
Submitted:
23 August 2023
Posted:
24 August 2023
You are already at the latest version
Abstract
(1) Background: Endoscopic submucosal dissection (ESD) has been widely accepted as the standard method for treating early-stage cancer or precancerous lesions in the upper gastrointestinal tract, however it may be difficult in patients with liver cirrhosis due to coagulation dysfunction or presence of gastroesophageal varices. We aimed to demonstrate the safety and efficacy of ESD in these population. (2) Methods: We retrospectively collected the clinical data and analyzed. Patients inclusion criteria: 1) patients with liver cirrhosis; 2) patients who underwent ESD; 3) patients diagnosed of early-stage cancer or precancerous lesions in the upper gastrointestinal tract. (3) Results: Eight patients were enrolled from April 2019 to April 2023, of whom 3 were male and 5 female, with age ranging from 43 to 70 years old. Seven lesions were located in the stomach, and the other one lesion in the esophagus. ESD was performed successfully in all patients, and the resected lesion size ranged from 2 to 6 cm. Only one patient encountered postoperative complication, chest pain and fever. No recurrence of noticed during a follow-up of 6 to 36 months. (4) Conclusions: ESD is safe and effective for treating upper gastrointestinal early-stage cancer or precancerous lesions in patients with liver cirrhosis.
Keywords:
early-stage cancer
; precancerous lesion
; endoscopic submucosal dissection
; liver cirrhosis
1. Introduction
Upper gastrointestinal cancers, mainly referring to esophageal and gastric cancers, are two of the most common cancer around the world, with high incidence and mortality rate, especially is Asian counties, such as China, Korea and Japan [1]. With the development of patients’ awareness and equipment of cancer screening, more and more early-stage cancer and precancerous lesions are found, which ultimately declined cancer-related mortality [2]. Early-stage cancer and precancerous lesions are associated with a better prognosis when timely treated. The treatment of these lesions mainly includes endoscopic and surgical resection, endoscopic resection is less expensive, less trauma, and offers faster recovery and better quality of life compared to surgery without compromising overall survival and disease specific survival [3,4,5,6]. Among various endoscopic methods, endoscopic submucosal dissection (ESD) is superior to others with a higher en bloc resection and curative resection rate [7,8], thus ESD has been widely accepted as the primary treatment option of early esophageal and gastric cancer in many countries.
Liver cirrhosis is another major health problem in Asian countries, especially in China, giving the high incidence of hepatitis B virus (HBV) and hepatitis C virus (HCV) infection [9]. Patients with liver cirrhosis are considered as high-risk candidates for invasive treatments including ESD due to the tendency to bleed and the vulnerability of tissues [10]. Although several studies have reported the safety and efficacy of ESD or related techniques in these population [11,12,13,14,15], many concerns have not been solved satisfactorily, for example, the proper perioperative management, how to deal with co-exiting esophagogastric varices, the minimum requirement of platelet account, etc. In the present study, we retrospectively collected and analyzed the clinical data of patients with co-exiting early esophageal/gastric cancer or precancerous lesions and liver cirrhosis, to explore the safety and efficacy of ESD in these population, as well as to explore the proper perioperative management.
2. Materials and Methods
2.1. Patients
We retrospectively collected the clinical data of enrolled patients at Department of Gastroenterology, the Second Xiangya Hospital of Central South University, from April 2019 to April 2023. Patients meted the following criteria were retrospectively enrolled in the analysis: 1) patients diagnosed of early-stage cancer or precancerous lesions in the upper gastrointestinal tract; 2) patients were diagnosed of liver cirrhosis before or simultaneously found with the cancerous of precancerous lesion; 3) patients underwent ESD at our hospital. The exclusion criteria of the study were as follows: 1) Patients with incomplete information; 2) patients who underwent surgery; 3) patients who underwent ESD at other hospitals, but sent the specimen to our hospital for confirmed diagnosis; 4) patients with severe cardiopulmonary disease who could not tolerate ESD procedure. This study was conducted in accordance with the Declaration of Helsinki, and was approved by the ethics committee of our hospital. All patients were informed of the potential risk of ESD and alternative treatment methods, and signed the informed consent form.
2.2. Endoscopic equiments and accessories
The ESD procedures were performed under general anesthesia using a single-channel endoscopy (GIF-Q260J ; Olympus Corp., Tokyo, Japan) with a transparent cap (D-201-11802, Olympus) attached to the front. A carbon dioxide insufffator (UCR ; Olympus) was used. Other equipment and accessories included a high-frequency generator (ICC 200 ; ERBE Elektromedizin GmbH, Tübingen, Germany), an argon plasma coagulation unit (APC300 ; ERBE), a dual knife (KD-650 L/Q, Olympus Corp., Tokyo, Japan), and an injection needle (NM-4L-1 ; Olympus). Submucosal injection in ESD was made with a mixed solution of 100 mL saline + 5 mL 0.2% indigo carmine + 1 mg epinephrine.
2.3. ESD procedure
The ESD was performed as previously reported [16,17]. Brieffy, the procedure had following steps : (a) determining the area of lesions using narrow band imaging and magnifying endoscopy; (b) marking the margin of the lesion ; (c) submucosal injection ; (d) circumferential mucosal incision ; (e) dissection of the lesion ; (f) management of the artificial ulcer ; Figure 1 and Figure 2 depicts an example of esophageal and gastric ESD.
