
Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Clinical outcomes of dental restorations depends primarily on the choice of materials used and their fabrication processes. The spectrum of dental CAD-CAM (Computer-Aided Design Computer-Aided Manufacturing) materials presents a wide range of variables on what may be the most suitable material for the clinical case. This narrative review focuses on CAD-CAM dental materials based on their mechanical properties and in relation to their clinical applications. A literature review was performed on PubMed, Scopus, Web of Knowledge, and Cochrane Library. Articles addressing at least one of the following topics regarding dental materials for CAD-CAM systems: manufacturers, mechanical features, materials ’composition optical properties, clinical indications and / or outcomes were included in the review. A flowchart was performed as de-scribed in the PRISMA guidelines. Among the 564 articles found, 63 were analyzed and evaluated. Within the limitation of this narrative review, it can be concluded that all CAD-CAM materials presents a wide range of clinical applications due to their improved mechanical properties. Specifically, in addition to materials that have been in use for a long time (such as feldspathic ceramics), resin block composites can also be used for permanent restorations.
Keywords:
CAD-CAM materials
; digital dentistry
; prosthodontics
1. Introduction
The introduction of “digital workflow” can be considered a turning point in dentistry [1]. In fact, the development of digital dentistry leads to an impressive change in daily clinical practice due to the synergy between new digital systems and considerable improvements in the mechanical and aesthetic features of dental materials produced with these technologies, thus reducing treatment times while maintaining high standards of precision and aesthetics [2,3]. Briefly, the dental digital workflow steps of CAD/CAM (Computer-Aided Design Computer-Aided Manufacturing) system are [4]:
- 1)
- Scanning dental record by an intraoral scanner connected to a dedicated software
- 2)
- Processing the digital data with a program that allows the visualization of the dental product
- 3)
- Manufacturing processes performed by subtractive (by milling it from a prefabricated block) or additive techniques [1]
CAD / CAM technology was first developed in the 80's. The idea of this system was the result of the collaboration of three research centers, the University of Zurich with the Brains and Brandestini Instruments of Switzerland, Hennson International of France, and the University of Minnesota center [5,6]. The purpose of the authors was to rehabilitate the patient with a prosthetic restoration in a short time and without the traditional impression-making method. Forward, the entire dental CAD-CAM system, including scanners, printers, and latest generation software, is revolutionizing the manufacturing process [5-7]. Among the strengths, previous studies reported greater efficiency and comfort of digital scanning compared to conventional impressions [7,8]. In fact, CAD-CAM restorations offer a good combination of esthetics, durability, and functionality in a single restoration [9]. It was reported that CAD-CAM restorations, such as fixed dental prostheses supported by natural teeth and implants, have sufficient marginal adaptation and lead to reduced plaque accumulation with a lower incidence of periodontal inflammation and development of caries. Intraoral scanner reduces the procedure time, increases patient comfort, and allows to reach an adequate level of precision (4 to 80 microns for scans with a limited area) [10]. Nevertheless, CAD-CAM technology is still considered quite expensive, and its application requires highly trained personnel, with a learning curve that can range from a few days to several months [11]. In addition, the survival rate of CAD-CAM restorations may differ based on the types of materials used. It is impossible to date to make comparisons between the conventionally and digitally realized prosthetic restorations in terms of survival rate. [10,11]. Several classifications about CAD-CAM materials have been described in literature, for example a classification made by materials, processing route and type of manufacturing [12-14]. Among the classifications made by material, the CAD-CAM materials can be classified as silicate ceramics, oxide ceramics, composite resins, PMMA (polymethyl methacrylate), PEEK, and PICN polymer infiltrated ceramic network material and of course metal [12]. Another type of classification is by its processing route, in fact they can be classified as Laboratory sides and Chairside [13]. A further classification has been recently considered, for example by additive or subtractive manufacturing [14]. The spectrum of dental CAD-CAM materials covers a wide range of compositions [15] as shown in Figure 1. Each material has different processing parameters and the whole system should be adapted based on the features of specific materials [16]. Dental CAD-CAM materials differ according to their composition and their mechanical and physical properties guide the dental practitioners to select the most appropriate material to be used [15,16]. Starting from the crucial role of recent CAD-CAM materials, this narrative review aims to identify the clinical applications of these materials related to the improvement of their mechanical characteristics.
2. Materials and Methods
2.1. Search strategy
This narrative review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement and the PICO(S) approach (Patient or Population, Intervention, Control or Comparison, Outcome, and Study types) [17] as shown in Figure 2. Extensive research on the literature and papers related to dental materials used for CAD-CAM restorations was performed on the databases of PubMed (Medline), Scopus, Web of Knowledge, and Cochrane Library. Additionally, the "snowballing" approach was used to identify further papers by reading the reference lists of records that have already been found. The research was performed by using combinations of the following keywords: "computer aided design " OR “cad/cam " OR “digital dentistry “AND “dental materials” OR “prosthetic dentistry” OR “restorative dentistry”. The search included only English-language articles and the electronic search of papers published in the last five years was conducted. The cut-off point (2017) was selected because the advancement rate in the technological level of scanner hardware and software and dental CAD-CAM material science has considerably improved in the last 5 year [14] The search strategy used a combination of free-text words. To exclude duplicates, the references of the identified records were uploaded as Research Information Systems files into Zotero (RRCHNM, Fairfax, Virginia). The PICO question was then chosen as follows: P-population: teeth to be partially or totally rehabilitated; I-intervention: CAD/CAM materials restorations; C-control: conventionally produced/manufactured restorations (natural teeth and implants); O-outcome: clinical applications; S-study designs: in vivo and in vitro study, systematic and narrative reviews. The search strategy according to the focused PICOS question is presented in Table 1.
2.2. Inclusion and exclusion criteria
Articles were considered appropriate when satisfying the following inclusion criteria:
- 1)
- Articles addressing at least one of the following topics regarding dental materials for CAD-CAM systems: clinical indications and/or outcomes, manufacturers, mechanical features (flexural strength, hardness, and elastic modulus) and materials’ composition or optical properties.
- 2)
- Studies performed in vitro or in vivo.
- 3)
- Systematic and Narrative reviews.
Articles that did not have the above information were excluded from the review.
3. Results
The search strategy reported 564 records, including duplicates: 246 from PubMed, 85 from Scopus, 155 from Web of Knowledge, 78 from Cochrane Library, and 15 with the “snowballing” approach. The duplicates were eliminated, thus all the selected databases produced 295 records. After the analysis of titles, abstracts, and mesh words, the researchers excluded 194 records which did not meet the inclusion criteria. Among the remaining 101 studies, 38 more were excluded after a full-text examination since these records did not present considerable information regarding the clinical applications of CAD/CAM dental materials in daily practice. The remaining 63 articles were included in this narrative review. The workflow of the review screening process is reported in Figure 2, in accordance with the “PRISMA 2009 Flow Diagram” [17]. Data obtained are the result of the correlation of the chemical-physical properties of the CAD - CAM materials in relation to their clinical outcomes as reported in Table 2 and Table 3.
