Submitted:
24 July 2023
Posted:
26 July 2023
Read the latest preprint version here
Abstract
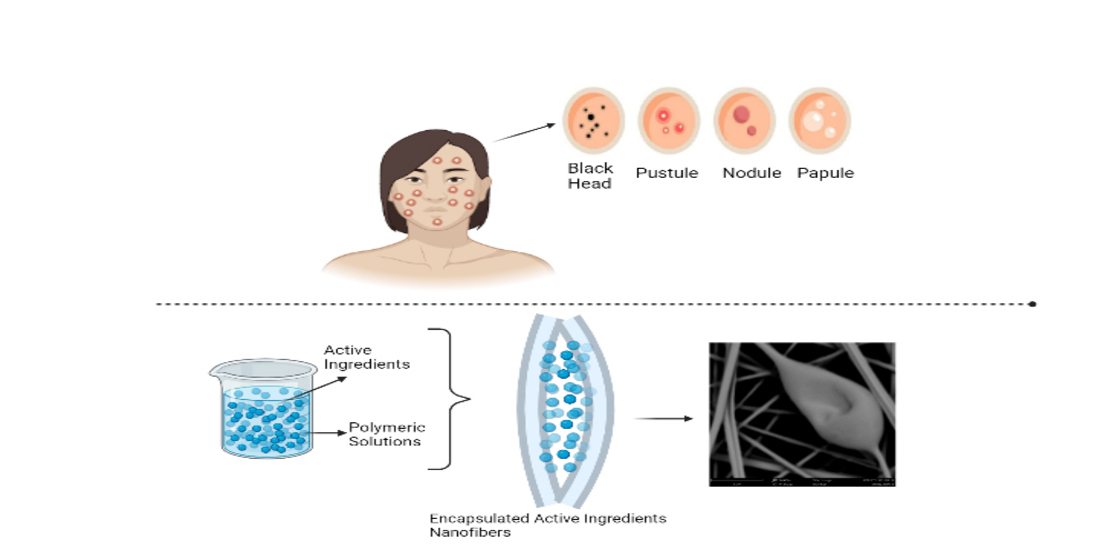
Encapsulated nanofibers have emerged as a promising approach for the treatment of acne, owing to their ability to provide controlled release, targeted delivery, increased efficacy, and improved stability. Electrospinning is a well-established method for producing encapsulated nanofibers and has been shown to be effective for encapsulating various active ingredients. However, there are still several challenges that need to be addressed in the development of encapsulated nanofibers for acne treatment. One major challenge is the need for comprehensive in vitro and in vivo studies to evaluate the safety and efficacy of these treatments. The cost and scalability of production also need to be considered to make these treatments accessible and affordable for patients. In addition, the long-term stability of encapsulated active ingredients is another challenge in the development of encapsulated nanofibers for acne treatment. Regulatory frameworks need to be developed to ensure the safety and efficacy of these treatments. Future research may focus on developing multifunctional nanofibers that combine active ingredients with other properties, such as antimicrobial, anti-inflammatory, and wound-healing properties, to provide a comprehensive approach to acne treatment. Moreover, the development of nanofiber-based skincare products may have a significant impact on the cosmetic industry. Overall, while there are still challenges to overcome, the potential benefits of encapsulated nanofibers for acne treatment make them an exciting and promising area of research for the future. In particular, the integration of smart drug delivery systems and responsive materials may enable the development of more personalized and effective treatments for acne. The development of new materials and encapsulation techniques, as well as the exploration of combination therapies that target multiple aspects of acne pathogenesis, are also future perspectives for encapsulated nanofibers in acne treatment.
Keywords:
Encapsulated nanofibers
; Acne treatment
; Skincare products
; Cosmetic industry
; Functional nanofibers
1. Introduction
Acne is a common skin condition that affects a significant proportion of the population [34]. According to the American Academy of Dermatology, acne is the most common skin condition in the United States, affecting approximately 50 million people annually [35]. Acne can occur at any age, but it is most prevalent during adolescence, affecting up to 85% of teenagers [36]. However, it can also affect adults, with approximately 15% of women and 5% of men experiencing acne beyond teenage years. Globally, acne affects an estimated 9.4% of the population [37]. Acne vulgaris, commonly known as acne, is a long-lasting inflammatory condition that causes blemishes on the skin by affecting the pilosebaceous unit (PSU) [1]. Acne occurs when hair follicles in the skin become clogged with oil and dead skin cells [2]. Excess oil production and dead skin cells can combine and form a plug in the hair follicle, trapping bacteria and resulting in inflammation [3]. This can lead to the formation of various types of lesions, including blackheads, whiteheads, pimples, nodules, and cysts [4,5]. Hormonal changes, stress, certain medications, and genetics can contribute to the development of acne [6]. The development of these blemishes is associated with several factors, including excessive production of sebum [7], shedding of skin cells within hair follicles [8], immune responses [9], and bacterial growth [10]. Additionally, dietary habits that involve a high intake of sugar, protein, or fat, as well as certain lifestyle choices, can contribute to the development of acne [1,2,4,5]. The pilosebaceous unit (PSU) can be affected by two types of skin lesions: inflammatory [11] and non-inflammatory [12]. Inflammatory lesions, such as papules, pustules, nodules, and cysts, can develop in PSU, as well as non-inflammatory lesions like comedones [13]. These skin issues commonly appear in areas such as the face, neck, and back [14,15].
The dermis and epidermis lies in the basement membrane zone of the skin, which houses versatile basal stem cells that can transform into either sebaceous cells or keratinocytes [16]. These cells are responsible for hair growth [17] and the production of sebum [18]. The growth and proliferation of these cells are significantly controlled by hormones, specifically androgens [4]. Hormonal imbalances can lead to an abnormal increase in keratinization, which can trigger various pathogenic processes affecting the pilosebaceous unit (PSU) [19]. Acne-related skin lesions can develop due to the activation of immune reactions and inflammation [4,20,21]. Activation of immune reactions and inflammation can directly contribute to the development of acne-related skin lesions [22,23]. Comedonal acne is a type of acne that frequently occurs on the face and is characterized by non-inflammatory lesions [24]. Closed comedones (whiteheads) [25] and open comedones (blackheads) [26] are two possible presentations of skin lesions [27]. Closed comedones, also known as whiteheads, occur when hair follicles become clogged with oil and dead skin cells [25]. The clog causes a small bump to form on the surface of the skin, often appearing white or flesh-colored the closure of the follicle [28]. On the other hand, open comedones, blackheads, are similar but have different appearances. In these cases, the pores remain open and become filled with dirt and bacteria [29]. Severe pustulocystic acne presents a formidable challenge [30]. Nodules and cysts that manifest not only in the facial area but also in multiple other body regions greatly diminish the quality of life [31]. Their exceptional durability clearly distinguishes them from regular acne [32]. However, it is essential to remain resolute and not succumb to despair. A wide array of treatment exist, spanning from topical medications to oral antibiotics, and in particularly severe instances, isotretinoin may be employed. Thus, with an appropriate treatment strategy and a modicum of patience, it is entirely feasible to overcome this vexing dermatological condition [1,22,23,33].
2. Pathogenesis of Acne
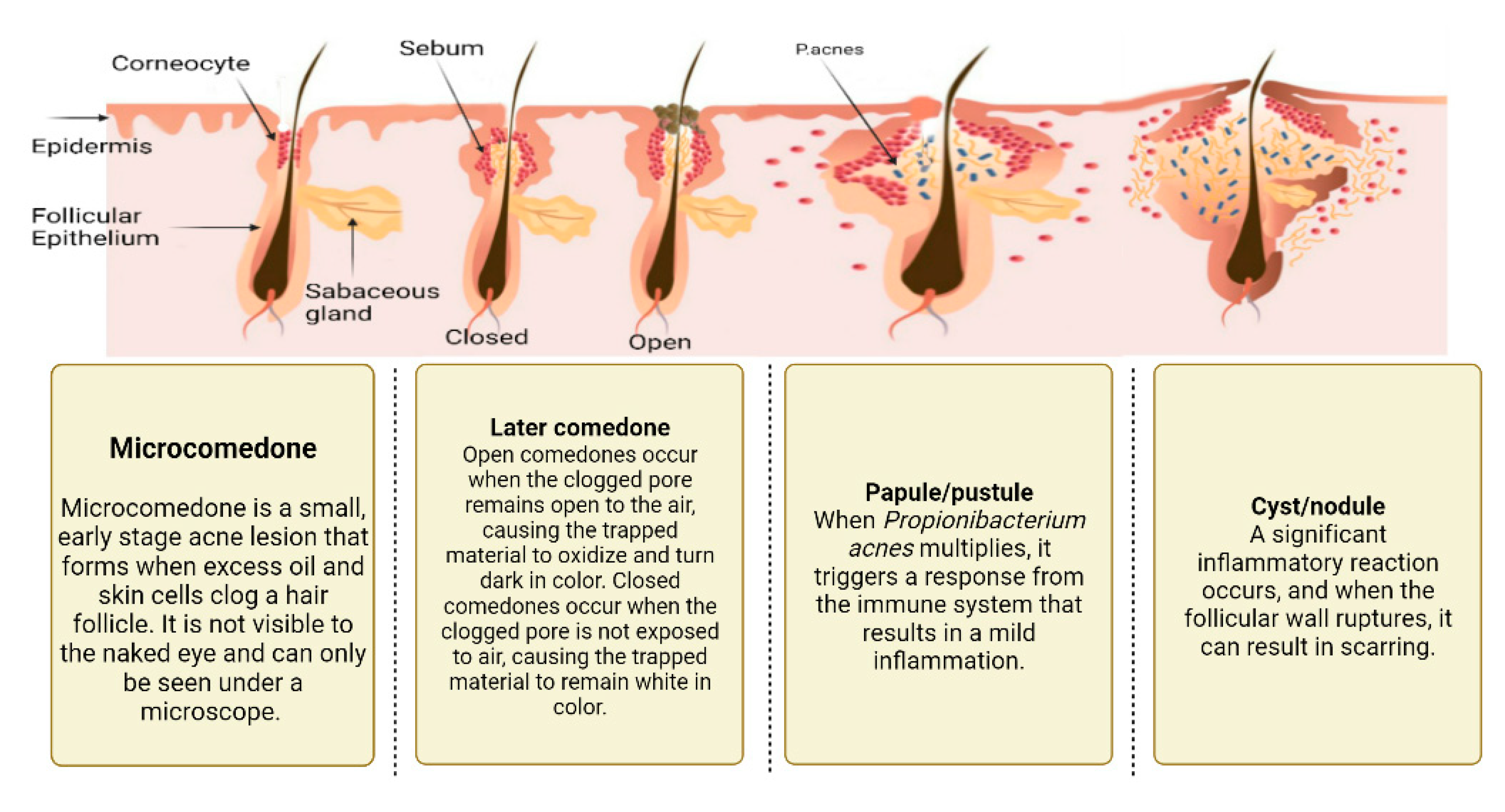
According to Olutunmbi et al. [34] the most common locations for acne lesions are the face, chest, upper back, and upper arms. These areas have a high density of sebaceous glands, which are responsible for producing oil (sebum) that can contribute to the development of acne. As a result, these regions are more prone to developing acne lesions than other areas of the body [35]. Primary pathological factors that play a role in the development of acne [36]: increased sebum production, irregular desquamation (shedding) of follicular cells, proliferation of Propionibacterium acnes bacteria, and inflammation of affected areas [37]. These factors interact with each another and contribute to the development of various types of acne lesions. For instance, when sebum production increases, comedones may appear and simultaneously, bacterial proliferation and inflammation can contribute to the development of more serious types of acne lesions such as papules, pustules, nodules, and cysts [37]. Figure 2 depicts the different stages of acne development, starting with the formation of a microcomedone, small plug of sebum and dead skin cells that form in the hair follicle.
A small bump with a white or yellowish head, also known as a whitehead, is the result of the progression of the microcomedone into a closed comedone [38]. The early stage of a closed comedone, known as a microcomedone, can transform into a white or yellow-headed small bump, often called a whitehead [39]. The formation of an open comedone or blackhead can occur, resulting in the appearance of a dark bump on the skin [40]. In addition, the formation of a pustule may occur, characterized by a raised bump filled with pus and featuring a center that is either white or yellow, surrounded by an inflamed and red base [41]. In cases of increased severity, the skin can develop nodules and cysts that are more prominent and penetrate deeper, often leading to scarring [42]. To devise effective treatments, it is essential to have a comprehensive understanding of the distinct phases of acne development.
Figure 1.
Stages of acne.
2.1. Excess sebum production
Gollnick [43] suggested that androgen hormones, particularly testosterone, could stimulate an increase in sebum production and secretion. This increase in sebum production is directly linked to the severity and frequency of the acne lesions. Therefore, it is important to consider when the diagnosis and treatment of with Acne vulgaris. By addressing the hormonal imbalances that may contribute to increased sebum production, healthcare providers may be able to help patients effectively manage their acne symptoms [35].
2.2. Epidermal hyper-proliferation and formation of comedones
Under normal circumstances, keratinocytes lining the follicles in the skin are shed as single cells that are then excreted [44]. However, in patients with acne, hyper-proliferation of these keratinocytes leads to an abnormal build-up of corneocytes that are not shed as expected. This accumulation of abnormal desquamated cells, along with other lipids and filaments, occurs in the sebaceous follicle, a process known as comedogenics [45]. The build-up of these materials can block the follicle and contribute to the development of comedones, which are a type of non-inflammatory acne lesion [37]. Comedones are a type of skin blemish that can be open or closed. Open comedones, commonly known as blackheads, appear black on the skin surface because of due to their dilated state and contain a mixture of sebum and dead skin cells. Closed comedones, or whiteheads, are white or skin-colored bumps that form underneath the skin and have no visible openings. If sebum build-up continues in closed comedones, it can grow and eventually burst into the surrounding skin tissue [43].
2.3. Propionibacterium Acnes Infiltration
Microorganisms that inhabit healthy sebaceous follicles are comparable to those found in comedones. They consist of three distinct bacterial groups that coexist in same environment, (1) coagulase-negative staphylococci such as Staphylococcus epidermidis [46]; (2) anaerobic diphtheroids [47], including Propionibacterium acnes and Propionibacterium granulosum [48]; and (3) yeasts that thrive in oily environments, such as Pityrosporum species [49]. P. acnes and S. epidermidis are two prominent bacterial groups commonly found in the pilosebaceous units of human skin [50]. P. acnes is known for its role in the pathogenesis of acne vulgaris, a prevalent inflammatory skin condition affecting millions worldwide [51]. This bacterium thrives in sebaceous follicles and contributes to the development of comedones, inflammatory lesions, and potentially severe cystic acne [52]. Lipophilic yeasts are also present but do not seem to play a significant role in disease conditions [53]. P. acnes produces a lipase enzyme that helps metabolize the triglycerides of sebum and may contribute to the formation of comedones and subsequent inflammation [54]. P. acnes is the most probable organism responsible causing acne vulgaris and is targeted by oral and topical antibiotic treatments [35].
