Submitted:
18 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Opium smoking for long hours and over many years is common in Iran, and the Covid-19 pan-demic and false beliefs about the protective effects of that opium against COVID-19 infection has caused the increasing of opium smoking during the pandemic. The aim of this study was to in-vestigate the relationship between non-ergonomic positions of traditional opium smoking in Iran with the occurrence of neck pain and disability, forward head posture and hyperkyphosis. In this cross-sectional and correlation study 120 people who smoke opium were selected based on the inclusion criteria and were interviewed about their addiction profile and evaluated for the pres-ence of pain and disability in the neck by Maudsley Addiction Profile, Leeds Dependence Ques-tionnaire, the Visual Analog Scale and Neck Disability Index. Also, they were evaluated about forward head posture (FHP) through side view photography and hyperkyphosis (HK) through flexible ruler. Data were analyzed by correlation coefficient tests and stepwise linear regression. There was a significant relation between homelessness, the duration of lifetime opium smoking (months), the duration of daily opium smoking (minutes) and drug dependence severity with the severity of neck pain, neck disability, forward head posture and hyperkyphosis. Homelessness is the strongest predictive variable of the possibility of neck pain and disability, FHP and HK, fol-lowed by ‘‘the number of months of opium smoking’’ and ‘‘the number of minutes of opium smoking in one day’’ respectively. Increasing the duration of sitting in non-ergonomic positions can lead to neck pain and disability, FHP and HK due to their non-neutral posture in opium smokers.
Keywords:
Opiates
; Opium smoking
; Neck pain
; Neck disability
; Forward head posture
; Hyperkyphosis
; Drug use disorder
; Iran
1. Introduction
Most researchers and scientists believe that addiction is a brain disease, and although they may not agree on specific neurological symptoms, they all agree that addiction has a neurobiological basis, and in addition to substance dependence, it also leads to addictive behaviors. In other words, in addition to dependence on the consumption of a substance, a person may also become dependent on the method of consumption of that substance and the tools of its consumption in the form of behavioral addiction (1, 2). Iran is one of the countries that faces the most problems in the field of addiction. Iran has seized more opium, morphine, and heroin than any other country in the world, based on 2022 world drug report. 98% of the opium seized in the world comes from Iran, because in addition to the international transit route, many people there have a long history and culture of opium smoking, and it is tied to the geopolitics of the region (3, 4). More than 2000,000 people are using drug daily in Iran and more than 70% of them are opiates users (5). Many addictive behaviors have shown pathogenesis in the same neurocircuitry of substance use disorder (6), and it seems that opium smokers have a combination of addictive behavior and substance dependence. In fact, using opium through smoking is an addictive behavior that is added to their dependence on opium. Opium smoking is very common due to its historical background and the special geographical conditions of Iran, and unfortunately following the outbreak of the Covid-19 pandemic and the false beliefs that opium smoking stops the spread of the Coronavirus, opium smoking increased further (7) and more than 90% of drug use in Iran is through smoking (5). In the ranking of health problems that are the cause of the most disabilities in Iran, drug use disorders are in the fourth place, and among the factors that cause death and disability, it ranks eighth (8). Drug dependents for various reasons [non-ergonomic position when using (smoking or inhalation), lack of movement and inactivity (9), malnutrition (10) and heavy smoking (11)], seem to be more prone to some of the musculoskeletal disorders. Opium dependents when smoke opium, they use three special types of tools called 'Vafour', 'Gholgholi', and 'Sikh-o-sang' in uncomfortable positions where their head tilts forward more than normal. It also can cause in their spine, making them curved over and sometimes leaning to one side (12, 13). If opium smoking in this way, which is common, continues for several hours a day and for many years, the risk of neck musculoskeletal disorder will be high, like many work-related musculoskeletal disorder caused by non-ergonomic position (14, 15).
On the other hand, musculoskeletal disorders are one of the most common health concerns in the world and in the classification of disabling health problems in 2017, musculoskeletal disorders are among the most common causes of disability and reduction of life years without disability, and lower back and neck pains are in the fourth category of these problems (16, 17). Also, in the similar report from 2020, it was announced that spinal problems and headaches are among the top ten causes of disability in the age groups between 10 to 24 years and 25 to 49 years old (18). Musculoskeletal disorders are often acquired and caused by work or non-ergonomic positions (19). Various physical and mechanical risk factors such as: long-term repetitive work (especially in non-ergonomic position), continuous lifting or lifting a heavy load, pushing, pulling or carrying heavy loads, can cause or aggravate these disorders. There is a close relationship between these disorders and improper use of body mechanics (20, 21). Bending forward and turning the neck, incorrect sitting and standing positions, and also doing repetitive manual activities are the most important factors for neck musculoskeletal disorders and there is a positive relationship between neck pain and incorrect sitting or standing position. Neck and shoulder’s muscles and joints problems are also significantly related to poor postures (15, 22). Neck pain and disability is one of the most common work-related musculoskeletal disorders (23). Neck pain and disability are common in many occupations and daily and repetitive activities of life and even sports, where the upper body and upper limbs are in uncomfortable positions or a position in which the upper limb is repeatedly held forward and up (24, 25). While smoking opium, people keep their upper limbs and hands up and forward, and this position is repeated several hours a day. In the same category of jobs and daily activities and sports mentioned above, forward head posture (FHP) and hyperkyphosis (HK) are also very common, and for example, office workers and industrial brokers and even some sports such as cyclists show a higher rate of forward head posture and kyphosis (26-30). Tilting of the head and neck forward and creating a kyphotic hump in the spine can also be seen in opium smokers when they sit and smoke opium. Taking into consideration that the incidence of physical disorders has increased in today's urban life, it is very important to document the incidence and prevalence of these disorders and the factors that underlie them, in different age groups, gender, occupation, etc.,. Since very few and incomplete researches have been done in this field on people with drug use disorder, both in Iran and in other countries, and in the field of addiction, most of the researches have been from the psychiatric, psychological and social aspects, the purpose of this study is to investigate the relationship between opium smoking and the incidence of neck pain and disability, forward head posture and kyphosis in opium smokers in Tehran.
