Submitted:
21 July 2023
Posted:
24 July 2023
You are already at the latest version
Abstract
Objective: To evaluate the effect of care bundles on treatment compliance and intestinal barrier function in patients with refractory septic shock in the intensive care units (ICUs). Methods: In this retrospective study, the clinical data of 94 patients with refractory septic shock admitted to our hospital between June 2020 and April 2022 were collected. Patients with routine nursing were included in the routine group, and those with care bundles were assigned to the care bundles group, with 47 cases in each group. Outcome measures included nursing efficiency, treatment compliance, sequential organ failure assessment (SOFA) score, acute physiology and chronic health evaluation (APACHE II) score, intestinal barrier function, inflammation factor level, treatment outcome and complications. Results: Care bundles resulted in significantly higher nursing efficiency and treatment compliance versus routine care (P<0.05). Patients receiving care bundles showed significantly higher SOFA scores and APACHE II scores than those receiving routine care (P<0.05). Intestinal fatty-acid binding protein (I-FABP), diamine oxidase (DAO), lactate, endotoxin, and intestinal dysfunction scores in the care bundles group were significantly lower than those in the conventional group after treatment (P<0.05). Care bundles were associated with significantly lower levels of procalcitonin (PCT) and hypersensitive C-reactive protein (hsCRP), shorter time to symptom relief, ICU treatment time, and duration of mechanical ventilation, and lower 28-d morbidity and mortality versus routine care (P<0.05). Patients in the care bundles group had a significantly lower incidence of complications than those in the routine group (P<0.05). Conclusion: Care bundles effectively enhance treatment compliance, improve intestinal barrier function and treatment outcomes, reduce the inflammatory response, and decrease the risk of SOFA score, APACHE II score, and complications in patients with refractory septic shock.
Keywords:
Care bundles
; ICU
; Refractory septic shock
; Treatment compliance
; Intestinal barrier function
1. Introduction
Refractory septic shock is a systemic inflammatory response syndrome with an incidence of about 9.4% in the intensive care units (ICUs) [1]. Despite abundant in-depth studies in recent years [2], the morbidity and mortality rate of this disease remains at a high level. Refractory septic shock is one of the main causes of death in ICU patients, and the reduction of the risk of death in patients with refractory septic shock remains a challenging clinical issue [3]. Research [4] has shown that conventional symptomatic treatment could mitigate the symptoms of the disease, but no standardized approach to patient care during treatment has been established, leading to a lack of access to efficient care interventions and a slow recovery for most patients. It has been demonstrated [5] that early and correct diagnosis and care are essential to control disease progression. Care bundles are a collection of care interventions that require healthcare professionals to provide safe and efficient care to patients when treatment is performed under unavoidable risks, thereby enhancing the efficiency of disease management [6]. Related research [7], such as the Critical Care Branch of the Chinese Medical Association, also indicated the significance of care bundles in improving the treatment outcome of patients with refractory septic shock. To this end, the current study was performed to evaluate the effect of care bundles on treatment compliance and intestinal barrier function in patients with refractory septic shock in the ICU.
2. Materials and methods
2.1. Participants
In this retrospective study, the clinical data of 94 patients with refractory septic shock admitted to our hospital between June 2020 and April 2022 were collected. Patients with routine nursing were included in the routine group, and those with care bundles were assigned to the care bundles group, with 47 cases in each group.
2.2. Inclusion and exclusion criteria
Inclusion criteria: 1) the patients were diagnosed with refractory septic shock by the relevant clinical test results; 2) with obvious infectious lesions and elevated inflammatory indexes; 3) with complete clinical data of the patients.
Exclusion criteria: 1) with oncological diseases; 2) with a history of severe intestinal diseases or related surgeries; 3) with systemic diseases; 4) with recent (3 months) use of glucocorticoids, immunosuppressants, antibacterial and other drugs; 5) with abnormal liver and kidney functions; 6) with psychiatric diseases or dementia.
2.3. Treatment methods
(1) Patients in both groups were given relevant basic treatment after admission, including anti-infection, cardiac strengthening, blood volume supplementation, improvement of microcirculation, and fluid resuscitation.