4. Discussion
4.1. Silicate Ceramics (Glass Ceramics)
Chemically silica-based ceramics are non-metallic materials containing a glassy matrix. In general, the presence of glass in their compositions contributes to the brittleness, low fracture strength and resistance [18]. They are translucent and have excellent optical properties due to their natural appearance. In addition, they require hydrofluoric (HF) acid etching (to enhance micromechanical retention) and adhesive bonding (which can increase mechanical properties). After acid etching, the glassy matrix is dissolved, and crystalline phase is exposed so that the surface of the ceramic becomes suitable for the interlocking of resin cement. Among silicate ceramics, it is worth mentioning the following: traditional feldespathic, lithium silicate, lithium disilicate and leucite reinforced ceramics [19].
4.1.1. Feldespathic
This type of silicate ceramic is the first one used with CAD-CAM systems, especially by chairside. From a chemical point of view, they are considered ternary material systems composed of clay/kaolin, quartz (silica) and naturally occurring feldspar (a mixture of potassium and sodium aluminosilicate). Potassium feldspar (K2A12Si6O16) forms leucite crystals (crystalline phase) which, depending on the amount, increase the intrinsic strength of the restoration [20].
They have excellent optical properties, in fact their color and translucency are close to natural teeth, even if among the glass-based ceramics they are the weakest ones as they tend to fracture. In addition, they require etching with 9.6% hydrofluoric acid for 1 minute and then the silane application. That is why, they are indicated for inlay, onlay, anterior and posterior restorations and, in general, for veneers (also for veneering metal substructures, with a coefficient of thermal expansion approximately 10% or less) [20]. Cerec blocs Densply Sirona, Pennsylvania and Vitabloc Mark II, Real- Life, TriLuxe, VITA Zahnfabrik are the most representative blocs of this category [14,20].
4.1.2. Leucite-Reinforced
They are particle-filled glasses with a composition of the synthetic category (leucite-based, up to 45%) depending on the manufacturers [20,21]. In the literature, several benefits have been reached through reinforcing the matrix with leucite, thus improving the flexural strength (up to 104 Mpa) [21]. In addition, the reinforcement through leucite allows it to have a high thermal contraction coefficient [21]. Moreover, leucite-based ceramics present good translucency properties because their index of refraction is close to feldspathic glasses. Leucite reinforcement also permits a selected etching, thus ameliorating micromechanical bond [16]. Leucite-reinforced materials present high translucency and have great optical properties, which make it preferable to use them in esthetic areas compared to non-load bearing areas. A commercial example is represented by IPS Empress CAD, IPS Classic, Ivoclar Vivadent [19]. They are indicated for veneers, inlays, onlays, and single crowns [19].
4.1.3. Lithium silicate
Also, lithium silicate ceramics are included among silicate ceramics and could be considered as a progression of silicate ceramic [22]. From a chemical point of view, they are composed of a crystalline phase (lithium disilicate) and lithium orthophosphate. The mechanical strength of lithium silicate ceramics is increased thanks to the homogeneously dispersed crystalline phase. It is frequently enriched with Zirconia (approximately 10% of zirconia dioxide) thus combining very high mechanical properties and optical characteristics [23]. Lithium silicates have a flexural strength around 400Mpa, and good color stability compared to high-translucency zirconia or nanoceramics. VITA Suprinity PC by VITA Zahnfabrik, Celtra Duo by Densply Sirona are examples of lithium silicate ceramics. The use of silicate ceramics is limited to single crowns (better in anterior regions), veneers and inlays/onlays.
4.1.4. Lithium Disilicate
Lithium disilicate (Li2Si2O5) is characterized by 65% of lithium disilicate crystal, from 2 to 5 μm in length and 0.8 μm in diameter, inserted in an amorphous glassy matrix (in fact this is classified as a glass-ceramic). Thanks to its chemical composition (Li2Si2O5) lithium disilicate has great mechanical properties among which: flexural strength: 350 MPa, fracture toughness (KIC): 3.3 MPa m ½, heat extrusion temperature: 920° C, thermal expansion coefficient (CTE): 10.6 + 0.25 ppm/°C, high translucency [21,23,24].
Thanks to the high translucency of these ceramics, they are a popular choice for esthetic demanding cases, but the variability of flexural strength of CAD-CAM blocks depends on manufacturer [25]. These ceramic blocks showed good clinical success when used in non-load-bearing areas, but the good mechanical properties allow them to extend their applications, especially when it comes to veneers, inlays/onlays, single crowns or small bridges (up to 3 units). IPS e.max CAD by Ivoclar Vivadent is the most representative for this group of materials. According to a recent study, this presents a flexural strength of about 360 MPa. VITA Suprinity PC (VITA Zahnfabrik), Celtra Duo (Dentsply Sirona), and Obsidian (Glidewell Laboratories, Newport Beach, California) are commercial examples [23,25].
4.2. Oxide Ceramics
These materials have very favorable mechanical properties, and they are mainly suggested for crowns, implant components, and Fixed Dental Prosthesis (FDPs) with multiple units in anterior and posterior areas, even if their aesthetic properties are somewhat inferior to silicate ceramics [26].
4.2.1. Zirconium oxide ceramics
Chemically, zirconia is a metal oxide with polymorphism and allotropy properties defined as an “all-ceramic” material in dentistry. Moreover, it has different crystallographic structures such as monoclinic, tetragonal, and cubic that could differentiate the mechanical and optical characteristics [27]. Above 2370 ºC, the oxide zirconium assumes the cubic structure; between 2370 ºC and 1170 ºC a tetragonal structure and below 1170 ºC, the monoclinic one. Therefore, while it is cooled to room temperature, this assumes the monoclinic structure, a stable crystalline configuration unfortunately poorly resistant to repeated mechanical stress. They are composed in the form of Yttria-stabilized tetragonal zirconia polycrystal (Y-TZP). The presence of yttrium oxide, at different concentration percentages (3-5%), decreases their mechanical properties. Y-TZP shows optimal mechanical properties and a remarkable fracture resistance, from 5 to 10 MPa√m, as well as a flexural strength of 900-1400 MPa [28]. Some commercial examples are: Nobelprocera Zirconia, Nobel Biocare; Lava Plus,3M ESPE. Several articles demonstrated a survival rate up to 100% after 5 years with FDPs rehabilitation [29,30].
Due to their excellent mechanical properties and above all their optical properties, the application of these CAD-CAM materials is very wide, and they can be used for single crown or multiple rehabilitation (bridges in anterior or posterior region, up to entire full-arch rehabilitations on implants or natural teeth) [31].
4.2.2. Aluminum oxide ceramics
They are composed of glass-infiltrated aluminum oxide core ceramics. Specifically, the chemical composition is made of densely packed sintered Al2O3 (80 to 82 wt%) as ceramic core material followed by an infiltration with molten glass. The flexural strength is about 500 Mpa, so they are recommended for the fabrication of anterior three-unit fixed dental prosthesis, crowns and for posterior rehabilitation [32]. The most famous commercial examples are InCeram Alumina, VITA Zahnfabrik, Bad Sackingen, Germany [32]. In general, alumina crowns show acceptable long-term survival rates, thus demonstrating up to 100% of survival rates after a 7-year period [33,34].
