Submitted:
29 July 2023
Posted:
31 July 2023
You are already at the latest version
Abstract
Progressive loss of retinal ganglionic cells (RGC) causes blindness in glaucoma. Elevated intraocular pressure (IOP) is the most important, treatable risk factor. Currently, the management of glaucoma is centred at reducing the IOP, and drugs in the form of topical drops are the first line of management. Drugs reduce IOP either by suppressing aqueous humour secretion or improving the aqueous humour outflow. Newer drugs added during the past three decades to the armamentarium of glaucoma treatment have targeted the aqueous outflow. With an evolving understanding of the pathogenesis of glaucoma, the role of 24-hour IOP control and other IOP-independent risk factors affecting ocular blood flow and RGC toxicity is also recognised. The role of available drugs in controlling IOP over 24-hours is being evaluated. Improvement of ocular blood flow and neuroprotection are seen as potential drug targets in preventing the loss of RGC. In this article, we review the pharmacotherapy of glaucoma based on current therapeutic principles.
Keywords:
glaucoma
; pharmacotherapy
; intraocular pressure
; 24-hour IOP control
; neuroprotection
; adjuvent therapy
; ocular blood flow
Introduction
Glaucoma, characterised by progressive loss of retinal ganglionic cells (RGC) [1], is the cause of 11 % of global blindness in individuals aged 50 years and older [2]. The risk of blindness is related to the level of untreated intraocular pressure (IOP), wider IOP fluctuations [3], the extent of RGC loss at the time of diagnosis [4], and compliance with treatment [5]. The only modifiable risk factors are IOP and its fluctuations, which can be achieved with drugs, LASER, and surgical intervention. The effective IOP-lowering, called target IOP, slows down the progression of glaucoma and delays blindness [6]. However, in a subset of patients, RGC continue to die even after effective IOP-lowering. In these patients’ the role of IOP fluctuations, and other IOP-independent factors like ocular blood flow and neurotoxicity is anticipated. The current interventions mainly lower the IOP, and their other benefits like 24-hour IOP control, ocular blood flow regulation, and neuroprotection are being explored.
Medical intervention in the form of topical eye drops is often offered as the first-line therapy. Several drugs of different classes are available that effectively lower the IOP [7]. In this article, we review the pharmacotherapy of glaucoma based on the current understanding of therapeutic principles.
Pathophysiology of glaucoma
Axons of approximately 1.2 million RGC converge at the scleral lamina cribrosa to exit from the eye and form the optic nerve head (ONH), -the intra-ocular portion of the optic nerve. The ONH is visible on fundus examination as a pinkish disc with a peripheral rim of axons, called the neuroretinal rim (NRR) and a central space filled with glial cells, known as the optic disc cup (Figure 1a). The death of RGC manifests as focal or diffuse loss of NRR and an alteration in cup-to-disc ratio (CDR), characteristic of glaucomatous damage (Figure 1b). RGC death is most often due to elevated IOP [8]. The pressure-induced changes at the level of lamina cribrosa [9] affect the retrograde transport of essential factors [10] to the cellular body of the RGC, which culminates in apoptosis and RGC death.
The net IOP is an outcome of the relationship between the rate of aqueous secretion, the rate of aqueous drainage, and episcleral venous pressure [11]. It is the drainage of aqueous humour that is almost always impaired in all types of glaucoma. The aqueous drains through two independent pathways-trabecular meshwork (or conventional or major pathway), and the uveoscleral pathway (or non-conventional or minor pathway). Conventional outflow accounts for nearly 85% of aqueous drainage, and 5-25% of drainage is through uveoscleral outflow [12]. The aqueous drainage decreases with age through trabecular meshwork pathway [13] as well as the uveoscleral pathway [14]. The IOP increases following impaired aqueous drainage through the trabecular meshwork. The mechanisms responsible for impaired aqueous drainage through the trabecular meshwork are documented primarily based on the gonioscopic state of the angles of the anterior chamber. In open-angle conditions, the resistance to aqueous outflow is at the level of the trabecular meshwork [15], whereas in angle-closure conditions, access to the trabecular meshwork is blocked by iris tissue [16].
Targets for pharmacotherapy
Currently, the management of glaucoma is limited to lowering the IOP. The two ways in which IOP can be lowered are by reducing aqueous humour secretion and improving aqueous humour drainage. The, global availability of topical IOP-lowering drugs varies based on approval by the official local controlling body. Pilocarpine, a cholinergic agent, was the first topical drug used to treat glaucoma [17]. The latest addition to the armamentarium of IOP-lowering drugs is Omidenepag Isopropyl (OMPI), which was approved by the FDA in 2022 to treat open-angle glaucoma and ocular hypertension [18] (Figure 2). Topical IOP-lowering drugs are available either as monotherapy or as fixed-drug combinations (FDC). These drugs fall broadly into two groups (Table 1) based on their main mechanism of IOP reduction: One, which reduces IOP by suppressing the aqueous humour secretion, and two, which reduce IOP by improving the aqueous humour outflow. The latter is further sub-grouped based on whether these drugs reduce IOP by improving aqueous outflow through the conventional or unconventional pathway (Figure 3). IOP-lowering drugs developed in the early years targeted aqueous secretion reduction until the role of prostaglandin analogues in facilitating the aqueous outflow was recognized. The recent addition of drugs acting on the trabecular meshwork represents the most physiological way of reducing IOP. Few drugs lower IOP by more than one mechanism (Table 2) but are grouped based on their chief mechanism of IOP reduction. Based on their target mechanism of action, currently available IOP-lowering drugs are classified into seven classes.
Aqueous suppressants drugs
Beta-adrenergic antagonists
Three types of beta-adrenergic receptors are known: β1, β2, and β3. In the human eye, beta-adrenoceptors have been localised in the ciliary process [19], extraocular muscles, conjunctiva, epithelium and endothelium of the cornea, trabecular meshwork, and ciliary muscle [20]. The precise mechanism of β-adrenergic receptor antagonism-mediated decrease in aqueous humour secretion is not completely understood. In non-primate animal studies, beta-blockers decrease aqueous humour secretion by inhibiting catecholamine-stimulated synthesis of cyclic-adenosine monophosphate [21] Ocular beta-blockers are competitive inhibitors of β1 and β2 receptors, having a very low affinity for β3 receptors. Non-selective ocular beta-blocker drugs like timolol inhibit both β1 and β2 receptors, whereas selective inhibitors such as betaxolol block only the β1 receptors. In animal experimental studies beta-blockers reduced ocular blood flow [22].
Adrenergic agonists
Alpha-adrenergic drugs lower IOP through their agonist action on α-2 adrenergic receptors. The α- 2 adrenergic receptors have been localised in the ciliary body, retinal pigmented epithelium-choriocapillaris, iris, and neurosensory retina in the human eye, and the predominant subtype in the ciliary body is α-2A [23]. The activation of α-2 receptors in the ciliary body reduces aqueous secretion. The precise mechanism leading to a decrease in aqueous humour secretion is not known but appears to mediate through a decrease in intracellular cyclic adenosine monophosphate (cAMP) level [24]. These drugs may have some effect on the outflow pathway owing to the presence of α-2A receptors [25]. Three drugs available in the topical form are apraclonidine, brimonidine and clonidine. All three drugs are α-2 agonists but have some α-1 properties, which result in conjunctival vasoconstriction, lid retraction, and slight mydriasis. Brimonidine increases uveoscleral outflow, and this effect is supposed to be the main mechanism for IOP reduction in long-term treatment [14]. In experimental studies on mice, brimonidine reduced episcleral venous pressure [26]. Apraclonidine does not appear to improve uveoscleral outflow but perhaps reduces aqueous secretion and episcleral venous pressure [27,28]. The presence of alpha-adrenergic receptors in the retina is seen as a potential target for the neuroprotective effects of these drugs [29]. Brimodine did not show cause any clinically beneficial improvement in ocular blood flow in humans. [30, 31].
Carbonic anhydrase inhibitors
Carbonic anhydrase inhibitors (CAIs) belong to sulphonamide compounds and are the only class of IOP-lowering drugs that is available in both, topical and systemic, formulations for glaucoma treatment. Topical as well as systemic CAIs lower the IOP by reducing aqueous humour formation by inhibiting the enzyme carbonic anhydrase II (CA II) isoform in the epithelial cells of ciliary processes [32]. Inhibition of CA II reduces the formation and accumulation of bicarbonate ions, with a resultant decrease in sodium and fluid accumulation in the posterior chamber [33]. Systemic CAIs are non-selective and inhibit CA II and CA IV isoenzymes. The non-selective inhibition of CA isoenzymes by oral acetazolamide accounts for greater IOP reduction compared to topical CAIs [34]. Their role in improving the ocular blood flow has been studied in humans [30, 31]. In topical form, two drugs are available: dorzolamide 2% and brinzolamide 1%.
Uveoscleral outflow drugs
Prostaglandin analogues
The PGF2α subtype of FP receptors and the EP2 subtype of EP receptors [35] regulate IOP. The circular muscles and collagenous connective tissue of ciliary tissue have both PGF2α and EP1 receptors. Through activation of these receptors, PGA increases the expression of metalloproteinases 1, 2, 3 and 9 in human ciliary muscle cells [36, 37]. The increased level of metalloproteinases results in remodeling of the extracellular matrix of the ciliary muscle bundles of the uveoscleral pathway, which augments the aqueous outflow [38]. The PGF2α analogues except for bimatoprost, which is an amide prodrug; rest are ester prodrugs of the corresponding acids, including PGEP2 receptor analogue OMPI. These drugs are hydrolysed by corneal esterase into biologically active agents [39, 40, 41]. The OMPI is supposed to increase aqueous outflow through both the trabecular meshwork and uveoscleral pathway [42].
Trabecular outflow drugs
Cholinergic
Cholinergic or parasympathomimetic drugs mediate their pharmacological effects through direct stimulation of muscarinic receptors located on the ciliary muscle and iris sphincter. Of the five subtypes of receptors, the iris-ciliary body-trabecular meshwork in human eyes predominantly has M3 types of muscarinic receptors [43, 44]. Direct stimulation of these receptors contracts ciliary muscle, which pulls the scleral spur, resulting in the widening of trabecular meshwork lamellae and an increase in aqueous humour outflow. This mechanism is responsible for the IOP-lowering effects of these drugs in ocular hypertension and open-angle glaucoma. The same action also results in reduced uveoscleral outflow [45, 46]. Contrarily, direct stimulation of M3 receptors on TM results in decreased aqueous outflow, but the net effect is improved aqueous outflow through TM and reduction in IOP [47]. Lower concentrations of pilocarpine increased the outflow facility in human cadaveric eyes with a disinserted ciliary body [48]. In the case of angle-closure diseases, these drugs mediate their effect through action on M3 receptors located on the sphincter pupillae muscle of the iris. The muscle contraction results in meiosis (hence, also called miotics), which widens the angle in eyes with narrow angles, resulting in improved aqueous outflow through the TM and a lowering of IOP. Pilocarpine is the most widely available topical cholinergic drug.
Nitic Oxide donors
Nitric oxide (NO) is synthesised endogenously in the human body, including the trabecular meshwork, Schlemm’s canal, and ciliary body, from L-arginine NO synthase enzyme [49, 50].
The NO donor drugs have targets in the conventional pathway [40]. Latanoprostene bunod (LBN), 0.024%, is a nitic oxide (NO)-donating PGF2α analogue that is hydrolysed to latanoprost acid and butanediol mononitrate, a NO-donating moiety [40]. Latanoprost increases aqueous outflow through the uveoscleral pathway, whereas the butanediol mononitrate metabolites 1,4-butanediol and NO are supposed to enhance aqueous outflow through the trabecular meshwork [50]. The NO activates the soluble guanylyl cyclase/cyclic guanosine monophosphate signaling pathway, which inhibits the Rho pathway, promoting trabecular meshwork and Schlemm’s canal cytoskeletal relaxation to improve aqueous humour outflow [51].
Rho Kinase inhibitors
These drugs act by inhibiting the action of Rho-associated protein kinase (ROCK), a low molecular weight effector protein that is associated with the regulation of actin cytoskeleton organization and cellular processes [52]. (ROCK has two isoforms ROCK 1 and ROCK 2, both of which are expressed in trabecular meshwork [53]. ROCK inhibits two enzymes, LIM kinase and myosin light chain phosphatase (MLCP), which respectively facilitate actin fibre relaxation and polymerisation, resulting in increased resistance to aqueous outflow in trabecular meshwork [54]. Rho-Kinase inhibition results in actin fibre contraction and depolymerisation and facilitates aqueous outflow through the trabecular meshwork [53]. The reduction of aqueous secretion through norepinephrine transporter inhibition has been seen in non-human primates and non-primate animals [55]. In animal studies, these drugs lowered IOP by increasing aqueous outflow, reducing aqueous secretion, and decreasing episcleral venous pressure [56]. Two ROCK inhibitor drugs are available in topical forms to treat glaucoma: Netarsudil 0.02% and Ripasudil 0.4%.
Therapeutic efficacy
The therapeutic efficacy of IOP-lowering drugs can be described in terms of their effect on IOP-related characteristics and IOP-independent benefits promoting the survival of RGC. The clinically relevant pharmacodynamic properties are summarised in Table 3.
