
Submitted:
08 August 2023
Posted:
10 August 2023
You are already at the latest version
Abstract
Chlorhexidine digluconate (CHX) has shown the ability to significantly reduce inflammation and marginal bone loss (MBL) at 1-year follow-up but limited data exists regarding its long-term efficacy in peri implant stability. The objective was to compare the long-term effects of a placebo gel (16 patients in Group A) or a 0.20% CHX gel (15 patients in Group B) used at each previous surgical and prosthetic stage. Follow-ups were conducted in 2022, investigating by biological, radiological, clinical, mechanical evaluation the long-term effects. Data were statistically analyzed. The research achieved a 96.7% implant success rate over five years, but 41.9% of patients didn't attend annual oral hygiene check-ups. The average MBL was 1.04 ± 0.39 mm, with no significant differences between the two groups. Notably, patients who attended regular periodontal check-ups experienced significantly less MBL than those who didn't (p <0.05). At five years, the effects of CHX were reduced, with both groups showing moderate bone loss. The results suggest early disinfection could enhance both short and long-term outcomes. In fact, patient with initial minor MBL preserve this advantage also at 5 years of follow-up. Additionally, the data underscore the importance of annual check-ups in early detection and management of biological and mechanical complications.
Keywords:
Chlorhexidine Gel
; marginal bone loss
; Peri-implantitis
; implant survival rate
; implant decontamination
; dental implant complication.
1. Introduction
Dental implants, widely recognized as a trustworthy and predictable avenue for the restoration of missing teeth, largely owe their success to the process of osseointegration, which fosters implant integration with the patient's newly formed bone. According to worldwide literature, the survival rate of implants over a span of 5 years is approximately 90-98%, while it is about 89-95% over 10 years [1,2,3,4]
However, despite its widespread use and reliability, dental implant treatment is not devoid of complications. Early issues may include the failure of osseointegration, postoperative infections, or a lack of primary stability. More protracted concerns encompass marginal bone loss (MBL), peri-implantitis, and implant overload [5,6,7,8,9].
The research community has given considerable attention to MBL, given its critical role in maintaining both the functional and aesthetic outcomes of implant treatment [10,11]. Historically, during the first year of implant loading, some degree of peri-implant bone loss is frequently observed, which typically diminishes in subsequent years. Albrektsson et al. in 1986 [11] cited MBL as one of the primary criteria in assessing implant success rate, defining MBL up to 1 mm within the first year of implant loading and an average annual MBL of 0.2 mm during the follow-up period as success criteria [11]. Various potential contributing factors have been discussed, including implant configuration, the implant neck region, surface treatment, surgical trauma, the platform switching technique, the quantity of peri-implant soft tissue, implant placement tech-nique, residual crestal bone, and microgap at the junction of the implant and abutment. This has allowed a reduction over the years of the MBL but without a total elimination. [8,12,13,14] The microgap has been implicated as a principal site for bacterial colonization, and thereby a significant contributor to MBL [15,16,17,18]. This minuscule space, usually lying between 10 and 135 μm, is the subject of ongoing research efforts aimed at reducing its size and improving the implant-abutment connection [15,17,18,19,20,21]. Even though the use of more advanced connection types has allowed some reduction in the microgap size, no existing connection type has yet succeeded in completely eliminating this area of potential bacterial ingress during long-term clinical use [16,17]. The existing microgap could cause micromotions and bacterial penetration, leading to a peri-implant inflammatory reaction and subsequent bone loss. [15,16,17]. A perpetual infiltrate of inflammatory cells at the fixture-abutment border has been observed in animal studies, suggesting a defensive response of the host to bacterial invasion [18]. In an effort to reduce bacterial load during the surgical and postsurgical stages, rigid protocols have been established, often involving the use of local antiseptics such as chlorhexidine (CHX). Renowned for its plaque inhibitory capabilities and broad-spectrum antimicrobial activity, CHX is a critical adjunct in current clinical practices, including oral and implant surgery. However, its benefits are often constrained by its short-term application [19,22]. In our previous study it was investigated the efficacy of CHX gel, used in strict protocol in all surgical and prosthetic phases of component connection and disconnection, yielded encouraging results [23]. Specifically, it was an in vivo randomized and controlled patient study that compared two groups. The test group used chlorhexidine during all phases, while the control group used a placebo. The results showed that the use of CHX led to a reduction in short-term (12-month) peri-implant bone resorption after implant placement, demonstrating that a strict disinfection protocol of the microgap zone was effective in maintaining bone [23]. Subsequently, in a second study by D'ercole et al. in 2020 on the same patients, microbiological and immunohistochemical investigations were performed, demonstrating a reduction in inflammatory response and bacterial load in patients treated with CHX [24].
Given the demonstrated short-term efficacy of CHX in reducing bacterial load and MBL, the objective of this experimental study was to monitor the long-term outcomes of the same patient group and analyze peri-implant bone stability after more than 5 years. The null hypothesis was that there would be no difference in MBL after five years of follow-up between the use of CHX and placebo gel during the clinical and prosthetic phases. The primary objective was to evaluate MBL at 5 years of follow-up.
The secondary objectives were to:
- correlate the MBL described in the first study [23] and evaluate its trend over time.
- analyze biological complications at 5 years of follow-up.
Additionally, mechanical complications were assessed to provide a more comprehensive analysis, unrelated to biological aspects, but offering a broader perspective on the overall health of dental implants at the 5-year of follow-up.
2. Materials and Methods
2.1. Study design and sample
The study represents a second part of a prospective, randomized, controlled, double-blind clinical trial designed according to the Helsinki Declaration protocol. The allocation ratio was 1:1. The study was approved on 23/07/2015 by the Interinstitutional Ethical Committee of the University of Chieti-Pescara, Chieti, Italy; committee report n. 14. All patients provided written informed consent for treatment and enrollment in the study. The study was registered on clinicaltrials.gov with registration number NCT03431766. The second part of the study involved a long-term follow-up of the same patients. Therefore, data related to these patients were monitored over time and analyzed.
The study adhered to the CONSORT statement for improving the quality of RCTs.
Inclusion and exclusion criteria were previously detailed [23]. A brief resume of material and methods section starting from the begin of the study.
The study incorporated participants aged 18-75 with good overall and oral health, in need of single crown implant-supported restorations, and with sufficient healing time and cortical bone thickness. Adequate dimensions of attached gingiva or keratinized tissue were also required. However, those with poor oral hygiene, active periodontal disease, insufficient bone thickness, or who had undergone bone augmentation procedures were not included. Additionally, patients with immediate loading protocols, uncontrolled diabetes, immune disorders, or those who smoked or had bruxism, were also excluded.
Thirty-four patients (age range 29-75 years; mean age 52.28) with no significant medical history, 14 females and 20 males, all non-smokers, were recruited as candidates for single implant placement and prosthetic rehabilitation. Patients were enrolled from December 2015 to March 2017 and were treated at the Medical, Oral and Biotechnological Sciences Outpatient Clinic of the "G. d'Annunzio" University of Chieti-Pescara, Italy. Patients were randomly divided into group A (control) (placebo gel (Placebo, Polifarma Wellness Srl, Rome, Italy)) and group B (test) (CHX gel (Plak-Gel; Polifarma Wellness Srl, Rome, Italy)) using computer-generated random numbers, centralized with sealed opaque envelopes provided in sequence by the study consultant. Patients were informed of all study procedures but blinded to the different gels used in the study.
2.2. Sample size and randomization
The MBL was used to estimate the number of patients to be randomized. Following the publication by Annibali et al.2012 [25], a sample size of 15 patients per group was calculated to have a minimum difference in MBL between the two groups of -0.55 mm at follow-up with an expected standard deviation of 0.5 mm. The value of α was determined to be 0.05, while the test power was 0.80. The Pass 3 software and the two-sample T-test with equal variance were used for the calculation. The number of patients were increased by 20% in order to offset patient loss at follow-up that could invalidate the test. Eighteen patients were then selected for each group.