4.3. Hybrid Ceramics
4.3.1. PICN
Polymer infiltrated ceramic network (PICN) material has both ceramic and polymer properties. It is defined as a double mesh hybrid material, with ceramic and polymer. The PICN polymerization process involves the production of a presintered porous ceramic network that is infiltrated by a polymer in a capillary manner. PICN has better wear resistance than composite resins and exhibits high flexural strength and elasticity like that of dentin [35]. The dominant ceramic network demonstrates to have a good wear resistance and the interpenetration of ceramic and polymer prevents crack propagation in the material. As a newly introduced material, there are still no studies with long-term follow-up PICN restorations. The color range of the material is limited, there are no adequate follow-ups for its durability on cervical areas and discolorations [36]. The PICN is indicated for veneers, inlays / onlays, anterior and posterior single crowns and for implant prostheses. However, this material is more suitable for posterior reconstructions due to the lower aesthetic yield [35,36]. PICN composite CAD/CAM blocks have been applied to indirect tooth restoration, where several basic and clinical studies have used a commercially available PICN composite named VITA ENAMIC, which comprises a silicate glass ceramic skeleton with infiltrated acrylic resin [37]. Previous studies demonstrated how PICN composites suitably mimic human enamel, specifically in terms of mechanical features [38,39].
4.3.2. Nanoceramics
Nanoceramics have the same resin composite microstructure but in different portions. They have a polymeric matrix and a filler of ceramic nanoparticles (size less than 100 nm) about 80% of weight. These fillers may be composed of conventional ceramic, polycrystalline ceramic (zirconia), or a combination of both [40]. Nanoceramics have characteristics similar to the natural tooth. In fact, they present a flexural strength usually close to 200 MPa, a compression strength up to 380 MPa, and an abrasion rate around 2 to 10 microns per year. The elastic modulus is around 15 GPa [40,41]. These characteristics indicate these materials for single tooth restoration or small bridges, preferably in the posterior area and the moke-up allows a possible application in the anterior sector [42]. However, the matrix is a polymer that will wear faster than the ceramic, making it more abrasive than antagonists compared to traditional ceramics [43]. These materials are indicated for veneers, inlay / onlay, anterior and posterior single crowns, anterior and posterior bridges [42,43].
Lava Ultimate (3M ESPE, USA) is in the group of nanoceramics and used in conjunction with CAD / CAM systems [44]. As a reason of the strong chemical bonds formed between nanoceramic structure and resin, the material has high fracture strength. Besides, fexural strength of the material is 200 MPa [45]. Lauvahutanon et al. reported the elastic modulus of Lava Ultimate as 29.8 GPa and stated that this value is very close to the dentin [46]. For this reason, it was thought that the force-absorbing property of the material is high enough and this allows fabrication of posterior nanoceramic restorations [47].
4.4. Resin Matrix Ceramics
4.4.1. PMMA
PMMA (IUPAC name: poly [1- (methoxy carbonyl) -1-methyl ethylene]) is a synthetic polymer prepared by the free radical addition and polymerization of methyl methacrylate (C5O2H8) to poly methyl methacrylate (C5O2H8) n [48]. PMMA gained popularity in the dentistry field due to its peculiar features such as its low density, good aesthetics, cost-effectiveness, ease of handling and modular physical and mechanical properties [49].
Increased interest in PMMA restorations encouraged the development of PMMA blocks with enhanced optical and physical properties, (eg, Telio CAD, Ivoclar Vivadent, Shaan, Liechtenstein and VITA CAD-Temp MultiColor Blocks, VITA Zahnfabrik, Bad Sackingen, Germany) [50-52]. Heat-cured PMMA restorations are easily polished to achieve enhanced aesthetics. PMMA is commonly used for prosthetic dental applications, including the fabrication of artificial teeth, denture bases, dentures, obturators, orthodontic retainers, temporary or provisional crowns, and for the repair of dental prostheses [52].
Although the chemistry of CAD / CAM PMMA is similar to that of conventional heat cured PMMA, CAD / CAM PMMA exhibits superiority in hardness, flexural strength, flexural modulus and impact strength [53]. The improvement of these mechanical properties has led to the use of CAD / CAM PMMA fixed even when a long term (up to one year) provisional restoration is required [54-56]. Moreover, the increased hydrophobicity of CAD / CAM PMMA compared to the conventional one reduces the accumulation of plaque on the surfaces of CAD / CAM prostheses and a reduced adhesion of Candida Albicans, the main pathogen of prosthetic stomatitis, has also been reported [57].
4.4.2. PEEK
Polyetheretherketone (PEEK) is a semi-crystalline thermoplastic polymer used in the dental field as a material for metal-free structures, removable fixed dental prostheses, fixed prostheses supported by implants, overdentures retained by implants, endocrowns and fixed dental prostheses bonded with resin [58].
PEKK exhibits good wear resistance, low tendency to retain plaque and high bond strength with veneering composites and luting cements, moreover, has a low modulus of elasticity of 4 GPa, and is as elastic as bone, providing a cushioning effect and reduction of the stresses transferred to the abutment teeth [59]. Accuracy of fit of removable partial dentures fabricated by conventional techniques and CAD / CAM PEEK dentures have been compared with the latter resulting in comparable, and in some instances, a more superior fit to conventional techniques [60,61]. Moreover, the two-body wear test of PEEK was more favorable compared to the other CAD / CAM composite resin and PMMA material. In vitro testing of PEEK molar crowns fabricated on zirconia and titanium abutments in a chewing simulator resulted in acceptable fracture strength property, recommending them for clinical application [62]. However, this material is not available nowadays for clinical use as clinical studies on their performance are lacking.
Among the most used CAD/CAM PEEK manufacturers PEEK “blanks” (Juvora dental PEEK CAD/CAM-Rohling, Straumann, Basel, Switzerland) can be applied to mill frameworks for dentures or FDPs and BioHPP™ (Bio High Performance Polymer, Bredent, Senden, Germany) is approved by the manufacturer for three to four-unit FDPs, telescopic restorations, implant abutments, and secondary structures associated with bar-supported prostheses [63,64].
4.4.3. Resin Composite Blocks (RCBs)
Resin Composite Blocks (RCBs) designed for CAD / CAM are produced by the incorporation of filler particles into a mixture of monomers that are cured under high temperature and high pressure [65-67]. This polymerization method allows, compared to traditional resin composites, a greater homogeneity of the material with a lower presence of defects and pores and a greater degree of conversion that reduces the absorption of water improving mechanical features such as resistance to fracture, resistance to bending and wear [68]. Most CAD / CAM RCBs have urethanodimethacrylate (UDMA) as a polymer matrix which has a lower solubility and water absorption capacity, allowing the restorations to have greater color stability [69]. Furthermore, these new dimethacrylates have an addition-fragmentation monomer with an enhancement of their translucency, which can promote the increase of DC and hardness (VH) during polishing procedures, achieving an optimum clinical performance [70]. The Paradigm MZ100 (3M Oral Care, Seefeld, Germany) was the first CAD / CAM composite material with a flexural strength of 157 MPa, similar to that of feldspar ceramic materials [71]. Other examples of RCB CAD / CAM include:
- -
- Tetric CAD (Ivoclar Vivadent, Liechtenstein) is a resinous matrix consisting of Bis-GMA, Bis-EMA, TEGDMA, UDMA, filled with 70% barium glass and silicon dioxide particles. This composite has a flexural strength of 273.8 MPa and an elastic modulus of 10.2 GPa [72].
- -
- LuxaCam Composite (LUXA) (DMG; Hamburg, Germany) is a resin matrix composed of 70% silicate-glass filling particles. This composite demonstrates a flexural strength of 164 MPa and an elastic modulus of 10.1 GPa. [73].