2.4. Preoperative and postoperative management
Platelet were infused preoperatively in patients with platelet account of less than 50x10^9/L, frensh frozen plasma were infused for patients with coagulation dysfunction (mainly impaired INR), and albumin were infused for patients with blood albumin <30g/L. Intraoperative bleeding was recorded as the necessity of endoscopic hemostasis during ESD [14]. Postoperative bleeding was defined as any of the following: apparent hematemesis or melena, unstable vital signs, and a >2 g/dL decrease in hemoglobin concentration after ESD. Patients were kept nil per os (NPO) for 24 to 48 hours, then on a liquid diet for 3 days, and returned gradually to a normal diet within 2 weeks. An intravenous proton pump inhibitor was used during the hospital stay and then orally for another 4 weeks for gastric lesions. Postoperative observations included vital signs, recording of complaints of abdominal/ chest pain, dyspnea, haematemesis, melena, and abdominal distention, and an abdominal/chest examination.
2.5. Pathological assessment
The specimens were fixed, embedded in paraffin, and then sectioned. Hematoxylin and eosin staining was performed. En bloc resection refers to a resection that results in the removal of a single piece of tissue. R0 resection is defined as histologically complete tumor removal with tumor-free lateral and basal margins. A curative resection is defined as resected neoplasia restricted to the epithelium (m1) or lamina propria (m2) but not involving the muscularis mucosa (m3), with neoplasia-free vertical and radial margins and no lymphatic or vascular invasion.
2.6. Pathological assessment
Surveillance endoscopy was performed at 1, 3, 6, and 12 months and annually thereafter to observe healing of the wound and check for signs of stricture (for esophageal lesion) and recurrence.
3. Results
3.1. Basic clinical characteristics
During April 2019 to April 2023, a total of 106 patients with early esophageal cancer or precancerous lesions and 342 patients with early gastric cancer or precancerous lesions received ESD in our hospital. Among whom 8 patients had comorbid liver cirrhosis, and 7 patients had gastric lesions while the other one had esophageal lesion. Thus the incidence of comorbid liver cirrhosis was 0.94% (1/106, for early esophageal cancer of precancerous lesion) and 2.05% (7/342, for early gastric cancer of precancerous lesion).
Of the 8 patients, 3 were male and 5 were female, with age ranging from 43 to 70 years old. The course of liver cirrhosis was 0 to 5 years (0 means liver cirrhosis were found during assessment of the gastric lesion), and 4 patients had gastroesophageal varices and 2 of them had a history of endoscopic variceal therapy. Abnormal platelet count, anemia, impaired INR and low albumin were found in 6, 6, 3 and 6 patients, retrospectively (see in detail in Table 1).
As for the location of lesions, 7 were located at the stomach (5 in gastric antrum, 2 in gastric body) and the other one in lower esophagus. Among the 4 patients with GOV, the lesions were far from GOV in 3 patients, while the other patient with superficial esophageal cancer on esophageal varices. Two patients received esophageal variceal ligation before endoscopic treatment, and the ESD was performed 2 and 4 weeks later, respectively. Two, 3 and 2 patients received perioperative platelet, frensh frozen plasma and albumin infusion, retrospectively.
3.2. Treatment outcomes
ESD was performed successfully in all the patients, the operation time ranged from 45 to 230 minutes. Intraoperative bleeding was encountered in 4 patients. For the patient with esophageal lesion, a fully covered metal stent was inserted because of the following reasons: intraoperative bleeding was noticed owing to the submucosal esophageal varices, unintentional injury of the muscularis propria layer was noticed, and prevent stricture that may result from circumferencial ESD. The stent was removed 4 weeks later. The resected specimen measured from 2x1.8 cm to 6x2 cm, and en bloc resection was achieved in 6 of the 8 patients (75%). As for pathological results, 3 were gastric adenocarcinoma, 2 were gastric high grade intraepithelial neoplasia, 1 was gastric low grade intraepithelial neoplasia, 1 was gastric adenoma, and the remaining one was esophageal squamous cell carcinoma (ESCC). Curative resection was achieved in 5 patients (62.5%). The patients had ESCC had chest pain for 3 days and fever for 4 days (highest temperature 38.4 centigrade), and the symptoms relieved with antibiotics. And postoperative pathological result revealed submucosal infiltration (sm2) with negative vertical and lateral margin, and further surgery was recommended, however he refused. No recurrence or esophageal stricture was noticed during a follow up of 5 months. For the 7 patients with gastric lesions, no postoperative complication was reported, and no recurrence was noticed during a follow-up of 3 to 45 months.
