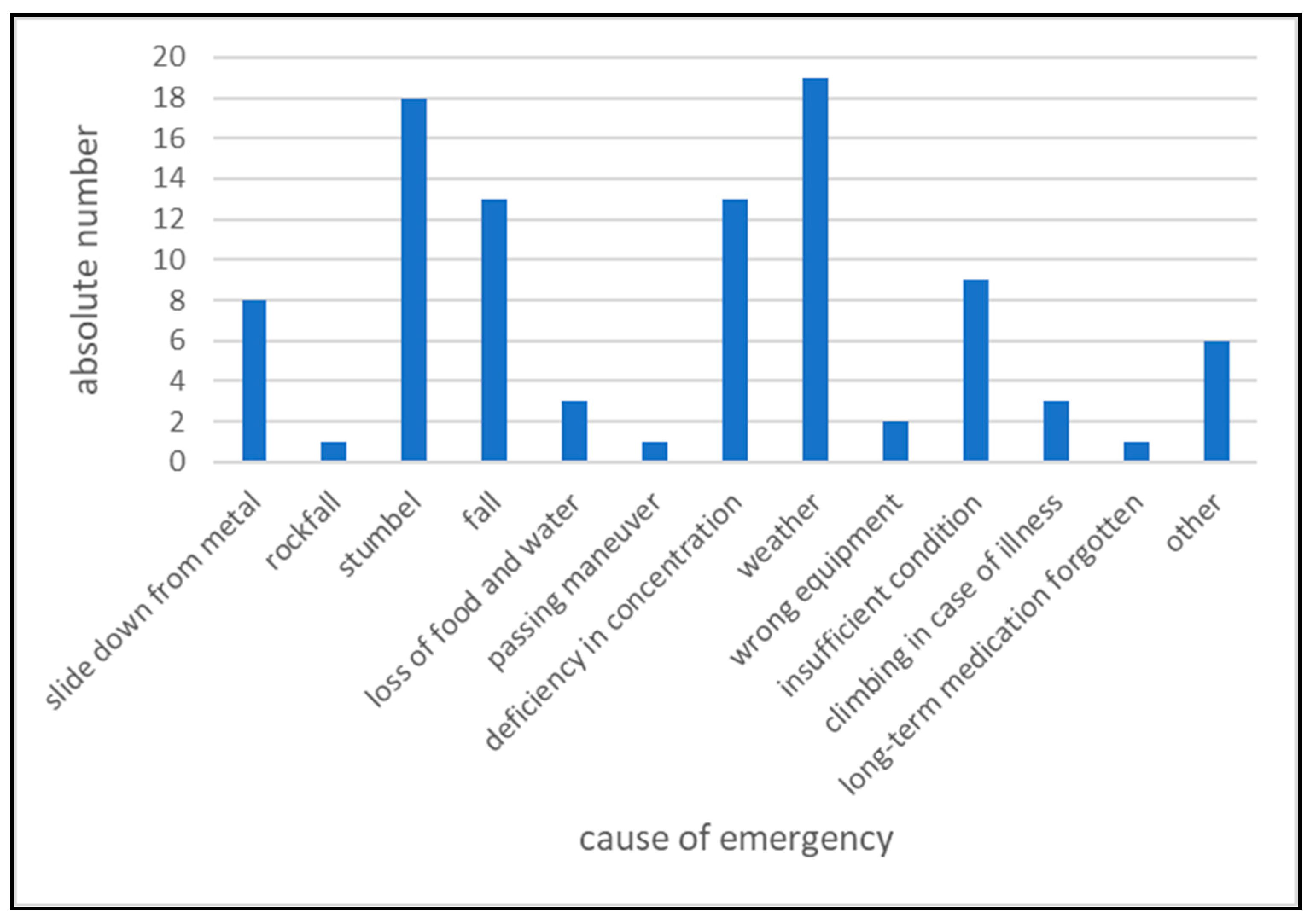
Figure 5.
Emergency and safety equipment carried along by the collective.
