
Submitted:
27 July 2023
Posted:
15 August 2023
You are already at the latest version
Abstract
Resilience has been defined as one's competence to maintain a mental health state and overall well-being when undergoing grave stress or facing significant adversities. Numerous resili-ence-investigating research tools were developed over the years, with the Connor-Davidson Re-silience Scale (CD-RISC), a self-rated tool presenting valuable psychometric properties, remaining one of the most prominent. We aimed to translate and validate the brief CD-RISC-10 in a convenient sample of 584 nurses in Greece's secondary and tertiary health care system. We conducted a con-firmatory factor analysis and known-groups validity and estimated the reliability of the CD-RISC-10. Our confirmatory factor analysis revealed that the scale had a unifactorial structure since all the model fit indices were very good. Moreover, the reliability of the CD-RISC-10 was very good since Cronbach's alpha was 0.924 and McDonald's omega was 0.925. Therefore, the Greek version of the CD-RISC-10 confirmed the factor structure of the original one and had very good validity and reliability.
Keywords:
CD-RISC
; translation
; Greek
; validation
; resilience
; nurses
1. Introduction
Resilience comprises a psychological construct developed in the last quarter of the 20th century to encompass innate mechanisms and 'individuals’ characteristics that protect people from psychotic disorders [1–5]. It has been defined as a dynamic capacity fostered throughout one’s life course [2, 4] via distinct mechanisms while subjected to numerous determinant factors [2, 4, 5]. Despite being primarily identified as a positive personality trait in children and psychiatric patients [6, 7], nowadays, there is a consensus on the construct of resilience formulating a metatheory depicting and rationalizing the continuous evolution of ‘one’s innate predisposition to adapt and recover from adversities rather quickly that can be either enhanced or diminished under each respective life circumstances [8–11].
In particular, the constructs’ origins run back to the early psychiatric literature that primarily described it as a personality trait with a preventive effect in children under adverse circumstances that lessened their vulnerability [6]. Later on, resilience was recognized as an integral yet regular developmental trait with an interactive nature and the term was attributed to a dynamic character [10]. With the prominence of positive psychology and the consequence of kinship towards strengthening competencies instead of targeting flaws and limitations [12], resilience was acknowledged as the determining factor of one’s well-being regardless of whether a person suffers from a psychiatric disease [12].
Even though there is no concrete definition of resilience, it has been recognized as this multitude of behaviours, thoughts, and actions [13, 14] that enable individuals to retain a sense of coherence under distress, consequently leading them to adopt and manifest efficient coping skills, to maintain their composure under challenging circumstances they perceive as manageable and yet meaningful [15,16,17,18]. Pan-human contextual qualities have also been ascribed to it and thus regarded as the capability related to self-regulation and socially appropriate demeanours within the socio-culture construct of communities [13, 19].
Over the last four decades, research in the field has highlighted that resilience forms a multifaceted quality that, due to its dynamic core, varies significantly over time depending on the concurrent circumstances, one’s age, gender, ethnicity, and cultural background [7, 20–23]. Resilience has been found to correlate positively with physical and mental well-being, self-efficacy, gratitude, and optimism while negatively with depression, post-traumatic stress disorder (PTSD) and generalized anxiety disorder [24,25,26,27,28,29].
A theory developed to elaborate more on this ever-changing nature of resilience was the one by Richardson and colleagues, suggesting that one’s resilience capacity at a time is the sole outcome of his “biopsychospiritual homeostasis” processes- competence of fully adapting his/her body, spirit, and mind in the circumstances he/she is under at this point, despite any stressors, given his determined coping abilities, constructive or not. This outcome which might be positive or negative, can be manifested as a higher homeostasis level, i.e., an opportunity for personal growth, a comeback to his baseline homeostasis levels, a lower homeostasis level, or a problematic state full of dysfunctional coping mechanisms and self-destructive behaviours [7].
It has been suggested that resilient persons come across as more adaptive, especially within social settings that require an essential sense of morale [30], as they appear to be experiencing more positive emotions despite the adverse circumstances and challenges they may face [29]. That is why personality facets such as hope have been found to enhance the sense of self-efficacy, leading individuals to deploy more efficient and effective adaptive behaviours [7]. Furthermore, mutual support within groups has been positively associated with one’s mental health [31], reinforcing coping abilities [31]. Therefore, resilience was recognized as a mental health index measuring one’s coping capacity. Besides recognizing hardiness, a protective factor against developing trauma and PTSD, resilience has been centrefold for health promotion and well-being in recent years [23].
In the early 90s, Wagnild and Young developed the 25-item Resilience Scale [30] to explore resilience in adolescent populations; a research tool deemed suitable for adult resilience assessment as validated via its deployment in numerous studies [32,33,34,35,36,37,38]. The 25-item scale depicted resilience’s five primary components: Equanimity, perseverance, self-reliance, meaningfulness, and existential aloneness [32], while an abridged 14-item scale, with significant psychometric properties translated to numerous languages [12, 36], has been formulated from the original one to encompass stress-related protective factors that result in better-coping outcomes [32]. From the validation processes across different populations, it was suggested that scoring in the Resilience Scale was positively correlated with age due to the construct’s dynamic character, whereas no statistically significant correlation with gender was identified [12]. Many relevant scales have been established, with the Resilience Attitudes and Skills Profile, the Resilience Scale for Adults, and the Brief Resilience Scale [34,35,36,37] being among them.
