
Submitted:
07 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Purpose: To compare refractive prediction error (PE)s between phacotrabeculectomy and phacoemulsification. Methods: Refractive PE was defined as the difference of spherical equivalent between the predicted value using the Barrett Universal II formula and the actual value obtained at postoperative one month. Forty-eight eyes that had undergone phacotrabeculectomy (19 eyes, open-angle glaucoma; 29 eyes, angle-closure glaucoma) were matched with 48 eyes that had undergone phacoemulsification by age, average keratometry value and axial length (AL), and their PEs were compared. The factors associated with PE were analyzed by multivariable regression analyses. Results: Phacotrabeculectomy group showed a larger absolute PE compared to the phacoemulsification group (0.51 ± 0.37 Diopters vs. 0.38 ± 0.22, P=0.033). Larger absolute PE was associated with longer AL (P=0.010) and higher intraocular pressure (IOP) difference (P=0.012). Hyperopic shift (PE>0) was associated with shallower preoperative anterior chamber depth (ACD) (P=0.024) and larger IOP difference (P=0.031). In the phacotrabeculectomy group, the PE was inversely correlated with AL: long eyes showed myopic shift and short eyes hyperopic shift (P=0.002). Conclusions: Surgeons should be aware of the possibility of worse refractive outcomes when planning phacotrabeculectomy especially in eyes with high preoperative IOP, shallow ACD, and/or extreme AL.
Keywords:
phacotrabeculectomy
; glaucoma
; cataract surgery
; prediction error
; refraction
1. Introduction
Glaucoma and cataract are major and often coexisting causes of visual impairment in the elderly [1]. When these diseases require surgical intervention, clinicians have to decide whether to perform glaucoma filtration surgery and phacoemulsification at the same time or sequentially. Phacotrabeculectomy has several advantages in terms of minimizing postoperative IOP spikes and reducing surgery time and cost, with less recovery time [2,3,4]. Even in cases with angle-closure glaucoma (ACG), phacotrabeculectomy has been reported to be a better option than phacoemulsification alone [5,6].
As a refractive surgery, however, phacotrabeculectomy has a limitation. Trabeculectomy induces changes to ocular biometry with regard to axial length (AL) and anterior chamber depth (ACD) [7,8,9,10,11]. Such changes might increase prediction error, since intraocular lens (IOL) power calculation is based on preoperative ocular biometry. Several studies have compared refractive outcomes between phacotrabeculectomy and phacoemulsification alone [11,12,13,14,15,16,17]. The results, however, were inconsistent, and moreover, the prediction error had been calculated using a third-generation IOL calculation formula, which uses only AL and keratometry values to determine the effective lens position [18]. Currently, IOL power calculation is based on fourth-generation formulas that incorporate additional variables, including ACD, in order to predict the effective lens position more accurately [18,19]. This enhanced accuracy might not be relevant to phacotrabeculectomy cases though, since glaucoma patients with uncontrolled intraocular pressure (IOP) would have pathologic aqueous outflow pathway and, thus, deviated preoperative ACD values. Further, this deformation would be different between ACG and open-angle glaucoma (OAG) patients. For purposes of clarification and confirmation, therefore, the present study compared post-phacotrabeculectomy and phacoemulsification prediction errors using a fourth-generation IOL power calculation formula (i.e., the Barrett II Universal formula).
2. Materials and Methods
This retrospective comparative study was conducted following the tenets set forth in the Declaration of Helsinki, and was approved by the Institutional Review Board of Seoul National University Boramae Medical Center. Between January 2009 and June 2022, glaucoma patients who had undergone uncomplicated phacotrabeculectomy performed by either of two glaucoma specialists (KML or SHK) at the Seoul National University Boramae Medical Center were included. Control cases were chosen from among phacoemulsification cases (without glaucoma) performed by the same surgeons to match each phacotrabeculectomy case in age, average keratometry value (average K), and axial length (AL). The exclusion criteria were as follows: extracapsular bag location of IOL (sulcus or scleral fixation); previous history of ocular surgery such as corneal refractive surgery; surgical complications such as posterior capsular rupture or concomitant anterior/posterior vitrectomy, and less than one-month follow-up on refractive errors.
Preoperatively, all of the subjects underwent comprehensive ophthalmologic examinations that included best-corrected visual acuity (BCVA) assessment, refraction, slit-lamp biomicroscopy, Goldmann applanation tonometry, gonioscopy, dilated funduscopic examination, keratometry (RKT-7700; Nidek, Hiroshi, Japan), and ocular biometry (IOLMaster version 5; Carl Zeiss Meditec, Dublin, CA, USA). In all phacotrabeculectomy cases, IOP and ocular biometry were measured after maximal medical treatment to reduce IOP as much as possible. Among the ocular biometry values, ACD and AL were used in the analysis.