4. Discussion
Liver cirrhosis is the 11th most common cause of death globally and China alone accounts for approximately 11% of the deaths [9,18]. Patients with liver cirrhosis have an increased incidence of esophageal and gastric cancer due to the fact that liver cirrhosis and esophageal/gastric cancer share some common risk factors such as alcohol intake, smoking, obesity, etc [19,20]. A 2.6-fold increased prevalence of gastric cancer and esophageal cancer was observed in patients with liver cirrhosis as compared to the general population [20,21]. Usually periodic endoscopy is performed for surveillance of GOV, the high incidence suggest that we should also pay attention to early esophageal/gastric cancer in liver cirrhosis patients. In our study, 7 of the 8 patients found the lesion during screening or surveillance of GOV. However, little is known about the incidence of early esophageal/gastric cancer in patients with liver cirrhosis. Zhu et al. [14] reported a proportion of 4.24% (25/565) patients had comorbid liver cirrhosis in patients with early esophageal cancer who underwent endoscopic submucosal tunnel dissection. In our study, 0.94% of patients had comorbid liver cirrhosis among patients with early esophageal cancer/precancerous lesions who received ESD. And we reported a proportion of 2.05% of patients had liver cirrhosis in patients received ESD for early gastric cancer or precancerous lesions. As far as we known, this is the first study who reported the incidence of comorbid liver cirrhosis in patients received gastric ESD for early cancer of precancerous lesions.
Endoscopic resection has been the standard method for treatment of early stage esophageal/gastric cancer and precancerous lesions. ESD offers higher complete resection rate, higher en bloc resection rate, and lower local recurrence rate than EMR, thus is recommended as the first choice, especially for lesion >2cm [7,8]. However, ESD in patients with liver cirrhosis is challenging due to the presence of GOV, ascites, coagulation disorders and/or thrombocytopenia. A systematic review and meta-analysis revealed that pooled rates of immediate & delayed bleeding, perforation, and death during EMR and/or ESD in patients with cirrhosis were 9.5% (CI 4.0–21.1), 6.6% (CI 4.2–10.3), 2.1% (CI 1.1–3.9) and 0.6% (CI 0.2–1.7), with only immediate bleeding rate higher than that in general population [22]. A multicenter observational study enrolled 134 early esophageal tumor lesions in 112 patients with liver cirrhosis reported 3(2.7%) perforations, 8 (7.1%) delayed bleedings, 8 (7.1%) sepsis, 6 (5.4%) cirrhosis decompensations within 30 days and 22 (19.6%) esophageal strictures [15]. A systematic review enrolling 68 gastric ESD patients reported a total of 8 (13.1%) post-ESD bleeding and 1 (1.6%) perforation [23]. As for intraoperative bleeding, Zhu et al. [14] reported a rate of 48% (12/25) during endoscopic submucosal tunnel dissection for early esophageal carcinoma in patients with liver cirrhosis, and Kwon et al. [24] reported 47% during endoscopic resection of gastric mucosal lesions in patients with chronic renal failure and liver cirrhosis. In the present study, intraoperative bleeding was found in 50% (4/8) patients, which is similar to the above reports.
Proper preoperative management of coagulopathy and thrombocytopenia is the prerequisite of the safety of invasive procedure such as ESD, usually frensh frozen plasma or platelet infusion is recommended [10,17]. Repici et al. [23] found that INR >1.33 and/or platelets count <105 000/mm3 should be regarded at increased risk of bleeding following ESD. While some studies have suggested that INR < 1.5 and platelet count > 50 000/mm3 can be used as critical values for patients with cirrhosis in assessing tolerance of invasive surgery [10,25]. In vitro studies have shown that a platelet count of (20-30) × 1000/mm3 is enough to produce thrombin for the maximum amplitude in thromboelastography to be normal [26]. Zhang et al. [27] reported 1 case with a platelet count < 30 × 1000/mm3 , and the patient count was > 30 × 1000/mm3 after infusion with frozen platelets before endoscopic treatment, no obvious bleeding was observed during or after ESD. In the present study, 2 of 3 patients with INR >1.33 and all the 2 patients with platelets counts less than 50 000/mm3 encountered intraoperative bleeding, which suggested that a platelets count of > 50 × 1000/mm3 is acceptable for endoscopic treatments in patients with liver cirrhosis.
Another major concern is the presence of GOV, as it may increase the rate of bleeding and other complications, especially when the lesion in on or adjacent to GOV. Therefore, it is necessary to comprehensively assess the positional relationship between the lesions and GOV, the risk of variceal bleeding, the risk of GOV injury during the ESD procedure, the risk of infiltration or metastasis of delayed treatment of mucosal lesions, the endoscopist’s experience and so on [27]. In our opinion, if the early cancer or precancerous lesion is far from GOV, and patients are with low risk of variceal bleeding, ESD can be performed first; for patients with high risk of variceal bleeding, ESD should be performed after management of GOV or simultaneously with management of GOV. No consensus has been reached regarding the optimal interval between GOV management and ESD in this situation, we suggest ESD performed within 4 weeks of GOV management. In our study, 3 patients had lesions far from GOV, and 2 of them managed GOV first, and ESD was performed 2 and 4 weeks later, and ESD was immediately performed in the other one patient as only mild esophageal varices was noticed. If the lesion is located overlying or adjacent to GOV, the risk of bleeding will be increased remarkably. If high risk of GOV exists, and the lesion had low risk of infiltration or metastasis, GOV should be performed firstly; for patients with high risk lesion and low risk of variceal bleeding, the lesion should be performed first; for patients with both high risk of lesion and variceal bleeding, they could be managed simultaneously. In our study, one patient had esophageal cancer overlying the esophageal varices, ESD was successfully performed although intraoperative bleeding was encountered. As for the management strategy of GOV, no consensus was reached. Either endoscopic or interventional therapy is acceptable for patients with early cancer of precancerous lesion far from GOV, While some researchers recommend against endoscopic treatment as it may induce submucosal fibrosis which will increase the technical difficulty of subsequent ESD [28,29], therefore transjugular intrahepatic portosystemic shunt (TIPS) or balloon-occluded retrograde transvenous obliteration were used to prevent variceal bleeding [15,30,31,32]. Endoscopic radiofrequency ablation and laparoscopic-endoscopic cooperative surgery have also been reported for management of such patients [33,34]. Zhang et al. reported the endoscopic treatment outcome of 15 cases (had 16 lesions) of upper gastrointestinal early cancer of precancerous lesion with GOV. Among the 16 mucosal lesions, 2 (12.5%) were located overlying the GOV, 6 (37.5%) were located beside the GOV, and 8 (50%) were located far from the GOV. And 5 (33.3%) were untreated for GOV during the ESD perioperative period, 1 (6.7%) was treated for GOV after ESD, 6 were treated for GOV before ESD, 1 (6.7%) was treated for GOV before ESD and during ESD, and 2 (13.3%) were treated for GOV during ESD [27]. In a multicenter study, 134 lesions in 112 patients were treated by endoscopic method, with esophageal varices in 71 procedures. To prevent bleeding, 7 patients underwent a TIPS, 8 had EBL before resection, 15 received vasoactive drugs, and 9 underwent EBL during the resection procedure.