2.3. Surgical and prosthetic treatment
During the initial evaluation, all subjects underwent clinical and radiographic examinations before scheduling their surgical procedures. Throughout all stages, a gel containing 0.20% CHX in Group B (Plak-Gel; Polifarma Wellness Srl, Rome, Italy) or in Group A a placebo gel (Placebo, Polifarma Wellness Srl, Rome, Italy) was applied inside the connection. The gels were indistinguishable in packaging, color, and odor. The identity of the gels was only disclosed after data collection by the gel-preparer. Prior to the procedure, patients rinsed their mouths with a 0.2% chlorhexidine digluconate solution for 2 minutes to decrease bacterial presence. All patients received a 2 g/day antibiotic therapy for 6 days (Augmentin; Glaxo-Smithkline Beecham, Brentford, UK) along with postoperative instructions. Implant insertions (Cortex classic, Cortex, Shalomi, Israel) were carried out by two qualified operators at T0. A healing abutment was positioned at 8 weeks (T1), followed by the placement of a temporary acrylic restoration at week 16 (T2). A single crown implant supported cemented restoration was realized in porcelain-fused-to-metal and inserted 18-20 weeks post-implant insertion (T3). The first radiological examination was performed at 12 months of follow up (T4). The long-term follow-up period was set at 5 years (T5), during which patients were encouraged to attend regular check-ups and oral hygiene sessions. In 2022, all patients were invited for a follow-up visit that included periapical X-ray evaluations of marginal bone loss, full mouth plaque and bleeding scores, as well as recording any mechanical complications and/or failures as better explain in “patients analysis section.
2.4. Patients analysis
Implant success was assessed based on the clinical and radiographic criteria established by Papaspyridakos et al. 2012 [26]. Data were collected in patient-specific Clinical Record Forms (CRFs). Peri-implant and gingival indices, including Full Mouth Plaque Score (FMPS) and Full Mouth Bleeding Score (FMBS), were recorded at every stage of the study. As thoroughly explained [23], radiographs and clinical records were consistently taken throughout the study. To compare radiographic changes in the marginal peri-implant bone, an analogical intraoral radiograph was taken, processed on digital software for scientific evaluations with an accuracy of less than 0.1 mm and the mean value between the mesial and distal region was used for analysis.
Customized commercially available Rinn film holders were employed for each subject to achieve a highly reproducible and accurate image. Radiographs were repeated at each time point, and follow-up analyses were also recorded at the 5-year mark (T5). In each radiograph, the distances from the fixture's apex to the mesial and distal crestal bone levels at the first bone-implant contact were measured. Additionally, the length and diameter of the implants were gauged to ensure accurate measurement, even if the implant appeared slightly angled on the radiograph. Based on these measurements, a computerized calibration was executed, and linear measurements of Marginal Bone Loss (MBL) were determined using ImageJ 1.48 (Bethesda, MD).
At follow up visit one single examiner recorded and analyzed the following information:
- -
- Periapical X-ray
- -
- FMPS and FMBS
- -
- Frequency of annual follow-up visit
Moreover any mechanical complications were recorded to provide a more comprehensive overview of the peri-implant health of the treated patients.
2.5. Statistical analysis
Statistical tests were conducted using Excel (Microsoft, Redmond, WA, USA), and GraphPad 8 software (San Diego, California USA). The statistical tests to be used were predetermined by the study protocol. Patients were included in the statistical evaluation, and data were presented with means and standard deviations (SD). Analysis of variance (Student's t-test) was used to assess differences between groups, at 5 different time points considered in the study. Significance was set at p=0.05.
3. Results
40 patients were initially screened for inclusion and exclusion criteria. 34 patients were enrolled for single implant-supported restoration. Six patients were rejected for not meeting the inclusion criteria. Furthermore, two patients were excluded after randomization due to poor oral hygiene at the surgery appointment. 32 patients were enrolled and studied for a single implant restoration in the previous study. Out of the 32 patients, 31 were included in the evaluation performed at 5 years of follow-up. Thus, 1 patient were excluded because he moved far away from the clinic.
The remaining 31 patients belongs to: 16 patients in Group A (placebo gel control group), and 15 patients in Group B (chlorhexidine gel).
Intraoral photo a T4 and T5 of the same case presented at 12 months of follow-up [23] was shown in Figure 1.
Among the analyzed patients, only 1 implant failure was recorded (belonging to Group A), demonstrating a total success rate of 96.7% at 5 years. At 12 months, the success rate was 100%. The patient complained of pain and mobility during the T5 follow-up visit. At first, prosthetic screw loosening was suspected. During the appointment, however, the implant was removed while removing the restoration. Except for the patient who had implant failure, all other restorations were in good general health. No patient reported pain, paresthesia, or other biological complications related to implant placement. Data regarding enrolled patients were shown on Table 1.
Of the controlled patients, 18 were presented for follow-up visits and oral hygiene sessions over the years. The remaining 13 unfortunately did not undergo maintenance sessions and follow-up visits. That is, 41.9% of patients were out of control by the dentist. At T5 Periodontal indices were collected for all patients and then subjected to rigorous periodontal hygiene control. The periodontal indices recorded had an overall mean value of less than 25%. However, by dividing the various groups, different scores were obtained. No statistically significant difference was found between Group A and B. On the contrary, a statistically significant difference (p <0.05) was found between the group receiving hygiene maintenance and the group that did not, as shown in Table 1.
All performed radiographs allowed monitoring of bone resorption over the 5 years. A global bone loss of 1.04 ± 0.39 mm was recorded. However, different analyses have been proposed to understand the trend over the years. The MBLs were recorded and divided by group membership as shown in Table 2 and Figure 2 and Figure 3, with no statistically significant differences observed between the groups. Figure 4 showed different MBL into the two groups during the different stages from T0 to T5. A statistically significant difference was detected when it was compared patients under annually periodontal control and patient that did not undergo to annually control visit and professional oral hygiene.
In addition, several mechanical complications were recorded over time (loosening of the screw, chipping of the ceramic or fracture, decementation of the crown). Specifically, 7 crowns (22.5%) have shown screw loosening over the years, despite being tightened according to the protocol suggested by the company. In 5 cases, the unscrewing occurred multiple times (16.1%). Other minor complications recorded were crown decementation over the years (3 cases, 9.6%), no case of ceramic coating fracture, 2 cases of chipping (6.4% of cases). In a single case, a caries was recorded on the mesial element of the implant restoration, in a patient who had never presented for annual hygiene maintenance sessions during the years. Rx was shown in Figure 5. No major mechanical complications (abutment or implant fracture) were recorded.
4. Discussion
The aim of the present study was to demonstrate the potential efficacy of chlorhexidine in maintaining single implant-supported rehabilitations. However, the data showed no statistically significant difference between the test group and the control group corcerning the primary objective. Therefore, the null hypothesis is accepted, suggesting that CHX has no influence on MBL after five years of follow-up. However, the secondary objectives yielded intriguing results with statistically significant differences, as explained below.
The patient group was previously evaluated after 1 year of loading, where a 100% survival rate was reported. Among the patients who returned for a follow-up, only one implant was removed due to failure, demonstrating a total success rate of 96.7% at 5 years. The overall 5-year outcome is consistent with studies on other implant systems [27,28,29]. For instance, Doornewaard et al. reported a 5-year survival rate of 97.3%, independent of the implant surface [29].