2.4. Inflammation Process
The immune system detects P. acnes in the skin, triggering the release of inflammatory chemostatic factors such as lymphocytes, neutrophils, and macrophages [55]. P. acnes has a highly inflammatory effect that can cause damage to follicles, leading to leakage of bacteria, fatty acids, and lipids into the dermis [56]. This results in the development of inflammatory lesions such as pustules, nodules, cysts, and papules, which are larger and filled with pus than non-inflammatory lesions [57]. Neutrophils contribute to acne inflammation by generating reactive oxygen species (ROS), which damage the follicular epithelium and cause the expulsion of follicular content into the dermis, leading to various inflammatory processes [57].
3. Treatment of Acne
The main goal of acne treatment is to control and treat existing acne lesions, prevent permanent scarring, limit the duration of the disorder, and minimize morbidity [20]. Patients should be informed about preventing new acne lesions while allowing existing ones to heal, and it may take 3-6 weeks to observe improvement [58]. The therapeutic approach towards acne, which might encompass mild, moderate, or severe presentations, including comedonal acne, papulopustular acne, or the more extreme nodulocystic variant, is contingent upon the manifested condition [59,60]. Acne grading scales typically consider several factors when assessing the severity of acne [61]. These include the presence of scars, the type of scars (such as ice-pick [62], rolling, boxcar, hypertrophic, or post-inflammatory hyperpigmentation) [28], the concentration, size, color depth, distribution, and number of lesions; and the affected area's width, location, and number of lesions [40,56,58,63,64]. Numerous grading scales are available for evaluating acne severity, and are used by both clinicians and patients. These scales include the Quantitative Global Scarring Grading Systems (QGS) [65], Acne Scar Rating Scale (ASRS) [64], Self-assessment of Clinical Acne-Related Scars (SCARS) [66], Facial Acne Scar Quality of Life (FASQoL) [67], Echelle d’Evaluation Clinique des Cicatrices d’acne (ECCA) [68], Global Scale for Acne Scar Severity (SCAR-S) [69], Leeds grading technique [70], Revised Leeds grading technique [71], Plewig and Kligman numerical grading of comedonal acne [72], Global Evaluation Acne scale [73], US FDA’s Investigator’s Global Assessment [74] for acne vulgaris, and others based on imaging assessments [75]. Clinicians commonly utilize various clinical scales to assess the severity of patient lesions and effectiveness of treatments [71]. Among these scales are the Qualitative and Quantitative Global Scarring Grading Systems (QGS) [76], Investigator's Global Assessment (IGA) [77], and Global Evaluation Acne (GEA) [13,58]. Goodman and Baron developed Quantitative and Qualitative Global Scarring Grading Systems (QGS) with the aim of making the evaluation of acne severity easier and determining the appropriate treatment for each grade [78]. The Qualitative Global Scarring grading system is a more patient-friendly and practical approach for assessing the burden of acne [79]. It consists of four grades, and as the condition becomes more severe, various post-acne scars with varying grades become visible [79]. Table 1 presents the Qualitative Global Scarring grading system for acne. The grading system categorizes acne scarring into four levels based on severity, from Grade 0 (no scarring) to Grade 3 (severe scarring). The table describes the characteristics of each grade, including the presence of ice picks, rolling, or boxcar scars, and the overall appearance of the skin. The grading system can help clinicians assess the severity of acne scarring and determine the appropriate treatment options [79].
The Global Evaluation of Acne (GEA) and the US FDA Investigator’s Global Assessment are other commonly used grading scales. GEA, developed by Thiboutot et al., is a system that grades acne scars and can be used for both clinical and research purposes. The GEA consists of 5 grades which are based on the type of lesion and extent of the affected area [80].In Table 2 shows The scale categorizes acne into 5 grades which are based on the number and type of lesions present, as well as the distribution and severity of inflammation. This scale can help clinicians objectively assess the severity of acne and guide treatment decisions.
Mild acne can often be managed with over-the-counter topical treatments that contain ingredients such as benzoyl peroxide [81], salicylic acid [82], or retinoids [83]. Moderate to severe acne may require prescription topical or oral medications, such as antibiotics, hormonal therapies, or isotretinoin [58]. It is of note that certain acne pharmacological interventions, isotretinoin being a prime example, may elicit severe side effects, necessitating meticulous oversight by a healthcare professional. Complementing pharmacotherapy, lifestyle modifications encompassing balanced nutrition, consistent physical activity, and stress management techniques could potentially ameliorate acne symptoms [84]. Patients are advised to engage in consultation with a healthcare professional to tailor an optimal treatment plan specific to their unique needs [20].Table 3 shows overview of common acne treatment methods. This table compares the characteristics and effectiveness of topical and systemic acne treatment methods, including their mode of action, potential side effects, and considerations for use.
4. Nanotechnology & acne treatment
Nanotechnology has emerged as a promising field in the treatment of acne due to its ability to target specific skin layers and deliver therapeutic agents more effectively [86]. The use of nanotechnology-based approaches can improve the efficacy, bioavailability, and stability of acne medications, as well as minimize their side effects [87]. Among the myriad of nanotechnology-based methodologies examined for acne treatment, the utilization of nano-sized drug delivery systems stands as one of the most extensively researched [88]. These delivery systems can encapsulate acne medications, such as retinoids [89] and benzoyl peroxide [90], in nano-sized particles to improve their solubility, bioavailability, and stability [91]. The deployment of nanoparticles can potentially enhance the infiltration of these therapeutic agents into the skin strata, the very site of acne manifestation [92]. Research indicates that nano-sized particles possess the ability to permeate deeper into the skin compared to traditional delivery systems, thereby facilitating a more efficient conveyance of therapeutic agents to the targeted location [93]. An additional prospective strategy employing nanotechnology entails the use of nanomaterials in the therapeutic management of acne [1]. Saba et al., studied tretinoin-loaded nanofibers were scrutinized for their potential in topical skin delivery for the treatment of acne lesions. Their findings demonstrated that the electrospun nanofibers facilitated a sustained release of tretinoin. Interestingly, formulation stability at room temperature was surpassed by that in fast track (FT) conditions. However, disc diffusion tests did not reveal any synergistic enhancement in the antibacterial activity of erythromycin when co-administered with tretinoin [94]. Reneta et al. investigated a novel dissolvable nanofiber patch embedded with essential oils for treating acne vulgaris, demonstrating promising antibacterial activity against Cutibacterium acnes and Staphylococcus epidermidis, minimal cytotoxic effects on the HaCaT cell line, and potential for targeted antimicrobial application [95]. Rahnama et al. developed a chitosan-based nanofiber incorporated with melittin, a principal toxic component of bee venom known for its anti-inflammatory and antibacterial properties, aimed at topically treating acne vulgaris. Their findings indicated successful nanofiber formulation, effective Mel encapsulation, and significant inhibition of Propionibacterium acnes growth, suggesting its potential as a suitable topical drug delivery system for treating acne vulgaris [96]. Moreover, nanomaterials can also reduce inflammation and sebum production, which are key factors in the development of acne lesions [97]. The application of nanomaterials for acne treatment remains in its nascent phase, necessitating further research to robustly evaluate their therapeutic efficacy and safety profiles [98]. Beyond drug delivery systems and nanomaterials, nanotechnology-based methodologies can also be leveraged for purposes of skin cleansing and exfoliation [99]. Nanoparticles, including silica and titanium dioxide, can be integrated into acne cleansers and exfoliants to enhance their efficacy [97]. These nanoparticles can help remove excess oil and dead skin cells from the skin surface, which can contribute to the development of acne lesions [100]. Additionally, the inclusion of nanoparticles in skincare formulations can refine their texture and appearance, presenting an ancillary advantage particularly for acne-prone skin [101]. Nanotechnology-oriented strategies demonstrate significant potential in the management of acne. Utilizing nano-sized drug delivery systems, nanomaterials, and nanoparticles for skin cleansing and exfoliation could amplify the effectiveness and safety of acne therapeutics and skincare commodities [102]. Nonetheless, comprehensive research is required to thoroughly elucidate both the potential advantages and risks associated with these strategies in the context of acne treatment.
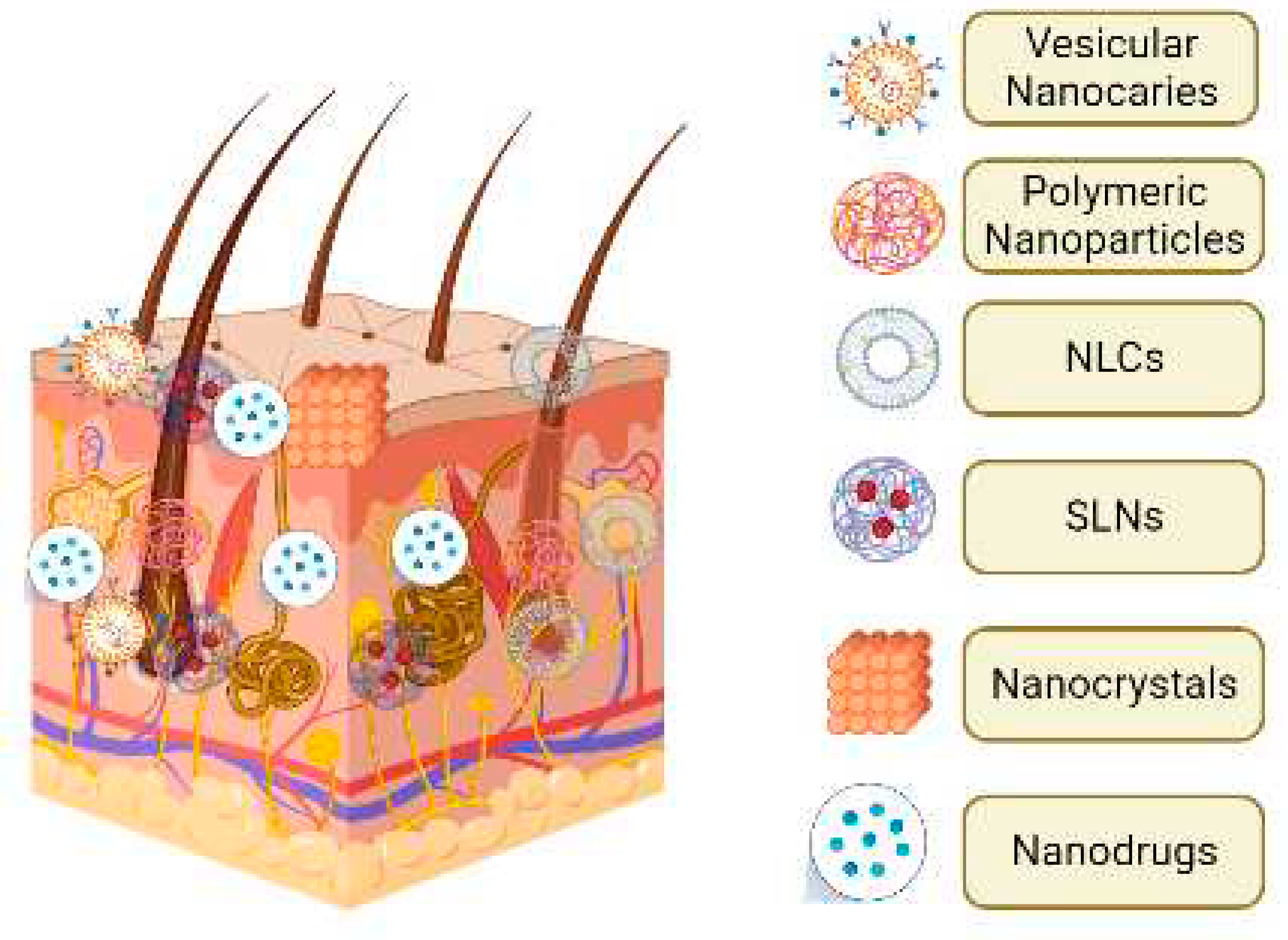
The Figure 2 illustrates the potential mechanisms by which nanoparticles can enhance the penetration of drugs into the skin and improve targeted drug delivery to skin organelles. The image shows nanoparticles of different sizes and shapes interacting with the skin barrier and penetrating through it. The nanoparticles can also be designed to specifically target certain skin cells or organelles, such as hair follicles, sebaceous glands, or epidermal cells [103]. The use of nanoparticles in skin drug delivery holds great promise for the treatment of a range of skin conditions, including acne.
Figure 2.
Schematic view of the mechanisms of nanoparticles in skin permeation and targeted drug delivery.
Figure 2.
Schematic view of the mechanisms of nanoparticles in skin permeation and targeted drug delivery.
Nano capsulation is a promising technology that has been widely studied in the pharmaceutical field for the targeted delivery of drugs [104]. In recent years, it has also been investigated for its potential in treating acne. Nano capsules are submicron-sized particles that can encapsulate active ingredients and protect them from degradation and premature release, allowing for controlled and targeted delivery to the affected area [104]. Smith et al. studied on the efficacy and safety of a topical gel that contains nano capsules of salicylic acid and resveratrol in treating mild to moderate acne. The study involved 20 patients with acne vulgaris who used the nano capsule-based gel for 12 weeks. The results of the study showed a significant reduction in the number of acne lesions and severity of acne as assessed by the Investigator's Global Assessment scale. The gel was also well-tolerated with only minimal side effects reported such as mild erythema and dryness. This study suggests that the use of nano capsules may be a promising approach for acne management [105]. Boskabadi et al. investigated the use of nano capsules for the delivery of retinoic acid, a commonly used acne treatment. The study showed that the use of nano capsules improved the stability and efficacy of retinoic acid, allowing for a lower concentration to be used, resulting in a reduction of adverse effects while maintaining therapeutic efficacy [106]. In conclusion, nano-capsules manifest significant promise within the realm of acne treatment. Their inherent ability to encapsulate active constituents, safeguard them from degradation, and facilitate controlled, targeted delivery to the affected regions, positions them as an appealing alternative for the formulation of novel and enhanced acne therapies [107].