In general, trabeculectomy was performed through the fornix-based conjunctival flap and superior rectangular 3.5 × 2.5 mm scleral flap with intraoperative mitomycin C (0.4 mg/mL for 3 minutes). The scleral flap and conjunctiva were sutured with interrupted 10-0 nylon sutures. Phacoemulsification was performed through a 2.75 mm clear corneal incision at a different site from the trabeculectomy, and single-piece acrylic IOLs were placed in the bag in all cases. The corneal wound was repaired with a 10-0 nylon interrupted suture in the combined phacotrabeculectomy group and with stromal hydration in the phacoemulsification group. The postoperative IOP and refractive errors were measured at one month after surgery. ΔIOP was defined as the difference between preoperative IOP and postoperative IOP. The prediction error was obtained by subtracting the actual postoperative spherical equivalent (SE) from the predicted SE using the Barrett Universal II formula.
Data analysis
The intergroup comparisons (phacotrabeculectomy vs. phacoemulsification) were performed by way of the independent t-test for the continuous variables and by chi-square testing for the categorical variables. Comparisons by diagnosis (OAG, ACG, and control) were performed by analysis of variance (ANOVA) test, applying the post hoc Scheffe test for the continuous variables and the chi-square test for the categorical variables. Univariable and multivariable analyses were run to determine the factors associated with prediction errors, and parameters with a P value less than 0.10 in the univariable analysis were included in the subsequent multivariable analysis. A logistic regression analysis was performed to determine the factors associated with hyperopic shift (prediction error > 0). Statistical analyses were performed with commercially available software (Stata version 16.0; StataCorp, College Station, TX, USA). The data herein are presented as mean ± standard deviations except where stated otherwise, and the cutoff for statistical significance was set to P < 0.05.
3. Results
A total 53 phacotrabeculectomy eyes were enrolled between January 2009 and June 2022. Of these, one eye was excluded due to combined anterior vitrectomy due to zonular laxity, one eye due to IOL sulcus insertion, one eye due to previous history of trabeculectomy, and two eyes due to follow-up loss in the aspect of refractive errors, which resulted in a final sample of 48 eyes of 48 subjects (19 OAG eyes and 29 ACG eyes). During the same period, 48 eyes were matched by age, average keratometry value and AL from the uneventful phacoemulsification cases without glaucoma history. The two groups’ demographic and clinical characteristics are summarized in Table 1: there were no differences in age, sex distribution, AL, or average K, whereas the phacotrabeculectomy group had higher preoperative IOP (P < 0.001), larger ∆IOP (P < 0.001), and shallower preoperative ACD (P = 0.047).
The prediction error was −0.23 ± 0.59 Diopters in the phacotrabeculectomy group and −0.31 ± 0.31 in the phacoemulsification group (P = 0.436). The absolute prediction error (absolute value of prediction error) was larger in the phacotrabeculectomy group than in the phacoemulsification group (0.51 ± 0.37 Diopters vs. 0.38 ± 0.22, P = 0.033, Table 1). The factors associated with the absolute prediction errors were analyzed by multiple regression analyses using two models, which showed that longer AL (P = 0.010 in model 1, P = 0.020 in model 2), larger ΔIOP (P = 0.012), and phacotrabeculectomy (P = 0.025) were associated with larger absolute prediction error (Table 2).
Hyperopic shift of prediction error was observed in 23 (24%) cases: 15 phacotrabeculectomy cases and 8 phacoemulsification cases (P = 0.094). The logistic regression analyses revealed that shallower preoperative ACD (P = 0.024) and larger ΔIOP (P = 0.004 in model 1, P = 0.031 in model 2) were associated with higher odds of hyperopic shift (Table 3).
The phacotrabeculectomy group consisted of OAG and ACG subgroups. The AL was longer in the OAG subgroup than in the control or ACG subgroup (24.6 ± 1.7 mm vs. 23.6 ± 1.6 mm vs. 22.8 ± 0.7 mm, P < 0.001), whereas the preoperative ACD was shallower in ACG than in the control or OAG (2.43 ± 0.31 µm vs. 2.99 ± 0.54 µm vs. 3.28 ± 0.38 µm, P < 0.001). ΔIOP was in the (highest to lowest) order of ACG, OAG, and control group (21.1 ± 12.7 mmHg vs. 9.5 ± 6.7 mmHg vs. 2.1 ± 2.6 mmHg, P < 0.001). The prediction errors were −0.41 ± 0.51 Diopters in OAG and −0.12 ± 0.62 in ACG, neither of which statistically differed from the control group (P = 0.077). In the multiple regression analysis, the prediction error showed statistical significance with AL (P = 0.002) and a marginal significance with preoperative ACD (P = 0.056, Table 4, Figure 1, Video S1).