The present study had several limitation. Firstly, this is a single center, retrospective study in a tertiary hospital with relatively small sample size. This may due to the low incidence of such patients. Secondly, ESD in such patients were performed by experienced endoscopist, thus the results may not be directly generalized. Thirdly, no comparison with non-cirrhotic patients was made due to the small sample size. In a word, our preliminary study revealed that ESD is safe and effective for treating upper gastrointestinal early-stage cancer of precancerous lesions in patients with liver cirrhosis. Proper perioperative management of coagulation dysfunction, platelet reduction and low albumin is helpful to gurantee the safety of ESD.
Author Contributions
Conceptualization, Y.T. and J.G.; investigation, J.G.; data curation, R.L., C.L. and L.L.; writing—original draft preparation, Y.T. and Y.Q.; writing—review and editing, Y.T. and J.G. ; supervision, L.D.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding given.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Second Xiangya Hospital of Central South University (protocol code LYF2020129).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the staff from Department of Pathology, the Second Xiangya Hospital of Central South University, who provided precise pathohistological results of the resected lesions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Zhang, X.; Li, M.; Chen, S.; Hu, J.; Guo, Q.; Liu, R.; Zheng, H.; Jin, Z.; Yuan, Y.; Xi, Y.; Hua, B. Endoscopic Screening in Asian Countries Is Associated With Reduced Gastric Cancer Mortality: A Meta-analysis and Systematic Review. Gastroenterology. 2018, 155, 347–354.e9. [Google Scholar] [CrossRef]
- Liu, Q.; Ding, L.; Qiu, X.; Meng, F. Updated evaluation of endoscopic submucosal dissection versus surgery for early gastric cancer: A systematic review and meta-analysis. Int J Surg. 2020, 73, 28–41. [Google Scholar] [CrossRef]
- Bestetti, A.M.; de Moura, D.T.H.; Proença, I.M.; Junior, E.S.D.M.; Ribeiro, I.B.; Sasso, J.G.R.J.; Kum, A.S.T.; Sánchez-Luna, S.A.; Marques Bernardo, W.; de Moura, E.G.H. Endoscopic Resection Versus Surgery in the Treatment of Early Gastric Cancer: A Systematic Review and Meta-Analysis. Front Oncol. 2022, 12, 939244. [Google Scholar] [CrossRef]
- Zheng, H.; Kang, N.; Huang, Y.; Zhao, Y.; Zhang, R. Endoscopic resection versus esophagectomy for early esophageal cancer: a meta-analysis. Transl Cancer Res. 2021, 10, 2653–2662. [Google Scholar] [CrossRef]
- Lu, W.; Li, P.; Wen, W.; Jian, Y. Comparison of Long-Term Survival Between cT1N0 Stage Esophageal Cancer Patients Receiving Endoscopic Dissection and Esophagectomy: A Meta-Analysis. Front Surg. 2022, 9, 917689. [Google Scholar] [CrossRef]
- Tao, M.; Zhou, X.; Hu, M.; Pan, J. Endoscopic submucosal dissection versus endoscopic mucosal resection for patients with early gastric cancer: a meta-analysis. BMJ Open. 2019, 9, e025803. [Google Scholar] [CrossRef]
- Hu, W.; Yu, J.; Yao, N.; Li, X.; Yang, Y.; Wang, L.; Sun, M.; Guo, Y.; Wang, H.; Yan, S.; Li, B. Efficacy and Safety of Four Different Endoscopic Treatments for Early Esophageal Cancer: a Network Meta-analysis. J Gastrointest Surg. 2022, 26, 1097–1108. [Google Scholar] [CrossRef]
- Chinese Society of Hepatology,Chinese Medical Association. [Chinese guidelines on the management of liver cirrhosis]. Zhonghua Gan Zang Bing Za Zhi. 2019, 27, 846–865. [Google Scholar] [CrossRef]
- Ferro, D.; Angelico, F.; Caldwell, S.H.; Violi, F. Bleeding and thrombosis in cirrhotic patients: what really matters? Dig Liver Dis. 2012, 44, 275–9. [Google Scholar] [CrossRef]
- Choe, W.H.; Kim, J.H.; Park, J.H.; Kim, H.U.; Cho, D.H.; Lee, S.P.; Lee, T.Y.; Lee, S.Y.; Sung, I.K.; Park, H.S.; Shim, C.S. Endoscopic Submucosal Dissection of Early Gastric Cancer in Patients with Liver Cirrhosis. Dig Dis Sci. 2018, 63, 466–473. [Google Scholar] [CrossRef]
