Submitted:
21 July 2023
Posted:
24 July 2023
You are already at the latest version
Abstract
Objective: To study the factors affecting the time of umbilical cord shedding in premature infants.Methods: A total of 151 premature infants who were born in the obstetrics department of a Class III hospital in Hefei from November 2020 to June 2021 were selected as subjects. All premature infants and their families met the complete inclusion criteria. A total of 33 related factors from 3 aspects, including the birth situation of premature infants, the condition of premature infants in hospital and the condition of pregnant mothers, were collected for univariate analysis and multiple Logistic regression analysis. The relevant factors affecting the umbilical cord shedding time of premature infants were screened through the univariate analysis results, and the main factors affecting the umbilical cord shedding time of premature infants were screened through the multiple Logistic regression analysis results.it was found that the weight, gestural age, admission age, whether the premature infants were combined with NRDS, the use of antibiotics, the duration in the warm box, the initial temperature in the warm box, the duration of light therapy, the degree of Apgar for 1 minute, the maternal education level had an effect on the time of umbilical cord shedding of premature infants (P < 0.05). Through Logistic multiple regression analysis, it was screened that the duration of premature infants in the incubator was the main factor affecting the umbilical cord shedding time of premature infants (P < 0.05).Conclusion: Factors such as premature infants' weight, gestural age, admission age, whether they are combined with NRDS, antibiotic use, duration in the incubator, initial temperature in the incubator, duration of phototherapy, Apgar level of 1 minute, and maternal education level will affect the umbilical cord shedding time of premature infants. Among them, duration in the incubator is the main factor affecting the umbilical cord shedding time of premature infants.
Keywords:
premature infants
; umbilical cord shedding time
; influencing factors
1. Preface
Neonates with gestational age less than 37 weeks (< 260 days) are clinically called pre-term infant [1]. Among them, those with gestational age of 34~36+6 weeks are late preterm infants, those with gestational age of 32~33+6 weeks are middle preterm infants, those with gestational age of 28~31+6 weeks are very preterm infants, and those with gestational age < 28 weeks are ultra-preterm infants [2]. The shorter the gestational age, the smaller the weight, the shorter the length. Clinically, those with birth weight < 2500g are called low birth weight infants, those with birth weight < 1500g are called very low birth weight infants, and those with birth weight < 1000g are called ultra-low birth weight infants [3].
According to the systematic assessment [4] published by the World Health Organization in 2019, the incidence of premature infants was 10.6% globally on average and 6.9% in China. With the continuous progress of perinatal medicine and the improvement of treatment of newborn babies year by year, the birth rate and survival rate of premature babies have gradually improved [5]. As premature infants have delicate skin, weak barrier function, incomplete humoral and cellular immune function, lower IgG and complement levels than full-term newborns, they are prone to various infections. Relevant studies [6] have confirmed that the younger the gestational age and lower the weight of preterm fetuses, the higher the risk of complications of various serious infections, which may even endanger the life of the fetus.
The umbilical cord is the link between the fetus and the mother for oxygen and material exchange. When the newborn is cut off and ligation, the remaining part of the umbilical cord will form ischemic necrosis, liquefaction, drying and even fall off [7]. The umbilical cord of a full-term newborn will fall off 3 to 7 days after ligature, but the umbilical blood tube in the newborn can only be completely closed after 3 to 4 weeks. Therefore, the umbilical cord is one of the important ways to cause neonatal infection [8]. Omphalitis is a common infectious disease in the neonatal period, which is caused by the inflammatory reaction caused by improper umbilical cord care or infection after the birth of the newborn. The clinical manifestations are reswelling of the umbilical ring and the presence of small granulation surface in the umbilical depression, or purulent secretions and pus in the umbilical cord stump. The common pathogenic bacteria include Staphylococcus aureus, streptococcus hemolytic, Escherichia coli, etc. The occurrence of this disease can seriously endanger the health of newborns [9]. As the body resistance of premature infants is weaker than that of full-term newborns, the risk of umbilical infection of premature infants is higher, and even life-threatening in severe cases [10]. Up to now, there are a lot of clinical studies on the time and influencing factors of cord shedding in full-term newborns, but there is no relatively clear cut-off time for cord shedding in premature infants. Therefore, this study conducted a study on the timing and influencing factors of umbilical cord shedding in premature infants, and the report is as follows.
2. Objects and methods
2.1. Research object
A total of 151 premature infants born in the obstetrics department of a Class III hospital in Hefei and admitted to the neonatal department of the hospital from November 2020 to June 2021 were selected as the research objects. Inclusion criteria: ① gestational age < 37 weeks, length of hospital stay > 48 hours; (2) The parents of premature infants have normal cognitive function and can understand the explanations related to the attention of medical staff on neonatal umbilical care; (3) Parents of premature infants voluntarily participated in this study and were willing to cooperate with the institute.