However, one of the most prominent remains the Connor-Davidson Resilience Scale [39], a brief, 25-item self-rated resilience tool with valuable psychometric properties [39]. The CD-RISC is synthesized by 25 affirmations answered via a 5-item Likert scale where “0” equals to “not true at all” and “4” to “true nearly all of the time”. The basis for rating lies in the frequency with which one experiences what the affirmations describe hence total scoring ranging from 0 to 100, and the highest ones reflecting greater resilience [39]. Its preliminary analyses in differing samples from the general population, psychiatric inpatients, primary healthcare, and clinical trials established reference values for being or not resilient. In particular, for the general population, the exploratory factor analysis resulted in highlighting the constructs of “personal competence, high standards and tenacity”, “trust in one’s instincts, tolerance of negative affect, and strengthening effect of stress”, “positive acceptance of change and secure relationships”, “control”, and “spirituality” [39].
In a recent study among 744 critical care nurses, the factor structure of the CD-RISC abridged version was intended to be established while further validating it by analyzing its construct validity [40]. The factors identified were “personal competence”, “perseverance”, and “leadership”, all portraying successful examples of coping mechanisms adopted by nurses to overcome the stressors of the Intensive Care Unit (ICU) environment, with eigenvalues>1.0 and an explained variance of 59%. In addition, in this study, it was found that CD-RISC can differentiate between nurses that cope well after having experienced a traumatic event and those who do not, noting that those nurses that met the PTSD diagnostic criteria presented as less resilient [40].
Additionally, in a study assessing participants’ levels of resilience while identifying associating personal factors and physical activity behaviours, the interrelation between resilience and physical activity emerged [41]. Through the CD-RISC deployment in a sample of 93 New Zealand ICU nurses, resilience was found to be correlated positively with physical job demanding factors, including occupational physical demands, physical activity level, moderate to vigorous occupational physical activity engagement, and dynamic standing at work, highlighting that resilient nurses present greater tolerance to high physical work stress [42].
The 25-item CD-RISC was applied in a 2020 study exploring social support, resilience, and mental health associations in 1521 Chinese healthcare professionals following the COVID-19 pandemic outbreak [43]. Personnel with less overall experience or lesser crisis management experience appeared less resilient, with significantly lower scores on the scale compared to the more experienced ones in tenacity, strength, and optimism. Resilience, especially in tenacity and strength, was also a predictive factor for novel personnel’s mental health status amid adversities [44]. A corresponding study on 114 healthcare professionals sent to the Hubei area to support the regional health system’s operation identified occupation, education, and mental health training as resilience-determining factors [45]. Doctors, bachelor holders, and those who spent extended time on mental health training appeared more resilient, while resilience positively correlated to active coping and training [45]. In another study among 52 critical care professionals with the 10-item CD-RISC [44], resilience was found to be positively correlated to mental health, all the while casting a mediating role to the three burnout dimensions “emotional exhaustion”, “depersonalization”, and “personal accomplishment”. A mix-methods approach was adopted to estimate healthcare professionals’ distress and resilience status during the COVID-19 pandemic to study crucial resilience metatheory parameters [46].
This study aimed to translate into Greek and validate the psychometric properties of the CD-RISC-10 and investigate the resilience levels among a convenience sample of nurses currently working in the Greek public healthcare system.
2. Materials and Methods
2.1. Sample and data collection
A convenient sample of 584 male and female nurses (response rate 89.3%), recruited from 10 Greek public general hospitals of secondary and tertiary health care system, participated in this cross-sectional study from September to December 2022. The study description was uploaded to the hospitals’ official web page with the invitation to participate, while printed wall announcements were also placed in all hospital departments. Following the participants’ briefing about the research procedures and the voluntary and anonymous nature of their participation throughout all the study stages, all subjects gave their informed consent for inclusion before participating. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Faculty of Nursing, National and Kapodistrian University of Athens (reference number; 417, September 2022).
2.2. Measures
The Connor- Davidson Resilience Scale (CD-RISC-10)
The Greek CD-RISC version consists of 10 affirmations describing different aspects of resilience corresponding to flexibility, self-efficacy, emotion regulation, optimism, and cognitive focus/maintaining attention under stress. Each affirmation is assigned to a 5-item Likert scale ranging from 0 “not true” to 4 “true nearly all time”. Overall score can range from 0 to 40, with higher scores indicating greater resilience. The respondent is asked to provide his/her answer based on his/her experiences over the previous 30 days, whether those affirmations are true for him/her and to what extent.