(2) Patients in the routine group received routine care including psychological intervention, condition detection, vital sign monitoring, and infection care.
(3) Patients in the care bundles group received care bundles. ① Establishment of a care bundles team: The care bundles team consists of a nurse manager, two physicians, and five nursing staff, and the team members were trained in terms of the purpose, pathways and methods of care bundles. ② Medication guidance: Blood and sputum specimens of patients were collected for testing before the administration of antibiotics, and the corresponding medication regimen was formulated according to the test results [8]. ③Medication care: When pathogen culture and drug sensitivity tests are not performed, nursing staff provided patients with broad-spectrum antibiotics for treatment according to medical prescription. If the patient received vasoactive drugs during treatment, the patient's heart rate and blood pressure were closely observed. Patients with a low heart rate required timely interventions. ④Guidance on oxygen therapy: The changes in vital signs of patients were closely monitored and relevant blood gas indicators were recorded. The patient's oral foreign body was cleaned regularly, and mechanical ventilation was performed when necessary. ⑤ Safety care: Close monitoring of the patient was performed. The patient's infusion limb was fixed to avoid situations such as the detachment of needles [9]. ⑥ Nutritional care: The patient's nasogastric tube was set in advance during the patient's treatment, and the nutrient was injected into the patient through the nasogastric tube. The infusion speed and flow rate were strictly controlled to prevent food backflow and stress caused by cold nutrients [10]. ⑦ Complication care: Prompt replacement of catheters and urine bags was performed to avoid bacterial infections, and timely sputum aspiration was conducted to avoid or prevent pneumonia. ⑧ Psychological care: nursing staff communicated with patients to enhance their treatment self-confidence and effectively relieve their mental stress, thus effectively enhancing treatment compliance [11].
2.4. Outcome measures
(1) Nursing efficiency: Markedly effective: after nursing care, the patient's clinically relevant symptoms were significantly relieved, consciousness returned to normal, and no complications occurred; Effective: after care, the patient's clinically relevant symptoms were relieved, consciousness was restored, and no or minor complications occurred; Ineffective: after care, the patient's clinically relevant symptoms were not relieved or even worsened.
(2) Treatment compliance: Complete compliance: patients were fully cooperative with daily care and medication administration; Good compliance: patients were relatively more cooperative with daily care and medication administration, with the number of times of resistance less than 5; Poor compliance: patients were relatively uncooperative with daily care and medication administration, with frequent resistance.
(3) Sequential organ failure assessment (SOFA) score: The prognosis of patients was assessed before and after care by using the SOFA score, with a total score of 24 points. The higher the score, the worse the prognosis.
(4) Acute physiology and chronic health evaluation (APACHE II) score: Before and after care, the patients' recovery was evaluated by APACHE II score, with a total score of 60 points. Higher scores indicated poorer recovery.
(5) Intestinal barrier function: In the present study, the indicators for assessing the intestinal barrier function of patients included human plasma intestinal fatty acid binding protein (IFABP), plasma magnesium diamine oxide (DAO), lactate, endotoxin, and intestinal dysfunction score. Before and after nursing care, 4 ml of morning fasting venous blood was collected from patients, and the fluid was routinely centrifuged and sent for examination. The levels of IFABP, DAO, lactate, and endotoxin were determined using a double antibody sandwich assay. Before and after care, patients' gastrointestinal function was assessed using the Intestinal Dysfunction Score, a scale with a total score of 18. The higher the score, the worse the gastrointestinal function.
(6) Level of inflammatory indexes: The indexes used to assess the intestinal barrier function of patients in this study included procalcitonin (PCT) and hypersensitive C-reactive protein (hs-CRP). Before and after care, 4 ml of fasting venous blood was collected from patients in the early morning, and the fluid was routinely centrifuged and sent for testing, and the PCT and hs-CRP levels were measured by enzyme-linked immunosorbent assay.
