Submitted:
19 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Cannabidiol, is the first cannabis-derived drug approved for the treatment of Lennox-Gastaut syndrome (LGS), Dravet syndrome (DS), and Tuberous Sclerosis Complex (TSC). The current study performed a descriptive analysis followed by a disproportionality analysis of potential adverse events caused by CBD extracted from the database VigiBase®. Further, biological plausibility of the association between CBD and the serotonin 5-HT1A receptor, as possible cause of adverse events was analyzed and discussed. Data were extracted from VigiBase® database using VigiLyze® signal detection and signal management tool. Adverse events in VigiBase® reports were coded using MedDRA, version 19 of Preferred Terms (PTs). Data were uploaded into SPSS software and analyzed via disproportionality analysis. Statistically significant disproportionality signals for CBD were found for “weight decreased” 5.19 (95% CI: 4.54 - 5.70), “hypophagia” 3.68 (95% CI: 3.22 - 5.27), and “insomnia” 1.6 (95% CI: 1.40 - 1.83). Positive IC025 values were found for “weight decreased” (2.2), “hypophagia” (1.3), and “insomnia” (0.5), indicating a surplus of reported cases. CBD’s interactions with 5-HT1A serotonin receptors may offer a potential biological explanation for the occurrence of insomnia in patients. It is noteworthy that the risk profiles mentioned in the prescribing information for CBD as antiepileptic agent by regulatory agencies showed disparities specifically related to the adverse event “insomnia”.
Keywords:
cannabidiol
; cannabis
; adverse reaction
; adverse event
; pharmacovigilance
; serotonin
; 5-HT1A receptor
1. Introduction
Cannabis sativa is a plant containing greater than 100 active cannabinoids, and several of them have been identified and isolated [1]. These cannabinoids have been used for various purposes throughout history, including religious, recreational, and medicinal uses, specifically as anti- inflammatory, antiemetic, anxiolytic, and seizure disorders [2,3]. Among the many cannabinoids present in Cannabis, two of the most abundant and well-known ones are delta-9- tetrahydrocannabinol (THC) and cannabidiol (CBD). THC (delta-9-tetrahydrocannabinol) and CBD (cannabidiol) indeed have the same molecular formula, C21H30O2, but their structures differ slightly, resulting in different pharmacological activities. These structural differences result in variations in how THC and CBD interact with brain receptors (e.g., cannabinoid receptors) and other biological targets, leading to distinct pharmacological activities and effects [4].
Cannabis recreational use is known to cause “high” or intoxicating effects primarily due to THC’s psychotomimetic properties. CBD does not cause THC-like euphoric and psychotomimetic effects, and has garnered increasing attention due to its potential therapeutic benefits. While THC and CBD are both present in Cannabis, THC was generally found in higher concentrations compared to CBD [5]. However, the exact ratios of THC to CBD can vary depending on the specific Cannabis strain or cultivar. These differences in cannabinoid composition contribute to the varying effects and uses of different Cannabis products [6].
Pharmacological activity and therapeutic applications of THC, the active component of Cannabis, have been prominently studied over the years [7,8]. While the exact mechanisms of CBD are not yet fully understood, even if significant progress has been made through randomized clinical trials, animal model studies, and real-world data [9,10,11]. CBD showed to have a weak link with cannabinoid receptors 1 (CB1) and cannabinoid receptor 2 (CB2) [12], but binds to the peroxisome proliferator-activated receptor gamma [13] and has a high affinity for orphan receptors GPR55 [14]. Some of the cannabinoid-mediated effects attributed to CBD may be due to its ability to inhibit endocannabinoid degradation due to the FAAH enzyme, thus increasing anandamide level [15]. CBD has been found to be the most potent and efficacious phytocannabinoid activating transient receptor potential vanilloid (TRPV)2 and, at lower values, also TRPV1 [16]. CBD has the capability to inhibit the reuptake of adenosine, prolonging the activity of this endogenous neurotransmitters [17]. The equilibrative nucleoside transporter type (ENT)-1, regulating the concentration of adenosine, is inhibited by CBD causing indirect agonistic activity of adenosine receptor signaling [18]. CBD is an allosteric modulator at mu and delta opioid receptors [19] and has also inhibitory activity on sodium, calcium, and potassium channels, which is partially explaining its anticonvulsant effects [20]. CBD exhibits agonistic activity on serotonin 5-HT1A receptors. In this regard, it is noteworthy the finding that CBD is a full agonist towards serotonergic 5-HT1A receptor. As well as serotonin does, CBD increases [35S] GTPcS binding at this receptor and reduces cAMP concentration at equivalent levels of receptor occupancy [21]. The [35S] GTPgammaS assay measures the level of G protein activation following agonist occupation [22]. Serotonin is believed to be involved in several cannabis effects, such as relief of anxiety and pain [23] and is of great importance also for the hedonic tone, reinforcement processes [24] and sleep-wake cycle [25]. Furthermore, CBD has been proven to directly activate serotonin 5-HT1A receptors, which are associated with mood regulation, anxiety, and stress responses suggesting that can reduce acute autonomic responses to stress and its delayed emotional consequences by facilitating 5-HT1A receptor-mediated neurotransmission [26].