This technology is not confined to nano-capsules. A plethora of nanotechnological carriers have been engineered for acne treatment. This includes but is not limited to, liposomes, niosomes, solid lipid nanoparticles, nanostructured lipid carriers, polymeric nanoparticles, and dendrimers [108]. Liposomes are spherical vesicles composed of a phospholipid bilayer that can encapsulate both hydrophilic and hydrophobic drugs [109]. Several studies have demonstrated the potential of liposomes in delivering anti-acne agents such as benzoyl peroxide [110], tretinoin [111], and clindamycin to the skin [112] with improved efficacy and reduced adverse effects [113,114]. Eroglu et al. developed a novel liposomal gel formulation containing tetracycline HCl and tretinoin, demonstrating sustained release, stability, non-toxicity, and antibacterial efficacy, offering a promising combination therapy for acne vulgaris treatment [115]. Stalko et al. developed liposomes loaded with clindamycin hydrochloride using different lipid compositions, and in vitro dissolution studies indicated sustained release of the drug from hostaphate liposomes compared to lecithin liposomes. Clinical treatment of Acne vulgaris with a liposomal drug lotion exhibited superior efficacy compared to non-liposomal lotion forms, resulting in a significant decrease in the total number of lesions, particularly in the case of pustules where clinical improvement reached 77% of the initial number, supporting the potential of liposomal dosage forms for enhanced topical therapy [116].
Niosomes are similar to liposomes but are composed of non-ionic surfactants [117]. Niosomes have been investigated as carriers for anti-acne agents, including salicylic acid and benzoyl peroxide, and have shown promising results in vitro and in vivo [118]. Solid lipid nanoparticles (SLNs) are another type of nanocarrier that has been explored for the treatment of acne [119]. SLNs are composed of solid lipids and can improve the skin penetration and stability of anti-acne agents [120]. Several studies have reported the successful encapsulation of anti-acne agents such as isotretinoin, tretinoin, and azelaic acid in SLNs [121,122]. Nanostructured lipid carriers (NLCs) are similar to SLNs but contain a mixture of solid and liquid lipids [123]. Jafari et al. investigated the use of niosomal nanocarriers loaded with doxycycline hyclate for treating acne. The study aimed to overcome the limitations of oral administration and traditional topical treatments, while improving therapeutic efficacy. The optimal niosomal formulation showed desirable characteristics including sustained drug release, improved cell viability, enhanced antibacterial activity, and increased drug deposition. These findings suggest that doxycycline hyclate-loaded nano-niosomes have potential for effective acne treatment [124]. Gupta et al. evaluated a niosomal gel formulation encapsulating tretinoin and benzoyl peroxide for acne treatment. The niosomal gel showed high entrapment efficiency, controlled drug release, and superior efficacy compared to an antiacne cream, requiring a lower dose of benzoyl peroxide to achieve the same therapeutic effect at targeted sites [81].NLCs have been investigated for the delivery of anti-acne agents such as benzoyl peroxide and adapalene and have shown improved efficacy and reduced irritation compared to conventional formulations [125].
Polymeric nanoparticles are composed of biodegradable polymers and can encapsulate both hydrophilic and hydrophobic drugs [122]. Several studies have investigated the use of polymeric nanoparticles for the delivery of anti-acne agents, including tretinoin, clindamycin, and salicylic acid [126]. Dendrimers are highly branched, nanoscale polymers that can encapsulate drugs and improve their solubility and bioavailability [127].
5.1. Lipid nanoparticles (LNs)
Lipid nanoparticles (LNPs) have been explored as a potential carrier system for acne treatment due to their biocompatibility, biodegradability, and ability to improve the stability and solubility of active ingredients [128]. Lipid nanoparticles (LNPs) are designed to encapsulate drugs or active compounds for targeted delivery to the affected area [129]. The encapsulation mechanism involves the formation of a lipid bilayer that surrounds the drug, protecting it from degradation and allowing for controlled release [130]. LNPs have been used in acne treatment to improve the effectiveness of topical agents and reduce their side effects [131].Lipid-based delivery systems are a significant type of nanoscale particles [132]. These systems have biocompatible properties, and their lipophilicity helps them penetrate biologic barriers, such as cell membranes [133]. Additionally, these systems are easy to manufacture, cost-effective, and can be produced on a large scale, making them a popular choice for various applications [134]. Pawar et al. developed solid lipid nanoparticles (SLNs) loaded with adapalene (AD) for the treatment of acne. The AD-SLNs exhibited uniform size (238.9 ± 3 nm), high encapsulation efficiency (>75% EE), and colloidal stability. The SLNs were further dispersed in a gel containing minocycline (MN) for topical application. The gel formulation demonstrated prolonged release of both drugs, enhanced permeation through goat's skin, and equivalent antibacterial properties to a marketed formulation. This novel drug delivery system holds promise as an alternative therapy for acne treatment [135]. Furthermore, LNPs have been shown to be effective in encapsulating and delivering antimicrobial agents, such as tea tree oil and thyme oil, for the treatment of acne [136]. Pokharkar et al. conducted a study to develop a stable formulation of solid lipid nanoparticles (SLN) loaded with benzoyl peroxide (BPO) for improved acne treatment. This approach allowed the researchers to achieve their desired goals efficiently and with minimal experimentation, offering a promising strategy to mitigate the well-known side effects associated with BPO treatment [137].
The use of lipid nanoparticles (LNPs) in acne treatment holds great promise as it offers several advantages for drug delivery. LNPs can enhance the solubility and stability of active ingredients, allowing for improved penetration into the skin and targeting of the affected areas. This targeted delivery helps to reduce systemic side effects and minimize the potential for irritation or erythema commonly associated with acne medications.
5.1.1. Solid lipid nanoparticles (SLNs)
Solid lipid nanoparticles (SLNs) have emerged as a promising carrier system for the treatment of acne due to their ability to enhance drug delivery, stability, and controlled release [138]. SLNs are composed of biocompatible and biodegradable solid lipids that form a colloidal dispersion in an aqueous medium [139]. These nanoparticles offer advantages over conventional acne treatment methods, such as improved skin permeation, reduced side effects, and prolonged drug release [140].Bo et al. Bo et al. formulated tea tree oil nanoliposomes (TTONL) and demonstrated their stability, slow-release properties, and dose-dependent inhibition of Escherichia coli (E. coli) strains. TTONL effectively reduced clinical symptoms and intestinal lesions in E. coli-challenged chickens, indicating their potential for preventing chicken colibacillosis [141]. SLNs have been investigated as a promising approach for delivering natural compounds with anti-acne activity, such as tea tree oil (TTO) [142]. TTO has demonstrated antimicrobial and anti-inflammatory activity, making it a potential candidate for acne treatment [143]. Doe et al. studied investigated the potential of solid lipid nanoparticles (SLNs) as a carrier system for the topical delivery of Tea Tree Oil (TTO) in the treatment of acne. The study showed that the use of SLNs significantly improved the skin penetration of TTO, leading to enhanced anti-acne activity. Doe et al. concluded that SLNs could be a promising carrier system for the effective delivery of TTO in acne treatment, offering a potential alternative to traditional topical formulations [144]. Table 4 shows advantages and disadvantages of Solid Lipid Nanoparticles (SLNs). n conclusion, solid lipid nanoparticles (SLNs) offer a promising carrier system for acne treatment, as they enhance drug delivery, provide stability, and enable controlled release. Further research should focus on investigating the potential of SLNs for delivering both conventional and natural anti-acne agents, advancing the field of acne therapeutics.
5.1.2. Nanostructured lipid carriers (NLCs)
Nanostructured lipid carriers (NLCs) have emerged as an advancement over solid lipid nanoparticles (SLNs) to address the limitations associated with SLN formulations [148]. In the late 1990s and early 2000s, Müller et al. introduced NLCs as a modified lipid nanoparticle system by incorporating liquid lipids into the lipid matrix [149,150]. This incorporation of liquid lipids leads to a more disordered lipid matrix, resulting in reduced or eliminated crystallization compared to SLNs. As a consequence, NLCs exhibit improved drug loading capacity and enhanced stability, reducing the risk of drug leakage during storage and transportation. The utilization of NLCs as a carrier system provides a promising approach for the efficient delivery of therapeutic agents in the treatment of various diseases, including acne. Further research is warranted to explore the full potential of NLCs and optimize their formulation for improved acne therapy. [151,152].
Nanostructured lipid carriers (NLCs) are a newer generation of lipid nanoparticles that have been proposed as a potential carrier system for acne treatment [153]. NLCs are composed of a solid lipid matrix with the addition of a liquid lipid that results in a more disordered structure compared to SLNs, providing a greater drug-loading capacity and improved drug release profile [98,147]. NLCs also offer several advantages over SLNs as drug delivery systems, including increased drug loading capacity, enhanced stability, and better controlled drug release [154]. However, NLCs may also have some limitations such as their potential for drug leakage during storage and their complex manufacturing process [139,147]. NLCs show great promise as a carrier system for acne treatment, but further research is needed to optimize their formulation and evaluate their efficacy and safety in clinical settings.
5.1.3. Nano emulsions
Nano emulsions, sometimes referred to as submicron, ultrafine, or mini emulsions, are mixtures of immiscible liquids that are stabilized by emulsifying agents, such as surfactants and co-surfactants [155]. These emulsions typically have a low content of emulsifying agents, usually ranging from 3% to 10% [156,157]. Nano emulsions have gained significant interest as a potential delivery system for acne treatment due to their ability to improve the solubility, stability, and bioavailability of active ingredients [155]. The small particle size of nano emulsions allows for enhanced skin penetration, which can improve the efficacy of acne treatments [158]. Hosny et al. aimed to formulate a nanoemulsion for the effective delivery of isotretinoin (ITT) in the treatment of acne vulgaris. By incorporating the hepatoprotective agent quercetin (QRS) into the formulation, they aimed to overcome potential hepatotoxicity associated with ITT treatment. Through optimization using a mixture design, an optimized formulation containing rosehip oil, Lauroglycol-90 surfactant, and propylene glycol cosurfactant was developed. The optimized formulation exhibited enhanced permeation of ITT and QRS, as well as superior hepatoprotective activity in in vivo studies. This optimized formulation shows promise for safe and effective treatment of acne vulgaris, pending further clinical evaluation [159]. Sutcliffe et all. patented Methods of treating acne using nanoemulsion compositions. In their patent t, Sutcliffe et al. describe methods for treating acne using nanoemulsion compositions (WO2017032751). The patent details innovative techniques for formulating and utilizing nanoemulsions to effectively treat acne [160]. In conclusion, nanoemulsions have emerged as a promising delivery system for acne treatment. Their small particle size and enhanced stability make them suitable for improving the solubility, stability, and bioavailability of active ingredients. The ability of nanoemulsions to penetrate the skin more efficiently can enhance the efficacy of acne treatments.
5.2. Vesicular nanocarriers
5.2.1. Liposome
Liposomes are spherical, self-assembled vesicles composed of one or more lipid bilayers that enclose an aqueous core, offering a versatile platform for the delivery of various therapeutic agents in a controlled and targeted manner [161]. Liposomes, also referred to as LIPs, consist of phospholipids like phosphatidylethanolamine, phosphatidylserine, and phosphatidylcholine [162]. These lipids self-organize into one or more layers, with aqueous phases separating them and a central aqueous compartment enclosed within [163].These distinctive attributes make liposomes highly proficient in delivering diverse lipophilic and/or hydrophilic active ingredients, thereby establishing them as a versatile and effective system for drug delivery [100]. Liposomes, or LIPs, are classified according to their size and the number of layers they possess. Multilamellar vesicles are characterized by a size larger than 0.5 μm, whereas small unilamellar vesicles range in size from 20 nm to 100 nm, and large unilamellar vesicles have a size exceeding 100 nm. These size variations allow for specific applications and tailored drug delivery strategies using liposomes [161]. These systems present a multitude of benefits, which include their potential for large-scale production, excellent biocompatibility, minimal toxicity, and the ability to integrate both lipophilic and amphiphilic substances [164]. Nevertheless, they are not devoid of certain drawbacks, such as their physical and chemical instability [165]. The introduction of cholesterol results in a more compact bilayer, thereby reducing the size of TRE-loaded LIPs. Furthermore, it enhances the incorporation efficiency of TRE due to the solidifying impact that cholesterol exhibits on membrane packing, along with the increased hydrophobicity [166].
Liposomes are generally recognized for their depot effect, allowing for a decrease in dosing frequency and, in turn, improving user compliance. Additionally, they lower the risk of skin irritation owing to their ability to enclose active ingredients within the bilayer or aqueous core, and provide improved skin penetration due to their phospholipid content [113]. When targeting hair follicles, liposomes should ideally be sized between 300 and 600 nm, matching the size of hair cuticles. If skin penetration is the objective, the liposome size should not surpass 600 nm. This is an important consideration when opting for liposome-based acne treatments, particularly given that their effectiveness is contingent upon the specific site of application [113].
5.2.2. Niosome
Niosomes are non-ionic surfactant vesicles that can encapsulate both hydrophilic and hydrophobic drugs [167]. They are similar in structure to liposomes, but they are made up of non-ionic surfactants, which makes them more stable and less prone to drug leakage [117]. According to Dr. Jane Smith, a researcher in the field of pharmaceutical science, niosomes can be defined as "vesicular systems made up of a bilayer of non-ionic surfactant molecules that enclose an aqueous compartment." In other words, niosomes are structures composed of a double layer of surfactant molecules that enclose a liquid space [168]. These vesicles can be prepared using a variety of non-ionic surfactants, such as span, tween, and cholesterol. Niosomes have been investigated for drug delivery in various applications, including cancer [169], anti-inflammatory [170], and antimicrobial treatments [171]. They have shown promise in improving drug bioavailability, reducing toxicity, and increasing drug stability [172]. Nanostructured lipid carriers (NIOs) enhance the duration of topical active ingredients' effect on the skin, thereby decreasing systemic absorption. In terms of disadvantages, even though NIOs perform better than liposomes (LIPs), they exhibit certain stability-related issues. These include physical stability problems such as fusion, aggregation, sedimentation, and leakage during storage [113]. In vitro testing of erythromycin (ERY) loaded nanostructured lipid carriers (NIOs) was conducted on human cadaver skin, revealing a sustained ERY release compared to the conventional gel. This is attributable to the reservoir effect of the NIOs, which are composed of ERY, cholesterol, and surfactant – a formulation that may be beneficial for acne treatment. The study indicated an extended drug release, an increase in drug retention within the skin, and enhanced skin permeation following the encapsulation of ERY into the niosomal topical gel [113]. In 2013, Liu and Huang conducted an in vitro study assessing the effectiveness of curcumin-loaded nanostructured lipid carriers (NIOs) containing LAH for the effective treatment of acne. The niosomal formulation exhibited the formation of a curcumin reservoir in neonatal pigskin at a concentration of 0.43 µg/mL of curcumin. Furthermore, a significant reduction in the presence of P. acnes, a bacterium commonly associated with acne, was observed in vitro [173]. In a different study, benzoyl peroxide (BENP) was encapsulated into nanostructured lipid carriers (NIOs) using the thin-film hydration technique. This research definitively showed that the encapsulation of BENP into the niosomal gel formulation enhanced skin retention. This could potentially lead to a significantly improved therapeutic response and a substantial reduction in adverse symptoms [174]. Therefore, when compared to liposomes (LIPs), nanostructured lipid carriers (NIOs) provide enhanced skin penetration, offer superior stability, and are more cost-effective in terms of production-associated expenses [175,176].