The license to adapt CD-RISC was granted by its developers following dedicated electronic communication. Translation to Greek was performed following the proposed procedure for intercultural adaptation of self-reference questionnaires [47]. Two independent, experienced researchers fluent in English translated the questionnaire into Greek. Consequently, the two texts were compared question by question until a consensus was reached. The revised text of the resulting Greek version was translated into English by two bilingual researchers who compared their translations for inconsistencies. The final text was compared with the original English scale text to confirm its linguistic accuracy. The cognitive debriefing process involved pre-testing the translated questionnaire in a few nurses to identify linguistic issues and adequate translation alternatives while assessing participants’ comprehension of the questions included. Due to COVID-19 restrictions, an electronic questionnaire was constructed using Google Forms with approximately 10-15 minutes of completion time.
2.3. Data analysis
Mean (), standard deviation (SD), median, minimum value and maximum values are used to describe continuous variables, and numbers (percentages) to describe categorical variables.
We conducted confirmatory factor analysis (CFA) to confirm the unifactorial structure of the Greek version of CD-RISC-10. The scale followed the normal distribution; thus, we used the maximum likelihood estimator. We checked the goodness of fit indices in CFA by measuring the following: chi-square/degree of freedom (x2/df); root mean square error of approximation (RMSEA); goodness of fit index (GFI); adjusted goodness of fit index (AGFI); Tucker–Lewis index (TLI); incremental fit index (IFI); normed fit index (NFI); comparative fit index (CFI). The acceptable value for x2/df is less than 5, for RMSEA is less than 0.10, and for all other indices higher than 0.90 [48,49,50,51]. Additionally, we calculated standardized regression weights between the 10 items and the one factor. We used AMOS version 21 (Amos Development Corporation, 2018) to conduct CFA.
Additionally, we estimated the known-groups validity of the CD-RISC-10. In that case, we assessed the relationship between nurses’ demographic and job characteristics and the total score on CD-RISC-10. We used Pearson’s correlation coefficient to assess the correlation between age and CD-RISC-10 score, Spearman’s correlation coefficient to assess the correlation between experience and CD-RISC-10 score, and independent samples t-test to assess the relationship between gender, marital status, children, job position, and educational level and CD-RISC-10 score. P-values less than 0.05 were considered statistically significant. We used IBM SPSS 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.) to perform the analysis.
Finally, we estimated the reliability of the CD-RISC-10 by calculating the following: Cronbach’s alpha, McDonald’s Omega, corrected item-total correlations, and Cronbach’s alpha when a single item was deleted for the ten items of the CD-RISC-10. Cronbach’s alpha and McDonald’s Omega values higher than 0.7 are considered acceptable [52].
3. Results
Respondents included 584 registered nurses. The mean age was 45.8 years (SD: 6.4), ranging from 23 to 65. Among our sample, 51.7% were females, and 48.3% were males. Most nurses were married (86.7%), and more than half had children (58.6%). Most nurses have been working in internal departments (71.2%). One out of two nurses possessed an MSc/PhD diploma (52.5%). Mean years of work experience were 14.1 (SD: 9.8), ranging from 1 to 31. The demographic and job characteristics of the sample are shown in Table 1.
Descriptive statistics for the CD-RISC-10 are shown in Table 2. The mean score for the CD-RISC-10 was 22.6 (SD: 8.0). The minimum and maximum score was 1 and 40, respectively.
CFA for the CD-RISC-10 is shown in Figure 1. The fit indices of the model were very good: x2/df = 4.662, RMSEA = 0.079, GFI = 0.951, AGFI = 0.905, TLI = 0.955, IFI = 0.972, NFI = 0.965, and CFI = 0.972. Moreover, the standardized regression weights between the 10 items and the one factor ranged from 0.670 to 0.810 (p < 0.001 in all cases). Therefore, the Greek version of the CD-RISC-10 confirmed the factor structure of the original one.
Cronbach’s alpha for the CD-RISC-10 was 0.924, and McDonald’s omega was 0.925 indicating excellent reliability. Similarly, Cronbach’s alpha for the scale decreased if any item was deleted (Table 3). Additionally, corrected item-total correlation coefficients ranged from 0.636 to 0.776 (p-value < 0.001 in all items), indicating very good reliability (Table 3).
Known-groups validity of the CD-RISC-10 is shown in Table 4. We found that nurses with children had higher levels of resilience (p<0.001). In particular, mean CD-RISC-10 score for nurses with children was 23.6 and for those without children was 20.6. Also, we found that higher educational level was associated with resilience since mean CD-RISC-10 score for nurses with PhD/MSc was 23.8 and for those without PhD/MSc was 22.2 (p=0.02). Females’ resilience was higher than males (23.2 vs. 22.1) but this relationship was not statistically significant (p=0.01).
4. Discussion
Our study aimed to translate into Greek the CD-RISC-10 scale while validating its psychometric properties and exploring the levels of resilience among nurses currently working in the Greek public healthcare system. In total, 584 nurses from 10 distinct public hospitals of secondary and tertiary health care, 51.5% of whom were females and 48.3% males, with a mean age of 45.8±6.4 years; corresponding demographic characteristics have been previously recorded for the Greek general population [53]. Most of the nurses in the study were leaving with family/partner/spouce (89.6%) and had children (58.6%), while 3 out of 4 worked in internal departments. Across the study sample, mean work experience was estimated at 14.1±9.8 years, ranging between 1 and 31 total work experience in years.