2. Materials and Methods
2.1. Participants
This cross-sectional and correlation study was done in 2022 in Tehran. 120 people who use opiates were selected from the clients of outpatient treatment centers in Tehran based on the necessary criteria and were evaluated for the presence of pain and disability in the neck. The main inclusion criteria include the diagnosis of substance use disorder and dependence according to the ICD-11 criteria (31), also, their main used drug was opium and their predominant method of consumption was smoking, as well as the ability to stand, age between 25 and 50 years, and Body Mass Index (BMI) below 27.5 (because in this age range and BMI, the probability of skeletal-muscular disorders is less), and the exclusion criteria also include a history of neuromuscular or skeletal disease, a past history of surgery in the spine and shoulder girdle, history of championship or regular exercise, any imbalance caused by a specific disease, any clear postural deformity or anatomical disorder and using of smartphones and tablets more than half to an hour (0.5-1 h) a day (32). The sample size was estimated by using G*Power software and based on the number of variables in cross-sectional correlation studies, statistical power 80% and significance level 0.05 (105 people).
2.1. Tools and data gathering
Data gathering was done by, demographic questionnaire, The Maudsley Addiction Profile (33), the Persian version of the Leeds Dependence Questionnaire (34), the Visual Analog Scale, and Neck Disability Index (35). Also, the practical measurements of this study were done through photography and curved ruler, both of which are valid and reliable methods for evaluating forward head posture and hyperkyphosis (36, 37).
In order to evaluate the forward head posture in this study, the craniovertebral angle was measured. To measure the craniovertebral angle, photography was used from the side view. In this way, using a Canon digital camera, made in Japan (Canon PowerShot G11 10MP, Japan), the person was photographed from a distance of 265 cm. The person was standing sideways next to the wall and the camera was placed at a height in line with his shoulder and completely perpendicular to the sagittal plane of his body. The photos were transferred to the AUTOCAD-2013 software and the craniovertebral angle was measured.
The examination of the spine curvature in the thoracic region and the measurement of the thoracic kyphosis angle were performed as follows: the person was standing in a normal and relaxed position and after moving the head, neck and upper limbs several times (in order to relax the muscles from any stress and contraction), they stood up straight in a upright posture and motionless with the spine in a completely neutral straightened position. A flexible ruler (brand name: Staedtler Mars 24-inch, Germany) is placed completely tangentially on the thoracic spine from T2 to T12, then the ruler is transferred to a sheet of A3 paper while keeping the same curve completely, and the curved line on The paper was drawn. The kyphosis angle was measured using this equation: α=4arctan(2h/l)
2.1. Data analysis
Statistical analysis was done by SPSS software version 23 through Shapiro-Wilk test, correlation coefficient tests (Goodman and Kruskal's lambda, Pearson and Spearman) and stepwise linear regression.
2.1. Ethical consideration
The study design and research method has been approved by the ethics committee of the University of Social Welfare and Rehabilitation Sciences with the code of IR.USWR.REC.1398.120. We obtained informed consent from all participants. This article is extracted from the doctoral thesis of the first author.
3. Results
3.1.1. Basic variables
The demographic characteristics of the samples and their substance use profile are presented in Table 1.
3.1.2. Main variables
There was a significant relation between the age of continues opium smoking, homelessness, the duration of lifetime opium smoking (in months) and the duration of daily opium smoking (in minutes) with the severity of neck pain, but age of occasional opium smoking, BMI, job, drug use duration, opium smoking method and drug dependence severity had no significant relationship with neck pain (Table 2). Also, neck disability showed significant correlation with homelessness, the duration of lifetime opium smoking (months), the duration of daily opium smoking (minutes) and drug dependence severity; but there was no significant relationship between BMI, age of occasional or continues opium smoking and drug use duration with neck disability (Table 3).
Neck disability and disorders were almost twice as correlated with opium smoking through a ‘Wafour’ (a type of vape that is a traditional tool of opium smoking in the Middle East and Persian Gulf countries), compared to opium smoking through a hookah (a small opium smoking hookah called ‘‘Gholgholi’’ in Iran) or through spoke & pin (Sikh-o-Sang). But neck pain was not different between different methods of opium smoking.
In order to investigate the correlation between forward head posture and hyperkyphosis with independent variables, the correlation coefficient between them was calculated. As the results are available in Table 4, forward head posture and hyperkyphosis have significant and moderate reverse correlation with age of continues opium smoking. Homelessness had the strongest significant correlation with forward head posture and hyperkyphosis. Also Opium smoking duration (month) and Daily opium smoking time (minutes) were significantly and strongly correlated with forward head posture and hyperkyphosis and drug dependence severity showed significant moderate correlation with FHP and HK.