4. Discussion
In this study, we discovered that absolute prediction error was larger in the phacotrabeculectomy group than in the phacoemulsification group. Longer AL and larger IOP change were the risk factors for higher absolute prediction error. Hyperopic shift (= positive value of prediction error) was associated with shallower preoperative ACD and larger IOP change, both of which were more common in ACG eyes. In the phacotrabeculectomy group, the prediction error showed an inverse correlation with AL, which means that eyes with long AL showed myopic shift while eyes with short AL showed hyperopic shift. To the best of our knowledge, this study is the first to compare prediction errors after phacotrabeculectomy and phacoemulsification using the Barrett Universal II formula, which incorporates both ACD and AL as measured preoperatively.
Final refractive errors can be either myopic (= negative value of prediction error) or hyperopic (= positive value of prediction error) by prediction. The phacotrabeculectomy group had larger deviations from the prediction in both myopic and hyperopic shift cases, and thus, averaging them would have concealed the actual refractive errors; this is why we used the absolute value of prediction error. Several studies also have reported worse refractive outcomes when phacoemulsification and trabeculectomy were performed simultaneously [12,13,15,17]. In the current study, AL and larger IOP change were both associated with larger prediction error. We speculated that the final refractive error would be affected more in the phacotrabeculectomy group, since AL and IOP presumably would have changed more after phacotrabeculectomy.
AL is known to be shortened after either trabeculectomy [7,9,10,20] or phacotrabeculectomy [11], and extent of AL decrease is correlated with amount of IOP reduction [7,10,11,20]. Although AL shortening also has been reported after phacoemulsification alone, AL shortening was more prominent after phacotrabeculectomy in that study [11]. Accordingly, postoperative AL would deviate more from preoperative AL in phacotrabeculectomy than in phacoemulsification. Since the IOL power calculation formulas were developed based on phacoemulsification data, their predictions would be less accurate in phacotrabeculectomy cases. Notably, Lee et al. reported a post-trabeculectomy association between prediction error and IOP change [13]. We speculated that large IOP change would be associated with greater AL shortening, which would result in more prediction error in phacotrabeculectomy.
Several studies, however, have reported that prediction error did not differ between phacotrabeculectomy and phacoemulsification [11,14,16]. These studies calculated prediction error using the SRK II formula (if AL ≤ 26 mm) and SRK/T formula (if AL > 26 mm) [14] or the average of the SRK/T, Holladay 1, and Hoffer Q formulas [11]. As third-generation formulas, all of them (SRK/T, SRK II, Holladay 1, Hoffer Q) use only AL and keratometry values in their IOL power calculation, under the assumption that the effective lens position is directly related to AL [18,21]. We speculated that the non-applicatoin of ACD might have been the reason for the lack of intergroup difference in those studies. In the OAG eyes with high preoperative IOP, the preoperative ACD might have been over-measured due to stasis of aqueous humor in the anterior chamber. If so, the actual effective lens position after phacotrabeculectomy would have been more anteriorly located than the effective lens position calculated from the preoperative ACD, resulting thereby in myopic shift. Contrastingly, in ACG eyes with shallow ACD, the actual effective lens position after phacotrabeculectomy would be more posteriorly located due to anterior chamber deepening, thus resulting in hyperopic shift. To summarize, prediction errors might occur even with the use of fourth-generation formulas, since these measure not only the AL but also many other parameters, including ACD, for more accurate determination of effective lens position.
Prediction error also is dependent on the applied formula, since it is well known that the accuracy of each formula is dependent on the AL range [21,22]. For consistency of comparison, however, it would be better to use a singular IOL calculation formula. Superiority of the Barrett Universal II formula over SRK/T formula was proven in phacotrabeculectomy cases [23]. Thus, we used the Barrett Universal II formula, which is considered to be one of the best options for covering the entire AL range [19,24]. By this means, we demonstrated worse refractive outcomes in the phacotrabeculectomy group over the entire range of AL.