IOP independent
Ocular blood flow
Low ocular perfusion is associated with RGC damage in primary open-angle glaucoma and progression [110-112]. Ocular perfusion pressure (OPP) is calculated as the difference between mean arterial pressure (MAP) and IOP [113]. The MAP is derived from systolic and diastolic blood pressures. Topical drops affect IOP and blood pressure and are therefore supposed to alter OPP. Bimatoprost increased OPP in open-angle glaucoma and ocular hypertension patients [91]. Latanoprost increased ocular perfusion pressure (OPP) in non-glaucomatous eyes [114]. In normal-tension glaucoma (NTG) patients with mean baseline IOP in the low teens, latanoprost did not affect OPP [115] but increased in NTG patients with IOP in the upper teens [116]. Tafluprost improved ocular blood flow in experimental studies [117]. The effect of timolol on OPP is not clear. Several studies have noted no change [116], an increase when calculated with diastolic blood pressure but reduced OPP when calculated with systolic blood pressure [114], or only a daytime increase in OPP without any change in nocturnal or 24-hour OPP [118]. Brimonidine 0.2% did not affect OPP in patients with normal tension glaucoma [119]. Pilocarpine increased systolic OPP in non-glaucomatous eyes [120]. Both dorzolamide and brinzolamide increase ocular blood flow [121]. Latanoprostene bunod 0.024% induced a significant increase in optic nerve head blood volume and oxygen saturation in healthy subjects aged between 21 and 62 years [122]. The FDC of brinzolamide/brimonidine did not change OPP in patients with open-angle glaucoma and ocular hypertension [118]. The clinical advantage of improved OPP in preserving the RGC is difficult to estimate in isolation from IOP-lowering.
Neuroprotection
In animal studies, the neuroprotective effects of IOP-lowering drugs, independent of IOP reduction, have been studied. Brimonidine 2% prevented loss of RGC in the chronic ocular hypertension rat model [123]. Indirect evidence of the presumed neuroprotective effect of brimonidine 2% comes from clinical studies. Brimonidine -2%- treated patients had an improvement in contrast sensitivity compared to patients treated with timolol, with comparable IOP reduction [124]. However, in a non-comparative study in open-angle glaucoma patients with travoprost, a reduction in IOP has been associated with improvement in central and peripheral contrast sensitivities [125]. Contrast sensitivity and retinal nerve fibre loss (RNFL) are not strongly correlated in clinical studies [126]. In ocular hypertension patients, RNFL loss was less with brimonidine 0.2% compared to timolol, irrespective of IOP reduction [127]. In clinical trials, IOP reduction has been shown to delay glaucoma progression [128], which may surrogate the neuroprotective effect. The neuroprotective effect of PGA, independent of IOP, was demonstrated against glutamate- or hypoxia-induced RGC death using rat primary RGC culture at clinically available intracameral concentrations [129]. Rho-kinase inhibitors are presumed to have neuroprotective effects based on their neuroprotective capabilities, such as cell survival and axon regeneration, in non-ocular tissue studies [130].
The development of drugs enhancing ocular blood flow or offering neuroprotective effects is still in the pre-clinical stage. The evidence for the available drugs is not strong enough to advocate their preferential use for these additional benefits.
Choice of therapy
All IOP-lowering drugs currently available are approved for use in adults with primary open-angle glaucoma and ocular hypertension. These drugs have been studied for their efficacy and safety in other types of glaucoma as well. PGF2α agonists reduce IOP by 25-35% with once-daily dosing in patients with normal tension glaucoma [131, 132], pigment dispersion syndrome [133], primary angle-closure glaucoma [134, 135], and pseudo-exfoliation glaucoma. In pseudo-exfoliation glaucoma, lower IOP was achieved with bimatoprost 0.03% [136] and travoprost 0.04% [137] when compared to latanoprost 0.005%. OMPI is effective in open-angle glaucoma and ocular hypertension and reduces IOP in patients with poor or no response to latanoprost. OMPI effectively reduced IOP ≥20% from the wash-out period baseline in nearly 85% of poor or non-latanoprost responder patients with open-angle glaucoma [138]. Substitution with PGA or non-PGA drugs may be effective in lowering IOP in poor or non-responders [66, 139]. OMPI is effective in NTG [140] and secondary glaucoma [141].
The NO donor drug, latanoprostene bunod, is not inferior to latanoprost 0.005% in reducing IOP in open angle glaucoma and ocular hypertension [40].
Beta-blockers are used in a twice-daily regimen spaced at 12-hours intervals. A once daily dose of timolol 0.1% gel was equally effective as a 0.5% solution twice-daily in lowering IOP [142]. Beta-blockers are used for all types of glaucoma. Betaxolol reduced IOP nearly by 18% in normal tension glaucoma with baseline IOP in the mid-teens [143]. Beta-blockers are the drug of choice after PGA, provided their use is not limited by their systemic side effects.
Apraclonidine is approved for short-term control of IOP due to the high rate of allergic reactions and tachyphylaxis and is mainly used to suppress post-laser IOP spikes. Brimonidine is used for long-term control of IOP in open-angle glaucoma and ocular hypertension. Brimonidine tartrate 0.2% has been shown to reduce IOP by 18% in normal tension glaucoma [144], but in this study, the mean baseline IOP was in the upper teens (17.3±0.7 mmHg). With a baseline mean IOP in the lower teens (13.9±1.2mmHg) brimonidine 0.1% preserved with sodium chloride reduced IOP by 10% [145]. Alpha-agonist drugs, except for apraclonidine, which is hydrophilic, are lipophilic and easily penetrate through the cornea and blood-brain barrier. The CNS absorption of topical brimonidine resulted in hypotension and sedation in non-primate animal studies [146]. Because of CNS depressant effects in children [147], brimonidine is contraindicated for use in neonates and infants and is to be used with caution in patients on CNS depressants and children below 12 years.
Systemic CAIs are indicated for short-term use for the immediate management of very high IOP in conditions like acute angle-closure crisis or lens-related glaucoma. Long-term use of oral acetazolamide, especially in the elderly, may lead to life-threatening metabolic acidosis [148]. Dorzolamide and brinzolamide have been shown to produce comparable IOP reductions in open-angle and angle-closure glaucoma. The mean IOP reduction in eyes with angle- closure was slightly lower compared to eyes with open angle glaucoma but the difference was not statistically significant [149]. In normal-tension glaucoma with a mean IOP of 16.8±0.9 mmHg, dorzolamide reduced IOP by 18% at 4 weeks [142]. CAIs have been shown to reduce IOP in several types of glaucoma, including in young children [150].
The IOP-lowering effect of pilocarpine approximately begins 60 minutes after ocular instillation, and peaks at 75 minutes, and lasts from four to eight hours [151]. Pilocarpine reduces IOP by 20-25%. In contemporary clinical practice, pilocarpine 2% is mainly used in the management of angle-closure diseases. It is used for its meiotic effect before and/or after laser iridotomy, iridoplasty procedures, and acute angle closure crisis to open an occluded angle once iris ischemia resolves. Pilocarpine and other cholinergic drugs are contraindicated in uveitis and inflammatory secondary glaucoma because their miotic effect may aggravate posterior synechiae formation [152].
Pilocarpine is finding newer applications beyond IOP control. Diluted concentrations (0.125% and 0.0625%) are used in the diagnosis of Adie’s tonic pupil [153]. Newer indications for pilocarpine use are the management of xerostomia [154] and presbyopia [155].
ROCK inhibitors, netarsudil 0.02% is indicated in a once-daily dose, whereas ripasudil is given twice-daily. The IOP reduction with these drugs is between 15 and 25% in open-angle glaucoma and ocular hypertension [60]. Ripasudil effectively reduced IOP in uveitic glaucoma, exfoliation glaucoma, and steroid-induced glaucoma [156].
Tolerability and safety
Systemic side effects
Systemic side effects are a major limitation of beta blockers. The drugs in this class may worsen symptoms of coughing, dyspnoea, bronchial spasm, and wheezing in patients with reactive diseases. The bronchospasm seen with beta-blockers is due to the presence of β2-receptors on the smooth muscles of the airways [157]. The effect is more common and pronounced with non-selective agents in susceptible individuals [158]. The bronchoconstriction in otherwise healthy individuals without pre-existing reactive airways is not clinically significant [159]. Betaxolol has a 20-fold higher affinity for β1-receptors than for β2-receptors. The risk of airway obstruction among non-susceptible persons without prior history of respiratory diseases was similar for selective and non-selective topical beta-blockers [160]. Eyelid closure, nasolacrimal occlusion for 5 minutes, or pressing the eye with tissue paper after applying the eyedrop reduced the systemic absorption of timolol by 60-67% [151, 161]. However, how these manoeuvres affect respiratory functions is not known? The long-term use of beta-blocker eye drops has not been found to increase the risk of falls, dizziness, or orthostatic hypotension in older patients [162]. Therefore, the presence of cardio-pulmonary diseases like bronchial asthma, chronic obstructive pulmonary disease (COPD), sinus bradycardia, and AV blocks is a relative or absolute contraindication for the use of beta-blockers, especially non-selective ones.
Cholinergic drugs may cause sweating, gastro-intestinal (salivation, nausea, vomiting, diarrhoea), respiratory (bronchospasm), and cardio-vascular (bradycardia, hypotension) symptoms due to their action through M1 and M2 receptors following systemic absorption [151, 163].
Apraclonidine reduced heart rate and systolic blood pressure [164] when used to suppress post-LASER IOP spikes. Brimonidine 0.2% reduced both systolic and diastolic blood pressure significantly [165] but not the pulse rate [166] when compared to baseline values. The systolic and diastolic blood pressures are the determinants of ocular perfusion pressure [167]. The precise role of OPP in the causation and progression of glaucoma is not yet clear.
The systemic side effects of topical CAIs are rare, except for the bitter taste. Metabolic acidosis in premature newborns [168], and adults with impaired renal function [169, 170] has been reported.
Local side effects
A stinging sensation immediately after applying drugs is seen with some of these drugs. This is related to the physiochemical properties of ophthalmic drug solutions. The topical dorzolamide is formulated in an acidic pH solution (~5.6), which is necessary for good ocular absorption but causes a stinging sensation on application. Brinzolamide, being lipophilic, has good corneal penetration and is formulated in an ophthalmic solution close to physiological pH (7.4), which keeps it free from unpleasant stinging sensations. Several studies have shown that brinzolamide is better tolerated than dorzolamide [173, 174]. Among PGA, stinging is more common with LBN than latanoprost [40].
Blurred vision, transient or prolonged, is a common adverse effect of most topical IOP-lowering drugs. Transient blurred vision results from changes in the refractive indices of the tear film due to changes in its tonicity. Pilocarpine causes ciliary spasms and induces accommodation, which results in brow aches and blurred vision. The blurred vision results from myopia caused by forward displacement and thickening of the lens [175]. This is troublesome, especially, for young patients. In presbyopic patients, this results in improved near vision. Alpha-adrenergic agonist drugs also cause headaches and fatigue in some patients [176].
Conjunctival hyperaemia is common with PGA, including OMPI, and ROCK inhibitors [177, 178]. Among PGA drugs, it is most common with bimatoprost 0.003% and least common with latanoprost 0.005% [57, 62]. Contrarily, the vasoconstrictive effects of α-adrenergic agonist drugs result in conjunctival blanching, a dry nose, and a dry mouth [176]. Most IOP-lowering drugs reduce Schirmer score, and ocular surface disease index, which is supposed to be because of preservatives [179].
The exact incidence of periorbital contact dermatitis with IOP -lowering drugs is not known. It has been reported with timolol, betaxolol [180], pilocarpine [181], brimonidine [182, 183], dorzolamide [184], brinzolamide [185], bimatoprost [186], and latanoprost [187]. A cross-reactivity among beta-blockers has been observed [180], which is presumed to result from the common lateral aliphatic chain in their structure [188]. Brinzolamide and dorzolamide have been associated with toxic epidermal necrolysis in patients with impaired hepatic functions [189].
PGA drugs may cause cosmetically unacceptable, though reversible, changes in periorbital tissues, collectively described as prostaglandin-associated peri-orbitopathy [190]. This includes changes in the eyelid and orbit: hyperpigmentation of eyelashes and periorbital skin; loss of peri-orbital fat; deepening of lid sulci; mild enophthalmos; and tight eyelids. These changes are seen with all types of PGF2α analogue drugs but are most marked with bimatoprost 0.03% [191]. The higher absorption of drugs in peri-orbital skin [192], which interferes with cellular adipose tissue metabolism [191], and causes peri-orbitopathy. Discontinuation of therapy or switching to an alternate, milder form may reverse changes in weeks or months [190].
Corneal edema has been reported with brinzolamide in eyes with normal endothelial count [193], which is reversible [194]. Dorzolamide may cause irreversible corneal decompensation in eye with compromised cornea or complicated ocular history [195]. CAIs attenuate bicarbonate efflux by reversibly inhibiting CA II in corneal endothelial cells, which results in fluid retention [196]. Until a safe endothelial count for the use of CAI drugs is known, these drugs should be used with caution in patients with compensated cornea. A decrease in the number and density of corneal sub-basal nerve fibre bundles without affecting keratocyte density or corneal endothelial characteristics has been observed with chronic use of topical IOP-lowering drugs in glaucomatous patients and healthy controls with normal endothelial cell count [197].
Granulomatous anterior uveitis may be seen with brimonidine 2% use [198, 199]. The inflammation reverses with discontinuation of brimonidine and a short shot of topical corticosteroid therapy, but IOP control may need surgical intervention in a proportion of patients with high IOP glaucoma [199]. PGA is better avoided in eyes with iritis, herpes simplex keratitis, and eyes at risk of developing cystoid macular edema [65, 200].