(7) Treatment outcome: The indicators to assess the patient's treatment outcome included time to symptom relief, ICU treatment time, duration of mechanical ventilation, and 28-d morbidity and mortality rate.
(8) Complications: Possible complication conditions during the patient's therapeutic care include multi-organ failure, pulmonary edema, dizziness and headache, nausea and vomiting.
2.5. Statistical analysis
GraphPad Prism 8 was used to plot the graphics, and SPSS22.0 was used for data management and analyses. Measurement data were expressed as mean ± standard deviation (±s) and analyzed using the t-test. Count data were expressed as rates(%) and analyzed using the chi-square test. Statistical difference in the difference was indicated by P<0.05.
3. Results
3.1. Patient characteristics
In the routine group, there were 31 males and 16 females, aged 22-78 (53.47±8.22) years, 22 cases of pulmonary infection, 9 cases of biliary tract infection, 7 cases of abdominal infection, 4 cases of urinary tract infection, and 5 cases of other infections. There were 26 cases of high school and below and 21 cases of junior college and above. In the care bundles group, there were 30 males and 17 females, aged 21-77 (53.52±8.19) years, 19 cases of pulmonary infection, 8 cases of biliary tract infection, 8 cases of abdominal infection, 6 cases of urinary tract infection, and 6 cases of other infections. There were 28 cases of high school and below and 19 cases of junior college and above. The patient characteristics between the two groups were comparable (P>0.05) (Table 1).
3.2. Clinical efficiency
The total efficiency of care for patients in the routine group was 59.6% (28/47), including 11 markedly effective cases, 17 effective cases, and 19 ineffective cases. The total efficiency of patient care in the care bundles group was 80.9% (38/47), including 16 markedly effective cases, 22 effective cases, and 9 ineffective cases. Care bundles resulted in a significantly higher clinical efficiency versus routine care (P<0.05) (Table 2).
3.3. Treatment compliance
The compliance rate of routine group patients was 63.8% (30/47), including 13 cases of complete compliance, 17 cases of good compliance, and 17 cases of poor compliance. The compliance rate of care bundles group patients was 95.7%(45/47), including 22 cases of complete compliance, 23 cases of good compliance, and 2 cases of poor compliance. Treatment compliance was significantly higher in the care bundles group than in the routine group (P<0.05) (Table 3).
3.4. SOFA scores and APACHE II scores
In the routine group, the SOFA scores before and after care were (9.15±2.21, 3.82±1.05) and APACHE II scores were (18.54±3.16, 11.05±2.47). In the care bundles group, the SOFA scores before and after care were (9.11±2.17, 2.72±0.75) and APACHE II scores were (18.49±3.12, 9.11±1.84). Before care, the difference in the SOFA scores and APACHE II scores did not come up to the statistical standard (P>0.05). The SOFA score and APACHE II score were significantly lower in the care bundles group than in the routine group after treatment (P<0.05) (Figure 1).
3.5. Intestinal barrier function
There was no significant difference in the IFABP, DAO, lactate, endotoxin, and intestinal dysfunction scores between the two groups before treatment (P>0.05). Care bundles resulted in significantly lower IFABP, DAO, lactate, endotoxin, and intestinal dysfunction scores versus routine care (P<0.05) (Table 4).
3.6. Inflammatory factor levels
In the routine group, the PCT before and after care was (8.53±0.97, 6.17±1.25) and hsCRP was (29.45±5.79, 26.31±4.97). In the care bundles group, the PCT before and after care was (8.39±0.89, 5.31±1.18) and hsCRP was (29.62±5.82, 22.42±5.46). No significant differences were observed in the PCT and hs-CRP levels between the two groups (P>0.05). The PCT and hsCRP levels were significantly lower in the care bundles group than in the routine group after treatment (P<0.05) (Figure 2).