Interestingly, our phacoemulsification group also showed a myopic shift of −0.3 Diopters. One possible explanation is twofold. First, AL shortening also was noted after phacoemulsification only [11]. This change may vary among individuals, since it might be associated with tissue properties, as supported by a previous study showing that eyes with differing corneal hysteresis showed differing AL shortening after trabeculectomy [25]. Thus, comparison of populations with different tissue properties would lead to slight myopic shifts from predictions. The second part of our tentative explanation for the myopic shift in the phacoemulsification group is the difference in crystalline lens anatomy among individuals. The geometric center of the crystalline lens is located anteriorly to the exact half point along the lens thickness: that is, there is more convexity to the posterior side than to the anterior side [26]. Thus, the effective lens position might be also located more anteriorly than the calculated position after phacoemulsification. Moreover, this anterior/posterior difference of lens shape is affected by both thickness and age [26]. Further study accounting for these factors would be helpful in order to reduce refractive errors after either phacotrabeculectomy or phacoemulsification.
This study has several limitations. First, the sample size was relatively small and not evenly distributed along the whole range of AL. Second, due to the retrospective nature of the study, the applied treatment protocol in the phacotrabeculectomy group (e.g., preoperative anti-glaucoma medications) might have differed among patients. Third, we were unable to obtain postoperative AL and ACD for comparison. Further prospective longitudinal study would be helpful in order to evaluate the effect of ocular biometry changes on final refractive outcomes after phacotrabeculectomy. Fourth, the follow-up period was short: the final refractive errors were determined at postoperative one month. Although several studies have reported that refractive error was stabilized one week after phacoemulsification [27,28], it is unknown whether the same would be true after phacotrabeculectomy [29,30]. Some post-phacotrabeculectomy patients have shown unstable refractive errors when followed up for longer periods [29]. Chung et al. however, reported non-difference of long-term refractive outcomes between phacotrabeculectomy and phacoemulsification groups [30]. Nevertheless, it should be noted that refractive error could change with IOP change, especially in glaucoma patients who had undergone phacotrabeculectomy and been followed up longer. Fifth and finally, we were unable to suggest a better way to minimize prediction error. Simply, we categorized high-risk patients of worse refractive outcome, and part of prediction error might originate from the disease such as ACG from phacotrabeculectomy itself. Our results, however, may be helpful to clinicians who are planning surgery by noticing them the high-risk patients of worse refractive outcomes regardless of the reasons. Future study should focus on such patients in order to find a means of achieving better refractive outcomes.
In conclusion, refractive prediction error was larger in phacotrabeculectomy than in phacoemulsification cases. Such inaccuracies may accrue from AL and IOP changes, both of which resulted in changes of effective lens position. Surgeons therefore should be aware of the possibility of worse refractive outcomes when planning phacotrabeculectomy in eyes with high preoperative IOP, shallow ACD, and/or extreme AL.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Video S1: Three-dimensional scatter plot of whole data set allowing for rotation and zooming for close inspection.
Author Contributions
J.H.S and K.M.L contributed to the design, data collection and analysis, writing, and editing the manuscript; S.H.K contributed to review of the manuscript; S.H.O contributed to data interpretation and analysis. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI22C0786). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
This retrospective comparative study was conducted following the tenets set forth in the Declaration of Helsinki, and was approved by the Institutional Review Board of Seoul National University Boramae Medical Center.