However, data analysis has revealed interesting differences in the 5-year follow-up controls of the various patients. Firstly, global MBL demonstrated minimal bone resorption in both groups, with a global bone loss of 1.04 ± 0.39 mm mm recorded. It is known that this data is strongly influenced by numerous factors such as implant design, the patient, clinical procedures, and the design of the implant neck [8]. However, some bone loss is expected during the first year of function due to remodeling and adaptation [8,11,23]. Other authors have evaluated the course of bone resorption in different groups [30,31,32]. For example, Zumstein et al. in 2019 assessed the MBL trend in a specific implant morphology in patients treated with or without GBR procedures [30]. The results showed no statistically significant differences between the groups, with a global MBL of 0.7 ± 0.7 mm after 1 year and 0.8 ± 0.6 mm after 5 years, in line with the results presented here. However, different factors influenced bone remodeling in Zumstein et al.'s 2019 study, including age, gender, implant position, biotype, implant diameter, implant length, indication, surgical/loading protocol, and ISQ at prosthesis delivery [31]. The data presented here has shown that the use of chlorhexidine did not affect MBL at 5 years. However, at 12 months, the same patients showed statistically significant differences in terms of MBL [23]. Specifically, at T4 (12-month follow-up), patients treated with CHX showed an MBL of 0.68 ± 0.15 mm compared to 0.94 ± 0.34 mm in the control group. In the same patients, MBL of 0.91 ± 0.33 mm (CHX) and 1.16 ± 0.42 mm (control) were present at 5-year follow-up. No statistically significant difference was present between the two groups at 5 years, but an advantage in terms of MBL was retained in the CHX group at 5-year follow-up. Trend analysis confirmed the maintenance of this advantage in all patients treated with CHX. Zumstein et al. in 2019 analyzed MBL among different factors, confirming that the trend of MBL remains unchanged from 1 to 5 years depending on the analyzed criteria. Age, implant position, and gingival biotype showed statistically significant MBL differences. The groups that showed an advantage at 1 year retained the same at 5-year follow-up [31]. Similarly, patients treated with CHX maintained an advantage in terms of MBL even at 5 years. These data demonstrate how early risk factor control, including decontamination of the connection with CHX, allows for more effective maintenance and less bone remodeling over time.
The effects of CHX have also been extensively investigated in the surgical treatment of peri-implantitis [19,22]. However, its benefits are limited due to its short-term application. Some studies have shown that CHX can successfully kill bacteria in biofilms grown on titanium surfaces [21,33,34]. However, CHX seems to be only modestly effective in removing the biofilm [35]. It shows a limited killing effect related to time exposure. Therefore, the application of CHX in all early stages allowed for the control of bacterial contamination, showing reduced MBL up to 12 months [23]. In another study by D'ercole et al. (2020) on the same patients, microbiological and immunohistochemical investigations demonstrated a reduction in inflammatory response and bacterial load in patients treated with CHX [24]. At 5 years of follow-up, the effect had disappeared, but the advantage in terms of MBL was still maintained.
MBL was also evaluated by dividing patients into those under strict periodontal control (at least 1 annual visit) and those out of control. In this sense, statistically significant differences emerged between the two groups, where the latter showed a statistically higher MBL. Among the risk factors for implant failure, hygienic maintenance and control visits still represent a challenge. On the other hand, an incorrect use of periodontal hygiene aids can alter the surface roughness of titanium, increasing bacterial proliferation. Therefore, not only proper patient maintenance but also correct techniques and instrumentation are necessary to manage the follow-up of implant patients [36]. Some studies have shown that patients with periodontitis had lower implant survival rates and higher incidence of complications after implant restoration [37,38]. The rates of peri-implantitis in patients with periodontitis are higher than those in healthy individuals [39,40]. It is essential to emphasize that the importance of recalls and follow-up appointments to ensure oral health has been widely demonstrated, even in patients with special needs. In these patients, those under periodontal control can maintain a higher level of oral health, ensuring a more favorable prognosis [41]. However, other studies proposed that under the condition of strictly controlled periodontitis, the implant survival rate could also be at a high level [42,43,44,45]. Patients with poor periodontal hygiene control not only showed a worsening of MBL but also a higher presence of gingival indices and other complications compared to patients under strict control. The recorded periodontal indices (plaque index and bleeding index) had an overall mean value of less than 25%. However, a statistically significant difference (p <0.05) was found between the group receiving hygiene maintenance and the group that did not. Different data emerge in the literature on this topic. Some studies show implant loss rates higher than 15% in untreated periodontitis patients. On the other hand, comparable survival rates have been demonstrated in patients with periodontitis under strict periodontal control [31]. This data demonstrates that despite the decontamination of the connection made with CHX, poor hygiene control promoted worsening in terms of gingival indices and MBL over time, nullifying any beneficial effects of the initial CHX treatment.
It is important to bear in mind that in addition to controlling biological complications (gingival indices, MBL, and survival rate), hygiene control also helps to control mechanical complications and the onset of any additional problems. Among the patients with poor hygiene control, one had secondary caries beneath an old restoration on a tooth adjacent to the implant. Among the mechanical complications (22.5%), loosening was experienced over the years, despite being tightened according to the protocol suggested by the company. Screw loosening is a commonly observed implant complication [46,47,48]. Jemt et al. reported that screw loosening occurred in 27.3% of 107 single-implant restorations placed in more than 90 patients [47]. For 5 years, Kreissl et al. observed partially edentulous patients who had undergone implant treatment and reported screw loosening in 6.7% of cases [48]. Cho et al. observed 213 dental implant patients over a period of 3 to 7 years and reported that screw loosening occurred in 10.3% of single-implant restoration cases and 12.1% of multiple implant restorations [49]. Screw loosening was observed in 7.2% of the implants, typically occurring once (77.7%), followed by twice (14.4%) and more than twice (7.9%). Most cases occurred within six months of loading (50.4%). Data varies depending on implant diameter and restoration type (screw-retained or cement-retained) [46]. In our patients, 22.5% presented screw loosening, with 16.1% experiencing multiple loosening episodes. These data confirm that abutment loosening remains the primary mechanical complication in cement-retained restorations. Ceramic chipping was present in 6.4% of cases, and crown decementation in 9.6%, indicating a lower incidence than decementation. Overall, the data demonstrate good survival of single implant-supported restorations, with minor bone loss demonstrated between 1 and 5 years of follow-up, particularly when associated with good periodontal hygiene control. Similar results were found in previous clinical studies of two-piece dental implants with a horizontal offset, which showed only minor changes over time and bone levels close to the implant shoulder [46]. However, bone loss in the present study was within the regular range for this type of implant, mostly occurring within the first year after loading, especially in the group that did not receive CHX treatment.
5. Conclusions
At 5 years of follow-up, CHX has certainly lost its effect, as both groups experienced moderate bone loss. It is known from the initial published study that patients treated with CHX during all surgical and prosthetic phases had reduced MBL at 12 months. The same patients also showed a reduced MBL at 5 years in absolute terms. It is therefore possible to hypothesize that better short-term management has beneficial effects even at 5 years of follow-up. For this reason, it could be interesting to conduct further studies to evaluate a method for administering CHX over an extended period, using hydrogels as molecules to deliver CHX in the peri-implant zone [50]. De Cremer et al. in 2017 in vitro provide a proof of concept of the sustained release of chlorhexidine through the Ti/SiO2 material thereby preventing and eradicating biofilm formation on the surface of the dental implant. These types of investigations should be expanded to better understand the potential of sustained release of CHX.
Finally, in patients with poor periodontal hygiene control, MBL and periodontal indices are statistically worse. Periodontal hygiene control remains a fundamental aspect in the management of implant patients as a tool to intercept biological and mechanical problems with the implants or adjacent teeth.
Author Contributions
Conceptualization, G.M. and B.S.; methodology, G.D’A., E.M.; software, G.D’A. G.T.; validation, B.S, L.M.; formal analysis, R.S., G.T.; investigation, G.D’A., R.S.; resources, S.C., B.S.; data curation, R.S. E.M.; writing—original draft preparation, G.D’A., E.M., and G.M.; writing—review and editing, B.S., G.T. and L.M.; supervision, S.C., B.S; project administration, S.C., B.S.; funding acquisition, S.C. and B.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Italian Ministry of Education, University and Research (Ministero dell’Università e della Ricerca-MUR), ex 60% 2022 S.C.