3.7. Treatment outcomes
The time to symptom relief, time to ICU treatment, time to mechanical ventilation, and 28-d morbidity and mortality rates for patients in the routine group were [11.38±3.92, 12.95±1.97, 14.09±4.53, and 36.2% (17/47)]. The time to symptom relief, time to ICU treatment, time to mechanical ventilation, and 28-d morbidity and mortality rates for patients in the care bundles group were [6.13±1.21, 8.53±1.52, 11.92±3.03, and 19.1% (9/47)]. Care bundles were associated with significantly shorter time to symptom relief, time to ICU treatment, and time to mechanical ventilation, and lower 28-d morbidity and mortality rates versus routine care (P<0.05) (Figure 3).
3.8. Complications
The incidence of complications in the routine group was 21.3% (10/47), including 2 cases of multi-organ failure, 1 case of pulmonary edema, 4 cases of dizziness and headache, and 3 cases of nausea and vomiting. The incidence of complications in the care bundles group was 4.3% (2/47), including 0 cases of multi-organ failure, 0 cases of pulmonary edema, 1 case of dizziness and headache, and 1 case of nausea and vomiting. The incidence of complications in the care bundles group was significantly lower than that in the routine group (P<0.05) (Table 5).
4. Discussion
The onset of refractory septic shock disease increases microcirculatory perfusion obstruction, decreases effective circulation, increases the patient's stress response, and causes a dramatic endocrine imbalance, which seriously threatens the life and health safety of patients [12]. In recent years, the number of deaths due to septic shock disease has been increasing in China. Therefore, clinical attention to the care of such patients should be enhanced to reduce patient stress and risk of death by maximizing the time available for treatment [13].
Care bundles are a series of evidence-based treatment and care interventions applied to patients with acute or refractory clinical conditions to provide further optimization of patient care [14]. The results of previous research [14] have shown that the use of care bundles for patients with refractory septic shock is effective in improving treatment outcomes, which was similar to the results of the present study. It has been reported that [15] patients with refractory septic shock frequently experience a significant decrease in treatment compliance due to pain or negative emotions such as fear. Currently, most clinical nursing staff only follow routine procedures for symptomatic care, and no constructive nursing interventions that are specific to the patient and the disease are effectively adopted [16]. Prior research has also identified the superior nursing efficiency of care bundles versus routine care in the management of multiple diseases [17]. The results of the present study showed that care bundles resulted in significantly higher nursing efficiency and treatment compliance and a lower incidence of complications, suggesting the effectiveness of care bundles in the management of refractory septic shock. A study [18] found that patients with refractory septic shock are usually comorbid with severe circulatory impairment as well as metabolic dysfunctions, and another study [19] confirmed that intestinal dysfunction worsens in patients as their condition deteriorates, which compromises the intestinal barrier function of patients and exacerbates the inflammatory response [20]. In addition, patients receiving care bundles showed significantly lower IFABP, DAO, lactate, endotoxin, and intestinal dysfunction scores versus those with routine care, indicating that care bundles further improve intestinal barrier function and alleviate inflammatory response in patients with refractory septic shock compared to previous clinical routine care. APACHE II is a common index for clinical assessment of chronic organ insufficiency or immunosuppressed status, while the SOFA score is a key index to determine the prognosis of patients, and both indexes are available to assess the risk of the subsequent death of patients [21]. The results of the current study revealed lower SOFA scores and APACHE II scores after care bundles intervention versus routine care, suggesting that care bundles were associated with enhanced patient characteristics and a reduced risk of death.