Adjunctive therapy
Adjunctive therapy is defined as one or more secondary interventions used concurrently with a primary intervention to enhance treatment effectiveness [203]. The effective reduction in IOP to preserve the RGC required more than one drug in 40-50% of the patients in major clinical trials [204, 205]. Hence, in glaucoma management, adjunctive therapy can be defined as -the concomitant use of a second or subsequent IOP-lowering drug(s) to achieve the target IOP while continuing the first-line therapy. The PGA is used as first-line therapy in almost all cases of glaucoma due to its superior IOP-lowering effect, better 24-hour IOP control, convenient once-daily dosing, and absence of systemic side effects. Almost any drug of any class, except cholinergic, can be used as adjunctive therapy to PGA. The concomitant use of pilocarpine and PGA drugs may be mutually antagonistic [206]. In study on non-human primates, pilocarpine reduced the uveoscleral outflow. [207] However, alteration in the order and timing of administration of pilocarpine and latanoprost has been found effective in achieving additional IOP reduction [208].
Similarly, cholinergic and ROCK inhibitors drugs seem to have an antagonistic effect. Pilocarpine acts through the M3 receptor by inducing the contraction of the ciliary muscle which pulls the scleral spur, and resulting in the widening of the trabecular meshwork lamellae and an increase in aqueous humour outflow. Contrarily, ROCK inhibitors relax trabecular meshwork cells to open spaces. When used concomitantly, pilocarpine did not affect the relaxation effect of the ROCK inhibitor but had no additive effect, and pilocarpine interfered with the IOP reduction by ripasudil at the peak IOP reduction [209].
The IOP-lowering effect of topical CAIs as adjunctive therapy to PGA is superior to timolol or brimonidine [210-213]. The PGA induces a CA enzyme in epithelial cells of the ciliary process, which results in increased aqueous humour formation [214]. This slightly reduces the efficacy of PGA drugs. Since CAIs suppress this PGA-induced activity of the CA enzyme, they result in more efficacious IOP reduction as an adjunctive therapy when compared with timolol or brimonidine. Compared to timolol 0.5% twice daily, brinzolamide 1% twice daily added to latanoprost 0.005% monotherapy resulted in superior IOP reduction and flattening of diurnal variation [210]. The adjunctive IOP-lowering effect of timolol 0.5% (3.9 mmHg) with travoprost 0.004% was superior to brimonidine 2% (2.3 mmHg) [214]. A meta-analysis comparing the effectiveness of brimonidine and CAIs as adjunctive therapies to PGAs and beta-blocker found that brimonidine was superior to CAIs in reducing acrophase and trough IOP as well as diurnal fluctuation [215]. Adjunctive therapy with FDC of brinzolamide/timolol to travoprost was superior to FDC of brimonidine/timolol in controlling mean 24-hour IOP owing to the greater efficacy in the late afternoon and during the night [216].
The addition of dorzolamide 2% to timolol 0.5% (6.8±1.7 mmHg) was more effective in lowering IOP in comparison to its addition to brimonidine 0.2% (5.6±1.9mmHg) [217]. OMPI (0.0006%) has been shown to have an additive IOP-lowering effect with beta-blockers, CAIs, and alpha-2 adrenergic agonist drugs in normotensive conscious monkeys. The additive effect of OMPI was maximum with brimonidine 2% [218].
Additive therapy of netarsudil with timolol or latanoprost reduced the mean pooled IOP by 2.66 mmHg [60]. Ripasudil caused an additional IOP reduction of 0.75 mmHg when added to timolol therapy. The additional IOP reduction with any drug is less when used as adjunctive therapy, compared to when used alone [219].
Conclusions
Over a century since the first evidence emerged, the medical management of glaucoma has evolved. In the past 30 years, many new drugs have made the journey from labs to clinics. The newer drugs target the pathophysiology of glaucoma and reduce IOP by improving the aqueous outflow. The focus is on compounds that act on the trabecular meshwork, have greater IOP-lowering efficacy, and have minimal local and systemic adverse effects. An understanding of drug efficacy helps select the most appropriate drug for the set target pressure. From the patient’s perspective, the most efficacious drug with minimal adverse effects is desirable. In this article, we reviewed all the available classes of IOP-lowering drugs concerning current therapeutic principles like absolute IOP reduction, 24-hour IOP control, nocturnal effect, and IOP-independent benefits. We also investigated the efficacy of adjuvant therapy, and its rationality when combining two or more drugs. The local adverse effects of IOP-lowering drugs are troublesome, especially those affecting the ocular surface. The availability of preservative-free formulations and new drug delivery systems would help overcome some of these adversities soon.
References
- Ventura, L.M.; Sorokac, N.; Santos, R.D.L.; Feuer, W.J.; Porciatti, V. The Relationship between Retinal Ganglion Cell Function and Retinal Nerve Fiber Thickness in Early Glaucoma. Investig. Opthalmology Vis. Sci. 2006, 47, 3904–3911. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Blindness and Vision Impairment Collaborators.; Vision Loss Expert Group of the Global Burden of Disease Study.; Steinmetz J.D. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to vision 2020: the right to sight: an analysis for the global burden of disease study. Lancet. Glob. Health. 2021, 9, e144–e160.
- Kooner, K.S.; Al Bdoor, M.; Cho, B.J.; Adams-Huet, B. Risk factors for progression to blindness in high tension primary open-angle glaucoma: Comparison of blind and non-blind subjects. Clin. Ophthalmol. 2008, 2, 757–762. [Google Scholar] [CrossRef]
- Oliver, J.E.; Hattenhauer, M.G.; Herman, D.; Hodge, D.O.; Kennedy, R.; Fang-Yen, M.; Johnson, D.H. Blindness and glaucoma: a comparison of patients progressing to blindness from glaucoma with patients maintaining vision. Am. J. Ophthalmol. 2002, 133, 764–772. [Google Scholar] [CrossRef]
- Paula, J.S.; Furtado, J.M.; Santos, A.S.; Coelho, R.d.M.; Rocha, E.M.; Rodrigues, M.d.L.V. Risk factors for blindness in patients with open-angle glaucoma followed-up for at least 15 years. Arq. Bras. de Oftalmol. 2012, 75, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Vaswani, R.; Singh, A. Importance of defining a target intra-ocular pressure: A Meta-Analysis. Invest. Ophthalmol. Vis. Sci.2012, 53:5052. Invest. Ophthalmol. Vis. Sci. 2012, 53, 5052. [Google Scholar]
- Boland, M.V.; Ervin, A.-M.; Friedman, D.S.; Jampel, H.D.; Hawkins, B.S.; Vollenweider, D.; Chelladurai, Y.; Ward, D.; Suarez-Cuervo, C.; Robinson, K.A. Comparative Effectiveness of Treatments for Open-Angle Glaucoma: A Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2013, 158, 271–279. [Google Scholar] [CrossRef]
- Qu, J.; Wang, D.; Grosskreutz, C.L. Mechanisms of retinal ganglion cell injury and defence in glaucoma. Exp. Eye. Res. 2010, 91, 48–53. [Google Scholar]
- Burgoyne, C.F.; Downs, J.C.; Bellezza, A.J.; Suh, J.-K.F.; Hart, R.T. The optic nerve head as a biomechanical structure: a new paradigm for understanding the role of IOP-related stress and strain in the pathophysiology of glaucomatous optic nerve head damage. Prog. Retin. Eye Res. 2005, 24, 39–73. [Google Scholar] [CrossRef]
- Quigley, H.A.; McKinnon, S.J.; Zack, D.J.; Pease, M.E.; Kerrigan-Baumrind, L.A.; Kerrigan, D.F.; Mitchell, R.S. Retrograde axonal transport of BDNF in retinal ganglion cells is blocked by acute IOP elevation in rats. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3460–3466. [Google Scholar]
- Brubaker, R.F. Goldmann’s equation and clinical measures of aqueous dynamics. Exp. Eye. Res. 2004, 78, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Bill, A. Uveoscleral drainage of aqueous humor: physiology and pharmacology. Prog. Clin. Biol. Res. 1989, 312, 417–427. [Google Scholar] [PubMed]
- Miyazaki, M.; Segawa, K.; Urakawa, Y. Age-related changes in the trabecular meshwork of the normal human eye. Jpn. J. Ophthalmol. 1987, 31, 558–569. [Google Scholar]
- Toris, C.B.; Camras, C.B.; E Yablonski, M. Acute versus chronic effects of brimonidine on aqueous humor dynamics in ocular hypertensive patients. Arch. Ophthalmol. 1999, 128, 8–14. [Google Scholar] [CrossRef]
- Acott, T.S.; Kelley, M.J.; Keller, K.E.; Vranka, J.A.; Abu-Hassan, D.W.; Li, X.; Aga, M.; Bradley, J.M. Intraocular Pressure Homeostasis: Maintaining Balance in a High-Pressure Environment. J. Ocul. Pharmacol. Ther. 2014, 30, 94–101. [Google Scholar] [CrossRef]
- Gedde, S.J.; Chen, P.P.; Muir, K.W.; Vinod, K.; Lind, J.T.; Wright, M.M.; Li, T.; Mansberger, S. L; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Angle-Closure Disease Preferred Practice Pattern®. Ophthalmology. 2021, 128, P30–P70. [Google Scholar]
- Realini, T. A History of Glaucoma Pharmacology. Optom. Vis. Sci. 2011, 88, 36–38. [Google Scholar] [CrossRef]
- US Food and Drug Administration. New drug approval 215092; 22.09.2022. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2022/215092Orig1s000ltr (accessed on 23 June 2023).
- E Trope, G.; Clark, B. Beta adrenergic receptors in pigmented ciliary processes. Br. J. Ophthalmol. 1982, 66, 788–792. [Google Scholar] [CrossRef]
- Elena, P.-P.; Denis, P.; Kosina-Boix, M.; Saraux, H.; Lapalus, P.; Casini, G.; Monte, M.D.; Fornaciari, I.; Filippi, L.; Bagnoli, P.; et al. Beta Adrenergic Binding Sites in the Human Eye: An Autoradiographic Study. J. Ocul. Pharmacol. Ther. 1990, 6, 143–149. [Google Scholar] [CrossRef]
- Bartels, S.P.; O Roth, H.; Jumblatt, M.M.; Neufeld, A.H. Pharmacological effects of topical timolol in the rabbit eye. Investig. Ophthalmol. Vis. Sci. 1980, 19. [Google Scholar]
- Bylund, D.B.; Chacko, D.M. Characterization of alpha2 adrenergic receptor subtypes in human ocular tissue homogenates. Investig. Ophthalmol. Vis. Sci. 1999, 40. [Google Scholar]
- Chiou, G.C.; Chen, Y. Effects of Antiglaucoma Drugs on Ocular Blood Flow in Ocular Hypertensive Rabbits. J. Ocul. Pharmacol. Ther. 1993, 9, 13–24. [Google Scholar] [CrossRef]
- Gilsbach, R.; Röser, C.; Beetz, N.; Brede, M.; Hadamek, K.; Haubold, M.; Leemhuis, J.; Philipp, M.; Schneider, J.; Urbanski, M.; et al. Genetic Dissection of α2-Adrenoceptor Functions in Adrenergic versus Nonadrenergic Cells. Mol. Pharmacol. 2009, 75, 1160–1170. [Google Scholar] [CrossRef] [PubMed]
- Stamer, W.D.; Huang, Y.; Seftor, R.E.; Svensson, S.S.; Snyder, R.W.; Regan, J.W. Cultured human trabecular meshwork cells express functional alpha 2A adrenergic receptors. Investig. Ophthalmol. Vis. Sci. 1996, 37, 2426–2433. [Google Scholar]