Institutional Review Board Statement
This study was approved on 23/07/2015 by the Interinstitutional Ethical Committee of the University of Chieti-Pescara, Chieti, Italy; committee report n. 14. A Patients gave written informed consent and received information about the study protocol. The study was conducted in accordance with the principles of the Helsinki Declaration established by the World Medical Association regarding human subjects.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. Trial registration: Trial is registered with ClinicalTrials.gov Identifier: (Registration Number: NCT03431766). Registered 13/02/2018, retrospectively registered.
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no conflict of interest.
References
- Simonis, P.; Dufour, T.; Tenenbaum, H. Long-term implant survival and success: a 10-16-year follow-up of non-submerged dental implants. Clin. Oral Implants Res. 2010, 21, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Filius, M.A.P.; Vissink, A.; Cune, M.S.; Raghoebar, G.M.; Visser, A. Long-term implant performance and patients' satisfaction in oligodontia. J. Dent. 2018, 71, 18–24. [Google Scholar] [CrossRef]
- Baumer, A.; Toekan, S.; Saure, D.; Korner, G. Survival and success of implants in a private periodontal practice: a 10-year retrospective study. BMC Oral Health 2020, 20, 92. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Martins, M.D.; Wennerberg, A. Immediate placement of implants into infected sites: a systematic review. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl 1), e1–e16. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Berglundh, T.; Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Berardini, M.; Trisi, P.; Sinjari, B.; Rutjes, A.W.; Caputi, S. The Effects of High Insertion Torque Versus Low Insertion Torque on Marginal Bone Resorption and Implant Failure Rates: A Systematic Review With Meta-Analyses. Implant Dent. 2016, 25, 532–540. [Google Scholar] [CrossRef]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and esthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implants Res. 2012, 23 (Suppl 6), 2–21. [Google Scholar] [CrossRef]
- Caricasulo, R.; Malchiodi, L.; Ghensi, P.; Fantozzi, G.; Cucchi, A. The influence of implant-abutment connection to peri-implant bone loss: A systematic review and meta-analysis. Clin. Implant Dent. Relat. Res. 2018, 20, 653–664. [Google Scholar] [CrossRef]
- Krisam, J.; Ott, L.; Schmitz, S.; et al. Factors affecting the early failure of implants placed in a dental practice with a specialization in implantology - a retrospective study. BMC Oral Health 2019, 19, 208. [Google Scholar] [CrossRef]
- Coli, P.; Christiaens, V.; Sennerby, L.; Bruyn, H. Reliability of periodontal diagnostic tools for monitoring peri-implant health and disease. Periodontol. 2000 2017, 73, 203–217. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.A.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar] [PubMed]
- Lombardi, T.; Berton, F.; Salgarello, S.; Barbalonga, E.; Rapani, A.; Piovesana, F.; Gregorio, C.; Barbati, G.; Di Lenarda, R.; Stacchi, C. Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study. J. Clin. Med. 2019, 8, 1168. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.S.; Araujo, M.A.; Benfatti, C.A.; Araujo, C.R.; Piattelli, A.; Perrotti, V.; Iezzi, G. Comparative histological and histomorphometrical evaluation of marginal bone resorption around external hexagon and Morse cone implants: an experimental study in dogs. Implant Dent. 2014, 23, 270–276. [Google Scholar] [CrossRef]
- Rivara, F.; Macaluso, G.M.; Toffoli, A.; Calciolari, E.; Goldoni, M.; Lumetti, S. The effect of a 2-mm inter-implant distance on esthetic outcomes in immediately non-occlusally loaded platform shifted implants in healed ridges: 12-month results of a randomized clinical trial. Clin. Implant Dent. Relat. Res. 2020, 22, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Dellow, A.G.; Driessen, C.H.; Nel, H.J. Scanning electron microscopy evaluation of the interfacial fit of interchanged components of four dental implant systems. Int. J. Prosthodont. 1997, 10, 216–221. [Google Scholar]
- D'Ercole, S.; Tripodi, D.; Ravera, L.; Perrotti, V.; Piattelli, A.; Iezzi, G. Bacterial leakage in Morse Cone internal connection implants using different torque values: an in vitro study. Implant Dent. 2014, 23, 175–179. [Google Scholar] [CrossRef]
- Scarano, A.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Iezzi, G. Sealing capability of implant-abutment junction under cyclic loading: a toluidine blue in vitro study. J. Appl. Biomater. Funct. Mater. 2015, 13, e293–e295. [Google Scholar] [CrossRef]
- Ericsson, I.; Persson, L.G.; Berglundh, T.; Marinello, C.P.; Lindhe, J.; Klinge, B. Different types of inflammatory reactions in peri-implant soft tissues. J. Clin. Periodontol. 1995, 22, 255–261. [Google Scholar] [CrossRef]
- Faveri, M.; Gursky, L.C.; Feres, M.; Shibli, J.A.; Salvador, S.L.; de Figueiredo, L.C. Scaling and root planing and chlorhexidine mouthrinses in the treatment of chronic periodontitis: a randomized, placebo-controlled clinical trial. J. Clin. Periodontol. 2006, 33, 819–828. [Google Scholar] [CrossRef]
- Carcuac, O.; Abrahamsson, I.; Charalampakis, G.; Berglundh, T. The effect of the local use of chlorhexidine in surgical treatment of experimental peri-implantitis in dogs. J. Clin. Periodontol. 2015, 42, 196–203. [Google Scholar] [CrossRef]
- de Waal, Y.C.M.; Raghoebar, G.M.; Meijer, H.J.A.; Winkel, E.G.; van Winkelhoff, A.J. Implant decontamination with 2% chlorhexidine during surgical peri-implantitis treatment: a randomized, double-blind, controlled trial. Clin. Oral Implants Res. 2015, 26, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennstr√∂m, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D'Addazio, G.; De Tullio, I.; Traini, T.; Caputi, S. Peri-Implant Bone Resorption during Healing Abutment Placement: The Effect of a 0.20% Chlorhexidine Gel vs. Placebo-A Randomized Double Blind Controlled Human Study. Biomed. Res. Int. 2018, 2018, 5326340. [Google Scholar] [CrossRef] [PubMed]
- D'Ercole, S.; D'Addazio, G.; Di Lodovico, S.; Traini, T.; Di Giulio, M.; Sinjari, B. Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study. J. Clin. Med. 2020, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Annibali, S.; Bignozzi, I.; Cristalli, M.P.; Graziani, F.; La Monaca, G.; Polimeni, A. Peri-implant marginal bone level: a systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants. J. Clin. Periodontol. 2012, 39, 1097–113. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: a systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Laurell, L.; Lundgren, D. Marginal bone level changes at dental implants after 5 years in function: a meta-analysis. Clin. Implant Dent. Relat. Res. 2011, 13, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; HaÃäkansson, J.; WennstroÃàm, J.L.; Tomasi, C.; Larsson, M.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: early and late implant loss. J. Dent. Res. 2015, 94, 44S–51S. [Google Scholar] [CrossRef] [PubMed]
- Doornewaard, R.; Christiaens, V.; De Bruyn, H.; et al. Long-term effect of surface roughness and patients' factors on crestal bone loss at dental implants. A systematic review and meta-analysis. Clin. Implant Dent. Relat. Res. 2017, 19, 372–399. [Google Scholar] [CrossRef] [PubMed]