Data Availability Statement
The data generated during this study are available from the corresponding author on reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to vision 2020: The right to sight: An analysis for the global burden of disease study. Lancet Glob Health 2021, 9, e144–e160. [CrossRef]
- Krupin, T.; Feitl, M.E.; Bishop, K.I. Postoperative intraocular pressure rise in open-angle glaucoma patients after cataract or combined cataract-filtration surgery. Ophthalmology 1989, 96, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Murchison, J.F., Jr.; Shields, M.B. Limbal-based vs. fornix-based conjunctival flaps in combined extracapsular cataract surgery and glaucoma filtering procedure. Am J Ophthalmol 1990, 109, 709–715. [Google Scholar] [CrossRef]
- Vaideanu, D.; Mandal, K.; Hildreth, A.; Fraser, S.G.; Phelan, P.S. Visual and refractive outcome of one-site phacotrabeculectomy compared with temporal approach phacoemulsification. Clin Ophthalmol 2008, 2, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.; Li, E.Y.; Tsoi, K.K.F.; Kwong, Y.Y.; Tham, C.C. Cost-effectiveness of phacoemulsification versus combined phacotrabeculectomy for treating primary angle closure glaucoma. J Glaucoma 2017, 26, 911–922. [Google Scholar] [CrossRef] [PubMed]
- El Sayed, Y.M.; Elhusseiny, A.M.; Albalkini, A.S.; El Sheikh, R.H.; Osman, M.A. Mitomycin c-augmented phacotrabeculectomy versus phacoemulsification in primary angle-closure glaucoma: A randomized controlled study. J Glaucoma 2019, 28, 911–915. [Google Scholar] [CrossRef]
- Francis, B.A.; Wang, M.; Lei, H.; Du, L.; Minckler, D.; Green, R.; Roland, C. Changes in axial length following trabeculectomy and glaucoma drainage device surgery. Br J Ophthalmol 2005, 89, 17–20. [Google Scholar] [CrossRef]
- Claridge, K.; Galbraith, J.; Karmel, V.; Bates, A. The effect of trabeculectomy on refraction, keratometry and corneal topography. Eye 1995, 9, 292–298. [Google Scholar] [CrossRef]
- Husain, R.; Li, W.; Gazzard, G.; Foster, P.J.; Chew, P.T.; Oen, F.T.; Phillips, R.; Khaw, P.T.; Seah, S.K.; Aung, T. Longitudinal changes in anterior chamber depth and axial length in asian subjects after trabeculectomy surgery. Br J Ophthalmol 2013, 97, 852–856. [Google Scholar] [CrossRef]
- Kook, M.S.; Kim, H.B.; Lee, S.U. Short-term effect of mitomycin-c augmented trabeculectomy on axial length and corneal astigmatism. J Cataract Refract Surg 2001, 27, 518–523. [Google Scholar] [CrossRef]
- Law, S.K.; Mansury, A.M.; Vasudev, D.; Caprioli, J. Effects of combined cataract surgery and trabeculectomy with mitomycin c on ocular dimensions. Br J Ophthalmol 2005, 89, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.W.; Lee, Y.H.; Kim, D.W.; Lee, T.; Hong, S.; Seong, G.J.; Kim, C.Y. Effect of trabeculectomy on the accuracy of intraocular lens calculations in patients with open-angle glaucoma. Clin Exp Ophthalmol 2016, 44, 465–471. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, C.E.; Park, J.H.; Seo, S.; Lee, K.W. Refractive error induced by combined phacotrabeculectomy. jkos 2018, 59, 1173–1180. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Su, C.-C.; Wang, T.-H.; Huang, J.-Y. Refractive outcomes of cataract surgery in patients receiving trabeculectomy—a comparative study of combined and sequential approaches. J Formos Med Assoc 2021, 120, 415–421. [Google Scholar] [CrossRef]
- Ong, C.; Nongpiur, M.; Peter, L.; Perera, S.A. Combined approach to phacoemulsification and trabeculectomy results in less ideal refractive outcomes compared with the sequential approach. J Glaucoma 2016, 25, e873–e878. [Google Scholar] [CrossRef]
- Tzu, J.H.; Shah, C.T.; Galor, A.; Junk, A.K.; Sastry, A.; Wellik, S.R. Refractive outcomes of combined cataract and glaucoma surgery. J Glaucoma 2015, 24, 161–164. [Google Scholar] [CrossRef]
- Chan, J.C.; Lai, J.S.; Tham, C.C. Comparison of postoperative refractive outcome in phacotrabeculectomy and phacoemulsification with posterior chamber intraocular lens implantation. J Glaucoma 2006, 15, 26–29. [Google Scholar] [CrossRef]