- -
- Grandio Blocks (VOCO GmbH, Germany) is a resin matrix highly nanohybrid filled (86%) with a flexural strength of 330 MPa and an elastic modulus of 18 GPa offer physical properties that mimic natural human tissues, such as thermocycling. [74-75].
These CAD / CAM composites, according to the manufacturers' indications, can be used to perform inlays, onlays, veneers, partial crowns, crowns, and multi-unit, up to three bridge units [72].
5. Conclusions
Within the limitation of this narrative review, it can be concluded that Silicate ceramics (Feldspathic, Leucite Reinforced, Lithium Silicate and Lithium Disilicate), presents high success rate for single crown restoration. Lithium Silicate and Disilicate, due to their high value of translucency, are recommended for the anterior restorations. Regarding oxide ceramics, the clinical application of Aluminium and especially Zirconium, is very broad (Zirconium is used for bridges in anterior or posterior region, up to entire full-arch rehabilitations on implants or natural teeth). As for Hybrid Ceramics, the use of PICN (Polymer infiltrated ceramic network) is indicated for inlays / onlays, and in general for posterior single crowns, due to their lower aesthetic yield. Among Resin Matrix Ceramics, PMMA(Polymethylmethacrylate) is used for temporary or provisional crowns, and PEEK (Polyetheretherketone) is a good choice for metal-free structures, endocrowns and fixed dental prostheses. Recently, Resin composite blocks, thanks to the improvement of their mechanical and aesthetic properties, are becoming real alternatives for definitive restorations such as inlays, onlays, veneers, partial crowns, and bridges (also multi-unit, up to three bridge units).
Author Contributions
Conceptualization, B.S., and S.C.; methodology, I.R. and M.S.; software, G.D., I.R. and M.S.; validation, B.S.; formal analysis, I.R., M.S., E.M. and G.T.; investigation, I.R.; resources, S.C.; data curation, G.D., M.S. and I.R.; writing—original draft preparation, I.R. and M.S.; writing—review and editing, B.S.; visualization, S.C., and B.S.; supervision, B.S.; project administration, B.S., and S.C.; funding acquisition, B.S. and S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Barenghi, L.; Barenghi, A.; Garagiola, U.; Di Blasio, A.; Giannì, A.B.; Spadari, F. Pros and Cons of CAD/CAM Technology for Infection Prevention in Dental Settings during COVID-19 Outbreak. Sensors (Basel) 2021, 22, 49. [Google Scholar] [CrossRef]
- Orsini, G.; Tosco, V.; Monterubbianesi, R.; Orilisi, G.; Putignano, A. A New Era in Restorative Dentistry. In The First Out-Standing 50 Years of “Università Politecnica delle Marche”: Research Achievements in Life Sciences; Longhi, S., Monteriù, A., Freddi, A., Aquilanti, L., Ceravolo, M.G., Carnevali, O., Giordano, M., Moroncini, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 319–334. ISBN 978-3-030-33832-9. [Google Scholar]
- Tapie, L.; Lebon, N.; Mawussi, B.; Fron Chabouis, H.; Duret, F.; Attal, J.P. Understanding dental CAD/CAM for restorations--the digital workflow from a mechanical engineering viewpoint. Int J Comput Dent. 2015, 18, 21–44. [Google Scholar] [PubMed]
- Ahmed, K.E. We're Going Digital: The Current State of CAD/CAM Dentistry in Prosthodontics. Prim Dent J. 2018, 7, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Li, R.W.K.; Chow, T.W.; Matinlinna, J.P. Ceramic dental biomaterials and CAD/CAM technology: State of the art. J. Prosthodont. Res. 2014, 58, 208–216. [Google Scholar] [CrossRef]
- Papadiochou, S.; Pissiotis, A.L. Marginal adaptation and CAD-CAM technology: A systematic review of restorative material and fabrication techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Otto, T.; Dent, M. Case series Clinical Results from a Long-Term Case Series using Chairside CEREC CAD-CAM Inlays and Onlays. Int. J. Prosthodont. 2008, 21, 53–59. [Google Scholar]
- Alghazzawi, T.F. Advancements in CAD/CAM technology: Options for practical implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef]
- Saponaro, P.C.; Yilmaz, B.; Heshmati, R.H.; McGlumphy, E.A. Clinical performance of CAD-CAM-fabricated complete dentures: A cross-sectional study. J. Prosthet. Dent. 2016, 116, 431–435. [Google Scholar] [CrossRef]
- Vecsei, B.; Joós-Kovács, G.; Borbély, J.; Hermann, P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems—An In Vitro study. J. Prosthodont. Res. 2017, 61, 177–184. [Google Scholar] [CrossRef]
- Grzebieluch, W.; Mikulewicz, M.; Kaczmarek, U. Resin Composite Materials for Chairside CAD/CAM Restorations: A Comparison of Selected Mechanical Properties. J Healthc Eng. 2021, 8828954. [Google Scholar] [CrossRef]
- Tiu, J.; Belli, R.; Lohbauer, U. Contemporary CAD/CAM Materials in Dentistry. Curr Oral Health Rep. 2019, 6, 250–256. [Google Scholar] [CrossRef]
- Sulaiman, T.A. Materials in digital dentistry-A review. J Esthet Restor Dent. 2020, 32, 71–181. [Google Scholar] [CrossRef]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Lambert, H.; Durand, J.C.; Jacquot, B.; Fages, M. Dental biomaterials for chairside CAD/CAM: State of the art. J. Adv. Prosthodont. 2017, 9, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D. G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P. C.; Ioannidis, J. P.; Clarke, M.; Devereaux, P. J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ (Clinical research ed.) 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Skorulska, A.; Piszko, P.; Rybak, Z.; Szymonowicz, M.; Dobrzyński, M. Review on Polymer, Ceramic and Composite Materials for CAD/CAM Indirect Restorations in Dentistry-Application, Mechanical Characteristics and Comparison. Materials 2021, 14, 1592. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R. Novel zirconia materials in dentistry. J Dent Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.; Bonfante, E.A. A new classification system for all-ceramic and ceramic-like restorative materials. Int J Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H. Craig's Restorative Dental Materials, 14th Ed. ed; United Kingdom, 2019; p. 226. [Google Scholar]
- Hinz, S.; Bensel, T.; Bömicke, W.; Henningsen, A.; Rudolph, J.; Boeckler, A.F. Impact of the Veneering Technique and Framework Material on the Failure Loads of All-Ceramic Computer-Aided Design/Computer-Aided Manufacturing Fixed Partial Dentures. Materials (Basel). 2022, 15, 756. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Rollo, M.L.; Cardelli, P.; Rexhepi, I.; Murmura, G.; Al-Haj Husain, N.; Sinjari, B.; Traini, T.; Özcan, M.; Caputi, S. Fracture Resistance of Zirconia-Reinforced Lithium Silicate Ceramic Crowns Cemented with Conventional or Adhesive Systems: An In Vitro Study. Materials 2020, 13, 2012. [Google Scholar] [CrossRef]