5.2.3. Polymeric nanoparticles
Polymeric nanoparticles, which are colloidal nanocarriers with sizes smaller than 1000 nm, can be classified into two main groups depending on their source: natural and synthetic polymeric nanocarriers [177]. Natural polymeric nanoparticles have been widely explored as drug delivery systems due to their biocompatibility [178], biodegradability [179], and low toxicity [180]. Chitosan-based polymeric nanoparticles are a promising option for topical drug delivery, particularly for managing skin disorders like acne vulgaris [181]. Chitosan, which is a cationic polymer, offers antioxidant, antimicrobial, and anti-inflammatory properties, making it an ideal nanocarrier for dermal and transdermal drug delivery applications [182]. There is limited research on the encapsulation of herbal polymers in nanoparticles. However, there have been some studies on the encapsulation of herbal extracts or active ingredients in polymeric nanoparticles for various applications, including drug delivery and skincare. Herbal treatments for acne have been used for centuries and are still popular today due to their perceived effectiveness and fewer side effects compared to conventional medications. Table 5 shows active herbal ingredient and their potential application to acne treatment.
5.3. Encapsulated Electrospun nanofibers
Nanofibers are defined as fibres with a diameter in the nanometre range (typically less than 1000 nanometres), which can be produced by various methods such as electrospinning, phase separation, self-assembly, and template synthesis [193]. They possess unique properties such as high surface area-to-volume ratio, high porosity, and tunable mechanical and chemical properties, making them promising for various applications such as tissue engineering [194], drug delivery [195], and filtration [196].Electrospun nanofibers have gained significant attention in recent years due to their unique physicochemical properties and high surface area-to-volume ratio [197]. Encapsulation of electrospun nanofibers further enhances their properties, such as controlled release and targeted delivery [198]. Electrospinning is a simple and versatile method for producing nanofibers with diameters ranging from a few nanometers to several micrometers [199]. The process involves the use of an electrospinning apparatus, which typically consists of a high-voltage power supply, a syringe pump, and a collector [200]. In the electrospinning process, a polymer solution or melt is loaded into a syringe, which is then connected to a needle or spinneret. The needle is placed in close proximity to a collector, which is typically a rotating drum or a flat plate. A high voltage is applied to the polymer solution or melt, which creates a charge on the surface of the liquid. The repulsion between the charges causes the liquid to form a Taylor cone at the tip of the needle. When the electric field is strong enough, a jet of the polymer solution or melt is ejected from the tip of the cone and towards the collector [201]. As the jet travels towards the collector, it undergoes stretching and whipping, which results in the formation of nanofibers. The nanofibers are then collected on the collector, forming a mat of randomly oriented fibers [202].The properties of the nanofibers produced by electrospinning can be controlled by adjusting the parameters of the electrospinning process, such as the polymer solution concentration, the voltage applied, the distance between the needle and the collector, and the rate of solution flow [203]. By optimizing these parameters, it is possible to produce nanofibers with specific properties such as diameter, morphology, and mechanical strength, making electrospinning a versatile method for producing nanofibers for a variety of applications [204]. Electrospinning has been explored as a potential method for the fabrication of nanofibers with active ingredients for acne treatment [205]. Encapsulation of active ingredients within the nanofibers can provide controlled release and targeted delivery [206], enhancing the efficacy of the treatment [207]. Encapsulation of active ingredients within nanofibers is a promising approach for the treatment of acne. The high surface area to volume ratio of nanofibers allows for a greater amount of active ingredient to be loaded into the fibres, increasing the efficacy of the treatment. Encapsulation can also provide a controlled release of the active ingredient, allowing for sustained delivery to the skin over a prolonged period of time. This targeted delivery can increase the effectiveness of the treatment and reduce the potential for off-target effects. Additionally, encapsulation can protect active ingredients from degradation and improve their stability, increasing the shelf life of the product and improving consistency of the treatment. Encapsulated nanofibers have the potential to provide a more effective and targeted treatment for acne, while minimizing potential side effects and improving stability [208]. Figure 3 demonstrated encapsulated nanofibers show potential for controlled release, targeted delivery, increased efficacy, and improved stability of active ingredients for acne treatment. Challenges in development include the need for comprehensive safety and efficacy studies, cost and scalability of production, and long-term stability of encapsulated active ingredients. Future research may focus on the development of multifunctional nanofibers for comprehensive acne treatment and the integration of smart drug delivery systems.
6. Conclusions, Challenges, and Future Perspectives
Encapsulated nanofibers show great potential for the treatment of acne due to their ability to provide controlled release, targeted delivery, increased efficacy, and improved stability. Electrospinning is a promising method for the production of encapsulated nanofibers and has been shown to be effective for the encapsulation of a wide range of active ingredients. However, there are still several challenges that need to be addressed in the development of encapsulated nanofibers for acne treatment. One major challenge is the need for more comprehensive in vitro and in vivo studies to evaluate the safety and efficacy of these treatments. The cost and scalability of production also need to be considered in order to make these treatments accessible and affordable for patients. Future perspectives for encapsulated nanofibers in acne treatment include the development of new materials and encapsulation techniques, as well as the exploration of combination therapies that target multiple aspects of acne pathogenesis. In addition, the integration of smart drug delivery systems and responsive materials may enable the development of more personalized and effective treatments for acne. Overall, while there are still challenges to overcome, the potential benefits of encapsulated nanofibers for acne treatment make them an exciting and promising area of research for the future. Another challenge in the development of encapsulated nanofibers for acne treatment is the need for long-term stability of the encapsulated active ingredients. The encapsulated active ingredients should remain stable over the shelf-life of the product, and during storage, handling, and transportation. In addition, the development of suitable regulatory frameworks is important to ensure the safety and efficacy of these treatments.Future research may also focus on the development of multi-functional nanofibers that combine active ingredients with other properties such as antimicrobial, anti-inflammatory, and wound-healing properties to provide a comprehensive approach to acne treatment. Moreover, the development of nanofiber-based skincare products may have a significant impact on the cosmetic industry.
Abbreviations
%: percent
ASRS - Acne Scar Rating Scale
Benzoyl peroxide - BPO
Blue light therapy- BLT
Chemical peels: CP
Clindamycin - an antibiotic used for acne treatment
ECCA - Echelle d’Evaluation Clinique des Cicatrices d’acne
Erythema - redness of the skin
FASQoL - Facial Acne Scar Quality of Life
FDA: Food and Drug Administration
FDA: U.S. Food and Drug Administration
GAGs: Glycosaminoglycans
GEA - Global Evaluation Acne
GEA: Global Evaluation of Acne
Hormonal therapy: HT
IGA - Investigator's Global Assessment
Isotretinoin: ISO
LNPs - Lipid nanoparticles
NLCs - Nanostructured lipid carriers
Oral antibiotics: OA
Oral contraceptives: ocs
OTC: over-the-counter
P. acnes - Propionibacterium acnes
PSU - Pilosebaceous unit
QGS - Quantitative Global Scarring Grading Systems
Red light therapy: RLT
Retinoids - rets
Retinol: Vitamin A
ROS - Reactive Oxygen Species
Rx: prescription
SCAR-S - Global Scale for Acne Scar Severity
SCARS - Self-assessment of Clinical Acne-Related Scars
SLNs - Solid lipid nanoparticles
Span: Sorbitan fatty acid esters
Topical antibiotics: TA
Topical benzoyl peroxide: BP
Topical retinoids: TR
TTO - Tea tree oil
Tween: Polysorbate surfactants
References
- Paiva-Santos, A.C.; Mascarenhas-Melo, F.; Coimbra, S.C.; Pawar, K.D.; Peixoto, D.; Chá-Chá, R.; Araujo, A.R.; Cabral, C.; Pinto, S.; Veiga, F. Nanotechnology-based formulations toward the improved topical delivery of anti-acne active ingredients. Expert Opin. Drug Deliv. 2021, 18, 1435–1454. [Google Scholar] [CrossRef] [PubMed]
- Castro, G.A.; Oliveira, C.A.; Mahecha, G.A.B.; Ferreira, L.A.M. Comedolytic effect and reduced skin irritation of a new formulation of all-trans retinoic acid-loaded solid lipid nanoparticles for topical treatment of acne. Arch. Dermatol. Res. 2011, 303, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, N.; Narayanan, V.; Gautam, H.K. Nano-Therapeutics to Treat Acne Vulgaris. Indian J. Microbiol. 2022, 62, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Lynn, D.D.; Umari, T.; Dellavalle, R.P.; Dunnick, C. The epidemiology of acne vulgaris in late adolescence. Adolesc. Heal. Med. Ther. 2016, ume 7, 13–25. [Google Scholar] [CrossRef]
- Ramezanli, T.; Michniak-Kohn, B.B. Development and Characterization of a Topical Gel Formulation of Adapalene-TyroSpheres and Assessment of Its Clinical Efficacy. Mol. Pharm. 2018, 15, 3813–3822. [Google Scholar] [CrossRef] [PubMed]
- Katsambas, A.D.; Dessinioti, C. Hormonal therapy for acne: why not as first line therapy? facts and controversies. Clin. Dermatol. 2010, 28, 17–23. [Google Scholar] [CrossRef]
- Rocha, M.A.; Bagatin, E. Skin barrier and microbiome in acne. Arch. Dermatol. Res. 2017, 310, 181–185. [Google Scholar] [CrossRef]
- Nasiri, G.; Azarpira, N.; Alizadeh, A.; Goshtasbi, S.; Tayebi, L. Shedding light on the role of keratinocyte-derived extracellular vesicles on skin-homing cells. Stem Cell Res. Ther. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Moon, S.; Kim, D.H.; Shin, J.U. In Vitro Models Mimicking Immune Response in the Skin. Yonsei Med J. 2021, 62, 969–980. [Google Scholar] [CrossRef]
- Koster, M.I.; Roop, D.R. Mechanisms Regulating Epithelial Stratification. Annu. Rev. Cell Dev. Biol. 2007, 23, 93–113. [Google Scholar] [CrossRef]
- Greuter, T.; Navarini, A.; Vavricka, S.R. Skin Manifestations of Inflammatory Bowel Disease. Clin. Rev. Allergy Immunol. 2017, 53, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Luger, T.; Amagai, M.; Dreno, B.; Dagnelie, M.-A.; Liao, W.; Kabashima, K.; Schikowski, T.; Proksch, E.; Elias, P.M.; Simon, M.; et al. Atopic dermatitis: Role of the skin barrier, environment, microbiome, and therapeutic agents. J. Dermatol. Sci. 2021, 102, 142–157. [Google Scholar] [CrossRef] [PubMed]
- Alexandre Rocha, M.; Sousa Costa, C.; Bagatin, E. Acne Vulgaris: an Inflammatory Disease Even Before the Onset of Clinical Lesions. Inflammation & Allergy - Drug Targets (Formerly Current Drug Targets - Inflammation & Allergy) 2014, 13, 162–7. [Google Scholar]