5. Conclusions
Care bundles effectively enhance treatment compliance, improve intestinal barrier function and treatment outcomes, reduce the inflammatory response, and decrease SOFA scores, APACHE II scores, and the incidence of complications in patients with refractory septic shock.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions
The authors declare that this work was done by the authors named in this article and all liabilities pertaining to claims relating to the content of this article will be borne by them. All authors reviewed the manuscript. All authors have read and approved the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Font, M.D., B. Thyagarajan, and A.K. Khanna, Sepsis and Septic Shock - Basics of diagnosis, pathophysiology and clinical decision making. Med Clin North Am, 2020. 104(4): p. 573-585. [CrossRef]
- Shankar-Hari, M., et al., Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama, 2016. 315(8): p. 775-87. [CrossRef]
- Russell, J.A., B. Rush, and J. Boyd, Pathophysiology of Septic Shock. Crit Care Clin, 2018. 34(1): p. 43-61. [CrossRef]
- Osborn, T.M., Severe Sepsis and Septic Shock Trials (ProCESS, ARISE, ProMISe): What is Optimal Resuscitation? Crit Care Clin, 2017. 33(2): p. 323-344. [CrossRef]
- Thompson, K., B. Venkatesh, and S. Finfer, Sepsis and septic shock: current approaches to management. Intern Med J, 2019. 49(2): p. 160-170. [CrossRef]
- Liu, C.X., et al., Study on clinical nursing pathway to promote the effective implementation of sepsis bundle in septic shock. Eur J Med Res, 2021. 26(1): p. 69. [CrossRef]
- [Consensus on diagnosis and treatment of invasive fungal infection in patients with severe liver disease]. Zhonghua Gan Zang Bing Za Zhi, 2022. 30(2): p. 159-168.
- Arabi, Y.M., et al., Electronic early notification of sepsis in hospitalized ward patients: a study protocol for a stepped-wedge cluster randomized controlled trial. Trials, 2021. 22(1): p. 695. [CrossRef]
- Wang, D., et al., [Visualized analysis of literature on sepsis caused by Gram positive bacteria in SinoMed]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue, 2020. 32(3): p. 294-300.
- Kowalkowski, M., et al., Protocol for a two-arm pragmatic stepped-wedge hybrid effectiveness-implementation trial evaluating Engagement and Collaborative Management to Proactively Advance Sepsis Survivorship (ENCOMPASS). BMC Health Serv Res, 2021. 21(1): p. 544. [CrossRef]
- Tan, D., et al., Patient, provider, and system factors that contribute to health care-associated infection and sepsis development in patients after a traumatic injury: An integrative review. Aust Crit Care, 2021. 34(3): p. 269-277. [CrossRef]
- Chua, W.L., et al., Nurses' knowledge and confidence in recognizing and managing patients with sepsis: A multi-site cross-sectional study. J Adv Nurs, 2022. [CrossRef]
- Amer, Y.S., et al., Quality assessment of clinical practice guidelines for neonatal sepsis using the Appraisal of Guidelines for Research and Evaluation (AGREE) II Instrument: A systematic review of neonatal guidelines. Front Pediatr, 2022. 10: p. 891572. [CrossRef]
- Dunn, H., et al., Cluster Analysis in Nursing Research: An Introduction, Historical Perspective, and Future Directions. West J Nurs Res, 2018. 40(11): p. 1658-1676. [CrossRef]
- Trochet, C., et al., [Septic shock, organisation and nursing care]. Rev Infirm, 2020. 69(260-261): p. 22-24.
- Alp, E., H. Erdem, and J. Rello, Management of septic shock and severe infections in migrants and returning travelers requiring critical care. Eur J Clin Microbiol Infect Dis, 2016. 35(4): p. 527-33. [CrossRef]
- Dalimonte, M.A., J.R. DeGrado, and K.E. Anger, Vasoactive Agents for Adult Septic Shock: An Update and Review. J Pharm Pract, 2020. 33(4): p. 523-532. [CrossRef]
- Bughrara, N., J.L. Diaz-Gomez, and A. Pustavoitau, Perioperative Management of Patients with Sepsis and Septic Shock, Part II: Ultrasound Support for Resuscitation. Anesthesiol Clin, 2020. 38(1): p. 123-134. [CrossRef]
- Berg, D. and H. Gerlach, Recent advances in understanding and managing sepsis. F1000Res, 2018. 7. [CrossRef]
- Patel, J.J., A. Shukla, and D.K. Heyland, Enteral nutrition in septic shock: A pathophysiologic conundrum. JPEN J Parenter Enteral Nutr, 2021. 45(S2): p. 74-78. [CrossRef]
- Gottlieb, M., Early goal-directed therapy versus usual care in the management of septic shock. Cjem, 2017. 19(1): p. 65-67. [CrossRef]
Figure 1.
SOFA scores and APACHE II scores (±s). Note: * indicates P<0.05.