2.2. Methods
2.2.1. General investigation
A total of 33 related factors were collected from 3 aspects: the birth situation of premature infants, the condition of premature infants in hospital and the condition of pregnant mothers. ① Birth status of premature infants: gender, birth weight, gestational age, age at admission, location of umbilical cord shedding, parity, whether NRDS are combined, whether they are test-tube babies. ② Conditions of premature infants in hospital: whether oxygen was used and how it was used, whether antibiotics were used and how long it was used, time in warm tank, temperature in tank, final temperature, duration of phototherapy, white blood cell level on admission, CRP level on admission, Apgar level of 1 minute and Apgar level of 5 minutes. (3) Maternal status: maternal age, BMI grade, education level, family residence, work nature, method of delivery, gestational diabetes mellitus, gestational hypertension, placenta previa, premature rupture of membranes, gestational infection, other diseases, pregnancy with arrhythmia, hypothyroidism, history of cesarean section, etc. The position of umbilical ligature of premature infants was 0.5-1.0cm away from the umbilical wheel, without delayed umbilical ligature.
2.2.2. Management in hospital umbilical department
Relevant medical staff shall be responsible for checking the umbilical cord of premature infants every day and accurately recording the time of umbilical cord shedding; For premature infants with umbilical cords still attached when discharged from hospital, professional nursing staff should educate their families about relevant knowledge. The specific measures of umbilical department management in the hospital are as follows: ① Management of ward environment and articles: relevant personnel should set the ward environment temperature at 24~26℃ and humidity at 45~55%. In the hospital room, relevant personnel are required to use the air disinfector for disinfection at least 2 times a day for 2 hours each time; Ventilate at least twice a day for 30 minutes each time. For cotton and cloth items used by premature infants, it is required to use high-temperature disinfection after cleaning; For disposable goods and disinfectants and other daily use items should be strictly in accordance with the standards for use and treatment. (2) Warm box management: For children with warm box needs, our hospital unified use of Ningbo David warm box, model is YP-90, the relative humidity of the warm box is set at 55~65%, the sterilization water for injection in the warm box is guaranteed to be replaced daily, the inside and outside of the warm box wiping disinfection is guaranteed to be carried out daily, and ensure that the weekly replacement and thorough disinfection of the warm box, and the replacement of the warm box shade. (3) Umbilical cord management: According to WHO [11], in the case of strictly aseptic operation of umbilical cord amputation, routine disinfection of the broken umbilical cord of infants and the surrounding skin should not be carried out, the umbilical cord stump of infants should be exposed, the umbilical cord stump should not be bandaged, and the umbilical cord stump should only be kept clean and dry. Premature infants admitted to hospital at birth should have their umbilical cord removed immediately, and for small babies, the diaper should be reversed and the umbilical cord stump left exposed.The umbilical cord of premature infants should not be stained with water. If it is stained with water, relevant personnel should use sterile cotton swabs to dip and dry it in time. Before and after the umbilical cord falls off, the umbilical cord appears ooze blood, ooze liquid infant, relevant personnel need to give timely umbilical cord care, umbilical cord care specific measures are: use 3% hydrogen peroxide to clean the umbilical fossa and tissue around the umbilical cord, then use 0.5% andofol for umbilical fossa disinfection, until the umbilical fossa clean without ooze. When the infant umbilical part is contaminated by feces, urine, etc., the relevant personnel need to clean and disinfect it in time. (4) Personnel management: In this study, obstetrical and neonatal medical staff involved in the management of premature infants' umbilical departments were uniformly trained by our hospital for umbilical department management, and homogenized umbilical department management was given. (5) Premature infants are admitted to the neonatology department after discharge from obstetrics department. During the period of obstetrics and after admission to the neonatology department, the umbilical department of premature infants in hospital should be managed according to the management methods.
2.2.3. Follow-up
For premature infants whose umbilical cord has not fallen off at the time of discharge, the relevant medical staff should follow up the infants daily until the umbilical cord has fallen off. Upon discharge, professional nursing staff should give standardized umbilical cord management education to children's families: (1) Nursing staff for premature infants should be relatively fixed and cannot be changed frequently; ② The feeding of premature infants after discharge should follow the principles of safety, health and adequate nutrition. (3) Clearly inform the family members that the umbilical cord of premature infants should not be wrapped, avoid pulling, and the umbilical cord of infants should be cleaned and disinfected in time when it is contaminated; (4) Family members should be told to strictly wash hands and disinfect the family members who may come into contact with premature infants; ⑤ Inform the nursing staff that the clothes, towels, blankets, shoes and socks used by premature infants should be made of cotton and soft as far as possible, and should be exposed to the sun regularly to remove bacteria. Milk utensils should be boiled and disinfected before each use.