- Olsen, T. Calculation of intraocular lens power: A review. Acta Ophthalmol Scand 2007, 85, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.X.; Van Heerden, A.; Atik, A.; Petsoglou, C. Intraocular lens power formula accuracy: Comparison of 7 formulas. J Cataract Refract Surg 2016, 42, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Cashwell, L.F.; Martin, C.A. Axial length decrease accompanying successful glaucoma filtration surgery. Ophthalmology 1999, 106, 2307–2311. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.X.; Chang, D.F. Intraocular lens power formulas, biometry, and intraoperative aberrometry: A review. Ophthalmology 2021, 128, e94–e114. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Eom, Y.; Yoon, E.G.; Choi, Y.; Song, J.S.; Jeong, J.W.; Park, S.K.; Kim, H.M. Algorithmic intraocular lens power calculation formula selection by keratometry, anterior chamber depth and axial length. Acta Ophthalmol 2022, 100, e701–e709. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K.; Kamiya, K.; Iida, Y.; Kasahara, M.; Shoji, N. Predictability of combined cataract surgery and trabeculectomy using barrett universal ii formula. PLoS One 2022, 17, e0270363. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Holladay, J.T.; Chang, W.J. Accuracy of intraocular lens calculation formulas. Ophthalmology 2018, 125, 169–178. [Google Scholar] [CrossRef]
- Huang, C.; Zhang, M.; Huang, Y.; Chen, B.; Lam, D.S.; Congdon, N. Corneal hysteresis is correlated with reduction in axial length after trabeculectomy. Curr Eye Res 2012, 37, 381–387. [Google Scholar] [CrossRef]
- Haddad, J.S.; Rocha, K.M.; Yeh, K.; Waring, G.O.t. Lens anatomy parameters with intraoperative spectral-domain optical coherence tomography in cataractous eyes. Clin Ophthalmol 2019, 13, 253–260. [Google Scholar] [CrossRef]
- Khan, A.M.; Waldner, D.M.; Luong, M.; Sanders, E.; Crichton, A.; Ford, B.A. Stabilization of refractive error and associated factors following small incision phacoemulsification cataract surgery. BMC Ophthalmol 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Ostri, C.; Holfort, S.K.; Fich, M.S.; Riise, P. Automated refraction is stable 1 week after uncomplicated cataract surgery. Acta Ophthalmol (Copenh) 2018, 96, 149–153. [Google Scholar] [CrossRef]
- Kang, Y.S.; Sung, M.S.; Heo, H.; Ji, Y.S.; Park, S.W. Long-term outcomes of prediction error after combined phacoemulsification and trabeculectomy in glaucoma patients. BMC Ophthalmol 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Chung, J.K.; Wi, J.M.; Lee, K.B.; Ahn, B.H.; Hwang, Y.H.; Kim, M.; Jung, J.J.; Yoo, Y.C. Long-term comparison of postoperative refractive outcomes between phacotrabeculectomy and phacoemulsification. J Cataract Refract Surg 2018, 44, 964–970. [Google Scholar] [CrossRef]
Figure 1.
Scatter plot of prediction errors (based on the Barrett Universal ll formula) according to axial length (AL) and anterior chamber depth (ACD). The red dots indicate angle-closure glaucoma (ACG) patients, the blue dots open-angle glaucoma (OAG) patients, and the green dots control patients who had undergone phacoemulsification only. In the three-dimensional plot (left), intraocular pressure (IOP) change is marked by sphere size: large sphere, ΔIOP ≥ 10 mmHg; small sphere, ΔIOP ≤ 10 mmHg. The regression lines are drawn for AL (right top) and ACD (right bottom). Please note the larger prediction error in the OAG and ACG patients who had undergone phacotrabeculectomy: OAG patients with long AL showed myopic shift, while ACG patients with short ACD showed hyperopic shift. Prediction error was larger in cases with remarkable IOP change.
Figure 1.
Scatter plot of prediction errors (based on the Barrett Universal ll formula) according to axial length (AL) and anterior chamber depth (ACD). The red dots indicate angle-closure glaucoma (ACG) patients, the blue dots open-angle glaucoma (OAG) patients, and the green dots control patients who had undergone phacoemulsification only. In the three-dimensional plot (left), intraocular pressure (IOP) change is marked by sphere size: large sphere, ΔIOP ≥ 10 mmHg; small sphere, ΔIOP ≤ 10 mmHg. The regression lines are drawn for AL (right top) and ACD (right bottom). Please note the larger prediction error in the OAG and ACG patients who had undergone phacotrabeculectomy: OAG patients with long AL showed myopic shift, while ACG patients with short ACD showed hyperopic shift. Prediction error was larger in cases with remarkable IOP change.