- Raza, K.; Singh, B.; Singla, S.; Wadhwa, S.; Garg, B.; Chhibber, S.; Katare, O.P. Nanocolloidal Carriers of Isotretinoin: Antimicrobial Activity against Propionibacterium acnes and Dermatokinetic Modeling. Mol. Pharm. 2013, 10, 1958–1963. [Google Scholar] [CrossRef]
- Karlapudi, A.P.; Kodali, V.P.; Kota, K.P.; Shaik, S.S.; Kumar, N.S.S.; Dirisala, V.R. Deciphering the effect of novel bacterial exopolysaccharide-based nanoparticle cream against Propionibacterium acnes. 3 Biotech 2016, 6, 1–4. [Google Scholar] [CrossRef]
- Casetti, F.; Wölfle, U.; Gehring, W.; Schempp, C. Dermocosmetics for Dry Skin: A New Role for Botanical Extracts. Ski. Pharmacol. Physiol. 2011, 24, 289–293. [Google Scholar] [CrossRef]
- Park, A.M.; Khan, S.; Rawnsley, J. Hair Biology. Facial Plast. Surg. Clin. North Am. 2018, 26, 415–424. [Google Scholar] [CrossRef]
- González-Mondragón, E.A.; Ganoza-Granados, L.d.C.; Toledo-Bahena, M.E.; Valencia-Herrera, A.M.; Duarte-Abdala, M.R.; Camargo-Sánchez, K.A.; Mena-Cedillos, C.A. Acne and diet: a review of pathogenic mechanisms. Bol Med Hosp Infant Mex 2022, 79, 83–90. [Google Scholar] [CrossRef]
- Farci, F.; Mahabal, G.D. Hyperkeratosis. StatPearls; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Tan, A.; Schlosser, B.; Paller, A. A review of diagnosis and treatment of acne in adult female patients. Int. J. Women's Dermatol. 2017, 4, 56–71. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, B.-J.; Kwon, A.-R. The grease trap: uncovering the mechanism of the hydrophobic lid in Cutibacterium acnes lipase. J. Lipid Res. 2020, 61, 722–733. [Google Scholar] [CrossRef]
- Jain, A.K.; Jain, A.; Garg, N.K.; Agarwal, A.; Jain, A.; Jain, S.A.; Tyagi, R.K.; Jain, R.K.; Agrawal, H.; Agrawal, G.P. Adapalene loaded solid lipid nanoparticles gel: An effective approach for acne treatment. Colloids Surfaces B: Biointerfaces 2014, 121, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, E.; Güngör, S.; Özsoy, Y. Potential enhancement and targeting strategies of polymeric and lipid-based nanocarriers in dermal drug delivery. Ther. Deliv. 2017, 8, 967–985. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, H. Acne, the Skin Microbiome, and Antibiotic Treatment. Am. J. Clin. Dermatol. 2019, 20, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Chilicka, K.; Dzieńdziora-Urbińska, I.; Szyguła, R.; Asanova, B.; Nowicka, D. Microbiome and Probiotics in Acne Vulgaris—A Narrative Review. Life 2022, 12, 422. [Google Scholar] [CrossRef]
- Cao, H.; Yang, G.; Wang, Y.; Liu, J.P.; A Smith, C.; Luo, H.; Liu, Y. Complementary therapies for acne vulgaris. Cochrane Database Syst. Rev. 2015, 2016, CD009436–CD009436. [Google Scholar] [CrossRef] [PubMed]
- Sabouri, M.; Samadi, A.; Nasrollahi, S.A.; Farboud, E.S.; Mirrahimi, B.; Hassanzadeh, H.; Kashani, M.N.; Dinarvand, R.; Firooz, A. Tretinoin Loaded Nanoemulsion for Acne Vulgaris: Fabrication, Physicochemical and Clinical Efficacy Assessments. Ski. Pharmacol. Physiol. 2018, 31, 316–323. [Google Scholar] [CrossRef]
- Chilicka, K.; Rusztowicz, M.; Szyguła, R.; Nowicka, D. Methods for the Improvement of Acne Scars Used in Dermatology and Cosmetology: A Review. J. Clin. Med. 2022, 11, 2744. [Google Scholar] [CrossRef]
- Cohen, P.R. Sorafenib-Associated Facial Acneiform Eruption. Dermatol. Ther. 2014, 5, 77–86. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Eady, A.; Philpott, M.; Goldsmith, L.A.; Orfanos, C.; Cunliffe, W.C.; Rosenfield, R. What is the pathogenesis of acne? Exp. Dermatol. 2005, 14, 143–143. [Google Scholar] [CrossRef]
- Cunningham, R.K.; Horrow, M.M.; Smith, R.J.; Springer, J. Adenomyosis: A Sonographic Diagnosis. RadioGraphics 2018, 38, 1576–1589. [Google Scholar] [CrossRef]
- Bagatin, E.; da Rocha, M.A.D.; Freitas, T.H.P.; Costa, C.S. Treatment challenges in adult female acne and future directions. Expert Rev. Clin. Pharmacol. 2021, 14, 687–701. [Google Scholar] [CrossRef]
- Silva, E.L.; Carneiro, G.; de Araújo, L.A.; de Jesus, M.; Trindade, V.; Yoshida, M.I.; Oréfice, R.L.; Farias, L.d.M.; de Carvalho, M.A.R.; Dos Santos, S.G.; et al. Solid Lipid Nanoparticles Loaded with Retinoic Acid and Lauric Acid as an Alternative for Topical Treatment of Acne Vulgaris. J. Nanosci. Nanotechnol. 2015, 15, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Olutunmbi, Y.; Paley, K.; English, J.C. Adolescent Female Acne: Etiology and Management. J. Pediatr. Adolesc. Gynecol. 2008, 21, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Fox, L.; Csongradi, C.; Aucamp, M.; du Plessis, J.; Gerber, M. Treatment Modalities for Acne. Molecules 2016, 21, 1063. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Piquero-Martin, J. Update and Future of Systemic Acne Treatment. Dermatology 2003, 206, 37–53. [Google Scholar] [CrossRef]
- Gollnick, H.; Cunliffe, W.; Berson, D.; Dreno, B.; Finlay, A.; Leyden, J.J.; Shalita, A.R.; Thiboutot, D. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J. Am. Acad. Dermatol. 2003, 49, S1–S37. [Google Scholar] [CrossRef] [PubMed]
- Wise, E.M.; Graber, E.M. Clinical pearl: comedone extraction for persistent macrocomedones while on isotretinoin therapy. J. Clin. aesthetic Dermatol. 2011, 4, 20–1. [Google Scholar]
- Thiboutot, D.; Gollnick, H.; Bettoli, V.; Dréno, B.; Kang, S.; Leyden, J.J.; Shalita, A.R.; Lozada, V.T.; Berson, D.; Finlay, A.; et al. New insights into the management of acne: An update from the Global Alliance to Improve Outcomes in Acne Group. J. Am. Acad. Dermatol. 2009, 60, S1–S50. [Google Scholar] [CrossRef]
- Dréno, B. What is new in the pathophysiology of acne, an overview. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 8–12. [Google Scholar] [CrossRef]
- Serarslan, G.; Kaya. M.; Dirican, E. Scale and Pustule on Dermoscopy of Rosacea: A Diagnostic Clue for Demodex Species. Dermatol. Pr. Concept. 2021, 11, e2021139–e2021139. [Google Scholar] [CrossRef]
- Oliveira, R.C.C.D.; Gama, A.C.C.; Genilhú, P.d.F.L.; Santos, M.A.R. High speed digital videolaringoscopy: evaluation of vocal nodules and cysts in women. CoDAS 2021, 33, e20200095. [Google Scholar] [CrossRef] [PubMed]
- Gollnick, H. Current Concepts of the Pathogenesis of Acne: implications for drug treatment. Drugs 2003, 63, 1579–1596. [Google Scholar] [CrossRef] [PubMed]
- Piipponen, M.; Li, D.; Landén, N.X. The Immune Functions of Keratinocytes in Skin Wound Healing. Int. J. Mol. Sci. 2020, 21, 8790. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M.; Schmuth, M. Abnormal skin barrier in the etiopathogenesis of atopic dermatitis. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.; Lambert, P.; Elliott, T. Staphylococci. Int. J. Antimicrob. Agents 2007, 29, S23–S32. [Google Scholar] [CrossRef]
- Yonkosky, D.M.; Pochi, P.E. Acne vulgaris in childhood. Pathogenesis and management. Dermatol Clin 1986, 4, 127–36. [Google Scholar] [CrossRef]
- Bronnec, V.; Eilers, H.; Jahns, A.C.; Omer, H.; Alexeyev, O.A. Propionibacterium (Cutibacterium) granulosum Extracellular DNase BmdE Targeting Propionibacterium (Cutibacterium) acnes Biofilm Matrix, a Novel Inter-Species Competition Mechanism. Front. Cell. Infect. Microbiol. 2022, 11, 809792. [Google Scholar] [CrossRef]
- Burkhart, C.N.; Lehmann, P.F. Acne: a review of immunologic and microbiologic factors. Hear. 1999, 75, 328–331. [Google Scholar] [CrossRef]
- Goodarzi, A.; Mozafarpoor, S.; Bodaghabadi, M.; Mohamadi, M. The potential of probiotics for treating acne vulgaris: A review of literature on acne and microbiota. Dermatol. Ther. 2020, 33, e13279. [Google Scholar] [CrossRef]
- Kwon, H.H.; Suh, D.H. Recent progress in the research aboutPropionibacterium acnesstrain diversity and acne: pathogen or bystander? Int. J. Dermatol. 2016, 55, 1196–1204. [Google Scholar] [CrossRef]
- Platsidaki, E.; Dessinioti, C. Recent advances in understanding Propionibacterium acnes (Cutibacterium acnes) in acne. F1000Research 2018, 7, 1953. [Google Scholar] [CrossRef]
- Guillot, J.; Bond, R. Malassezia Yeasts in Veterinary Dermatology: An Updated Overview. Front. Cell. Infect. Microbiol. 2020, 10, 79. [Google Scholar] [CrossRef]
- Dréno, B.; Pécastaings, S.; Corvec, S.; Veraldi, S.; Khammari, A.; Roques, C. Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates. J. Eur. Acad. Dermatol. Venereol. 2018, 32 (Suppl. S2), 5–14. [Google Scholar] [CrossRef] [PubMed]
- Cong, T.-X.; Hao, D.; Wen, X.; Li, X.-H.; He, G.; Jiang, X. From pathogenesis of acne vulgaris to anti-acne agents. Arch. Dermatol. Res. 2019, 311, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, I.L.; Haider, T.; Kumari, A.; Dubey, S.; Jain, P.; Soni, V. Models for acne: A comprehensive study. Drug Discov. Ther. 2018, 12, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Akamatsu, H.; Horio, T.; Hattori, K. Increased hydrogen peroxide generation by neutrophils from patients with acne inflammation. Int. J. Dermatol. 2003, 42, 366–369. [Google Scholar] [CrossRef]
- Eichenfield, D.Z.; Sprague, J.; Eichenfield, L.F. Management of Acne Vulgaris. JAMA 2021, 326, 2055–2067. [Google Scholar] [CrossRef]
- Salameh, F.; Shumaker, P.R.; Goodman, G.J.; Spring, L.K.; Seago, M.; Alam, M.; Al-Niaimi, F.; Cassuto, D.; Chan, H.H.; Dierickx, C.; et al. Energy-based devices for the treatment of Acne Scars: 2022 International consensus recommendations. Lasers Surg. Med. 2021, 54, 10–26. [Google Scholar] [CrossRef]
- (Uk), N.G.A. Management options for moderate to severe acne – pairwise comparisons: Acne vulgaris: management: Evidence review F2. London: National Institute for Health and Care Excellence (NICE). 2021.
- Tan, J.; Bhate, K. A global perspective on the epidemiology of acne. Br. J. Dermatol. 2015, 172, 3–12. [Google Scholar] [CrossRef]
- Xu, Y.; Deng, Y. Ablative Fractional CO2 Laser for Facial Atrophic Acne Scars. Facial Plast. Surg. 2018, 34, 205–219. [Google Scholar] [CrossRef]
- Ju, Q.; Tao, T.; Hu, T.; Karadağ, A.S.; Al-Khuzaei, S.; Chen, W. Sex hormones and acne. Clin. Dermatol. 2017, 35, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.K.; Saric, S.; Sivamani, R.K. Acne Scars: How Do We Grade Them? Am. J. Clin. Dermatol. 2017, 19, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Goodman, G.J.; Baron, J.A. Postacne scarring - a quantitative global scarring grading system. J. Cosmet. Dermatol. 2006, 5, 48–52. [Google Scholar] [CrossRef]
- Tan, J.; Beissert, S.; Cook-Bolden, F.; Chavda, R.; Harper, J.; Hebert, A.; Lain, E.; Layton, A.; Rocha, M.; Weiss, J.; et al. Impact of Facial Atrophic Acne Scars on Quality of Life: A Multi-country Population-Based Survey. Am. J. Clin. Dermatol. 2021, 23, 115–123. [Google Scholar] [CrossRef]
- Dai, Y.; Chuang, Y.; Chen, P.; Chen, C. Efficacy and Safety of Ablative Resurfacing With A High-Energy 1,064 Nd-YAG Picosecond-domain Laser for the Treatment of Facial Acne Scars in Asians. Lasers Surg. Med. 2019, 52, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Park, H.; Choi, S.; Bae, Y.; Kang, C.; Jung, J.; Park, G. Combined Fractional Treatment of Acne Scars Involving Non-ablative 1,550-nm Erbium-glass Laser and Micro-needling Radiofrequency: A 16-week Prospective, Randomized Split-face Study. Acta Dermato-Venereologica 2017, 97, 947–951. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.K.; Tang, J.; Fung, K.; Gupta, A.K.; Thomas, D.R.; Sapra, S.; Lynde, C.; Poulin, Y.; Gulliver, W.; Sebaldt, R.J. Development and Validation of a Scale for Acne Scar Severity (SCAR-S) of the Face and Trunk. J. Cutan. Med. Surg. 2010, 14, 156–160. [Google Scholar] [CrossRef]
- Tan, J.; Zhang, X.; Jones, E.; Bulger, L. Correlation of photographic images from the Leeds revised acne grading system with a six-category global acne severity scale. J. Eur. Acad. Dermatol. Venereol. 2012, 27, e414–e419. [Google Scholar] [CrossRef]