- Zumstein, T.; SchuÃàtz, S.; Sahlin, H.; Sennerby, L. Factors influencing marginal bone loss at a hydrophilic implant design placed with or without GBR procedures: A 5-year retrospective study. Clin. Implant Dent. Relat. Res. 2019, 21, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fan, Y.; Lin, Z.; Song, Z.; Shu, R.; Xie, Y. Survival rate and potential risk indicators of implant loss in non-smokers and systemically healthy periodontitis patients: An up to 9-year retrospective study. J. Periodont Res. 2021, 56, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.M.; Geng, W.; Luo, C.C. Prosthetic complications of fixed dental prostheses supported by locking-taper implants: a retrospective study with a mean follow-up of 5 years. BMC Oral Health 2021, 21, 476. [Google Scholar] [CrossRef] [PubMed]
- Gosau, D.M.; Hahnel, S.; Schwarz, F.; Gerlach, T.; Reichert, T.E.; BuÃàrgers, R. Effect of six different peri-implantitis disinfection methods on in vivo human oral biofilm. Clin. Oral Implants Res. 2010, 21, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Chin, M.Y.; Sandham, A.; de Vries, J.; van der Mei, H.C.; Busscher, H.J. Biofilm formation on surface characterized micro-implants for skeletal anchorage in orthodontics. Biomaterials 2007, 28, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Ntrouka, V.I.; Slot, D.E.; Louropoulou, A.; Van der Weijden, F. The effect of chemotherapeutic agents on contaminated titanium surfaces: a systematic review. Clin. Oral Implants Res. 2011, 22, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D'Addazio, G.; Bozzi, M.; Celletti, R.; Traini, T.; Mavriqi, L.; Caputi, S. Comparison of a Novel Ultrasonic Scaler Tip vs. Conventional Design on a Titanium Surface. Materials 2018, 11, 2345. [Google Scholar] [CrossRef]
- Anitua, E.; Orive, G.; Aguirre, J.J.; Ardanza, B.; Andia, I. 5-year clinical experience with BTI dental implants: risk factors for implant failure. J. Clin. Periodontol. 2008, 35, 724–732. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Huynh-Ba, G. History of treated periodontitis and smoking as risks for implant therapy. Int. J. Oral Maxillofac. Implants 2009, 24 (Suppl), 39–68. [Google Scholar] [PubMed]
- Mayta-Tovalino, F.; Mendoza-Martiarena, Y.; Romero-Tapia, P.; et al. An 11-Year Retrospective Research Study of the Predictive Factors of Peri-Implantitis and Implant Failure: Analytic-Multicentric Study of 1279 Implants in Peru. Int. J. Dent. 2019, 2019, 3527872. [Google Scholar] [CrossRef]
- Renvert, S.; Quirynen, M. Risk indicators for peri-implantitis. A narrative review. Clin. Oral Implants Res. 2015, 26, 15–44. [Google Scholar] [CrossRef]
- D'Addazio, G.; Santilli, M.; Sinjari, B.; Xhajanka, E.; Rexhepi, I.; Mangifesta, R.; Caputi, S. Access to Dental Care-A Survey from Dentists, People with Disabilities and Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 1556. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Zorzano, L.A.; Estefania-Fresco, R.; Telletxea, O.; Bravo, M. Prevalence of peri-implant inflammatory disease in patients with a history of periodontal disease who receive supportive periodontal therapy. Clin. Oral Implants Res. 2015, 26, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Bellosta, S.; Bravo, M.; Subira, C.; Echeverria, J.J. Retrospective study of the long-term survival of 980 implants placed in a periodontal practice. Int. J. Oral Maxillofac. Implants 2010, 25, 613–619. [Google Scholar] [PubMed]
- Goh, M.S.; Hong, E.J.; Chang, M. Prevalence and risk indicators of peri-implantitis in Korean patients with a history of periodontal disease: a cross-sectional study. J. Periodontal Implant Sci. 2017, 47, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Seki, K.; HaÃäkansson, J. Implant Treatment with 12-Year Follow-Up in a Patient with Severe Chronic Periodontitis: A Case Report and Literature Review. Case Rep. Dent. 2019, 2019, 3715159. [Google Scholar] [CrossRef]
- Lee, K.Y.; Shin, K.S.; Jung, J.H.; Cho, H.W.; Kwon, K.H.; Kim, Y.L. Clinical study on screw loosening in dental implant prostheses: a 6-year retrospective study. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 133–142. [Google Scholar] [CrossRef]
- Jemt, T.; Laney, W.R.; Harris, D.; Henry, P.J.; Krogh, P.H., Jr.; Polizzi, G.; Zarb, G.A.; Herrmann, I. Osseointegrated implants for single tooth replacement: a 1-year report from a multicenter prospective study. Int. J. Oral Maxillofac. Implants 1991, 6, 29–36. [Google Scholar] [PubMed]
- Kreissl, M.E.; Gerds, T.; Muche, R.; Heydecke, G.; Strub, J.R. Technical complications of implant-supported fixed partial dentures in partially edentulous cases after an average observation period of 5 years. Clin. Oral Implants Res. 2007, 18, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.C.; Small, P.N.; Elian, N.; Tarnow, D. Screw loosening for standard and wide diameter implants in partially edentulous cases: 3- to 7-year longitudinal data. Implant Dent. 2004, 13, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Di Crescenzo, A.; Bardini, L.; Sinjari, B.; Traini, T.; Marinelli, L.; Carraro, M.; Germani, R.; Di Profio, P.; Caputi, S.; Di Stefano, A.; Bonchio, M.; Paolucci, F.; Fontana, A. Surfactant hydrogels for the dispersion of carbon-nanotube-based catalysts. Chemistry 2013, 19, 16415–16423. [Google Scholar] [CrossRef] [PubMed]
- De Cremer, K.; Braem, A.; Gerits, E.; De Brucker, K.; Vandamme, K.; Martens, J.A.; Michiels, J.; Vleugels, J.; Cammue, B.P.; Thevissen, K. Controlled Release of Chlorhexidine from a Mesoporous Silica-Containing Macroporous Titanium Dental Implant Prevents Microbial Biofilm Formation. Eur. Cells Mater. 2017, 33, 13–27. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical images at different time points: (A-B) Occlusal and vestibular vision a T4 (12 months of Follow-up); (C-D) Occlusal and vestibular vision of same patients a T5 (5 years of follow-up).
Figure 1.
Clinical images at different time points: (A-B) Occlusal and vestibular vision a T4 (12 months of Follow-up); (C-D) Occlusal and vestibular vision of same patients a T5 (5 years of follow-up).

Figure 2.
Statistical analysis of MBL: (A) MBL comparison a T5 between patient of Group A and B. No statistical differences were found at 5 years of follow up; (B) MBL comparison between T4 and T5 in patients belonging to Group A. No statistical differences were found between these two time points; (C) MBL comparison between T4 and T5 in patients belonging to Group B. a slight statistical difference was found in these two time points. * (P≤0.05); (D) MBL comparison at T5 between patients under periodontal control or not (PUC vs NON PUC). a statistical difference was found in MBL in patients under control. ** (P≤0.001); (E) MBL comparison between patients under periodontal control (PUC) between T4 and T5. No statistical differences were found between these two time points; (F) MBL comparison between patients that didn’t undergo at control visit (NON PUC), at T4 vs T5. a statistical difference was found in MBL in patients under control. * (P≤0.05); .
Figure 2.
Statistical analysis of MBL: (A) MBL comparison a T5 between patient of Group A and B. No statistical differences were found at 5 years of follow up; (B) MBL comparison between T4 and T5 in patients belonging to Group A. No statistical differences were found between these two time points; (C) MBL comparison between T4 and T5 in patients belonging to Group B. a slight statistical difference was found in these two time points. * (P≤0.05); (D) MBL comparison at T5 between patients under periodontal control or not (PUC vs NON PUC). a statistical difference was found in MBL in patients under control. ** (P≤0.001); (E) MBL comparison between patients under periodontal control (PUC) between T4 and T5. No statistical differences were found between these two time points; (F) MBL comparison between patients that didn’t undergo at control visit (NON PUC), at T4 vs T5. a statistical difference was found in MBL in patients under control. * (P≤0.05); .