2.3. Observation Indicators
In this study, the self-made scale was used to analyze the time of premature umbilical cord shedding and its related factors.
2.4. Statistical Methods
Epidata 3.1 software was used for double entry of questionnaires, and SPSS 24.0 software was used for statistical processing. Qualitative data were described by case number and component ratio, and Chi-square test was used for comparison between groups. Quantitative data conforming to normal distribution were described by mean and standard deviation, while those not conforming to normal distribution were described by median and quartile spacing, and rank sum test was used for comparison between groups. Logistic regression analysis was used to determine the main influencing factors of the time of umbilical cord shedding in premature infants. P < 0.05 was considered statistically significant.
3. Results
3.1. Single factor analysis
In this study, among the 151 premature infants, 4 cases had umbilical cord shedding time less than 7 days, accounting for 2.65%. 75 cases (49.67%) lost their umbilical cord 7-14 days; There were 72 cases with umbilical cord shedding time > 14 days, accounting for 47.68%. Univariate analysis showed that the weight, gestural age, admission age, whether the premature infants were combined with NRDS, the use of antibiotics, the duration in the warm box, the initial temperature in the warm box, the duration of phototherapy, the degree of Apgar for 1 minute, and the maternal education level had an effect on the time of umbilical cord shedding of premature infants (P < 0.05). Gender of premature infant, location of umbilical cord loss, parity, whether it was IVF, whether oxygen was used and how oxygen was used, final temperature of warming tank, white blood cell level at admission, CRP level at admission, Apgar 5 min degree, maternal age, BMI grade, family residence, job type, delivery mode, gestational diabetes mellitus, gestational hypertension, placenta previa, premature rupture of membranes, gestational infection, other diseases, pregnancy complicated with arrhythmia, hypothyroidism and cesarean section history had no effect on the time of umbilical cord loss of premature infants (P > 0.05). See Table 1 for details.
3.2. Multiple Logistic regression analysis of factors affecting the time of premature infants' umbilical shedding
Statistically significant indicators in the univariate analysis are taken as independent variables, and the assignment of independent variables is shown in Table 2. Through Logistic multiple regression analysis, it was screened that the duration of premature infants in the incubator was the main factor affecting the umbilical cord shedding time of premature infants (P < 0.05). See Table 3 and Figure 1 for details.
4. Discuss
The umbilical cord is a tubular structure connecting the fetus and placenta in mammals, which is composed of two arteries and a vein [12]. The umbilical cord plays a variety of roles. It not only provides oxygen and nutrients to the fetus and excretes waste, but also acts as an active toy for the fetus. The fetus often moves around in the mother, and the umbilical cord is the only thing available for the fetus [13]. When a newborn is born, the umbilical cord will spontaneously fall off. Under normal circumstances, most of the residual umbilical cord of a newborn will fall off around 3-7 days, but there are also many newborns whose residual umbilical cord will fall off for more than 10 days or even more, and it is rare that some fetuses have delayed falling off for more than 30 days [14]. The appearance of the newborn umbilical cord is turbid white, and the blood vessels are composed of Wharton glue. After birth, the umbilical cord is ligated, the water in Wharton glue is lost, and the stump of the umbilical cord is dried and falls off. After healing, the umbilical fossae is formed [15]. Relevant studies [16] point out that delayed shedding of neonatal umbilical stump will bring great mental and psychological burden to mothers and their families, and at the same time, it will also bury hidden dangers for neonatal umbilical cord infection. For example, the umbilical stump of infants does not fall off for a long time. As an open wound, umbilical stump is easy to be invaded and regenerated by bacteria, causing local or even systemic infection of infants. In severe cases, infants can be critically born. Premature infants are live born with gestational age less than 37 weeks. Due to low gestational age, low body weight, thinner cortex, less subcutaneous fat and other reasons, premature infants are at higher risk of umbilical infection [17]. Previous clinical studies [18,19] have clarified the time and influencing factors of cord shedding in full-term newborns, but there are still no clinical reports on the time and influencing factors of cord shedding in premature infants. It is of great significance to identify the time and influencing factors of umbilical cord shedding in premature infants to prevent adverse events such as umbilical cord infection and improve the prognosis of premature infants. Based on this, 151 premature infants were selected as research objects in this study, aiming to study the related factors affecting the time of umbilical cord shedding in premature infants.