- Kim, S.H.; Joo, M.K.; Yoo, A.Y.; Kim, S.M.; Kim, W.S.; Lee, B.J.; Park, J.J.; Chun, H.J.; Lee, S.W. Long-term outcome of the endoscopic submucosal dissection of early gastric cancer: A comparison between patients with and without liver cirrhosis. Oncol Lett. 2022, 24, 404. [Google Scholar] [CrossRef]
- Yabuta, T.; Nishihara, A.; Hayashi, Y.; Yamada, T.; Takehara, T. Outcomes of ESD for patients with early gastric cancer and comorbid liver cirrhosis: a propensity score analysis. Surg Endosc. 2015, 29, 1560–6. [Google Scholar] [CrossRef]
- Zhu, L.L.; Liu, L.X.; Wu, J.C.; Gan, T.; Yang, J.L. Endoscopic submucosal tunnel dissection for early esophageal squamous cell carcinoma in patients with cirrhosis: A propensity score analysis. World J Clin Cases. 2022, 10, 11325–11337. [Google Scholar] [CrossRef]
- Simonnot, M.; Deprez, P.H.; Pioche, M.; Albuisson, E.; Wallenhorst, T.; Caillol, F.; Koch, S.; Coron, E.; Archambeaud, I.; Jacques, J.; Basile, P.; Caillo, L.; Degand, T.; Lepilliez, V.; Grandval, P.; Culetto, A.; Vanbiervliet, G.; Camus Duboc, M.; Gronier, O.; Leal, C.; Albouys, J.; Chevaux, J.B.; Barret, M.; Schaefer, M. Endoscopic resection of early esophageal tumors in patients with cirrhosis or portal hypertension: a multicenter observational study. Endoscopy. 2023 Jul 13. [CrossRef]
- Gong, J.; Zhou, B.Y.; Liang, C.B.; Zhou, H.J.; Wang, H.Y.; Tan, Y.Y.; Liu, D.L. Comparison between tunneling and standard endoscopic submucosal dissection for treatment of large esophageal superficial neoplasm. Acta Gastroenterol Belg. 2019, 82, 469–474. [Google Scholar]
- Esaki, M.; Ihara, E.; Gotoda, T. Endoscopic instruments and techniques in endoscopic submucosal dissection for early gastric cancer. Expert Rev Gastroenterol Hepatol. 2021, 15, 1009–1020. [Google Scholar] [CrossRef]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Zullo, A.; Romiti, A.; Tomao, S.; Hassan, C.; Rinaldi, V.; Giustini, M.; Morini, S.; Taggi, F. Gastric cancer prevalence in patients with liver cirrhosis. Eur J Cancer Prev. 2003, 12, 179–82. [Google Scholar] [CrossRef]
- Randi, G.; Altieri, A.; Gallus, S.; Franceschi, S.; Negri, E.; Talamini, R.; La Vecchia, C. History of cirrhosis and risk of digestive tract neoplasms. Ann Oncol. 2005, 16, 1551–5. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, H.T.; Friis, S.; Olsen, J.H.; Thulstrup, A.M.; Mellemkjaer, L.; Linet, M.; Trichopoulos, D.; Vilstrup, H.; Olsen, J. Risk of liver and other types of cancer in patients with cirrhosis: a nationwide cohort study in Denmark. Hepatology. 1998, 28, 921–5. [Google Scholar] [CrossRef] [PubMed]
- Chandan, S.; Deliwala, S.; Khan, S.R.; Ramai, D.; Mohan, B.P.; Bilal, M.; Facciorusso, A.; Kassab, L.L.; Kamal, F.; Dhindsa, B.; Perisetti, A.; Adler, D.G. Advanced Endoscopic Resection Techniques in Cirrhosis-A Systematic Review and Meta-Analysis of Outcomes. Dig Dis Sci. 2022, 67, 4813–4826. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Pagano, N.; Hassan, C.; Cavenati, S.; Rando, G.; Spaggiari, P.; Sharma, P.; Zullo, A. Endoscopic submucosal dissection of gastric neoplastic lesions in patients with liver cirrhosis: a systematic review. J Gastrointestin Liver Dis. 2012, 21, 303–7. [Google Scholar] [PubMed]
- Kwon, Y.L.; Kim, E.S.; Lee, K.I.; Kim, Y.J.; Park, C.W.; Kim, Y.J.; Seo, H.J.; Cho, K.B.; Park, K.S.; Jang, B.K.; Chung, W.J.; Hwang, J.S. Endoscopic treatments of gastric mucosal lesions are not riskier in patients with chronic renal failure or liver cirrhosis. Surg Endosc. 2011, 25, 1994–9. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Hassan, C.; Bruzzese, V. Comment to “Bleeding and thrombosis in cirrhotic patients: what really matters? ”. Dig Liver Dis. 2012, 44, 1049. [Google Scholar] [CrossRef]