- Yamagishi, R.; Honjo, M.; Aihara, M. Effect of IOP-lowering drugs on episcleral venous pressure in mouse eye. Invest. Ophthalmol. Vis. Sci. 2018, 59, 2712. [Google Scholar]
- Gharagozloo, N.Z.; Relf, S.J.; Brubaker, R.F. Aqueous Flow is Reduced by the Alpha-adrenergic Agonist, Apraclonidine Hydrochloride (ALO 2145). Ophthalmology 1988, 95, 1217–1220. [Google Scholar] [CrossRef]
- Toris, C.B.; Tafoya, M.E.; Camras, C.B.; Yablonski, M.E. Effects of Apraclonidine on Aqueous Humor Dynamics in Human Eyes. Ophthalmology 1995, 102, 456–461. [Google Scholar] [CrossRef]
- Goldberg, I.; Galanopoulos, A. Clinical efficacy and neuroprotective effects of brimonidine in the management of glaucoma and ocular hypertension. Clin. Ophthalmol. 2009, 3, 117–122. [Google Scholar] [CrossRef]
- Simsek, T.; Yanik, B.; Conkbayir, I.; Zilelioglu, O.; Eliacik, M.; Erdur, S.K.; Altıok, I.B.; Gulkilik, G.; Aslan, C.A.; Kaya, F.; et al. Comparative Analysis of the Effects of Brimonidine and Dorzolamide on Ocular Blood Flow Velocity in Patients with Newly Diagnosed Primary Open-Angle Glaucoma. J. Ocul. Pharmacol. Ther. 2006, 22, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Enz, T.J.; Bittner, M.; Tribble, J.R.; Williams, P.A.; Thiel, M.A.; Schmid, M.K.; Bachmann, L.M.; Bochmann, F. Comparative Assessment of Retinal Blood Flow Velocity Changes Following Brimonidine and Brinzolamide Administration Using Retinal Function Imaging. Transl. Vis. Sci. Technol. 2022, 11, 16. [Google Scholar] [CrossRef]
- Krupin, T.; Sly, W.S.; Whyte, M.P.; Dodgson, S.J. Failure of Acetazolamide to Decrease Intraocular Pressure in Patients with Carbonic Anhydrase II Deficiency. Am. J. Ophthalmol. 1985, 99, 396–399. [Google Scholar] [CrossRef]
- Maren, T.H. The rates of movement of Na+, Cl-, and HCO-3 from plasma to posterior chamber: effect of acetazolamide and relation to the treatment of glaucoma. Investig. Ophthalmol. 1976, 15, 356–364. [Google Scholar]
- Maus, T.L.; Larsson, L.-I.; McLaren, J.W.; Brubaker, R.F. Comparison of Dorzolamide and Acetazolamide as Suppressors of Aqueous Humor Flow in Humans. Arch. Ophthalmol. 1997, 115, 45–49. [Google Scholar] [CrossRef]
- Camras, C.B.; Bito, L.Z.; E Eakins, K. Reduction of intraocular pressure by prostaglandins applied topically to the eyes of conscious rabbits. Investig. Ophthalmol. Vis. Sci. 1977, 16, 1125–1134. [Google Scholar]
- Lindsey, J.D.; Kashiwagi, K.; Boyle, D.; Kashiwagi, F.; Firestein, G.S.; Weinreb, R.N. Prostaglandins increase proMMP-1 and proMMP-3 secretion by human ciliary smooth muscle cells. Curr. Eye Res. 1996, 15, 869–875. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Kashiwagi, K.; Kashiwagi, F.; Tsukahara, S.; Lindsey, J.D. Prostaglandins increase matrix metalloproteinase release from human ciliary smooth muscle cells. Investig. Ophthalmol. Vis. Sci. 1997, 38. [Google Scholar]
- Ocklind, A. Effect of Latanoprost on the Extracellular Matrix of the Ciliary Muscle. A Study on Cultured Cells and Tissue Sections. Exp. Eye Res. 1998, 67, 179–191. [Google Scholar] [CrossRef]
- Davies, S.S.; Ju, W.-K.; Neufeld, A.H.; Abran, D.; Chemtob, S.; Roberts, L.J. Hydrolysis of Bimatoprost (Lumigan) to its Free Acid by Ocular TissueIn Vitro. J. Ocul. Pharmacol. Ther. 2003, 19, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Ong, T.; Scassellati Sforzolini, B.; Vittitow, J.L.; Singh, K.; Kaufman, P.L. VOYAGER study group. A randomised, controlled comparison of latanoprostene bunod and latanoprost 0.005% in the treatment of ocular hypertension and open-angle glaucoma: the VOYAGER study. Br. J. Ophthalmol. 2015, 99, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Kirihara, T.; Taniguchi, T.; Yamamura, K.; Iwamura, R.; Yoneda, K.; Odani-Kawabata, N.; Shimazaki, A.; Matsugi, T.; Shams, N.; Zhang, J.-Z. Pharmacologic Characterization of Omidenepag Isopropyl, a Novel Selective EP2 Receptor Agonist, as an Ocular Hypotensive Agent. Investig. Opthalmology Vis. Sci. 2018, 59, 145–153. [Google Scholar] [CrossRef]
- Fuwa, M.; Toris, C.B.; Fan, S.; Taniguchi, T.; Ichikawa, M.; Odani-Kawabata, N.; Iwamura, R.; Yoneda, K.; Matsugi, T.; Shams, N.K.; et al. Effects of a Novel Selective EP2 Receptor Agonist, Omidenepag Isopropyl, on Aqueous Humor Dynamics in Laser-Induced Ocular Hypertensive Monkeys. J. Ocul. Pharmacol. Ther. 2018, 34, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Gil, D.W.; A Krauss, H.; Bogardus, A.M.; WoldeMussie, E. Muscarinic receptor subtypes in human iris-ciliary body measured by immunoprecipitation. Investig. Ophthalmol. Vis. Sci. 1997, 38, 1434–1442. [Google Scholar]
- Wiederholt, M.; Schäfer, R.; Wagner, U.; Lepple-Wienhues, A. Contractile response of the isolated trabecular meshwork and ciliary muscle to cholinergic and adrenergic agents. Ger. J. Ophthalmol. 1996, 5, 146–153. [Google Scholar]
- Bleiman, B.S.; Schwartz, A.L. Paradoxical Intraocular Pressure Response to Pilocarpine. Arch. Ophthalmol. 1979, 97, 1305–1306. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, P.L.; Bárány, E.H. Loss of acute pilocarpine effect on outflow facility following surgical disinsertion and retrodisplacement of the ciliary muscle from the scleral spur in the cynomolgus monkey. Investig. Ophthalmol. 1976, 15, 793–807. [Google Scholar]
- Wiederholt, M.; Thieme, H.; Stumpff, F. The regulation of trabecular meshwork and ciliary muscle contractility. Prog. Retin. Eye Res. 2000, 19, 271–295. [Google Scholar] [CrossRef]
- A Erickson, K.; Schroeder, A. Direct effects of muscarinic agents on the outflow pathways in human eyes. Investig. Ophthalmol. Vis. Sci. 2000, 41. [Google Scholar]
- Schneemann, A.; Dijkstra, B.G.; Berg, T.J.v.D.; Kamphuis, W.; Hoyng, P.F. Nitric oxide/guanylate cyclase pathways and flow in anterior segment perfusion. Graefe’s Arch. Clin. Exp. Ophthalmol. 2002, 240, 936–941. [Google Scholar] [CrossRef]
- Cavet, M.E.; Vittitow, J.L.; Impagnatiello, F.; Ongini, E.; Bastia, E. Nitric Oxide (NO): An Emerging Target for the Treatment of Glaucoma. Investig. Opthalmology Vis. Sci. 2014, 55, 5005–5015. [Google Scholar] [CrossRef]
- Kaufman, P.L. Latanoprostene bunod ophthalmic solution 0.024% for IOP lowering in glaucoma and ocular hypertension. Expert Opin. Pharmacother. 2017, 18, 433–444. [Google Scholar] [CrossRef]
- Ishizaki, T.; Maekawa, M.; Fujisawa, K.; Okawa, K.; Iwamatsu, A.; Fujita, A.; Watanabe, N.; Saito, Y.; Kakizuka, A.; Morii, N.; et al. The small GTP-binding protein Rho binds to and activates a 160 kDa Ser/Thr protein kinase homologous to myotonic dystrophy kinase. EMBO J. 1996, 15, 1885–1893. [Google Scholar] [CrossRef]
- Rao, P.V.; Pattabiraman, P.P.; Kopczynski, C. Role of the Rho GTPase/Rho kinase signaling pathway in pathogenesis and treatment of glaucoma: Bench to bedside research. Exp. Eye Res. 2017, 158, 23–32. [Google Scholar] [CrossRef]
- 54. Buffault, J.; Brignole-Baudouin, F.; Reboussin, É.; Kessal, K.; Labbé, A.; Mélik Parsadaniantz, S.; Baudouin, C. The Dual Effect of Rho-Kinase Inhibition on Trabecular Meshwork Cells Cytoskeleton and Extracellular Matrix in an In Vitro Model of Glaucoma. J. Clin. Med. 2022, 11, 1001. [Google Scholar] [CrossRef]
- Wang, R.-F.; Williamson, J.E.; Kopczynski, C.; Serle, J.B. Effect of 0.04% AR-13324, a ROCK, and Norepinephrine Transporter Inhibitor, on Aqueous Humor Dynamics in Normotensive Monkey Eyes. Eur. J. Gastroenterol. Hepatol. 2015, 24, 51–54. [Google Scholar] [CrossRef]
- Toris, C.B.; McLaughlin, M.A.; Dworak, D.P.; Fan, S.; Havens, S.; Zhan, G.-L.; Horan, N.; Prasanna, G. Effects of Rho Kinase Inhibitors on Intraocular Pressure and Aqueous Humor Dynamics in Nonhuman Primates and Rabbits. J. Ocul. Pharmacol. Ther. 2016, 32, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.C.; Konstas, A.G.; Nelson, L.A.; Kruft, B. Meta-analysis of 24-Hour Intraocular Pressure Studies Evaluating the Efficacy of Glaucoma Medicines. Ophthalmology 2008, 115, 1117–1122.e1. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative effectiveness of first-line medications for primary open-angle glaucoma: A systematic review and network meta-analysis. Ophthalmology. 2016, 123, 129–140. [Google Scholar] [CrossRef] [PubMed]
- van der Valk, R.; Webers, C.A.; Schouten, J.S.; Zeegers, M.P.; Hendrikse, F.; Prins, M.H. Intraocular Pressure–Lowering Effects of All Commonly Used Glaucoma Drugs: A Meta-analysis of Randomized Clinical Trials. Ophthalmology 2005, 112, 1177–1185. [Google Scholar] [CrossRef]
- Freiberg, J.C.; von Spreckelsen, A.; Khachatryan, N.; Kolko, M.; Azuara-Blanco, A.; Virgili, G. Rho kinase inhibitor for primary open-angle glaucoma and ocular hypertension. Cochrane Database Syst. Rev. 2022, 6, CD013817. [Google Scholar] [CrossRef]
- Moussa, W.G.E.H.; Farhat, R.G.; Nehme, J.C.; Sahyoun, M.A.; Schakal, A.R.; Jalkh, A.E.; Karam, M.P.A.; Azar, G.G. Comparison of Efficacy and Ocular Surface Disease Index Score between Bimatoprost, Latanoprost, Travoprost, and Tafluprost in Glaucoma Patients. J. Ophthalmol. 2018, 2018, 1319628. [Google Scholar] [CrossRef]
- Tang, W.; Zhang, F.; Liu, K.; Duan, X. Efficacy, and safety of prostaglandin analogues in primary open-angle glaucoma or ocular hypertension patients: A meta-analysis. Medicine. (Baltimore) 2019, 98, e16597. [Google Scholar] [PubMed]
- Lin, L.; Zhao, Y.J.; Chew, P.T.; Sng, C.C.A.; Wong, H.-T.; Yip, L.W.; Wu, T.S.; Bautista, D.; Teng, M.; Khoo, A.L.; et al. Comparative Efficacy and Tolerability of Topical Prostaglandin Analogues for Primary Open-Angle Glaucoma and Ocular Hypertension. Ann. Pharmacother. 2014, 48, 1585–1593. [Google Scholar] [CrossRef]
- Matsuo, M.; Matsuoka, Y.; Tanito, M. Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension. Clin. Ophthalmol. 2022, ume 16, 1261–1279. [Google Scholar] [CrossRef]
- Aihara, M.; Lu, F.; Kawata, H.; Iwata, A.; Odani-Kawabata, N.; Shams, N.K. Omidenepag isopropyl versus latanoprost in primary open-angle glaucoma and ocular hypertension: the Phase 3 AYAME Study. Am. J. Ophthalmol. 2020, 220, 53–63. [Google Scholar] [CrossRef]
- Cai, Z.; Cao, M.; Liu, K.; Duan, X. Analysis of the Responsiveness of Latanoprost, Travoprost, Bimatoprost, and Tafluprost in the Treatment of OAG/OHT Patients. J. Ophthalmol. 2021, 2021, 5586719. [Google Scholar] [CrossRef]
- Zimmerman, T.J.; Kaufman, H.E. Timolol, dose response and duration of action. Arch. Ophthalmol. 1977, 95, 605–607. [Google Scholar] [CrossRef]
- Berry, D.P. Jr.; Van Buskirk, E.M.; Shields, M.B. Betaxolol and timolol: A comparison of efficacy and side effects. Arch. Ophthalmol. 1984, 102, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Schadlu, R.; Maus, T.L.; Nau, C.B.; Brubaker, R.F. Comparison of the efficacy of apraclonidine and brimonidine as aqueous suppressants in humans. Arch. Ophthalmol. 1998, 116, 1441–1444. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, A.; Singh, G. Efficacy of three different formulations of brimonidine for control of intraocular pressure in primary open-angle glaucoma: A 6-week randomized trial. Oman. J. Ophthalmol. 2018, 11, 140–143. [Google Scholar] [CrossRef]