- Mavriqi, L.; Valente, F.; Murmura, G.; Sinjari, B.; Macrì, M.; Trubiani, O.; Caputi, S.; Traini, T. Lithium disilicate and zirconia reinforced lithium silicate glass-ceramics for CAD/CAM dental restorations: biocompatibility, mechanical and microstructural properties after crystallization. J Dent. 2022, 119, 104054. [Google Scholar] [CrossRef]
- Fabian Fonzar, R.; Carrabba, M.; Sedda, M.; Ferrari, M.; Goracci, C.; Vichi, A. Flexural resistance of heat-pressed and CAD-CAM lithium disilicate with different translucencies. Dental materials: official publication of the Academy of Dental Materials. 2017, 33, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Gardell, E.; Larsson, C.; von Steyern, P. V. Translucent Zirconium Dioxide and Lithium Disilicate: A 3-Year Follow-up of a Prospective, Practice-Based Randomized Controlled Trial on Posterior Monolithic Crowns. The International journal of prosthodontics 2021, 34, 163–172. [Google Scholar] [CrossRef]
- Traini, T.; Gherlone, E.; Parabita, S.F.; Caputi, S.; Piattelli, A. Fracture toughness and hardness of a Y-TZP dental ceramic after mechanical surface treatments. Clin Oral Investig. 2014, 18, 707–14. [Google Scholar] [CrossRef]
- Guazzato, M.; Albakry, M.; Ringer, S.P.; Swain, M.V. Strength, fracture toughness, and microstructure of a selection of all-ceramic materials. Part II. Zirconia-based dental ceramics. Dent Mater 2004, 20, 449–56. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.; Caldari, M.; Scotti, R.; Group, A.C.R. Clinical evaluation of tooth-supported zirconia-based fixed dental prostheses: a retrospective cohort study from the AIOP clinical research group. Int. J.Prosthodont. 2015, 28, 236–8. [Google Scholar] [CrossRef]
- Pihlaja, J.; Näpänkangas, R.; Raustia, A. Outcome of zirconia partial fixed dental prostheses made by predoctoral dental students: A clinical retrospective study after 3 to 7 years of clinical service. J Prosthet Dent. 2016, 116, 40–46. [Google Scholar] [CrossRef]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N. U. Time-efficiency and cost-analysis comparing three digital workflows for treatment with monolithic zirconia implant fixed dental prostheses: A double-blinded RCT. Journal of dentistry 2021, 113, 103779. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M. A.; Skroch, M.; Schmidt, A.; Rehmann, P.; Wöstmann, B. Monitoring fatigue damage in different CAD/CAM materials: A new approach with optical coherence tomography. Journal of prosthodontic research. 2021, 65, 31–38. [Google Scholar] [CrossRef]
- Ozer, F.; Mante, F.K.; Chiche, G.; Saleh, N.; Takeichi, T.; Blatz, M.B. A retrospective survey on long-term survival of posterior zirconia and porcelain-fused-to-metal crowns in private practice. Quintessence Int. 2014, 45, 31–38. [Google Scholar]
- Selz, C.F; Strub, J.R; Vach, K.; Guess, P.C. Long-term performance of posterior InCeram Alumina crowns cemented with different luting agents: a prospective, randomized clinical split-mouth study over 5 years. Clin. Oral Investig. 2014, 18, 1695–703. [Google Scholar] [CrossRef]
- Kawajiri, Y.; Ikeda, H.; Nagamatsu, Y.; Masaki, C.; Hosokawa, R.; Shimizu, H. PICN Nanocomposite as Dental CAD/CAM Block Comparable to Human Tooth in Terms of Hardness and Flexural Modulus. Materials. 2021, 14, 1182. [Google Scholar] [CrossRef]
- Kang, L.; Zhou, Y.; Lan, J.; Yu, Y.; Cai, Q.; Yang, X. Effect of resin composition on performance of polymer-infiltrated feldsparnetwork composites for dental restoration. Dent. Mater. J. 2020, 39, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Steinbrenner, H. Multichromatic and highly translucent hybrid ceramic Vita Enamic. International journal of computerized dentistry. 2018, 21, 239–250. [Google Scholar] [PubMed]
- Yano, H.T.; Ikeda, H.; Nagamatsu, Y.; Masaki, C.; Hosokawa, R.; Shimizu, H. Correlation between microstructure of CAD/CAM composites and the silanization effect on adhesive bonding. J. Mech. Behav. Biomed. Mater. 2020, 101, 103441. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Kou, H.; Rao, J.; Liu, C.; Ning, C. Fabrication of enamel-like structure on polymer-infiltrated zirconia ceramics. Dent. Mater. 2021, 37, e245–e255. [Google Scholar] [CrossRef]
- Demirel, A.; Bezgin, T.; Akaltan, F.; Sarı, Ş. Resin Nanoceramic CAD/CAM Restoration of the Primary Molar: 3-Year Follow-Up Study. Case Rep Dent. 2017; 3517187. [Google Scholar]
- Heck, K.; Paterno, H.; Lederer, A.; Litzenburger, F.; Hickel, R.; Kunzelmann, K.H. Fatigue resistance of ultrathin CAD/CAM ceramic and nanoceramic composite occlusal veneers. Dent Mater. 2019, 35, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Al Amri, M.D.; Labban, N.; Alhijji, S.; Alamri, H.; Iskandar, M.; Platt, J.A. In Vitro Evaluation of Translucency and Color Stability of CAD/CAM Polymer-Infiltrated Ceramic Materials after Accelerated Aging. J Prosthodont. 2021, 30, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, F.A; Ayad, N.M.; ArRejaie, A.S.; Bahgat, H.A.; Baba, N.Z. Effect of Aging Regimens on Resin Nanoceramic Chairside CAD/CAM Material. J Prosthodont. 2017, 26, 432–439. [Google Scholar] [CrossRef]
- Yin, R.; Kim, Y.K.; Jang, Y.S.; Lee, J.J.; Lee, M.H.; Bae, T.S. Comparative evaluation of the mechanical properties of CAD/CAM dental blocks. Odontology. 2019, 107, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Ludovichetti, F.S.; Trindade, F.Z; Werner, A。; Kleverlaan, C.J.; Fonseca, R.G. Wear resistance and abrasiveness of CAD-CAM monolithic materials. J Prosthet Dent. 2018, 120, 318.e1–318.e8. [Google Scholar] [CrossRef]
- Lauvahutanon, S.; Shiozawa, M.; Takahashi, H.; Iwasaki, N.; Oki, M.; Finger, W. J.; Arksornnukit, M. Discoloration of various CAD/CAM blocks after immersion in coffee. Restorative dentistry & endodontics. 2017, 42, 9–18. [Google Scholar]
- Kurtulmus-Yilmaz, S.; Cengiz, E.; Ongun, S.; Karakaya, I. The Effect of Surface Treatments on the Mechanical and Optical Behaviors of CAD/CAM Restorative Materials. J Prosthodont. 2019, 28, e496–e503. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S. Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update. Polymers (Basel). 2020, 12, 2299. [Google Scholar] [CrossRef]
- Hassan, M.; Asghar, M.; Din, S.U.; Zafar, M.S. Chapter 8. In Thermoset Polymethacrylate-Based Materials for Dental Applications; Elsevier: Amsterdam, The Netherlands, 2019; pp. 273–308. [Google Scholar]