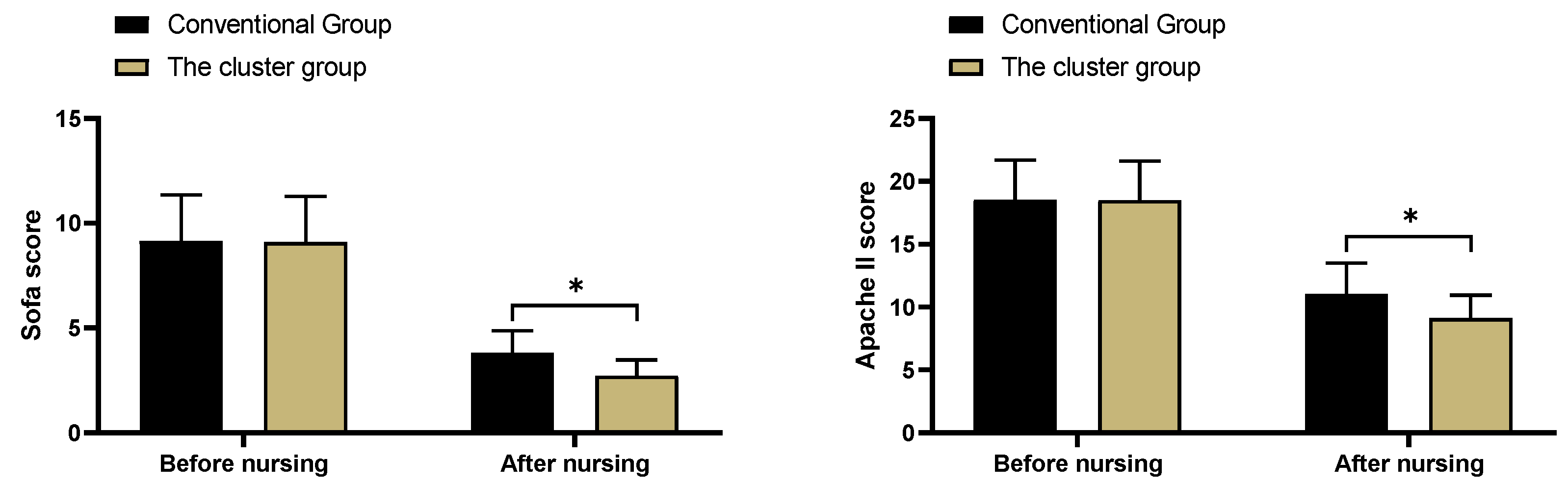
Figure 2.
Inflammatory factor levels (±s). Note: * indicates P<0.05.
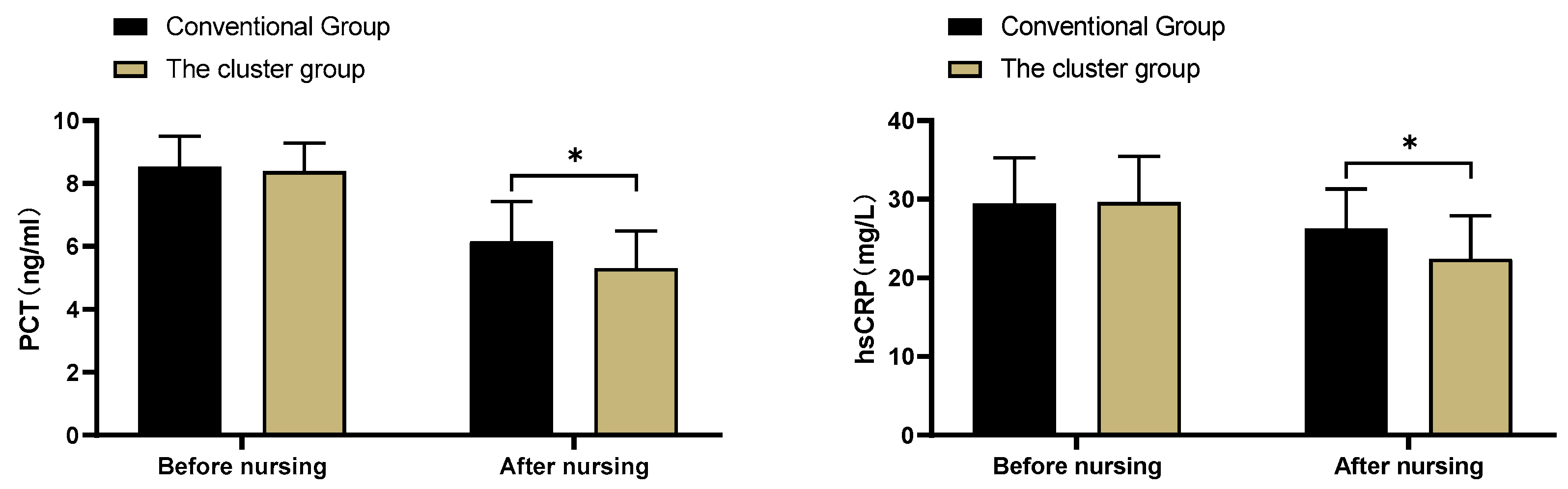
Figure 3.