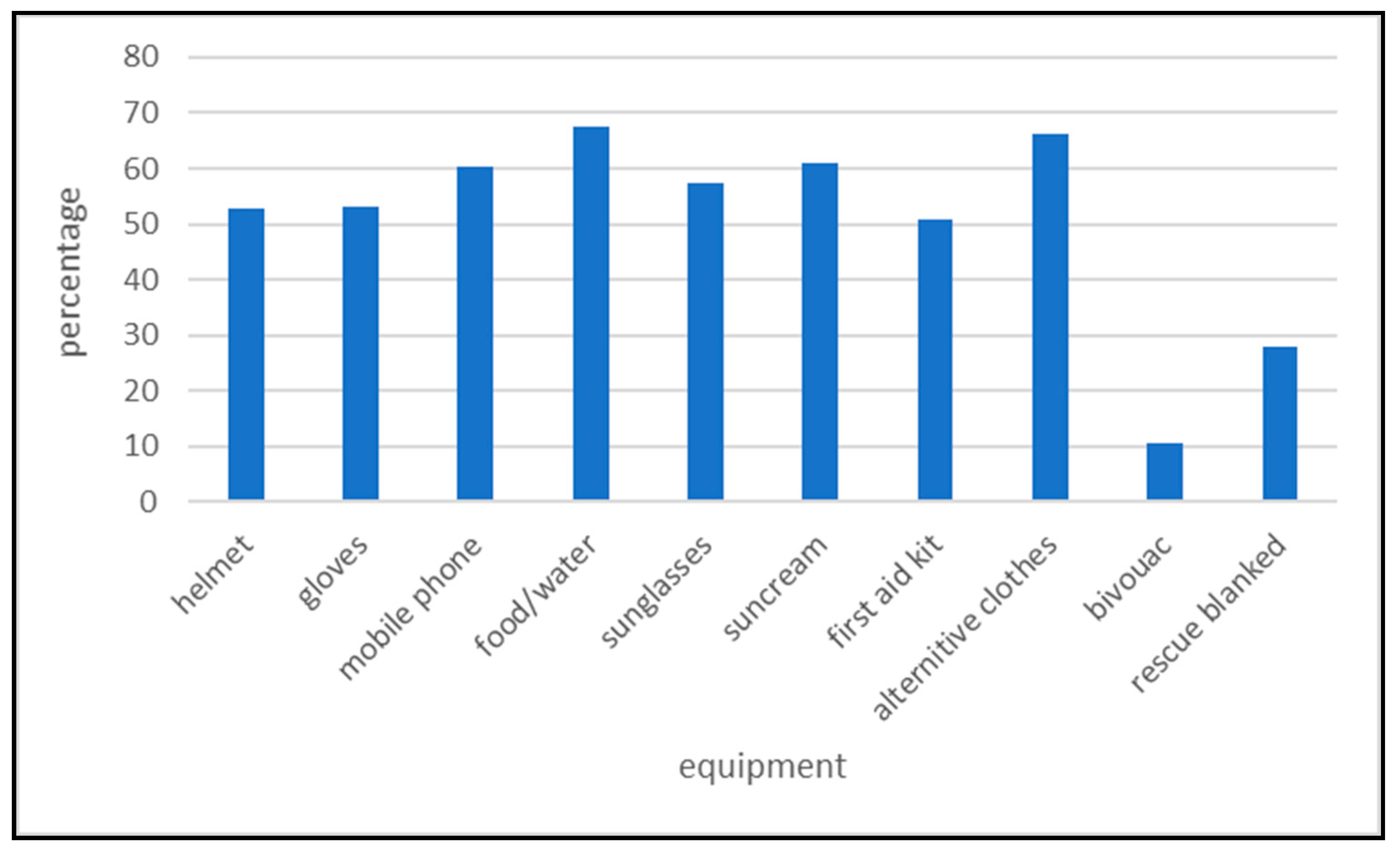
Figure 6.
Equipment of the first aid-kit.