- Arslan, M.; Alp, G.; Zaimoglu, A.; Murat, S. Evaluation of flexural strength and surface properties of pre-polymerized CAD/CAM PMMA-based polymers used for digital 3D complete dentures. Int J Comput Dent. 2018, 21, 31–40. [Google Scholar] [PubMed]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J. A comparison of the flexural and impact strengths and flexural modulus of CAD/CAM and conventional heat-cured polymethyl methacrylate (PMMA). J Prosthodont. 2018, 1–9. [Google Scholar] [CrossRef]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J; Ozcan, M. A comparison of the surface properties of CAD/CAM and conventional polymethylmethacrylate (PMMA). J Prosthodont. 2019, 28, 452–457. [Google Scholar] [CrossRef]
- Bidra, A.S.; Taylor, T.D.; Agar, J.R. Computer-aided technology for fabricating complete dentures: Systematic review of historical background, current status, and future perspectives. J. Prosthet. Dent. 2013, 109, 361–366. [Google Scholar] [CrossRef]
- Choi, J.J.E.; Uy, C.E.; Plaksina, P.; Ramani, R.S.; Ganjigatti, R.; Waddell, J.N. Bond Strength of denture teeth to heat-cured, CAD/CAM and 3D printed denture acrylics. J. Prosthodont. 2020, 29, 415–421. [Google Scholar] [CrossRef]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef]
- de Oliveira Limírio, J.; Gomes, J.; Alves Rezende, M.; Lemos, C.; Rosa, C.; Pellizzer, E. P. Mechanical properties of polymethyl methacrylate as a denture base: Conventional versus CAD-CAM resin - A systematic review and meta-analysis of in vitro studies. The Journal of prosthetic dentistry 2021. [Google Scholar] [CrossRef] [PubMed]
- Murat, S.; Alp, G.; Alatalı, C.; Uzun, M. In vitro evaluation of adhesion of candida albicans on CAD/CAM PMMA-based polymers. J. Prosthodont. 2019, 28, 873–879. [Google Scholar] [CrossRef]
- Papathanasiou, I.; Kamposiora, P.; Papavasiliou, G.; Ferrari, M. The use of PEEK in digital prosthodontics: A narrative review. BMC Oral Health. 2020, 20, 217. [Google Scholar] [CrossRef]
- Alexakou, E.; Damanaki, M.; Zoidis, P.; Bakiri, E.; Mouzis, N.; Smidt, G.; Kourtis, S. PEEK high performance polymers: a review of properties and clinical applications in prosthodontics and restorative dentistry. Eur J Prosthodont Restor Dent. 2019, 27, 113–21. [Google Scholar]
- Muhsin, S.A.; Wood, D.J.; Johnson, A.; Hatton, V.P. Effects of novel polyetheretherketone (PEEK) clasp design on retentive force at different tooth undercuts. J Oral Dent Res. 2018, 5, 13–25. [Google Scholar]
- Peng, T.Y.; Ogawa, Y.; Akebono, H.; Iwaguro, S.; Sugeta, A.; Shimoe, S. Finite element analysis and optimization of the mechanical properties of polyetheretherketone (PEEK) clasps for removable partial dentures. J Prosthodont Res. 2020, 64, 250–6. [Google Scholar] [CrossRef]
- Negm, E.E.; Aboutaleb, F.A.; Alam-Eldein, A.M. Virtual evaluation of the accuracy of fit and trueness in maxillary poly (etheretherketone) removable partial denture frameworks fabricated by direct and indirect CAD/CAM techniques. J Prosthodont. 2019, 28, 804–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, P.; Liu, H. L.; Zhang, L.; Liu, L. P.; Ma, C. F.; Chen, J. H. Polyetheretherketone versus titanium CAD-CAM framework for implant-supported fixed complete dentures: a retrospective study with up to 5-year follow-up. Journal of prosthodontic research 2021. [Google Scholar] [CrossRef]
- Arnold, C.; Hey, J.; Schweyen, R.; Setz, J.M. Accuracy of CAD-CAM-fabricated removable partial dentures. J Prosthet Dent. 2018, 119, 586–92. [Google Scholar] [CrossRef] [PubMed]
- Alamoush, R.A.; Silikas, N.; Salim, N.A.; Al-Nasrawi, S.; Satterthwaite, J.D. Effect of the Composition of CAD/CAM Composite Blocks on Mechanical Properties. BioMed Res Int. 2018, 4893143. [Google Scholar] [CrossRef] [PubMed]
- Alamoush, R.A.; Salim, N.A.; Silikas, N.; Satterthwaite, J.D. Long-term hydrolytic stability of CAD/CAM composite blocks. Eur J Oral Sci. 2022, 130, e12834. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, A.S.Q.S.; Labruna Moreira, A.D.; de Albuquerque, P.P.A.C.; de Menezes, L.R.; Pfeifer, C.S.; Schneider, L.F.J. Effect of monomer type on the CC degree of conversion, water sorption and solubility, and color stability of model dental composites. Dent Mater. 2017, 33, 394–401. [Google Scholar] [CrossRef]
- Marchesi, G.; Camurri Piloni, A.; Nicolin, V.; Turco, G.; Di Lenarda, R. Chairside CAD/CAM Materials: Current Trends of Clinical Uses. Biology (Basel). 2021, 10, 1170. [Google Scholar] [CrossRef]
- Liebermann, A.; Wimmer, T.; Schmidlin, P.R.; Scherer, H.; Löffler, P.; Roos, M.; Stawarczyk, B. Physico Mechanical Characterization of polyetheretherketone and current esthetic dental CAD/CAM polymers after aging in different storage media. J Prosthet Dent. 2016, 115, 321–328.e2. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Tosco, V.; Sabbatini, S.; Orilisi, G.; Conti, C.; Özcan, M.; Orsini, G.; Putignano, A. How Can Different Polishing Timing Influence Methacrylate and Dimethacrylate Bulk Fill Composites? Evaluation of Chemical and Physical Properties. Biomed Res Int. 2020, 1965818. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, A.; Ardu, S.; Bortolotto, T.; Krejci, I. Stain susceptibility of composite and ceramic CAD/CAM blocks versus direct resin composites with different resinous matrices. Odontology. 2017, 105, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Grzebieluch, W.; Mikulewicz, M.; Kaczmarek, U. Resin Composite Materials for Chairside CAD/CAM Restorations: A Comparison of Selected Mechanical Properties. J Healthc Eng. 2021, 8828954. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Skroch, M.; Schmidt, A.; Rehmann, P.; Wöstmann, B. Influence of Different Luting Systems on Microleakage of CAD/CAM Composite Crowns: A Pilot Study. Int J Prosthodont. 2019, 32, 530–532. [Google Scholar] [CrossRef]
- Vichi, A.; Goracci, C.; Carrabba, M.; Tozzi, G.; Louca, C. Flexural resistance of CAD-CAM blocks. Part 3: Polymer-based restorative materials for permanent restorations. Am J Dent. 2020, 33, 243–247. [Google Scholar]
- Wendler, M.; Stenger, A.; Ripper, J.; Priewich, E.; Belli, R.; Lohbauer, U. Mechanical degradation of contemporary CAD/CAM resin composite materials after water ageing. Dental materials: official publication of the Academy of Dental Materials 2021, 37, 1156–1167. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Classification of CAD-CAD materials based on their composition in dentistry.