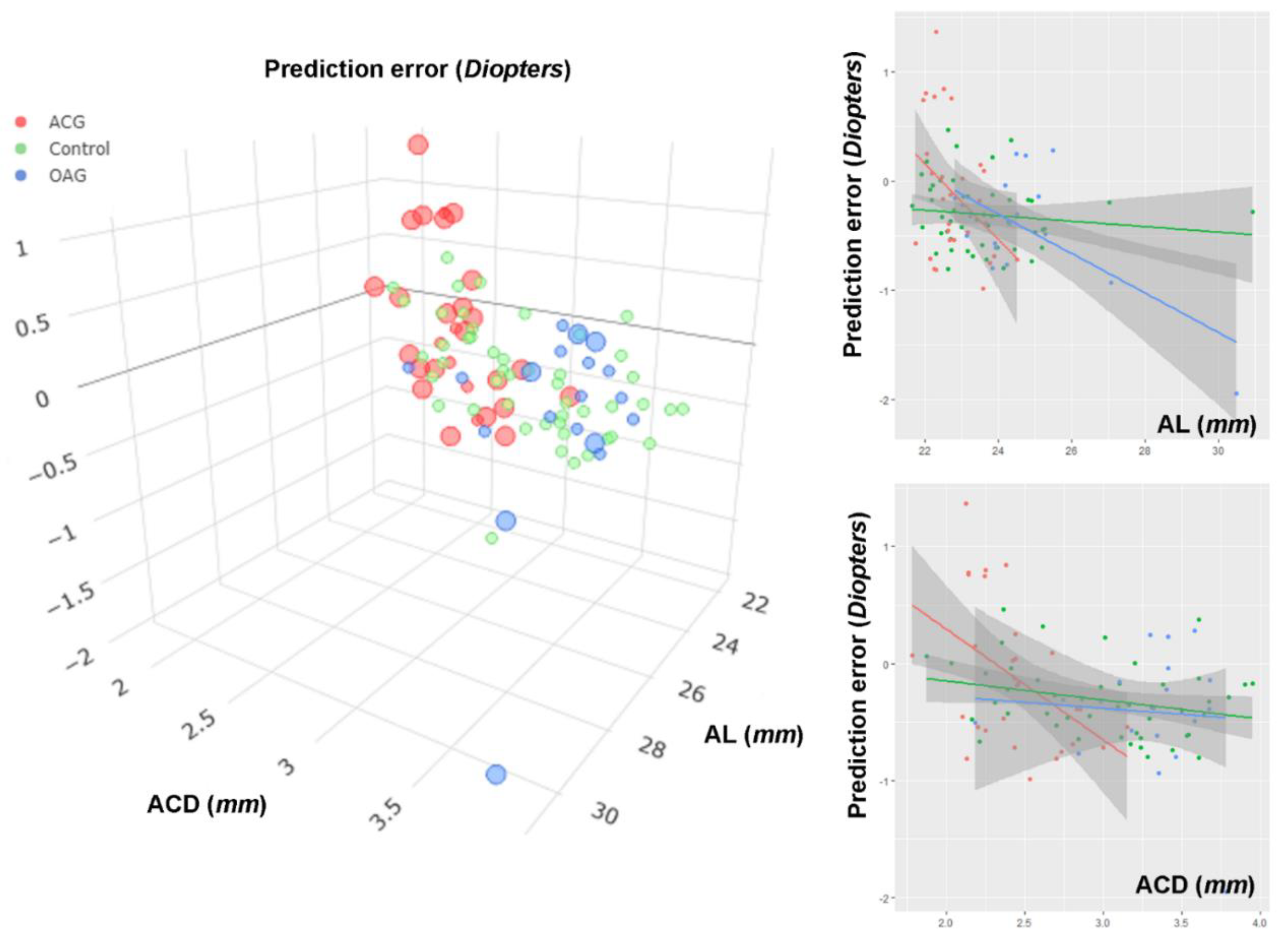

Table 1.
Demographic comparison.
| Phacotrabeculectomy (N = 48) |
Phacoemulsification (N = 48) |
P value | |
|---|---|---|---|
| Age, years | 66.1 ± 11.1 | 68.9 ± 10.0 | 0.198 a |
| Sex (Male/Female) | 19/29 | 20/28 | 0.835 b |
| AL, mm | 23.5 ± 1.5 | 23.6 ± 1.6 | 0.814 a |
| ACD, µm | 2.77 ± 0.54 | 2.99 ± 0.54 | 0.047 a |
| Average K, Diopter | 44.3 ± 1.6 | 44.4 ± 1.4 | 0.722 a |
| Preoperative IOP, mmHg | 27.6 ± 11.5 | 13.0 ± 3.9 | <0.001 a |
| ΔIOP, mmHg | 16.5 ± 12.1 | 2.1 ± 2.6 | <0.001 a |
| Prediction error, Diopter | −0.23 ± 0.59 | −0.31 ± 0.31 | 0.436 |
| Absolute prediction error, Diopter | 0.51 ± 0.37 | 0.38 ± 0.22 | 0.033 |
| Diagnosis | OAG (39.6%) ACG (60.4%) |
AL = axial length; ACD = anterior chamber depth; IOP = intraocular pressure; OAG = open-angle glaucoma; ACG = angle-closure glaucoma. a Comparison performed using independent-t test; b Comparison performed using Chi-square test.
Table 2.
