Submitted:
13 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
Manifestation of cystic hygroma in adulthood is very rare. In this study, we reported a rare case of Cervical Cystic Hygroma in Adults. We report 20 years old male with a diagnosis of left-side neck cystic Hygroma and discuss the presentation, diagnosis, and clinical, radiological, and operative aspects of it.
Keywords:
cystic hygroma
; adult
; neck cyst
; Iran
1. Introduction
Lymphatic malformation (Cystic Hygroma or lymphangioma) occurs as a result of sequestration or obstruction of developing lymph vessels in approximately 1 in 12,000 births (1).
Although the lesion can occur anywhere, the most common sites are in the posterior triangle of the neck, axilla, groin, and mediastinum (2).
The prevalence of this complication in adulthood is very rare. Adult presentation is related to congenital or acquired delay in lymphoid proliferation after trauma or previous respiratory infections (3).
causes of Cystic Hygroma in Adults include genetic and inherited conditions, developmental abnormalities, and environmental factors (4).
Symptoms and Presentation consist of swelling and cystic growths, Impact on adjacent organs and structures, and Potential pain or discomfort experienced (5).
Diagnosis of it based on medical history and physical examination, Imaging diagnostic tests (ultrasound, CT Scan, MRI.), Biopsy, or fluid analysis (6).
Treatment Options has surgical intervention and removal, Medications or injections for symptom management or physical therapy or rehabilitation post-surgery (7).
The rarity of cystic hygroma in adults has caused problems in its diagnosis and management and few studies have reported cystic hygroma in adults. In This study we report 20 years old male with a diagnosis of left-side neck cystic Hygroma.
2. Case Presentation
A 20-year-old male came to the Surgery ward of Golestan Hospital of Ahwaz (southwest of Iran) with a complaint of painless swelling on the right side of his neck for 5 years.
The patient was asymptomatic 5 years back after which he noticed a swelling in the neck; which has since gradually increased in size. The patient does not experience any difficulty swallowing or breathing. He didn’t tell any history of trauma or upper respiratory tract infection reported.
During the examination, a significant swelling was observed on the right side of the neck, measuring 100*30 mm. The surface of the swelling was soft and lobulated and non-tender. It was also fluctuant and extended into the right posterior triangle of the neck and right supraclavicular area (Figure 1).