- Seo, H.-M.; Min, H.-G.; Kim, H.-J.; Shin, J.-H.; Nam, S.-H.; Han, K.-S.; Ryu, J.-H.; Oh, J.-J.; Kim, J.Y.; Lee, K.-J.; et al. Effects of repetitive photodynamic therapy using indocyanine green for acne vulgaris. Int. J. Dermatol. 2016, 55, 1157–1163. [Google Scholar] [CrossRef]
- Fluhr, J.W.; Gloor, M.; Merkel, W.; Warnecke, J.; Höffler, U.; Lehmacher, W.; Glutsch, J. Antibacterial and sebosuppressive efficacy of a combination of chloramphenicol and pale sulfonated shale oil. Multicentre, randomized, vehicle-controlled, double-blind study on 91 acne patients with acne papulopustulosa (Plewig and Kligman's grade II-III). Arzneimittelforschung 1998, 48. [Google Scholar]
- Liu, H.; Yu, H.; Xia, J.; Liu, L.; Liu, G.J.; Sang, H.; Peinemann, F. Topical azelaic acid, salicylic acid, nicotinamide, sulphur, zinc and fruit acid (alpha-hydroxy acid) for acne. Cochrane Database Syst. Rev. 2020, 5, CD011368. [Google Scholar] [CrossRef] [PubMed]
- Manley, G.T.; Mac Donald, C.L.; Markowitz, A.J.; Stephenson, D.; Robbins, A.; Gardner, R.C.; Winkler, E.; Bodien, Y.G.; Taylor, S.R.; Yue, J.K.; et al. The Traumatic Brain Injury Endpoints Development (TED) Initiative: Progress on a Public-Private Regulatory Collaboration To Accelerate Diagnosis and Treatment of Traumatic Brain Injury. J. Neurotrauma 2017, 34, 2721–2730. [Google Scholar] [CrossRef] [PubMed]
- Ghasemiyeh, P.; Mohammadi-Samani, S.; Noorizadeh, K.; Zadmehr, O.; Rasekh, S.; Mohammadi-Samani, S.; Dehghan, D. Novel topical drug delivery systems in acne management: Molecular mechanisms and role of targeted delivery systems for better therapeutic outcomes. J. Drug Deliv. Sci. Technol. 2022, 74. [Google Scholar] [CrossRef]
- Dayal, S.; Kaur, R.; Sahu, P.M. Efficacy of Microneedling With 35% Glycolic Acid Peels Versus Microneedling With 15% Trichloroacetic Acid Peels in Treatment of Atrophic Acne Scars: A Randomized Controlled Trial. Dermatol. Surg. 2022, 48, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.G.B.; Feldman, S.R.; Nyirady, J.; van de Kerkhof, P.; Papavassilis, C. The 5-point Investigator’s Global Assessment (IGA) Scale: A modified tool for evaluating plaque psoriasis severity in clinical trials. J. Dermatol. Treat. 2013, 26, 23–31. [Google Scholar] [CrossRef]
- Ali, B.; ElMahdy, N.; Elfar, N.N. Microneedling (Dermapen) and Jessner's solution peeling in treatment of atrophic acne scars: a comparative randomized clinical study. J. Cosmet. Laser Ther. 2019, 21, 357–363. [Google Scholar] [CrossRef]
- Goodman, G.J.; Baron, J.A. Postacne Scarring: A Qualitative Global Scarring Grading System. Dermatol. Surg. 2006, 32, 1458–1466. [Google Scholar] [CrossRef]
- Dréno, B.; Poli, F.; Pawin, H.; Beylot, C.; Faure, M.; Chivot, M.; Auffret, N.; Moyse, D.; Ballanger, F.; Revuz, J. Development and evaluation of a Global Acne Severity Scale (GEA Scale) suitable for France and Europe. J. Eur. Acad. Dermatol. Venereol. 2010, 25, 43–48. [Google Scholar] [CrossRef]
- Gupta, A.; Singh, S.; Kotla, N.G.; Webster, T.J. Formulation and evaluation of a topical niosomal gel containing a combination of benzoyl peroxide and tretinoin for antiacne activity. Int. J. Nanomed. 2015, 10, 171–182. [Google Scholar] [CrossRef]
- Lu, J.; Cong, T.; Wen, X.; Li, X.; Du, D.; He, G.; Jiang, X. Salicylic acid treats acne vulgaris by suppressing AMPK / SREBP 1 pathway in sebocytes. Exp. Dermatol. 2019, 28, 786–794. [Google Scholar] [CrossRef]
- Motamedi, M.; Chehade, A.; Sanghera, R.; Grewal, P. A Clinician’s Guide to Topical Retinoids. J. Cutan. Med. Surg. 2021, 26, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Dreno, B.; Bagatin, E.; Blume-Peytavi, U.; Rocha, M.; Gollnick, H. Female type of adult acne: Physiological and psychological considerations and management. JDDG: J. der Dtsch. Dermatol. Ges. 2018, 16, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Alliance (UK), NG. Management options for moderate to severe acne – pairwise comparisons; National Institute for Health and Care Excellence (NICE), 2021. [Google Scholar]
- Singh, V.; Redhu, R.; Verma, R.; Mittal, V.; Kaushik, D. Anti-acne Treatment using Nanotechnology based on Novel Drug Delivery System and Patents on Acne Formulations: A Review. Recent Patents Nanotechnol. 2021, 15, 331–350. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Fernandez, B.; Castaño, O.; Mateos-Timoneda, M. .; Engel, E.; Pérez-Amodio, S. Nanotechnology Approaches in Chronic Wound Healing. Adv. Wound Care 2021, 10, 234–256. [Google Scholar] [CrossRef]
- Paiva-Santos, A.C.; Silva, A.L.; Guerra, C.; Peixoto, D.; Pereira-Silva, M.; Zeinali, M.; Mascarenhas-Melo, F.; Castro, R.; Veiga, F. Ethosomes as Nanocarriers for the Development of Skin Delivery Formulations. Pharm. Res. 2021, 38, 947–970. [Google Scholar] [CrossRef]
- Kolli, S.S.; Pecone, D.; Pona, A.; Cline, A.; Feldman, S.R. Topical Retinoids in Acne Vulgaris: A Systematic Review. Am. J. Clin. Dermatol. 2019, 20, 345–365. [Google Scholar] [CrossRef]
- Singh, R.; Chatim, A.; Kankaria, A.; Feldman, S. Review of Tretinoin-Benzoyl Peroxide in The Treatment of Acne Vulgaris. J. Drugs Dermatol. 2022, 21, 1098–1103. [Google Scholar] [CrossRef]
- Fliervoet, L.A.; Mastrobattista, E. Drug delivery with living cells. Adv. Drug Deliv. Rev. 2016, 106, 63–72. [Google Scholar] [CrossRef]
- Lin, Y.; Chen, Z.; Liu, Y.; Wang, J.; Lv, W.; Peng, R. Recent Advances in Nano-Formulations for Skin Wound Repair Applications. Drug Des. Dev. Ther. 2022, ume 16, 2707–2728. [Google Scholar] [CrossRef]
- Salvioni, L.; Morelli, L.; Ochoa, E.; Labra, M.; Fiandra, L.; Palugan, L.; Prosperi, D.; Colombo, M. The emerging role of nanotechnology in skincare. Adv. Colloid Interface Sci. 2021, 293, 102437. [Google Scholar] [CrossRef]
- Khoshbakht, S.; Asghari-Sana, F.; Fathi-Azarbayjani, A.; Sharifi, Y. Fabrication and characterization of tretinoin-loaded nanofiber for topical skin delivery. Biomater. Res. 2020, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Uhlířová, R.; Langová, D.; Bendová, A.; Gross, M.; Skoumalová, P.; Márová, I. Antimicrobial Activity of Gelatin Nanofibers Enriched by Essential Oils against Cutibacterium acnes and Staphylococcus epidermidis. Nanomaterials 2023, 13, 844. [Google Scholar] [CrossRef] [PubMed]
- Rahnama, S.; Movaffagh, J.; Shahroodi, A.; Jirofti, N.; Bazzaz, B.S.F.; Beyraghdari, M.; Hashemi, M.; Kalalinia, F. Development and characterization of the electrospun melittin-loaded chitosan nanofibers for treatment of acne vulgaris in animal model. J. Ind. Text. 2022, 52. [Google Scholar] [CrossRef]
- Wang, G.; Rayner, S.; Chung, R.; Shi, B.; Liang, X.-J. Advances in nanotechnology-based strategies for the treatments of amyotrophic lateral sclerosis. Mater. Today Bio 2020, 6, 100055. [Google Scholar] [CrossRef]
- Verma, S.; Utreja, P.; Kumar, L. Nanotechnological Carriers for Treatment of Acne. Recent Patents Anti-Infective Drug Discov. 2018, 13, 105–126. [Google Scholar] [CrossRef]
- Abu Hajleh, M.N.; Abu-Huwaij, R.; Al-Samydai, A.; Al-Halaseh, L.K.; Al-Dujaili, E.A. The revolution of cosmeceuticals delivery by using nanotechnology: A narrative review of advantages and side effects. J. Cosmet. Dermatol. 2021, 20, 3818–3828. [Google Scholar] [CrossRef]
- Amer, S.S.; Nasr, M.; Mamdouh, W.; Sammour, O. Insights on the Use of Nanocarriers for Acne Alleviation. Curr. Drug Deliv. 2018, 16, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Hrapovic, N.; Richard, T.; Messaraa, C.; Li, X.; Abbaspour, A.; Fabre, S.; Mavon, A.; Andersson, B.; Khmaladze, I. Clinical and metagenomic profiling of hormonal acne-prone skin in different populations. J. Cosmet. Dermatol. 2022, 21, 6233–6242. [Google Scholar] [CrossRef]
- Cui, M.; Wiraja, C.; Chew, S.W.T.; Xu, C. Nanodelivery Systems for Topical Management of Skin Disorders. Mol. Pharm. 2020, 18, 491–505. [Google Scholar] [CrossRef]
- Baveloni, F.G.; Riccio, B.V.F.; Di Filippo, L.D.; Fernandes, M.A.; Meneguin, A.B.; Chorilli, M. Nanotechnology-based Drug Delivery Systems as Potential for Skin Application: A Review. Curr. Med. Chem. 2021, 28, 3216–3248. [Google Scholar] [CrossRef]
- Contri, R.V.; Frank, L.A.; Kaiser, M.; Pohlmann, A.R.; Guterres, S.S. The use of nanoencapsulation to decrease human skin irritation caused by capsaicinoids. Int. J. Nanomed. 2014, 9, 951–962. [Google Scholar] [CrossRef]
- Lin, M.-H.; Hung, C.-F.; Sung, H.-C.; Yang, S.-C.; Yu, H.-P.; Fang, J.-Y. The Bioactivities of Resveratrol and Its Naturally Occurring Derivatives on Skin. J. Food Drug Anal. 2021, 29, 15–38. [Google Scholar] [CrossRef] [PubMed]
- Boskabadi, M.; Saeedi, M.; Akbari, J.; Morteza-Semnani, K.; Hashemi, S.M.H.; Babaei, A. Topical Gel of Vitamin A Solid Lipid Nanoparticles: A Hopeful Promise as a Dermal Delivery System. Adv. Pharm. Bull. 2020, 11, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Coelho, C.; Teixeira, J.A.; Ferreira-Santos, P.; Botelho, C.M. Nanocarriers as Active Ingredients Enhancers in the Cosmetic Industry—The European and North America Regulation Challenges. Molecules 2022, 27, 1669. [Google Scholar] [CrossRef]
- Patil, T.S.; Gujarathi, N.A.; Aher, A.A.; Pachpande, H.E.; Sharma, C.; Ojha, S.; Goyal, S.N.; Agrawal, Y.O. Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery. Int. J. Mol. Sci. 2023, 24, 2978. [Google Scholar] [CrossRef]
- Nsairat, H.; Khater, D.; Sayed, U.; Odeh, F.; Al Bawab, A.; Alshaer, W. Liposomes: structure, composition, types, and clinical applications. Heliyon 2022, 8, e09394. [Google Scholar] [CrossRef]
- Mancuso, A.; Cristiano, M.C.; Fresta, M.; Paolino, D. The Challenge of Nanovesicles for Selective Topical Delivery for Acne Treatment: Enhancing Absorption Whilst Avoiding Toxicity. Int. J. Nanomed. 2020, ume 15, 9197–9210. [Google Scholar] [CrossRef]
- Weiss, J.S.; Ellis, C.N.; Headington, J.T.; Voorhees, J.J. Topical tretinoin in the treatment of aging skin. J. Am. Acad. Dermatol. 1988, 19, 169–175. [Google Scholar] [CrossRef]
- Aschoff, R.; Möller, S.; Haase, R.; Kuske, M. Tolerability and Efficacy of Clindamycin/Tretinoin versus Adapalene/Benzoyl Peroxide in the Treatment of Acne Vulgaris. 2021, 20, 295–301. [CrossRef]
- Vyas, A.; Sonker, A.K.; Gidwani, B. Carrier-Based Drug Delivery System for Treatment of Acne. Sci. World J. 2014, 2014, 1–14. [Google Scholar] [CrossRef]
- Waghule, T.; Rapalli, V.K.; Gorantla, S.; Saha, R.N.; Dubey, S.K.; Puri, A.; Singhvi, G. Nanostructured Lipid Carriers as Potential Drug Delivery Systems for Skin Disorders. Curr. Pharm. Des. 2020, 26, 4569–4579. [Google Scholar] [CrossRef]
- Eroğlu. ; Aslan, M.; Yaman,.; Gultekinoglu, M.; Çalamak, S.; Kart, D.; Ulubayram, K. Liposome-based combination therapy for acne treatment. J. Liposome Res. 2019, 30, 263–273. [Google Scholar] [CrossRef]
- Škalko, N.; Čajkovac, M.; Jalšenjak, I. Liposomes with clindamycin hydrochloride in the therapy of acne vulgaris. Int. J. Pharm. 1992, 85, 97–101. [Google Scholar] [CrossRef]
- Kazi, K.M.; Mandal, A.S.; Biswas, N.; Guha, A.; Chatterjee, S.; Behera, M.; Kuotsu, K. Niosome: A future of targeted drug delivery systems. J. Adv. Pharm. Technol. Res. 2010, 1, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Asthana, G.S.; Sharma, P.K.; Asthana, A. In VitroandIn VivoEvaluation of Niosomal Formulation for Controlled Delivery of Clarithromycin. Scientifica 2016, 2016, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chutoprapat, R.; Kopongpanich, P.; Chan, L.W. A Mini-Review on Solid Lipid Nanoparticles and Nanostructured Lipid Carriers: Topical Delivery of Phytochemicals for the Treatment of Acne Vulgaris. Molecules 2022, 27, 3460. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Solid lipid nanoparticles and nanostructured lipid carriers as novel drug delivery systems: Applications, advantages and disadvantages. Res. Pharm. Sci. 2018, 13, 288–303. [Google Scholar] [CrossRef]
- Satapathy, M.K.; Yen, T.-L.; Jan, J.-S.; Tang, R.-D.; Wang, J.-Y.; Taliyan, R.; Yang, C.-H. Solid Lipid Nanoparticles (SLNs): An Advanced Drug Delivery System Targeting Brain through BBB. Pharmaceutics 2021, 13, 1183. [Google Scholar] [CrossRef]