Univariate analysis results in this study showed that the weight, gestational age, admission age, whether the premature infants were combined with NRDS, antibiotic use, length in the warm box, initial temperature in the warm box, duration of phototherapy, Apgar degree of 1 minute, maternal education level had an impact on the umbilical cord shedding time of premature infants (P < 0.05). The above single factors affecting the umbilical shedding time of premature infants were taken as independent variables and assigned into multiple Logistic regression analysis. It was found that the duration of premature infants in the incubator was the main factor affecting the umbilical shedding time of premature infants (P < 0.05). Due to the immature body temperature regulation ability of premature infants, most newborn preterm infants will have hypothermia within a few hours after birth, which is easy to lead to hypoglycemia, metabolic acidosis and other conditions in newborns. In severe cases, it can even lead to intracranial hemorrhage and other critical conditions in newborns, which seriously threatens the life safety of premature infants [20]. Therefore, newborn preterm infants are often placed in neonatal warm box to keep warm in clinical practice. The warm box can provide suitable temperature and humidity for premature infants and an extra-uterine environment similar to the mother's uterus, so as to help premature infants reduce the discomfort caused by premature birth and hypothermia as much as possible. Meanwhile, the warm box is also an important instrument for critically ill newborn transport [21]. The initial temperature of the warm box is set according to the gestational age, weight and age of premature infants, etc. The warm box will also monitor the temperature changes of premature infants in real time and make dynamic feedback adjustment in time [22]. The relative humidity of the warm box of premature infants is usually set at 55%-65%, which is significantly higher than the daily ambient humidity value. Studies [23] have pointed out that keeping the neonatal umbilical cord clean and dry on a daily basis can help accelerate the shedding time of the neonatal umbilical cord. However, in this study, premature infants have to be temporarily placed in the incubator due to their low gestational age and weight, and the relative humidity in the incubator is significantly higher than the ambient humidity outside the incubator, which is obviously not conducive to the premature umbilical cord shedding as soon as possible. Scholar Gowa [24] et al. also pointed out that if the neonatal warm box is too humid, aquatic bacteria will breed rapidly, thus endangering the health of infants. Therefore, in the use of newborn premature infants warm box, relevant personnel should strictly carry out aseptic treatment, and strengthen the awareness of disinfection and isolation of nursing staff, so as to reduce the risk of bacterial infection of newborn premature infants. At the same time, strict control should also be carried out on whether to use the warm box and how long to use the warm box according to the physical conditions of premature infants, so as to reduce the risk of delayed loss of stump umbilical cord of newborn premature infants. Umbilical cord infection is an important precursor of neonatal sepsis, and sepsis is an important independent risk factor for neonatal death [25]. Relevant studies [26] have shown that the clinical fatality rate of sepsis ranges from 0.0 to 14.4%. Therefore, it is very necessary to avoid delayed umbilical cord shedding in neonatal preterm infants. However, due to the limitations of time, operating space and the number of included samples, this study did not make a comparative analysis of the specific situation of newborn premature infants suffering from bacterial infection. In future studies, we will continue to expand the research scale and add more samples for further exploration, modification and improvement.
5. Conclusion
Factors such as premature infants' weight, gestural age, admission age, whether they are combined with NRDS, antibiotic use, duration in the incubator, initial temperature in the incubator, duration of phototherapy, Apgar level of 1 minute, and maternal education level will affect the umbilical cord shedding time of premature infants. Among them, duration in the incubator is the main factor affecting the umbilical cord shedding time of premature infants.
References
- Carter, B.S. , How Do We Regard the Preemie at the Margins of Viability? J Pediatr, 2017, 188, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Reis, Z.S.N. , et al. , Prematurity detection evaluating interaction between the skin of the newborn and light: proto-col for the preemie-test multicentre clinical trial in Brazilian hospitals to validate a new medical device. BMJ Open, 2019, 9, e027442. [Google Scholar]
- Knorr, A.; Giambanco, D.; Staude, M.V.; Germain, M.; Porter, C.; Serino, E.; Gauvreau, K.; DeGrazia, M. Feasibility and Safety of the Preemie Orthotic Device to Manage Deformational Plagiocephaly in Extremely Low Birth Weight Infants. Adv. Neonatal Care 2019, 19, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Perumal, N. , et al. , Implications for quantifying early life growth trajectories of term-born infants using INTER-GROWTH-21st newborn size standards at birth in conjunction with World Health Organization child growth standards in the postnatal period. Paediatr Perinat Epidemiol, 2022, 36, 839–850. [Google Scholar]
- Lee, E.; Schofield, D.; Owens, C.E.; Oei, J.-L. An economic analysis of the cost of survival of micro preemies: A systematic review. Semin. Fetal Neonatal Med. 2022, 27, 101336. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.; Benitz, W. ; COMMITTEE ON FETUS AND NEWBORN Umbilical Cord Care in the Newborn Infant. Pediatrics 2016, 138, e20162149. [Google Scholar] [CrossRef] [PubMed]
- Leante Castellanos, J.L. , et al. , [Recommendations for the care of the umbilical cord in the newborn]. An Pediatr (Engl Ed), 2019, 90, 401.e1–401e5. [Google Scholar]
- Shang, Y. and Y. Sun, Comparison of the effectiveness of different umbilical cord care in infants: A protocol for systematic review and network meta-analysis. Medicine (Baltimore), 2019, 98, e14440. [Google Scholar]
- Painter, K., S. Anand, and K. Philip, Omphalitis, in StatPearls. 2022, StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL).