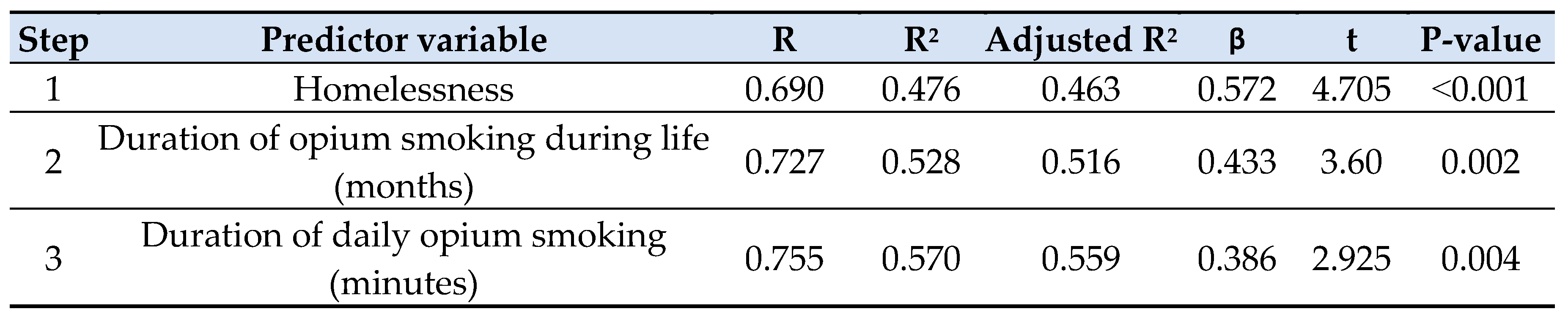
In order to investigate the effect of independent variables in predicting the occurrence of neck problems and disability, forward head posture and hyperkyphosis stepwise regression analysis was used. As presented in Table 5, Table 6 and Table 7 homelessness is the strongest predictive variable for the possibility of neck musculoskeletal disorders and disability, FHP and HK. Also, the number of months of opium smoking and the number of minutes of smoking in one day are other variables that increase the coefficient of determination (R2 and adjusted R2) in the regression analysis for predicting neck disability and hyperkyphosis, but about the forward head posture, the daily duration of opium smoking entered the regression table ahead of the number of months of opium smoking in the lifetime. (Table 5, Table 6 and Table 7).
4. Discussion
The current study was aimed to investigate the relationship between drug dependence and its severity, as well as its smoking use with neck pain and disabilities. The findings of this study showed that increasing the opium smoking can have negative effects on some functions of the neck and cause pain and limitations in its ability.
Sedentary life style in today's modern societies is the source of many health concerns (38), and Iran has a special position compared to other countries in the world due to the reasons stated earlier.
In Iran, it is common for opium addicts to smoke opium (or residue of smoked opium) for several years and for long hours a day with various tools such as ‘Wafour’ (or Vafour), ‘Hookah’, etc. in non-ergonomic positions (12) and it can be a major potential risk factor for the occurrence of postural disorders and skeletal problems of the upper body, beside of shorter smoking time period of heroin and cannabis which are more common in other countries (3). Therefore, this issue may not be as important as Iran in other countries. There are still no similar studies from other countries in this field so that we can compare their results with the results of this study. Only the impact of homelessness on the occurrence of health problems is a proven fact in previous researches. For instance, in the study of Sun et al., the existence of a direct and significant correlation between homelessness and more pain and musculoskeletal disorders has been shown (39). This relationship has been proven in other studies (40).
Iran is the second country in terms of severe opioid addiction and has the highest rate of heroin and opium addiction per capita in the world. So among the population aged 15 to 60, one out of every five people has non-permanent drug abuse and one out of every 17 people is a permanent user (3). The non-ergonomic and harmful position that drug users give to their spine during opium smoking is the cause of pain and disability in the cervical vertebrae. Moreover, the results of this study also report a significant relationship between the occurrence of neck pain and the younger age of continuous drug use, the method of use, the number of months of opium smoking and daily opium smoking duration in minutes. There was no similar study to compare these results in other countries. Only Daneshmandi et al. in their study showed that spine disorders and postures deformities are more prevalent in prison addicts of Iran (41). In explaining the occurrence of pain, it can be said that: repetitive work in an incorrect and non-neutral position leads to postural pressure, fatigue and pain (42). It has also been proven that according to their work habits or work needs, people are placed in wrong and non-standard body positions, which after a while causes them various pains, which are postural pains (43). Similar to what was found about opium smokers in this study, it was also found in previous studies for dentists that working for several hours a day in harmful positions causes many kinds of neck musculoskeletal disorders (44, 45).
Forward head posture showed a high significant correlation with the number of months of opium smoking during life and the daily duration of opium smoking, while it was not correlated with the total duration of drug use (i.e. of any type of substance and any method of use). These results make the relation and alignment of opium smoking with forward head posture more important and increase the possibility of a causal relationship between them. Although there are no similar studies in this field, we can refer to other studies that are somewhat similar to these studies. The prevalence of forward head posture in office workers who work on a desktop, or gamers who often put their head and neck forward and non-neutral position for long hours, are similar examples of opium smoking positions (46, 47).
Also, hyperkyphosis showed a high positive and significant correlation with the number of months of opium smoking during life and the number of daily minutes of opium smoking. This correlation should also be investigated more and more precisely in future studies in terms of the existence of a causal relationship between them. If it has been proven that dentists and farmers have similar positions during work, the risk of hyperkyphosis increases in them in the long run (48, 49). Neck disability, which was significantly correlated with opiate smoking, was similarly more common in office workers who experienced similar non-ergonomic positions (50).
As the results of regression analysis showed, homelessness is the strongest predictor of musculoskeletal neck disorders. Although there is no similar research to emphasize the significant relationship obtained in this study; however in explaining this relationship, we can point to other secondary causes, which are caused by homelessness. Lack of movement, insufficient and unhealthy nutrition, sitting and sleeping in non-ergonomic positions and heavy smoking are the consequences of homelessness that can aggravate the occurrence of skeletal disorders. Previous studies have also shown a positive relationship between neck pain and neck musculoskeletal disorders with incorrect sitting or standing and sleeping positions (22, 49, 51). Previous studies have also indicated the effect of malnutrition on muscle weakness, especially in the axial muscles (which can cause disability and spinal deviation) (52). Also, the occurrence of musculoskeletal pain due to tissue malnutrition caused by smoking has been emphasized in people who lift heavy loads for their jobs (53), and the occurrence of pain and musculoskeletal disorders caused by hypovitaminosis D due to malnutrition has also been proven before (54).