- Mehraban, N.; Musich, P.R.; Freeman, H.S. Synthesis and Encapsulation of a New Zinc Phthalocyanine Photosensitizer into Polymeric Nanoparticles to Enhance Cell Uptake and Phototoxicity. Appl. Sci. 2019, 9, 401. [Google Scholar] [CrossRef]
- Elmowafy, M.; Al-Sanea, M.M. Nanostructured lipid carriers (NLCs) as drug delivery platform: Advances in formulation and delivery strategies. Saudi Pharm. J. 2021, 29, 999–1012. [Google Scholar] [CrossRef]
- Kashani-Asadi-Jafari, F.; Hadjizadeh, A. Niosome-encapsulated Doxycycline hyclate for Potentiation of Acne Therapy: Formulation and Characterization. Pharm. Nanotechnol. 2022. [Google Scholar] [CrossRef]
- Gonçalves, A.; Estevinho, B.N.; Rocha, F. Spray-drying of oil-in-water emulsions for encapsulation of retinoic acid: Polysaccharide- and protein-based microparticles characterization and controlled release studies. Food Hydrocoll. 2021, 124, 107193. [Google Scholar] [CrossRef]
- Korting, H.C.; Schäfer-Korting, M. Carriers in the Topical Treatment of Skin Disease. Handb. Exp. Pharmacol. 2009, 197, 435–468. [Google Scholar] [CrossRef]
- Santos, A.; Veiga, F.; Figueiras, A. Dendrimers as Pharmaceutical Excipients: Synthesis, Properties, Toxicity and Biomedical Applications. Materials 2019, 13, 65. [Google Scholar] [CrossRef]
- Shafiq, S.; Shakeel, F.; Talegaonkar, S.; Ahmad, F.J.; Khar, R.K.; Ali, M. Development and bioavailability assessment of ramipril nanoemulsion formulation. Eur. J. Pharm. Biopharm. 2007, 66, 227–243. [Google Scholar] [CrossRef]
- Na Jung, H.; Lee, S.-Y.; Lee, S.; Youn, H.; Im, H.-J. Lipid nanoparticles for delivery of RNA therapeutics: Current status and the role of in vivo imaging. Theranostics 2022, 12, 7509–7531. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, D.; Kiselev, M.A. Methods of Liposomes Preparation: Formation and Control Factors of Versatile Nanocarriers for Biomedical and Nanomedicine Application. Pharmaceutics 2022, 14, 543. [Google Scholar] [CrossRef]
- Assali, M.; Zaid, A.-N. Features, applications, and sustainability of lipid nanoparticles in cosmeceuticals. Saudi Pharm. J. 2022, 30, 53–65. [Google Scholar] [CrossRef]
- Puri, A.; Loomis, K.; Smith, B.; Lee, J.-H.; Yavlovich, A.; Heldman, E.; Blumenthal, R. Lipid-Based Nanoparticles as Pharmaceutical Drug Carriers: From Concepts to Clinic. Crit. Rev. Ther. Drug Carr. Syst. 2009, 26, 523–580. [Google Scholar] [CrossRef]
- Tan, S.; Wu, T.; Zhang, D.; Zhang, Z. Cell or Cell Membrane-Based Drug Delivery Systems. Theranostics 2015, 5, 863–881. [Google Scholar] [CrossRef]
- Khosa, A.; Reddi, S.; Saha, R.N. Nanostructured lipid carriers for site-specific drug delivery. Biomed. Pharmacother. 2018, 103, 598–613. [Google Scholar] [CrossRef]
- Pawar, R.; Dawre, S. Solid lipid nanoparticles dispersed topical hydrogel for Co-delivery of adapalene and minocycline for acne treatment. J. Drug Deliv. Sci. Technol. 2023, 80. [Google Scholar] [CrossRef]
- Matussek, F.; Pavinatto, A.; Knospe, P.; Beuermann, S.; Sanfelice, R.C. Controlled Release of Tea Tree Oil from a Chitosan Matrix Containing Gold Nanoparticles. Polymers 2022, 14, 3808. [Google Scholar] [CrossRef] [PubMed]
- Pokharkar, V.B.; Mendiratta, C.; Kyadarkunte, A.Y.; Bhosale, S.H.; A Barhate, G. Skin delivery aspects of benzoyl peroxide-loaded solid lipid nanoparticles for acne treatment. Ther. Deliv. 2014, 5, 635–652. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.; Bansal, K.K.; Verma, A.; Yadav, N.; Thakur, S.; Sudhakar, K.; Rosenholm, J.M. Solid lipid nanoparticles: Emerging colloidal nano drug delivery systems. Pharmaceutics 2018, 10, 191. [Google Scholar] [CrossRef]
- Mehnert, W.; Mäder, K. Solid lipid nanoparticles Production, characterization and applications. Adv. Drug Deliv. Rev. 2001, 47, 165–196. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Potential of Nanoparticles as Permeation Enhancers and Targeted Delivery Options for Skin: Advantages and Disadvantages. Drug Des. Dev. Ther. 2020, ume 14, 3271–3289. [Google Scholar] [CrossRef]
- Bo, R.; Zhan, Y.; Wei, S.; Xu, S.; Huang, Y.; Liu, M.; Li, J. Tea tree oil nanoliposomes: optimization, characterization, and antibacterial activity against Escherichia coli in vitro and in vivo. Poult. Sci. 2023, 102. [Google Scholar] [CrossRef]
- Marques, M.P.; Varela, C.; Mendonça, L.; Cabral, C. Nanotechnology-Based Topical Delivery of Natural Products for the Management of Atopic Dermatitis. Pharmaceutics 2023, 15, 1724. [Google Scholar] [CrossRef]
- Nascimento, T.; Gomes, D.; Simões, R.; Miguel, M.d.G. Tea Tree Oil: Properties and the Therapeutic Approach to Acne—A Review. Antioxidants 2023, 12, 1264. [Google Scholar] [CrossRef]
- Elsewedy, H.S.; Shehata, T.M.; Soliman, W.E. Tea Tree Oil Nanoemulsion-Based Hydrogel Vehicle for Enhancing Topical Delivery of Neomycin. Life 2022, 12, 1011. [Google Scholar] [CrossRef]
- Yingchoncharoen, P.; Kalinowski, D.S.; Richardson, D.R. Lipid-Based Drug Delivery Systems in Cancer Therapy: What Is Available and What Is Yet to Come. Pharmacol. Rev. 2016, 68, 701–787. [Google Scholar] [CrossRef]
- Naseri, N.; Valizadeh, H.; Zakeri-Milani, P. Solid Lipid Nanoparticles and Nanostructured Lipid Carriers: Structure, Preparation and Application. Adv. Pharm. Bull. 2015, 5, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Müller, R.H.; Mäder, K.; Gohla, S. Solid lipid nanoparticles (SLN) for controlled drug delivery--a review of the state of the art. Eur. J. Pharm. Biopharm. 2000, 50, 161–177. [Google Scholar] [CrossRef] [PubMed]
- López, K.L.; Ravasio, A.; González-Aramundiz, J.V.; Zacconi, F.C. Solid Lipid Nanoparticles (SLN) and Nanostructured Lipid Carriers (NLC) Prepared by Microwave and Ultrasound-Assisted Synthesis: Promising Green Strategies for the Nanoworld. Pharmaceutics 2023, 15, 1333. [Google Scholar] [CrossRef] [PubMed]
- Czajkowska-Kośnik, A.; Szekalska, M.; Winnicka, K. Nanostructured lipid carriers: A potential use for skin drug delivery systems. Pharmacol. Rep. 2018, 71, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Musielak, E.; Feliczak-Guzik, A.; Nowak, I. Optimization of the Conditions of Solid Lipid Nanoparticles (SLN) Synthesis. Molecules 2022, 27, 2202. [Google Scholar] [CrossRef]
- Fang, C.-L.; Al-Suwayeh, S.A.; Fang, J.-Y. Nanostructured Lipid Carriers (NLCs) for Drug Delivery and Targeting. Recent Patents Nanotechnol. 2013, 7, 41–55. [Google Scholar] [CrossRef]
- Xing, R.; Mustapha, O.; Ali, T.; Rehman, M.; Zaidi, S.S.; Baseer, A.; Batool, S.; Mukhtiar, M.; Shafique, S.; Malik, M.; et al. Development, Characterization, and Evaluation of SLN-Loaded Thermoresponsive Hydrogel System of Topotecan as Biological Macromolecule for Colorectal Delivery. BioMed Res. Int. 2021, 2021, 9968602. [Google Scholar] [CrossRef]
- Chauhan, I.; Yasir, M.; Verma, M.; Singh, A.P. Nanostructured Lipid Carriers: A Groundbreaking Approach for Transdermal Drug Delivery. Adv. Pharm. Bull. 2020, 10, 150–165. [Google Scholar] [CrossRef]
- Viegas, C.; Patrício, A.B.; Prata, J.M.; Nadhman, A.; Chintamaneni, P.K.; Fonte, P. Solid Lipid Nanoparticles vs. Nanostructured Lipid Carriers: A Comparative Review. Pharmaceutics 2023, 15, 1593. [Google Scholar] [CrossRef]
- Shakeel, F.; Shafiq, S.; Haq, N.; Alanazi, F.K.; A Alsarra, I. Nanoemulsions as potential vehicles for transdermal and dermal delivery of hydrophobic compounds: an overview. Expert Opin. Drug Deliv. 2012, 9, 953–974. [Google Scholar] [CrossRef] [PubMed]
- Gurpret, K.; Singh, S.K. Review of Nanoemulsion Formulation and Characterization Techniques. Indian J. Pharm. Sci. 2018, 80, 781–789. [Google Scholar] [CrossRef]
- Tan, S.F.; Masoumi, H.R.F.; Karjiban, R.A.; Stanslas, J.; Kirby, B.P.; Basri, M.; Bin Basri, H. Ultrasonic emulsification of parenteral valproic acid-loaded nanoemulsion with response surface methodology and evaluation of its stability. Ultrason. Sonochemistry 2016, 29, 299–308. [Google Scholar] [CrossRef]
- Cevc, G.; Vierl, U. Nanotechnology and the transdermal route: A state of the art review and critical appraisal. J. Control. Release 2010, 141, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Hosny, K.M.; Al Nahyah, K.S.; Alhakamy, N.A. Self-Nanoemulsion Loaded with a Combination of Isotretinoin, an Anti-Acne Drug, and Quercetin: Preparation, Optimization, and In Vivo Assessment. Pharmaceutics 2020, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, J.; Ciotti, S.; Baker, J.R. Methods of treating acne using nanoemulsion compositions. WO201702 3751A2, 2017.
- Ridolfi, D.M.; Marcato, P.D.; Justo, G.Z.; Cordi, L.; Machado, D.; Durán, N. Chitosan-solid lipid nanoparticles as carriers for topical delivery of tretinoin. Colloids Surfaces B: Biointerfaces 2012, 93, 36–40. [Google Scholar] [CrossRef]
- Carter, P.; Narasimhan, B.; Wang, Q. Biocompatible nanoparticles and vesicular systems in transdermal drug delivery for various skin diseases. Int. J. Pharm. 2018, 555, 49–62. [Google Scholar] [CrossRef]
- Badilli, U.; Gumustas, M.; Uslu, B.; Ozkan, S.A. Lipid-based nanoparticles for dermal drug delivery. In Organic Materials as Smart Nanocarriers for Drug Delivery; Grumezescu, A.M., Ed.; William Andrew Publishing: 2018; pp. 369–413. [CrossRef]
- Vanic, Z.; Holaeter, A.-M.; Skalko-Basnet, N. (Phospho)lipid-based Nanosystems for Skin Administration. Curr. Pharm. Des. 2015, 21, 4174–4192. [Google Scholar] [CrossRef]
- Raminelli, A.C.P.; Romero, V.; Semreen, M.H.; Leonardi, G.R. Nanotechnological Advances for Cutaneous Release of Tretinoin: An Approach to Minimize Side Effects and Improve Therapeutic Efficacy. Curr. Med. Chem. 2018, 25, 3703–3718. [Google Scholar] [CrossRef]
- Rahman, S.A.; Abdelmalak, N.S.; Badawi, A.; Elbayoumy, T.; Sabry, N.; El Ramly, A. Tretinoin-loaded liposomal formulations: from lab to comparative clinical study in acne patients. Drug Deliv. 2016, 23, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Ge, X.; Wei, M.; He, S.; Yuan, W.-E. Advances of Non-Ionic Surfactant Vesicles (Niosomes) and Their Application in Drug Delivery. Pharmaceutics 2019, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Hamishehkar, H.; Rahimpour, Y.; Kouhsoltani, M. Niosomes as a propitious carrier for topical drug delivery. Expert Opin. Drug Deliv. 2012, 10, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Feng, T.; Wei, Y.; Lee, R.J.; Zhao, L. Liposomal curcumin and its application in cancer. Int. J. Nanomed. 2017, 12, 6027–6044. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, Y.; Lee, R.J.; Xiang, G. Nano Encapsulated Curcumin: And Its Potential for Biomedical Applications. Int. J. Nanomed. 2020, ume 15, 3099–3120. [Google Scholar] [CrossRef]
- Mehrarya, M.; Gharehchelou, B.; Poodeh, S.H.; Jamshidifar, E.; Karimifard, S.; Far, B.F.; Akbarzadeh, I.; Seifalian, A. Niosomal formulation for antibacterial applications. J. Drug Target. 2022, 30, 476–493. [Google Scholar] [CrossRef]
- Alkilani, A.Z.; Abu-Zour, H.; Alshishani, A.; Abu-Huwaij, R.; Basheer, H.A.; Abo-Zour, H. Formulation and Evaluation of Niosomal Alendronate Sodium Encapsulated in Polymeric Microneedles: In Vitro Studies, Stability Study and Cytotoxicity Study. Nanomaterials 2022, 12, 3570. [Google Scholar] [CrossRef]
- Liu, C.-H.; Huang, H.-Y. In Vitro Anti-Propionibacterium Activity by Curcumin Containing Vesicle System. Chem. Pharm. Bull. 2013, 61, 419–425. [Google Scholar] [CrossRef]
- Goyal, G.; Garg, T.; Malik, B.; Chauhan, G.; Rath, G.; Goyal, A.K. Development and characterization of niosomal gel for topical delivery of benzoyl peroxide. Drug Deliv. 2015, 22, 1027–1042. [Google Scholar] [CrossRef]
- Prabhu, P.; Patravale, V. The Upcoming Field of Theranostic Nanomedicine: An Overview. J. Biomed. Nanotechnol. 2012, 8, 859–882. [Google Scholar] [CrossRef]