- Kawaguchi, C.; Takahashi, Y.; Hanesaka, Y.; Yoshioka, A. The in vitro analysis of the coagulation mechanism of activated factor VII using thrombelastogram. Thromb Haemost. 2002, 88, 768–72. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, Y.D.; Chai, N.L.; Yao, Y.; Gao, F.; Liu, B.; He, Z.D.; Bai, L.; Huang, X.; Gao, C.; Linghu, E.Q.; Li, L.Y. Endoscopic submucosal dissection for early cancers or precancerous lesions of the upper GI tract in cirrhotic patients with esophagogastric varices: 10-year experience from a large tertiary center in China. Gastrointest Endosc. 2023, 97, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Sawaguchi, M.; Jin, M.; Matsuhashi, T.; Ohba, R.; Hatakeyama, N.; Koizumi, S.; Onochi, K.; Yamada, Y.; Kanazawa, N.; Kimura, Y.; Tawaraya, S.; Watanabe, N.; Suzuki, Y.; Mashima, H.; Ohnishi, H. The feasibility of endoscopic submucosal dissection for superficial esophageal cancer in patients with cirrhosis (with video). Gastrointest Endosc. 2014, 79, 681–5. [Google Scholar] [CrossRef]
- Jovani, M.; Anderloni, A.; Carrara, S.; Loriga, A.; Ciscato, C.; Ferrara, E.C.; Repici, A. Circumferential endoscopic submucosal dissection of a squamous cell carcinoma in a cirrhotic patient with esophageal varices. Gastrointest Endosc. 2015, 82, 963–4, discussion 964. [Google Scholar] [CrossRef]
- Masui, Y.; Ohno, K.; Itai, R.; Kurokami, T.; Endo, S. Successful endoscopic submucosal dissection of early gastric cancer located on gastric varices after treatment with balloon-occluded retrograde transvenous obliteration. Clin J Gastroenterol. 2021, 14, 1550–1554. [Google Scholar] [CrossRef]
- Xu, Z.G.; Zhao, Y.B.; Yu, J.; Bai, J.Y.; Liu, E.; Tang, B.; Yang, S.M. Novel endoscopic treatment strategy for early esophageal cancer in cirrhotic patients with esophageal varices. Oncol Lett. 2019, 18, 2560–2567. [Google Scholar] [CrossRef]
- von Renteln, D.; Riecken, B.; Muehleisen, H.; Caca, K. Transjugular intrahepatic portosystemic shunt and endoscopic submucosal dissection for treatment of early gastric cancer in a cirrhotic patient. Endoscopy. 2008, 40 Suppl 2, E32–3. [Google Scholar] [CrossRef]
- Wang, W.L.; Chang, I.W.; Chen, C.C.; Chang, C.Y.; Mo, L.R.; Lin, J.T.; Wang, H.P.; Lee, C.T. A case series on the use of circumferential radiofrequency ablation for early esophageal squamous neoplasias in patients with esophageal varices. Gastrointest Endosc. 2017, 85, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Namikawa, T.; Iwabu, J.; Munekage, M.; Uemura, S.; Maeda, H.; Kitagawa, H.; Nakayama, T.; Fukuhara, H.; Inoue, K.; Al-Sheikh, M.; Jaiswal, N.; Kobayashi, M.; Hanazaki, K. Laparoscopic-endoscopic cooperative surgery for early gastric cancer with gastroesophageal varices. Asian J Endosc Surg. 2020, 13, 539–543. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Endoscopic submucosal dissection (ESD) for superficial esophageal cancer. A, endoscopic image showing esophageal varices at the lower esophagus. B, endoscopic image showing a 0-IIb lesion at the lower esophagus. C, narrow band image of the lesion. D, narrow band image and magnifying endoscopy revealed that intraepithelial papillary capillary loop of type B1 and B2. E, marking the margin of the lesion. F, mucosal and submucosal excision at the anal side of the lesion. G, the would surface after ESD. H, a fully covered metal stent was inserted after completion of ESD.
Figure 1.
Endoscopic submucosal dissection (ESD) for superficial esophageal cancer. A, endoscopic image showing esophageal varices at the lower esophagus. B, endoscopic image showing a 0-IIb lesion at the lower esophagus. C, narrow band image of the lesion. D, narrow band image and magnifying endoscopy revealed that intraepithelial papillary capillary loop of type B1 and B2. E, marking the margin of the lesion. F, mucosal and submucosal excision at the anal side of the lesion. G, the would surface after ESD. H, a fully covered metal stent was inserted after completion of ESD.