There were some limitations in this study that should be considered. First and the main limitation of this topic (no this study) was the lack of similar studies; both in Iran and in other countries. In fact, after paying attention to the possibility of this problem (incidence of complications of non-ergonomic positions in opium smokers in Iran), in the next step and literatures review, no reports of similar studies were found. It seems that this issue is not so important in other countries (perhaps due to the shorter smoking time, considering the nature of the types of consumable drugs) and it has not been discussed in Iran yet. Therefore, it was necessary to design research using more basic methods and prove the existence of correlation. It is recommended to use research methods such as case-control and even prospective studies in order to stronger establishing of achieved correlations in this study. The second limitation of the study was that unfortunately, the female samples refused to participate in the study and we had to settle for the results of the men.
5. Conclusions
Non-ergonomic positions due to opium smoking have strong relationship with neck pain and disability, and posture deformities such as forward head posture and hyper-kyphosis. Opium smoking in different methods for long hours a day, which continues for years can lead to neck pain, neck musculoskeletal disorders, decreasing in craniovertebral angle (forward head posture) and increasing in thoracic kyphosis angle (hyper-kyphosis).
Author Contributions
Study concept and design was done by AM.A., A.F., O.M. and M.N. Data gathering and data analysis was done by O.M. All the authors contribute to drafting, writing and editing of the article.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study design and research method has been approved by the ethics committee of the University of Social Welfare and Rehabilitation Sciences with the code of IR.USWR.REC.1398.120.
Informed Consent Statement
We obtained informed consent from all participants.
Acknowledgments
In this way, we thank the participants of both groups for participating in this study.
Conflicts of Interest
The authors declare no personal, organizational and financial conflict of interest.
References
- Leshner, A.I. Addiction Is a Brain Disease. Issues in Science and Technology 2001, 17, 75–80 http://wwwjstororg/stable/43314081. [Google Scholar]
- Heilig, M.; MacKillop, J.; Martinez, D.; Rehm, J.; Leggio, L.; Vanderschuren, L.J.M.J. Addiction as a brain disease revised: why it still matters, and the need for consilience. Neuropsychopharmacology 2021, 46, 1715–1723. [Google Scholar] [CrossRef] [PubMed]
- UNODC. World Drug Report 2022. Vienna, Austria: (United Nations publication, 2022); 2022. Available online: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2022.html.
- Zarghami, M. Iranian Common Attitude Toward Opium Consumption. Iran. J. Psychiatry Behav. Sci. 2015, 9, e2074. [Google Scholar] [CrossRef] [PubMed]
- Rafiey H, Alipour F, Madani S, Narenjiha H. Rapid situation assessment of drug abuse in Iran, 2018. Tehran: Department of Research and Education, Drug Control Headquarters. 2018.
- Potenza, M.N. Clinical neuropsychiatric considerations regarding nonsubstance or behavioral addictions. Dialog- Clin. Neurosci. 2017, 19, 281–291. [CrossRef]
- Mahdavi, A.; Aliramezany, M. Addiction and Covid-19 Disease: Risks and Misconceptions. Addiction and Health 2021, 13, 66–67. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 2018, 392, 1923–1994. [Google Scholar]
- Muller, A.E.; Skurtveit, S.; Clausen, T. Many correlates of poor quality of life among substance users entering treatment are not addiction-specific. Heal. Qual. Life Outcomes 2016, 14, 39. [Google Scholar] [CrossRef]
- Mahboub, N.; Rizk, R.; Karavetian, M.; de Vries, N. Nutritional status and eating habits of people who use drugs and/or are undergoing treatment for recovery: a narrative review. Nutr. Rev. 2020, 79, 627–635. [Google Scholar] [CrossRef]
- Liu, L.; Li, F.T. Optimal decision of deferred payment supply chain considering bilateral risk-aversion degree. Math. Prob. Eng. 2018, 2018, 4184190. [Google Scholar] [CrossRef]
- Regavim RB. The most sovereign of masters: The history of opium in modern Iran, 1850–1955: University of Pennsylvania; 2012.
- Ghiabi M. Part One. Drugs Politics: Managing Disorder in the Islamic Republic of Iran. Cambridge: Cambridge University Press; 2019. p. 33-4. [CrossRef]
- Abaraogu, U.; Odebiyi, D.; Olawale, O. Association between postures and work-related musculoskeletal discomforts (WRMD) among beverage bottling workers. Work 2016, 54, 113–119. [Google Scholar] [CrossRef]
- Balogh, I.; Arvidsson, I.; Björk, J.; Hansson, G.Å.; Ohlsson, K.; Skerfving, S.; Nordander, C. Work-related neck and upper limb disorders – quantitative exposure–response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet. Disord. 2019, 20, 139. [Google Scholar] [CrossRef]
- Cooper, C. Global, regional, and national disability-adjusted life-years (DALY) for 359 diseases and injuries and health life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 2018, 392, 1859–1922. [Google Scholar]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- da Costa, B.; Vieira, E. Stretching to reduce work-related musculoskeletal disorders: A systematic review. J. Rehabilitation Med. 2008, 40, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Anghel, M.; Argesanu, V.; Talpos-Niculescu, C.; Lungeanu, D. Musculoskeletal disorders (MSDs)-consequences of prolonged static postures. Journal of Experimental Medical & Surgical Research 2007, 4, 167–172. [Google Scholar]
- Lee, Y.; Park, H. Workers' Perception of the Changes of Work Environment and its Relation to the Occurrence of Work-Related Musculoskeletal Disorders. Journal of Occupational Health 2007, 49, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Diana, V. Literature Review : Effect of Static Conditions on Musculoskeletal Disorders (MSDs). Basic Appl. Nurs. Res. J. 2021, 2, 52–59. [Google Scholar] [CrossRef]
- Epstein, S.; Sparer, E.H.; Tran, B.N.; Ruan, Q.Z.; Dennerlein, J.T.; Singhal, D.; Lee, B.T. Prevalence of Work-Related Musculoskeletal Disorders Among Surgeons and Interventionalists. JAMA Surg. 2018, 153, e174947. [Google Scholar] [CrossRef]
- Pascarelli, E.F.; Hsu, Y.-P. Understanding work-related upper extremity disorders: clinical findings in 485 computer users, musicians, and others. J. Occup. Rehabilitation 2001, 11, 1–21. [Google Scholar] [CrossRef]
- Chowdhury, S.K.; Zhou, Y.; Wan, B.; Reddy, C.; Zhang, X. Neck Strength and Endurance and Associated Personal and Work-Related Factors. Hum. Factors: J. Hum. Factors Ergon. Soc. 2021, 64, 1013–1026. [CrossRef]
- Gallagher, S. Physical limitations and musculoskeletal complaints associated with work in unusual or restricted postures: A literature review. J. Saf. Res. 2005, 36, 51–61. [Google Scholar] [CrossRef]
- Grabara, M. Comparison of posture among adolescent male volleyball players and non-athletes. Biol. Sport 2014, 32, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Muyor, J.; López-Miñarro, P.; Alacid, F. Comparison of sagittal lumbar curvature between elite cyclists and non-athletes. Sci. Sports 2013, 28, e167–e173. [Google Scholar] [CrossRef]
- Bagherian S, Rahnama N, Mahmudi F, editors. Investigation of Curves of the spinal cord of the table tennis athletes. Proceedings of the 6th National Conference on Physical Education Students; 2011.