Factors associated with absolute prediction error.
| Univariable analysis | Multivariable analysis (Model 1) a | Multivariable analysis (Model 2) a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | P | Coefficient | 95% CI | P | Coefficient | 95% CI | P | |
| Age, years | −0.001 | −0.007, 0.005 | 0.765 | ||||||
| Female (vs. male sex) | −0.062 | −0.190, 0.066 | 0.341 | ||||||
| AL, mm | 0.046 | 0.006, 0.087 | 0.026 | 0.053 | 0.013, 0.092 | 0.010 | 0.047 | 0.008, 0.087 | 0.020 |
| ACD, µm | 0.031 | −0.086, 0.148 | 0.598 | ||||||
| Average K, Diopter | −0.009 | −0.051, 0.034 | 0.694 | ||||||
| ΔIOP, mmHg | 0.006 | 0.001, 0.012 | 0.030 | 0.007 | 0.002, 0.012 | 0.012 | |||
| Phacotrabeculectomy (vs. control group) | 0.135 | 0.011, 0.258 | 0.033 | 0.138 | 0.018, 0.259 | 0.025 | |||
CI = confidence interval; AL = axial length; ACD = anterior chamber depth; IOP = intraocular pressure; a Variables with P < 0.10 in the univariable analysis were included in the subsequent multivariable analysis. Owing to multicollinearity between the groups and ΔIOP, two multivariable analysis models were constructed. The result of multivariable analysis with backward elimination was equivalent to that of Model 1. Statistically significant values (P < 0.05) are shown in bold.
Table 3.
Risk factors for hyperopic prediction error.
| Univariable analysis | Multivariable analysis (Model 1) a | Multivariable analysis (Model 2) a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| Age, years | 1.030 | 0.982, 1.081 | 0.220 | ||||||
| Female (vs. male sex) | 1.784 | 0.655, 4.856 | 0.257 | ||||||
| AL, mm | 0.570 | 0.341, 0.953 | 0.032 | 0.637 | 0.380, 1.067 | 0.087 | |||
| ACD, µm | 0.180 | 0.062, 0.517 | 0.001 | 0.277 | 0.091, 0.842 | 0.024 | |||
| Average K, Diopter | 1.186 | 0.862, 1.631 | 0.296 | ||||||
| ΔIOP, mmHg | 1.072 | 1.028, 1.118 | 0.001 | 1.066 | 1.021, 1.113 | 0.004 | 1.051 | 1.005, 1.099 | 0.031 |
CI = confidence interval; AL = axial length; ACD = anterior chamber depth; IOP = intraocular pressure; a Variables with P < 0.10 in the univariable analysis were included in the subsequent multivariable analysis. Because of multicollinearity between AL and ACD, two models were constructed. The result of multivariable analysis with backward elimination was equivalent to that of Model 2. Statistically significant values (P < 0.05) are shown in bold.
Table 4.
Factors associated with prediction error after phacotrabeculectomy.
| Univariable analysis | Multivariable analysis (Model 1) a |
Multivariable analysis (Model 2) a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | P | Coefficient | 95% CI | P | Coefficient | 95% CI | P | |
| Age, years | 0.007 | −0.008, 0.023 | 0.359 | ||||||
| Female (vs. male sex) | 0.402 | 0.068, 0.736 | 0.019 | 0.146 | −0.206, 0.498 | 0.407 | 0.296 | −0.063, 0.654 | 0.103 |
| AL, mm | −0.195 | −0.297, −0.094 | <0.001 | −0.213 | −0.346, −0.080 | 0.002 | |||
| ACD, µm | −0.418 | −0.720, −0.115 | 0.008 | −0.472 | −0.957, 0.013 | 0.056 | |||
| Average K, Diopter | 0.064 | −0.043, 0.171 | 0.236 | ||||||
| ΔIOP, mmHg | 0.012 | −0.002, 0.026 | 0.084 | 0.011 | −0.004, 0026 | 0.133 | 0.005 | −0.011, 0.020 | 0.556 |
| ACG (vs. OAG) | 0.294 | −0.049, 0.638 | 0.091 | −0.277 | −0.709, 0.155 | 0.203 | −0.273 | −0.814, 0.268 | 0.315 |
CI = confidence interval; AL = axial length; ACD = anterior chamber depth; IOP = intraocular pressure; ACG = angle-closure glaucoma; OAG = open-angle glaucoma; a Variables with P < 0.10 in the univariable analysis were included in the subsequent multivariable analysis. Because of multicollinearity between AL and ACD, two models were constructed. Multivariable analysis with backward elimination left only AL as the associative factor. Statistically significant values (P < 0.05) are shown in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