The spiral chest CT scan with and without contrast was normal but in the spiral with and without contrast Neck CT Scan was a multi-lobulated hypodense area at supraclavicular regions measuring about 82*42 mm Suggestive of cystic hygroma. This is shown in Figure 2.
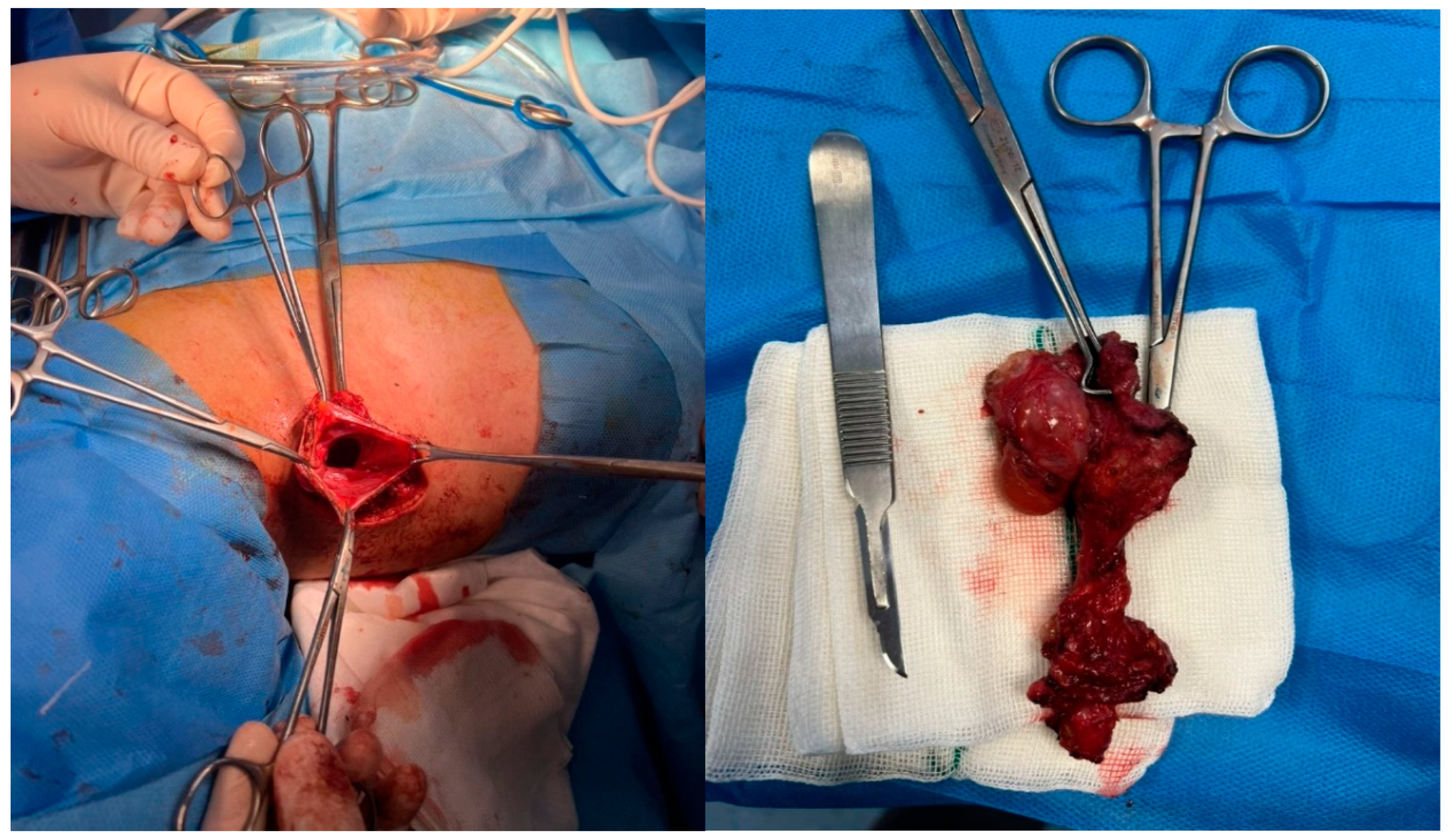
The patient underwent radical cyst resection (Figure 3). Because the cyst extended under the right clavicle (from the anterior view) to the posterior triangle of the neck, a classic cervical incision (posterior of the sternocleidomastoid muscle) was performed. The cyst was adherent to the surrounding tissues and the right internal jugular vein, that was released. The vessels and nerves of that area were saved. We used talcum powder to prevent recurrence.
3. Discussion
Manifestation of cystic hygroma in adulthood is very rare and its cause is controversial, but it is probably due to delayed proliferation of congenital lymphatic malformation, trauma, and upper respiratory tract infection (8).
A neck swelling that is painless, gradually increasing in size, asymptomatic, and without any compression symptoms is similar to the cases reported by Gow et al. (8), Kalsotra et al (9), and Nasr et al (10).
Cystic hygroma could be classified into septated (multiloculated) or nonseptated single cavity (monoloculated) types in our case it was multiloculate that similar to results of Nasr et al [9]. In multiloculated cystic hygromas, Surgery might be the most suitable choice but keeping surgical complications at a minimum is necessary.
Magnetic resonance imaging (MRI), computed tomography (CT), and ultrasonography (US) are all helpful in the diagnosis of a cystic neck mass. The MRI provides detailed images of soft tissues and can also reveal the association between the lesion and underlying structures. Contrast can be utilized to distinguish between hemangiomas and lymphangiomas. CT Scan has a risk of radiation exposure, and it can be difficult to distinguish it from surrounding tissue with similar properties. The use of contrast can help to improve visualization of the cyst wall and its relation to nearby blood vessels. The US study is the least invasive option and can effectively display the relationship between the cyst and the surrounding structures.
The patient underwent a CT scan and ultrasonography of the neck which revealed swelling in the right posterior triangle and right supraclavicular area. According to Morley SE (11), Karakas O (12), and Nasr et al, it is important to evaluate neck cystic hygroma using a combination of neck CT scan, ultrasonography (USG), and Magnetic Resonant Imaging (MRI).
There are various treatment options for this condition, such as surgery (recommended), percutaneous drainage, sclerotherapy, laser therapy, and radiofrequency ablation (10).