- Sadeghi MG, G.A. Iraj, F. Comparing selected spinal column postural abnormalities of professional and amateur Wushu athletes with those of non-athletes. Journal of Research in Rehabilitation Sciences. 2012;8(3):582-9.
- Poznyak, V.; Reed, G.M.; Medina-Mora, M.E. Aligning the ICD-11 classification of disorders due to substance use with global service needs. Epidemiology Psychiatr. Sci. 2017, 27, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Neupane S, Ali U, Mathew A. Text neck syndrome-systematic review. Imperial journal of interdisciplinary research. 2017;3(7):141-8.
- Marsden, J.; Gossop, M.; Stewart, D.; Best, D.; Farrell, M.; Lehmann, P.; Edwards, C.; Strang, J. The Maudsley Addiction Profile (MAP): a brief instrument for assessing treatment outcome. Addiction 1998, 93, 1857–1867. [Google Scholar] [CrossRef] [PubMed]
- Massah, O.; Rafiey, H.; Shariatirad, S.; Radfar, S.R.; Ahounbar, E.; Farhoudian, A. The Validity and Reliability of the Persian Version of the Leeds Dependence Questionnaire. Iran. Rehabilitation J. 2019, 91–96. [Google Scholar] [CrossRef]
- Mousavi, S.J.; Parnianpour, M.; Montazeri, A.; Mehdian, H.; Karimi, A.; Abedi, M.; Ashtiani, A.A.; Mobini, B.; Hadian, M.R. Translation and Validation Study of the Iranian Versions of the Neck Disability Index and the Neck Pain and Disability Scale. Spine 2007, 32, E825–E831. [Google Scholar] [CrossRef]
- Mylonas, K.; Tsekoura, M.; Billis, E.; Aggelopoulos, P.; Tsepis, E.; Fousekis, K. Reliability and Validity of Non-radiographic Methods of Forward Head Posture Measurement: A Systematic Review. Cureus 2022, 14, e27696. [Google Scholar] [CrossRef]
- Khalkhali-Zavieh, M.; Parnian-Pour, M.; Karimi, H.; Mobini, B.; Kazem-Nezhad, A. The Validity and Reliability of Measurement of Thoracic Kyphosis Using Flexible Ruler in Postural Hyper Kyphotic Patients. Archives of Rehabilitation. 2003, 4, 18–23 http://rehabilitationjuswracir/article. [Google Scholar]
- Biddle, S.J.; García, E.B.; Pedišić, Ž.; Bennie, J.; Vergeer, I.; Wiesner, G. Screen Time, Other Sedentary Behaviours, and Obesity Risk in Adults: A Review of Reviews. Curr. Obes. Rep. 2017, 6, 134–147. [Google Scholar] [CrossRef]
- Sun, S.; Irestig, R.; Burström, B.; Beijer, U.; Burström, K. Health-related quality of life (EQ-5D) among homeless persons compared to a general population sample in Stockholm County, 2006. Scand. J. Public Heal. 2012, 40, 115–125. [Google Scholar] [CrossRef]
- van Laere, I.; de Wit, M.; Klazinga, N. Shelter-based convalescence for homeless adults in Amsterdam: a descriptive study. BMC Heal. Serv. Res. 2009, 9, 208–208. [Google Scholar] [CrossRef] [PubMed]
- Daneshmandi, H.; Rahmani, F.; Neshati, A. The Study of Posture and Aerobic Power of Addicts. Journal of Applied Exercise Physiology 2007, 3, 11–21. [Google Scholar]
- Haslegrave, C.M. What do we mean by a ‘working posture’? Ergonomics 1994, 37, 781–799. [Google Scholar] [CrossRef] [PubMed]
- da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am. J. Ind. Med. 2009, 53, 285–323. [Google Scholar] [CrossRef] [PubMed]
- Morse, T.; Bruneau, H.; Dussetschleger, J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work 2010, 35, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhou, W.; Aisaiti, A.; Wang, B.; Zhang, J.; Svensson, P.; Wang, K. Dentists have a high occupational risk of neck disorders with impact on somatosensory function and neck mobility. J. Occup. Heal. 2021, 63, e12269. [Google Scholar] [CrossRef]
- Ashok, K.; Purushothaman, V.K.; Muniandy, Y. Prevalence of forward head posture in electronic gamers and associated factors. International Journal of Aging Health and Movement 2020, 2, 19–27. [Google Scholar]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The Relationship Between Forward Head Posture and Neck Pain: a Systematic Review and Meta-Analysis. Curr. Rev. Musculoskelet. Med. 2019, 12, 562–577. [Google Scholar] [CrossRef]
- Alexopoulos, E.C.; Stathi, I.-C.; Charizani, F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet. Disord. 2004, 5, 16. [Google Scholar] [CrossRef]
- Jain, R.; Meena, M.L.; Dangayach, G.S. Prevalence and risk factors of musculoskeletal disorders among farmers involved in manual farm operations. Int. J. Occup. Environ. Health 2018, 1–6. [Google Scholar] [CrossRef]
- Medin-Ceylan, C.; Korkmaz, M.D.; Sahbaz, T.; Karacay, B.C. Risk factors of neck disability in computer-using office workers: a cross-sectional study. Int. J. Occup. Saf. Ergon. 2022, 29, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cui, Y.; He, L.; Xu, X.; Yuan, Z.; Jin, X.; Li, Z. Work-Related Musculoskeletal Disorders and Risk Factors among Chinese Medical Staff of Obstetrics and Gynecology. Int. J. Environ. Res. Public Heal. 2017, 14, 562. [Google Scholar] [CrossRef] [PubMed]
- Garrido, E.M.; Di Lodovico, L.; Dicembre, M.; Duquesnoy, M.; Ohanyan, H.; Melchior, J.-C.; Hanachi, M. Evaluation of muscle-skeletal strength and peak expiratory flow in severely malnourished inpatients with anorexia nervosa: A pilot study. Nutrition 2021, 85, 111133. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, W.; Natvig, B.; Bruusgaard, D. Smoking, heavy physical work and low back pain: A four-year prospective study. Occup. Med. 1999, 49, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Arabi, A.; El Rassi, R.; Fuleihan, G.E.-H. Hypovitaminosis D in developing countries—prevalence, risk factors and outcomes. Nat. Rev. Endocrinol. 2010, 6, 550–561. [Google Scholar] [CrossRef]

Table 1.