According to participants’ answers, the affirmations with the highest mean score were “think of myself as a strong person when facing challenges” (M=2.68, SD=0.88), “adapt to change” (M=2.57, S.D.=0.98), “believe I can achieve goals despite obstacles” (M=2.44, SD=0.97) and “under pressure, I stay focused” (M=2.33, SD=0.92). On the contrary, participants score the lowest on the affirmations “see humorous side of things” (M=1.79, SD=1.00), “stress makes me stronger” (M=1.99, SD=1.19), and “not easily discouraged by failure” (M=2.06, SD=0.99). The mean total score on the scale was 22.6 (SD: 8.0), with a minimum and maximum of 1 and 40, respectively, indicating average levels of resilience among the study participants. From the respective scores in the scale’s items could be assumed that the nurses working within the Greek public healthcare system hospitals tend to adapt to adverse circumstances, challenges, and stressors, even though having not fully developed their resilience competencies or adequate coping capacities.
The Confirmatory Factor Analysis resulted in deeming the tool highly reliable as Cronbach’s alpha for the translated scale was estimated at 0.924 and McDonald’s omega at 0.925, while corrected item-total correlation coefficients ranged from 0.636 to 0.776 (p-value < 0.001 in all items). Its sound psychometric properties have been highlighted from the primary scale’s validating studies. Among CD-RISC’s strengths as highly important have as well been acknowledged its potency to explore and depict different levels of resilience across population groups that are characterized by their differentiated degree of resilience, i.e., psychiatric patients and the general population, or adolescents and adults, as well as its unwavering psychometric properties [39,40,41,42,43,44]. Our methods and analysis approach agree with a suggestion that recently emerged in the literature claiming that besides CD-RISC being the most widely applied unidimensional resilience scale, it is important to assess its factor structure, reliability, discriminant, and predictive validity each and every time that the tool will be deployed within a novel context [54].
From the correlations among participants’ demographics and professional characteristics with the CD-RISC-10 score, statistically significant relations emerged between holding a PhD/MSc, having children and resilience. In particular, nurses holding a PhD/MSc appeared to have higher levels of resilience as their score on the CD-RISC-10 scale was 23.8, whereas those without a PhD/MSc scored 22.2 (p=0.02). This finding is consistent with a recent study where resilience was correlated positively with educational level, on-the-job and continuous training [45]. Contrary to previous findings that supported the positive association between work experience and resilience [43, 45], in our study, neither job position (p=0.46) nor work experience (p=0.50) were found to have a statistically significant effect. Furthermore, in our sample, nurses with children presented with higher levels of resilience (p<0.001) as their mean score on the scale were 23.6, while those without children 20.6. Similarly, this finding was also observed in the study by Afshari et al. [59]. One possible explanation for this finding could be that having children and worrying about the self and their children about getting infected with COVID-19 have been among the factors contributing to anxiety and stress in nurses, which may play an important role in reducing nurses’ resilience.
Concerning gender, in our sample, female nurses appeared more resilient than males (23.2 vs. 22.1), a relationship that was not statistically significant (p=0.01). Similar findings over the years have emphasized that despite the differences in scoring in the CD-RISC scales between males and females, gender does not affect one’s levels of resilience, as no statistically significant relations have been identified in corresponding studies (i.e., focusing on adult nurses, adult healthcare professionals) [39,40,41,42,43,44]. Interestingly, a study in healthcare professionals amid the challenges and adversities they faced when combating the COVID-19 pandemic concluded that neither gender nor age impact resilience capacity[55]. Our findings agree with that, as no statistically significant association was found between participants’ age and scoring on the scale.
Notwithstanding, this study is characterized by a few limitations and strengths. The convenience sampling method adopted for this survey might entail potential selection bias. However, the study sample exhibits analogous demographics and gender distribution to the recorded ones for the Greek general population [53], affecting the tool’s psychometric evaluation slightly, if none at all, given women’s predominant role in the nursing profession [56]. Additionally, the source population’s demographic and professional characteristics of the hospitals participating in the study remain unknown, impeding us from comparing the study sample with the source population. A significant strength of the study is that it offers a reliable tool that its use in future research could provide a deeper understanding of factors that determine resilience, especially in heavily burdened professional groups such as nursing personnel.
Nowadays, healthcare professionals significantly struggle as many stressors impact them, apart from their personal lives and their professionals. Occupational ones, including time constraints, scheduling, burdened workloads, spiritual and ethical distress, uncertainty, and a sense of cancellation, trigger negative emotional and behavioural responses to the suffering of patients they care for [42]. Healthcare professionals, especially nurses in closed departments, are predominantly exposed to grave stressors, as indicated by the high prevalence of burnout syndrome [40], a secondary indicator of their challenged mental health and consequently reduced resilience capacity. Given this predicament, additional studies in the field are required to explore their levels of resilience and provide a better understanding of the factors that primarily affect it.
