
Submitted:
28 July 2023
Posted:
31 July 2023
You are already at the latest version
Abstract
Non-small-cell lung cancer (NSCLC) is the second most common cancer worldwide, resulting in 1.8 million deaths/year. Most of the patients are diagnosed with a metastatic disease. Central Nervous System is one of the major metastatic sites. Brain metastases are associated with severe neurological symptoms, shorter survival and worst clinical outcomes. Brain radiotherapy and systemic oncological therapies are currently used for controlling both cancer progression and neurological symptoms. Brain radiotherapy includes stereotactic brain ablative radiotherapy (SBRT) or whole brain radiotherapy (WBRT). SBRT is applied for single or multiple (≤ 4) small lesions (< 3 cm), while WBRT represents the best treatment choice in case of multiple and large brain metastases. In both cases radiotherapy application can represent an overtreatment causing severe toxicities without achieving a significant clinical benefit. So far, some scores have been proposed to define the potential clinical benefits derived from brain radiotherapy. However, most of them are not well validated into clinical practice. In this article, by presenting a clinical case of a patient with advanced NSCLC carrying a BRAFV600E mutation and brain metastases, we review the variables as well as the potential applicable scores to be considered in order to predict clinical outcomes and benefits from brain radiotherapy in patients with NSCLC and brain metastases.
Keywords:
brain metastases
; NSCLC
; predictive biomarkers for radiotherapy
; radiotherapy
; prognostic scores
; WBRT
; BRAF mutation
1. Introduction
Non-small-cell lung cancer (NSCLC) is the second most common cancer worldwide, resulting in 2 million diagnoses and 1.8 million deaths per year [1,2]. The most important risk factor for NSCLC is cigarette smoke because of its carcinogenic chemicals [3]. This risk increases to the number of cigarettes smoked per day as well as per years spent in smoking; other well-known risk factors are asbestos, radon and silica exposure [3]. There are different histologic subtypes of NSCLC including squamous cell carcinoma, adenocarcinoma, adeno-squamous carcinoma, large-cell carcinoma and NSCLC not otherwise specified (NOS) [4]. Types of NSCLC are also classified in oncogene or non-oncogene addicted based on the presence/absence of specific tumor alterations [5,6]. The former includes tumors carrying KRAS (20-30%), EGFR (10-15%), ALK (3-7%), BRAF (2-4%), cMET (2-4%), ROS1 (1-2%), RET (1-2%), HER2 (1-2%) and NTRK (0.5-1%) alterations [5,6]. Treatment of NSCLC includes surgery, chemotherapy, targeted therapy, immunotherapy and radiotherapy. Surgery with tumor resection represents the primary treatment for stage I and II NSCLC [3,7,8] while for stage III disease it is an important component of the multimodality approach in association with radiotherapy and chemotherapy [3,9]. Chemotherapy can include the combination of platinum derivatives (cisplatin or carboplatin) with other cytotoxic agents such as gemcitabine, paclitaxel, pemetrexed, nab-paclitaxel and vinorelbine as well as use of single chemotherapeutic agents both in early and advanced disease [3,10,11,12,13]. Targeted therapy with tyrosine kinase inhibitors is only applicable to small subset of patients carrying oncogene alterations. It currently includes KRASG12C inhibitors (sotorasib and adagrasib [14,15]), EGFR inhibitors (first-generation: erlotinib and gefitinib; second-generation: afatinib and dacomitinib; third-generation: osimertinib) [16,17,18,19,20,21,22], ALK inhibitors (first-generation: crizotinib; second-generation: alectinib, brigatinib, ceritinib, and ensartinib; third-generation: lorlatinib) [23,24,25,26,27,28], BRAF inhibitors (dabrafenib) [29], cMET inhibitors (capmatinib and tepotinib) [30,31], ROS1 inhibitors (first-generation: crizotinib; second-generation: entrectinib) [32,33], RET inhibitors (pralsetinib and selpercatinib) [34,35], HER 2 targeting agents (trastuzumab deruxtecan) [36] and NTRK inhibitors (entrectinib and larotrectinib) [37,38]. Immunotherapy with immune checkpoint inhibitors (ICIs) such as anti-programmed cell death-1 (PD-1) (cemiplimab, nivolumab and pembrolizumab) [39,40,41,42,43,44,45,46], anti-programmed death-ligand 1 (PD-L1) (atezolizumab and durvalumab) [47,48,49] and anti-cytotoxic T-lymphocyte antigen-4 (CTLA-4) (ipilimumab) [42] is revolutionizing the treatment landscape of non-oncogene addicted NSCLC, being utilized as a single agent or in combination with chemotherapy in both early and advanced stage of the disease [39,40,41,42,43,44,45,46,47,48,49,50,51,52,53]. Lastly, radiotherapy is currently used either with a radical intent, in combination with chemotherapy for treatment of primary tumors, or as a single agent with palliative intent, for treatment of bone or brain metastases [3,9,54,55,56,57,58]. The latter represent a major site of the metastatic disease [59,60,61] and are consequence of a complex process that includes induction of angiogenesis, malignant cell blood dissemination, extravasation, proliferation and survival [62]. Brain radiotherapy is administrated either as stereotactic ablative radiotherapy (SBRT) or as whole brain radiotherapy (WBRT), based on patient and tumor characteristics [56,58,63,64,65,66]. SBRT delivers a high dose to limited size targets, representing a reasonable strategy for patients not candidate to surgery in presence of 1 to 4 brain metastases < 3 cm. On the other hand, WBRT is the best choice in case of multiple and large brain metastases [56,58,63,64,65,66]. In both cases, radiotherapy is utilized both to relieve neurological symptoms and to inhibit tumor progression but its limited efficacy and derived neurotoxicity can lead to select best supportive care as a valid alternative option [58,67,68,69]. As a result, there is the need to define potential biomarkers which can help to identify patients who can really benefit from brain radiotherapy, avoiding useless treatments. So far, some scoring systems have been proposed [70,71,72]. Here, by presenting the clinical outcomes obtained from WBRT in a patient with brain metastases from an advanced NSCLC carrying a BRAFV600E mutation, we analysed the potential variables as well as the available scoring systems useful to predict clinical outcomes and benefits from brain radiotherapy in patients with NSCLC and brain metastases.
2. Case Presentation
In January 2023, a 62-year-old Caucasian male, no smoker, went to first aid of University Hospital "San Giovanni di Dio e Ruggi d'Aragona” because of dyspnea, visual impairments and dizziness. His neurological syndrome got worse in a few hours. Radiological evaluation with CT scan demonstrated presence of multiple brain metastases localized in the left frontal, right frontoparietal and occipital lobes as well as in the right cerebellar hemisphere. Massive edema, compression of cerebellum, right lateral ventricle and subfalcine herniation were also described (Figure 1a,b). Other tumor localizations included presence of a large mass in the right-upper lung lobe and multiple lymph nodal, liver (10mm) and spleen (30 mm) metastases (Figure 1c,d).