- Stewart, W.C.; Konstas, A.G.; Kruft, B.; Mathis, H.M.; Stewart, J.A. Meta-Analysis of 24-h Intraocular Pressure Fluctuation Studies and the Efficacy of Glaucoma Medicines. J. Ocul. Pharmacol. Ther. 2010, 26, 175–180. [Google Scholar] [CrossRef]
- Harris, L.S.; Galin, M.A. Dose Response Analysis of Pilocarpine-Induced Ocular Hypotension. Arch. Ophthalmol. 1970, 84, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Diestelhorst, M. The additive intraocular pressure-lowering effect of latanoprost 0.005% daily once and pilocarpine 2% t.i.d. in patients with open-angle glaucoma or ocular hypertension. a 6-month, randomized, multicenter study. German Latanoprost Study Group. Graefes. Arch. Clin. Exp. Ophthalmol. 2000, 238, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Hartenbaum, D.; Maloney, S.; Vaccarelli, L.; Liss, C.; Wilson, H.; Gormley, G.J. Comparison of dorzolamide and pilocarpine as adjunctive therapy in patients with open-angle glaucoma and ocular hypertension. Clin. Ther. 1999, 21, 1533–1538. [Google Scholar] [CrossRef]
- Ikegami, K.; Shigeyoshi, Y.; Masubuchi, S. Circadian Regulation of IOP Rhythm by Dual Pathways of Glucocorticoids and the Sympathetic Nervous System. Investig. Opthalmology Vis. Sci. 2020, 61, 26. [Google Scholar] [CrossRef]
- Liu, J.H.K.; Weinreb, R.N. Asymmetry of Habitual 24-Hour Intraocular Pressure Rhythm in Glaucoma Patients. Investig. Opthalmology Vis. Sci. 2014, 55, 7398–7402. [Google Scholar] [CrossRef]
- Neroev, V.; Malishevskaya, T.; Weinert, D.; Astakhov, S.; Kolomeichuk, S.; Cornelissen, G.; Kabitskaya, Y.; Boiko, E.; Nemtsova, I.; Gubin, D. Disruption of 24-Hour Rhythm in Intraocular Pressure Correlates with Retinal Ganglion Cell Loss in Glaucoma. Int. J. Mol. Sci. 2020, 22, 359. [Google Scholar] [CrossRef] [PubMed]
- Matlach, J.; Bender, S.; König, J.; Binder, H.; Pfeiffer, N.; Hoffmann, E.M. Investigation of intraocular pressure fluctuation as a risk factor of glaucoma progression. Clin. Ophthalmol. 2018, ume 13, 9–16. [Google Scholar] [CrossRef]
- Drance, S.M. The Significance of the Diurnal Tension Variations in Normal and Glaucomatous Eyes. Arch. Ophthalmol. 1960, 64, 494–501. [Google Scholar] [CrossRef]
- Tsironi, S.; Almaliotis, D.; Ntonti, P.; Sidiropoulos, G.; Theodoridou, E.; Theofrastou, E.; Karachrysafi, S.; Psimenidou, E.; Sarafi, A.; Kapourani, V.; et al. Clinical Outcomes of the Implementation of IOP Monitoring, in and out of Office Time, to 1500 Patients—A Cohort Study. Vision 2022, 6, 69. [Google Scholar] [CrossRef]
- Barkana, Y.; Anis, S.; Liebmann, J.; Tello, C.; Ritch, R. Clinical Utility of Intraocular Pressure Monitoring Outside of Normal Office Hours in Patients With Glaucoma. Arch. Ophthalmol. 2006, 124, 793–797. [Google Scholar] [CrossRef]
- Orzalesi, N.; Rossetti, L.; Invernizzi, T.; Bottoli, A.; Autelitano, A. Effect of timolol, latanoprost, and dorzolamide on circadian IOP in glaucoma or ocular hypertension. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2566–2573. [Google Scholar]
- Yildirim, N.; Sahin, A.; Gultekin, S. The Effect of Latanoprost, Bimatoprost, and Travoprost on Circadian Variation of Intraocular Pressure in Patients With Open-angle Glaucoma. Eur. J. Gastroenterol. Hepatol. 2008, 17, 36–39. [Google Scholar] [CrossRef]
- Orzalesi, N.; Rossetti, L.; Bottoli, A.; Fogagnolo, P. Comparison of the Effects of Latanoprost, Travoprost, and Bimatoprost on Circadian Intraocular Pressure in Patients with Glaucoma or Ocular Hypertension. Ophthalmology 2006, 113, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Konstas, A.G.; Stewart, W.C.; Topouzis, F.; Tersis, I.; Holmes, K.T.; Stangos, N.T. Brimonidine 0.2% given two or three times daily versus timolol maleate 0.5% in primary open-angle glaucoma. Arch. Ophthalmol. 2001, 131, 729–733. [Google Scholar] [CrossRef]
- Orzalesi, N.; Rossetti, L.; Bottoli, A.; Fumagalli, E.; Fogagnolo, P. The Effect of Latanoprost, Brimonidine, and a Fixed Combination of Timolol and Dorzolamide on Circadian Intraocular Pressure in Patients With Glaucoma or Ocular Hypertension. Arch. Ophthalmol. 2003, 121, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Medeiros, F.A.; Slight, J.R.; Weinreb, R.N. Diurnal and Nocturnal Effects of Brimonidine Monotherapy on Intraocular Pressure. Ophthalmology 2010, 117, 2075–2079. [Google Scholar] [CrossRef]
- Gulati, V.; Fan, S.; Zhao, M.; Maslonka, M.A.; Gangahar, C.; Toris, C.B. Diurnal and Nocturnal Variations in Aqueous Humor Dynamics of Patients With Ocular Hypertension Undergoing Medical Therapy. JAMA Ophthalmol 2012, 130, 677–684. [Google Scholar] [CrossRef]
- Lee, P.W.-Y.; Doyle, A.; Stewart, J.A.; Kristoffersen, C.J.; Stewart, W.C. Meta-analysis of timolol on diurnal and nighttime intraocular pressure and blood pressure. Eur. J. Ophthalmol. 2010, 20, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- E Topper, J.; Brubaker, R.F. Effects of timolol, epinephrine, and acetazolamide on aqueous flow during sleep. Investig. Ophthalmol. Vis. Sci. 1985, 26, 1315–1319. [Google Scholar]
- Oddone, F.; Rossetti, L.; Tanga, L.; Berardo, F.; Ferrazza, M.; Michelessi, M.; Roberti, G.; Manni, G.; Centofanti, M. Effects of Topical Bimatoprost 0.01% and Timolol 0.5% on Circadian IOP, Blood Pressure and Perfusion Pressure in Patients with Glaucoma or Ocular Hypertension: A Randomized, Double Masked, Placebo-Controlled Clinical Trial. PLOS ONE 2015, 10, e0140601. [Google Scholar] [CrossRef]
- Liu, J.H.; Slight, J.R.; Vittitow, J.L.; Sforzolini, B.S.; Weinreb, R.N. Efficacy of Latanoprostene Bunod 0.024% Compared With Timolol 0.5% in Lowering Intraocular Pressure Over 24 Hours. Am. J. Ophthalmol. 2016, 169, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Walters, T.R.; DuBiner, H.B.; Carpenter, S.P.; Khan, B.; VanDenburgh, A.M. 24-Hour IOP control with once-daily bimatoprost, timolol gel-forming solution, or latanoprost: a 1-month, randomized, comparative clinical trial. Surv. Ophthalmol. 2004, 49, S26–S35. [Google Scholar] [CrossRef] [PubMed]
- 94. Shiratori, N.; Nishio, Y.; Takeda, A.; Sugimoto, S.; Takazawa, K.; Otsuka, N.; Ishida, N.; Shii, D.; Hori, K.; Nakamoto, K. Twenty-four-hour intraocular pressure control with omidenepag isopropyl 0.002% in patients with glaucoma and ocular hypertension. Clin. Ophthalmol. 2021, 15, 3997–4003. [Google Scholar] [CrossRef] [PubMed]
- Van de Velde, S.; Van Bergen, T.; Sijnave, D.; Hollanders, K.; Castermans, K.; Defert, O.; Leysen, D.; Vandewalle, E.; Moons, L.; Stalmans, I. AMA0076, a Novel, Locally Acting Rho Kinase Inhibitor, Potently Lowers Intraocular Pressure in New Zealand White Rabbits with Minimal Hyperemia. Investig. Opthalmology Vis. Sci. 2014, 55, 1006–1016. [Google Scholar] [CrossRef]
- Araujo, S.V.; Bond, J.B.; Wilson, R.P.; Moster, M.R.; Schmidt, C.M. Jr.; Spaeth, G.L. Long term effect of apraclonidine. Br. J. Ophthalmol. 1995, 79, 1098–1101. [Google Scholar] [CrossRef]
- Derick, R.J.; Robin, A.L.; Walters, T.R.; Barnebey, H.S.; Choplin, N.; Schuman, J.; Kelley, E.P.; Chen, K.; Stoecker, J.F. Brimonidine tartrate: a one-month dose response study. Ophthalmology. 1997, 104, 131–136. [Google Scholar] [CrossRef]
- Strahlman, E.; Tipping, R.; Vogel, R. A Double-Masked, Randomized 1-Year Study Comparing Dorzolamide (Trusopt), Timolol, and Betaxolol. Arch. Ophthalmol. 1995, 113, 1009–1016. [Google Scholar] [CrossRef]
- Bito, L.Z. A new approach to the medical management of glaucoma, from the bench to the clinic, and beyond: the Proctor Lecture. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1126–1133. [Google Scholar]
- Riva, I.; Katsanos, A.; Floriani, I.; Biagioli, E.; Konstas, A.G.; Centofanti, M.; Quaranta, L. Long-term 24-hour Intraocular Pressure Control With Travoprost Monotherapy in Patients With Primary Open-angle Glaucoma. Eur. J. Gastroenterol. Hepatol. 2014, 23, 535–540. [Google Scholar] [CrossRef]
- Steinert, R.F.; Thomas, J.V.; Boger, W.P. Long-term Drift and Continued Efficacy After Multiyear Timolol Therapy. Arch. Ophthalmol. 1981, 99, 100–103. [Google Scholar] [CrossRef]
- Piltz, J.; Gross, R.; Shin, D.H.; Beiser, J.A.; Dorr, D.A.; Kass, M.A.; Gordon, M.O. Contralateral effect of topical beta-adrenergic antagonists in initial one-eyed trials in the ocular hypertension treatment study. Am. J. Ophthalmol. 2000, 130, 441–453. [Google Scholar] [CrossRef]
- 103. Yuksel, N.; Karabas, L.; Altintas, O.; Yildirim, Y.; Caglar, Y. A Comparison of the Short-Term Hypotensive Effects and Side Effects of Unilateral Brimonidine and Apraclonidine in Patients with Elevated Intraocular Pressure. Ophthalmologica 2002, 216, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.L.; Senthil, S.; Garudadri, C.S. Contralateral intraocular pressure lowering effect of prostaglandin analogues. Indian J. Ophthalmol. 2014, 62, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Dunham, C.N.; Spaide, R.F.; Dunham, G. The contralateral reduction of intraocular pressure by timolol. Br. J. Ophthalmol. 1994, 78, 38–40. [Google Scholar] [CrossRef]
- Sit, A.J.; Gupta, D.; Kazemi, A.; McKee, H.; Challa, P.; Liu, K.C.; Lopez, J.; Kopczynski, C.; Heah, T. Netarsudil Improves Trabecular Outflow Facility in Patients with Primary Open Angle Glaucoma or Ocular Hypertension: A Phase 2 Study. Am. J. Ophthalmol. 2021, 226, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Chen, V.; Cruz, M.; Pottenburgh, J.; Saeedi, O.J. Precise quantification of episcleral venous flow rates inhuman subjects before and after netarsudil 0. 02%. Invest. Ophthalmol. Vis. Sci. 2022, 63, 3497. [Google Scholar]
- Suzuki, M.; Suzuki, Y.; Komori, R.; Orii, Y.; Arimura, S.; Iwasaki, K.; Takamura, Y.; Inatani, M. Aqueous column changes in the episcleral veins after the instillation of ripasudil versus latanoprost: a randomized, double-blind, crossover clinical trial. Sci. Rep. 2022, 12, 15255. [Google Scholar] [CrossRef]
- Lee, S.S.; Burke, J.; Shen, J.; Almazan, A.; Orilla, W.; Hughes, P.; Zhang, J.; Li, H.; Struble, C.; Miller, P.E.; et al. EMGT Group. Bimatoprost sustained-release intracameral implant reduces episcleral venous pressure in dogs. Veter- Ophthalmol. 2018, 21, 376–381. [Google Scholar] [CrossRef]
- Leske, M.C.; Heijl, A.; Hyman, L.; Bengtsson, B.; Dong, L.; Yang, Z. Predictors of Long-term Progression in the Early Manifest Glaucoma Trial. Ophthalmology 2007, 114, 1965–1972. [Google Scholar] [CrossRef]
- Leske, M.C.; Wu, S.-Y.; Hennis, A.; Honkanen, R.; Nemesure, B. Risk Factors for Incident Open-angle Glaucoma: The Barbados Eye Studies. Ophthalmology 2008, 115, 85–93. [Google Scholar] [CrossRef]