With researchers’ interest being progressively more focused on exploring healthcare professionals coping mechanisms and resilience potential, different studies deploy the CD-RISC to address them, all the while translations and cultural adaptations of validated scales [57], such as CD-RISC, are imperative for the facilitated administration of potent research tools across more populations, to identify as well individuals’ psychosocial deficits and mental health needs [53].To this end, future studies are important to explore the potential role of biological factors (e.g., catecholamines) in determining one’s resilience capacity over and above the implementation of behavioural interventions, such as physical activities and exercise, that preliminary evidence suggests [39].
The importance of investigating healthcare professional’s resilience with a scale as the CD-RISC lies with the scale’s main properties, which, apart from remaining unchanged independently of the scale’s length and cultural adaptations, facilitates the identification of factors that may enhance or hinder it, all the while indicating adequate strategies for improving one’s coping skills [54]. Investigating healthcare professional’s resilience through the CD-RISC in different populations while investigating additional contributing parameters would assist in ascertaining any potentially contributing factors to burnout and adverse outcomes creating a series of implications leading to changing the organizational culture of healthcare organizations and even encourage the adoption of human resource management resilience dedicated policies [58].
5. Conclusions
The Greek version of the CD-RISC-10 confirmed the factor structure of the original one and validated its prominent psychometric properties. The CD-RISC-10 Greek version showed great validity and reliability, a highly suitable tool for investigating the Greek population's resilience capacity. The mean total score on the scale indicates average resilience levels among the study participants. We found that while age and gender do not affect one’s resilience competence, having children and/or a higher educational level (i.e., holding an MSc/PhD degree) do so. Future studies should involve other healthcare professionals as well while focusing on obtaining a robust tool suitable for assessing levels of resilience among professionals in the field and exploring the impact of biological parameters and behavioural interventions, such as sleep patterns, nutritional habits, and physical activity/ exercise participation etc. might pose.
Author Contributions
Conceptualization, Bellali, Th.; Methodology and formal analysis, Galanis, P.; Writing original draft preparation, Psomiadi, M.E.; Writing, review and editing, Karagkounis, C., Psomiadi, M.E., Manomenidis, G, Liamopoulou, E., Bellali, Th. Panayiotou, G., Galanis, P.; Supervision, Bellali, Th., Galanis, P. and Panayiotou, G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Honzik, M.P. Life-span development. Annual Review of Psychology 1984, 35, 309–331. [Google Scholar] [CrossRef] [PubMed]
- Richmond, G.B.; Beardslee, W.R. Research and practical implications for paediatricians. Developmental and Behavioral Pediatrics 1988, 9, 157–163. [Google Scholar]
- Beardslee, W.R. The role of self-understanding in resilient individuals: The development of a perspective. American Journal of Orthopsychiatry 1989, 59, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Psychosocial Resilience and protective mechanisms. American Journal of Orthopsychiatry 1987, 57, 316–331. [Google Scholar] [CrossRef]
- Caplan, G. Loss, stress, and mental health. Community Mental Health Journal 1990, 26, 27–48. [Google Scholar] [CrossRef] [PubMed]
- Earvolino-Ramirez, M. Resilience: A concept analysis. Nursing Forum 2007, 42, 73–82. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. Journal of Clinical Psychology 2002, 58, 307–321. [Google Scholar] [CrossRef]
- Wagnild, G.M. The Resilience Scale User’s Guide for the US English version of The Resilience Scale and The 14-Item Resilience Scale (RS-14). Worden, MT: The Resilience Center, 2009.
- Wagnild, G.M. Resilience and successful ageing: Comparison among low- and high-income older adults. Journal of Gerontological Nursing 2003, 29, 42–49. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Development 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Fletcher, D.; Sarkar, M. Psychological resilience. Eur. Psychol 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Luthar, S. Resilience in development: A synthesis of research across five decades. In: Cicchetti D, Cohen DJ, eds. Developmental psychopathology: risk, disorder, and adaptation. 2 ed. New York: John Wiley & Sons Inc, 2006, 739–95.
- Manyena, S.B. The concept of resilience revisited. Disasters 2006, 30, 434–50. [Google Scholar] [CrossRef]
- Streb, M.; Häller, P.; Michael, T. PTSD in paramedics: resilience and sense of coherence. Behav Cogn Psychother 2014, 42, 452–63. [Google Scholar] [CrossRef]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and the relation with health: a systematic review. J Epidemiol Community Health 2006, 60, 376–81. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the mystery of health: how people manage stress and stay well. Jossey-bass, 1987.
- Antonovsky, H.; Sagy, S. The development of a sense of coherence and its impact on responses to stress situations. J Soc Psychol 1986, 126, 213–26. [Google Scholar] [PubMed]
- Ungar, M. The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. American Journal of Orthopsychiatry 2011, 81, 1–17. [Google Scholar] [CrossRef]
- Garmezy, N. Stress resistant children: the search for protective factors. In: Recent research in developmental psychopathology, book suppl number 4 to J Child Psychol Psych. Oxford: Pergamon Press, 1985.