Basal tumoral markers were in normal range, except neuron-specific enolase (NSE) (14.9 ng/ml). Baseline ECG showed sinus rhythm at 82 bpm and a QTc of 425 ms. Blood pressure was 125/80 mmHg and SpO2 was 98%. According to brain metastasis localization, the patient had pyramidal syndrome, numbness, ocular ptosis, spastic paraplegia and aphasia, neurocognitive decline and loss of self-care. Analysis of biohumoral parameters demonstrated a significant increase of lactate dehydrogenase (LDH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), iron, ferritin, bilirubin (especially non-direct index), blood urea and glycemic levels while those of albumin, transferrin, sodium, potassium and calcium were reduced. Blood count was normal. Eastern Cooperative Oncology Group Performance Status (ECOG PS) was 3. Karnofsky performance status (KPS) was 40%. Supportive care was immediately started with administration of dexamethasone 8 mg every 8 hours, mannitol 18% every 6 hours and levetiracetam 500 mg bid. Following 4 days of treatment support, the patient gained a little benefit in neurological symptomatology and a percutaneous CT-assisted lung biopsy was performed. Following 7 days, tumor histopathological analysis confirmed the diagnosis of lung adenocarcinoma with PD-L1 tumor proportion score (TPS) between 1 and 49%. Based on better neurological symptoms and clinical conditions WBRT was immediately started (30 Gy in 10 fractions). During the following 7 days from the end of radiotherapy, molecular analysis of tumor biopsy demonstrated the presence of BRAFV600E mutation. Based on this result, the patient was candidate to BRAF and MEK inhibitor combination with dabrafenib and trametinib. However, at same time, neurological symptoms got worse with development of pyramidal syndrome, ocular ptosis, spastic paraplegia, aphasia, neurocognitive decline and inability to swallow. As a result, dabrafenib and trametinib were not started. Comparison of biohumoral parameters with those of pre-radiotherapy treatment demonstrated a decrease in hemoglobin (HGB) levels, red blood cell (RBC) and platelet (PLT) count (11.4 g/dl vs 14.1 g/dl for HGB; 7.42 x 106/µl vs 6.02 x 106/µl for RBC and 282 x 103/µl vs 161 x 103/µl for PLT), while white blood cell (WBC), neutrophil (NEU) count and NEU-to-lymphocyte ratio (NLR) were increased (25.3 x 103/µl vs 17.14 x 103/µl for WBC, 24.14 x 103/µl vs 16.02 x 103/µl for NEU and 34 vs 54 for NLR). Cardiac evaluation showed a progressive elevation of heart rate (maximum value of 179 bpm), atrial flutter development and alterations in ST trait. Tumoral markers were higher than basal (Ca 125 was 49.9 U/ml vs 26.6 U/ml and Ca 19.9 was 36.6 U/ml vs 19 U/ml). Unfortunately, following 6 days, despite of specific cardiologic treatment, clinical conditions got worse, and patient died.
3. Discussion
SBRT and WBRT play a major role in the treatment of brain metastases. WBRT represents the best choice of treatment in case of multiple and large brain metastases, regardless of tumor type. In NSCLC, WBRT has been shown to improve both neurological symptoms and disease control [60,63,73]. Nevertheless, WBRT is also associated to temporary or persistent toxicity [58,64,74]. The former includes alopecia, dermatitis, fatigue, otitis, nausea and alterations in both memory and executive functions [63,64,75]. Persistent toxicity includes impaired physiological function of hippocampus, ataxia, insomnia, dysphasia and dementia [64,74,76,77,78,79]. WBRT toxicity can be reduced by exclusion of selective brain areas such as the hippocampus, leading to an improvement of neurocognitive function, functional autonomy and quality of life [64,75,80]. In the case we have described, WBRT included the hippocampus area, severe toxicities were reported, and no clinical benefit was achieved. Brain metastases were derived from a NSCLC carrying a BRAFV600E mutation. In this type of tumor, administration of BRAF and MEK inhibitors has demonstrated to improve both overall survival and response rate, even in presence of brain metastases [29]. However, to the best of our knowledge, no clinical study has evaluated the intracranial efficacy of BRAF and MEK inhibitor combination in BRAFV600E NSCLC patients with multiple symptomatic brain metastases. In contrast, several preclinical and clinical studies have been investigating the combination of BRAF inhibitor and radiotherapy as well as of BRAF and MEK inhibitors in melanoma patients carrying similar alterations in BRAF, even in presence of multiple brain metastases. [81,82,83,84,85,86]. It has been shown that aberrant activation of RAS/BRAF pathway in melanoma cells increases the resistance to radiations while its inhibition restores the radio-sensitization of cancer cells [84,87,88]. In addition, Sambade et al. have demonstrated a synergistic effect of BRAF inhibitor and radiation in melanoma cell death through an increase in G1 arrest of cancer cells, laying the basis for combinatorial therapeutic approach [89]. Unfortunately, even in melanoma patients, the combination of BRAF inhibitor and radiation has been limited by a significantly increase of severe toxicities [90,91,92,93,94,95,96,97,98]. As a result, BRAF inhibitors are administered before or later WBRT. On the other hand, several lines of evidence have demonstrated a relevant clinical benefit obtained by BRAF and MEK inhibitors in melanoma patients carrying BRAFV600E [82,99,100]. In this setting, BRAF and MEK inhibitor combination induces 68% of intracranial disease control rate (stable disease, partial response and complete response of 37%, 26% and 5%, respectively) [101]. Further studies are needed to validate the efficacy of the combination of BRAF and MEK inhibitors in NSCLC patients carrying BRAFV600E mutation with brain metastases.