- Kaplan, R.L.; Cruz, A.T.; Freedman, S.B.; Smith, K.; Freeman, J.; Lane, R.D.; Michelson, K.A.; Marble, R.D.; Middelberg, L.K.; Bergmann, K.R.; et al. Omphalitis and Concurrent Serious Bacterial Infection. PEDIATRICS 2022, 149. [Google Scholar] [CrossRef]
- de Rooy, L. and A. Johns, Management of the vulnerable baby on the postnatal ward and transitional care unit. Early Hum Dev, 2010, 86, p. 281–5. [Google Scholar]
- Rabe, H.; Diaz-Rossello, J.L.; Duley, L.; Dowswell, T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst. Rev. 2012, CD003248. [Google Scholar] [CrossRef]
- Draiko, C.V.; McKague, K.; Maturu, J.D.; Joyce, S. The effect of umbilical cord cleansing with chlorhexidine gel on neonatal mortality among the community births in South Sudan: a quasi-experimental study. Pan Afr. Med J. 2021, 38. [Google Scholar] [CrossRef]
- El-Naggar, W.; Afifi, J.; Dorling, J.; Bodani, J.; Cieslak, Z.; Canning, R.; Ye, X.Y.; Crane, J.; Lee, S.K.; Shah, P.S. A Comparison of Strategies for Managing the Umbilical Cord at Birth in Preterm Infants. J. Pediatr. 2020, 225, 58–64e4. [Google Scholar] [CrossRef]
- Wei, F.; Kong, D.; Li, T.; Li, A.; Tan, Y.; Fang, J.; Zhuang, X.; Lai, C.; Xu, W.; Dong, H.; et al. Efficacy and safety of umbilical cord mesenchymal stem cells for the treatment of patients with COVID-19. Clinics 2021, 76, e2604. [Google Scholar] [CrossRef]
- Seidler, A.L.; Gyte, G.M.; Rabe, H.; Díaz-Rossello, J.L.; Duley, L.; Aziz, K.; Costa-Nobre, D.T.; Davis, P.G.; Schmölzer, G.M.; Ovelman, C.; et al. Umbilical Cord Management for Newborns <34 Weeks' Gestation: A Meta-analysis. PEDIATRICS 2021, 147. [Google Scholar] [CrossRef]
- Riskin, A. and D. Bader, [Premature infant's nutrition--feeding strategies]. Harefuah, 2004, 143, 60–6, 84, 83. [Google Scholar]
- Nosan, G. and D. Paro-Panjan, Umbilical cord care: national survey, literature review and recommendations. J Matern Fetal Neonatal Med, 2017, 30, 1655–1658. [Google Scholar]
- Mlodawski, J.; Mlodawska, M.; Przybysz, N.; Bielak, A.; Detka, K.; Pasiarski, M.; Rokita, W. Collection of umbilical cord blood and the risk of complications in postpartum women after natural labour in the context of the possibility of umbilical cord stem cells usage in clinical practice. Ginekol. Polska 2021, 92, 205–209. [Google Scholar] [CrossRef]
- Ashrafi, A.H.; Levy, V.Y. Management strategies for the preemie ductus. Curr. Opin. Cardiol. 2019, 34, 41–45. [Google Scholar] [CrossRef]
- Couper, J. , Micro-preemie Parents' Perceptions of Trauma-Informed Developmental Neuroprotective Care and Nursing Support. Adv Neonatal Care, 2022, 22, 422–431. [Google Scholar] [CrossRef]
- Fraguela, A.; Matlalcuatzi, F.D.; Ramos. M. Mathematical modelling of thermoregulation processes for premature infants in closed convectively heated incubators. Comput. Biol. Med. 2015, 57, 159–172. [Google Scholar] [CrossRef]
- Glass, L. and A. Valdez, Preterm Infant Incubator Humidity Levels: A Systematic Review. Adv Neonatal Care, 2021, 21, 297–307. [Google Scholar]
- Gowa, M.A.; Rakhia, A.; Bozdar, M.H.; Noonari, M.; Raza, S.J. A Quasi Experimental study to Compare Thermo-regulator blanket with conventional method (incubator) for temperature regulations in preterm, Low Birth weight neonates landing at Emergency department of a tertiary care pediatric facility. J. Pak. Med Assoc. 2022, 72, 1044–1047. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.; Greenhalgh, M.; McGuire, W. Early planned removal of umbilical venous catheters to prevent infection in newborn infants. 2016. [Google Scholar] [CrossRef]
- Sobczak, A. , et al. , Umbilical catheters as vectors for generalized bacterial infection in premature infants regard-less of antibiotic use. J Med Microbiol, 2019, 68, 1306–1313. [Google Scholar]
Figure 1.