Use of CBD is generally considered safe, however, its safety profile is not completely defined. List of important risks for CBD licensed as antiepileptic agent includes hepatocellular injury, somnolence and sedation, lethargy, pneumonia, rash hypersensitivity reactions [27]. This information is based on available data obtained with clinical studies which supported requirement of medicinal authorization. Poor data are existing from real world data, even though, with a recent previous study analyzing European database EudraVigilance we suggested that precautions should be adopted for appropriate monitoring of CBD potential adverse effects used as antiepileptic, such as awareness of interactions with other drugs, epilepsy aggravation, and drug effectiveness [28]. Starting from this point of view, in the present study the relationship between CBD safety profile and serotonin involvement in potential adverse reactions has been investigated. In particular, the objectives of the study were to perform a descriptive analysis of spontaneous reports of adverse reactions to CBD licensed as antiepileptic agent in the VigiBase® database followed by a disproportionality analysis of selected adverse events potentially associated with activity at the serotonin 5-HT1A receptor level and finally to investigate on the biological plausibility of the interaction between this receptor and CBD.
2.0. Methods
Data were extracted from the Uppsala Monitoring Centre (UMC) database VigiBase®. VigiBase® holds over 30 million anonymised individual case safety report (ICSRs) of suspected adverse effects related to medicines use (as of January 2023). In this database, the information is recorded in a structured form, its purpose is to provide the evidence from which potential medicine safety hazards (signals) may be detected and communicated. Demographic characteristics (age, sex, area of residence, notifier’s country) and details concerning the reported effect (suspected drugs, concomitant drugs, adverse drug reaction, date of occurrence, and seriousness) are collected in the database [29]. Adverse events in Vigibase® reports are coded using the Medical Dictionary for Regulatory Activities (MedDRA, version 19.0) of Preferred Terms (PTs). PTs of MedDRA are intended to represent a single medical concept, linked with broader Higher-Level Terms (HLT), Higher Level Group Terms, and System Organ Classes (MedDRA Hierarchy, 2023) [30]. All cases linked to CBD administration recorded in Vigibase® up to 15 May 2023 were analyzed.
2.1. Case of interest definition
Hence, we sought a potential pharmacovigilance signal for the use of medical CBD and adverse reactions potentially associated with the serotonin receptor 5HT1A, using the PT terms: weight decreased, insomnia, dizziness, hypophagia, and palpitations.
2.2. Exposure definition
All reports of the term “Cannabidiol” recorded in Vigibase® up to 15 May 2023 were identified using the Vigibase browser Vigilyse®.
2.3. Statistical Analysis
A descriptive analysis was done for adverse reactions potentially linked to CBD use as antiepileptic agent contained in the database VigiBase® until December 2022.
A disproportionality analysis by using VigiBase®, the World Health Organization Pharmacovigilance Database, was performed based on two different measures, the reporting odds ratio (ROR) and the information component (IC). The ROR, as an approximate of the odds ratio (used in case–control studies), used to assess the strength of disproportionality. Reports linked to CBD were compared with all the other ICSR of VigiBase®. A ROR equal to 1 states the absence of signal, conversely, a ROR greater than 1 indicates a signal and the existence of the association. Higher the ROR, stronger is the association. The precision of the approximate ROR is reflected by a 95% confidence interval (95% CI). Consequently, a ROR is statistically significant when the lower bound of its 95% CI is greater than 1 [31,32]. The IC compares observed and expected values for the combination of a given drug and an ADR to yield associations between them. The positivity of the IC reveals the superiority of the number of observed reports over the number of expected reports. IC is a logarithmic measure of the strength of the association between a drug and a single type of adverse reaction [33].
We followed as guide “The Reporting of A Disproportionality analysis for drUg Safety signal detection using spontaneously reported adverse events in Pharmacovigilance (READUS-PV)”. READUS-PV is an international collaborative which aim at developing the first reporting recommendations for studies using disproportionality analyses in databases of spontaneously reported adverse events (https://readus-statement.org).
3.0. Results
3.1 Characteristics of the reports
The reports examined in this study were sent from various countries, with the USA being the most represented, the other countries whose reports we have analyzed are France, Spain, Italy, Canada, Australia, Uruguay and the United Kingdom. From January 2009 to May 15, 2023, VigiBase® collected 12,702 ICSR related to CBD, of which 5466 (43.0%) corresponding to criteria for serious adverse reactions.
A total of 820 ICSRs (6.5% of whole CBD-related ICSRs) correspond to events potentially related to 5-HT1A activation. They mainly originated from USA (754; 92.0%) and mostly from consumers (463 reports; 56.5%). Gender was frequently not reported (524; 63.9%), while in the remaining part there is a substantial balance between men and women (149 Vs 147, respectively). Stratification for age suggests that the age group most affected is represented by adults aging between 18 and 44 years with 57 cases (7%), even if in most of the cases the age of the subject is not reported (685; 83.5%). The most used product was Epidiolex (753 ICSRs, 91.8%), while the other cases were distributed as follows: CBD oil 15 cases (1.8%), unknown CBD formula 47 (5.7%). The most represented diseases for which CBD was employed were Lennox-Gastaut Syndrome (315 reports; 38.4%) and Epilepsy (200 reports; 24.4%; Table 1).