We performed a complete surgical excision in our case, as it is the most effective treatment for adult cystic Hygroma that’s similar to Nasr (10), Piłkowski et al (13),
Managing Cystic Hygroma can be challenging due to its tendency to spread locally and reoccur after surgery. However, studies have shown that recurrence out of complete excision of the cystic hygroma 81% and if only a portion of the lymphatic malformation is removed, there is a much higher recurrence rate of 88%.
Morbidity is related to cosmetic disfigurement and involvement of critical structures (nerves, blood vessels, lymphatics, and the airway).
Considering that the rate of recurrence is between 5 and 50%, we used talcum powder to prevent recurrence during the operation and evaluated the patient every six months in terms of recurrence symptoms.
4. Conclusion
Cystic hygromas are a rare occurrence in adults. They are typically asymptomatic, rarely complicated, and can be mistaken for a cystic neck mass. This study shows that surgical resection is a safe and effective treatment of cystic hygroma in adults. Surgery is a safe and efficient way to treat medical conditions, with minimal risk of complications during the procedure. we used talcum powder to prevent recurrence and evaluated the patient every six months.
Funding
No Funding
Acknowledgement
We thank for patient for her consent to publish the case report. The authors would like to give a special thank you to the colleagues at Golestan Hospital, Joundishapour faculty of Medical Sciences, for his guidance and encouragement.
Conflicts of Interest
The authors declared no conflict of interest
References
- Levy AT, Berghella V, Al-Kouatly HB. Outcome of 45, X fetuses with cystic hygroma: A systematic review. American Journal of Medical Genetics Part A. 2021 Jan;185(1):26-32. [CrossRef]
- Noia G, Maltese PE, Zampino G, D'Errico M, Cammalleri V, Convertini P, Marceddu G, Mueller M, Guerri G, Bertelli M. Cystic hygroma: A preliminary genetic study and a short review from the literature. Lymphatic research and biology. 2019 Feb 1;17(1):30-9. [CrossRef]
- McInerney NJ, O’Keeffe N, Nae A, Morariu J, Timon C. Cystic hygroma in adults: a single-centre experience and review of the literature. Irish Journal of Medical Science (1971-). 2023 Jan 16:1-5. [CrossRef]
- Varshney A, Gangavatiker R. Recurrent cystic hygroma in adult: A case report. Indian Journal of Case Reports. 2021 Jun 28:241-3. [CrossRef]
- Jayabal P. A case of cystic hygroma in adults and its management. Annals of Indian Academy of Otorhinolaryngology Head and Neck Surgery¦ Volume. 2021 Jan;5(1):30.
- Kadam SS, Kadam T. Cystic hygroma in a young adult: A case report and recent management. Tumor Discov. 2022 Aug 30;1(2):151. [CrossRef]
- Malik ZU, Hashmi JS, Khan T, Mahmood K, Amer K, Farani TM, Kazmi SA. Adult onset unilocular cystic hygroma in posterior triangle neck: an unusual patient with detailed review of literature. Pakistan Journal of Medical and Health Sciences. 2021;15(4):676-80.
- Gow L, Gulati R, Khan A, Mihaimeed F. Adult-onset cystic hygroma: a case report and review of management. Grand rounds. 2011 Mar 1;11(1):5-11. [CrossRef]
- Kalsotra P, Prusty A, Gupta A, Manhas M. Cervical cystic hygroma in an Adult.
- Nasr B. Abdulhakim Al Tamimi, Mohmmed Issa, Ali Amri, Saeed Al Bahlooli, Anwar Al_Jounaeed, Ahmed Ramadan, Abdulkarim Saleh, Abdulfattah Al Domini. Cystic Hygroma of the Neck in Adult Patient. Journal of Surgery and Research. 2021;4:778-83. [CrossRef]
- Morley SE, Ramesar KC, Macleod DA. Cystic hygroma in an adult: a case report. Journal of the Royal College of Surgeons of Edinburgh. 1999 Feb 1;44(1):57-8.
- Karakas O, Karakas E, Boyaci FN, Yildizhan M, Demir S, Saglam MA, Cullu N. Cervicomediastinal giant cystic hygroma: a case report. Journal of Clinical Medicine Research. 2013 Feb;5(1):61.