Besides BRAF and MEK inhibitors, in our case, the combination of chemotherapy and anti-PD-1-based immunotherapy could represent an alternative therapeutic approach. In the definition of the best therapeutic algorithm, one should take into account that besides oncogene alterations PD-L1 tumor expression plays a major role for treatment choice in advanced NSCLC patients [42,45,46]. As a result, in the patient we have described, according to PD-L1 tumor expression, platinum-based chemotherapy and anti-PD-based immunotherapy could represent an alternative therapeutic option. This therapeutic approach has clearly demonstrated to improve both response rate and survival outcomes of treated patients as compared to standard platinum-based chemotherapy [45,46]. However, so far, no study has compared which is the most effective therapeutic approach in NSCLC patients and no study testing sequential strategies such as BRAF and MEK inhibitor combination as compared to the combination of immunotherapy and chemotherapy in NSCLC patients carrying BRAFV600E is available. In BRAFV600E melanoma patients, two recent clinical studies have shown that presence of BRAFV600E mutation may influence the best therapeutic sequence in advanced melanoma. Specifically, a major benefit is achieved from an up-front immunotherapy as compared to up-front BRAF and MEK inhibitor combination [102,103]. In the clinical case we have described administration of chemotherapy and anti-PD-1-based immunotherapy was limited by i) availability of clinical data in the setting of patients carrying BRAFV600E with symptomatic brain metastases; ii) detrimental effect of high dose steroids on the efficacy of anti-PD-1 therapy; iii) the clinical conditions of the patient (PS ECOG 3, KPS 3); and iv) Italian guideline indications that limits administration of platinum-based chemotherapy and anti-PD-1 therapy following failure to prior BRAF and MEK inhibitor combination. One could expect that based on the faster activity the combination of BRAF and MEK inhibitors should represent the best therapeutic option in this specific subgroup of patients. Further prospective studies are needed to clarify this specific aspect.
In our case, we did not promptly start BRAF and MEK inhibitor combination since tumor oncogene analysis was still pending. We promptly started WBRT just following histological tumor analysis because of neurological symptoms. As a result, we were unable to assess the potential tumor brain response and clinical benefit deriving from sequential strategies of targeting agents and radiotherapy. In any case, WBRT alone did not provide any clinical benefit, severe toxicities were developed and BRAF and MEK inhibitors were not then administrated. Based on the obtained results, one might suppose that best supportive care could be a valid alternative option to WBRT. So far, some score systems have been proposed to predict clinical outcomes from WBRT in patients with brain metastases. They include the Radiation Therapy Oncology Group–Recursive Partitioning Analysis (RTOG-RPA) and the WBRT-30-NSCLC scores [71,104]. The RTOG-RPA score is a statistical methodology which creates a regression tree according to prognostic significance. For its validation, both pre-treatment and treatment-related variables were analyzed [104] (Table 1).
Among all the prognostic variables identified (Table 2), three RPA classes were defined.
In the first class were included patients who had KPS ≥ 70, age < 65 years and no extracranial disease. In the second were included patients with a KPS ≥ 70 and at least one unfavorable prognostic factor. The last group included patients with a KPS < 70. According to this score, an increased survival from WBRT for brain metastases was obtained only patients in first class [104]. In contrast no benefit was achieved in patients with a KPS ≤ 70 and higher tumor burden.
The second score system, the WBRT-30-NSCLC score was developed for patients with intracerebral metastases from NSCLC. Eight factors were investigated in NSCLC patients receiving WBRT including age, gender, KPS, interval from diagnosis of NSCLC to WBRT, pre-WBRT systemic treatment, primary tumor control, number of intracerebral metastases, and metastasis outside the brain (Table 3) [71]. Among the variables analyzed, age, KPS, systemic treatment and metastasis outside the brain were found to correlate with 6-month patient survival.
Then for each identified prognostic variable a score was assigned (Table 4) and 4 groups of patients were identified with 6-month survival rates of 3, 26, 65, and 100% [71].
Patients with a score of 9–10 points were proposed to be treated with a short-course WBRT because their survival was poor, while NSCLC patients with a score of 17–18 points should receive long-course WBRT, being their survival longer [71]. Whether we compare these scores the WBRT-30-NSCLC score appears to be more accurate for NSCLC as it identifies patients with intracerebral metastases from NSCLC who will die within 6 months or survive longer. However, both scoring systems display some limitations. First, they both do not distinguish between WBRT with hippocampal inclusion from that with hippocampal exclusion. Second, both scores do not consider the biological and molecular features of tumors as well as evaluation of biohumoral parameters of NSCLC patients. Exclusion of hippocampal area from radiotherapy field has a lower impact on neurological declines and preserves memory and concentration. On the other hand, evaluation of biohumoral parameters can help to identify patients with short lifespan. In our case, we did not apply any of the scoring systems available. Analysis of class risk score by both scoring systems shows a poor risk class for both RTOG-RPA and WBRT-30-NSCLC. As a result, although the patient was affected from a BRAFV600E NSCLC with multiple sites of metastasis (brain, spleen, and liver), both scoring systems were efficient in predicting no clinical benefit from WBRT. Currently no scoring systems are available for this type of patient as well as for other types of oncogene addicted tumors. Further studies are needed to grant personalized radiotherapy treatment for this patient population. In our case, besides the clinical features analyzed in both scoring systems, we also detected a progressive heart failure, an elevation of tumoral markers, a lowering of serum hemoglobin levels, an increasing of platelet count and a worsening of liver and renal function. These parameters should also be considered since they may help to identify an imminent exitus of the patient and therefore no benefit from WBRT. Among these parameters, NLR might be one of the best candidates as prognostic and/or predictive factor. Indeed, two studies have already demonstrated that high values of both pre-treatment and post-treatment NLR predict for poor survival in NSCLC patients brain metastases treated with SBRT or WBRT [105,106]. In our patient both pre-treatment and post-treatment NLRs were extremely high and correlated with poor prognosis and with no benefits from WBRT. However, to validate the prognostic/predictive role of these parameters including NLR, further studies in the specific subset of NSCLC patients with brain metastases carrying BRAFV600E mutation treated with WBRT are needed. Lastly, beyond the value of the specific parameters, our case report seems to suggest that a rapid worsening of these parameters may be the best factor to predict which patients have the worst prognosis. In these conditions as well as for poor risk classes from RTOG-RPA and WBRT-30-NSCLC scores, best supportive care should lead to select best supportive care as a valid alternative option in order to avoid a useless treatment.
Author Contributions
Conception and design: A.L. and F.S.; Writing—review and/or revision of the manuscript: A.L., L.L., G.P., F.S.; Study supervision: S.P. Other (discussed results and implications of findings): F.S., S.P. All authors have read and agreed to the published version of the manuscript.