Demographic characteristics and opium use profile of participants.
| Variables | Mean | SD |
|---|---|---|
| Age | 39.30 | 5.05 |
| Weight | 72.70 | 6.48 |
| Height | 1.73 | 6.13 |
| BMI | 24.29 | 2.12 |
| Age of first drug use (any kind of drug) | 19.35 | 6.45 |
| Age of occasional drug use (any kind of drug) | 21.05 | 5.15 |
| Age of occasional opium smoking | 23.45 | 5.85 |
| Age of continues opium smoking | 28.20 | 6.15 |
| Duration of opium smoking during life (months) | 110.45 | 31.70 |
| Duration of daily opium smoking (minutes) | 212.35 | 48.45 |
| Dependence severity score | 25.20 | 4.35 |
Table 2.
Correlation between neck pain and predictor variables of study.
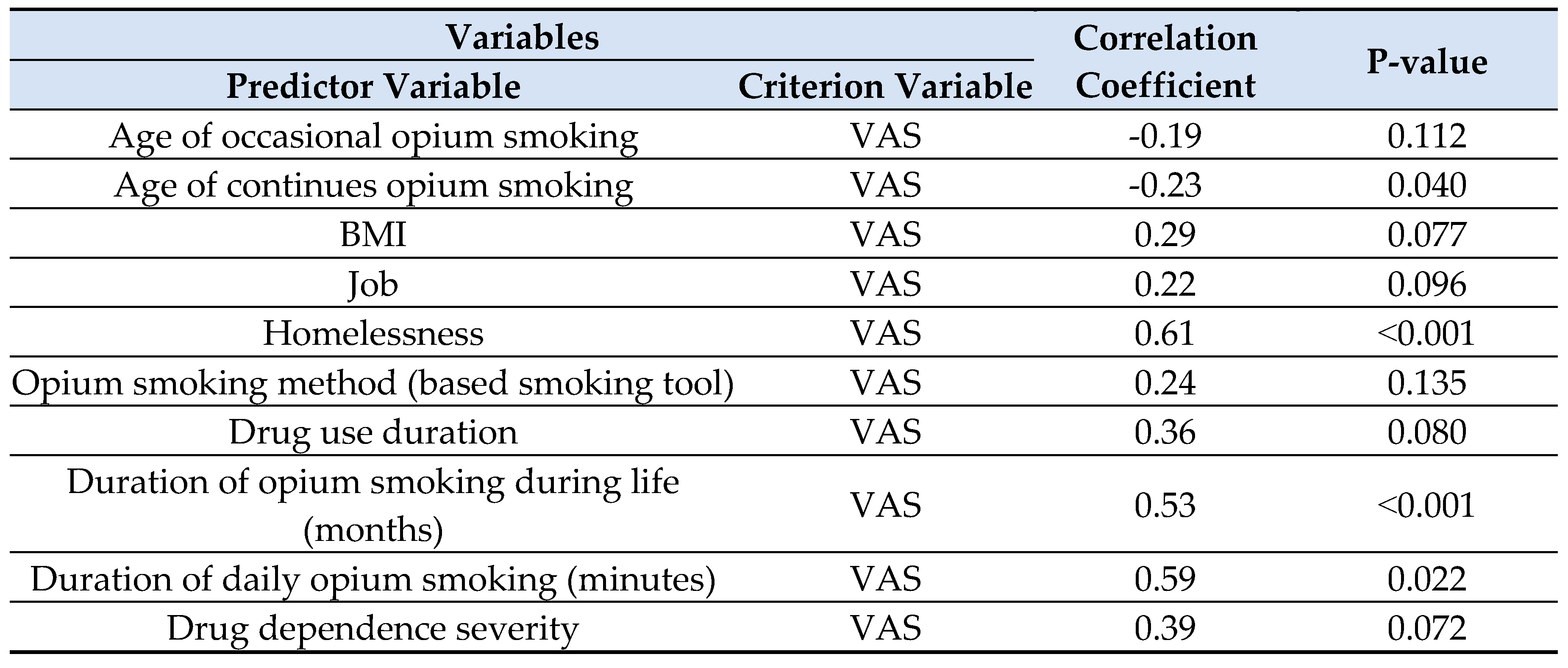
Table 3.
Correlation between neck disability and predictor variables of study.