Forest map of multiple Logistic regression analysis of factors affecting the timing of premature omphalus shedding.
Figure 1.
Forest map of multiple Logistic regression analysis of factors affecting the timing of premature omphalus shedding.
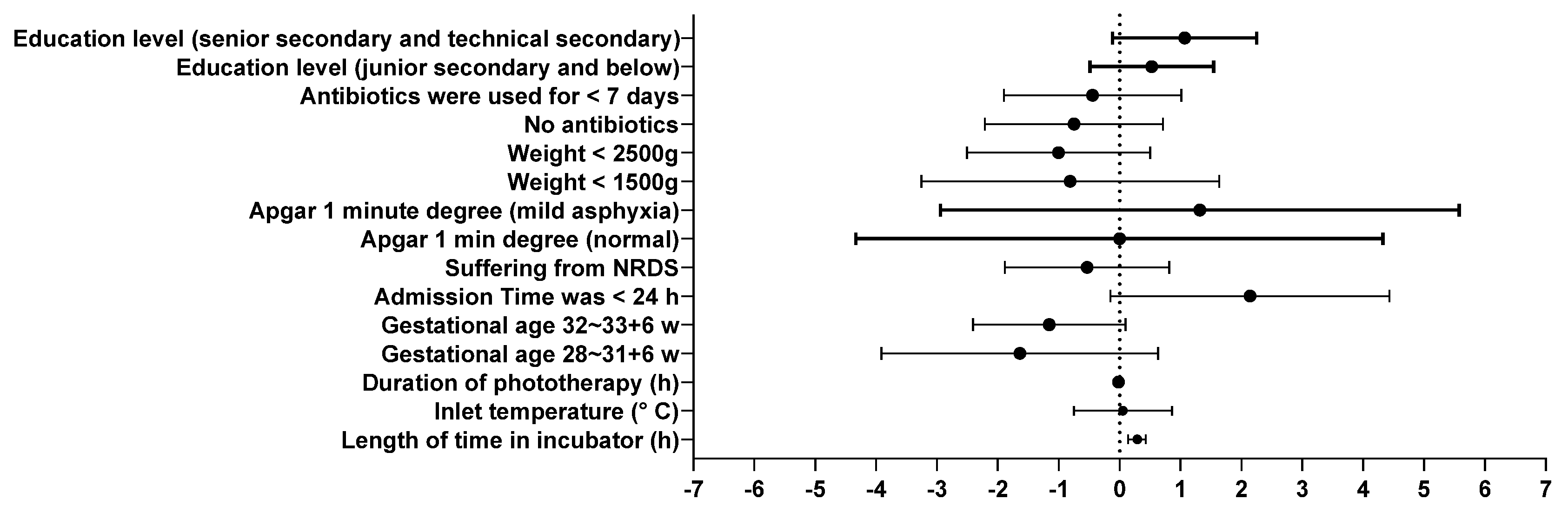

Table 1.
Univariate analysis on the time of umbilical cord shedding in premature infants (n=151).