Funding
None.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
The authors wish to gratefully acknowledge the patient and his family for allowing us to publish his clinical case.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ricotti, A.; Sciannameo, V.; Balzi, W.; Roncadori, A.; Canavese, P.; Avitabile, A.; Massa, I.; Berchialla, P. Incidence and Prevalence Analysis of Non-Small-Cell and Small-Cell Lung Cancer Using Administrative Data. Int. J. Environ. Res. Public Heal. 2021, 18, 9076. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA: A Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-Small Cell Lung Cancer: Epidemiology, Risk Factors, Treatment, and Survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Ferrara, M.G.; Di Noia, V.; D’argento, E.; Vita, E.; Damiano, P.; Cannella, A.; Ribelli, M.; Pilotto, S.; Milella, M.; Tortora, G.; et al. Oncogene-Addicted Non-Small-Cell Lung Cancer: Treatment Opportunities and Future Perspectives. Cancers 2020, 12, 1196. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef]
- Ginsberg, R.J.; Rubinstein, L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Ann. Thorac. Surg. 1995, 60, 615–623. [Google Scholar] [CrossRef]
- Billmeier, S.E.; Ayanian, J.Z.; Zaslavsky, A.M.; Nerenz, D.R.; Jaklitsch, M.T.; Rogers, S.O. Predictors and Outcomes of Limited Resection for Early-Stage Non-Small Cell Lung Cancer. Clin. Med. (Russian Journal) 2011, 103, 1621–1629. [Google Scholar] [CrossRef]
- Yoon, S.M.; Shaikh, T.; Hallman, M. Therapeutic management options for stage III non-small cell lung cancer. World J. Clin. Oncol. 2017, 8, 1–20. [Google Scholar] [CrossRef]
- Gilligan, D.; Nicolson, M.; Smith, I.; Groen, H.; Dalesio, O.; Goldstraw, P.; Hatton, M.; Hopwood, P.; Manegold, C.; Schramel, F.; et al. Preoperative chemotherapy in patients with resectable non-small cell lung cancer: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial and update of systematic review. Lancet 2007, 369, 1929–1937. [Google Scholar] [CrossRef]
- Felip, E.; Rosell, R.; Maestre, J.A.; Rodríguez-Paniagua, J.M.; Morán, T.; Astudillo, J.; Alonso, G.; Borro, J.M.; González-Larriba, J.L.; Torres, A.; et al. Preoperative Chemotherapy Plus Surgery Versus Surgery Plus Adjuvant Chemotherapy Versus Surgery Alone in Early-Stage Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2010, 28, 3138–3145. [Google Scholar] [CrossRef]
- Pignon, J.-P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.-Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Paz-Ares, L.; de Marinis, F.; Dediu, M.; Thomas, M.; Pujol, J.-L.; Bidoli, P.; Molinier, O.; Sahoo, T.P.; Laack, E.; Reck, M.; et al. Maintenance therapy with pemetrexed plus best supportive care versus placebo plus best supportive care after induction therapy with pemetrexed plus cisplatin for advanced non-squamous non-small-cell lung cancer (PARAMOUNT): a double-blind, phase 3, randomised controlled trial. Lancet Oncol. 2012, 13, 247–255. [Google Scholar] [CrossRef]
- Skoulidis, F.; Li, B.T.; Dy, G.K.; Price, T.J.; Falchook, G.S.; Wolf, J.; Italiano, A.; Schuler, M.; Borghaei, H.; Barlesi, F.; et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. New Engl. J. Med. 2021, 384, 2371–2381. [Google Scholar] [CrossRef]
- Jänne, P.A.; Riely, G.J.; Gadgeel, S.M.; Heist, R.S.; Ou, S.-H.I.; Pacheco, J.M.; Johnson, M.L.; Sabari, J.K.; Leventakos, K.; Yau, E.; et al. Adagrasib in Non–Small-Cell Lung Cancer Harboring a KRASG12C Mutation. New Engl. J. Med. 2022, 387, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2009, 11, 121–128. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or Chemotherapy for Non–Small-Cell Lung Cancer with Mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.-H.; Yamamoto, N.; Obyrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.-M.; Boyer, M.; et al. Phase III Study of Afatinib or Cisplatin Plus Pemetrexed in Patients With Metastatic Lung Adenocarcinoma With EGFR Mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef]
- Mok, T.S.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Lee, M.; Linke, R.; Rosell, R.; Corral, J.; et al. Improvement in Overall Survival in a Randomized Study That Compared Dacomitinib With Gefitinib in Patients With Advanced Non–Small-Cell Lung Cancer and EGFR-Activating Mutations. J. Clin. Oncol. 2018, 36, 2244–2250. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus Chemotherapy in AdvancedALK-Positive Lung Cancer. New Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.H.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef]
- Soria, J.-C.; Tan, D.S.W.; Chiari, R.; Wu, Y.-L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.-J.; et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK -rearranged non-small-cell lung cancer (ASCEND-4): a randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.-J.; Yang, J.C.-H.; Han, J.-Y.; Lee, J.-S.; Hochmair, M.J.; Li, J.Y.-C.; Chang, G.-C.; Lee, K.H.; et al. Brigatinib versus Crizotinib in ALK-Positive Non–Small-Cell Lung Cancer. New Engl. J. Med. 2018, 379, 2027–2039. [Google Scholar] [CrossRef]
- Horn, L.; Wang, Z.; Wu, G.; Poddubskaya, E.; Mok, T.; Reck, M.; Wakelee, H.; Chiappori, A.A.; Lee, D.H.; Breder, V.; et al. Ensartinib vs Crizotinib for Patients With Anaplastic Lymphoma Kinase−Positive Non–Small Cell Lung Cancer: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Bauer, T.M.; de Marinis, F.; Felip, E.; Goto, Y.; Liu, G.; Mazieres, J.; Kim, D.-W.; Mok, T.; Polli, A.; et al. First-Line Lorlatinib or Crizotinib in Advanced ALK-Positive Lung Cancer. New Engl. J. Med. 2020, 383, 2018–2029. [Google Scholar] [CrossRef]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M., Jr.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: an open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.; Tan, D.S.; Hida, T.; de Jonge, M.; Orlov, S.V.; et al. Capmatinib inMETExon 14–Mutated orMET-Amplified Non–Small-Cell Lung Cancer. New Engl. J. Med. 2020, 383, 944–957. [Google Scholar] [CrossRef]