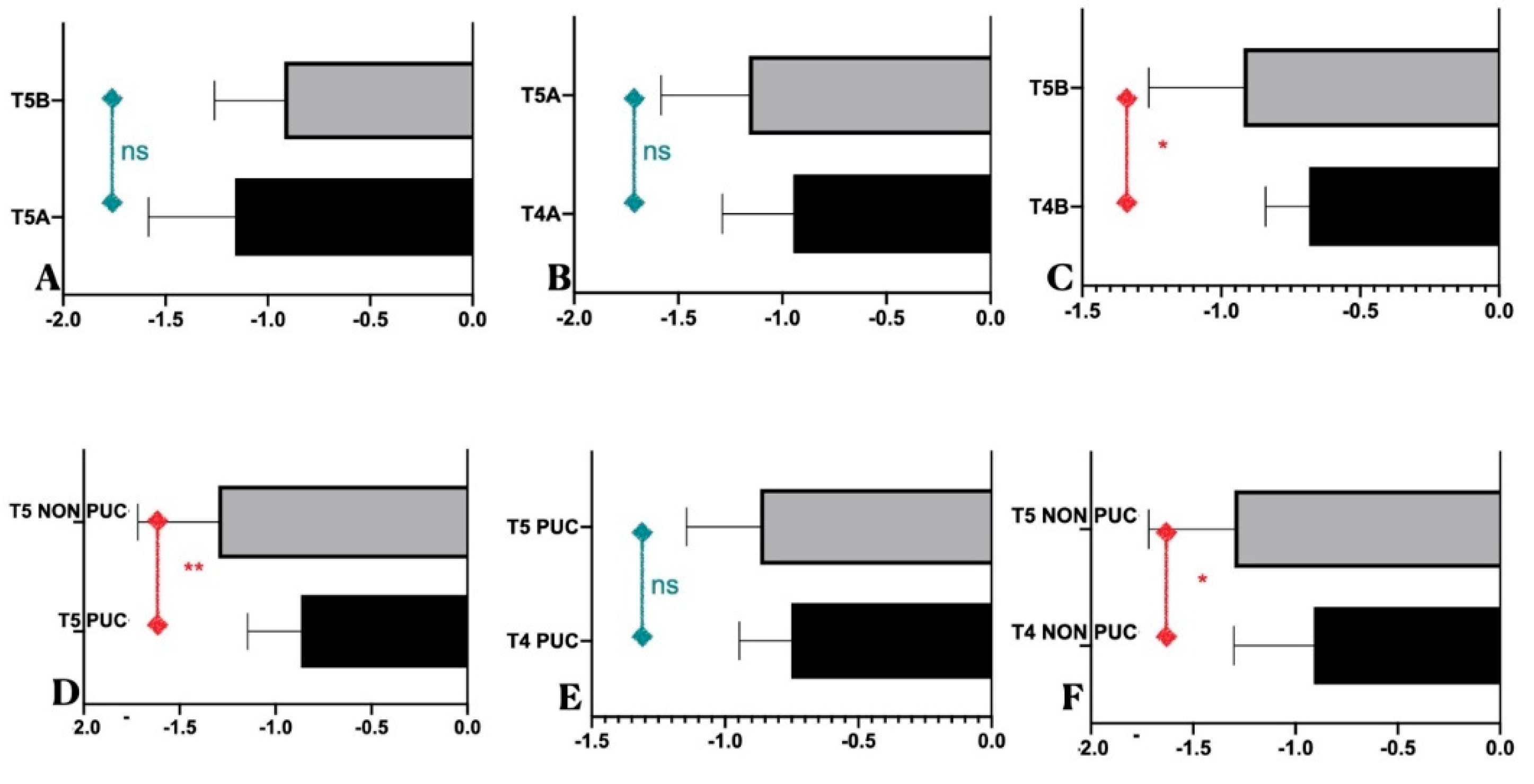
Figure 3.
S Graphical representation of MBL during every surgical and prosthetic stage till T5. (A) Global MBL; (B) MBL in Group A vs Group B.
Figure 3.
S Graphical representation of MBL during every surgical and prosthetic stage till T5. (A) Global MBL; (B) MBL in Group A vs Group B.
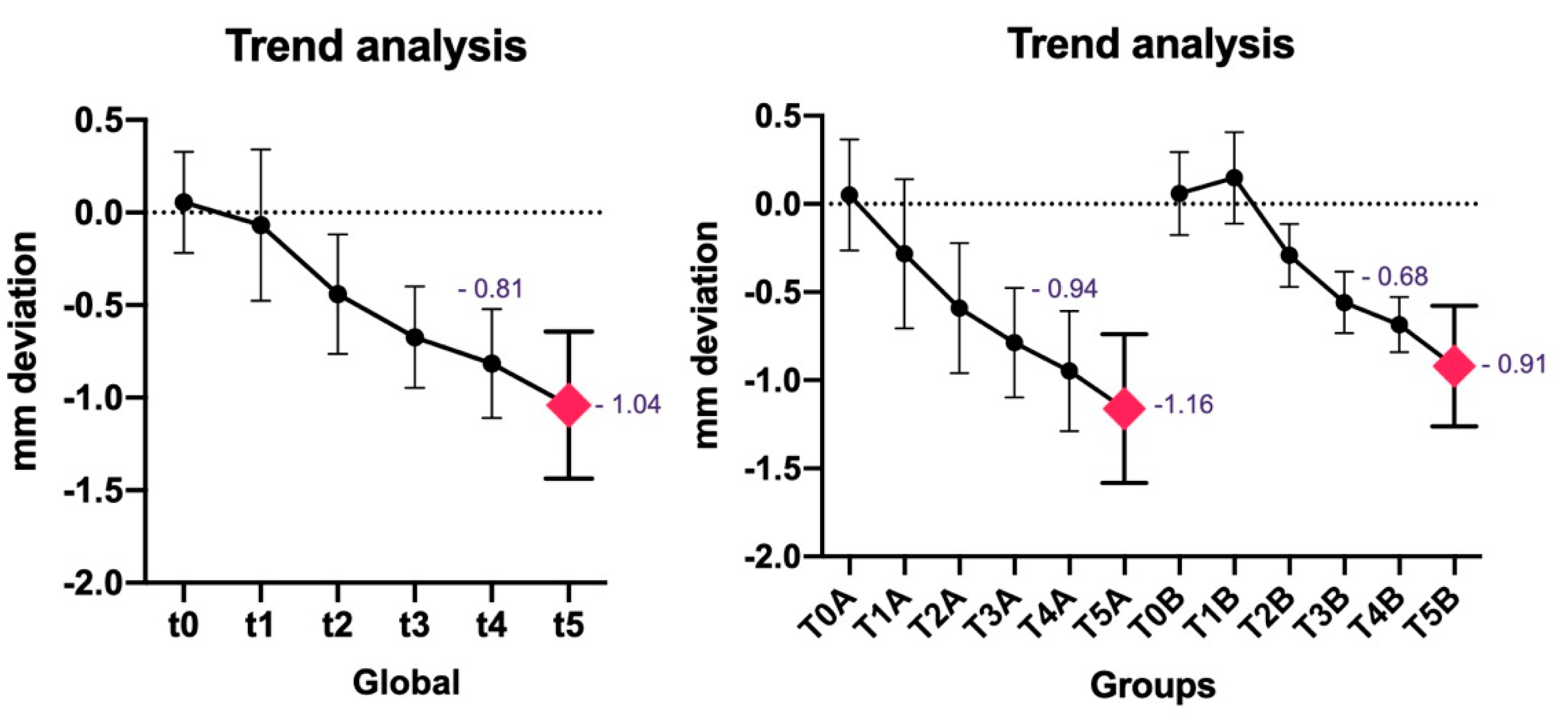
Figure 4.