3.2. Disproportionality analysis
Among the selected events, “Weight decreased” was related to the highest ROR values with 5.2 (95% CI 4.5; 5.7), followed by “Hypophagia” 3.7 (3.2; 5.3), and “Insomnia” 1.6 (1.4; 1.8). “Dizziness” and “Palpitations” were related with a negative ROR (0.2 [0.2 – 0.3] and 0.1 [0.1; 0.2], respectively).
IC component results confirmed the ROR ones. Data on IC025, extracted by the VigiBase® database was also reported. They show an IC positive for the adverse reactions “Weight decreased”, “Hypophagia”, and “Insomnia” (Table 2).
3.3. Characteristics of insomnia reports
Among signals of adverse reactions analyzed, only “Insomnia” is not mentioned in other studies nor within the summary of product characteristics (SmPC) of Epidiolex, a medicinal product regularly licensed and based on CBD [34]. Thus, we performed a post hoc analysis only on its related ICSRs (n=221). As already seen for the general data, here too there are not many ICSRs that report the data on age (25; 11.3%), but among those in which it is present, the most represented age group is from 2 to 11 years (8; 3.6%). As for sex, we also find in this case a slightly more representative number for the male than the female (28 vs 25; 12.7% and 11.3%). Regarding the drugs used, the use of Epidiolex (206; 93.2%) stands out (Table 3).
We have reported the indications of use extrapolated from reports on insomnia: the most represented therapeutic indications are Lennox-Gastaut and epilepsy respectively with 73 (33.0%) and 59 (26.7%) reports (Figure 1). In the cases of insomnia found in individual reports, serious cases reported are 48 (21.7%).
4. Discussion
Quantitative analysis of spontaneous adverse drug reaction signaling is a routinary activity in research defining drug safety and reporting odds ratio (ROR) and information component (IC) are among the most common methods used. Results of the present study show that adverse reactions to CBD traceable in the database VigiBase® are mostly reported when people take the licensed drug Epidiolex generally use as antiepileptic agent, while adverse reactions linked to unlicensed CBD oil are reported in a minor percentage. Application of statistical methods reveals that among all adverse events to CBD potentially associated with the serotonin receptor 5HT1A, ROR is increased for “Weight decreased”, “Hypophagia”, “Insomnia”. Both “Weight decreased” and “Hypophagia” are adverse reactions included in the risk management published for CBD used as drug, however, the adverse reactions “Insomnia” has not ever signaled by data available from clinical studies.
ROR indicates the odds of an adverse reaction occurring with a substance or a drug, in comparison to the odds of the same adverse reaction when occurring with all the other substances or drugs in the database [35]. Information component (IC) indicates if a particular association between a substance or a drug and an adverse reaction is signaled more often than it can be expected in the remaining whole adverse reactions in the database. In this case, the value of IC is positive and means that the association event/drug is not expected. When the substance (or drug) and the particular adverse reactions are not dependent, the value of IC is zero [36]. In the present study calculation of ROR for the adverse reaction “Insomnia” reveals that risk linked to its occurrence is moderately higher (1.60; C.I. 1.40-1.83) and IC analysis indicates that it is signaled more often than expected. Insomnia is a sleep disorder defined as chronic dissatisfaction with sleep quantity and/or quality. It is associated with difficulty initiating and/or maintaining sleep, early morning awakening, and unrefreshing sleep [37].
Despite increased use of medicinal cannabis to treat insomnia and other sleep disorders, the evidence supporting therapeutic utility of cannabinoid therapies in sleep disorders is not strong [38]. Positive effects of CBD against insomnia were observed in an old small clinical study, however, more recent clinical research showed that sleep architecture polysomnography was not changed by acute daily administration of 300 mg of CBD [39]. CBD is generally considered a substance causing somnolence instead than insomnia, however, effects of CBD on sleep are not yet fully understood. In clinical studies in which 25/mg/kg CBD in children affected by epilepsy, somnolence and sedation was detected. However, CBD reduces metabolism of concomitant anticonvulsants used, thus sedation observed in these trials could be indirectly caused by its inhibitory effect [40]. Drowsiness was also reported as one of the most common side effects in a Phase 1 trial of CBD in carried out in healthy volunteers, but without any difference compared to placebo and the highest frequency of the effect with the too much higher dose of 6000 mg, while the unit dose as antiepileptic is 100 mg [41]. Furthermore, insomnia related to CBD use could be due to the known CBD activity as a negative allosteric modulator of the CB1 receptor [42], so the possibility exists that CBD could exhibit stimulating or inhibiting properties at different doses.