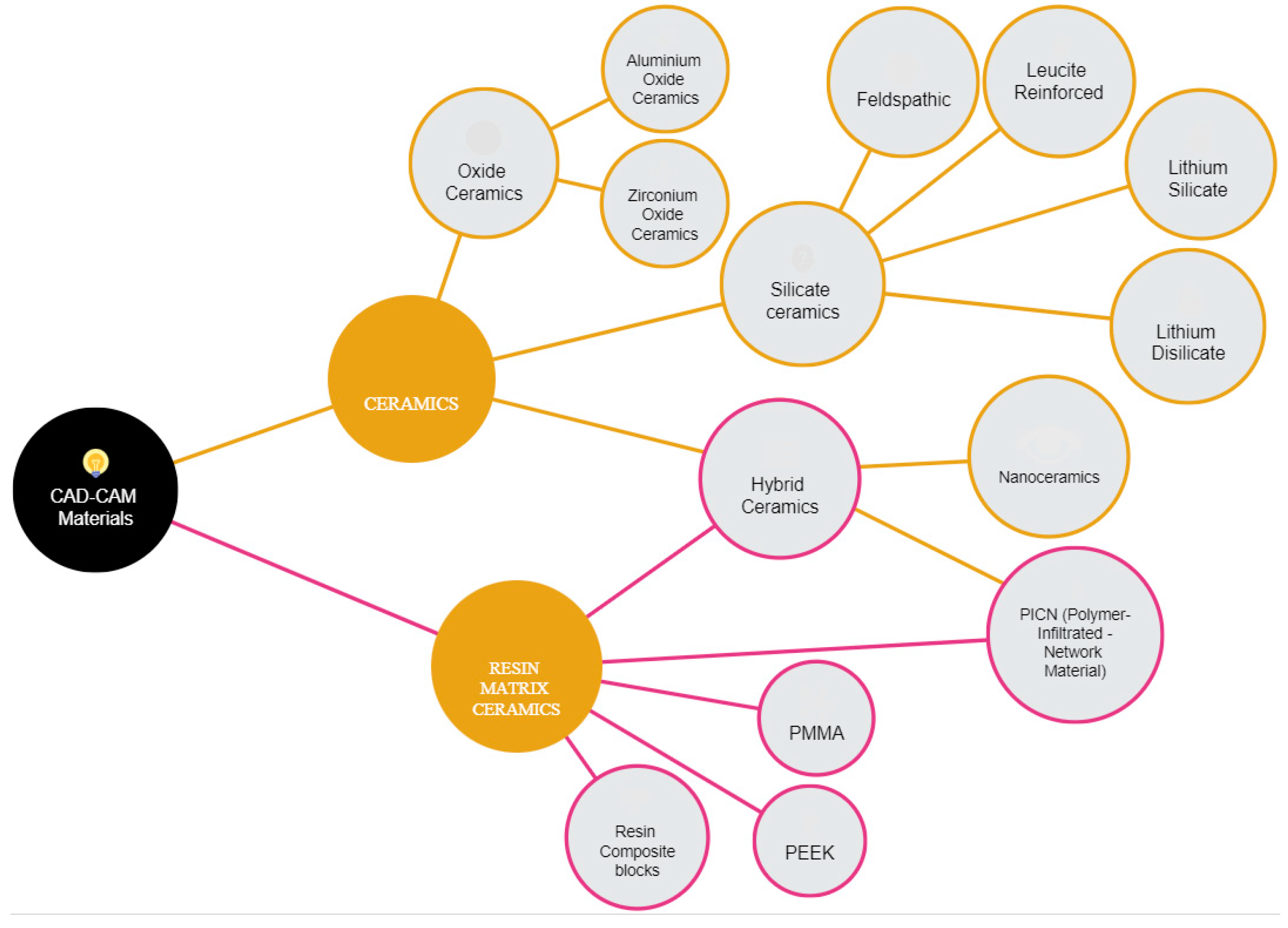
Figure 2.
Search flowchart as described in the PRISMA guidelines. Caption: (n = number of records).
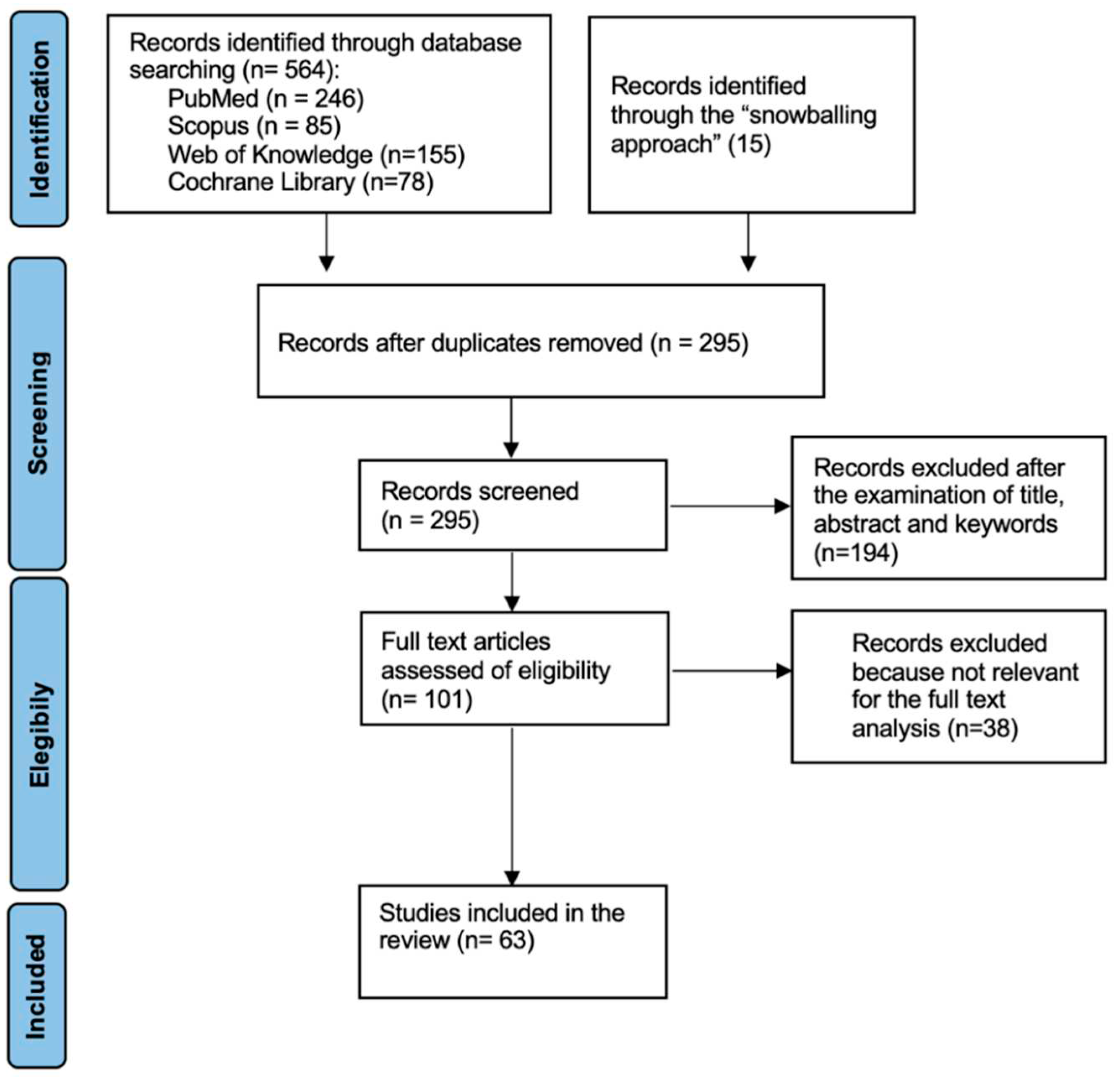

Table 1.