Radiographs from the two groups. (A-E) Patient from Group B (test group) from T0 to T4. A minimal bone gain was present at the second surgical stage; (F-J) Patient from Group A (control group); (K) radiograph of same patient from group A at T5. 0 bone loss were present a 5 year of follow-up; (L) radiograph of same patient from group A at T5. A slight bone loss were present a 5 year of follow-up;.
Figure 4.
Radiographs from the two groups. (A-E) Patient from Group B (test group) from T0 to T4. A minimal bone gain was present at the second surgical stage; (F-J) Patient from Group A (control group); (K) radiograph of same patient from group A at T5. 0 bone loss were present a 5 year of follow-up; (L) radiograph of same patient from group A at T5. A slight bone loss were present a 5 year of follow-up;.
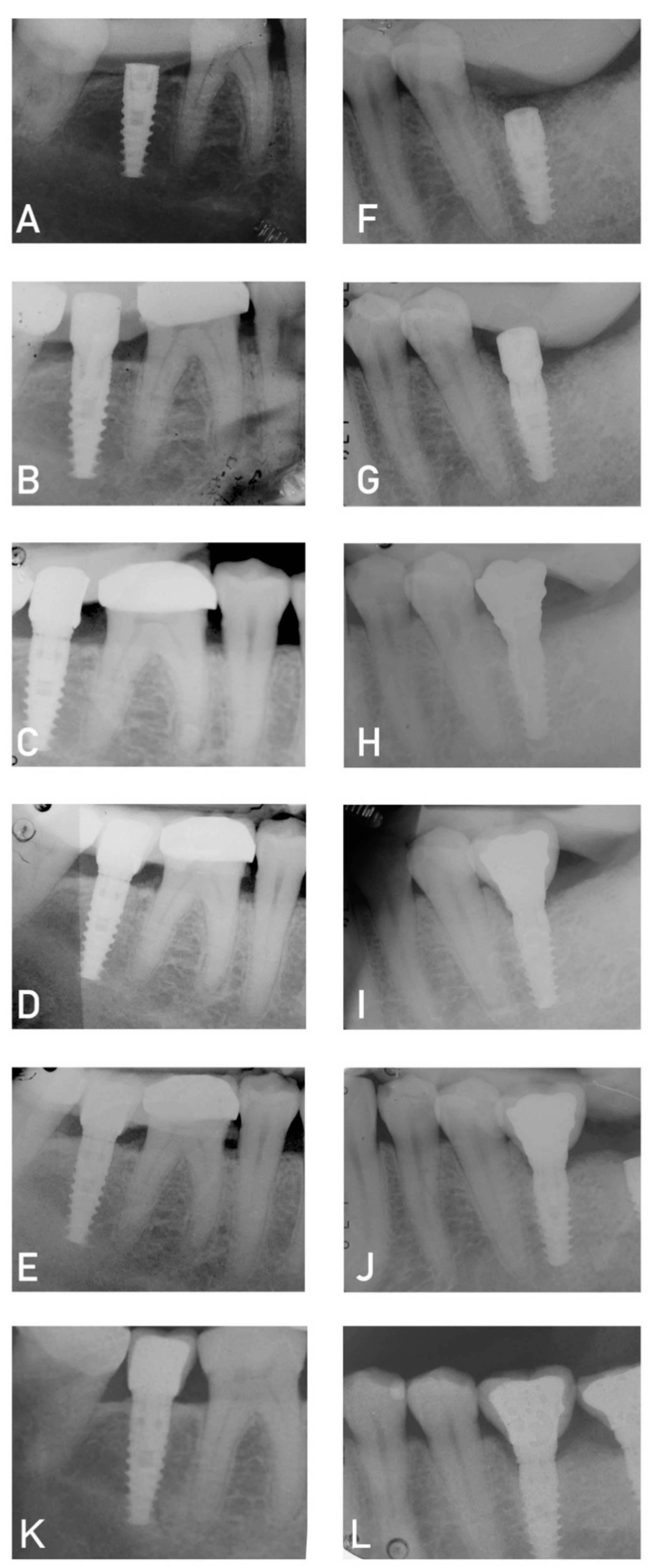
Figure 5.
Periapical radiographs: (A) T4 (12 months of follow-up); (B) T5 (5 years of follow-up). The patient didn’t undergo at the control visit. a caries was identified under the old restoration in the mesial portion of the adjacent tooth.
Figure 5.
Periapical radiographs: (A) T4 (12 months of follow-up); (B) T5 (5 years of follow-up). The patient didn’t undergo at the control visit. a caries was identified under the old restoration in the mesial portion of the adjacent tooth.
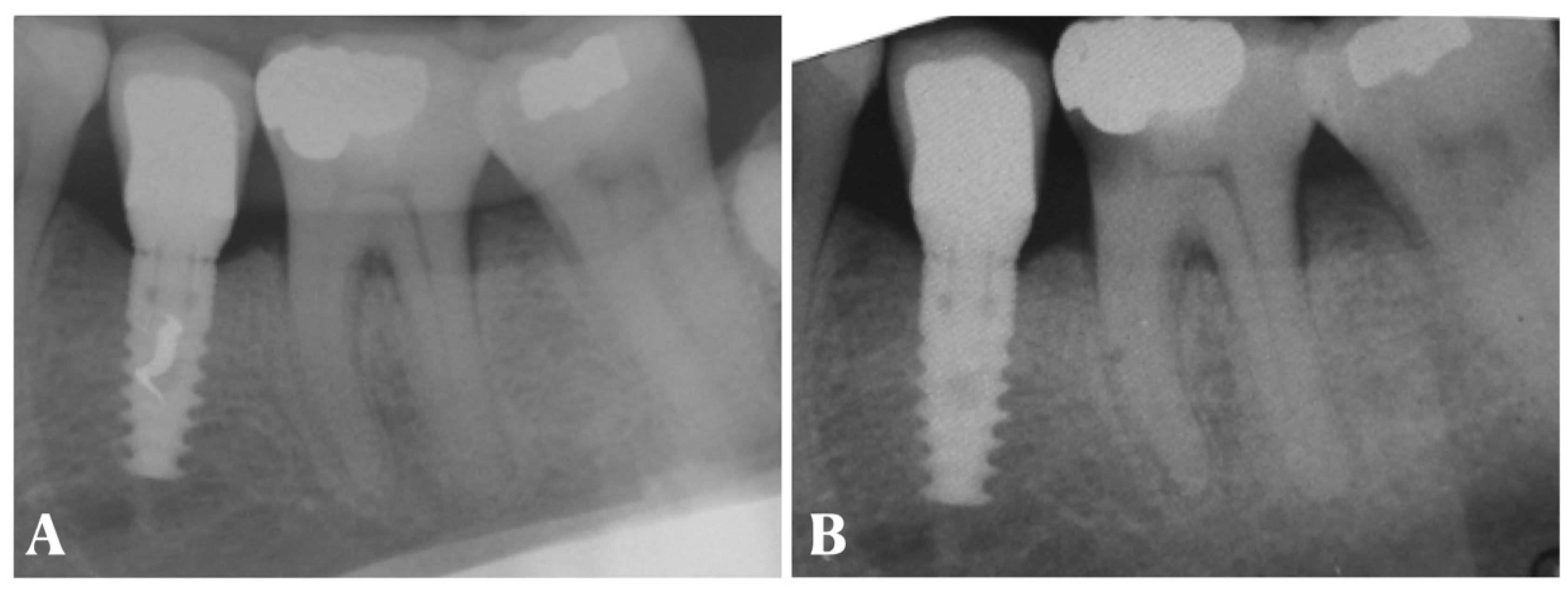

Table 1.