Biological plausibility of the link between CBD and insomnia has to be found in the mechanism of action of the cannabinoid. As above yet exposed CBD can influence serotonergic system activity, in particular acting on the 5-HT1A receptor. Serotonergic neurons in the brain stem Raphe nuclei are responsible for the initiation and maintenance of slow wave sleep and for the ‘priming’ of rapid eye movement sleep [43]. 5-HT1A autoreceptors play a role in controlling serotonergic tone through a negative feedback inhibition in response to increases in serotonin; thus, the growing autoreceptor desensitization may be the cause for the delayed onset of action of the antidepressants selective serotonin reuptake inhibitors (SSRIs) [44]. The 5-HT1A receptor subtype is a heptahelical G protein coupled receptor associated with inhibitory G proteins (Gi/Go) [45] and widely distributed throughout the CNS in both pre- and postsynaptic sites. It is one of the most abundant and widely expressed in the brain as autoreceptor or heteroreceptor [46], 5-HT1A autoreceptors play a role in controlling serotonergic tone through a negative feedback inhibition in response to increases in serotonin; thus, growing autoreceptor desensitization may be the cause for the delayed onset of action of SSRIs. The expression of 5-HT1A receptor in the limbic system and brain stem nuclei raphe support its role in regulating functions like mood and memory [47,48]. At this regard, it has been hypothesized that 5-HT1A receptor activation modulates anxiety [49] and the response to antidepressant drugs [50].
It has been shown that systemic administration of 8-hydroxy-2-(di-n-propilamino)tetralin (8-OH-DPAT), selective 5-HT1A receptor agonist [51], in doses ranging from 0.010-0.375 mg/kg consistently increases waking, and reduces slow wave sleep and rapid eye movement sleep [52]. Finally, the role played by of serotonin, and in particular by the 5-HT1A receptor, in the regulation of cycle sleep/wakefulness is controversial. It is thought that agonistic activity towards the 5-HT1A receptors could increase waking or sleep depending on the route of administration and the brain region involved [53].
In conclusion, analysis of real-world data from VigiBase® suggests that, in order of risks linked to CBD utilization, insomnia could emerge as potential adverse reaction not signaled by clinical trials and in risk management of licensed drugs containing it. Biological plausibility of causal relationship between between CBD and insomnia can be explained through the knowledge of the mechanism of action of the cannabinoid and its potential influence on serotonergic system activity, by acting on the 5-HT1A receptor. In order to reach definitive or more stable conclusions, better quality of data is needed. It will provide clearer results to be communicated to physicians and consumers using or prescribing CBD for treatment or for well-being. Furthermore, as people who suffer from insomnia with the use of cannabidiol are mostly patients with epilepsy, it is important to verify the external validity of these results to establish the extent to which it is possible to generalize the findings of this study to the general population.
Supplementary Materials
Not applicable.
Author Contributions
“Conceptualization, F.S., F.C., L.M., C.M.; methodology, F.C.; software, F.C., L.M.; validation, F.S., F.C.; formal analysis, F.C,; investigation, L.M., C.M.; resources, F.S.; data curation, F.C., L.M., C.M.; writing—original draft preparation, F.S., F.C., L.M., C.M.;.; writing—review and editing, F.S., F.C., L.M., C.M.;.supervision, F.S..; project administration, F.C.;. All authors have read and agreed to the published version of the manuscript.”.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available from VigiBase upon formal request to the Uppsala Monitoring Centre-WHO Collaborating Centre for International Drug Monitoring.
Acknowledgments
We are grateful to the Uppsala Monitoring Centre(UMC)-World health Organization (WHO) Collaborating Centre for International Drug Monitoring for allowing data access and use. The information comes from a variety of sources, and the probability that the suspected adverse effect is drug-related is not the same in all safety reports. The information does not represent the opinion of the UMC or WHO.
Conflicts of Interest
“The authors declare no conflict of interest.”