- Paik, P.K.; Felip, E.; Veillon, R.; Sakai, H.; Cortot, A.B.; Garassino, M.C.; Mazieres, J.; Viteri, S.; Senellart, H.; Van Meerbeeck, J.; et al. Tepotinib in Non–Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. N. Engl. J. Med. 2020, 383, 931–943. [Google Scholar] [CrossRef]
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef]
- Drilon, A.; Siena, S.; Dziadziuszko, R.; Barlesi, F.; Krebs, M.G.; Shaw, A.T.; de Braud, F.; Rolfo, C.; Ahn, M.-J.; Wolf, J.; et al. Entrectinib in ROS1 fusion-positive non-small-cell lung cancer: integrated analysis of three phase 1–2 trials. Lancet Oncol. 2019, 21, 261–270. [Google Scholar] [CrossRef]
- Gainor, J.F.; Curigliano, G.; Kim, D.-W.; Lee, D.H.; Besse, B.; Baik, C.S.; Doebele, R.C.; A Cassier, P.; Lopes, G.; Tan, D.S.W.; et al. Pralsetinib for RET fusion-positive non-small-cell lung cancer (ARROW): a multi-cohort, open-label, phase 1/2 study. Lancet Oncol. 2021, 22, 959–969. [Google Scholar] [CrossRef]
- Drilon, A.; Oxnard, G.R.; Tan, D.S.; Loong, H.H.; Johnson, M.; Gainor, J.; McCoach, C.E.; Gautschi, O.; Besse, B.; Cho, B.C.; et al. Efficacy of Selpercatinib in RET Fusion–Positive Non–Small-Cell Lung Cancer. New Engl. J. Med. 2020, 383, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazières, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-Mutant Non–Small-Cell Lung Cancer. New Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; Dubois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion–Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2015, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1–Selected Patients with NSCLC. New Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- O’brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M.; et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB–IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csőszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. IMpower010 Investigators. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB–IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. New Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.M.; E McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: a pooled analysis of two randomised trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef]
- Stanic, S.; Paulus, R.; Timmerman, R.D.; Michalski, J.M.; Barriger, R.B.; Bezjak, A.; Videtic, G.M.; Bradley, J. No Clinically Significant Changes in Pulmonary Function Following Stereotactic Body Radiation Therapy for Early- Stage Peripheral Non-Small Cell Lung Cancer: An Analysis of RTOG 0236. Int. J. Radiat. Oncol. 2014, 88, 1092–1099. [Google Scholar] [CrossRef]
- Nieder, C.; Guckenberger, M.; Gaspar, L.E.; Rusthoven, C.G.; De Ruysscher, D.; Sahgal, A.; Nguyen, T.; Grosu, A.L.; Mehta, M.P. Management of patients with brain metastases from non-small cell lung cancer and adverse prognostic features: multi-national radiation treatment recommendations are heterogeneous. Radiat. Oncol. 2019, 14, 33. [Google Scholar] [CrossRef]
- Tang, X.; Hu, Q.; Chen, Y.; Wang, X.; Li, X.; Cheng, K.; Cao, D. Optimal dose-fractionation schedule of palliative radiotherapy for patients with bone metastases: a protocol for systematic review and network meta-analysis. BMJ Open 2020, 10, e033120. [Google Scholar] [CrossRef]
- Zabel, A.; Debus, J. Treatment of brain metastases from non-small-cell lung cancer (NSCLC): radiotherapy. Lung Cancer 2004, 45, S247–S252. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary Report on the Graded Prognostic Assessment: An Accurate and Facile Diagnosis-Specific Tool to Estimate Survival for Patients With Brain Metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef]
- Sas-Korczynska, B.; Rucinska, M. WBRT for brain metastases from non-small cell lung cancer: for whom and when?—Contemporary point of view. J. Thorac. Dis. 2021, 13, 3246–3257. [Google Scholar] [CrossRef]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of Brain Metastases. Curr. Oncol. Rep. 2011, 14, 48–54. [Google Scholar] [CrossRef]
- Ebben, J.D.; You, M. Brain metastasis in lung cancer: Building a molecular and systems-level understanding to improve outcomes. Int. J. Biochem. Cell Biol. 2016, 78, 288–296. [Google Scholar] [CrossRef]
- Rancoule, C.; Vallard, A.; Guy, J.-B.; Espenel, S.; Diao, P.; Chargari, C.; Magné, N. Brain metastases from non-small cell lung carcinoma: Changing concepts for improving patients’ outcome. Crit. Rev. Oncol. 2017, 116, 32–37. [Google Scholar] [CrossRef]
- Shaw, M.G.; Ball, D.L. Treatment of Brain Metastases in Lung Cancer: Strategies to Avoid/Reduce Late Complications of Whole Brain Radiation Therapy. Curr. Treat. Options Oncol. 2013, 14, 553–567. [Google Scholar] [CrossRef]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.-P.; et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef]
- Li, H.; Li, W.; Qi, C.; Zhou, L.; Wen, F.; Qu, Y.; Yu, H. Optimizing Whole Brain Radiotherapy Treatment and Dose for Patients With Brain Metastases From Small Cell Lung Cancer. Front. Oncol. 2021, 11, 726613. [Google Scholar] [CrossRef]
- Garsa, A.; Jang, J.K.; Baxi, S.; Chen, C.; Akinniranye, O.; Hall, O.; Larkin, J.; Motala, A.; Hempel, S. Radiation Therapy for Brain Metastases: A Systematic Review. Pr. Radiat. Oncol. 2021, 11, 354–365. [Google Scholar] [CrossRef]