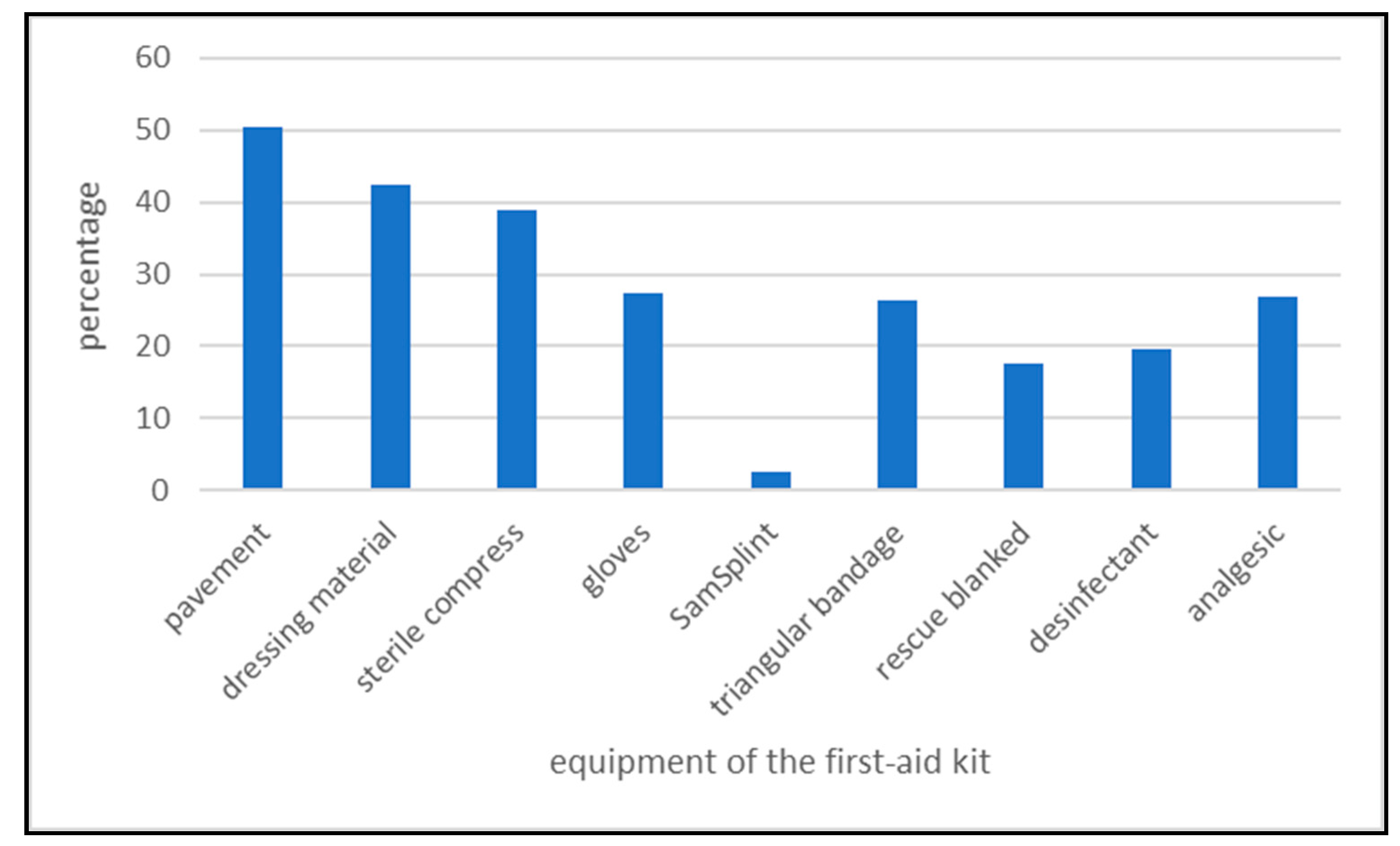
Figure 7.
Correct answers per person (VF climbers of the actual study and a control group which had the same questionnaire (data from [6], P<0.001).
Figure 7.
Correct answers per person (VF climbers of the actual study and a control group which had the same questionnaire (data from [6], P<0.001).