References
- Morales P, Hurst DP, Reggio PH. Molecular Targets of the Phytocannabinoids: A Complex Picture. Prog Chem Org Nat Prod. 2017;103:103-131. [CrossRef]
- Rosenberg EC, Tsien RW, Whalley BJ, Devinsky O. Cannabinoids and Epilepsy. Neurotherapeutics. 2015;12(4):747-68. [CrossRef]
- Galaj E, Xi ZX. Possible Receptor Mechanisms Underlying Cannabidiol Effects on Addictive-like Behaviors in Experimental Animals. Int J Mol Sci. 2020;22(1):134. [CrossRef]
- de Almeida DL, Devi LA. Diversity of molecular targets and signaling pathways for CBD. Pharmacol Res Perspect. 2020;8(6):e00682. [CrossRef]
- Freeman TP, Craft S, Wilson J, Stylianou S, ElSohly M, Di Forti M, Lynskey MT. Changes in delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) concentrations in cannabis over time: systematic review and meta-analysis. Addiction. 2021;116(5):1000-1010. [CrossRef] [PubMed]
- Salehi A, Puchalski K, Shokoohinia Y, Zolfaghari B, Asgary S. Differentiating Cannabis Products: Drugs, Food, and Supplements. Front Pharmacol. 2022;13:906038. [CrossRef]
- Costa, B. On the pharmacological properties of Delta9-tetrahydrocannabinol (THC). Chem Biodivers. 2007;4(8):1664-77. [CrossRef] [PubMed]
- Calapai F, Cardia L, Sorbara EE, Navarra M, Gangemi S, Calapai G, Mannucci C. Cannabinoids, Blood-Brain Barrier, and Brain Disposition. Pharmaceutics. 2020;12(3):265. [CrossRef]
- Britch SC, Babalonis S, Walsh SL. Cannabidiol: pharmacology and therapeutic targets. Psychopharmacology (Berl). 2021;238(1):9-28. [CrossRef]
- Mannucci C, Navarra M, Calapai F, Spagnolo EV, Busardò FP, Cas RD, Ippolito FM, Calapai G. Neurological Aspects of Medical Use of Cannabidiol. CNS Neurol Disord Drug Targets. 2017;16(5):541-553. [CrossRef] [PubMed]
- Calapai G, Mannucci C, Chinou I, Cardia L, Calapai F, Sorbara EE, Firenzuoli B, Ricca V, Gensini GF, Firenzuoli F. Preclinical and Clinical Evidence Supporting Use of Cannabidiol in Psychiatry. Evid Based Complement Alternat Med. 2019;2019:2509129. [CrossRef]
- Pertwee, RG. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol. 2008;153(2):199-215. [CrossRef]
- Granja AG, Carrillo-Salinas F, Pagani A, Gómez-Cañas M, Negri R, Navarrete C, Mecha M, Mestre L, Fiebich BL, Cantarero I, Calzado MA, Bellido ML, Fernandez-Ruiz J, Appendino G, Guaza C, Muñoz E. A cannabigerol quinone alleviates neuroinflammation in a chronic model of multiple sclerosis. J Neuroimmune Pharmacol. 2012;7(4):1002-16. [CrossRef] [PubMed]
- Ryberg E, Larsson N, Sjögren S, Hjorth S, Hermansson NO, Leonova J, Elebring T, Nilsson K, Drmota T, Greasley PJ. The orphan receptor GPR55 is a novel cannabinoid receptor. Br J Pharmacol. 2007;152(7):1092-101. [CrossRef]
- De Petrocellis L, Ligresti A, Moriello AS, Allarà M, Bisogno T, Petrosino S, Stott CG, Di Marzo V. Effects of cannabinoids and cannabinoid-enriched Cannabis extracts on TRP channels and endocannabinoid metabolic enzymes. Br J Pharmacol. 2011;163(7):1479-94. [CrossRef]
- De Petrocellis L, Schiano Moriello A, Imperatore R, Cristino L, Starowicz K, Di Marzo V. A re-evaluation of 9-HODE activity at TRPV1 channels in comparison with anandamide: enantioselectivity and effects at other TRP channels and in sensory neurons. Br J Pharmacol. 2012;167(8):1643-51. [CrossRef]
- Pandolfo P, Silveirinha V, dos Santos-Rodrigues A, Venance L, Ledent C, Takahashi RN, Cunha RA, Köfalvi A. Cannabinoids inhibit the synaptic uptake of adenosine and dopamine in the rat and mouse striatum. Eur J Pharmacol. 2011;655(1-3):38-45. [CrossRef] [PubMed]
- Castillo A, Tolón MR, Fernández-Ruiz J, Romero J, Martinez-Orgado J. The neuroprotective effect of cannabidiol in an in vitro model of newborn hypoxic-ischemic brain damage in mice is mediated by CB(2) and adenosine receptors. Neurobiol Dis. 2010;37(2):434-40. [CrossRef] [PubMed]
- Kathmann M, Flau K, Redmer A, Tränkle C, Schlicker E. Cannabidiol is an allosteric modulator at mu- and delta-opioid receptors. Naunyn Schmiedebergs Arch Pharmacol. 2006;372(5):354-61. [CrossRef] [PubMed]
- Xu C, Zhang Y, Gozal D, Carney P. Channelopathy of Dravet Syndrome and Potential Neuroprotective Effects of Cannabidiol. J Cent Nerv Syst Dis. 2021;13:11795735211048045. [CrossRef]
- Russo EB, Burnett A, Hall B, Parker KK. Agonistic properties of cannabidiol at 5-HT1a receptors. Neurochem Res. 2005;30(8):1037-43. [CrossRef] [PubMed]
- Harrison C, Traynor JR. The [35S]GTPgammaS binding assay: approaches and applications in pharmacology. Life Sci. 2003;74(4):489-508. [CrossRef] [PubMed]
- Russo, EB. Clinical endocannabinoid deficiency (CECD): can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions? Neuro Endocrinol Lett. 2008;29(2):192-200. [PubMed]
- Müller CP, Homberg JR. The role of serotonin in drug use and addiction. Behav Brain Res. 2015;277:146-92. [CrossRef] [PubMed]
- Vaseghi S, Arjmandi-Rad S, Nasehi M, Zarrindast MR. Cannabinoids and sleep-wake cycle: The potential role of serotonin. Behav Brain Res. 2021;412:113440. [CrossRef] [PubMed]
- Resstel LB, Tavares RF, Lisboa SF, Joca SR, Corrêa FM, Guimarães FS. 5-HT1A receptors are involved in the cannabidiol-induced attenuation of behavioural and cardiovascular responses to acute restraint stress in rats. Br J Pharmacol. 2009;156(1):181-8. [CrossRef]
- epidyolex-epar-risk-management-plan-summary_en.pdf. Accessed , 2023. https://www.ema.europa.eu/en/documents/rmp-summary/epidyolex-epar-risk-management-plan-summary_en. 15 July.