- Gaspar, L.E.; Mehta, M.P.; Patchell, R.A.; Burri, S.H.; Robinson, P.D.; Morris, R.E.; Ammirati, M.; Andrews, D.W.; Asher, A.L.; Cobbs, C.S.; et al. The role of whole brain radiation therapy in the management of newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline. J. Neuro-Oncology 2009, 96, 17–32. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases: A Randomized Controlled Trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef]
- Trikhirhisthit, K.; Setakornnukul, J.; Thephamongkhol, K. Added survival benefit of whole brain radiotherapy in brain metastatic non-small cell lung cancer: Development and external validation of an individual prediction model. Front. Oncol. 2022, 12, 911835. [Google Scholar] [CrossRef]
- Rades, D.; Hansen, H.C.; Schild, S.E.; Janssen, S. A New Diagnosis-Specific Survival Score for Patients to be Irradiated for Brain Metastases from Non-small Cell Lung Cancer. Lung 2019, 197, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Dunst, J.; Schild, S.E. A New Scoring System to Predicting the Survival of Patients Treated with Whole-Brain Radiotherapy for Brain Metastases. Strahlenther. und Onkol. 2008, 184, 251–255. [Google Scholar] [CrossRef]
- Mantovani, C.; Gastino, A.; Cerrato, M.; Badellino, S.; Ricardi, U.; Levis, M. Modern Radiation Therapy for the Management of Brain Metastases From Non-Small Cell Lung Cancer: Current Approaches and Future Directions. Front. Oncol. 2021, 11, 772789. [Google Scholar] [CrossRef]
- Wilke, C.; Grosshans, D.; Duman, J.; Brown, P.; Li, J. Radiation-induced cognitive toxicity: pathophysiology and interventions to reduce toxicity in adults. Neuro-Oncology 2017, 20, 597–607. [Google Scholar] [CrossRef]
- Brown, P.D.; Ahluwalia, M.S.; Khan, O.H.; Asher, A.L.; Wefel, J.S.; Gondi, V. Whole-Brain Radiotherapy for Brain Metastases: Evolution or Revolution? J. Clin. Oncol. 2018, 36, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Roman, D.D.; Sperduto, P.W. Neuropsychological effects of cranial radiation: current knowledge and future directions. Int. J. Radiat. Oncol. 1995, 31, 983–998. [Google Scholar] [CrossRef]
- Soussain, C.; Ricard, D.; Fike, J.R.; Mazeron, J.-J.; Psimaras, D.; Delattre, J.-Y. CNS complications of radiotherapy and chemotherapy. Lancet 2009, 374, 1639–1651. [Google Scholar] [CrossRef] [PubMed]
- Bompaire, F.; Lahutte, M.; Buffat, S.; Soussain, C.; Ardisson, A.E.; Terziev, R.; Sallansonnet-Froment, M.; De Greslan, T.; Edmond, S.; Saad, M.; et al. New insights in radiation-induced leukoencephalopathy: a prospective cross-sectional study. Support. Care Cancer 2018, 26, 4217–4226. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G.; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef]
- Wang, B.; Fu, S.; Huang, Y.; Liu, L.; Liang, Y.; An, W.; Fan, Y.; Zhao, Y. The Effect of Hippocampal Avoidance Whole Brain Radiotherapy on the Preservation of Long-Term Neurocognitive Function in Non-Small Cell Lung Cancer Patients With Brain Metastasis. Technol. Cancer Res. Treat. 2021, 20, 15330338211034268. [Google Scholar] [CrossRef] [PubMed]
- Greaves, W.O.; Verma, S.; Patel, K.P.; Davies, M.A.; Barkoh, B.A.; Galbincea, J.M.; Yao, H.; Lazar, A.J.; Aldape, K.D.; Medeiros, L.J.; et al. Frequency and Spectrum of BRAF Mutations in a Retrospective, Single-Institution Study of 1112 Cases of Melanoma. J. Mol. Diagn. 2013, 15, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.-J.; et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015, 386, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Brase, J.C.; Garrett, J.; Campbell, C.D.; Gasal, E.; Squires, M.; Gusenleitner, D.; Santinami, M.; Atkinson, V.; Mandalà, M.; et al. Adjuvant dabrafenib plus trametinib versus placebo in patients with resected, BRAFV600-mutant, stage III melanoma (COMBI-AD): exploratory biomarker analyses from a randomised, phase 3 trial. Lancet Oncol. 2020, 21, 358–372. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, A.R.; Chablani, P.; Siedow, M.R.; Miller, E.D.; Walston, S.; Kendra, K.L.; Wuthrick, E.; Williams, T.M. BRAF mutation correlates with worse local–regional control following radiation therapy in patients with stage III melanoma. Radiat. Oncol. 2021, 16, 181. [Google Scholar] [CrossRef]
- Long, G.V.; Menzies, A.M.; Nagrial, A.M.; Haydu, L.E.; Hamilton, A.L.; Mann, G.J.; Hughes, T.M.; Thompson, J.F.; Scolyer, R.A.; Kefford, R.F. Prognostic and Clinicopathologic Associations of Oncogenic BRAF in Metastatic Melanoma. J. Clin. Oncol. 2011, 29, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Menzies, A.M.; Haydu, L.E.; Visintin, L.; Carlino, M.S.; Howle, J.R.; Thompson, J.F.; Kefford, R.F.; Scolyer, R.A.; Long, G.V. Distinguishing Clinicopathologic Features of Patients with V600E and V600K BRAF-Mutant Metastatic Melanoma. Clin. Cancer Res. 2012, 18, 3242–3249. [Google Scholar] [CrossRef]
- Bernhard, E.J.; McKenna, W.G.; Hamilton, A.D.; Sebti, S.M.; Qian, Y.; Wu, J.M.; Muschel, R.J. Inhibiting Ras prenylation increases the radiosensitivity of human tumor cell lines with activating mutations of ras oncogenes. Cancer Res. 1998, 58, 1754–1761. [Google Scholar]
- Brunner, T.B.; Cengel, K.A.; Hahn, S.M.; Wu, J.; Fraker, D.L.; McKenna, W.G.; Bernhard, E.J. Pancreatic Cancer Cell Radiation Survival and Prenyltransferase Inhibition: The Role of K-Ras. Cancer Res 2005, 65, 8433–8441. [Google Scholar] [CrossRef]
- Sambade, M.J.; Peters, E.C.; Thomas, N.E.; Kaufmann, W.K.; Kimple, R.J.; Shields, J.M. Melanoma cells show a heterogeneous range of sensitivity to ionizing radiation and are radiosensitized by inhibition of B-RAF with PLX-4032. Radiother. Oncol. 2011, 98, 394–399. [Google Scholar] [CrossRef]