Treatment outcomes [±s, n(%)]. Note: * indicates P<0.05.
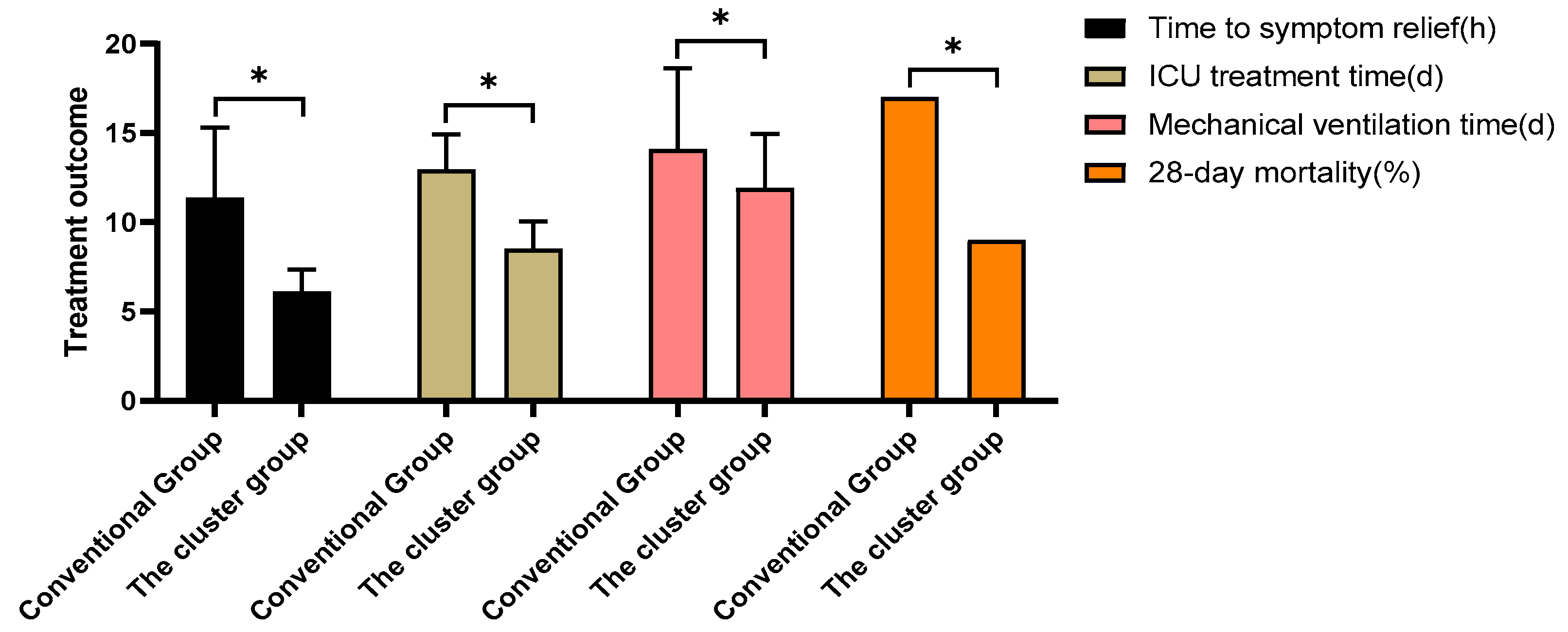

Table 1.