- Ammendolia I, Mannucci C, Cardia L, Calapai G, Gangemi S, Esposito E, Calapai F. Pharmacovigilance on cannabidiol as an antiepileptic agent. Front Pharmacol. 2023;14:1091978. [CrossRef]
- Lindquist, M. Use of triage strategies in the WHO signal-detection process. Drug Saf. 2007;30(7):635-7. [CrossRef] [PubMed]
- MedDRA Hierarchy | MedDRA. Accessed , 2023. https://www.meddra.org/how-to-use/basics/hierarchy. 15 July.
- Bate A, Evans SJ. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol Drug Saf. 2009; 18(6):427-436.
- Faillie, JL. Case-non-case studies: Principle, methods, bias and interpretation. Therapie. 2019;74(2):225-232. [CrossRef] [PubMed]
- Trillenberg P, Sprenger A, Machner B. Sensitivity and specificity in signal detection with the reporting odds ratio and the information component. Pharmacoepidemiol Drug Saf. 2023;32(8):910-917. [CrossRef] [PubMed]
- https://www.ema.europa.eu/en/documents/product-information/epidyolex-epar-product-information_en.pdf; accessed on 4 august 2023.
- Hauben M, Zhou X. Quantitative methods in pharmacovigilance: focus on signal detection. Drug Saf. 2003;26(3):159-86. [CrossRef] [PubMed]
- Palapra H, Viswam SK, Kalaiselvan V, Undela K. SGLT2 inhibitors associated pancreatitis: signal identification through disproportionality analysis of spontaneous reports and review of case reports. Int J Clin Pharm. 2022;44(6):1425-1433. [CrossRef] [PubMed]
- Blake MJ, Trinder JA, Allen NB. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: Implications for behavioral sleep interventions. Clin Psychol Rev. 2018;63:25-40. [CrossRef] [PubMed]
- Suraev AS, Marshall NS, Vandrey R, McCartney D, Benson MJ, McGregor IS, Grunstein RR, Hoyos CM. Cannabinoid therapies in the management of sleep disorders: A systematic review of preclinical and clinical studies. Sleep Med Rev. 2020;53:101339. [CrossRef] [PubMed]
- Linares IMP, Guimaraes FS, Eckeli A, Crippa ACS, Zuardi AW, Souza JDS, Hallak JE, Crippa JAS. No Acute Effects of Cannabidiol on the Sleep-Wake Cycle of Healthy Subjects: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Front Pharmacol. 2018;9:315. [CrossRef]
- Geffrey AL, Pollack SF, Bruno PL, Thiele EA. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia. 2015;56(8):1246-51. [CrossRef] [PubMed]
- Taylor L, Gidal B, Blakey G, Tayo B, Morrison G. A Phase I, Randomized, Double-Blind, Placebo-Controlled, Single Ascending Dose, Multiple Dose, and Food Effect Trial of the Safety, Tolerability and Pharmacokinetics of Highly Purified Cannabidiol in Healthy Subjects. CNS Drugs. 2018;32(11):1053-1067. Erratum in: CNS Drugs. 2019;33(4):397. PMID: 30374683; PMCID: PMC6223703. [CrossRef]
- Murillo-Rodríguez, E. The role of the CB1 receptor in the regulation of sleep. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(6):1420-7. [CrossRef] [PubMed]
- Jouvet, M. Sleep and serotonin: an unfinished story. Neuropsychopharmacology. 1999;21(2 Suppl):24S-27S. [CrossRef] [PubMed]
- Blier P, Piñeyro G, el Mansari M, Bergeron R, de Montigny C. Role of somatodendritic 5-HT autoreceptors in modulating 5-HT neurotransmission. Ann N Y Acad Sci. 1998;861:204-16. [CrossRef] [PubMed]
- Raymond JR, Mukhin YV, Gettys TW, Garnovskaya MN. The recombinant 5-HT1A receptor: G protein coupling and signalling pathways. Br J Pharmacol. 1999;127(8):1751-64. [CrossRef]
- Pompeiano M, Palacios JM, Mengod G. Distribution and cellular localization of mRNA coding for 5-HT1A receptor in the rat brain: correlation with receptor binding. J Neurosci. 1992;12(2):440-53. [CrossRef]
- Berumen LC, Rodríguez A, Miledi R, García-Alcocer G. Serotonin receptors in hippocampus. ScientificWorldJournal. 2012;2012:823493. [CrossRef]
- Brown JW, Sirlin EA, Benoit AM, Hoffman JM, Darnall RA. Activation of 5-HT1A receptors in medullary raphé disrupts sleep and decreases shivering during cooling in the conscious piglet. Am J Physiol Regul Integr Comp Physiol. 2008;294(3):R884-94. [CrossRef] [PubMed]
- Toth, M. 5-HT1A receptor knockout mouse as a genetic model of anxiety. Eur J Pharmacol. 2003;463(1-3):177-84. [CrossRef] [PubMed]
- Artigas, F. Developments in the field of antidepressants, where do we go now? Eur Neuropsychopharmacol. 2015;25(5):657-70. [CrossRef] [PubMed]
- Meneses A, Hong E. Mechanism of action of 8-OH-DPAT on learning and memory. Pharmacol Biochem Behav. 1994;49(4):1083-6. [CrossRef] [PubMed]
- Bjorvatn B, Fagerland S, Eid T, Ursin R. Sleep/waking effects of a selective 5-HT1A receptor agonist given systemically as well as perfused in the dorsal raphe nucleus in rats. Brain Res. 1997;770(1-2):81-8. [CrossRef] [PubMed]
- Fiske E, Portas CM, Grønli J, Sørensen E, Bjorvatn B, Bjørkum AA, Ursin R. Increased extracellular 5-HT but no change in sleep after perfusion of a 5-HT1A antagonist into the dorsal raphe nucleus of rats. Acta Physiol (Oxf). 2008;193(1):89-97. [CrossRef] [PubMed]
Figure 1.