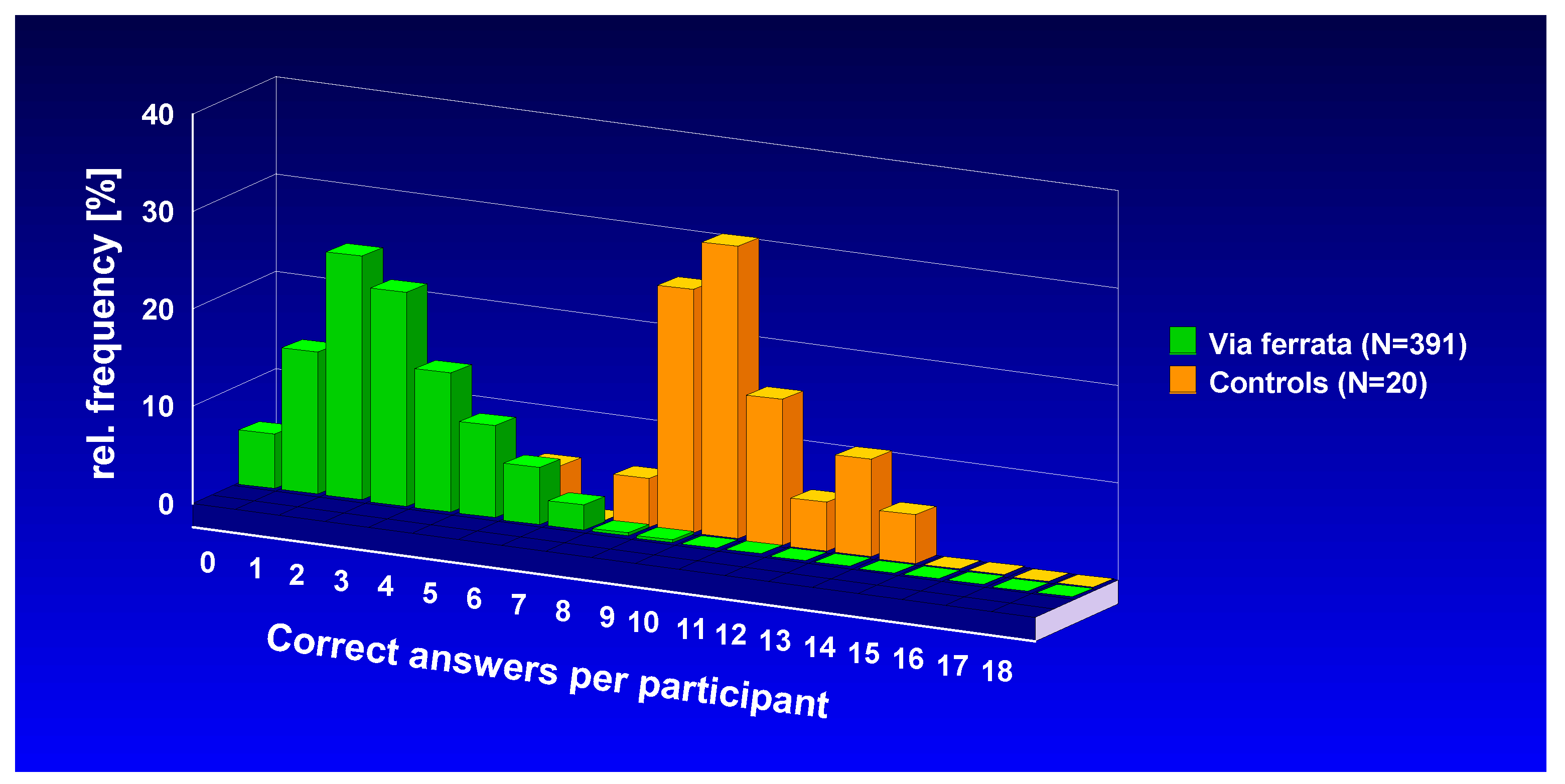
Figure 8.
Correct answers of the First Aid questionnaire.

Figure 9.
Comparison of the self-assesment “very good“ with the corresponding correct and wrong answers.
Figure 9.
Comparison of the self-assesment “very good“ with the corresponding correct and wrong answers.