- Cherecheanu, A.P.; Garhofer, G.; Schmidl, D.; Werkmeister, R.; Schmetterer, L. Ocular perfusion pressure and ocular blood flow in glaucoma. Curr. Opin. Pharmacol. 2013, 13, 36–42. [Google Scholar] [CrossRef]
- Hayreh, S.S. Blood flow in the optic nerve head and factors that may influence it. Prog. Retin. Eye. Res. 2001, 20, 595—624. [Google Scholar]
- Kolli, A.; Toris, C.B.; Reed, D.M.; Gilbert, J.; Sit, A.J.; Gulati, V.; Kazemi, A.; Fan, S.; Musch, D.C.; Moroi, S.E. The effects of topical timolol and latanoprost on calculated ocular perfusion pressure in non-glaucomatous volunteers. J. Ocul. Pharmacol. Ther. 2021, 37, 565–574. [Google Scholar] [CrossRef]
- Ishibashi, S.; Hirose, N.; Tawara, A.; Kubota, T. Effect of Latanoprost on the Diurnal Variations in the Intraocular and Ocular Perfusion Pressure in Normal Tension Glaucoma. Eur. J. Gastroenterol. Hepatol. 2006, 15, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Costagliola, C.; Parmeggiani, F.; Virgili, G.; Lamberti, G.; Incorvaia, C.; Perri, P.; Campa, C.; Sebastiani, A. Circadian changes of intraocular pressure and ocular perfusion pressure after timolol or latanoprost in Caucasians with normal-tension glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 246, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhou, X.; Zhao, Y.; Yang, X.; Zhou, D.; Chen, B.; Duan, X. Effects of Tafluprost on Ocular Blood Flow. Ophthalmol. Ther. 2022, 11, 1991–2003. [Google Scholar] [CrossRef] [PubMed]
- Seibold, L.K.; DeWitt, P.E.; Kroehl, M.E.; Kahook, M.Y. The 24-Hour Effects of Brinzolamide/Brimonidine Fixed Combination and Timolol on Intraocular Pressure and Ocular Perfusion Pressure. J. Ocul. Pharmacol. Ther. 2017, 33, 161–169. [Google Scholar] [CrossRef]
- Liu, C.J.-L.; Ko, Y.-C.; Cheng, C.-Y.; Chiu, A.W.; Chou, J.C.; Hsu, W.-M.; Liu, J.-H. Changes in intraocular pressure and ocular perfusion pressure after latanoprost 0.005% or brimonidine tartrate 0.2% in normal-tension glaucoma patients. Ophthalmology 2002, 109, 2241–2247. [Google Scholar] [CrossRef]
- Pillunat, L.E.; Stodtmeister, R.; Vetrugno, M.; Cardascia, N.; Cantatore, F.; Sborgia, C.; Gugleta, K.; Costa, V.P.; Harris, A.; Stefánsson, E.; et al. Effect of Different Antiglaucomatous Drugs on Ocular Perfusion Pressures. J. Ocul. Pharmacol. Ther. 1988, 4, 231–242. [Google Scholar] [CrossRef]
- Siesky, B.; Harris, A.; Brizendine, E.; Marques, C.; Loh, J.; Mackey, J.; Overton, J.; Netland, P. Literature Review and Meta-Analysis of Topical Carbonic Anhydrase Inhibitors and Ocular Blood Flow. Surv. Ophthalmol. 2009, 54, 33–46. [Google Scholar] [CrossRef]
- Samaha, D.; Diaconu, V.; Bouchard, J.F.; Desalliers, C.; Dupont, A. Effect of Latanoprostene Bunod on Optic Nerve Head Blood Flow. Optom. Vis. Sci. 2022, 99, 172–176. [Google Scholar] [CrossRef]
- WoldeMussie, E.; Ruiz, G.; Wijono, M.; Wheeler, L.A. Neuroprotection of retinal ganglion cells by brimonidine in rats with laser-induced chronic ocular hypertension. Investig. Ophthalmol. Vis. Sci. 2001, 42. [Google Scholar]
- Evans, D.W.; Hosking, S.L.; Gherghel, D.; Bartlett, J.D. Contrast sensitivity improves after brimonidine therapy in primary open angle glaucoma: a case for neuroprotection. Br. J. Ophthalmol. 2003, 87, 1463–1465. [Google Scholar] [CrossRef]
- Ichhpujani, P.; Rodrigues, A.M.; Kumar, S.; Singh, R.B. Analysing the change in contrast sensitivity post-travoprost treatment in primary open-angle glaucoma patients using Spaeth Richman contrast sensitivity test. Int. Ophthalmol. 2022, 43, 2037–2047. [Google Scholar] [CrossRef]
- Amanullah, S.; Okudolo, J.; Rahmatnejad, K.; Lin, S.-C.; Wizov, S.S.; Muhire, R.S.M.; Hark, L.A.; Zheng, C.X.; Zhan, T.; Spaeth, G.L. The relationship between contrast sensitivity and retinal nerve fiber layer thickness in patients with glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2415–2422. [Google Scholar] [CrossRef]
- Tsai, J.-C.; Chang, H.-W.; Arthur, S.; Cantor, L.B.; Goldenberg-Cohen, N.; Dadon-Bar-El, S.; Hasanreisoglu, M.; Avraham-Lubin, B.C.R.; Dratviman-Storobinsky, O.; Cohen, Y.; et al. Comparison of the Effects of Brimonidine 0.2% and Timolol 0.5% on Retinal Nerve Fiber Layer Thickness in Ocular Hypertensive Patients: A Prospective, Unmasked Study. J. Ocul. Pharmacol. Ther. 2005, 21, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, R.; Aihara, M.; Araie, M. Neuroprotective effects of prostaglandin analogues on retinal ganglion cell death independent of intraocular pressure reduction. Exp. Eye Res. 2011, 93, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.M.; Nagrale, P. Rho Kinase Inhibitors as a Neuroprotective Pharmacological Intervention for the Treatment of Glaucoma. Cureus 2022, 14, e28445. [Google Scholar] [CrossRef]
- Tomita, G.; Araie, M.; Kitazawa, Y.; Tsukahara, S. A three-year prospective, randomized and open comparison between latanoprost and timolol in Japanese normal-tension glaucoma patients. Eye 2014, 18, 984–989. [Google Scholar] [CrossRef]
- Inoue, K.; Fujimoto, T.; Shiokawa, M.; Tomita, G. Effects of treatment with bimatoprost 0.03% for 3 years in patients with normal-tension glaucoma. Clin. Ophthalmol. 2014, 8, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Carpineto, P.; Ciancaglini, M.; Gallenga, P.E. A 12-month, randomized, double-masked study comparing latanoprost with timolol in pigmentary glaucoma. Ophthalmology 1999, 106, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Sihota, R.; Saxena, R.; Agarwal, H.C.; Gulati, V. Crossover Comparison of Timolol and Latanoprost in Chronic PrimaryAngle-closure Glaucoma. Arch. Ophthalmol. 2004, 122, 185–189. [Google Scholar] [CrossRef]
- Chen, M.-J.; Chen, Y.-C.; Chou, C.-K.; Hsu, W.-M. Comparison of the Effects of Latanoprost and Travoprost on Intraocular Pressure in Chronic Angle-Closure Glaucoma. J. Ocul. Pharmacol. Ther. 2006, 22, 449–454. [Google Scholar] [CrossRef]
- Konstas, A.G.P.; Hollo, G.; Irkec, M.; Tsironi, S.; Durukan, I.; Goldenfeld, M.; Melamed, S. Diurnal IOP control with bimatoprost versus latanoprost in exfoliative glaucoma: a crossover, observer-masked, three-centre study. Br. J. Ophthalmol. 2006, 91, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Konstas, A.G.; Kozobolis, V.P.; Katsimpris, I.E.; Boboridis, K.; Koukoula, S.; Jenkins, J.N.; Stewart, W.C. Efficacy and Safety of Latanoprost versus Travoprost in Exfoliative Glaucoma Patients. Ophthalmology 2007, 114, 653–657. [Google Scholar] [CrossRef]
- Aihara, M.; Ropo, A.; Lu, F.; Kawata, H.; Iwata, A.; Odani-Kawabata, N.; Shams, N. Intraocular pressure-lowering effect of omidenepag isopropyl in latanoprost non-/low-responder patients with primary open-angle glaucoma or ocular hypertension: the FUJI study. Jpn. J. Ophthalmol. 2020, 64, 398–406. [Google Scholar] [CrossRef]
- Rossetti, L.; Gandolfi, S.; Traverso, C.; Montanari, P.; Uva, M.; Manni, G.; Carassa, R.; Mastropasqua, L.; Quaranta, L.; Marchini, G.; et al. An evaluation of the rate of nonresponders to latanoprost therapy. J. Glaucoma. 2006, 15, 238–243. [Google Scholar] [CrossRef]
- Inoue, K.; Inoue, J.; Kunimatsu-Sanuki, S.; Nozaki, N.; Shimizu, K.; Ishida, K.; Tomita, G. Short-Term Efficacy and Safety of Omidenepag Isopropyl in Patients with Normal-Tension Glaucoma. Clin. Ophthalmol. 2020, ume 14, 2943–2949. [Google Scholar] [CrossRef]
- Miki, A.; Miyamoto, E.; Ishida, N.; Shii, D.; Hori, K.; LESPOIR Research Group. Efficacy and safety of omidenepag isopropyl 0.002% ophthalmic solution: A retrospective analysis of real-world data in Japan. Adv. Ther. 2022, 39, 2085–2095. [Google Scholar] [CrossRef]
- Rouland, J.-F.; Morel-Mandrino, P.; Elena, P.-P.; Polzer, H.; Raj, P.S. Timolol 0.1% Gel (Nyogel 0.1%®) Once Daily versus Conventional Timolol 0.5% Solution Twice Daily: A Comparison of Efficacy and Safety. Ophthalmologica 2002, 216, 449–454. [Google Scholar] [CrossRef]
- Harris, A.; Arend, O.; Chung, H.S.; Kagemann, L.; Cantor, L.; Martin, B. A comparative study of betaxolol and dorzolamide effect on ocular circulation in normal-tension glaucoma patients. Ophthalmology 2000, 107, 430–434. [Google Scholar] [CrossRef]
- Gandolfi, S.; Cimino, L.; Mora, P. Effect of brimonidine on intraocular pressure in normal tension glaucoma: a short term clinical trial. Eur. J. Ophthalmol. 2003, 13, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Tsumura, T.; Yoshikawa, K.; Kimura, T.; Suzumura, H.; Kawashima, M.; Nanno, M.; Ishijima, K.; Takeda, R. The efficacy and safety of add-on 0. 1% brimonidine tartrate preserved with sodium chlorite in on-treatment Japanese normal-tension glaucoma patients. Clin. Ophthalmol. 2014, 8, 1681–1687. [Google Scholar] [PubMed]
- Ogata, N.; Kanda, T.; Kawahata, M.; Ichikawa, T.; Matsumoto, Y.; Morimitsu, W.; Nishino, Y.; Itoi, T.; Furumoto, K. Sedative and physiological effects of brimonidine tartrate ophthalmic solution in healthy cats. Veter- Anaesth. Analg. 2017, 44, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Enyedi, L.B.; Freedman, S.F. Safety and efficacy of brimonidine in children with glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2001, 5, 281–284. [Google Scholar] [CrossRef]
- Greiner, R.C.; Beasley, H.M.; Bodhireddy, H.; Bouterse, C.R.; Eggleston, M.T.; Pfeiffer, D.C. Revisiting acidosis in acetazolamide treatment of severe glaucoma: A case report. Am. J. Ophthalmol. Case Rep. 2022, 27, 101658. [Google Scholar] [CrossRef]
- Nakamura, Y.; Ishikawa, S.; Nakamura, Y.; Sakai, H.; Henzan, I.; Sawaguchi, S. 24-hour intraocular pressure in glaucoma patients randomized to receive dorzolamide or brinzolamide in combination with latanoprost. Clin. Ophthalmol. 2009, 3, 395–400. [Google Scholar]
- Ott, E.Z.; Mills, M.D.; Arango, S.; Getson, A.J.; Assaid, C.A.; Adamsons, I.A. A Randomized Trial Assessing Dorzolamide in Patients With Glaucoma Who Are Younger Than 6 Years. Arch. Ophthalmol. 2005, 123, 1177–1186. [Google Scholar] [CrossRef]
- Zimmerman, T.J.; Kooner, K.S.; Kandarakis, A.S.; Ziegler, L.P. Improving the Therapeutic Index of Topically Applied Ocular Drugs. Arch. Ophthalmol. 1984, 102, 551–553. [Google Scholar] [CrossRef]
- I Phillips, C.; Clark, C.V.; Levy, A.M. Posterior synechiae after glaucoma operations: aggravation by shallow anterior chamber and pilocarpine. Br. J. Ophthalmol. 1987, 71, 428–432. [Google Scholar] [CrossRef]
- Yoo, Y.-J.; Hwang, J.-M.; Yang, H.K. Dilute pilocarpine test for diagnosis of Adie’s tonic pupil. Sci. Rep. 2021, 11, 10089. [Google Scholar] [CrossRef]
- Tanasiewicz, M.; Hildebrandt, T.; Obersztyn, I. Xerostomia of Various Etiologies: A Review of the Literature. Adv. Clin. Exp. Med. 2016, 25, 199–206. [Google Scholar] [CrossRef]
- Tucker, T.; Early, J. Pilocarpine 1. 25% Ophthalmic Solution (Vuity) for the Treatment of Presbyopia.. 2023, 107, 659–660. [Google Scholar]