Therapeutic indications of individual cases of insomnia (N = 221) as suspected adverse reaction to cannabidiol.
Figure 1.
Therapeutic indications of individual cases of insomnia (N = 221) as suspected adverse reaction to cannabidiol.
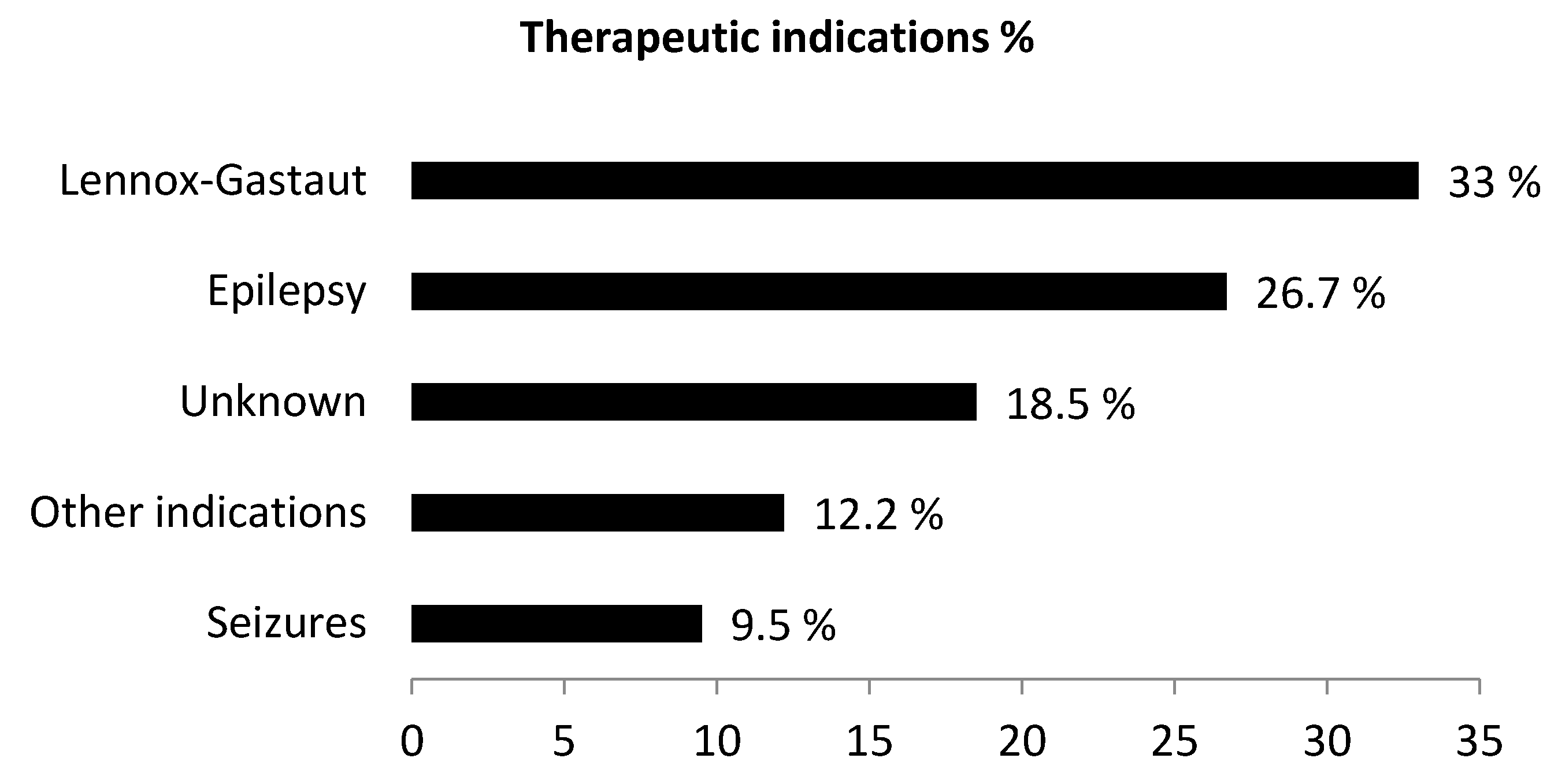

Table 1.