| General Information | The number of cases(n) | Shedding time(d,n) | X2/H value | P value | ||
|---|---|---|---|---|---|---|
| <7d | 7~14d | >14d | ||||
| gender | 0.813 | 0.666 | ||||
| male | 72 | 2 | 33 | 37 | ||
| female | 79 | 2 | 42 | 35 | ||
| Preterm weight | 13.069 | 0.042 | ||||
| <1000g | 5 | 0 | 0 | 5 | ||
| <1500g | 31 | 0 | 11 | 20 | ||
| <2500g | 94 | 4 | 51 | 39 | ||
| ≥2500g | 21 | 0 | 13 | 8 | ||
| Gestational age | 15.993 | 0.014 | ||||
| <28w | 5 | 0 | 0 | 5 | ||
| 28~31+6w | 29 | 0 | 12 | 17 | ||
| 32~33+6w | 42 | 0 | 18 | 24 | ||
| 34~36+6w | 75 | 4 | 45 | 26 | ||
| Length of admission (age) | 9.040 | 0.011 | ||||
| <24h | 145 | 3 | 70 | 72 | ||
| ≥24h | 6 | 1 | 5 | 0 | ||
| Where the umbilical cord came off | 3.990 | 0.136 | ||||
| The court | 82 | 4 | 42 | 36 | ||
| Outside the court | 69 | 0 | 33 | 36 | ||
| Child time | 4.228 | 0.121 | ||||
| singletons | 73 | 2 | 30 | 41 | ||
| Twins and above | 78 | 2 | 45 | 31 | ||
| Whether you have NRDS | 14.651 | 0.001 | ||||
| There are | 45 | 0 | 13 | 32 | ||
| There is no | 106 | 4 | 62 | 40 | ||
| Whether it is in vitro baby | 0.062 | 0.969 | ||||
| There are | 75 | 2 | 38 | 35 | ||
| There is no | 76 | 2 | 37 | 37 | ||
| Oxygen absorption mode | 10.771 | 0.096 | ||||
| There is no | 62 | 4 | 36 | 22 | ||
| Oxygen in box | 47 | 0 | 20 | 27 | ||
| Non-invasive ventilator | 39 | 0 | 18 | 21 | ||
| Invasive ventilator | 3 | 0 | 1 | 2 | ||
| Whether to use antibiotics | 25.040 | 0.000 | ||||
| no | 82 | 4 | 52 | 26 | ||
| Usage time <7d | 31 | 0 | 15 | 16 | ||
| Use time ≧7d | 38 | 0 | 8 | 30 | ||
| Time in the warm tank | 151 | 4 | 75 | 72 | 55.752 | 0.000 |
| Inlet temperature | 151 | 4 | 70 | 72 | 14.138 | 0.001 |
| Final temperature | 151 | 4 | 70 | 72 | 2.691 | 0.260 |
| Phototherapy duration | 151 | 4 | 75 | 72 | 11.162 | 0.004 |
| Admitted leukocyte | 151 | 4 | 75 | 72 | 1.703 | 0.427 |
| Hospitalized CRP | 151 | 4 | 75 | 72 | 2.131 | 0.345 |
| Apgar1 minute degree | 16.421 | 0.003 | ||||
| normal | 116 | 4 | 67 | 45 | ||
| Mild asphyxia | 29 | 0 | 6 | 23 | ||
| Severe asphyxia | 6 | 0 | 2 | 4 | ||
| Apgar5 minutes degree | 2.648 | 0.618 | ||||
| normal | 141 | 4 | 72 | 65 | ||
| Mild asphyxia | 9 | 0 | 3 | 6 | ||
| Severe asphyxia | 1 | 0 | 0 | 1 | ||
| Maternal age | 6.414 | 0.378 | ||||
| 20~30 | 52 | 1 | 21 | 30 | ||
| 30~40 | 94 | 3 | 53 | 38 | ||
| 40~50 | 4 | 0 | 1 | 3 | ||
| ≥50 | 1 | 0 | 0 | 1 | ||
| Maternal BMI rating | 4.439 | 0.350 | ||||
| Normal weight | 26 | 0 | 12 | 14 | ||
| overweight | 88 | 4 | 41 | 43 | ||
| obesity | 37 | 0 | 22 | 15 | ||
| Level of education | 10.336 | 0.035 | ||||
| Junior high school and below | 60 | 2 | 26 | 32 | ||
| High school and technical secondary school | 37 | 0 | 14 | 23 | ||
| College degree or above | 54 | 2 | 35 | 17 | ||
| Family residence | 0.619 | 0.734 | ||||
| Cities and towns | 121 | 3 | 62 | 56 | ||
| rural | 30 | 1 | 13 | 16 | ||
| Nature of Work | 6.127 | 0.190 | ||||
| brain-based | 59 | 2 | 35 | 22 | ||
| Physical strength is dominant | 21 | 0 | 7 | 14 | ||
| unemployed | 71 | 2 | 33 | 36 | ||
| Mode of delivery | 2.357 | 0.308 | ||||
| Cesarean section | 121 | 2 | 61 | 58 | ||
| Natural birth | 30 | 2 | 14 | 14 | ||
| Whether gestational diabetes is present | 4.473 | 0.107 | ||||
| There are | 52 | 1 | 32 | 19 | ||
| There is no | 99 | 3 | 43 | 53 | ||
| The presence of gestational hypertension | 4.035 | 0.133 | ||||
| There are | 41 | 1 | 15 | 25 | ||
| There is no | 110 | 3 | 60 | 47 | ||
| Whether placenta previa is present | 1.491 | 0.474 | ||||
| There are | 9 | 0 | 3 | 6 | ||
| There is no | 142 | 4 | 72 | 66 | ||
| Whether there is premature rupture of membranes | 1.233 | 0.540 | ||||
| There are | 28 | 0 | 13 | 15 | ||
| There is no | 123 | 4 | 62 | 57 | ||
| Whether there is pregnancy infection | 0.431 | 0.806 | ||||
| There are | 9 | 0 | 4 | 5 | ||
| There is no | 142 | 4 | 71 | 67 | ||
| Whether other diseases are present | 0.296 | 0.862 | ||||
| There are | 10 | 0 | 5 | 5 | ||
| There is no | 141 | 4 | 70 | 67 | ||
| Whether there is pregnancy with arrhythmia | 2.186 | 0.335 | ||||
| There are | 5 | 0 | 1 | 4 | ||
| There is no | 146 | 4 | 74 | 68 | ||
| Whether you have hypothyroidism | 2.052 | 0.358 | ||||
| There are | 17 | 1 | 6 | 10 | ||
| There is no | 134 | 3 | 69 | 62 | ||
| History of cesarean section | 1.005 | 0.605 | ||||
| There are | 15 | 0 | 9 | 6 | ||
| There is no | 136 | 4 | 66 | 66 | ||
Table 2.