- Rutter, M. Resilience in the face of adversity: protective factors and resistance to psychiatric disorders. Br J Psych 1985, 147, 598–611. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology. Am Psychologist 2000, 55, 5–14. [Google Scholar] [CrossRef]
- Waysman, M.; Schwarzwald, J.; Solomon, Z. Hardiness: an examination of its relationship with positive and negative long-term changes following trauma. J. Traumatic Stress 2001, 14, 531–54. [Google Scholar] [CrossRef] [PubMed]
- Abiola, T.; Udofia, O. Psychometric assessment of the Wagnild and Young’s resilience scale in Kano, Nigeria. BMC Res Notes 2011, 4, 509. [Google Scholar] [CrossRef]
- Damásio, B.F.; Borsa, J.C.; Da Silva, J.P. 14-item resilience scale (RS-14): Psychometric properties of the Brazilian version. J Nurs Meas 2011, 19, 131–145. [Google Scholar] [CrossRef]
- Baldwin, D.R.; Jackson, D.; Okoh, I.; Cannon, R.L. Resiliency and optimism: An African American senior citizen’s perspective. J Black Psychol 2011, 37, 24–41. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Tugade, M.M.; Waugh, C.E.; Larkin, G.R. What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J Pers Soc Psychol 2003, 84, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Scali, J.; Gandubert, C.; Ritchie, K.; Soulier, M.; Ancelin, M.L.; et al. Measuring resilience in adult women using the 10-items Connor-Davidson Resilience Scale (CD-RISC): Role of trauma exposure and anxiety disorders. PLoS One 2012, 7, e39879. [Google Scholar] [CrossRef] [PubMed]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J Pers Soc Psychol 2004, 86, 320–333. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas 1993, 1, 165–178. [Google Scholar] [PubMed]
- McCann, C.M.; Beddoe, E.; McCormick, K.; Huggard, P.; Kedge, S.; Adamson, C.; et al. Resilience in the health professions: a review of recent literature. Int. J. Well-being 2013, 3, 60–81. [Google Scholar] [CrossRef]
- Ahern, N.R.; Kiehl, E.M.; Sole, M.L.; Byers, J. A review of instruments measuring resilience. Issues Compr Pediatr Nurs 2006, 29, 103–125. [Google Scholar] [CrossRef]
- Losoi, H.; Turunen, S.; Waljas, M.; Helminen, M.; Ohman, J.; Julkunen, J.; Rosti-Otajarvi, E. Psychometric properties of the Finish version of the resilience scale and its short version. Psychology, Community & Health 2013, 2, 1–10. [Google Scholar]
- Wagnild, G.M. The Resilience Scale: User’s guide for the US English version of the Resilience Scale and the 14-item Resilience Scale ver. 3.33. Resilience Center, Montana, USA, 2016.
- Ntountoulaki, E.; Paika, V.; Kotsis, K.; Papaioannou, D.; Andreoulakis, E.; et al. The Greek version of the resilience scale (RS-14): Psychometric properties in three samples and associations with mental illness, suicidality, and quality of life. J Psychol Clin Psychiatry 2017, 7, 00450. [Google Scholar]
- Hurtes, K.P.; Allen, L.R. Measuring resiliency in youth: The resiliency attitudes and skills profile. Therap Recreat J 2001, 35, 333–347. [Google Scholar]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int J Methods Psychiatr Res 2003, 12, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; et al. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Oladipo, S.E.; Idemudia, E.S. Reliability and validity of Wagnild and Young’s resilience scale in a sample of Nigerian youth. J Psychology 2015, 6, 57–65. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Mealer, M.; Schmiege, S.; Meek, P. The Connor-Davidson Resilience Scale in critical care nurses: A psychometric analysis. J Nurs Meas 2016, 24, 28–39. [Google Scholar] [CrossRef]
- Yu, F.; Cavadino, A.; Mackay, L.; Ward, K.; King, A.; Smith, M. Physical activity and personal factors associated with nurse resilience in intensive care units. J Clin Nurs 2020, 29, 3246–3262. [Google Scholar] [CrossRef]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensive Crit Care Nurs 2017. [CrossRef]
- Cai, W.; Lianb, B.; Songa, X.; Houa, T.; Denga, G.; Lib, H. A cross-sectional study on mental health among health care workers during the outbreak of Corona Virus Disease 2019. Asian Journal of Psychiatry 2020, 51, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Arrogante, O. Mediator effect of resilience between burnout and health in nursing staff. Enferm. Clin 2014, 24, 283–289. [Google Scholar] [CrossRef]
- Mealer, M.; Jones, J.; Newman, J.; McFann, K.K.; Rothbaum, B.; Moss, M. The presence of resilience is associated with healthier psychological profile in intensive care unit (ICU) nurses: results of a national survey. Int. J. Nurs. Stud. 2012, 49, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, A.; Abegglen, S.; Berger-Estilita, J.; et al. Distress and resilience of healthcare professionals during the COVID-19 pandemic (DARVID): Study protocol for a mixed-methods research project. BMJ Open 2020, 10, e039832. [Google Scholar] [CrossRef]
- Beaton, D.; Bombardier, C.; Guillemin, F.; et al. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2020, 25, 3186–91. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Homburg, C. Applications of structural equation modeling in marketing and consumer research: A review. International Journal of Research in Marketing 1996, 13, 139–161. [Google Scholar] [CrossRef]
- Brown, T. Confirmatory Factor Analysis for Applied Research. 2nd ed. New York: The Guilford Press, 2015. New York.