Main characteristics of individual case safety reports (ICSRs) related to cannabidiol (CBD) collected in VigiBase®.
Table 1.
Main characteristics of individual case safety reports (ICSRs) related to cannabidiol (CBD) collected in VigiBase®.
| Main characteristics | N° cases (820) | % |
|---|---|---|
| Patient age | ||
| 28 days-23 months | 1 | 0.1% |
| 2 - 11 years | 23 | 2.8% |
| 12 - 17 years | 23 | 2.8% |
| 18 - 44 years | 57 | 7.0% |
| 45 - 64 years | 18 | 2.2% |
| 65 - 74 years | 6 | 0.7% |
| ≥ 75 years | 6 | 0.7% |
| Unknown | 685 | 83.5% |
| 28 days-23 months | 1 | 0.1% |
| Sex | ||
| Male | 149 | 18.2% |
| Female | 147 | 17.9% |
| Unknown | 524 | 63.9% |
| Countries | ||
| Usa | 754 | 92.0% |
| UK | 18 | 2.2% |
| France | 12 | 1.5% |
| Germany | 8 | 1.0% |
| other countries | 28 | 3.4% |
| Reporter qualification | ||
| Physician | 154 | 18.8% |
| Pharmacist | 22 | 2.7% |
| Other Health Professional | 179 | 21.8% |
| Consumer/Non Health Professional | 463 | 56.5% |
| Unknown | 8 | 1.0% |
| Drug/Product | ||
| Epidiolex | 753 | 91.8% |
| Unknown (Cannabidiol) | 47 | 5.7% |
| CBD oil | 15 | 1.8% |
| Convupidiol (Argentina) | 3 | 0.4% |
| Xannadiol (Uruguay) | 2 | 0.2% |
| Indication | ||
| Epilepsy NOS | 200 | 24.4% |
| Lennox Gastaut Syndrome | 315 | 38.4% |
| Seizures | 40 | 4.9% |
| Parzial seizure | 41 | 5% |
| Idiopatic epilepsy | 34 | 4.1% |
| Tuberous Sclerosis Complex | 11 | 1.3% |
| Product use for unknown indication | 79 | 9.6% |
| Other indications | 100 | 12.2% |
| Serious/non serious adverse reactions | ||
| Yes | 233 | 28.4% |
| No | 587 | 71.6% |
Table 2.
Reporting odds ratio (ROR), information component (IC) and IC025 of individual cases of suspected adverse reactions to cannabidiol (CBD) reported in VigiBase® signaling as suspected adverse reactions “weight decreased”, “hypophagya”, “insomnia”, “dizziness”, “palpitations”.
Table 2.
Reporting odds ratio (ROR), information component (IC) and IC025 of individual cases of suspected adverse reactions to cannabidiol (CBD) reported in VigiBase® signaling as suspected adverse reactions “weight decreased”, “hypophagya”, “insomnia”, “dizziness”, “palpitations”.
| Adverse reaction | N. of cases | ROR (95% CI) |
IC (IC025) |
|---|---|---|---|
| Weight decreased | 456 | 5.19° (4.54 - 5.70) |
2.4* (2.2) |
| Hypophagia | 30 | 3.68° (3.22 - 5.27) |
1.8* (1.3) |
| Insomnia | 221 | 1.60° (1.40 - 1.83) |
0.7* (0.5) |
| Dizziness | 118 | 0.23 (0.20 - 0.27) |
- 2.1 (-2.4) |
| Palpitations | 16 | 0.12 (0.10 - 0.19) |
- 3.1 (-3.9) |
° = statistically significant when the lower bound of 95% CI is greater than 1. * = positivity of the IC reveals the superiority of the number of observed reports over the number of expected reports.
Table 3.
Main characteristics of individual case safety reports (ICSRs) of insomnia related to cannabidiol (CBD) collected in VigiBase®.
Table 3.
Main characteristics of individual case safety reports (ICSRs) of insomnia related to cannabidiol (CBD) collected in VigiBase®.
| Main characteristics | N° cases (221) | % |
|---|---|---|
| Patient age | ||
| 2 - 11 years | 8 | 3.6% |
| 12 - 17 years | 5 | 2.3% |
| 18 - 44 years | 4 | 1.8% |
| 45 - 64 years | 4 | 1.8% |
| 65 - 74 years | 2 | 0.9% |
| ≥ 75 years | 2 | 0.9% |
| Unknown | 196 | 88.7% |
| Sex | ||
| Male | 28 | 12.7% |
| Female | 25 | 11.3% |
| Unknown | 168 | 76.0% |
| Drug/Product | ||
| Epidiolex | 206 | 93.2% |
| Unknown Cannabidiol | 11 | 5.0% |
| CBD oil | 2 | 0.9% |
| Convupidiol (Argentina) | 2 | 0.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