- Futakuchi, A.; Morimoto, T.; Ikeda, Y.; Tanihara, H.; Inoue, T.; Aihara, M.; Arimura, S.; Fukuchi, T.; Higashide, T.; Honjo, M.; et al. ROCK-S study group collaborators. Intraocular pressure-lowering effects of ripasudil in uveitic glaucoma, exfoliation glaucoma, and steroid-induced glaucoma patients: ROCK-S, a multicentre historical cohort study. Sci. Rep. 2020, 10, 10308. [Google Scholar] [CrossRef]
- Carstairs, J.R.; Nimmo, A.J.; Barnes, P.J. Autoradiographic visualization of beta-adrenoceptor subtypes in human lung. Am. Rev. Respir. Dis. 1985, 132, 541–547. [Google Scholar] [CrossRef]
- Avorn, J.; Glynn, R.J.; Gurwitz, J.H.; Bohn, R.L.; Monane, M.; Everitt, D.E.; Gilden, D.; Choodnovskiy, I. Adverse pulmonary effects of topical β-blockers used in the treatment of glaucoma. J. Glaucoma. 1995, 2, 158–165. [Google Scholar] [CrossRef]
- Sadiq, S.A.; Fielding, K.; Vernon, S.A. The effect of timolol drops on respiratory function. Eye 1998, 12, 386–389. [Google Scholar] [CrossRef]
- Kirwan, J.F.; Nightingale, J.A.; Bunce, C.; Wormald, R. Do selective topical beta antagonists for glaucoma have respiratory side effects? B.r J. Ophthalmol. 2004, 88, 196–198. [Google Scholar] [CrossRef]
- Müller, L.; Jensen, B.P.; Bachmann, L.M.; Wong, D.; Wells, A.P. New technique to reduce systemic side effects of timolol eye drops: The tissue press method—Cross-over clinical trial. Clin. Exp. Ophthalmol. 2019, 48, 24–30. [Google Scholar] [CrossRef]
- Ramdas, W.D.; van der Velde, N.; van der Cammen, T.J.; Wolfs, R.C. Evaluation of risk of falls and orthostatic hypotension in older, long-term topical beta-blocker users. Graefes. Arch. Clin. Exp. Ophthalmol. 2009, 247, 1235–1241. [Google Scholar]
- Farkouh, A.; Frigo, P.; Czejka, M. Systemic side effects of eye drops: a pharmacokinetic perspective. Clin. Ophthalmol. 2016, ume 10, 2433–2441. [Google Scholar] [CrossRef]
- Sridharrao, B.; Badrinath, S.S. Efficacy and safety of apraclonidine in patients undergoing anterior segment laser surgery. Br. J. Ophthalmol. 1989, 73, 884–887. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, L.; Gandolfo, F.; Turano, R.; Rovida, F.; Pizzolante, T.; Musig, A.; Gandolfo, E. Effects of Topical Hypotensive Drugs on Circadian IOP, Blood Pressure, and Calculated Diastolic Ocular Perfusion Pressure in Patients with Glaucoma. Investig. Opthalmology Vis. Sci. 2006, 47, 2917–2923. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, S.; Nitta, K.; Shirakashi, M.; Nitta, A.; Yamabayashi, S.; Kimura, T.; Ueda, T.; Takeda, R.; Matsumoto, S.; Yoshikawa, K. Multicenter, Randomized, Investigator-Masked Study Comparing Brimonidine Tartrate 0.1% and Timolol Maleate 0.5% as Adjunctive Therapies to Prostaglandin Analogues in Normal-Tension Glaucoma. Adv. Ther. 2017, 34, 1438–1448. [Google Scholar] [CrossRef]
- Zheng, Y.; Wong, T.Y.; Mitchell, P.; Friedman, D.S.; He, M.; Aung, T. Distribution of Ocular Perfusion Pressure and Its Relationship with Open-Angle Glaucoma: The Singapore Malay Eye Study. Investig. Opthalmology Vis. Sci. 2010, 51, 3399–3404. [Google Scholar] [CrossRef]
- Morris, S.; Geh, V.; Nischal, K.K.; Sahi, S.; Ahmed, M.A.S. Topical dorzolamide and metabolic acidosis in a neonate. Br. J. Ophthalmol. 2003, 87, 1052–1053. [Google Scholar] [CrossRef]
- Hoffmanová, I.; Sánchez, D. Metabolic acidosis and anaemia associated with dorzolamide in a patient with impaired renal function. Br. J. Clin. Pharmacol. 2018, 84, 796–799. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Ling, X.C.; Tsai, W.-H.; Liu, J.-S.; Kuo, K.-L. Risks of Topical Carbonic Anhydrase Inhibitors in Glaucoma Patients With Chronic Kidney Disease: A Nationwide Population-Based Study. Arch. Ophthalmol. 2023, 253, 49–55. [Google Scholar] [CrossRef]
- Levy, B.; Ramirez, N.; Novack, G.D.; Kopczynski, C. Ocular Hypotensive Safety and Systemic Absorption of AR-13324 Ophthalmic Solution in Normal Volunteers. Am. J. Ophthalmol. 2015, 159, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Defert, O.; Boland, S. Rho kinase inhibitors: a patent review (2014 – 2016). Expert Opin. Ther. Patents 2017, 27, 507–515. [Google Scholar] [CrossRef]
- Rouland, J.F.; Le Pen, C.; Gouveia Pinto, C.; Berto, P.; Berdeaux, G. Cost-minimisation study of dorzolamide versus brinzolamide in the treatment of ocular hypertension and primary open-angle glaucoma: in four European countries. Pharmacoeconomics. 2003, 21, 201–213. [Google Scholar] [CrossRef]
- Michaud, J.-E.; Friren, B. Comparison of topical brinzolamide 1% and dorzolamide 2% eye drops given twice daily in addition to timolol 0.5% in patients with primary open-angle glaucoma or ocular hypertension. Am. J. Ophthalmol. 2001, 132, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Abramson, D.H.; Coleman, D.J.; Forbes, M.; Franzen, L.A. Pilocarpine. Effect on the anterior chamber and lens thickness. Arch. Ophthalmol. 1972, 87, 615–620. [Google Scholar] [CrossRef]
- Schuman, J.S.; Horwitz, B.; Choplin, N.T.; David, R.; Albracht, D.; Chen, K. A 1-Year Study of Brimonidine Twice Daily in Glaucoma and Ocular Hypertension. Arch. Ophthalmol. 1997, 115, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Aihara, M.; Lu, F.; Kawata, H.; Iwata, A.; Odani-Kawabata, N. Twelve-month efficacy and safety of omidenepag isopropyl, a selective EP2 agonist, in open-angle glaucoma and ocular hypertension: the RENGE study. Jpn. J. Ophthalmol. 2021, 65, 810–819. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Araie, M. Phase 2 Randomized Clinical Study of a Rho Kinase Inhibitor, K-115, in Primary Open-Angle Glaucoma and Ocular Hypertension. Am. J. Ophthalmol. 2013, 156, 731–736. [Google Scholar] [CrossRef]
- Lopes, N.L.V.; Gracitelli, C.P.B.; Chalita, M.R.; De Faria, N.V.L. Ocular Surface Evaluation After the Substitution of Benzalkonium Chloride Preserved Prostaglandin Eye Drops by a Preservative-free Prostaglandin Analogue. Med hypothesis Discov. Innov. Ophthalmol. 2019, 8, 52–56. [Google Scholar] [PubMed]
- Nino, M.; Napolitano, M.; Scalvenzi, M. Allergic contact dermatitis due to the beta-blocker betaxolol in eyedrops, with cross-sensitivity to timolol. Contact. Dermatitis. 2010, 62, 319–320. [Google Scholar] [CrossRef]
- Cusano, F.; Luciano, S.; Capozzi, M.; Verrilli, D.A. Contact dermatitis from pilocarpine. Contact Dermat. 1993, 29, 99–99. [Google Scholar] [CrossRef]
- Sodhi, P.K.; Verma, L.; Ratan, J. Dermatological Side Effects of Brimonidine: A Report of Three Cases. J. Dermatol. 2003, 30, 697–700. [Google Scholar] [CrossRef]
- Napolitano, M.; Potestio, L.; Castagliola, C.; Fabbrocini, G.; Patruno, C. Allergic contact dermatitis probably due to brimonidine tartrate in eyedrops. Contact Dermat. 2021, 85, 382–384. [Google Scholar] [CrossRef]
- Mitsuyama, S.; Abe, F.; Higuchi, T. Allergic contact dermatitis due to dorzolamide eyedrops. Contact Dermat. 2021, 84, 58–59. [Google Scholar] [CrossRef]
- Navarro-Triviño, F.J.; Ruiz-Villaverde, R. Periocular allergic contact dermatitis caused by brinzolamide. Contact Dermat. 2020, 84, 274–276. [Google Scholar] [CrossRef]
- Sodhi, P.K.; Verma, L.; Ratan, S.K. Contact dermatitis from topical bimatoprost. Contact Dermat. 2004, 50, 50–50. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, T.H.; Kim, S.-C. Allergic Contact Dermatitis Caused by Topical Eye Drops Containing Latanoprost. Ann. Dermatol. 2014, 26, 269–270. [Google Scholar] [CrossRef]
- Corazza, M.; Virgili, A.; Maniovani, L.; Masieri, L.T. Allergic contact dermatitis from cross-reacting beta-blocking agents. Contact Dermat. 1993, 28, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Chun, J.S.; Yun, S.J.; Lee, J.B.; Kim, S.J.; Won, Y.H.; Lee, S.C. Toxic Epidermal Necrolysis Induced by the Topical Carbonic Anhydrase Inhibitors Brinzolamide and Dorzolamide. Ann. Dermatol. 2008, 20, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Sakata, R.; Shirato, S.; Miyata, K.; Aihara, M. Recovery from deepening of the upper eyelid sulcus after switching from bimatoprost to latanoprost. Jpn. J. Ophthalmol. 2013, 57, 179–184. [Google Scholar] [CrossRef]
- Choi, H.Y.; Lee, J.E.; Lee, J.W.; Park, H.J.; Lee, J.E.; Jung, H.E. In vitro study of antiadipogenic profile of latanoprost, travoprost, bimatoprost, and tafluprost in human orbital preadipocytes. J. Ocul. Pharmacol. Ther. 2012, 28, 146–152. [Google Scholar] [CrossRef]
- Woodward, D.F.; Krauss, A.H.-P.; Chen, J.; Liang, Y.; Li, C.; Protzman, C.E.; Bogardus, A.; Chen, R.; Kedzie, K.M.; Krauss, H.A.; et al. Pharmacological Characterization of a Novel Antiglaucoma Agent, Bimatoprost (AGN 192024). Experiment 2003, 305, 772–785. [Google Scholar] [CrossRef]
- Tanimura, H.; Minamoto, A.; Narai, A.; Hirayama, T.; Suzuki, M.; Mishima, H.K. Corneal Edema in Glaucoma Patients After the Addition of Brinzolamide 1% Ophthalmic Suspension. Jpn. J. Ophthalmol. 2005, 49, 332–333. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.C.; Chen, T. Brinzolamide induced reversible corneal decompensation. Br. J. Ophthalmol. 2005, 89, 389–390. [Google Scholar] [CrossRef]
- Adamsons, I. Irreversible corneal decompensation in patients treated with topical dorzolamide. Am. J. Ophthalmol. 1999, 128, 774–775. [Google Scholar] [CrossRef]
- Sugrue, M.F; Johns, B. Concentrations of dorzolamide in the pigmented rabbit eye after repeated dosing with TRUSOPT. Invest. Ophthalmol. Vis. Sci. 1999, 40, S171. [Google Scholar]
- Baratz, K.H.; Nau, C.B.; Winter, E.J.; McLaren, J.W.; O Hodge, D.; Herman, D.C.; Bourne, W.M. Effects of Glaucoma Medications on Corneal Endothelium, Keratocytes, and Subbasal Nerves Among Participants in the Ocular Hypertension Treatment Study. Cornea 2006, 25, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Beltz, J.; Zamir, E. ; Mbbs; Franzco; Franzco Brimonidine Induced Anterior Uveitis. Ocul. Immunol. Inflamm. 2014, 24, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Hopf, S.; Mercieca, K.; Pfeiffer, N.; Prokosch-Willing, V. Brimonidine-associated uveitis – a descriptive case series. BMC Ophthalmol. 2020, 20, 489. [Google Scholar] [CrossRef]
- Hu, J.; Vu, J.T.; Hong, B.; Gottlieb, C. Uveitis and cystoid macular oedema secondary to topical prostaglandin analogue use in ocular hypertension and open angle glaucoma. Br. J. Ophthalmol. 2020, 104, 1040–1044. [Google Scholar] [CrossRef]
- Abraham, S.V.; Teller, J.J. Influence of various miotics on cataract formation. Br. J. Ophthalmol. 1969, 53, 833–838. [Google Scholar] [CrossRef]
- Beasley, H.; Fraunfelder, F.T. Retinal Detachments and Topical Ocular Miotics. Ophthalmology 1979, 86, 95–98. [Google Scholar] [CrossRef]
- American Psychological Association. APA dictionary of psychology-Adjunctive therapy. Available from- https://dictionary.apa. Available online: https://dictionary.apa.org/adjunctive-therapy (accessed on 6 July 2023).