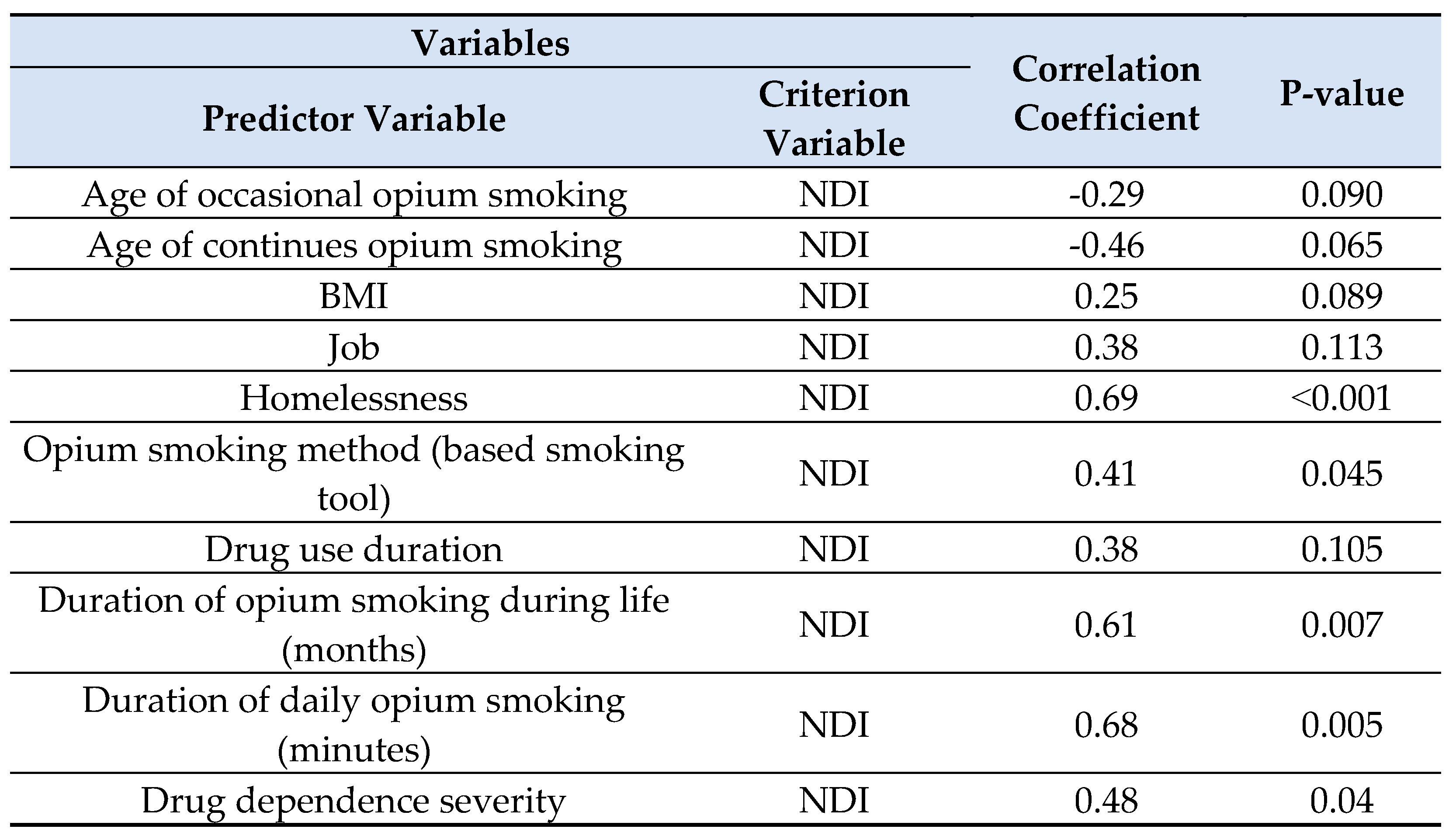
Table 4.
Correlation between forward head posture and hyperkyphosis with predictor variables of study.
Table 4.
Correlation between forward head posture and hyperkyphosis with predictor variables of study.
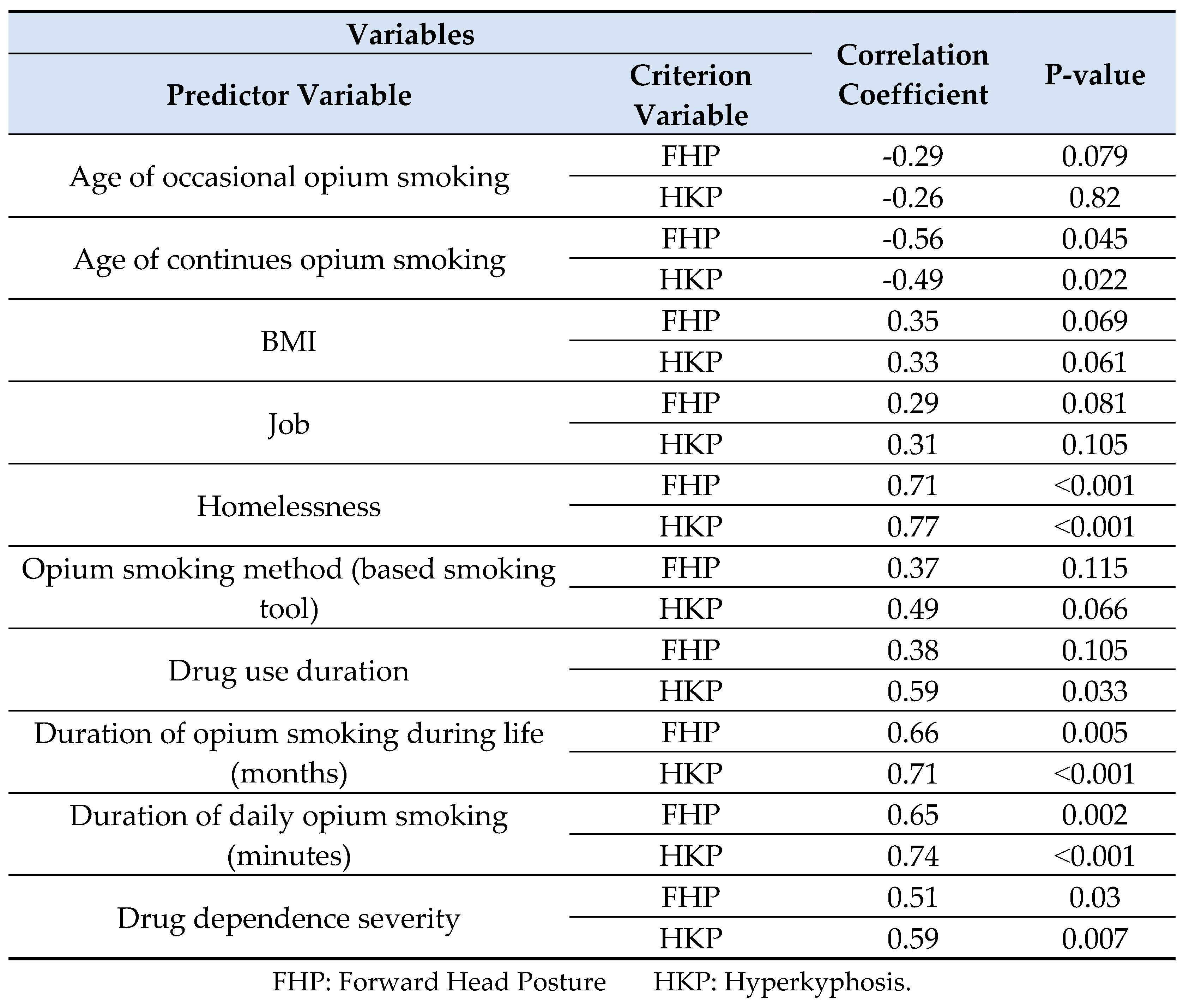
Table 5.
Stepwise regression analysis for neck disability (criterion variable) based on predictor variables.
Table 5.
Stepwise regression analysis for neck disability (criterion variable) based on predictor variables.
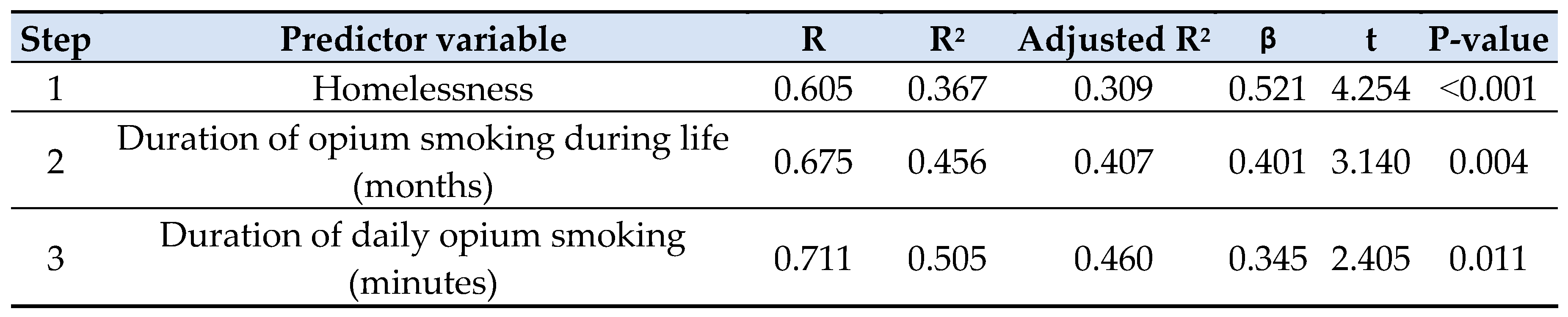