Assignment methods of argument variables.
| Independent variable | Assignment mode |
|---|---|
| Gestational age | <28w=1;28~31+6w=2;32~33+6w=3;34~36+6w=4 |
| Time of admission | <24h=1;≥24h=2 |
| Whether you have NRDS | Yes=1;no=2 |
| Preterm weight | <1000g=1;<1500g=2;<2500g=3;≥2500g=4 |
| Antibiotic use | There is no=1;<7d=2;≥7d=2 |
| Apgar score in 1 minute | normal=1;Mild asphyxia=2;Severe asphyxia=3 |
| Maternal education level | Junior high school and below=1;High school and technical secondary school=2;College degree or above=3 |
| Umbilical cord shedding time | <7d =1,7~14d =2,>14d=3 |
| Time in box | Original value entry |
| Inlet temperature | Original value entry |
| Phototherapy duration | Original value entry |
Table 3.
Multiple Logistic regression analysis of factors affecting the time of premature infants' umbilical shedding.
Table 3.
Multiple Logistic regression analysis of factors affecting the time of premature infants' umbilical shedding.
| variable | β | S.E | Wald | df | P | 95% CI | |
|---|---|---|---|---|---|---|---|
| The lower limit ceiling | |||||||
| Time in the warm tank(h) | 0.018 | 0.004 | 23.581 | 1 | 0.000 | 0.138 | 0.427 |
| Inlet temperature(℃) | 0.054 | 0.411 | 0.017 | 1 | 0.895 | -0.751 | 0.859 |
| Phototherapy duration(h) | -0.017 | 0.013 | 1.746 | 1 | 0.186 | -0.043 | 0.008 |
| Gestational age | |||||||
| <28w | 13.504 | 0.000 | . | 1 | . | 13.504 | 13.504 |
| 28~31+6w | -1.638 | 1.159 | 1.997 | 1 | 0.158 | -3.911 | 0.634 |
| 32~33+6w | -1.156 | 0.638 | 3.286 | 1 | 0.070 | -2.406 | 0.094 |
| 34~36+6w | Reference class | ||||||
| Time of admission | |||||||
| <24h | 2.142 | 1.168 | 3.361 | 1 | 0.067 | -0.148 | 4.432 |
| ≥24h | Reference class | ||||||
| Whether you have NRDS | |||||||
| Yes | -0.535 | 0.689 | 0.603 | 1 | 0.438 | -1.885 | 0.815 |
| No | Reference class | ||||||
| Apgar1 minute degree | |||||||
| normal | -0.003 | 2.207 | 0.000 | 1 | 0.999 | -4.330 | 4.323 |
| Mild asphyxia | 1.317 | 2.174 | 0.367 | 1 | 0.545 | -2.944 | 5.579 |
| Severe asphyxia | Reference class | ||||||
| weight | |||||||
| <1000g | 17.251 | 0.000 | . | 1 | . | 17.251 | 17.251 |
| <1500g | -.812 | 1.247 | 0.424 | 1 | 0.515 | -3.257 | 1.632 |
| <2500g | -1.005 | 0.768 | 1.712 | 1 | 0.191 | -2.510 | 0.500 |
| ≥2500g | Reference class | ||||||
| Whether to use antibiotics | |||||||
| No | -0.749 | 0.746 | 1.007 | 1 | 0.316 | -2.212 | 0.714 |
| Service time<7d | -0.444 | 0.743 | 0.358 | 1 | 0.550 | -1.900 | 1.011 |
| Service time≥7d | Reference class | ||||||
| Level of education | |||||||
| Junior high school and below | 0.527 | 0.518 | 1.036 | 1 | 0.309 | -0.488 | 1.543 |
| High school and technical secondary school | 1.068 | 0.604 | 3.123 | 1 | 0.077 | -0.116 | 2.252 |
| College degree or above | Reference class | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