Patient characteristics at T5. Patient number, Survival rate, Gengival indeces and statistiscal analysis of FMPS and FMBS. PUC= patients under periodontal control. NO-PUC= patients that didn’t undergo the periodontal control. Sig. **** (P≤0.0001), *** (P≤0.001).
Table 1.
Patient characteristics at T5. Patient number, Survival rate, Gengival indeces and statistiscal analysis of FMPS and FMBS. PUC= patients under periodontal control. NO-PUC= patients that didn’t undergo the periodontal control. Sig. **** (P≤0.0001), *** (P≤0.001).
| Total patients numbers | 32 | |||
|---|---|---|---|---|
| Patients evaluated at 5-year follow-up | 31 | |||
| Patients Group A | 16 | |||
| Patients Group B | 15 | |||
| Implant failed | 1 (Group A). implant removed | |||
| Survival rate | 96.7% | |||
| Patients under strict hygienic control (PUC) | 58.1% | |||
| Global Full mouth Plaque Score (FMPS) | 21,38% ± 5,65 | |||
| Global Full mouth Bleeding Score (FMBS) | 20,96% ± 4,76 | |||
| Group A | Group B | Sig. | ||
| FMPS (Group A- Group B) | 22,59% ± 5,93 | 19,83% ± 5,22 | P=0,18 ns | |
| FMBS (Group A- Group B) | 21,37% ± 5,46 | 20,39% ± 4,23 | P=0,59 ns | |
| FMPS (PUC / NO-PUC) | 17,81% ± 3,37 | 26,32% ± 4,42 | **** | |
| FMBS (PUC / NO-PUC) | 18,17% ± 2,88 | 24,95% ± 4,3 | *** | |
Table 2.
Table show all the involved patients. Specifically they were divided in Group A(control) and B (CHX gel). PUC= patients under periodontal control, NO-PUC= patients that didn’t undergo the periodontal control. All MBL were reported starting to T0 to T5 and FMPS and FMBS at T5 were reported. Patient ID34: the implant was removed.
Table 2.
Table show all the involved patients. Specifically they were divided in Group A(control) and B (CHX gel). PUC= patients under periodontal control, NO-PUC= patients that didn’t undergo the periodontal control. All MBL were reported starting to T0 to T5 and FMPS and FMBS at T5 were reported. Patient ID34: the implant was removed.
| ID PAT | SITE | GROUP | PUC/ NO-PUC | T0 | T1 | T2 | T3 | T4 | T5 | FMPS | FMBS | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 1.6 | A | NO-PUC | 0,22 | -0,06 | -0,49 | -0,73 | -1,51 | -1,6 | 22,4 | 24,5 | |
| 5 | 1.4 | A | PUC | 0 | -0,38 | -0,55 | -0,82 | -1,07 | -1,1 | 21,3 | 19,45 | |
| 7 | 4.6 | A | PUC | 0,49 | 0,12 | -0,2 | -0,84 | -0,95 | -1,2 | 24,5 | 17,54 | |
| 11 | 1.6 | A | NO-PUC | -0,62 | -1,53 | -1,75 | -1,76 | -1,84 | -2,2 | 25,6 | 18,34 | |
| 14 | 4.7 | A | PUC | -0,39 | -0,92 | -0,89 | -0,65 | -0,8 | -0,87 | 19,3 | 18,5 | |
| 17 | 3.6 | A | NO-PUC | -0,06 | -0,38 | -0,43 | -0,68 | -0,73 | -0,88 | 29,4 | 28,76 | |
| 20 | 3.6 | A | PUC | 0,06 | 0 | -0,44 | -0,6 | -0,63 | -0,7 | 16,6 | 19,5 | |
| 21 | 4.6 | A | PUC | 0,16 | -0,29 | -0,53 | -0,73 | -0,94 | -0,9 | 14,3 | 14,5 | |
| 23 | 4.6 | A | NO-PUC | -0,13 | -0,2 | -0,74 | -1,01 | -1,05 | -1,68 | 31,4 | 29,04 | |
| 24 | 3.5 | A | NO-PUC | -0,06 | -0,2 | -0,44 | -0,59 | -0,64 | -1,5 | 30,7 | 31,84 | |
| 25 | 2.2 | A | PUC | 0,6 | -0,06 | -0,46 | -0,71 | -0,77 | -0,82 | 24,3 | 19,12 | |
| 29 | 3.6 | A | PUC | -0,11 | -0,15 | -0,78 | -0,94 | -1,06 | -1,25 | 17,5 | 18,76 | |
| 30 | 3.7 | A | PUC | 0,05 | -0,09 | -0,25 | -0,38 | -0,58 | -0,87 | 15,4 | 14,45 | |
| 32 | 2.4 | A | NO-PUC | 0,35 | -0,05 | -0,52 | -0,79 | -0,9 | -1,1 | 29,87 | 27,12 | |
| 33 | 3.6 | A | PUC | 0,21 | -0,05 | -0,4 | -0,58 | -0,74 | -0,74 | 16,3 | 19,09 | |
| 34 | 4.6 | A | NO-PUC | -0,08 | -0,21 | -0,58 | -0,61 | -0,8 | REMOVED | 26,5 | 23,45 | |
| 1 | 3.6 | B | NO-PUC | 0,57 | 0,62 | 0 | -0,47 | -0,55 | -1 | 25,8 | 26,09 | |
| 4 | 3.6 | B | PUC | -0,17 | 0,03 | -0,5 | -0,71 | -0,81 | -1,32 | 14,6 | 21,45 | |
| 8 | 4.6 | B | NO-PUC | 0,2 | 0,21 | -0,48 | -0,74 | -0,79 | -1,2 | 29,45 | 24,59 | |
| 10 | 3.6 | B | PUC | -0,04 | 0 | -0,38 | -0,53 | -0,61 | -0,6 | 20,5 | 19,4 | |
| 12 | 2.4 | B | PUC | 0 | 0,1 | -0,35 | -0,55 | -0,71 | -1,1 | 20,4 | 22,22 | |
| 13 | 3.6 | B | NO-PUC | -0,02 | 0,15 | -0,37 | -0,67 | -0,89 | -1,25 | 19,3 | 18,41 | |
| 15 | 3.6 | B | NO-PUC | 0,16 | 0,39 | -0,08 | -0,61 | -0,74 | -1,45 | 17,9 | 19,45 | |
| 16 | 4.6 | B | PUC | 0,12 | 0,59 | -0,23 | -0,49 | -0,61 | -0,72 | 15,9 | 18,54 | |
| 18 | 1.5 | B | PUC | 0 | -0,36 | -0,57 | -0,69 | -0,77 | -0,8 | 14,1 | 13,4 | |
| 19 | 4.6 | B | PUC | 0,34 | 0,24 | 0 | -0,16 | -0,31 | -0,56 | 14,5 | 12,23 | |
| 22 | 2.4 | B | PUC | 0,29 | 0,28 | -0,29 | -0,88 | -0,95 | -0,23 | 14,5 | 16,98 | |
| 26 | 4.5 | B | PUC | -0,35 | -0,08 | -0,15 | -0,41 | -0,66 | -1,12 | 16,4 | 19,5 | |
| 27 | 3.7 | B | NO-PUC | 0 | -0,05 | -0,21 | -0,54 | -0,59 | -0,62 | 27,8 | 24,98 | |
| 28 | 2.5 | B | PUC | 0,06 | 0,18 | -0,3 | -0,37 | -0,57 | -0,72 | 20,12 | 22,45 | |
| 31 | 2.6 | B | NO-PUC | -0,26 | -0,08 | -0,46 | -0,56 | -0,7 | -1,1 | 26,23 | 26,23 | |
| MEAN | -0,8151613 mm | -1,04 mm | 21,38 % | 20,96 & | ||||||||
| ST. Dev | 0,28814199 | 0,39673669 | 5,65255588 | 4,76767566 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