- Harding, J.J.; Barker, C.A.; Carvajal, R.D.; Wolchok, J.D.; Chapman, P.B.; Lacouture, M.E. Cutis Verticis Gyrata in Association With Vemurafenib and Whole-Brain Radiotherapy. J. Clin. Oncol. 2014, 32, e54–e56. [Google Scholar] [CrossRef]
- Anker, C.J.; Grossmann, K.F.; Atkins, M.B.; Suneja, G.; Tarhini, A.A.; Kirkwood, J.M. Avoiding Severe Toxicity From Combined BRAF Inhibitor and Radiation Treatment: Consensus Guidelines from the Eastern Cooperative Oncology Group (ECOG). Int. J. Radiat. Oncol. 2016, 95, 632–646. [Google Scholar] [CrossRef] [PubMed]
- Anker, C.J.; Ribas, A.; Grossmann, A.H.; Chen, X.; Narra, K.K.; Akerley, W.; Andtbacka, R.H.I.; Noyes, R.D.; Shrieve, D.C.; Grossmann, K.F. Severe Liver and Skin Toxicity After Radiation and Vemurafenib in Metastatic Melanoma. J. Clin. Oncol. 2013, 31, e283–e287. [Google Scholar] [CrossRef] [PubMed]
- Forschner, A.; Zips, D.; Schraml, C.; Röcken, M.; Iordanou, E.; Leiter, U.; Weide, B.; Garbe, C.; Meier, F. Radiation recall dermatitis and radiation pneumonitis during treatment with vemurafenib. Melanoma Res. 2014, 24, 512–516. [Google Scholar] [CrossRef]
- Pulvirenti, T.; Hong, A.; Clements, A.; Forstner, D.; Suchowersky, A.; Guminski, A.; McNeil, C.; Hersey, P.; Fogarty, G.; Kefford, R.; et al. Acute Radiation Skin Toxicity Associated With BRAF Inhibitors. J. Clin. Oncol. 2016, 34, e17–e20. [Google Scholar] [CrossRef]
- Conen, K.; Mosna-Firlejczyk, K.; Rochlitz, C.; Wicki, A.; Itin, P.; Arnold, A.W.; Gross, M.; Zimmermann, F.; Zippelius, A. Vemurafenib-Induced Radiation Recall Dermatitis: Case Report and Review of the Literature. Dermatology 2014, 230, 1–4. [Google Scholar] [CrossRef]
- Lang, N.; Sterzing, F.; Enk, A.H.; Hassel, J.C. Cutis verticis gyrata-like skin toxicity during treatment of melanoma patients with the BRAF inhibitor vemurafenib after whole-brain radiotherapy is a consequence of the development of multiple follicular cysts and milia. Strahlenther. und Onkol. 2014, 190, 1080–1. [Google Scholar] [CrossRef]
- Hecht, M.; Zimmer, L.; Loquai, C.; Weishaupt, C.; Gutzmer, R.; Schuster, B.; Gleisner, S.; Schulze, B.; Goldinger, S.M.; Berking, C.; et al. Radiosensitization by BRAF inhibitor therapy—mechanism and frequency of toxicity in melanoma patients. Ann. Oncol. 2015, 26, 1238–1244. [Google Scholar] [CrossRef]
- Peuvrel, L.; Ruellan, A.-L.; Thillays, F.; Quereux, G.; Brocard, A.; Saint-Jean, M.; Aumont, M.; Drouet, F.; Dreno, B. Severe radiotherapy-induced extracutaneous toxicity under vemurafenib. Eur. J. Dermatol. 2013, 23, 879–881. [Google Scholar] [CrossRef]
- Ascierto, P.A.; McArthur, G.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Di Giacomo, A.M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Cobimetinib combined with vemurafenib in advanced BRAFV600-mutant melanoma (coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. 2016, 17, 1248–1260. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF -mutant melanoma (COLUMBUS): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2018, 19, 603–615. [Google Scholar] [CrossRef]
- Foppen, M.H.G.; Boogerd, W.; Blank, C.U.; van Thienen, J.V.; Haanen, J.B.; Brandsma, D. Clinical and radiological response of BRAF inhibition and MEK inhibition in patients with brain metastases from BRAF-mutated melanoma. Melanoma Res. 2018, 28, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Mandalà, M.; Ferrucci, P.F.; Guidoboni, M.; Rutkowski, P.; Ferraresi, V.; Arance, A.; Guida, M.; Maiello, E.; Gogas, H.; et al. Sequencing of Ipilimumab Plus Nivolumab and Encorafenib Plus Binimetinib for Untreated BRAF-Mutated Metastatic Melanoma (SECOMBIT): A Randomized, Three-Arm, Open-Label Phase II Trial. J. Clin. Oncol. 2023, 41, 212–221. [Google Scholar] [CrossRef]
- Atkins, M.B.; Lee, S.J.; Chmielowski, B.; Tarhini, A.A.; Cohen, G.I.; Truong, T.-G.; Moon, H.H.; Davar, D.; O'Rourke, M.; Stephenson, J.J.; et al. Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients With Advanced BRAF-Mutant Melanoma: The DREAMseq Trial—ECOG-ACRIN EA6134. J. Clin. Oncol. 2023, 41, 186–197. [Google Scholar] [CrossRef]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three radiation therapy oncology group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, M.; Switchenko, J.M.; Press, R.H.; Jhaveri, J.; Buchwald, Z.S.; Blumenfeld, P.A.; Marwaha, G.; Diaz, A.; Wang, D.; Abrams, R.A.; et al. Post-treatment neutrophil-to-lymphocyte ratio predicts for overall survival in brain metastases treated with stereotactic radiosurgery. J. Neuro-Oncology 2018, 139, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Doi, H.; Nakamatsu, K.; Anami, S.; Fukuda, K.; Inada, M.; Tatebe, H.; Ishikawa, K.; Kanamori, S.; Monzen, H.; Nishimura, Y. Neutrophil–to–Lymphocyte Ratio Predicts Survival After Whole-brain Radiotherapy in Non-small Cell Lung Cancer. Vivo 2019, 33, 195–201. [Google Scholar] [CrossRef]
Figure 1.
Whole body CT-scan performed at diagnosis in January 2023 showing the presence of multiple brain metastases localized in the right frontoparietal, occipital (panel a) and left frontal lobes (panel b). Large mass in the right-upper lung lobe (panel c), liver metastasis (10mm) and spleen metastasis (30 mm) (panel d) are also presented. .
Figure 1.
Whole body CT-scan performed at diagnosis in January 2023 showing the presence of multiple brain metastases localized in the right frontoparietal, occipital (panel a) and left frontal lobes (panel b). Large mass in the right-upper lung lobe (panel c), liver metastasis (10mm) and spleen metastasis (30 mm) (panel d) are also presented. .