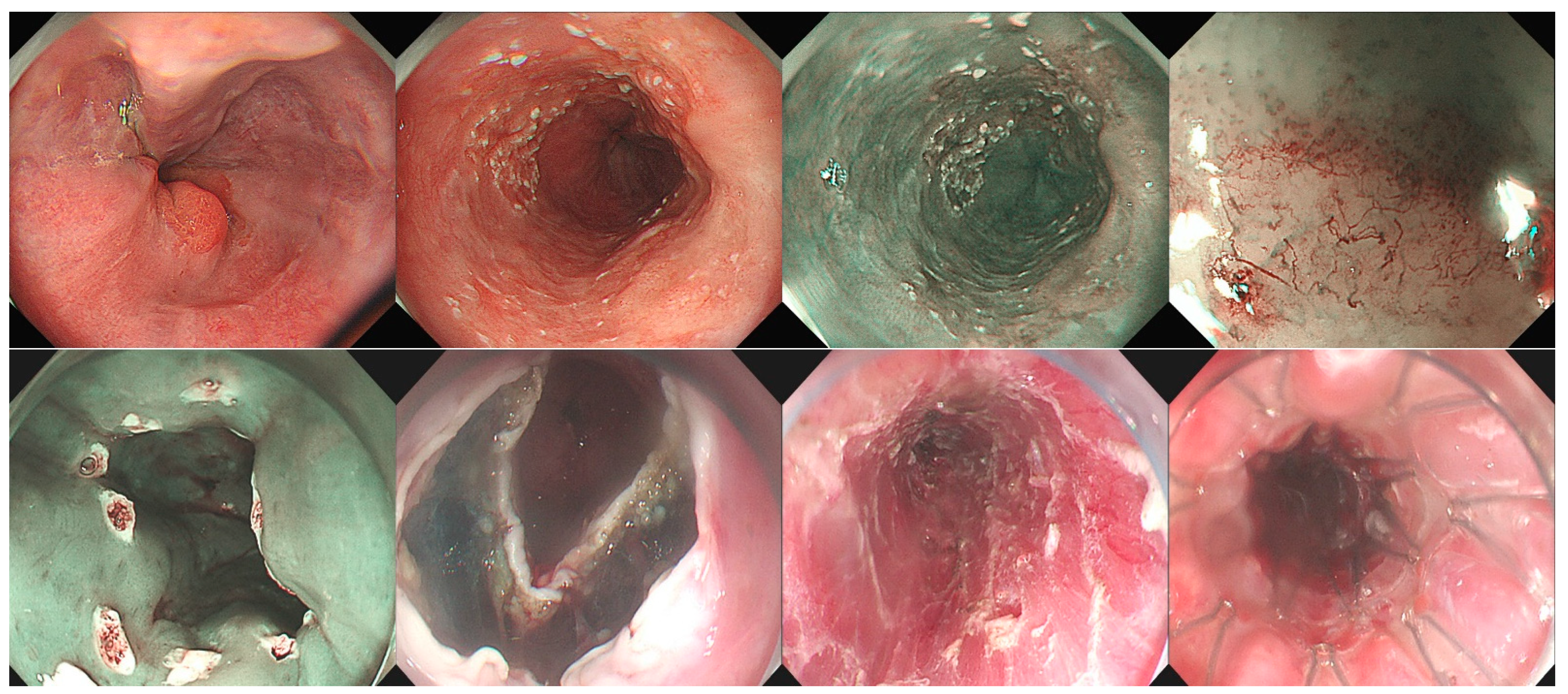
Figure 2.
Endoscopic submucosal dissection (ESD) for early gastric cancer. A, endoscopic image showing esophageal varices. B, endoscopic image showing gastric fundus ulceration owing to endoscopic cyanoacrylate injection for gastric varices. C, a 0-IIa+IIc lesion at the lesser curvature of gastric antrum. D, narrow band image and magnifying endoscopy revealed that the lesion had a demarcation line and irregular microsurface pattern. E, endoscopic ultrasonography revealed that the lesion restricted to the mucosal layer. F, marking the margin of the lesion. G, the would surface after ESD. H, the resected specimen.
Figure 2.
Endoscopic submucosal dissection (ESD) for early gastric cancer. A, endoscopic image showing esophageal varices. B, endoscopic image showing gastric fundus ulceration owing to endoscopic cyanoacrylate injection for gastric varices. C, a 0-IIa+IIc lesion at the lesser curvature of gastric antrum. D, narrow band image and magnifying endoscopy revealed that the lesion had a demarcation line and irregular microsurface pattern. E, endoscopic ultrasonography revealed that the lesion restricted to the mucosal layer. F, marking the margin of the lesion. G, the would surface after ESD. H, the resected specimen.