Patient characteristics [±s, n(%)].
| Routine group (n=47) | Care bundles group (n=47) | t/x² | P | |
| Sex | 0.047 | 0.829 | ||
| Male | 31 | 30 | ||
| Female | 16 | 17 | ||
| Age (year) | 22-78 | 21-77 | ||
| Mean age (year) | 53.47±8.22 | 53.52±8.19 | -0.03 | 0.976 |
| Site of infection | ||||
| Lung | 22 | 19 | 0.389 | 0.533 |
| Biliary tract | 9 | 8 | 0.072 | 0.789 |
| Abdominal cavity | 7 | 8 | 0.079 | 0.778 |
| Urinary system | 4 | 6 | 0.448 | 0.503 |
| Other | 5 | 6 | 0.103 | 0.748 |
| Education level | 0.174 | 0.677 | ||
| High school and below | 26 | 28 | ||
| Junior college and above | 21 | 19 |
Table 2.
Clinical efficiency [n(%)].
| Group | N | Markedly effective | Effective | Ineffective | Clinical efficiency (%) |
| Routine group | 47 | 11 | 17 | 19 | 59.6%(28/47) |
| care Bundles group | 47 | 16 | 22 | 9 | 80.9%(38/47) |
| x² | - | - | - | - | 5.087 |
| P | - | - | - | - | 0.024 |
Table 3.
Treatment compliance [n(%)].
| Group | n | Complete compliance | Good compliance | Poor compliance | Compliance (%) |
| Routine group | 47 | 13 | 17 | 17 | 63.8%(30/47) |
| Care bundles group | 47 | 22 | 23 | 2 | 95.7%(45/47) |
| x² | - | - | - | - | 14.842 |
| P | - | - | - | - | <0.001 |
Table 4.
Intestinal barrier function (±s).
| Group | n | IFABP (ng/ml) | DAO (mIU/ml) | Lactic acid (mmol/L) | |||
| Before care | After care | Before care | After care | Before care | After care | ||
| routine group | 47 | 64.28±10.31 | 56.45±10.12 | 9.24±1.35 | 7.25±1.26 | 1.86±0.45 | 1.68±0.33 |
| care bundles group | 47 | 64.33±10.45 | 45.63±9.71 | 9.18±1.41 | 5.44±0.71 | 1.91±0.39 | 1.41±0.31 |
| t | - | -0.023 | 5.289 | 0.211 | 8.58 | -0.576 | 4.088 |
| P | - | 0.982 | <0.001 | 0.833 | <0.001 | 0.566 | <0.001 |
| Group | n | Endotoxin (EU/ml) | Bowel dysfunction score | ||||
| Before care | After care | Before care | After care | ||||
| routine group | 47 | 0.78±0.14 | 0.72±0.13 | 10.42±2.23 | 6.39±1.84 | ||
| care bundles group | 47 | 0.80±0.15 | 0.61±0.09 | 10.39±2.27 | 4.26±1.31 | ||
| t | - | -0.668 | 4.769 | 0.065 | 6.465 | ||
| P | - | 0.506 | <0.001 | 0.948 | <0.001 | ||
Table 5.
Complications [n(%)].
| Routine group(n=47) | Care bundles group(n=47) | x² | P | |
| Multi-Organ Failure | 2 | 0 | - | - |
| Pulmonary edema | 1 | 0 | - | - |
| Dizziness and headache | 4 | 1 | - | - |
| Nausea and vomiting | 3 | 1 | - | - |
| Total incidence (%) | 21.3%(10/47) | 4.3%(2/47) | 6.114 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