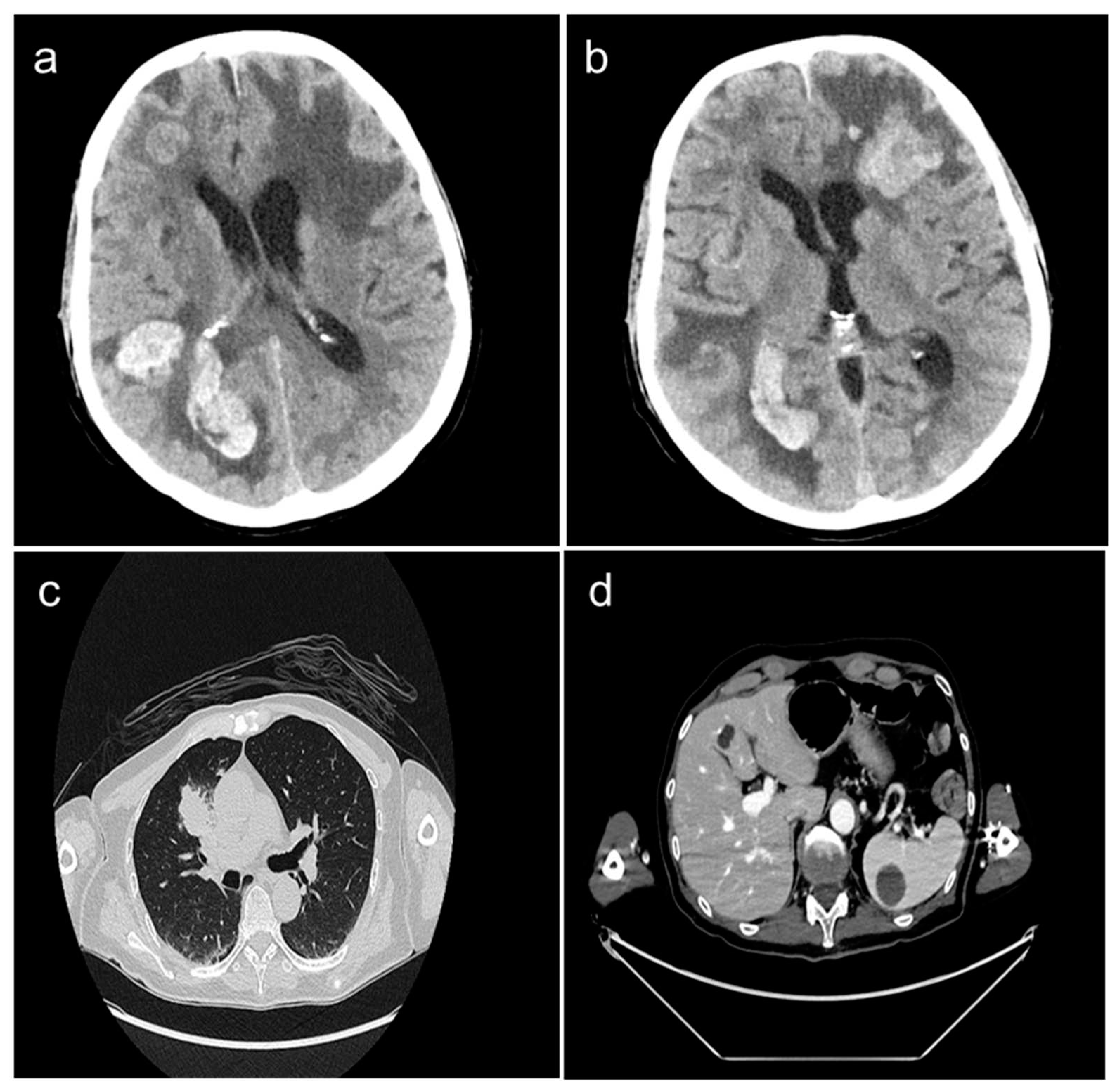

Table 1.
List of pre-treatment and treatment-related variables analyzed for the identification of RTOG-RPA scoring system.
Table 1.
List of pre-treatment and treatment-related variables analyzed for the identification of RTOG-RPA scoring system.
| Variable | Description |
|---|---|
| Brain metastases | Alone With other brain metastases |
| Primary lesion | Controlled Uncontrolled |
| Primary lesion site | Lung Breast Other |
| Histology | Squamous Adenocarcinoma Large cell Small cell Melanoma NSC Other |
| Prior brain surgery | None Yes |
|
Time interval from diagnosis of primary to brain metastases |
≤ 2 years > 2 years |
|
Headache |
Absent Present |
|
Seizure |
Absent Present |
|
Visual disturbance |
Absent Present |
|
Neurologic function |
None Minor Moderate Major |
|
Midline shift |
No Yes |
|
Mass effect |
No Yes |
|
Location of lesions |
Frontal Temporal Parietal Occipital Basal ganglia/thalamus Cerebellum Brainstem |
|
Sentinel location of lesions |
Frontal Temporal Parietal Occipital Basal ganglia/thalamus Cerebellum Brainstem |
|
Sentinel lesion side |
Left Right Midline |
|
Necrotic center |
No Yes |
|
Number of lesions |
Single Multiple |
|
Tumor response |
Complete Partial Stable Progression |
|
KPS |
30-40 50-60 70-80 90-100 |
|
Area (mm2) |
0-400 401-900 901-1600 > 1601 |
|
Age (years) |
< 40 40-44 45-49 50-54 55-59 60-64 65-69 > 70 |
|
Total dose (cGy) |
2400-3499 3500-4000 4001-5279 5280-6079 6080-6719 6720-9000 |
Abbreviations: cGy: centigray; KPS: Karnofsky performance status and NSC: non-small-cell.
Table 2.
Univariate analysis of pre-treatment and treatment-related variables tested for the identification of RTOG-RPA scoring system.
Table 2.
Univariate analysis of pre-treatment and treatment-related variables tested for the identification of RTOG-RPA scoring system.
| Variable | Comparison | p-Value |
|---|---|---|
| Brain metastases | alone vs with other metastases | < 0.0001 |
| KPS | ≥ 70 vs < 70 | < 0.0001 |
| Age (years) | < 65 vs ≥ 65 | < 0.0001 |
| Prior surgery | no vs yes | 0.005 |
| Histology | squamous vs small cell vs others | < 0.0001 |
| Primary lesion | controlled vs uncontrolled | < 0.0001 |
| Primary site | breast vs lung and others | 0.001 |
| Time interval | < 2 years vs > 2 years | 0.004 |
| Number of lesions | single vs multiple | 0.021 |
| Sentinel lesion side | left and/or right vs midline | 0.038 |
| Sentinel location | frontal, temporal, parietal, occipital and basal ganglia/thalamus vs cerebellum and brainstem | 0.033 |
| Neurologic function | no vs yes | < 0.0001 |
| Headache | no vs yes | 0.003 |
| Total dose (cGy) | ≥ 5200 vs < 5200 | < 0.0001 |
| Tumor response | complete or partial vs stable or progressive | 0.019 |
Abbreviations: cGy: centigray and KPS: Karnofsky performance status.
Table 3.
List of variables analyzed for the identification of WBRT-30-NSCLC scoring system.
| Variable | Description |
|---|---|
| Age (years) | ≤ 62 ≥ 63 |
| Gender | Male Female |
| KPS | < 70 70 > 70 |
| Interval from diagnosis of NSCLC to WBRT | ≤ 1 months ≥ 2 months |
| Pre-WBRT systemic treatment | No Yes |
|
Control of the primary tumor |
No Yes |
|
Number of intracerebral metastases |
1-3 ≥ 4 |
|
Metastasis outside the brain |
No Yes |
Abbreviations: KPS: Karnofsky performance status; NSCLC: Non-small-cell lung cancer and WBRT: whole brain radiotherapy.
Table 4.
WBRT-30-NSCLC score.
| Variable | Factor Score |
|---|---|
|
Age (years) ≤ 62 ≥ 63 |
4 2 |
|
KPS < 70 70 > 70 |
1 3 5 |
|
Pre-WBRT systemic treatment No Yes |
2 4 |
|
Number of intracerebral metastases |
|
| 1-3 ≥ 4 Metastasis outside the brain No Yes |
4 2 5 2 |
Abbreviations: KPS: Karnofsky performance status and WBRT: whole brain radiotherapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