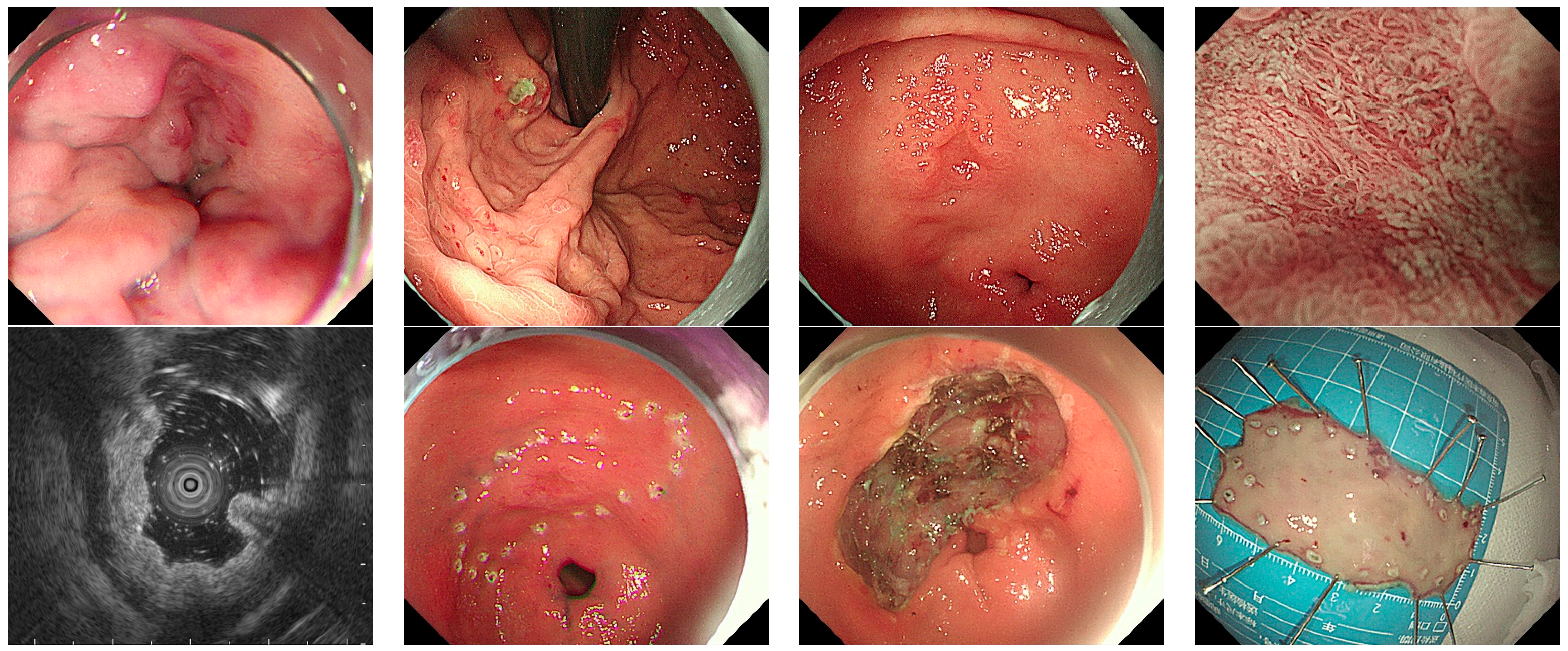

Table 1.
Basic clinical characteristics of the 8 patients.
| Case No. |
Sex | Age (year-old) | Course of liver cirrhosis | Etiology of liver cirrhosis | Presence of GOV | History of GOV therapy | PLT (x10^9/L) | Hb (g/L) | INR | ALB (g/L) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 68 | 1 year | HBV | Yes | No | 72 | 110 | 1.37 | 32.6 |
| 2 | Female | 70 | 5 years | cryptogenic | Yes | 2 times | 46 | 69 | 1.17 | 28.3 |
| 3 | Female | 59 | 1 week | HBV | No | No | 35 | 115 | 1.18 | 36.1 |
| 4 | Male | 52 | 5 years | cryptogenic | Yes | No | 96 | 113 | 1.43 | 27.5 |
| 5 | Male | 64 | 1 year | Alcoholic | Yes | 3 times | 56 | 111 | 1.45 | 32.3 |
| 6 | Female | 56 | 6 months | Budd-Chiari | No | No | 81 | 147 | 0.93 | 44.5 |
| 7 | Female | 64 | 0 | cryptogenic | No | No | 169 | 99 | 1.03 | 32.8 |
| 8 | Male | 43 | 8 months | HCV | No | No | 145 | 158 | 0.98 | 42.2 |
Table 2.
Characteristics and treatment outcome of the 8 patients.
| Case No. |
Location | Size (cm) | Relationship with GOV | Perioperative PLT infusion | Perioperative plasma infusion | Operation time (min) | Pathology | En bloc resection | Intraoperative bleeding | Postoperative complication | Follow up (month) | Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Gastric body | 2x2 | Far from | No | No | 110 | HGIN | Yes | No | No | 45 | No |
| 2 | Gastric antrum | 4x2 | Far from | Yes | Yes | 105 | Tub1 m2 | Yes | Yes | No | 15 | No |
| 3 | Gastric antrum | 4.4x3.5 | NA | Yes | No | 70 | Tub2 m3 | Yes | Yes | No | 3 | No |
| 4 | Esophagus | 6x2 | On | No | Yes | 180 | ESCC sm2 | Yes | Yes | Chest pain Fever |
5 | No |
| 5 | Gastric antrum | 4.5x3.5 | Far from | No | Yes | 230 | Tub1/Tub 2, m3 | No | Yes | No | 15 | No |
| 6 | Gastric antrum | 3x3 | NA | NO | No | 70 | LGIN | Yes | No | No | 18 | No |
| 7 | Gastric body | 2x1.8 | NA | No | No | 45 | Adenoma | Yes | No | No | 15 | No |
| 8 | Gastric antrum | 2.6x2 | NA | No | No | 70 | HGIN | No | No | No | 16 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