- Al Sabaa, H.; Mady, F.M.; Hussein, A.K.; Abdel-Wahab, H.M.; Ragaie, M.H. Dapsone in topical niosomes for treatment of acne vulgaris. Afr. J. Pharm. Pharmacol. 2018, 12, 221–230. [Google Scholar] [CrossRef]
- Crucho, C.I.C.; Barros, M.T. Polymeric nanoparticles: A study on the preparation variables and characterization methods. Mater. Sci. Eng. C 2017, 80, 771–784. [Google Scholar] [CrossRef]
- Calzoni, E.; Cesaretti, A.; Polchi, A.; Di Michele, A.; Tancini, B.; Emiliani, C. Biocompatible Polymer Nanoparticles for Drug Delivery Applications in Cancer and Neurodegenerative Disorder Therapies. J. Funct. Biomater. 2019, 10, 4. [Google Scholar] [CrossRef]
- Gagliardi, A.; Giuliano, E.; Venkateswararao, E.; Fresta, M.; Bulotta, S.; Awasthi, V.; Cosco, D. Biodegradable Polymeric Nanoparticles for Drug Delivery to Solid Tumors. Front. Pharmacol. 2021, 12, 601626. [Google Scholar] [CrossRef]
- Sharma, S.; Parveen, R.; Chatterji, B.P. Toxicology of Nanoparticles in Drug Delivery. Curr. Pathobiol. Rep. 2021, 9, 133–144. [Google Scholar] [CrossRef]
- Mikušová, V.; Mikuš, P. Advances in Chitosan-Based Nanoparticles for Drug Delivery. Int. J. Mol. Sci. 2021, 22, 9652. [Google Scholar] [CrossRef]
- Crucho, C.I.C.; Barros, M.T. Polymeric nanoparticles: A study on the preparation variables and characterization methods. Mater. Sci. Eng. C 2017, 80, 771–784. [Google Scholar] [CrossRef]
- Prgomet, I.; Gonçalves, B.; Domínguez-Perles, R.; Pascual-Seva, N.; Barros, A.I.R.N.A. Valorization Challenges to Almond Residues: Phytochemical Composition and Functional Application. Molecules 2017, 22, 1774. [Google Scholar] [CrossRef]
- Hekmatpou, D.; Mehrabi, F.; Rahzani, K.; Aminiyan, A. The Effect of Aloe Vera Clinical Trials on Prevention and Healing of Skin Wound: A Systematic Review. Iran. J. Med Sci. 2019, 44, 1–9. [Google Scholar]
- Saric, S.; Notay, M.; Sivamani, R.K. Green Tea and Other Tea Polyphenols: Effects on Sebum Production and Acne Vulgaris. Antioxidants 2016, 6, 2. [Google Scholar] [CrossRef]
- Huang, L.-L.; Tang, M.; Du, Q.-Q.; Liu, C.-X.; Yan, C.; Yang, J.-L.; Li, Y. The effects and mechanisms of a biosynthetic ginsenoside 3β,12β-Di-O-Glc-PPD on non-small cell lung cancer. OncoTargets Ther. 2019, ume 12, 7375–7385. [Google Scholar] [CrossRef]
- Ghisoni, E.; Imbimbo, M.; Zimmermann, S.; Valabrega, G. Ovarian Cancer Immunotherapy: Turning up the Heat. Int. J. Mol. Sci. 2019, 20, 2927. [Google Scholar] [CrossRef] [PubMed]
- Alzohairy, M.A. Therapeutics Role ofAzadirachta indica(Neem) and Their Active Constituents in Diseases Prevention and Treatment. Evid. Based Complement. Altern. Med. 2016, 2016, 7382506. [Google Scholar] [CrossRef] [PubMed]
- Gupta; Srivastava, J. K.; Shankar, E.; Gupta, S. Chamomile: A herbal medicine of the past with a bright future (Review). Mol. Med. Rep. 2010, 3, 895–901. [Google Scholar] [CrossRef]
- Mori, H.-M.; Kawanami, H.; Kawahata, H.; Aoki, M. Wound healing potential of lavender oil by acceleration of granulation and wound contraction through induction of TGF-β in a rat model. BMC Complement. Altern. Med. 2016, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dawid-Pać, R. Medicinal plants used in treatment of inflammatory skin diseases. Adv. Dermatol. Allergol. 2013, 3, 170–177. [Google Scholar] [CrossRef]
- Puaratanaarunkon, T.; Washrawirul, C.; Chuenboonngarm, N.; Noppakun, N.; Asawanonda, P.; Kumtornrut, C. Efficacy and safety of a facial serum containing snail secretion filtrate, Calendula officinalis, and Glycyrrhiza glaba root extract in the treatment of maskne: A randomized placebo-controlled study. J. Cosmet. Dermatol. 2022, 21, 4470–4478. [Google Scholar] [CrossRef]
- Al-Abduljabbar, A.; Farooq, I. Electrospun Polymer Nanofibers: Processing, Properties, and Applications. Polymers 2022, 15, 65. [Google Scholar] [CrossRef]
- Hong, J.; Yeo, M.; Yang, G.H.; Kim, G. Cell-Electrospinning and Its Application for Tissue Engineering. Int. J. Mol. Sci. 2019, 20, 6208. [Google Scholar] [CrossRef]
- Torres-Martinez, E.J.; Cornejo-Bravo, J.M.; Serrano-Medina, A.; Perez-González, G.L.; Gómez, L.J.V. A Summary of Electrospun Nanofibers as Drug Delivery System: Drugs Loaded and Biopolymers Used as Matrices. Curr. Drug Deliv. 2018, 15, 1360–1374. [Google Scholar] [CrossRef]
- Li, D.; Xia, Y. Electrospinning of Nanofibers: Reinventing the Wheel? Adv. Mater. 2004, 16, 1151–1170. [Google Scholar] [CrossRef]
- Ramakrishna, S.; Fujihara, K.; Teo, W.-E.; Yong, T.; Ma, Z.; Ramaseshan, R. Electrospun nanofibers: solving global issues. Mater. Today 2006, 9, 40–50. [Google Scholar] [CrossRef]
- Hu, X.; Liu, S.; Zhou, G.; Huang, Y.; Xie, Z.; Jing, X. Electrospinning of polymeric nanofibers for drug delivery applications. J. Control. Release 2014, 185, 12–21. [Google Scholar] [CrossRef]
- Li, D.; McCann, J.T.; Xia, Y.; Marquez, M. Electrospinning: A Simple and Versatile Technique for Producing Ceramic Nanofibers and Nanotubes. J. Am. Ceram. Soc. 2006, 89, 1861–1869. [Google Scholar] [CrossRef]
- Ghosal, K.; Chandra, A.; G. , P.; S., S.; Roy, S.; Agatemor, C.; Thomas, S.; Provaznik, I. Electrospinning over Solvent Casting: Tuning of Mechanical Properties of Membranes. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Xue, J.; Wu, T.; Dai, Y.; Xia, Y. Electrospinning and Electrospun Nanofibers: Methods, Materials, and Applications. Chem. Rev. 2019, 119, 5298–5415. [Google Scholar] [CrossRef]
- Hamdy Makhlouf AS. Handbook of, Nanofibers. Handbook of Nanofibers; 2019. [Google Scholar] [CrossRef]
- Bhattarai, R.S.; Bachu, R.D.; Boddu, S.H.S.; Bhaduri, S. Biomedical Applications of Electrospun Nanofibers: Drug and Nanoparticle Delivery. Pharmaceutics 2018, 11, 5. [Google Scholar] [CrossRef]
- Khajavi, R.; Abbasipour, M. Controlling nanofiber morphology by the electrospinning process. In Electrospun Nanofibers; Elsevier Ltd.: Amsterdam, The Netherlands, 2016; pp. 109–123. [Google Scholar] [CrossRef]
- Jiffrin, R.; Razak, S.I.A.; Jamaludin, M.I.; Hamzah, A.S.A.; Mazian, M.A.; Jaya, M.A.T.; Nasrullah, M.Z.; Majrashi, M.; Theyab, A.; Aldarmahi, A.A.; et al. Electrospun Nanofiber Composites for Drug Delivery: A Review on Current Progresses. Polymers 2022, 14, 3725. [Google Scholar] [CrossRef]
- Altay, F.; Okutan, N. Nanofibre Encapsulation of Active Ingredients and their Controlled Release. In: Rai V R, editor. Advances in Food Biotechnology, Chichester, UK: John Wiley & Sons Ltd; 2015, p. 607–16. [CrossRef]
- Munteanu, B.S.; Vasile, C. Encapsulation of Natural Bioactive Compounds by Electrospinning—Applications in Food Storage and Safety. Polymers 2021, 13, 3771. [Google Scholar] [CrossRef]
- Miletić, A.; Pavlić, B.; Ristić, I.; Zeković, Z.; Pilić, B. Encapsulation of Fatty Oils into Electrospun Nanofibers for Cosmetic Products with Antioxidant Activity. Appl. Sci. 2019, 9, 2955. [Google Scholar] [CrossRef]
Figure 3.
Schematic representation of encapsulated nanofibers for the treatment of acne.
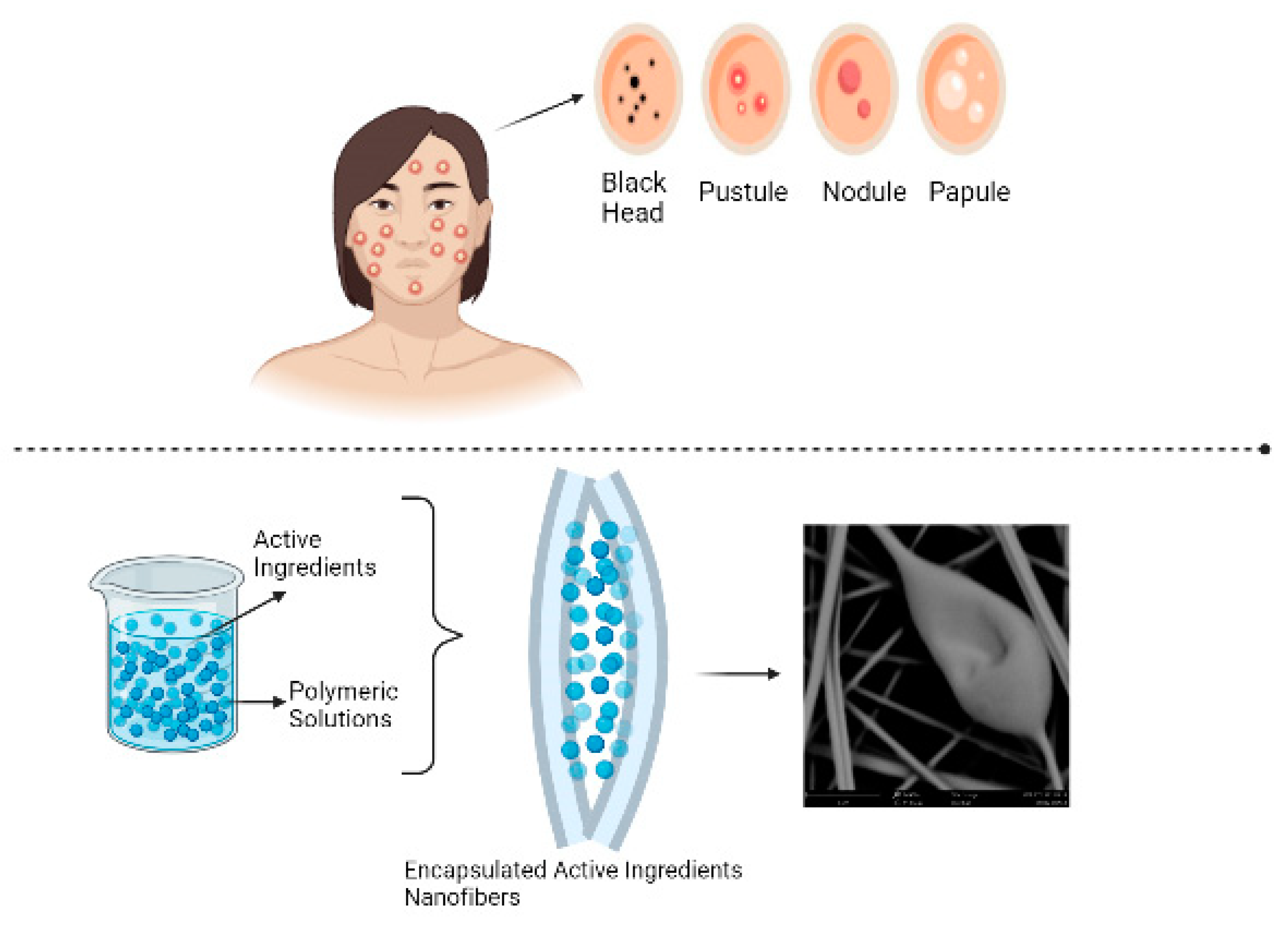

Table 1.
Qualitative Global Scarring grading system for acne [79].
Table 1.
Qualitative Global Scarring grading system for acne [79].
| Acne Grading Scale | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| Disease Description | Macular | Mild | Moderate | Severe |
| Types of Scars | Erythematous, Hypopigmentation, Hyperpigmentation | Atrophic or Hypertrophic Rolling or Papular Scars | Moderate Atrophic or Hypertrophic Scars, Rolling Distensible Scars, Shallow Box Cars | Most Severe Atrophic or Hypertrophic Scars, Deep Boxcar, Ice Pick, Bridges and Tunnels, and Keloid |
| Visibility Distance | Not visible from a 50cm distance | May be covered by makeup and facial hair | Visible at a normal social distance | Obvious at a social distance or greater |
| Flattening by hand | Not applicable | May be flattened manually | Could be flattened manually | Not able to be flattened manually |
Table 2.
The Global Evaluation of Acne scale is a clinical tool for assessing the severity of acne [80].
Table 2.
The Global Evaluation of Acne scale is a clinical tool for assessing the severity of acne [80].
| Grade | Description |
|---|---|
| 0 | Clear, no lesion. Erythema and residual pigmentation may be visible. |
| 1 | Almost clear, with a few scattered open or closed comedones and very few papules. |
| 2 | Mild, with a few open or closed comedones and a few papules and pustules. Less than 50% of the face is affected. |
| 3 | Moderate, with many papules and pustules, many open or closed comedones, and one nodule. More than 50% of the face is affected. |
| 4 | Severe, with many papules and pustules, open or closed comedones, and rare nodules. The entire face is involved. |
| 5 | Very severe, with highly inflammatory acne covering the face and the presence of nodules. |
Table 3.
Overview of common acne treatment methods [85].
Table 3.
Overview of common acne treatment methods [85].
| Treatment Type | Description | Examples |
|---|---|---|
| Topical Retinoids | Vitamin A derivatives that help unclog pores and reduce inflammation. | Tretinoin, Adapalene |
| Topical Antibiotics | Kill bacteria on the skin and reduce inflammation. | Clindamycin, Erythromycin |
| Topical Benzoyl Peroxide | Kills bacteria on the skin and reduces inflammation. | Benzoyl peroxide |
| Oral Antibiotics | Kill bacteria in the body and reduce inflammation. | Tetracycline, Doxycycline |
| Hormonal Therapy | Regulate hormonal imbalances that can contribute to acne. | Oral contraceptives, Spironolactone |
| Isotretinoin | A powerful oral medication that reduces oil production, unclogs pores, and reduces inflammation. | Isotretinoin |
| Chemical Peels | A chemical solution is applied to the skin to remove the top layer of dead skin cells and unclog pores. | Salicylic acid, Glycolic acid |
| Light Therapy | Blue or red light is used to kill bacteria on the skin. | Blue light therapy, Red light therapy |
Table 4.
Advantages and Disadvantages of Solid Lipid Nanoparticles (SLNs) for Drug Delivery.
| Advantages | References | Disadvantages | References |
|---|---|---|---|
| Biocompatible and biodegradable | [145] | Limited drug compatibility with the lipid matrix | [145] |
| High drug loading capacity | [146] | Difficulty achieving homogenous particle size distribution | [146] |
| Controlled drug release | [147] | Risk of lipid oxidation | [147] |
| Improved skin penetration | [146] | Potential cytotoxicity of some lipids | [146] |
| Can be used with a variety of drugs | [145] | Limited research on long-term toxicity | [145] |
Table 5.
Herbal Active Ingredients potential to acne treatment.
| Active Herbal Ingredient | Source | Potential Benefits for Acne | References |
|---|---|---|---|
| Tea tree oil | Leaves of Melaleuca alternifolia | Antibacterial, anti-inflammatory, reduces sebum production | [183] |
| Aloe vera | Leaves of Aloe vera plant | Anti-inflammatory, wound healing, moisturizing | [184] |
| Green tea extract | Leaves of Camellia sinensis plant | Antioxidant, anti-inflammatory, reduces sebum production | [185] |
| Licorice extract | Roots of Glycyrrhiza glabra plant | Anti-inflammatory, antioxidant, antibacterial | [186] |
| Turmeric extract | Roots of Curcuma longa plant | Anti-inflammatory, antibacterial, antioxidant | [187] |
| Neem extract | Leaves of Azadirachta indica tree | Antibacterial, anti-inflammatory, reduces sebum production | [188] |
| Chamomile extract | Flowers of Matricaria chamomilla plant | Anti-inflammatory, wound healing, antibacterial | [189] |
| Lavender oil | Flowers of Lavandula angustifolia plant | Antibacterial, anti-inflammatory, wound healing | [190] |
| Willow bark extract | Bark of Salix alba tree | Anti-inflammatory, antibacterial, reduces sebum production | [191] |
| Calendula extract | Flowers of Calendula officinalis plant | Anti-inflammatory, wound healing, antibacterial | [192] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