- Hu, L.; Bentler, PM. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Yusoff, M.S.B.; Arifin, W.N.; Hadie, S.N.H. ABC of Questionnaire Development and Validation for Survey Research. Education in Medicine Journal 2021, 13, 97–108. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 572–572. [Google Scholar] [CrossRef] [PubMed]
- Hellenic Statistical Authority. (2021). Population-Housing Census. [Internet]. Available at : https://www.statistics.gr/en/2021-census-pop-hous. 2021.
- Förster, C.; Duchek, S.; Geithner, S.; et al. Developing an integrated framework of healthcare leaders’ resilience. Rev Manag Sci 2023, 17, 1765–1788. [Google Scholar] [CrossRef]
- Lin, J.; Ren, Y.H.; Gan, H.J.; Chen, Y.; Huang, Y.F.; You, X.M. Factors associated with resilience among non-local medical workers sent to Wuhan, China during the COVID-19 outbreak. BMC Psychiatry 2020, 20, 417–423. [Google Scholar] [CrossRef]
- Zurlo, M.C.; Vallone, F.; Smith, A.P. Work-family conflict and psychophysical health conditions of nurses: Gender differences and moderating variables. Jpn J Nurs Sci. 2020, 7, e12324. [Google Scholar] [CrossRef]
- Bellali, T.; Minasidou, E.; Galanis, P.; Karagkounis, C.; Liamopoulou, P.; & Manomenidis, G.; & Manomenidis, G. Psychometric properties of the Bergen Work Addiction Scale in a Greek sample of health professionals. Health Psychology Report 2022. [CrossRef]
- Beaton, D.; Bombardier, C.; Guillemin, F.; et al. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2020, 25, 3186–91. [Google Scholar] [CrossRef] [PubMed]
- Afshari, D.; Nourollahi-darabad, M.; Chinisaz, N. Demographic predictors of resilience among nurses during the COVID-19 pandemic. Work 2021, 68, 297–303. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Confirmatory factor analysis for the CD-RISC-10.
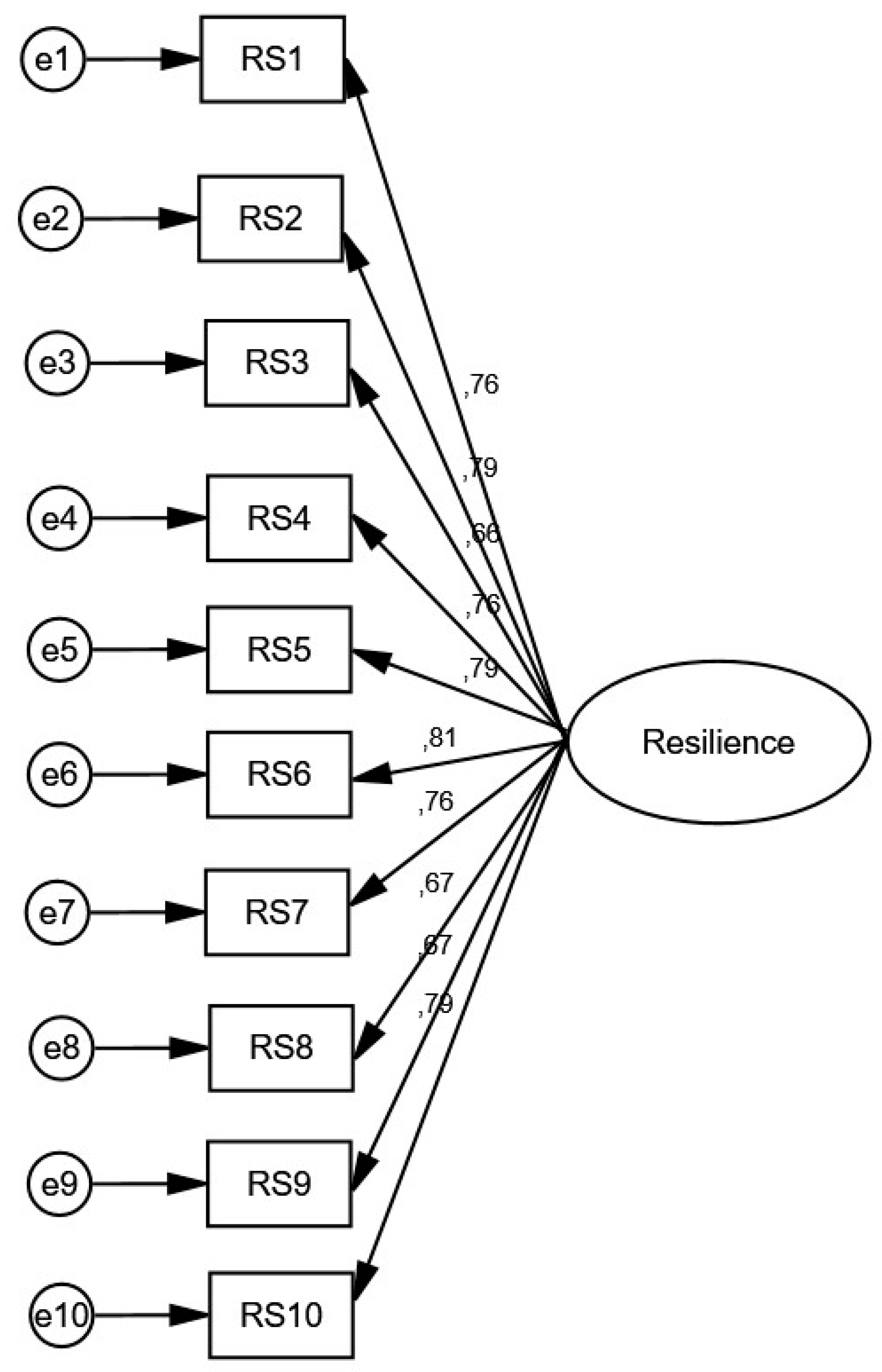

Table 1.