Search strategy according to the focused question (PICO).
| Focused Question (PICO) | Is there a greater range of clinical applications of CAD / CAM materials than traditional ones due to the improvement of their mechanical properties? |
|
|---|---|---|
|
Search strategy |
Population | teeth to be partially or totally rehabilitated |
| Intervention | CAD/CAM restorations. |
|
| Comparison | Conventionally manufactured restorations. | |
| Outcome | Clinical Application of these materials | |
Table 2.
Clinical application of CAD/CAM Materials included in the study.
| Materials | Clinical Application | References |
|---|---|---|
| Silicate Ceramics | ||
| Feldespathic | inlay, onlay, anterior and posterior restorations and for veneers | Sulaiman T. A. (2020) [14], Gracis, Stefano et al. (2015) [20] |
| Leucite-reinforced | veneers, inlays, onlays, and single crowns | Zhang Y et al (2018) [19], Gracis, Stefano et al. (2015) [20], H Ahmed et al. (2019) [21] |
| Lithium disilicate | veneers, inlays/onlays, single crowns or small bridges (up to 3 units) | H Ahmed et al. (2019) [21] Hinz, Sebastian et al. (2022) [22] D'Addazio, Gianmaria et al. (2020) [23] Mavriqi, Luan et al. (2021) [24] Fabian Fonzar, Riccardo et al. (2017) [25] |
| Lithium silicate | single crowns (better in anterior regions), veneers and inlays/onlays | Hinz, Sebastian et al. (2022) [22] D'Addazio, Gianmaria et al. (2020) [23] |
| Oxide Ceramics | ||
| Zirconium | bridges in anterior or posterior region, up to entire full-arch rehabilitations on implants or natural teeth | Traini, Tonino et al. (2014) [27] Guazzato, Massimiliano et al. (2004) [28] Monaco, Carlo et al. (2015) [29] Pihlaja, Juha et al. (2016) [30] Joda, Tim et al. (2021) [31] |
| Aluminum | anterior three-unit fixed dental prosthesis, crowns and for posterior rehabilitation | Schlenz, Maximiliane Amelie et al. (2021) [32] Ozer, Fusun et al. (2014) [33] Selz, Christian F et al. (2014) [34] |
| Resin Matrix Ceramics | ||
| PMMA | long term (up to one year) provisional restoration | Zafar, Muhammad Sohail (2020) [48] Hassan, M et al. (2019) [49] Arslan, Mustafa et al. (2018) [50] Al-Dwairi, Ziad N et al. (2018) [51] Al-Dwairi, Ziad N et al. (2019) [52] Bidra, Avinash S et al. (2013) [53] Choi, Joanne Jung Eun et al. (2020) [54] Kalberer, Nicole et al. (2019) [55] de Oliveira Limírio, João Pedro Justino et al. (2021) [56] Murat, Sema et al. (2019) [57] |
| PEEK | mill frameworks for dentures or FDPs, three to four-unit FDPs, telescopic restorations, implant abutments, and secondary structures associated with bar-supported prostheses | Papathanasiou, Ioannis et al. (2020) [58] Alexakou, E et al. (2019) [59] Muhsin, S.A et al. (2018) [60] Peng, Tzu-Yu et al. (2020) [61] Negm, Enas Elhamy et al. (2019) [62] Wang, Jing et al. (2021) [63] Arnold, Christin et al. (2018) [64] |
| Resin Block Composites | inlays, onlays, veneers, partial crowns, crowns, and multi-unit, up to three bridge units | Alamoush, Rasha A et al. (2018) [65] Alamoush, Rasha A et al. (2022) [66] Fonseca, Andrea Soares Q S et al. (2017) [67] Marchesi, Giulio et al. (2021) [68] Liebermann, Anja et al. (2016) [69] Monterubbianesi, Riccardo et al. (2020) [70] Alharbi, Amal et al. (2017) [71] Grzebieluch, Wojciech et al. (2021) [72] Schlenz, Maximiliane Amelie et al. (2019) [73] Vichi, Alessandro et al. (2020) [74] Wendler, Michael et al. (2021) [75] |
| Hybrid Ceramics | ||
| PICN | veneers, inlays / onlays, anterior and posterior single crowns and for implant prostheses | Kawajiri, Yohei et al. (2021) [35] Kang, Longzhao et al (2020) [36] Steinbrenner, Harald (2018) [37] Yano, Haruka Takesue et al. (2020) [38] Li, Ke et al. (2021) [39] |
| Nanoceramics | veneers, inlay / onlay, anterior and posterior single crowns, anterior and posterior bridges | Demirel, Akif et al. (2017) [40] Heck, Katrin et al. (2019) [41] Al Amri, Mohammad D et al. (2021) [42] Al-Harbi, Fahad A et al. (2017) [43] Yin, Ruizhi et al. (2019) [44] Ludovichetti, Francesco Saverio et al. (2018) [45] Lauvahutanon, Sasipin et al. (2017) [46] Kurtulmus-Yilmaz, Sevcan et al. (2019) [47] |
Table 3.
Summary of the CAD/CAM Materials included in the study and related to their mechanical properties.
Table 3.
Summary of the CAD/CAM Materials included in the study and related to their mechanical properties.
| Mechanical properties: | Flexural strength (MPa) | Vickers Hardness (VH) | Elastic Modulus (GPa) | References | Manufacturers |
|---|---|---|---|---|---|
| Silicate Ceramics | |||||
| Feldespathic | 97-133 | 640 ± 20 | 45 | [14,20] | CEREC Blocs, VITABLOC |
| Leucite-reinforced | 106-160 | 525-565 | 62-70 | [19-21] | IPS Empress CAD |
| Lithium disilicate | 130 | 452-731 | 58-110 | [21-25] | IPS E.max CAD, Ivoclar Vivadent) |
| Lithium silicate | 400 | up to 7000 | 70 | [22,23] | Suprinity PC (VITA Zahnfabri), Celtra Duo (Densply Sirona) |
| Oxide Ceramics | |||||
| Zirconium | 500–1200 | 12 | 210 | [27-31] | Nobelprocera Zirconia, Nobel Biocare; Lava Plus,3M ESPE |
| Aluminum | 500 | 18.3 | 206 | [32-34] | InCeram Alumina (Vita Zahnfabrik) |
| Resin Matrix Ceramics | |||||
| PMMA | 80 - 135 | 27.7411 | 2.68-3.43 | [48-57] | Telio CAD, Ivoclar Vivadent, VITA CAD-Temp MultiColor Blocks, (VITA Zahnfabrik) |
| PEEK | 165 - 185 | 26.1-28.5 | 4 | [58-64] | Juvora dental PEEK CAD/CAM- Rohling, Straumann, Bio High Performance Polymer, Bredent, Senden, Germany |
| Resin Block Composites | 80 | 65–98 | 2.8 | [65-75] | Grandio Blocks (VOCO GmbH), LuxaCam Composite (LUXA, DMG) |
| Hybrid Ceramics | |||||
| PICN | 107.8–153.7 | 204.8–299.2 | 13.0–2.2 | [35-39] | VITA ENAMIC (Vita Zahnfabrik) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