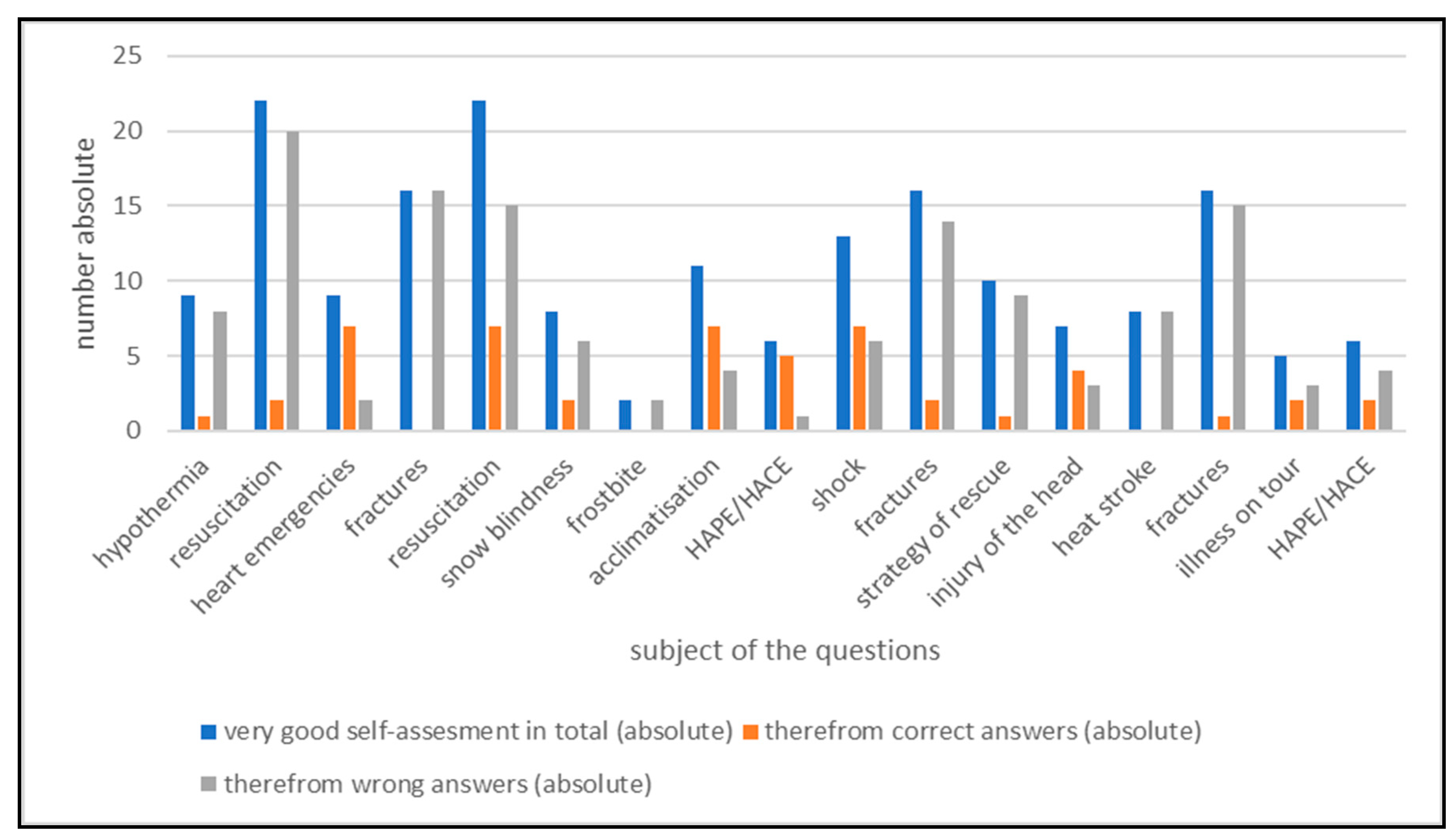
Figure 10.
Correct answers of VF climbers and those of an earlier study with trekkers in Nepal. KEME: “Knowledge and Education in Mountaineering Emergencies” which studied mountaineers in the Western Alps, [63]; KETE: “Knowledge and Education in Trekking Emergencies” which studied trekkers in the Himalayas [7], KETE1 in the Annapurna Region, KETE2 in the Everest Region.
Figure 10.
Correct answers of VF climbers and those of an earlier study with trekkers in Nepal. KEME: “Knowledge and Education in Mountaineering Emergencies” which studied mountaineers in the Western Alps, [63]; KETE: “Knowledge and Education in Trekking Emergencies” which studied trekkers in the Himalayas [7], KETE1 in the Annapurna Region, KETE2 in the Everest Region.


Table 1.
Grades and characteristics of Via ferrata [64].
Table 1.
Grades and characteristics of Via ferrata [64].
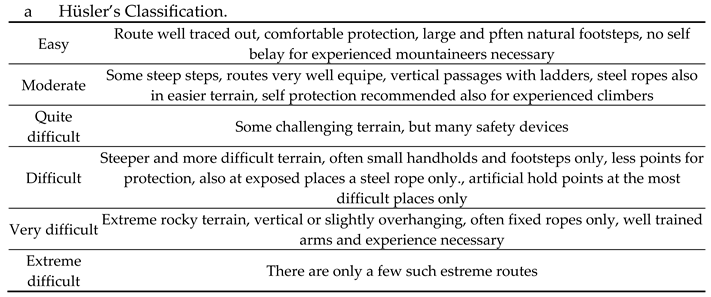
Table 2.
Decrease of FA knowledge over 3+ years indicated by the amount of correct answers.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