Demographic and job characteristics of the sample
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Males | 282 | 48.3* |
| Females | 301 | 51.5* |
| Age | 45.8a | 6.4b |
| Habitational status | ||
| Leaving alone | 78 | 13.4 |
| Leaving with Family/Partner/Spouce | 506 | 86.6 |
| Children | ||
| No | 157 | 19.5* |
| Yes | 424 | 58.6* |
| Job Position | ||
| Internal departments | 447 | 76.5 |
| ICU | 137 | 22.5 |
| MSc/PhD | ||
| No | 277 | 47.4 |
| Yes | 307 | 52.6 |
| Clinical experience | 14.1a | 9.8b |
a mean. b standard deviation. * The deviation from the sum to 100% is caused by missing values
Table 2.
Descriptive statistics for the CD-RISC-10.
| CD-RISC-10 items | Mean | Standard Deviation | Median | Minimum Value | Maximum Value |
|---|---|---|---|---|---|
| Adapt to change | 2.57 | 0.98 | 3 | 0 | 4 |
| Deal with whatever comes my way | 2.29 | 1.00 | 2 | 0 | 4 |
| See humorous side of things | 1.79 | 1.24 | 2 | 0 | 4 |
| Stress makes me stronger | 1.99 | 1.19 | 2 | 0 | 4 |
| Bounce back after illness or injury | 2.25 | 1.15 | 2 | 0 | 4 |
| Believe I can achieve goals despite obstacles | 2.44 | 0.97 | 2 | 0 | 4 |
| Under pressure, I stay focused | 2.33 | 0.92 | 2 | 0 | 4 |
| Not easily discouraged by failure | 2.06 | 0.99 | 2 | 0 | 4 |
| Think of myself as a strong person when facing challenges | 2.68 | 0.88 | 0.88 | 0 | 4 |
| Able to handle unpleasant feelings | 2.24 | 0.97 | 2 | 0 | 4 |
Table 3.
Cronbach’s alpha when a single item was deleted and corrected item-total correlation coefficient.
Table 3.
Cronbach’s alpha when a single item was deleted and corrected item-total correlation coefficient.
| CD-RISC-10 | Cronbach’s alpha when a single item was deleted | Corrected item-total correlation coefficient |
|---|---|---|
| Adapt to change | 0.915 | 0.728 |
| Deal with whatever comes my way | 0.914 | 0.755 |
| See humorous side of things | 0.922 | 0.636 |
| Stress makes me stronger | 0.915 | 0.734 |
| Bounce back after illness or injury | 0.913 | 0.759 |
| Believe I can achieve goals despite obstacles | 0.913 | 0.776 |
| Under pressure, I stay focused | 0.916 | 0.721 |
| Not easily discouraged by failure | 0.920 | 0.637 |
| Think of myself as a strong person when facing challenges | 0.920 | 0.637 |
| Able to handle unpleasant feelings | 0.913 | 0.758 |
Table 4.
Known-groups validity of the CD-RISC-10.
| Characteristics | Mean CD-RISC-10 score | Standard deviation | P-value |
|---|---|---|---|
| Gender | 0.11a | ||
| Males | 22.1 | 7.9 | |
| Females | 23.2 | 8.1 | |
| Age | 0.03b | 0.50b | |
| Marital status | 0.44a | ||
| Singles/divorced/widows | 24.0 | 8.1 | |
| Married | 23.0 | 7.8 | |
| Children | <0.001a | ||
| No | 20.6 | 7.4 | |
| Yes | 23.6 | 8.0 | |
| Job Position | 0.46 | ||
| Internal departments | 22.5 | 7.9 | |
| ICU | 23.1 | 8.2 | |
| PhD/MSc | 0.02a | ||
| No | 22.2 | 8.2 | |
| Yes | 23.8 | 7.5 | |
| Clinical experience | 0.03c | 0.50c |
a independent samples t-test. b Pearson’s correlation coefficient. c Spearman’s correlation coefficient
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