- Piłkowski M, Komorski J, Nienartowicz J, Nelke K. Cervical Cystic Hygroma in an Older Adult–a case study. Polski Przegląd Otorynolaryngologiczny. 2020 Dec 16;10(2):54-8.
Figure 1.
Male 20 years adult with Cystic Hygroma.

Figure 2.
Sagittal and Coronal view of the Neck CT Scan.
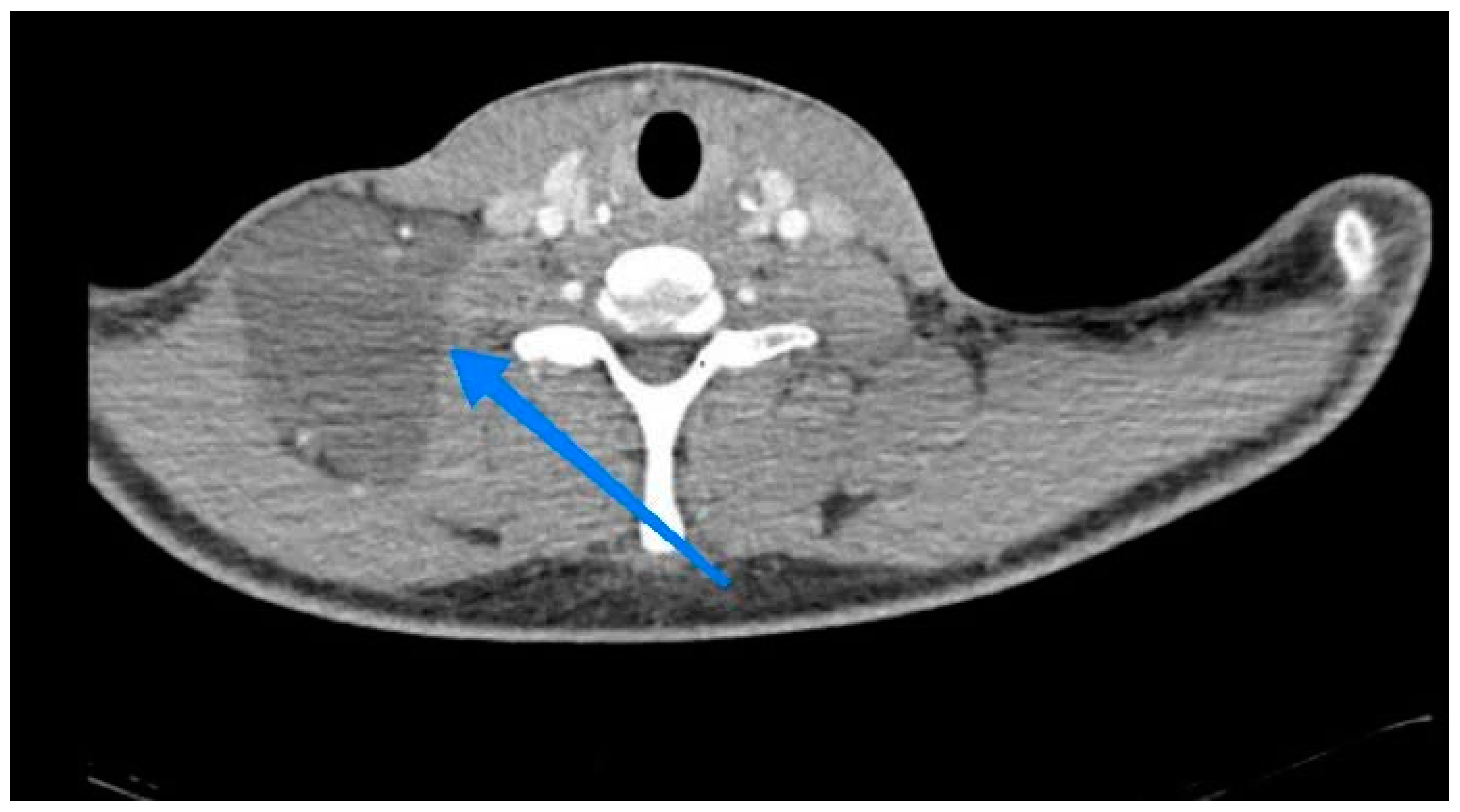
Figure 3.
Inoperative finding lobulated cystic lesion and clean field post cyst excision.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