- Lichter, P.R.; Musch, D.C.; Gillespie, B.W.; Guire, K.E.; Janz, N.K.; Wren, P.A.; Mills, R.P.; CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001, 108, 1943–1953. [Google Scholar] [CrossRef] [PubMed]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K. 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713, discussion 829-830. [Google Scholar] [CrossRef]
- Serle, J.B.; Wang, R.-F.; Mittag, T.W.; Shen, F.; Podos, S.M. Effect of Pilocarpine 4% in Combination With Latanoprost 0.005% or 8-iso Prostaglandin E2 0.1% on Intraocular Pressure in Laser-induced Glaucomatous Monkey Eyes. Eur. J. Gastroenterol. Hepatol. 2001, 10, 215–219. [Google Scholar] [CrossRef]
- Crawford, K.; Kaufman, P.L. Pilocarpine Antagonizes Prostaglandin F2α-Induced Ocular Hypotension in Monkeys. Arch. Ophthalmol. 1987, 105, 1112–1116. [Google Scholar] [CrossRef]
- Kent, A.R.; Vroman, D.T.; Thomas, T.J.; Hebert, R.L.; E Crosson, C. Interaction of pilocarpine with latanoprost in patients with glaucoma and ocular hypertension. J. Glaucoma 1999, 8, 257–262. [Google Scholar] [CrossRef]
- Yamagishi-Kimura, R.; Honjo, M.; Komizo, T.; Ono, T.; Yagi, A.; Lee, J.; Miyata, K.; Fujimoto, T.; Inoue, T.; Tanihara, H.; et al. Interaction Between Pilocarpine and Ripasudil on Intraocular Pressure, Pupil Diameter, and the Aqueous-Outflow Pathway. Investig. Opthalmology Vis. Sci. 2018, 59, 1844–1854. [Google Scholar] [CrossRef]
- Liu, J.H.; Medeiros, F.A.; Slight, J.R.; Weinreb, R.N. Comparing Diurnal and Nocturnal Effects of Brinzolamide and Timolol on Intraocular Pressure in Patients Receiving Latanoprost Monotherapy. Ophthalmology 2009, 116, 449–454. [Google Scholar] [CrossRef] [PubMed]
- O’connor, D.J.; Martone, J.F.; Mead, A. Additive intraocular pressure lowering effect of various medications with latanoprost. Am. J. Ophthalmol. 2002, 133, 836–837. [Google Scholar] [CrossRef]
- Feldman, R.M.; Tanna, A.P.; Gross, R.L.; Chuang, A.Z.; Baker, L.; Reynolds, A.; Prager, T.C. Additivity 398 Study Group. Comparison of the Ocular Hypotensive Efficacy of Adjunctive Brimonidine 0.15% or Brinzolamide 1% in Combination with Travoprost 0.004%. Ophthalmology 2007, 114, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Martinez-De-La-Casa, J.M.; Castillo, A.; Garcia-Feijoo, J.; Mendez-Hernandez, C.; Fernandez-Vidal, A.; Garcia-Sanchez, J. Concomitant administration of travoprost and brinzolamide versus fixed latanoprost/timolol combined therapy: three-month comparison of efficacy and safety. Curr. Med Res. Opin. 2004, 20, 1333–1339. [Google Scholar] [CrossRef]
- Reis, R.; Queiroz, C.F.; Santos, L.C.; Avila, M.P.; Magacho, L. A randomized, investigator-masked, 4-week study comparing timolol maleate 0.5%, brinzolamide 1%, and brimonidine tartrate 0.2% as adjunctive therapies to travoprost 0.004% in adults with primary open-angle glaucoma or ocular hypertension. Clin. Ther. 2006, 28, 552–559. [Google Scholar] [CrossRef]
- Cheng, J.W.; Cheng, S.W.; Yu, D.Y.; Wei, R.L.; Lu, G.C. Meta-analysis of α2-adrenergic agonists versus carbonic anhydrase inhibitors as adjunctive therapy. Curr. Med. Res. Opin. 2012, 28, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Konstas, A.G.P.; Holló, G.; Haidich, A.-B.; Mikropoulos, D.G.; Giannopoulos, T.; Voudouragkaki, I.C.; Paschalinou, E.; Konidaris, V.; Samples, J.R. Comparison of 24-Hour Intraocular Pressure Reduction Obtained with Brinzolamide/Timolol or Brimonidine/Timolol Fixed-Combination Adjunctive to Travoprost Therapy. J. Ocul. Pharmacol. Ther. 2013, 29, 652–657. [Google Scholar] [CrossRef]
- Öztürk, F.; Ermiş, S.S.; Inan. .; Idaǧ, A.A.; Yaman, S.; Craven, E.R.; Walters, T.R.; Williams, R.; Chou, C.; Cheetham, J.K.; et al. Comparison of the Efficacy and Safety of Dorzolamide 2% When Added to Brimonidine 0.2% or Timolol Maleate 0.5% in Patients with Primary Open-Angle Glaucoma. J. Ocul. Pharmacol. Ther. 2005, 21, 68–74. [Google Scholar] [CrossRef]
- Fuwa, M.; Shimazaki, A.; Odani-Kawabata, N.; Kirihara, T.; Taniguchi, T.; Iwamura, R.; Yoneda, K.; Kato, M.; Morishima, K.; Shams, N.K. Additive Intraocular Pressure-Lowering Effects of a Novel Selective EP2 Receptor Agonist, Omidenepag Isopropyl, Combined with Existing Antiglaucoma Agents in Conscious Ocular Normotensive Monkeys. J. Ocul. Pharmacol. Ther. 2021, 37, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Tanna, A.P.; Rademaker, A.W.; Stewart, W.C.; Feldman, R.M. Meta-analysis of the efficacy and safety of alpha2-adrenergic agonists, beta-adrenergic antagonists, and topical carbonic anhydrase inhibitors with prostaglandin analogs. Arch. Ophthalmol. 2010, 128, 825–833. [Google Scholar] [PubMed]
Figure 1.
(a) The optic nerve head with healthy neuroretinal rim, area surrounding the inside dotted circle. There inside doted circle, marked with blue arrow is cup. (b) The optic nerve in glaucomatous eye. Note the loss of NRR and increase in cup size, marked with blue line.
Figure 1.
(a) The optic nerve head with healthy neuroretinal rim, area surrounding the inside dotted circle. There inside doted circle, marked with blue arrow is cup. (b) The optic nerve in glaucomatous eye. Note the loss of NRR and increase in cup size, marked with blue line.
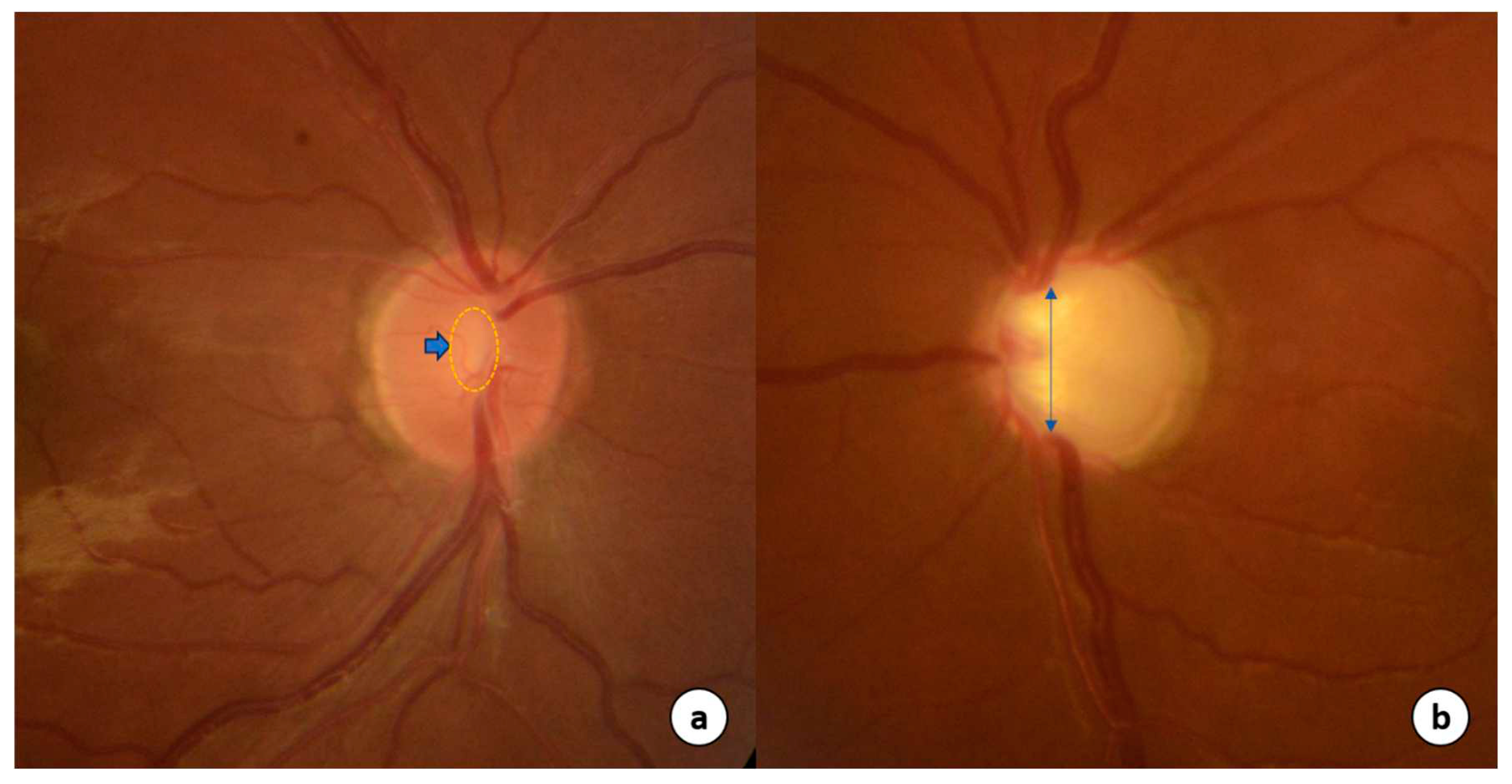
Figure 2.
The graphical representation of time-line of introduction of IOP-lowering drugs.

Figure 3.
Schematic diagram of structures of the anterior chamber of the eye to illustrate site of action and receptors of the IOP-lowering drugs.
Figure 3.
Schematic diagram of structures of the anterior chamber of the eye to illustrate site of action and receptors of the IOP-lowering drugs.


Table 1.
Classification of topical IOP-lowering drugs.
| Aqueous Suppressants Drugs |
|---|
| Alpha-adrenergic agonist |
| Apraclonidine 0.5% |
| Brimodine 0.1%, 0.15%, 0.2% |
| Beta-adrenergic antagonist |
| Betaxolol 0.5% |
| Timolol 0.5% |
| Carbonic anhydrase inhibitors (CAIs) |
| Brinzolamide 1% |
| Dorzolamide hydrochloride 2% |
| Aqueous Outflow Drugs |
| Trabecular meshwork outflow pathway |
| Cholinergic |
| Carbachol 0.75%,1.5%,3% |
| Demecarium 0.125%, 0.25% |
| Echothiophate 0.125% |
| Pilocarpine 1%,2% ,4% |
| Rho-Kinase inhibitors |
| Netarsudil 0.02% |
| Ripasudil 0.4% |
| Nitric acid donors |
| Latanoprostene bunod |
| Unconventional outflow pathway |
| Prostaglandin analogues |
| Bimatoprost 0.01%, 0.03% |
| Latanoprost 0.005% |
| Tafluprost 0.0015% |
| Travoprost 0.04% |
| Unoprostone Isopropyl 0.15% |
| Omidenepag Isopropyl 0.002% |
Table 2.
The IOP lowering mechanisms of topical drugs.
| Drugs | IOP related effects | IOP independent effects | ||||
|---|---|---|---|---|---|---|
| Aqueous secretion | Trabecular meshwork outflow | Uveoscleral pathway outflow | Episcleral venous pressure | Neuroprotection | Ocular blood flow | |
| Betaxolol | Decrease | No effect | No effect | |||
| Timolol | Decrease | No effect | No effect | No effect | Decrease [22] | |
| Apraclonidine | Decrease | Decrease [27] | Decrease [28] | |||
| Brimodine | Decrease | No effect | Increase [14] | Decrease [26] | + [29, 123, 124] | No effect [30,31] |
| Brinzolamide | Decrease | No effect | No effect | No effect | ? / No effect [31,121] | |
| Dorzolamide | Decrease | No effect | Increase [9, 110]/No effect [30] | |||
| Bimatoprost | Increase | Increase# | Increase | Increase/ Decrease [109] | ||
| Latanoprost | Increase | Increase# | Increase | Increase | Increase [11,13] | |
| Tafluprost | Increase# | Increase | Increase [117] | |||
| Travoprost | Increase | Increase# | Increase | Increase [13] | ||
| Unoprostone | Increase# | Increase | No effect | |||
| Omidenepag isopropyl | No effect | Increase | ||||
| Pilocarpine | No effect [46] | Increase | Decreases [206] | No effect | Increase [9,10] | |
| Latanoprostene bunod | Increase | Increase | Ongoing Trial | Increase [122] | ||
| Netarsudil | Decrease | Increase | No effect | Decrease [106, 107] | + [129, 130] | |
| Ripasudil | Increase | Decrease [108] | + [129, 130] | |||
Table 3.
The IOP related characteristics of topical drops [51-53, 56,65,83,110,203].
| Drug | Time | IOP reduction (%) | Washout period | |||
|---|---|---|---|---|---|---|
| Onset | Peak effect | Duration | Peak | Trough | ||
| Betaxolol | 30 minutes | 2 hours | 12 hours | -23 | -20 | 1 week |
| Timolol | 30 minutes | 2 hours | 12-24 hours | -27 | -26 | 4 weeks |
| Brinzolamide | 1 hour | 2-3 hours | 8-12 hours | -17 | -17 | 1 week |
| Dorzolamide | 1 hour | 3 hours | 8 hours | -22 | -17 | 1 week |
| Apraclonidine | 1 hour | 45-90 minutes | 6-8 hours | -27 | -20 | 1-2 weeks |
| Brimonidine | 1 hour | 2-3 hours | 8-10 hours | -19 | -14 | 1-2 weeks |
| Bimatoprost | 4 hours | 8-12 hours | 24 hours | -33 | -28 | 4-6 weeks |
| Latanoprost | 3-4 hours | 8-12 hours | 24 hours | -31 | -28 | 4-6 weeks |
| Tafluprost | 2-4 hours | 12 hours | 24 hours | -31 | -27 | 4-6 weeks |
| Travoprost | 2 hours | 12 hours | >24 hours | -31 | -29 | 4-6 weeks |
| Unoprostone | 30-90 minutes | 2-3 hours | 2-5 hours | -25 | -10 | 2-4 weeks |
| Omidenepag isopropyl | 2-4 hours | 12 hours | >24 hours | -25 | -20 | 1 week |
| Pilocarpine | 60 minutes | 75 minutes | 4-6 hours | -25 | -15 | 48 hours |
| Netarsudil | 1-2 hours | - | >24 hours | -25 | -18 | - |
| Ripasudil | 1-2 hours | - | 12 hours | - | - | |
| Latanoprostene bunod | 1-3 hours | 11-13 hours | 24 hours | -32 | -30 | 4-6 weeks |
| Acetazolamide | 30 minutes | 2 hours | 6-8 hours | - | - | 3 days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