Table 6.
Stepwise regression analysis for forward head posture (criterion variable) based on predictor variables.
Table 6.
Stepwise regression analysis for forward head posture (criterion variable) based on predictor variables.
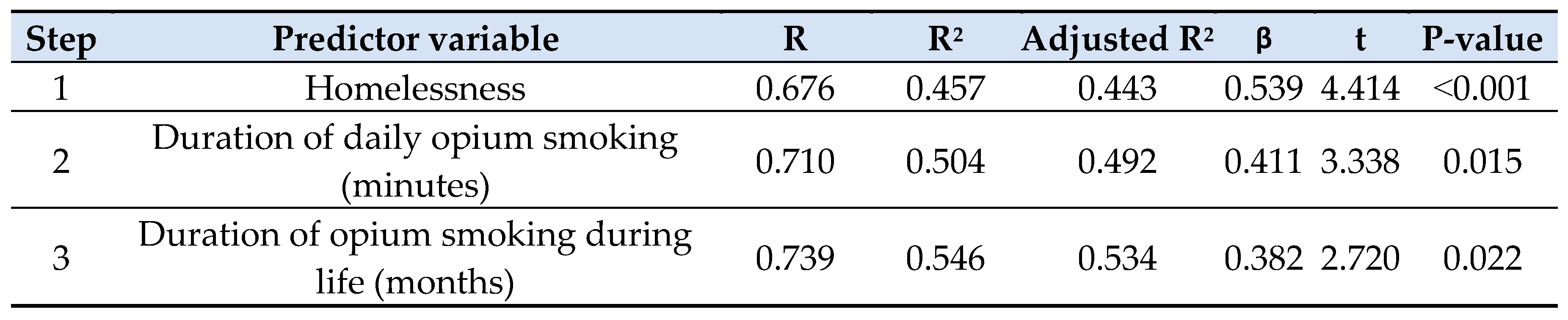
Table 7.
Stepwise regression analysis for hyperkyphosis (criterion variable) based on predictor variables.
Table 7.
Stepwise regression analysis for hyperkyphosis (criterion variable) based on predictor variables.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



